BY
R. J. M. BUCHANAN, M.D., F.R.C.P.LOND., &c.
PROFESSOR IN FORENSIC MEDICINE AND TOXICOLOGY,
UNIVERSITY OF LIVERPOOL;
HONORARY PHYSICIAN, ROYAL INFIRMARY,
LIVERPOOL;
FORMERLY HONORARY PHYSICIAN,
STANLEY HOSPITAL;
ASSISTANT HONORARY PHYSICIAN,
LIVERPOOL CHEST HOSPITAL, ETC.
EIGHTH EDITION,
REVISED AND ENLARGED
NEW YORK
WILLIAM WOOD AND COMPANY
MDCCCCXV
PRINTED IN GREAT BRITAIN
The present edition of Forensic Medicine, Toxicology, and Public Health has been issued in two volumes; the first, on Public Health, written by Professor Hope, has been already published separately. Hitherto the subjects have been dealt with in a single volume under the title of Husband‘s Forensic Medicine, but as they are now being taught by different lecturers and in separate classes in most of the medical schools, it has been thought advisable to issue the work in two parts. This volume on Forensic Medicine and Toxicology has been revised throughout, and certain alterations and additions have been made, whilst at the same time the view that the work is intended for students and junior practitioners has not been lost sight of.
The author expresses his indebtedness to Dr. M‘Fall, Demonstrator of Toxicology in the University of Liverpool, for his assistance in revising the section on “Toxicology,” and also to the publishers for the compilation of the index.
Apart from the general bibliography mentioned in the text, the works of Taylor and Stevenson, Dickson, Mann, Glaister, Petersen and Haynes, have been consulted.
A plate, showing the centre of ossification in the lower epiphysis of the femur in a full time fœtus, has been introduced at the last moment, and will be found opposite page 64. References to the subject may also be found on pages 33 and 174.
CONTENTS
| SECTION I | ||
| FORENSIC MEDICINE | ||
| CHAP. | PAGE | |
| Introduction | 1 | |
| I. | Legal Criminal Procedure | 2 |
| II. | Medical Evidence Generally, Identity | 11 |
| III. | Modes of Dying, Sudden Death, Signs of Death | 38 |
| IV. | Post-mortem Examinations and Exhumations, | |
| Instructions of the Crown Office in Scotland | 56 | |
| V. | Assaults, Homicide, and Wounds | 68 |
| VI. | Blood Stains, Spectra, and Biological Tests | 89 |
| VII. | Burns and Scalds, Contusions and Bruises | 110 |
| VIII. | Suffocation, Hanging, Strangling, and Throttling | 118 |
| IX. | Drowning | 127 |
| X. | Death from Starvation, Cold and Heat, | |
| Lightning and Electricity | 132 | |
| XI. | Offences against Chastity | 140 |
| XII. | Pregnancy and Delivery | 150 |
| XIII. | Fœticide, or Criminal Abortion | 159 |
| XIV. | Infanticide, Live Birth, Cause of Death to the Fœtus | 165 |
| XV. | Inheritance, Legitimacy, Impotence and Sterility, | |
| Survivorship, Malpraxis and Neglect of Duty, Feigned | ||
| Diseases, Exemption from Public Duties, Wills | 184 | |
| XVI. | Mental unsoundness, General Symptoms of Insanity, | |
| Mania, Melancholia, Dementia, Restraint of the Insane, | ||
| Forms of Medical Certificates, Testamentary Capacity | 192 | |
| SECTION II | ||
| TOXICOLOGY | ||
| I. | Definition of a Poison, Sale of Poisons, Classification | |
| of Poisons, Action of Poisons, General Evidence | ||
| of Poisoning, General Treatment in Cases of Poisoning, | ||
| General Methods of Examination for Poison | 227 | |
| II. | Division 1: Chemical—Corrosive Poisons | 246 |
| III. | Division 2: Vital—Metalloid Irritants | 267 |
| IV. | Metallic Irritants | 274 |
| V. | Vegetable and Animal Irritants | 317 |
| VI. | Food Poisoning (Bromatotoxismus | 328 |
| VII. | Vegetable Alkaloids | 335 |
| VIII. | Narcotic Poisons | 343 |
| IX. | Deliriant Poisons | 349 |
| X. | Inebriant Poisons | 354 |
| XI. | Sedative Poisons | 364 |
| XII. | Cerebral Poisons | 377 |
| XIII. | Neural Poisons | 385 |
| XIV. | Excitomotory Poisons | 388 |
| XV. | Irrespirable Gases | 397 |
| INDEX |
405 |
|
LIST OF ILLUSTRATIONS
| SECTION I | ||
| FORENSIC MEDICINE | ||
| Plate showing Centre of Ossification in the Lower Epiphysi of | PAGE | |
| Femur in full time Fœtus | To face 64 | |
| FIG. | ||
| 1. | Finger Prints | 24 |
| 2. | Finger Prints | 25 |
| 3. | Photo-micrograph of transverse section of Normal Hair Follicle | 27 |
| 4. | Photo-micrograph of Wool Fibres | 90 |
| 5. | Photo-micrograph of Flax Fibres | 91 |
| 6. | Photo-micrograph of Silk Fibres | 92 |
| 7. | Photo-micrograph of Cotton Fibres | 93 |
| 8. | Measurement of Blood Corpuscles (human) | 97 |
| 9. | Measurement of Blood Corpuscles (sheep) | 97 |
| 10. | Photo-micrograph of Red Blood Corpuscles from Domestic Fowl | 99 |
| 11. | Photo-micrograph of Blood Corpuscles of Fish | 99 |
| 12. | Photo-micrograph of Blood Corpuscles from a Dried Stain of the Blood of a Cod-fish | 100 |
| 13. | Photo-micrograph of a Frog‘s Blood showing oval nucleated Red Corpuscles | 101 |
| 14. | Photo-micrograph of Crystals of Hæmin | 102 |
| 15. | Blood Spectra | 104 |
| 16. | ||
| 17. | ||
| 18. | opposite 121 | |
| 19. | Hymen of Child of Four Years—Annular Type | 144 |
| 20. | Virgin Hymen, with Central Slit | 144 |
| 21. | Photo-micrograph of Human Spermatozoa | 147 |
| 22. | Deflorated Hymen, after Parturition, in Adult Woman | 149 |
| 23. | Abortion at Fourth Week | 159 |
| 24. | Abortion between Sixth and Eighth Week | 160 |
| 25. | Abortion at Tenth Week | 160 |
| 26. | Photo-micrograph of Human Milk | 177 |
| 27. | Photo-micrograph of Starch Granules | 179 |
| SECTION II | ||
| TOXICOLOGY | ||
| 28. | Photo-micrograph of Crystals of Oxalic Acid | 258 |
| 29. | Photo-micrograph of Crystals of Oxalic Acid | 259 |
| 30. | Photo-micrograph of Sublimate of Arsenious Acid obtained by Reinsch‘s Process | 284 |
| 31. | Dowzard‘s Apparatus for Gutzeit‘s Test for Arsenic | 285 |
| 32. | Photo-micrograph of Crystals of Tartarated Antimony | 292 |
| 33. | Photo-micrograph of Crystals of Tartarated Antimony | 293 |
| 34. | Photo-micrograph of Crystals of Corrosive Sublimate | 298 |
| 35. | Photo-micrograph of Globules of Mercury obtained by Reinsch‘s Process | 303 |
| 36. | Photo-micrograph of Crystals of Hydrochloride of Morphine | 339 |
| 37. | Photo-micrograph of Meconic Acid crystallised from Aqueous Solution | 340 |
| 38. | Photo-micrograph of Meconic Acid crystallised from an Alcoholic Solution | 340 |
| 39. | Photo-micrograph of Crystals of Cyanide of Silver obtained by the Vapour Test | 372 |
| 40. | Photo-micrograph of Crystals of Strychnine Sulphate from an Aqueous Solution | 389 |
| 41. | Photo-micrograph of Crystal of Strychnine Sulphate from Aqueous Solution | 389 |
| 42. | Photo-micrograph of Strychnine Sulphate, Film Preparation from Chloroform Solution | 391 |
| 43. | Photo-micrograph of Chromate of Strychnine | 391 |
| 44. | Photo-micrograph of Sulphocyanate of Strychnine | 392 |
| 45. | Photo-micrograph of Crystals of Brucine Sulphate | 395 |
| 46. | Photo-micrograph of Crystals of Brucine Sulphate | 395 |
FORENSIC MEDICINE
AND TOXICOLOGY
Medical Jurisprudence, Forensic Medicine, or Legal Medicine are terms for that science which teaches the application of the knowledge of all branches of medical and surgical science and art to the solution of every question connected with the conservation of the species and the administration of Justice. We find traces of this science in the Jewish law; among the Egyptians, according to Plutarch; and even among the Romans as early as the times of Numa Pompilius. Among German writers the term State Medicine includes both Medical Jurisprudence and Medical Police, Public Health, or Sanitary Science.
The special knowledge requisite to the Medical Jurist differs in many ways from that requisite for the art of healing the sick. The majority of medical students and practitioners may consider a simple exercise of common sense in the application of their general professional knowledge to the elucidation of problems of medico-legal import all that is requisite, and that no special training is necessary for the purpose. They may hope that it may never fall to their lot to be called upon to act in the capacity of medical jurists. It may occur, however, to any medical practitioner at any time of his professional career that his services be requisitioned by law for the purpose of elucidating problems of such a nature as will demand from him thought and judgment quite apart from those he exercises in the ordinary course of his medical and surgical practice. From such a requisition he has no escape; he cannot shift his responsibility to another, and it behoves him, therefore, to acquire a knowledge of Forensic Medicine, in order to guide him, when so called upon, to give such evidence as will enable a judge and jury to arrive at a just conclusion. The relations of all medical practitioners to the State are twofold—first, as healers of disease, and secondly, both as guardians of the innocent against unfounded criminal charges and aids towards the detection and punishment of crime.
The Coroner‘s Court.—The office of coroner is mentioned in a charter in 925. Coroners were formerly chosen for life by the freeholders of the district, but their election is now in the hands of the County Councils. Their duties were first clearly pointed out by the Act 4 Edw. I. c. 2, 1275 (De officio coronatoris).
At the present time the duties of the coroner are chiefly to hold inquiry into the cause of death when there is any reason to doubt that death resulted from natural causes.
When death results from natural causes, and under ordinary conditions, the medical attendant is bound, under a penalty of forty shillings, to certify as to the cause. The registrar of deaths accepts such a certificate when accompanied by oral testimony given by a person who was present at the time of death, and issues a certificate accordingly, authorising the interment of the deceased.
Should conditions obtain to prevent the medical attendant from forming an opinion as to the cause of death, or which would lead him to infer that death did not take place from natural causes, he should notify the matter to the coroner. Such would be necessary if death were directly or indirectly due to accident, or if death occurred within a reasonable time after an accident, although due to some other cause, or if an accident happened to deceased during the course of a chronic illness, the accident, however, not being in itself necessarily fatal.
It would be necessary also to notify the coroner if the death took place under circumstances which, to the medical attendant, appeared suspicious, such as might arise from culpable neglect or cruelty on the part of persons in charge of the deceased. The same would apply to cases in which the cause of death was unknown. A great responsibility rests on the medical practitioner, in that he is compelled under a penalty to certify as to the cause of death; while if he do so without due consideration, or carelessly, he renders himself liable to censure or legal proceedings.
It may happen that in certain cases—for example, where an accident befell the deceased during the course of a lingering illness, and which in itself had no causal relations to the death—the doctor may be prone to certify the death as from the illness alone, taking no note of the accident; and pressure may be brought to bear upon him by the relations of the deceased to so certify and save them the trouble and publicity [Pg 3] of an inquest. It should be remembered, however, that although the certificate be accepted by the registrar, and interment take place, the coroner, if informed of the matter, may order the body to be exhumed for the purposes of inquest.
There are coroners who, on receipt of information of death from uncertain causes, may elect, on evidence obtained apart from the medical practitioner, to notify the registrar authorising the interment without holding an inquest. The law, however, states that, “except upon holding an inquest, no order, warrant, or other document for the burial of the body shall be given by the coroner” (50 and 51 Vict.).
The Coroners Act (50 and 51 Vict.) provides that, when a coroner is informed that the dead body is lying within his jurisdiction, and there is reasonable cause to suspect that such person has died a violent or unnatural death, or a sudden death, of which the cause is unknown, or died in prison, he shall summon a jury of not less than twelve, or more than twenty-three, men to inquire touching the death of such person aforesaid.
If the deceased were attended at his death, or during his last illness, by a legally qualified medical practitioner, the coroner may summon such practitioner as a witness. If the deceased were not so attended in his last illness, the coroner may summon any legally qualified medical practitioner in actual practice, in or near the place where the death happened, to give evidence as to the cause of death. In either case the coroner may require the medical witness to make a post-mortem examination of the body, with or without analysis of the contents of the stomach or intestines.
Should a statement on oath be made by any one before the coroner, that in his belief the death of the deceased was caused partly or entirely by the improper or negligent treatment of a medical practitioner, such medical practitioner shall not make or assist at the post-mortem examination.
If a majority of the jury are not satisfied with the medical evidence, they may require the coroner, in writing, to summon another legally qualified practitioner, named by them, to make a post-mortem examination, with or without analysis of the contents of the stomach and intestines, and give evidence as to the cause of death. A medical practitioner who fails to obey the summons of a coroner, issued in pursuance of the Coroners Act, is liable to a penalty not exceeding five pounds, unless he shows good and sufficient cause for not having so done. When evidence has been given before a coroner or magistrate, and the case is afterwards sent for trial, copies of the medical report and depositions are given to the judge and counsel, so that evidence given at the trial is compared in detail with that given before the coroner or magistrate. In view of this, it is imperative on the part of medical witnesses to carefully consider their evidence before giving it.
The object of a coroner‘s inquest is to ascertain whether the death of the person, over whose body the inquest is held, was due to natural causes or not. [Pg 4]
The proceedings are not directed against any one, they do not constitute a trial, and hearsay evidence is admissible. The coroner and jury alone have the right to interrogate the witnesses. Counsel may be present in the interest of persons concerned with the inquest who may desire such assistance, but counsel may not cross-examine any witnesses, and may only question them by permission of and subject to the decision of the coroner.
Witnesses are examined on oath, their evidence is taken down, and should the case be transferred to a superior court, they are bound under a penalty to appear and give evidence. The coroner may adjourn an inquest for the purpose of obtaining further evidence, if he should deem it necessary.
Should the verdict of the jury charge a person with murder, the coroner issues a warrant for the arrest of the person, unless the person be already in custody. In the case of manslaughter the coroner may accept bail. According to the Act 4 Edw. I. c. 2, the coroner and jurors must view the body, this being absolutely necessary to give jurisdiction to him, and he has the power, within a convenient time after the death, to order a dead body to be disinterred for this purpose.
Order of Summons from the Coroner to a
Legally Qualified Medical Practitioner
Prosecution.—There was no Public Prosecutor in England until some years ago, when an Act was passed authorising the appointment of such an official, who should undertake the duty of prosecuting in certain and specific cases of public importance, and in districts where the appointment might be agreed upon. In ordinary circumstances it has usually been left to the person against whom a crime has been committed to prosecute the offender.
Magistrates‘ Court.—In the Magistrates‘ Court of Petty Sessions, the proceedings are for the purpose of investigating as to the culpability or non-culpability of a person accused of some criminal act, or criminal negligence. [Pg 5]
In this Court the accused person must be present, as the inquiry is relative to his guilt or innocence. Witnesses in this Court may be examined and cross-examined by counsel. A magisterial investigation cannot take place if no arrest have been made. The magistrate may deal summarily with cases of simple assault and such-like of minor import, but when the case is of a more serious nature, and in suspected manslaughter or murder, the accused person is committed to a superior Court for trial, such as the Court of Quarter Sessions, the Assize Court or, in London, the Central Criminal Court, all witnesses, medical or lay, being bound over to appear and give evidence. The summons to the Assizes is called a subpœna, and all witnesses receiving the same, when accompanied with reasonable travelling expenses, are bound to obey it.
Assizes.—The Assizes comprise two Courts, the Crown Court and the Civil Court. A separate judge presides over each. In the former only cases of a criminal nature are tried; in the latter suits are tried between two parties. Medical practitioners may be called upon to give evidence in either Court, according to the nature of the case in which they are directly concerned.
Prior to a case being investigated by a judge and petty jury, it has to come before the grand jury. This jury decides whether the case is a proper one to proceed to trial.
The grand jury hear the evidence of such witnesses as they think fit, apart from counsel. Should the grand jury consider the case one for trial, they return a “true bill,” and it goes before the judge and petty jury; if not, they “cut the bill,” and the accused is discharged.
Medical witnesses may be called upon, when under subpœna, to give evidence before the grand jury.
The Crown Court of Assize consists of a judge and a sworn jury of twelve men, called the petty jury. The latter hear the evidence of witnesses, and are guided by the summing up of the judge. They deliver a verdict after consideration of the evidence by which the accused person is found guilty or not guilty. The judge, after receiving the verdict, allots such punishment as he considers just. In certain cases the prisoner when convicted may appeal to the Court of Criminal Appeal.
In the Assize Courts only barristers can plead; in the Magistrates‘ Courts of Petty Sessions, solicitors or barristers may plead.
In the Courts of Assize the witnesses are subject to the following routine of examination. First, Examination-in-chief: this the witness undergoes at the hands of the barrister who is pleading on behalf of the party by whom the witness is called. In this examination such questions are put to the witness as may elicit answers conveying to the judge and jury a clear account of all the witness knows with regard to the case. After the examination-in-chief, the counsel of the opposite side subjects the witness to cross-examination, in such a way as to shake the evidence given by the witness during his examination in chief in points which would weigh against the prospects of his client. It is during cross-examination that a medical witness [Pg 6] may be subjected to questions which suggest answers capable of a different interpretation from those he had previously given. After cross-examination, the counsel for the party upon whose side the witness appears subjects the latter to re-examination, if he consider it necessary, during which he endeavours to clear up any doubtful points in the evidence given by the witness during cross-examination, with the purpose of eliciting an explanation of their meaning.
The judge and members of the jury may put such questions to the witness as they may consider necessary.
The same method of procedure applies to the higher Courts.
In Scotland public prosecutors are appointed by the Crown. The chief public prosecutor is the Lord-Advocate; next in rank come the Deputy-Advocates and Procurator-Fiscal. The Lord-Advocate and Deputies take charge of cases in the High Courts of Justiciary, the Procurator-Fiscal in the lower Courts.
The duties of the public prosecutor are to bring all accused persons to a bar of justice; and in addition he acts as the coroner does in England. Any person who is supposed to know anything about the case is interrogated by the Procurator-Fiscal, or is precognosced. The examination is made on oath; the written evidence constitutes the precognitions. Counsel for the accused or for the Crown may precognosce witnesses.
The preliminary examination of the accused takes place before the Sheriff or Justice, and he may commit the person for trial or liberate him, according to the evidence.
The precognitions, in cases of committal, are forwarded to the Crown Counsel in Edinburgh, who may stop the proceedings, or send the accused before the High Court, Circuit Court of Justiciary, or Sheriff, with or without a jury. The Justiciary Courts correspond to the Courts of Assize in England. Should the case be so transferred for trial, the witnesses are summoned by writ. A penalty of £5 may be imposed for disobedience to such writ, or imprisonment pending expression of regret before the Court, and tendering bail for appearance.
Common witnesses and medical witnesses to fact are not allowed in Court except when giving evidence. Expert witnesses may be allowed to remain in Court by mutual consent of counsel. When one expert witness is giving evidence, other experts are required to leave the Court, and no expert witness who may have been present during the examination of common witnesses is allowed to give evidence as to facts.
The verdicts of “Guilty” or “Not guilty” are similar to those given in England, but in addition a verdict of “Not proven” may be given, and all are final. In the case of the last two the accused cannot be tried again.
In Scotland the verdict of a bare majority of the jury holds good, whereas in England the decision must be unanimous. In the case of a suspicious death, or a dead body being discovered, [Pg 7] the Procurator-Fiscal, acting as a coroner does in England, but without a jury, may direct a medical man to examine the body and send in a report; but all reports must be certified on soul and conscience, without which they are of no value. Should the medical examiner be satisfied without making an internal examination, he may certify to the Procurator-Fiscal on the result of his external examination.
Should the Procurator-Fiscal consider it requisite to have a complete examination, he issues a warrant to that effect to the medical practitioner who has seen the case, and usually associates with him the most skilled practitioner available in the neighbourhood. The warrant consists of a petition by the Procurator-Fiscal, addressed to the local judge, setting forth the grounds of his application, and craving warrant to the inspectors named to make the necessary examination. This is signed by the Procurator-Fiscal, and countersigned by the Sheriff or local judge, if granted. The receivers of this warrant are empowered to take full custody of the body, and they should be careful to carry the warrant with them, or they may be refused admission pending its production, which may result in great waste of time, and end in a miscarriage of justice. The Procurator-Fiscal may supply to the medical inspectors portions of the precognitions likely to bear on the medical part of the inquiry. Medical men ought to be on their guard against performing dissections in cases evidently judicial without previously warning the proper law authorities, or without a warrant; for instances have occurred where, owing to the want of proper support, obstructions were thrown in the way which might have proved fatal to the value of the investigation; and, besides, the premature disclosure of the results of the inspection might frustrate other important steps of the precognition.
The medical men so engaged will, as a rule, find it to their interest to exclude all visitors, whether lay or professional, from the room during the dissection. The regulations issued by the Crown Office, Edinburgh, direct that no one should be allowed to be present at the examination out of mere curiosity, and recommend that any one not engaged in the inspection, but who is in attendance to give information, or for any other purpose, and who may afterwards become a witness, should remain in an adjoining room. The medical inspection often furnishes good tests of the value of other evidence in the case; therefore, it is desirable that the general witnesses should not have an opportunity of knowing what is observed in the dissection of the body. The notes of a case should be made at the time of inspection or immediately afterwards. In the case of post-mortem examinations it is better that while one inspector conducts the practical details of the examination, the other should take notes of its successive steps, indicating all the points inquired into, with the observations made, the appearances presented, negative as well as positive, stating simple facts alone, without either generalisations or opinions. These notes should be looked over by both inspectors before the body is sewn up, so that omissions in the notes, or in the inspection itself, may be then supplied. [Pg 8]
In England, except upon a subpœna, a medical man is not bound to attend as a witness at a trial, and then it should be served a reasonable time before the trial, in order that he may make proper arrangements for the carrying on of his business during his absence. In civil cases his reasonable expenses should be tendered to him at the time the subpœna is served, or within a reasonable time of the trial; and he may refuse to give evidence unless his charges are paid, provided his objection be stated before he has been sworn. A witness may be summoned from any part of the United Kingdom.
The question has been raised, whether a scientific witness was bound to attend when subpœnaed. The law on the point is enveloped in some obscurity; the better course is therefore to attend.
No tender of fees is necessary in criminal cases, “except in the case of witnesses living in one distinct part of the United Kingdom being required to attend subpœnas directing their attendance in another, who are not liable to punishment for disobedience of the process, unless at the time of service a reasonable and sufficient sum of money, to defray their expenses in coming, attending, and returning, have been tendered to them.” When summoned to two cases, the one civil, the other criminal, the witness must attend the criminal; or when both cases are the same, the one to which he first received the subpœna—notifying, however, to the counsel engaged on the other case his unavoidable absence, and giving the reasons which prevent his attendance.
In Scotland, witnesses are summoned by a writ or citation, which must be delivered at the residence of the witness a reasonable time before the trial. Delivery to a member of the family, or a servant not within the house, will not do. If access cannot be gained, the copy is fastened to the most patent door of the house. If the witness do not appear, and it be clearly shown that he was duly cited, a warrant for his apprehension may be issued, and he becomes liable to be incarcerated till he finds “caution” for his due attendance at the trial. His non-attendance may also, unless good excuse be forthcoming, render him liable to a fine, or unlaw, of a hundred merks Scots—about £5.
Form of Subpœna in England.—Where a medical witness has given evidence in a case in which the accused person has been committed for trial to a superior Court, he is summoned to give evidence at such Court in the following terms:
“George, by the grace of God, of the United Kingdom
of Great Britain and Ireland, King, Defender of the Faith,
To ______________________
Greeting: We command you, and every
of you, that all business being laid aside, and all excuses
ceasing, you do in your proper persons appear before our
Court of Quarter Sessions of the Peace (or other Court),
assigned to keep the peace in the City (or Borough) of
__________________________, and also to hear and determine
divers Felonies, Trespasses, and other Misdemeanours in our
said City (or Borough) committed, to be holden within the
_______________________, in the said City (or Borough),
on ____________________ the _______ day of _________
now next ensuing, at the hour of ten o‘clock in the forenoon
of the same day, to testify the truth and give evidence,
on our behalf, against __________________ in a case of
_____________; and this and every of you are in no wise to
omit, under the Penalty of Twenty Pounds for you and every
of you. Witness, ___________________, Esq., our Recorder
at ____________ aforesaid, the ________ day of _________
in the ________ year of our reign.”
In Scotland the following is the form of summons to appear before the High Court of Justiciary, and at an inquiry into a fatal accident:
(I.)
“To _________________________________________
“You are hereby lawfully cited to attend a sitting of the
High Court of Justiciary within the Criminal Court
__________, upon the ___________ day of _________
Nineteen hundred __________ years, at ____________
o‘clock _______ noon, as a witness in the case against
_______________________, prisoner in the Prison
of _______________, and that under the pain of
One Hundred Merks Scots.
“Note.—Any witness failing to appear in terms
of citation not only forfeits the penalty, but is
liable to be apprehended and imprisoned.
“(Preserve and bring this Copy with you.)”
Coroner‘s Court.—The Coroners Act states that fees for medical witnesses attending an inquest shall be, for attending to give evidence at an inquest whereat no post-mortem examination has been made by the witness, one guinea. For making a post-mortem examination and attending to give evidence, two guineas. No fee can be obtained for making a post-mortem examination by a medical practitioner, unless it be made by order of the coroner. Extra fees are not provided for when the inquest is adjourned. For an inquest held over the body of a person who has died in a lunatic asylum, public hospital, infirmary, workhouse infirmary, or other medical institution, whether endowed or supported by voluntary contributions, the medical officer of such institution shall not be entitled to a fee. Should the dead body of a person be taken to such an institution, the medical officer, if summoned to give evidence, is entitled to the usual fee. Such fees are paid at the termination of the inquest. [Pg 10]
Magistrates‘ Court.—If the witness reside within two miles of the Court, the fee is ten shillings and sixpence; beyond two miles, one guinea.
Courts of Quarter Sessions, and Central Criminal Court of London.—One guinea per day, and two shillings a night away from home, with threepence per mile each way travelling expenses.
Assize Court.—One guinea per day, with two shillings a night away from home, and a reasonable and sufficient amount for travelling expenses. If there be no railway, threepence a mile each way. Sundays are not included.
Court of Probate and Divorce.—One guinea per day within five miles of the General Post Office. If beyond, two or three guineas a day, with expenses out of pocket for coming and returning.
Court of Appeal.—One guinea a day if resident in London; two or three guineas, with travelling expenses, if from a distance.
County Court.—From fifteen shillings as an ordinary witness, with one guinea per day expenses if from home, to one to three guineas for qualifying as an expert witness. With attendance at Court one to two guineas and expenses one to three guineas per day.
In Civil Cases.—An arrangement is usually made with the solicitor for a fee; this should be made before accepting the subpœna. A written undertaking for payment, and properly stamped, should be obtained from the solicitor before giving evidence; in default of this, the witness should appeal to the judge from the witness-box before being sworn. After taking the oath a witness is bound to give evidence, and the solicitor may refer him to his client for the fee, which may lead to disappointment.
IN SCOTLAND
The fee for attendance at High Courts of Justiciary or the Sheriff Criminal Court is one guinea per day, if the Court be held in the town in which the medical witness lives. For a post-mortem examination and report, two guineas. For an analysis of blood or other stains on clothing, two to four guineas, depending upon the amount of work done.
If the witness come from a distance, he is allowed two guineas per day, both for the actual attendance at Court and also for each day occupied in travelling to and fro, with a guinea a day for travelling expenses.
On the subject of evidence it is necessary to say a few words, for it must be remembered that that which may be held to be evidence in logic may not be so in law. Nothing in law is intuitive—nothing is self-evident; everything must go through the process of proof by testimony.
Legal evidence is therefore composed of testimony, but all testimony is not necessarily evidence in law. Thus, if a witness declare that he saw a certain act committed, his testimony may be accepted as evidence; but if he state that his knowledge of a fact is obtained from another person, such information, although it contain an absolutely true description of what actually occurred, will not be received. In this case his testimony is simply hearsay, and as such is not admissible, except in the case of dying declarations, and in one or two other instances which do not, however, concern us.
Medical evidence may be divided under the following heads: (1) Documentary; (2) Oral or Parol; (3) Experimental.
Under this head are included Medical Certificates, Written Opinions, Medical Reports, and Dying Declarations.
Medical Certificates.—Certificates generally refer to death, to vaccination, to notification of infectious and industrial diseases, and in districts which have adopted it, the notification of births; to the state of health of an individual, &c. For those which have respect to the health or to the illness of an individual there is no particular legal form, as a certificate is merely a simple statement of a fact. The only essential condition is that it contains the exact truth, and any departure from this will entail heavy penalties. A statement signed by a registered medical practitioner, distinctly describing the condition of A or B, is all that is necessary as far as the law in England is concerned. In Scotland the law is somewhat different, for “A certificate of bad health by a physician or surgeon must bear to be on soul and conscience.” ... “In cases of homicide, and other crimes against the person, medical certificates produced respecting the nature of the injuries must be verified on oath by the medical persons who granted them” (Dictionary Scot. Law). In Scotland, the omission of the words “on soul and conscience” invalidates a certificate.
Certificates of death, of vaccination, of notification of infectious diseases, tuberculosis, industrial diseases, and births, and of insanity can be procured already printed in the forms prescribed by the law.
Certificates of the Cause of Death.—A medical practitioner who has been in attendance during the last illness of a person is legally [Pg 12] bound to give a certificate stating, “to the best of his knowledge and belief, the cause of death.” If he be unaware of the cause of death, or have reason to believe that death was not due to natural causes, or the result of violence, he may refuse the certificate. In such a case it is customary and desirable for the medical man to notify the Coroner of the circumstance as soon as possible. If he have no reasonable cause to prevent him supplying the certificate, he is liable to a penalty not exceeding forty shillings. In England and Ireland it is given to a relative of the deceased or legally authorised person, who must deliver it to the Registrar. In Scotland the doctor sends it to the Registrar direct. Not more than one certificate should be given. No fee is chargeable. The information on the certificate should be as clear, complete, and accurate as possible.
Notification of Births.—When the authorities of any district have adopted the Notification of Births Act of 1907, it is the duty of any person who has been in attendance on the mother at the time, or within six hours after the birth, to give notice of the birth in writing to the Medical Officer of Health of the district in which the child is born. The necessary certificate must be filled in and posted to the Medical Officer of Health within thirty-six hours of the time of birth. The certificate applies to any child dead or alive born after the twenty-eighth week of pregnancy. Should the relatives of, or other attendant upon the mother, fail to notify the birth, it is the duty of the medical attendant to do so, failing which he may be fined not exceeding twenty shillings.
Notification of Infectious Diseases.—By the Act of Parliament 1889, every medical practitioner attending on or called in to visit the patient, shall forthwith, on becoming aware that the patient is suffering from an infectious disease to which the Act applies, send to the Medical Officer of Health of the district a certificate stating the name of the patient, the situation of the building, and the infectious disease from which in the opinion of such medical practitioner the patient is suffering.
The notifiable diseases are: smallpox, cholera, diphtheria, membranous croup, erysipelas, scarlatina or scarlet fever, typhus, typhoid, enteric, relapsing, continued and puerperal fever.
By consent of the Local Government Board the Health Authorities may add other diseases as occasion may require for a time or permanently. Of these due notice is given to medical men. Tuberculosis and ophthalmia neonatorum are now notifiable. The fee for the certificate in private practice is 2s. 6d., if in a public institution, 1s. Failure to certify renders the medical man liable to a penalty of 40s.
Notification of Tuberculosis.—As mentioned previously, tuberculosis is now a disease notification of which is compulsory. Special forms are provided for the purpose.
Notification of Industrial Diseases.—Under the Factory and Workshop Act, 1901, every case of lead, phosphorus, arsenical, or mercurial poisoning, or anthrax, if contracted in a factory or workshop must be notified by the practitioner in attendance on the case. The certificate must be sent to the Chief Inspector of Factories at the Home [Pg 13] Office, London. The fee for notification is 2s. 6d. Other diseases may be added to the list by special order of the Home Office.
Written Opinions.—These generally refer to civil questions.
The Medical Report.—A Report is a document given in obedience to a demand by the public authorities in Scotland, and has reference chiefly to criminal cases. Medical Reports are sworn to as true by those who draw them up. According to Alison, it is not a sufficient objection that a Medical Report was made up at an interval after the occurrence of the circumstances to which it refers. The same high authority also states that should the writer of a Medical Report die before the trial, his Report may be used in evidence,—this may be doubted.
The necessity for simplicity in the arrangement and in the wording of their Reports cannot be too strongly urged on medical men. “A medical witness will do well to remember, also, that copies of his Report and depositions, either before a coroner or a magistrate, are usually placed in the hands of counsel as well as of the Court; and that his evidence, as it is given at the trial, is compared word for word with that which has already been put on record.” All hearsay statements and irrelevant matter should not be inserted in a Report; and the reporter should be particularly careful not to add any comments to his simple narration of facts. The use of superlatives is also very objectionable, as it partakes somewhat of exaggeration. All technical words or phrases should be as much as possible avoided; and where they are absolutely necessary, they should be briefly explained.
As a case in point, showing the necessity for care in the use of words, is the following from a published Paper by the late Sir R. Christison: “Some years ago, on an important trial in the High Court of Justiciary for assault, the public prosecutor attempted to prove that the person assailed had been wounded to the effusion of blood; which is held in law to be an aggravation of guilt in such cases. When the principal medical witness was examined as to the injuries inflicted, he was asked whether any blood had been effused; and he replied that a good deal must have been effused. But he meant that there was effusion of blood under the skin, constituting the contusion he had described; while the counsel and the Court at first received his answer as implying that there had been considerable loss of blood from a wound. The latter view was on the point of passing to the jury as a fact, when one of the judges detected the equivoque, and set the matter to rights.”[1]
In Scotland a medical practitioner may be called upon by the authorities to grant reports as to dead bodies, without performing a post-mortem examination.
In the first case, where a death has occurred unaccompanied by any suspicious circumstances, or where the evidence of suicide or death from accidental injury is apparent from a simple examination of the [Pg 14] body, a certificate “on soul and conscience,” stating the probable cause of death, is considered sufficient by the authorities, and a post-mortem is dispensed with. It is not necessary that the deceased be seen by the medical practitioner before death, “yet, from the suddenness of the death, the age of the deceased, and the symptoms spoken to by the friends, he may still be enabled, satisfactorily to himself, to certify the cause of death.” In England, such a case would be the subject of a coroner‘s inquest.
In the second case, he may be summoned by a constable to inspect a body found on the public road, or in any other unusual situation. In this case he is called not only to certify the fact, but also the probable cause of death. He may, under these circumstances, give a report of the external examination of the body, at the same time suggesting the necessity for further and more careful examination by dissection, &c., and this is considered the proper course for him to take. In England, in this case also, an inquest would be necessary. In all cases medical men will consult their own interests in giving these Reports.
A Medical Report consists of two parts—the Minute of the Examination, and the Reasoned Opinion on the first portion of the Report. In the case where the Report is made by two or more persons appointed for the purpose, the latter portion is written in the plural, and signed by each of the parties certifying.
The following is an outline of a Medical Report, which may be more or less modified to suit the requirements of the case:
FORM OF MEDICAL REPORT
(Date.)(Place of Examination.)
(Names of those who can speak to the Identity of the Body.)
I. MINUTE OF THE EXAMINATION
1. External Inspection
1. General Condition of the Body.—(a) Well or ill nourished.
(b) General colour. (c) Marks and scars. (d) Products of
disease—Ulcers, hernia, &c. (e) Injuries.
Caution.—There may be no external marks of injury, and
yet death may be due to violence. Extreme difficulty in
deciding if injury be inflicted before or after death.
2. Height.—Determined by measurement.
3. Age.—This can only be approximately guessed.
4. Sex.—This is, of course, only difficult when
putrefaction is far advanced. Hair found only on the
MONS VENERIS or PUBES
is characteristic of the female,
but if it extend upwards on the abdomen, equally so
of the male. No sex can be distinguished in the
embryo before the third month of intra-uterine life.
5. Colour of the Eyes.—Difficult of determination.
Why?
(a) Disagreement of observers.
(b)Presence of putrefaction.
6. Colour of the Hair.—This is necessary, in order to compare
hair of deceased with that found on suspected party.
7. Position of the Tongue.—Normal or abnormal, injured
or uninjured.
8. Condition and Number of the Teeth.—(a)Complete.
(b) Incomplete. (c) Any peculiarity as regards size
or form,
in order to compare with mark or bite on suspected party, &c.
[Pg 15]
9. Signs of Death.—Presence or absence of the
rigor mortis
or supervening putrefaction.
10. Condition and Contents of the Hands and Nails.—
(a) In the drowned: weeds, sand, and signs of long immersion.
(b) In those shot:scorching or blackening of the hand from powder,
or injury from recoil of the weapon.Is the weapon grasped firmly
in the hand? Cadaveric spasm? Cadaveric rigidity?
11. Condition of the Natural Openings of the Body—Nose,
Mouth, &c.—(a) Presence of sand or weeds in mouth
of those found in the water. (b) Presence of marks of
corrosive poisons. (c) Presence or absence of the
signs of virginity, or of recent injury about the parts.
12. Condition of the Neck.—(a) Presence of marks of
strangulation.
(b) Condition of the upper cervical vertebræ.
(c) Dangers to be avoided in determining the fracture or dislocation
the cervical vrtebræ. Great mobility of neck, sometimes present,
not due to injury of the bone.
II. THE REASONED OPINION
In this portion of the Report the inspectors state the nature of the conclusion at which they have arrived, and their reasons.
Recapitulation of the foregoing Rules.—It may be of advantage here to restate, in a tabular form, a few suggestions as to the composition of the Report:
N.B.—1. Let the Report be as short as possible, but state your views with clearness and distinctness. After stating the nature of the disease in any organ, report “all other organs healthy,” if they have been found so. To specify some organs, omitting others, may lead to a pressing inquiry from counsel as to the condition of the supra-renal capsules, or some other organ, and an unfounded doubt cast on the Report of the examiner. [Pg 16]
2. Always avoid the use of technical terms as far as possible, so that you may be saved the annoyance of having to explain your meaning in the witness-box.
3. Express all dates and numbers in writing. Measure all marks, and describe their size and appearance in writing. Carefully write all names of persons to whom reference is made. Take accurate notes, and from them compose your report. Make a list of all articles submitted for inspection and analysis, and label them.
4. State all facts clearly and chronologically. A fact is what is known directly and personally to witness, and not what has been repeated by some other person. Do not report hearsay testimony as matters of fact.
5. Every report should be written under the impression that it may come into court to be read.
6. Always avoid superlatives and all epithets of feeling or impressions on the mind.
7. Always avoid speculative opinions and reference to moral circumstances, unless specially required to do so.
8. State your conclusions at the end of the Report in as few sentences as possible.
9. Keep a rough draft of all your Reports, for future reference.
10. Transmit Report, signed and dated, without unnecessary delay, to the proper authorities.
Dying Declarations.—The principle on which these are accepted is founded, partly on the awful situation of the dying person, and partly on the absence of interested motives in one on the brink of eternity, and which is supposed to obviate the necessity of a cross-examination. The law presumes that any one cognisant of impending death will tell the truth, and such declarations are equal to evidence on oath. The greatest care must be taken by the medical man who is called in to see a person supposed to be dying, with regard to any declaration he or she may wish to make. He must be satisfied as to the mental condition of the person. The medical attendant should simply take the statement as it is made, writing it down on the spot, or as soon after as possible. The identical words used should be committed to paper, and no suggestions or interpretations of his own should be made. Leading questions should never be put, nor any attempt made to induce the patient to make any statement. When we consider the condition of the patient, the possibility of delirium induced by the severity of the injury, together with the dread of death, it is, to say the least, injudicious to introduce the suspected party into the room for the purpose of identification, though this procedure has been suggested by some writers. In every case, however, it is advisable for the medical attendant, as soon as he sees that the case must end fatally, to acquaint the patient in the presence of others of the fact, when any statements made may then be taken. It is preferable that such statements be made before a magistrate if time will allow. It should also be borne in mind by those receiving dying declarations, that in England “it must be shown that the deceased, at the time he made the statement, was under the impression that death was impending; not merely that he had received an injury from which death must ensue, but that, as the popular phrase goes, ‘he then believed he was on the point [Pg 17] of death’” (R. v. Forester). In one case (R. v. Fagent, 7 C. & P. 238) it was held that a declaration was inadmissible, because the person making it asked some one near her whether he thought she would “rise again”; and it was held that this showed such a hope of recovery as rendered the previous declaration inadmissible. The declaration should be signed by the person making it, and witnessed by some one present at the time.
In the case of Reg. v. Whitmarsh (Central Criminal Court, Sept. 19, 20, 21, 1896), 62 J.P. 680. Upon an indictment for the murder of a woman, who died as the result of the prisoner having used certain instruments or other means upon her with the intent to procure her miscarriage, it was shown that an inspector of police had seen her at Charing Cross Hospital. He asked her questions, and from her answers he wrote down a statement. The woman signed it. On July 7 the woman appeared to be in a dying condition, and was aware of it. She said she feared she must die, and asked to see her mother and a clergyman. The doctor told her that he had given up all hope, and that she might not live to see her mother. A magistrate saw her shortly afterwards, and read over to her the statement she made on June 29, and he affixed to it the following note, “This statement was read over to Alice Bayley by me, and is referred to in her dying declaration,” and signed. Held (Darling, J.), that though this statement might be admissible, it had better not be admitted in evidence. On the same day the woman had also made a statement to the magistrate, of which he had taken note, but before it was finished she became exhausted. The magistrate then took the statement of June 29, repeated portions of it to her in his own words, wrote these down, and asked her if it was correct. He then read the whole statement to her and she signed it. The statement commenced, “Having the fear of death before me, and being without hope of recovery”—concluding with the words, “And the statement I made on the 29th of June, and have now heard read over, is true.”
Justice Darling held this statement was admissible as a dying declaration.
In the case of Rex v. Smith, 65 J.P. 426 (Bruce, J., Central Criminal Court). A magistrate and a doctor visited a dying woman for the purpose of taking her statement. In reply to a question put to her by one of them, she said, “I am aware that I am seriously ill.” The magistrate asked her questions and the doctor wrote down the answers. At the trial the statement was objected to as inadmissible as a dying declaration on two grounds: Firstly, that the statement consists only of answers to questions put to her by the magistrate, and so comes within the ruling of Cave, J., in Reg. v. Mitchell, 17 Cox C.C. 503, that “a declaration should be taken down in the exact words which the person who makes it uses, in order that it may be possible from those words to arrive precisely at what the person meant. When a statement is not the ipsissima verba of the person making it, but is composed of a mixture of questions and answers, there are several objections open to its reception in evidence.... In the first [Pg 18] place, the questions may be leading questions, and in the condition of a person making a dying declaration there is always very great danger of leading questions being answered without their force and effect being fully comprehended.”
Secondly, the prosecution had not shown that at the time the woman made the statement she was in expectation of immediate death.
The judge held (1) That the prosecution had not proved that in her own opinion the woman was beyond all hope of recovery, and that therefore the statement was inadmissible; (2) That such a statement—the magistrate asking her questions and the doctor taking down only her answers in writing—was not admissible as a dying declaration.
In the case of Rex v. Holloway, 65 J.P. 712 (Wills, J., Central Criminal Court). The prisoner threw a burning lamp at his stepson and set fire to his stepdaughter, who succumbed to the burns she received. A deposition of the deceased girl was taken down by a magistrate. At the time it was taken it was intended that it should be in accordance with the provisions of the 1867 Act. The accused was present and had full opportunity of cross-examining the witness. The deposition was read over to the girl, and she assented to it, but could not sign it because of the injuries to her hands. The magistrate who took the deposition signed it. It was held that the deposition had been taken in accordance with the provisions of the Indictable Offences Act, 1848, sec. 17, and was admissible though it had not been signed by the girl.
The validity of a dying declaration has been called in question when made by a person who has suffered a severe concussion of the brain, and then recovered his sensibility. It is well known that under such circumstances the recollection of what took place before or after the injury is in many cases very imperfect, and the injured party may thus draw unintentionally upon his imagination for his facts. In Scotland, “the written deposition of a person who is dead is admissible, whether the person were the party injured or not, if he would have been a competent witness. It is not necessary that the deceased believe himself to be dying when he emits the deposition, for his consciousness of approaching death may be inferred from the nature of the wound, or the state of illness or other circumstances of the case. Such depositions are generally taken by a magistrate, but a declaration deliberately made, though without an oath, and taken down ‘by a creditable person,’ is admissible” (Macdonald, Scottish Criminal Law, p. 512).
A medical man may be called as a common witness, or as an expert witness. In the first case, he has only to state, as any other witness might do, the facts that have fallen under his observation; in the second, he has to interpret the facts he has himself observed, or to give his opinion on facts noticed by others. In stating his opinion, a medical witness must be prepared to back up his [Pg 19] opinion by such reasons as may be satisfactory to the understanding of his hearers, “and this is the principal qualification of a medical witness, that he make himself intelligible to ordinary comprehensions.” No man is bound to give any testimony by which he may render himself liable to any criminal prosecution. (See the ruling of Bailie, J., in the case of Mr. George Patmore, tried for the murder of John Scott in a duel.)
At the trial, the witness is first examined by the party who calls him: this is the examination-in-chief. He is then cross-examined by the opposite party; and, lastly, re-examined by the former party, when he is offered the privilege of explaining any discrepancies between his examination-in-chief and cross-examination, but he must not introduce any new matter, for by so doing he renders himself liable to be cross-examined on it.
The Use of Notes.—All notes should contain a plain statement of the facts, and, to render them admissible as evidence, they must be taken at the time, and duly attested. From the notes prepared as before mentioned a witness may refresh his memory, but they are not accepted in its place. A witness may not read his notes as evidence, nor may he refresh his memory by documents not his own and not produced, but he may refresh his memory by looking at a document received from the accused at the time of the offence, and kept by him (Geo. Wilson, jun., Aberdeen, May 1, 1861; 4 Irv. 42).
The Use of Books.—No witness is allowed to quote from books, or to quote the opinion of other medical men on the subject, but he may refer to facts. Sir Henry Littlejohn, in his papers on Medical Jurisprudence,[2] gives some useful hints on this subject. It appears that a medical witness, in an unguarded moment, stated that his opinion was corroborated by a distinguished member of the medical profession not engaged on the trial. The judge informed the witness that it was most irregular to have other medical men present at the dissection than those mentioned in the warrant, and that, if the witness did not feel qualified for conducting such dissections, he had better resign the post of medical inspector.
In England, at the request of both parties, the medical and scientific witnesses may be excluded from the Court, but as a general rule they are allowed to be in Court, and hear the whole of the evidence of the case. In Scotland they are always excluded, although, by mutual consent, “experts” may remain to hear the general evidence on which they are to express their opinions, but when an expert is giving his opinion the others must leave the Court. In the latter country also, a medical witness who has been in Court cannot be examined on the facts of the case, but only on matters of opinion. A medical man is, however, sometimes allowed, on a special motion, to remain, although he is to be examined as to facts, and withdrawn when other witnesses are to be examined as to facts to which he is to speak. (See case of E. W. Pritchard, H.C. 1865; 5 Irv. 88.) [Pg 20]
In giving evidence the witness should—(1) Speak loudly and distinctly. (2) Answer questions categorically—Yes or no. (3) Never use superlatives. (4) Give answers irrespective of results of trial. (5) Express no opinion as to guilt of prisoner; state facts only. (6) Avoid using technical terms. (7) Avoid long discussions, especially theoretical arguments.
When a quotation is made from a book by the examining counsel, the medical witness, before replying to a question based on it, should see that the quotation has been fairly and fully given, due regard being paid to the context. Neglect of this precaution may lead him into considerable difficulty.
A medical witness should remember that he is not retained for a party, but in the cause of justice. He must, therefore, be candid in his manner and simple in his language. Mr. Haslam remarks that, however dexterous a witness may show himself in fencing with the advocate, he should be aware that his evidence ought to impress the judge, and be convincing to the jury. Their belief must be the test by which his scientific opinion is to be established. That which may be deemed by the medical evidence clear and unequivocal, may not impress the judge, nor carry conviction to the jury.
The advice given by Sir W. Blizard may not be out of place here: “Be the plainest man in the world in a Court of Justice; never harbour a thought that if you do not appear positive, you must appear little and mean for ever after; many old practitioners have erred in this respect. Give your evidence in as concise, plain, and yet clear manner as possible; be intelligent, candid, open, and just, never aiming at appearing unnecessarily scientific. State all the sources by which you have gained your information. If you can, make your evidence a self-evident truth: thus, though the Court may at the time have too good or too mean an opinion of your judgment, yet they must deem you an honest man. Never, then, be dogmatic, or set yourself up for judge and jury; take no side whatever, be impartial, and you will be honest. In Courts of Judicature you will frequently hear the counsellors complain when a surgeon gives his opinion with any of the least kind of doubt, that he does not speak clearly; but if he is loud and positive, if he is technical and dogmatic, then he is allowed to be clear and right. I am sorry to have to observe that this is too frequently the case.”
Liability of Medical Men to reveal Professional Secrets.—The question has arisen how far a medical man is bound to reveal the secrets confided to him in his professional capacity as medical attendant. This question was raised by Mr. Cæsar Hawkins in the trial of the Duchess of Kingston (11 Harg. St. Tri. 243), before the House of Peers, and decided by Lord Mansfield thus: “Mr. Hawkins will understand that it is your (the other Peers) judgment and opinion that a surgeon has no privilege, where it is a material question in a civil or criminal course to know whether parties were married or whether a child was born, to say that his introduction to the parties was in the course [Pg 21] of his profession, and in that way he came to the knowledge of it. I take it for granted, that if Mr. Hawkins understands that, it is a satisfaction to him and a clear justification to all the world. If a surgeon was voluntarily to reveal these secrets, to be sure he would be guilty of a breach of honour, and of great indiscretion; but, to give that information in a Court of Justice, which, by the law of the land, he is bound to do, will never be imputed to him as any indiscretion whatever.” However objectionable it may be to the medical witness, and be considered by him a breach of professional confidence, to reveal in a Court of Law secrets known but to himself and patient, and regarded as sacred, he has no privilege but to reveal them if demanded as evidence, unless the evidence be such as might incriminate himself. This is not the ruling in most Continental countries, where the medical man claims the same privileges of secrecy as the priest in confessional.
Under this head will be treated Identity and the examination of the Living and the Dead, Real and Apparent Death, Cause of Death, Exhumations, and Autopsies.
Examination of the Living.—With regard to the identification of the living, the presence of a medical man is seldom required, but there are many occasions when his opinion may be sought. Thus, under the Factory Acts, he may have to examine children about whose age doubts may have arisen. The Table on p. 33, giving the periods at which the teeth appear, will assist him. A medical man may also be requested to give an opinion as to the mental soundness or unsoundness of an individual. He may also be consulted in cases where questions have arisen as to the existence and character of certain marks on the body—of deformities, either congenital or produced subsequent to birth, or of doubtful sex. The marks which most frequently give rise to differences of opinion are nævi materni, scars, and tattoo marks. In cases of doubtful sex, the male organs may resemble the female, the female the male, or they may be blended together in about equal proportions.
In all cases where an examination of a living person is required, the consent of the person must be obtained, the nature of the examination explained, and that any facts recorded will be used as evidence if required. If the person refuse to be examined then it must not be carried out.
Cicatrices.—The following questions may be put to the medical expert—(1) Do scars ever disappear? (2) Can the age of a scar be definitely stated?
In reply to the first and second questions, I shall quote the words of the late Professor Casper: “Consequently the scars occasioned by actual loss of substance, or by a wound healed by granulation, never disappear, and are always to be seen upon the body; but the scars of [Pg 22] leech bites, or lancet wounds, or of cupping instruments, may disappear after a lapse of time that cannot be more distinctly specified, and may therefore cease to be visible upon the body. It is extremely difficult, or impossible, to give any certain or positive opinion as to the age of a scar.”
All cicatrices should be examined with oblique light and the aid of a lens. In the early stages a cicatrix is of a red colour, changes to brown, and later to white, and the surface glistens. In the intermediate stages one could not give any positive evidence of the age of a cicatrix. The probability is that a red cicatrix is a recent one, a white cicatrix is not recent.
I have seen well-defined cicatrices upon the back of a Russian, after incisions made by the blades of a cupping instrument fourteen years previously, and in an Englishman after twenty-five years (R. J. M. Buchanan).
Devergie states that where the brand of a galley-slave has vanished, it may be recalled by slapping its usual position with the palm of the hand. The scar remains white, while the skin round it is reddened. A change of temperature to the part will sometimes cause the reappearance of a vanished scar. Washing may also help to reproduce scars. Cicatrices produced in childhood may grow with the ordinary growth of the individual. The shape of a cicatrix will depend upon the character of the wound which produced it; on the nature of the healing process; on the elasticity or tension of the skin; on the convexity of the part; and on the looseness of the subcutaneous cellular tissue. An incised wound healing by the “first intention” will most probably leave a white linear cicatrix; on the other hand, a wound healing by granulation will leave a more or less irregular scar. The position of a wound on the body also modifies the subsequent cicatrix; thus a linear cicatrix is produced when the wound is in the long diameter of the limb, a more or less oval one when across the limb. The retraction of the skin in the latter case tends to draw the skin at right angles to the line of incision, thus approximating the extremities of the cut, increasing it in breadth and lessening it in length. Owing to one or more of the above-mentioned conditions the typical cicatrix of an incised wound is elliptical, tending, however, in some cases to assume a circular form. Linear cicatrices are found chiefly between the fingers and toes, and where the cutaneous surfaces are concave. In gunshot wounds the resulting cicatrix is depressed and disc-shaped, and more or less adherent in the centre to the subcutaneous tissues, and if the weapon be fired close to the surface of the body, grains of unburnt powder may be seen in the surrounding skin. Cicatrices from burns are, as a rule, large, irregular, and superficial, and frequently give rise to deformity. A scar left by caustics is circumscribed, deep and depressed in the centre. Cicatrices in the groins are probably venereal; those in the neck and under the jaw, strumous. Scars from operation incisions are much less evident now than when wounds were more likely to suppurate and heal by granulation. It is remarkable, after an incision made with aseptic precautions and healing by first intent, as time [Pg 23] progresses the cicatrix becomes less and less noticeable, but they can be detected by methods described above. Fine punctures and stitch cicatrices may eventually leave little or no trace.
Dupuytren and Delpech state that the tissue formed in a cicatrix is never converted into true skin—the rete mucosum when once destroyed never being re-formed. It contains no sebaceous glands, sweat glands, or hair follicles, and is but slightly vascular. This may account for the white colour of ordinary cicatrices, but even to this rule exceptions may be taken, and dark brown patches of pigment have been known to mark the situation of old lacerated wounds. It must be remembered also that in irregular wounds and in incised wounds which may heal with an uneven joint, that portions of skin may become embedded or grow into the scar tissue and give rise to difficulty in forming an opinion. I have seen a well-defined dark coloration of the skin continue for three months after the application of a mustard plaster, followed at the time by desquamation.
Tattoo Marks.—With regard to tattoo marks, the question of their disappearance gave rise to considerable discussion in the celebrated Tichborne case. On this subject the experiments of Hutin, Tardieu, and Casper appear to point to the fact “that tattoo marks may become perfectly effaced during life,” but that after death the colouring matter with which the marks were made may be found in the lymphatic glands. This is especially the case when vermilion is used. The most permanent marks are made with Indian ink, powdered charcoal, gunpowder, washing blue or ink, and vermilion. These are given in the order of their permanency. Hutin found that in 506 men who had been formerly tattooed, the marks had disappeared from 47 of the number. Not only does permanency depend upon the colouring matter used, but also upon the depth to which it has penetrated. If superficial, it may gradually become effaced. If the material be carried down to the papillæ, it will remain permanent, and can only be removed in such a way as to leave a scar. But besides the spontaneous disappearance of tattoo marks from the lapse of time, these marks may be artificially removed, and in such a manner as to prevent the possibility of a definite opinion being given as to their primary character. The presence of a scar in the situation of a well-known tattoo mark is suspicious. Thus, the Claimant had a scar on a part where it was sworn that Arthur Orton had been tattooed. The application of strong acetic acid, potash, hydrochloric acid and glycerole of papain appears to be the means adopted for the removal of tattoo marks. Efforts are made to remove superficial tattoo marks by removing the particles with needles. Tattoo marks according to their position and design are useful evidence of identification.
Birth Marks.—The presence and characters of birth marks should be noted for purposes of identification. Their removal may be possible, but, except in such as are small and superficial, the process used for removal leaves traces behind in the [Pg 24] form of cicatrices or irregularities of surface, which may generally be detected in oblique light and with the aid of a good lens. Large moles or nævi may he excised, but a cicatrix will remain, which will differ in shape from the original mark.
Congenital Deformities.—These offer no difficulty and are in many cases permanent, such as intra-uterine amputations, constrictions, abnormality of limbs, &c. Such conditions as hare-lip, cleft-palate, herniæ;, &c., may be altered by surgical procedure, but leave permanent records of this. Peculiarities in twins are interesting as to their being of the “mirror image” or “identical” type.
Anthropometry.—This is principally used for the identity of habitual criminals. The Bertillon method is based upon certain measurements of the body, the principal of which are (1) the length of the head, (2) width of head, (3) length of body, (4) length of trunk while sitting, (5) distance between tips of mid-fingers with arms outstretched, (6) length of left forearm, left middle finger, and left foot, (7) length and width of right ear, (8) colour of irides. These measurements place the person in one or other class, according to the special system of classification.

Fig. 1.—First line (from left to right), plain impressions of whorl (thumb), arch (second finger), radial loop (forefinger).
Second line, rolled impressions of whorl (thumb), ulnar loop (fourth finger).
Finger Prints.—These are largely used as a means of identification in criminal cases, either by prints left upon articles, or by prints definitely made by the police authorities as a record for identification purposes.
On articles, the finger prints may be rendered more visible by dusting with some finely powdered material of dark colour which will adhere to the impression, which may then be photographed and enlarged. [Pg 25]
For purposes of record, the impressions are taken directly upon a suitable surface of the bulbs of the fingers and thumbs after having coated them with printer‘s ink. The impressions thus made show individual peculiarities in the distribution and arrangement of the ridges of the skin; and the chances of the markings of two individuals being alike is about one in sixty-four millions. By means of the pattern of these ridges, prints may be classified under the headings of arches, whorls, and loops, with certain recognised modifications of these. (See Figs. 1 and 2.)

Fig. 2.—First line (from left to right), plain impressions of whorl (forefinger), ulnar loop (thumb), arch (second finger).
Second line, rolled impressions of whorl (thumb), ulnar loop (third finger).
Eyes and Veins.—The angle of the eyes to the middle line of the face is an aid to identity; this will show whether the equator of the eye is on a plane at a right angle to the middle line, or above or below it. Tamassia lays much stress upon the arrangement of the veins on the back of the hands, which is an individual characteristic and one which is not easily altered or likely to be. By compressing the arms with a ligature the veins are made to stand out in relief and the backs of the hands are photographed.
Other Peculiarities.—The identity of the accused may be further proved by the absence or malformation of the teeth corresponding with a bite on the party assaulted, or the impression of the teeth on soft articles like cheese. Peculiarities of dentistry may be useful in identification. Or it may be proved that the wound inflicted could only have been made by a left-handed person, or in a manner peculiar to those engaged in the slaughtering of animals—e.g. is the cut from within outwards, as employed by butchers? The correspondence in the size and peculiarities of the foot of the prisoner and the footprints found in the vicinity of the [Pg 26] crime is important as evidence. There is considerable difference of opinion as to the size of a footprint on the ground, Mascar of Belgium asserting that it is smaller than the foot that made it, Caussè, on the contrary, that it is usually larger. It should be borne in mind that the size of the footprint varies in running, walking, and standing, being smallest in running and largest when the individual is standing, which may account for the difference of opinion of the two observers just mentioned. This fact should always be borne in mind when an examination is required to be made of the footprints in the neighbourhood of the crime. A mark in the footprint showing that the sole of the boot had been patched, or in the case of the naked foot that there was some deformity of the toes, would of necessity be important. The mark of the naked foot smeared with blood has, in several cases, led to the identification of the culprit. Photographs may be used as a means of identification. Casts of footprints may be taken by smearing the print carefully with oil, and pouring in liquid plaster of Paris, or by dusting it over with powdered paraffin wax, and then melting it by holding a hot iron over the print; this may be repeated until a sufficiently thick cast is obtained. Hot solution of gelatine in water, mixed with oxide of zinc and glycerine to the requisite consistence, may be used for the purpose.
Dyeing of Hair.—As a means of disguise the hair may be dyed, or the colour may be changed from dark to light. For darkening the hair, preparations containing permanganate of potash, or the acetate of lead, bismuth, or nitrate of silver, are most frequently employed. Sticks of nitrate of silver or lunar caustic are used for darkening eyebrows and moustachios. A wash containing sulphide of potassium is used before the application of the lead solution. This removes the grease, and helps the rapid formation of the black sulphide of lead. Preparations of henna are fashionable for the production of shades of copper to rich brown. To detect fraud, some of the suspected hair should be steeped in dilute nitric acid, the acid driven off by gentle heat, and the nitrate dissolved in distilled water, and then sulphuretted hydrogen passed through the solution, the result being the formation of the black sulphide of lead. If silver be present, the addition of hydrochloric acid will throw down the insoluble chloride of silver. If careful examination be made of dyed hair, it will be found that the dye is irregularly taken by the hair; the hair loses lustre, and I have not unfrequently seen the hair close to the scalp white, or at least several shades lighter than the rest. The scalp may also be seen more or less discoloured, especially when nitrate of silver is used and applied by the individual himself.
For lightening the natural colour, solutions of chlorine, of peroxide of hydrogen, nitric and nitro-hydrochloric acids, of varying strengths, are used. It must be remembered that the action of chlorine is by no means uniform. The hair retains the odour of chlorine for some time, even after repeated washing, and is hard, stiff, and brittle. Devergie states that he has not succeeded in producing a perfect [Pg 27] whitening of the hair in less than from twelve to twenty hours. It must be borne in mind that, under certain circumstances, dark hair may become suddenly white. I have seen large patches of grey hair over the head, the result of repeated attacks of neuralgia.
In the examination of persons whose hair is alleged to have been dyed, it is necessary to compare the dyed hair with that from other parts of the body, e.g. the pubes, or axilla, to wait and watch for irregularities of colour as the hair grows, new growth being free from dye, and if necessary to shave the part and compare the new growth with other hair, also to examine carefully the skin in the position where the dye has been applied. In one case which I noted, a man had been in the habit of touching the moustachios and eyebrows with lunar caustic, having previously damped it with his tongue; in time it produced argyria which coloured the whole of his face, the body generally, but most noticeable on the face.
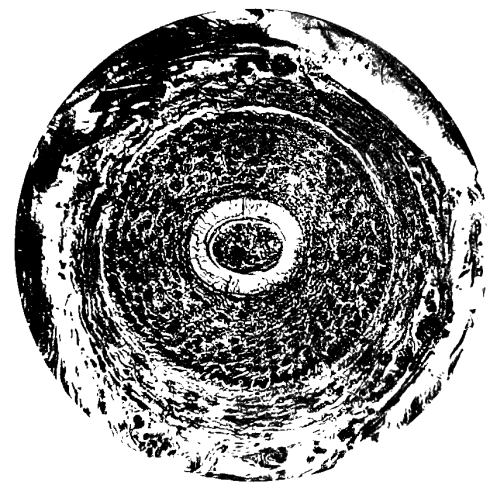
Fig. 3.—Photo-micrograph
of transverse section
of normal hair follicle, × 250.
(R. J. M. Buchanan.)
Carefully examine the bruises, wounds, &c., to see if they could have been inflicted as described. Ask no questions that may suggest an answer. Examine all weapons said to have been used, and hand them over to the police. In all cases where danger to life is imminent, send for the Authorities, and take dying declarations, as these may become evidence of vast importance, and, if properly taken, are as valid as if given on oath. [Pg 28]
Much of what has been said under the heading of identity of the living is applicable in examinations to establish identity of the dead. The latter requires certain special details of examination owing to the peculiar circumstances which may be present demanding them. The material subject to examination may be incomplete, and difficulties arise, so that it is essential to record every minute detail which may be of value as evidence.
The purposes of examination under this heading are mainly related to the questions of stature, age, sex, and special peculiarities of the body.
It will be useful here to emphasize the importance of making a detailed examination of the body. The examination, particularly the external inspection, should be made in daylight.
If the body be seen where first discovered, note should be taken of the exact position and attitude, of any signs of a struggle, of footprints to or from the body; of bottles, medicines, vomit, or excreta near the body, and which should be collected and retained. The expression and colour of the face, the condition of the hands, the condition of the dress as to tears and stains, the heat, amount of rigidity or putrefaction, the presence of wounds and vital reaction in them.
If the body has been removed from the place where found, make similar notes, remove the clothes, and compare any cuts if present in the clothes with those on the body. Record for identification—nævi, moles, tattoos, scars, hare-lip, cleft-palate, the mammæ, abnormalities of fingers, teeth, bones, limbs, joints, &c.
An examination of the mouth, for the presence or absence of false teeth, or of any peculiar formation of the jaw, may lead to the identification of the body. In the case of Dr. Parkman, the recognition by a dentist of the false teeth worn by the deceased led to identification of the remains, and also to the discovery of his murderer. The presence of an ununited fracture, as in the case of Livingstone, may lead to the identification of the body. In one case where a man was said to have died from a fracture of the ribs recently caused by a blow, it was found on examination that the bones were united by a firm callus, clearly showing that the skeleton produced could not be that of the man alleged to have been murdered.
Record the height and if possible the weight. Note the sex, the probable age, nutrition, and cleanliness or otherwise. Examine all wounds, bruises, and describe them carefully, and marks, e.g. strangulation or throttling. Examine the hands carefully and describe their peculiarities, also the colour of hair and eyes. Examine all the apertures of the body for foreign bodies, or abnormal conditions, and, in females, record carefully the condition of the external genitalia and the presence or absence of the hymen.
Although a more detailed account of the method of carrying out post-mortem examinations is given later on, it will not be out of place here to point out briefly the steps of examination. I would again [Pg 29] emphasize the importance of making a thorough and complete internal examination, leaving no organ unexamined. If there be no call for special examination of the thorax or abdomen first, commence with the examination of the surface of the brain, then proceed downwards. Note the direction of any wounds and their depth. Examine all organs for morbid changes, and in females, the vagina and uterus. Examine the larynx and œsophagus. Remove injured bones and examine joints. Remove the spinal cord. Always remember to note the contents of the stomach and bladder in reference to the period at which death may have occurred. Weigh all organs. Always remember the probability of poisoning, and make your examination accordingly.
All fragments or injured parts of a body or its organs should be preserved, and photographs taken of them.
It is better for two medical men to conduct the examination together. Do not make the examination without an order from the coroner. A medical man who is alleged as implicated in the cause of death should not be present.
Identification of the dead may present special difficulties where mutilation of the body has taken place, or where the body has been severely burnt, or is disfigured as in cases of explosions or advanced putrefaction. In such cases, fragments of clothes, ornaments, and dental work may afford valuable evidence.
Occupation Marks.—As an aid to identification, it is important to remember that certain trades leave marks by which those engaged in them may be identified.
Thus, in shoemakers there may be more or less depression of the lower portion of the sternum, due to constant pressure of the last against the bone.
Tailors work sitting, with the legs crossed and the body bent forward. The body is thus cramped, and the abdomen drawn in, and the thorax projects over it, due to the manner of sitting. They frequently have a soft red tumour on the external malleolus. A like tumour, but not so large, may also be found on the external edge of the foot, and a corn on the little toe.
Photographers have their fingers blackened by nitrate of silver, pyrogallic acid and other developers, or stained yellow with bichromate of potash.
Seamstresses have the index finger of the left hand roughened by the constant pricking of the needle.
Copyists have on the little finger of the right hand, near its extremity, a corn, and at the end of the middle finger a hard groove made by the pen.
Violinists have corns on the tips of the fingers of the left hand, harpists on both hands.
In smokers of pipes the incisors and canines are more or less worn by the mouthpiece, but sometimes the groove is between the canines and bicuspids. In cigarette smokers, the forefinger and thumb are stained with tobacco juice, also between the index and middle fingers, on the dorsum. [Pg 30]
In coachmen, corns may be formed between the thumb and index finger, and between the index and the second finger of the left hand, from the pressure of the reins, and between the thumb and index finger of the right hand, from the pressure of the whip.
In bricklayers, from the constant action of picking up bricks, the flattening of the tip of the thumb and index finger of the left hand is not uncommon.
Plasterers have corns on the external surfaces of the thumb and index finger, due to grasping the “hawk” on which the plaster is placed during their work.
Joiners and carpenters have callosities on the palm of the right hand from grasping their tools, and between the thumb and index finger of the right hand, also over the first interphalangeal joint of the right index finger. The right shoulder is lower than the left.
The finger-ends of turners and coppersmiths are also more or less flattened; in the latter, a deposit of the metal may take place.
To ascertain the time which may have elapsed since death.—This can scarcely be determined with precision, as so much depends upon the conditions under which the body may have been placed. The subject under consideration is, therefore, beset with difficulties, and its elucidation will require the greatest care on the part of the medical expert. A careful attention, however, to the subjects treated in the following pages will help to clear up many a doubtful point.
COOLING OF THE BODY
| (1) External circumstances. |
Covered by bed-clothes, or otherwise | |||
| unexposed, when cooling will be dry | ||||
| slower than in cold air quickly moving. | ||||
| (2) Condition of the | Slow, if fat. | |||
| body itself. | ||||
| 1. Wasting diseases. Quick. | ||||
| 2. Suffocation. Slow. | ||||
| (3) Kind of death. | 3. Cholera, yellow fever, | Increase | ||
| rheumatic fever, and | of heat | |||
| cerebro-spinal meningitis. | after death. | |||
The following circumstances must also be taken into consideration: (1) Age. (2) Air—(a) moving; and (b) at rest. (3) Moisture. (4) Warmth. (5) Nature of the supposed cause of death, as affecting cooling of the body, and promoting the rapid advance of putrefaction. (6) Presence or absence of the rigor mortis. Bodies may be preserved for months if exposed to intense cold.
The following Table, compiled from the experiments of Devergie, may be of use in aiding the expert to form his opinion, but it must be borne in mind that, from the great difficulties which surround the subject, the statements made are only approximately correct. The table is divided into four stages or periods, the last being that in which putrefaction commences:—
First.—From a few minutes to twenty hours after death—Animal heat more or less present, but seldom continuing longer than ten or twelve hours. Muscles contract on the application of galvanic stimuli, and in the earlier stage to blows. [Pg 31]
Second.—From ten hours to three days—Body quite cold and rigor mortis well marked; muscles do not contract on the application of stimuli. The age, mode of death, and other collateral circumstances must, more or less, be taken into consideration before an opinion can be given.
Third.—From three to eight days—The body is quite cold, and cadaveric rigidity has passed off. The muscles no longer respond to any galvanic or mechanical stimulus. The stage is modified and somewhat shortened in summer.
Fourth.—From six to twelve days—Commencement of putrefaction. Putrefaction may, however, take place on the first or second day after death; so that, as before stated, care must be taken before any positive decision can be given.
Stature.—As a general rule the length of the body is equal to the distance between the tips of the middle fingers with the arms outstretched. If an arm be missing, the length of the remaining one multiplied by two, with the addition of 6 inches for each clavicle and 1½ inches for the width of the sternum, will give the approximate height. The femur is said to be equal to .275 of the body height. If the skeleton be entire, the addition of 1½ inches for the soft parts should be made.
Where only a limb or long bone or part of one be available, it is not possible to give anything more than an approximate opinion of the height.
Sex.—When mutilation, putrefaction, or charring has taken place, by which the genitalia have been demolished, it may be difficult to determine the sex. Evidence will be afforded by the distribution of the pubic hair, which in the male reaches as high as the umbilicus, but is horizontal with few exceptions in the female. Males have more hair on the body generally.
The presence of moustachios and beard and the length of the hair on the head will assist in sex determination.
The breasts if present will denote the sex, also the uterus, which withstands putrefaction and burning to a marked degree.
Remains of clothing and ornaments will indicate the sex of the wearer.
Lineæ albicantes on the abdomen, buttocks, and breasts indicate the female sex, and the probable occurrence of previous pregnancies. It must, however, be remembered that lineæ albicantes occur in males who have been stout or had the abdomen distended by disease.
The Skeleton in Relation to Identification.—When a complete skeleton is submitted for examination, the chief points to elucidate are the age and sex. These will be noted further on. It may happen that a single bone, separate bones, or only a part of one is obtainable, when there may be considerable difficulty in expressing a definite opinion. The questions to be answered are: Are they human or belonging to the lower animals? When the bones are entire the answer is not very difficult to settle; but when parts of bones have to be dealt with, one has to be very careful in forming conclusions, and the fragments may [Pg 32] have to be submitted, to a skilled anatomist. One may not be able to express an opinion about bones of the lower animals, other than to state they are not human. The services of a skilled Comparative Osteologist may be necessary to decide the nature of the animal.
When fragments resembling bone have to be examined, the microscope will be necessary to determine their osseous structure. When several bones have to be examined it may be possible to build up part or the whole of a skeleton. Duplicate bones will indicate remains of more than one creature. All fragments and bones should be carefully described, measured, and photographed.
By the character of the bones one may be able to determine the sex to which they belong and the approximate age. As a general rule the bones of the female are smaller, lighter, and less marked by muscular and other attachments.
The thorax in the female is deeper than in the male, the sternum shorter and more convex, the ensiform cartilage thinner and ossified later in life. The cartilages of the ribs are larger and the ribs smaller than in the male. The ribs are more oblique and may show the results of long corset pressure. The body of the sternum is over twice the length of the manubrium in the male, less than this in the female.
The length of the twelfth rib in the male averages 103 mm., in the female 83.8 mm. The pelvis exhibits marked differences. The sacrum of the male is more curved than that of the female, which is straighter in the upper half and more curved in the lower. The male pelvis is more compact, deeper, rougher, and narrower. The pubic angle is smaller, the obturator foramen is oval, and the ischia incurved. The female pelvis is more open, shallower, wider, not so rough, a wider pubic angle, and shallower and broader symphysis, the ischia are everted, wider apart and flatter, and the obturator foramen triangular. The inlet of the female pelvis is greater in all its diameters.
The skull in the male is heavier and larger, the markings and ridges being more pronounced, the mastoid processes, occipital protuberance, zygomatic and superciliary ridges are more prominent, and the capacity greater than in the female.
In the female the jaw is less prominent and has a wider angle.
The lumbar curve is longer in the female, and the lumbo-sacral angle greater than in the male.
The angle made by the neck of the femur with the shaft is about a right angle in the female, more obtuse in the male. It must be remembered that these differences between the sexes are not present to the same degree before puberty, so that prior to it the examination offers little evidence as to sex.
When examining bones any injuries to their structure or other abnormalities should be noted. The skull must be carefully examined for fractures, especially the base, which may be easily overlooked. [Pg 33] Injuries to vertebræ should be looked for. The presence of callus will indicate that fracture has occurred at a period before death long enough for its formation.
Age.—There are several data which enable one to form a fairly accurate opinion as to the age of a body, these are especially useful in earlier years and intra-uterine life.
The more general are the size, height, development, the presence or absence of signs of puberty, the state of dentition, the greyness of the hair; in the female the atrophic condition of the uterus after the menopause, and the character of the lower jaw.
In addition are the time of life at which centres of ossification appear and the union of epiphyses to the shafts of bones and bones with each other.
In intra-uterine life centres of ossification appear by the end of the sixth month in the os calcis, manubrium, and the bodies and laminas of the sacral vertebræ; by the seventh, in the first piece of the body of the sternum and the astragalus; by the eighth, in the second piece of the body of the sternum; at full term in the cuboid, third piece of the sternal body, first coccygeal vertebra, and the lower epiphysis of the femur.
All traces of the fontanelles have disappeared by the end of the fourth year. The angle of the jaw in infants and young children is obtuse; as dentition proceeds, the body becomes deeper and the angle alters so that towards adult life it approaches a right angle, the ramus is longer and the body has become well developed with a mental foramen midway between upper and lower borders. In the new-born, the mental foramen is low down as the body of the jaw is practically all alveolar. In old people the angle again becomes obtuse and the alveolus disappears as the teeth are shed, and the mental foramen is at the upper border.
Table of the Eruption
of the Teeth
| Age— | Eruption of teeth. | Temporary. | ||||
| Lower | central | incisors, | 7 | months. | ||
| Upper | “ | “ | 8 | “ | ||
| “ | lateral | incisors, | 7-10 | “ | ||
| Lower | “ | “ | 10-12 | “ | ||
| First molars, | 12-14 | “ | ||||
| Canine teeth, | 18 | “ | ||||
| Second molars, | 22-24 | “ | ||||
| First molars, | 6 | years | Permanent. | |||
| Middle incisors, | 7 | “ | ||||
| Lateral incisors, | 8 | “ | ||||
| First bicuspids, | 9 | “ | ||||
| Second bicuspids, | 10 | “ | ||||
| Canines, | 11-12 | “ | ||||
| Second molars, | 12-13 | “ | ||||
| Wisdom teeth, | 18-25 | “ | ||||
Examine the lower jaw. The ramus forms an obtuse angle in full-grown fœtus, a right angle in adult life, obtuse in old age from loss of teeth.
Table showing the Periods at which Points
of Ossification appear after Birth
| Years of Life. |
Bones in which Centres of Ossification appear. |
| 1. | Fourth piece of the body of the sternum; coracoid process |
| of scapula; head of humerus; os magnum (carpus); | |
| head of femur; upper end of tibia; external cuneiform | |
| (tarsus). | |
| 2. | Lower end of radius; unciform (carpus); lower end of tibia; |
| lower end of fibula. | |
| 3. | Great tuberosity of humerus; patella; internal cuneiform (tarsus). |
| 3-4. | Upper end of fibula. |
| 4. | Great trochanter (femur); middle cuneiform (tarsus). |
| 4-5. | Scaphoid (tarsus); lower end of ulna. |
| 5. | Lesser tuberosity (humerus); internal condyle (humerus); |
| trapezium and semi-lunar (carpus). | |
| 5-6. | Upper end of radius. |
| 6. | Scaphoid (carpus). |
| 7. | Trapezoid (carpus). |
| 10. | Upper end of ulna. |
| 12. | Pisiform (carpus). |
| 13-14. | External condyle (humerus); small trochanter (femur). |
Periods of Union of Epiphyses
with the Shafts of Bones,
and of Bones with each other
Table showing the Development of the Embryo
according to the Lunar Months
Table giving the Measurements, according to the Months,
of the Extremities of the Fœtus in
the Order of their Development
| Third. | Fourth. | Fifth. | Sixth. | Seventh. | Eighth. | Full Period. | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Humerus | 3½ | lines. | 8 | lines. | 13-15 | lines. | 16 | lines. | 20-22 | lines. | 23-24 | lines. | 3 | inches. | ||
| Radius | 2½ | “ | 8 | “ | 12 | “ | 16 | “ | 17 | “ | 18-19 | “ | 2 | “ | 8 | lines. |
| Ulna | 3 | “ | 8 | “ | 13 | “ | 17 | “ | 18 | “ | 22-23 | “ | 2 | “ | 10 | “ |
| Femur | 2-3 | “ | 4-5 | “ | 12 | “ | 17 | “ | 19-21 | “ | 24 | “ | 3 | “ | 6 | “ |
| Tibia | 2-3 | “ | 4-5 | “ | 12 | “ | 17 | “ | 19-21 | “ | 21-23 | “ | 3 | “ | 2 | “ |
| Fibula | 2½ | “ | . . . | 12 | “ | 17 | “ | 19-21 | “ | 21-23 | “ | 3 | “ | 1 | “ | |
Table showing the Maximum and Minimum
Dimensions of the Osseous
Nucleus of the Inferior Femoral Epiphysis from
the Seventh
Month of Intra-Uterine Life to Two Years after Birth
| INTRA-UTERINE | EXTRA-UTERINE. | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Days. | Months. | |||||||||
| Seventh | Ninth | Mature | 1-8 | 9-15 | 16-28 | 1 | 3-6 | 7-12 | 2-24 | |
| lines | lines | lines | lines | lines | lines | lines | lines | lines | ||
| Maximum | 2 | 4 | 3½ | 3½ | 2½ | 5 | 4 | 8 | 7 | |
| Minimum | “ | ¾ | 1 | ¾ | 1½ | 2 | 2 | 3 | 5 | |
| No. of Children (125) examined |
31 | 9 | 52 | 8 | 3 | 2 | 9 | 3 | 6 | 2 |
Syncope—death beginning at the heart.
Asphyxia—death beginning at the lungs.
Coma—death beginning at the brain.
Syncope.—From δνγκοπτω, I strike down. Sudden arrest of the action of the heart.
This condition may be brought about by
Causes—Heart Disease.—Aortic regurgitation, fatty degeneration, &c.
Hæmorrhages from wounds of blood-vessels or the heart, profuse hæmoptysis or hæmatemesis, uterine hæmorrhage, bursting of varicose veins, bursting of aneurysms.
Shock.—Emotion; blows on the head or epigastrium; sudden evacuation of fluids from the body, as in emptying an over-distended bladder, tapping a hydrocele, ascites, or a pleural effusion. Extensive injuries to the body (railway and machinery accidents). Drinking large quantities of cold water when heated.
Exhaustive diseases, chronic or infective.
Symptoms.—Pallor of the face and mucous membranes, dimness of vision, cold perspirations, sense of impending death, restlessness, air hunger and gasping for breath, nausea, and, maybe, vomiting, noises in the ears, passing delirium, quick, feeble, and fluttering pulse, or the latter may be imperceptible at the wrist, insensibility, convulsions.
In ordinary fainting attacks many of the above symptoms are absent; such as are present are temporary. In collapse, consciousness is retained.
Post-mortem Signs.—The cavities of the heart contain a normal quantity of blood in death by asthenia, but may be almost empty when death is due to anæmia. The blood in asthenic death is simply arrested in its course; blood is, therefore, found in the large veins and in the arteries. The brain and the lungs are not engorged with blood.
Asphyxia.—From ἀ priv. et δφνξιϛ, pulse. Apnœa is the better term—ἀ priv. et πνεω, I respire; but this word is now used by physiologists to denote a cessation of the respiratory movements due to [Pg 39] artificially oxygenated blood. Blood in this condition fails to excite the respiratory centre in the medulla, and respiration ceases. To avoid confusion the term asphyxia had better be retained, especially as it is most commonly used and generally understood. Asphyxia, or death from defect in the quality of the blood, is brought about when any impediment is placed on the healthy action of the lungs. Experiment has shown that for a short time after respiration has ceased, the heart still continues to act, and that if the impediment to the proper aeration of the air by the lungs be removed, life may be prolonged. Taking therefore the primary meaning of the terms asphyxia and apnœa into consideration, it may be remarked that the latter precedes the former in point of time—asphyxia marking the period at which the action of the heart ceases, apnœa the cessation of the respiratory functions.
Causes of Asphyxia.—1. Mechanical obstruction to the air passages: foreign bodies, exudations, tumours, suffocation, strangulation, drowning, hanging, spasm of glottis from mechanical irritation, or irritant gases.
2. Interference with the action of the respiratory muscles: exhaustion of the muscles from cold; paralysis of muscles from injury to or disease of respiratory centre; poisons acting on the centre; continued pressure on walls of the chest; fixation of muscles from tetanus or strychnine poisoning.
3. Diseases of and injuries to the lungs: pleurisy with effusion, acute pneumonia, empyema, pneumothorax, pyopneumothorax, pulmonary apoplexy, embolism of pulmonary artery.
4. Inhalation of air deficient in oxygen.
Symptoms of Asphyxia.—Divided into three stages. First stage: deep, frequent, and laboured respiration; the extraordinary muscles of respiration are called into play. Second stage: the inspiratory muscles are less active than expiratory, convulsions of nearly all the muscles of the body occur. Third stage: paralysis of respiratory centres, dilated pupils, loss of consciousness, absence of reflexes. Gasping inspirations with prolonged intervals precede dissolution.
Post-mortem Signs.—Engorgement of the pulmonary artery, the right cavities of the heart, and vent cavæ; but on the left side of the heart the cavities, together with the aorta and pulmonary veins, are either empty or contain but little blood. It must be remembered, however, that cases of asphyxia do sometimes occur where the cavities on each side of the heart are empty, or nearly so. This is the case in the syncopal asphyxia of some writers. If also the obstruction to respiration be imperfect, the circulation may be continued for some time, congestion of one or more of the internal organs being the result. The blood is dark-coloured, contains much CO₂, and the hæmoglobin is almost completely reduced. The blood coagulates slowly.
Coma.—Insensibility ending in death. Causes.—Concussion of the brain, cerebral hæmorrhage, embolism, thrombosis, tumour, depressed fracture of skull, meningitis, and serous effusions; effects of poisons such as opium, alcohol, ptomaines, arsenic, barium, oxalic [Pg 40] and carbolic acids; in certain diseases of kidneys and liver, uræmia, cholæmia, acetonæmia, profound anæmia, e.g. pernicious, and as a terminal stage to acute or chronic diseases.
Symptoms of Coma.—Coma is generally preceded by stupor, from which the patient may be roused to a certain extent, but only temporarily. The reflexes in this stage may be exaggerated, and the power of swallowing fluids may be retained. When coma is present there is complete abolition of consciousness, sweating, the patient is powerless, the breathing stertorous. The temperature may vary according to the cause; normal or subnormal generally, it may rise in lesions of the pons Varolii. The pulse is generally full and bounding, the pupils dilated or contracted and insensitive to light, the conjunctival reflex absent. Mucus collects in the air-passages and causes “the death rattle,” and the breathing becomes more and more embarrassed and irregular. The reflexes are lost, and the sphincters relaxed.
Post-mortem Appearances.—Causal lesions are found in the brain or other organs; there is usually hyperæmia of the brain and spinal cord and their membranes, unless there be profound anæmia preceding death. The condition of the heart and lungs is not constant; the general appearances resemble those in death from asphyxia.
Table giving the Diagnosis of
Several
Forms of Insensibility
Injury to the Head—Concussion of the Brain.—The symptoms are very similar to those of shock, with unconsciousness, but it may be possible to rouse the person. The pupils are equal and dilated or contracted, and react sluggishly to light. The breathing is shallow and slow with sighing, the pulse feeble. The muscles are relaxed but not paralysed. Vomiting and involuntary micturition and defæcation may occur. The temperature is usually subnormal.
Cerebral Compression.—This, when due to injury, is usually associated with fracture of the skull and hæmorrhage. Insensibility is complete, the person cannot be roused. The pupils may be unequal, contracted or dilated, and may not react to light. The breathing is slow, stertorous, and may be irregular, or Cheyne-Stokes in type. The pulse is full and bounding, the cheeks are blown out during expiration. Paralysis, rigidity, or convulsions may be present on one side of the body. There may be retention of urine, with overflow incontinence.
In cases associated with severe fracture or hæmorrhage within the skull, the conjunctivæ may be chemosed, or there may be hæmorrhage from the nose or ear; and a flow of cerebro-spinal fluid may take place from the nose.
Alcohol.—In coma due to alcohol, there will be an alcoholic odour of the breath, alcohol in the stomach contents, and it can be detected in the urine. The odour of alcohol in the breath may be due to the administration of alcohol by an outsider [Pg 41] at the onset of the symptoms which have ended in the coma. The pupils are equal, contracted, the conjunctival reflex present, and the pupil dilates on pinching the skin of the neck. The pulse is rapid, at first strong it becomes feeble, the respirations snoring. If the coma be not complete, muscular inco-ordination may be noticed. The person can usually be aroused by stimulation.
In pure alcoholic coma the presence of the special features of coma from other causes will be absent. It must be remembered, however, that alcoholic coma may be combined with other kinds, and the more serious form should be kept in mind. Where there is the slightest doubt in the diagnosis, one‘s procedure should be ruled by the possibility of the graver cause.
Opium or Narcotic Poisoning.—The skin is usually perspiring freely, moist and cold; the countenance placid, pale and ghastly, the lips livid. The eyes are heavy, and the pupils contracted to a pin-head and equal, the conjunctival reflex usually present. There is the odour of opium in the breath. The pulse is slow, and the respiration stertorous and slow. There is no paralysis, and the person can be momentarily roused by a sharp question or blow.
Apoplexy.—The person is with difficulty, if ever, temporarily aroused. The face is red and bloated. Respiration suspirious and stertorous, and there is often Cheyne-Stokes breathing. The pupils are dilated or irregular; in pontine hæmorrhage, contracted. The temperature may at first be subnormal but gradually rises.
There may be rigidity of the limbs, or hemiplegia. The pulse is full and bounding, often of high tension with hardened arteries.
Albuminuria may be present.
Uræmia.—This is less profound than in cerebral hæmorrhage; the patient may be temporarily aroused; the onset is usually gradual. There is albuminuria with casts; albuminuric retinitis may be present. The pupils may be contracted or dilated. The breath has a peculiar so-called “uræmic odour.” The pulse is generally slow, the tension high, and the heart enlarged. The respirations are slow and sighing, and may be Cheyne-Stokes in type. There is no paralysis. There may have been preceding convulsions, and the coma may alternate with these attacks.
Anasarca may be present.
Diabetic Coma.—This may come on suddenly, and may occur unexpectedly in a person in whom diabetes has not been discovered up to the time of coma. There is sighing respiration, “air hunger.” The odour of acetone in the breath is present, and sugar in the urine.
Epilepsy.—Unconsciousness is profound, and comes on immediately with rigidity, followed by convulsions, unilateral, limited to the side of the face, jaws, head and neck or arm, or generalised. Bloody froth exudes from the mouth, the tongue being bitten. The eyes are wide open, the pupils dilated and insensible to light. Micturition may occur. After the convulsive attack has passed off, post-epileptic coma may remain, though usually for a short time only.
Syncope.—This has been described under modes of dying (p. 38). [Pg 42]
In all cases of coma when first seen examine the head for signs of injury, note the odour of the breath, observe the state of the pupils and their reactions, examine the limbs for paralysis, count the pulse and note its character, and the state of the arteries, note the size of the heart and auscultate it at each area. Count and note the character of the respirations, take the temperature, examine the urine, take note of the person‘s age, and inquire into the previous history.
Sudden death may proceed from natural or violent causes. From the former, death may occur unexpectedly and very rapidly, but as a rule the period of time occupied by the phenomena of “dying” is measurable, though inconstant. Should such period of time be immeasurable, death may be considered as instantaneous.
Apart from sudden death resulting from violence or poisoning, the common causes are as follows:—
1. Diseases of the heart: angina pectoris, valvular diseases with failure of compensation, especially aortic regurgitation, degeneration of the heart muscle, rupture of the heart, heart failure from diphtheria or toxic diseases.
2. Diseases of the blood-vessels: rupture of aneurysms or varicose veins, thrombosis, embolism.
3. Cerebral hæmorrhage, especially when in the region of the pons Varolii or cerebellum.
4. Lesions of the respiratory system: œdema or spasm of the glottis, membranous deposit or foreign bodies in the larynx or trachea, foreign bodies in the pharynx, tumours, whooping-cough, asthma, embolism of the pulmonary artery, air embolism, fat embolism, rupture of a vessel or aneurysm into the air-passages, as in phthisical cavities, pneumothorax, hæmothorax, pleuritic effusion, and in acute pneumonia.
5. Rupture of a gastric ulcer or ulcer of some other part of the alimentary tract.
6. Sudden hæmorrhage into the peritoneal cavity from ruptured uterus, ectopic gestation, &c.
7. Rupture of internal organs: distended bladder, spleen, pregnant uterus, or other abdominal viscus.
8. Hæmorrhage into the pancreas.
9. Conditions associated with the nervous system: mental emotions, epilepsy, uræmia, laryngismus stridulus in children.
10. Sudden death has occurred in Addison‘s disease, in diabetes, in cases of lymphatism or status lymphaticus in young people, during the early stage of chloroform anæsthesia, during simple vaginal examination in women, during the injection of fluids into the vagina or uterus. Bouvalat (Annales d‘Hygiène, 1892) relates a case in which, as the cannula of a syringe was being introduced into the os uteri of a woman with the object of criminal abortion, she fell back before any fluid was injected, and died in a few minutes. [Pg 43]
A similar case came under my notice, in which death took place while the husband of the woman was attempting to introduce a solution of 20 minims of tincture of iodine, mixed with water to measure two drachms, into her uterus through a No. 3 catheter.
Real or Apparent Death
It will be unnecessary here to discuss any of the theories put forward with regard to cases of apparent death or prolonged trance, but simply to note in the order of their occurrence the phenomena which attend real death.
Under this heading it is important to draw a distinction between “Somatic death” and “Molecular death.” “Somatic death” is defined as “the cessation of the vital functions and of the general renewal of tissue consequent on that cessation”; “Molecular death” is the death of the tissues themselves.
The signs of death occur as follows:—
1. Entire and continuous cessation of the respiration and circulation; no sounds heard on auscultation. The absence of the heart sounds is the most important sign of death, for even in the severest forms of syncope the cardiac pulsations, as shown by M. Bouchet, can with care be heard.
Tests for cessation of respiration:—
(a) Auscultation. (b) Placing a cold hand-mirror or empty drinking-glass over the mouth or nostrils, or a light feather, and noting the presence or absence of bedewing or movement. (c) Placing a shallow vessel, such as a saucer, full of water on the chest or abdomen, and observing the presence or absence of rippling of the fluid (Winslow‘s test).
Tests for cessation of the circulation:—
(a) Auscultation.
(b) Manual exploration of the principal arteries for pulsation or thrill.
(c) Magnus‘s test, applying a ligature tightly round a finger, sufficient to stop the venous but not the arterial circulation, and noticing whether or not a bloodless ring forms at the seat of ligature, and a zone of livid redness on the distal side of the ligature, the part becoming first red, then purple.
(d) Applying pressure to the finger-nail, and noticing whether the colour disappears on pressure, and a pink tinge appears after relaxing the pressure.
(e) Applying heat, such as dropping melted sealing-wax on the skin, and noting whether or not redness or vesication ensues. [Pg 44]
(f) Holding the hand, with the fingers abducted, against a strong fight, and observing whether or not the web of the fingers is translucent.
(g) Inserting a brightly polished needle into a fleshy part of the body, allowing it to remain for ten seconds or so in situ, and noticing whether it is tarnished or not on withdrawing it.
(h) Injecting hypodermically a solution of fluorescin (resorcin-phthalein and sodium bicarbonate, a gramme of each dissolved in 8 c.c. of water). No local discoloration of the skin takes place if the circulation has ceased, but if not, a yellowish-green coloration of the skin occurs round the seat of injection, and the substance may be detected in the blood at a part some distance from the seat of injection. By immersing some white silk threads in the blood drawn at a distance from the prick, then boiling them in distilled water, the latter will have a greenish colour if the fluorescin has been circulated (Icard‘s test).
These tests will detect whether the circulation has ceased or not, and so differentiate suspended animation from real death.
2. The lustre of the eye is lost immediately after death. It has, however, been stated that the iris will respond to the action of atropine and eserine for some hours after death, and that the action of the latter is always more marked than that of the former. The fundus as seen by ophthalmoscopic examination is altered, the normal redness changes to a yellowish-white, the vessels in the disc and just around it become empty, and the veins appear to contain bubbles of gas and the column of blood is broken up (Bouchet). A blackish round or oval stain has been described by M. Larcher on the sclerotic coat on the outer side, which he calls l‘imbibition cadavérique du fond de l‘œil. It is probably due to thinning of the sclerotic from evaporation, enabling the choroid to be seen through it. The spot precedes rigidity and is a forerunner of putrefaction.
3. The most powerful stimulus applied to the body does not cause any reaction. The muscles may, however, be made to contract shortly after death by the stimulus of a slight blow, or by galvanism.
4. The surface of the body becomes of an ashy-white colour.
(1) Persons of florid complexion retain this on the malar prominence for some time after death.
(2) The red or livid edges of ulcers.
(3) Blue, black, or red tattoo marks, if not effaced during life, do not disappear.—Ecchymoses retain the hue they had at the time of death.
(4) An “icteric” coloration existing at death, as in jaundice, never becomes white.
(5) A rosy tint of the skin on those poisoned by carbon monoxide.
(6) Dusky-red patches in those frozen to death.
(7) In certain cases of drowning, a rosy colour may be observed on the lips and malar prominences.
[Pg 45] 5. The temperature of the body at the time of death is retained for some time. As a sign of death the fall of temperature must be progressively continuous. Cooling will depend on the medium in which the body is placed, and mere coldness of the body is not a sign of death.
(1) Fat persons retain the heat longer than lean ones; adults longer than children or old persons. Bodies are cooled by—1. Radiation. 2. Conduction. 3. Convection.
(2) Bodies immersed in water cool more rapidly than in air. This fact may be of importance in determining survivorship in a case of drowning.
(3) Bodies in bed and covered by the clothes, or in cesspools and in dung-heaps, cool less rapidly than when exposed.
(4) Persons killed by lightning may keep warm longer than others.
(5) Death by suffocation retards the process of cooling.
(6) The body may be cold externally, but possesses a considerable amount of heat when the internal organs are exposed. Persons who have died of cholera, yellow fever, or suddenly of some acute disease—rheumatism—may retain for some hours a considerable amount of heat. It has even been asserted that in some diseases—cholera—there is an increase of temperature soon after death (Laycock), also after death due to some diseases of the nervous system as in pontine hæmorrhage and cerebro-spinal meningitis, and following prolonged muscular spasm as in tetanus.
(7) Most bodies, under ordinary circumstances, are, as a rule, quite cold in from eight to twelve hours after death. The rate of loss of temperature depends upon the difference between that of the body and its surroundings; it lessens as the body cools. It takes at least twenty-four hours for it to fall to the heat of the surrounding atmosphere.
6. Relaxation, primary flaccidity, more or less general, of the muscular system takes place.
“If the above signs are alone present, death must have taken place in from ten to twelve hours at the longest” (Casper). Exception: cadaveric spasm.
7. Want of elasticity in the eyeball: flaccidity of the iris. This condition invariably occurs in from twelve to eighteen hours after death.
8. Flattening of the muscles of those parts on which the body rests, due probably to loss of vital turgidity.
9. Hypostasis.—Suggillation, or post-mortem staining, is due to the gravitation of the blood to the most dependent parts of the body not subject to direct pressure. The hypostatic marks begin to form in from eight to twelve hours after death, and increase in size till putrefaction sets in. They alter their position with changes in the position of the body so long as the blood remains fluid, but when it has coagulated they remain permanent. Hypostasis may be mistaken for an ecchymosis or a bruise, and in the lungs for congestion, inflammation, &c. Errors may also occur with regard to the brain, stomach, kidneys, and intestines: in the last, the redness of inflammation is seen all over the parts, whereas the coloration of hypostasis is interrupted, [Pg 46] and this is best shown by drawing out the convolutions. The heart is an exception to the rule, but it may contain clots varying in size and colour. These are post-mortem formations. The use of the word suggillation is objectionable, as it has been used in opposite senses by Continental and British authors—some writers restricting the term to ecchymosis proper, others using it as synonymous with cadaveric lividity or external hypostasis.
(1) Meaning of the expression.—The gravitation of the blood in the capillaries after death, in obedience to the laws of inert matter.
(2) On what parts of the body usually seen?—On the most dependent parts of the body; on the whole of the back of the body, if the body be supine. The patches are irregular and slashed, terminate abruptly, and do not fade gradually into the surrounding colourless skin.
(3) At what period after death first observed?—In from eight to twelve hours, gradually extending in size till putrefaction sets in.
(4) Whether or not affected by death from hæmorrhage?—Formed after every kind of death, even after death due to hæmorrhage, although the coloration may not be quite so marked.
(5) Hypostasis is liable to be mistaken for ecchymosis—the result of injury.—Hypostasis must also not be confounded with the livid patches seen on the legs and feet of aged persons and on those who have died from typhus, chronic renal and cardiac disease, &c. The rose patches—“frost erythems”—seen on those who have died from exposure to cold, must not be mistaken for ecchymosis. The above patches are as frequently on the upper surfaces of the body as on the lower, and are not so extended as cadaveric lividities; the blood, moreover, which gives rise to them is diffused through the areolar tissue, and not incorporated with the true skin.
(6) How distinguished from ecchymosis?—Effused or coagulated blood is found when an incision is made in a true ecchymosis, however small, whereas a few bloody points are alone seen on a slight or deep incision into a post-mortem stain or true hypostasis. The seat of hypostasis is the superficial layer of the true skin. Hypostases are never raised above the surface, as ecchymoses sometimes are. In describing these two conditions, “ecchymosis” and “hypostasis,” it is preferable to describe the former as “discoloration from extravasated blood,” and the latter as “lividity after death.”
10. Cadaveric rigidity.—From the moment of death till the time when putrefaction sets in, the muscular structures of the body may be said to pass through three stages:—
(1) Muscular Irritability.—The muscles flaccid, but still possessing the power of contractility on the application of certain stimuli. Parts contracted during the act of dying—cadaveric spasm—as the muscles of the hand grasping a knife or other weapon, may continue so for some time after death.
(2) Cadaveric rigidity.—A state of rigidity, the power of contractility absent.
(3) Commencement of Putrefaction and Chemical Change.—Relaxation again present; all power of contraction lost, not to be regained.
Cadaveric rigidity, or rigor mortis, is a purely muscular phenomenon, and is not dependent on the nervous system, as it is not [Pg 47] prevented, though it may be delayed, by division of the nerves, and is as well marked in paralysed as in non-paralysed limbs. Cadaveric rigidity, which occurs early in the heart, must not be mistaken for hypertrophy, or its absence for dilatation. In every case the rigor mortis precedes putrefaction, and consists in a shortening and thickening of certain muscles, chiefly the flexor and adductor muscles of the extremities, and also the elevators of the lower jaw.
This condition commences in the involuntary muscles, and in the heart may simulate hypertrophy of that organ, then passes into the voluntary muscles of the back of the neck and lower jaw, and then into the muscles of the face, front of the neck, chest, and upper extremities, and then into the trunk muscles, and last of all, into those of the lower extremities. In most cases it passes off in the same order, the body becoming quite flaccid, the rigor mortis never returning. These phenomena occur whilst the body is cooling. The muscle becoming rigid is dying, the rigid muscle is dead. The cause of the rigor mortis is held to be due to the coagulation of the myosin. The reaction is acid from the presence of sarcolactic acid, but becomes alkaline during putrefaction.
If fresh difibrinated blood be passed through the rigid muscle, it will become flaccid, and respond by contraction to electric stimulation.
Cadaveric rigidity generally supervenes from eight to twenty hours after death, and may continue from a few hours to four or nine days.
The sooner rigidity comes on after death the sooner will it pass away, and the later the onset the longer it will last. It is a general rule that whatever exhausts the muscular irritability before death causes the early appearance and the more rapid disappearance of rigor mortis.
Conditions which modify the onset and duration of rigor mortis:—
(1) Age.—Transitory rigor mortis may appear in the immature fœtus according to the state of its muscular development.
It is feeble and disappears quickly in infants and young children.
It is usually well marked in adolescents and healthy adults, but feeble in old people.
(2) The Degree of Muscular Development of the Body.—Other things being equal, the greater the muscular development and muscular strength at the time of death, the slower is the onset of rigor mortis, and the longer its duration; the more feeble or exhausted the muscular condition, the more rapid the onset and the shorter its duration.
(3) The Temperature of the Environment of the Body.—In temperate and colder climates rigor mortis follows the usual course. A low temperature, below freezing-point, will retard the onset and favour the duration of rigor mortis, but if the body be suddenly thawed before rigor mortis has set in, it will appear rapidly and disappear more quickly than if it had not been subjected to the process of thawing.
If a body already in a condition of early rigidity be exposed to a temperature of 75° C., the rigidity becomes more marked, since albuminates in the muscles, other than the myosin, become coagulated in addition. This phenomenon has been called heat stiffening.
(4) Mode of Death.—After all exhausting diseases of long or short duration, rigor mortis appears early and passes off quickly, as in death from phthisis, cholera, typhus fever, typhoid, hydrophobia, scurvy, and occasionally in chronic Bright‘s disease.
[Pg 48] Death during alcoholic intoxication favours the duration of rigor mortis. After violent muscular exercise death is quickly followed by rigidity. Animals that have been hunted for some time before death stiffen very rapidly. When convulsions precede death, rigor mortis sets in early as a rule, but in certain cases, where death has been preceded by strong convulsions, rigidity may appear quickly, but last for some days, as in some cases of poisoning by strychnine.
Conditions which simulate rigor mortis:—
(1) Stiffening by Catalepsy.—In this condition the temperature of the body will remain at a degree compatible with life over a period incompatible with real death. If a limb be extended and rigid in catalepsy, after passive flexion of it, it will return to its former state.
(2) Rigidity from the Body being Frozen.—In this condition passive movement of the joints is accompanied by crackling due to fracture of their frozen contents.
(3) Heat Stiffening.—Is seen in the bodies of persons who have been suddenly immersed in boiling fluids; also to a certain degree in bodies of persons who have met their death by burning from paraffin lamp accidents.
Cadaveric Spasm or Instantaneous Rigor.—“When this phenomenon occurs the last act of life is crystallised in death.” It is a prolongation of the last vital contraction of the muscles into the rigidity of death. Cadaveric rigidity of the muscles must be distinguished from muscular spasm occurring at the moment of death.
They may thus he distinguished: In cadaveric rigidity any object placed in the hand prior to the onset of rigor mortis can be readily removed, even if the precaution be taken of binding it in the hand prior to the accession of rigor mortis.
In the case of muscular spasm the object is found grasped in the hand, and can only be with difficulty removed.
The difficulty experienced in removing a pistol or other weapon from the hand may point to suicide; its easy removal to homicide, the weapon having been placed there after death.
No adequate explanation of this phenomenon has yet been made. It is not an unusually early onset of rigor mortis in the muscles affected, because they do not share in the initial relaxation that precedes it, or the weapon would fall from the hand, and the bodies would not retain the peculiar attitudes which have been described in different instances. Nothing can simulate cadaveric spasm and it cannot be produced in any way after death. Instantaneous rigor only occurs in cases in which there has been great mental tension and nerve excitation before death. It is a continuation of probably the very last voluntary act of life.
A body showing the signs of death before mentioned (Nos. 1 to 10) [Pg 49] may be held to be that of a person who has been dead from two to three days at the longest (Casper).
Muscular states of the body between the period of somatic and molecular death:—
(1) Primary Flaccidity.—The muscles respond to electrical stimuli; the chemical reaction of the muscles is either neutral or faintly alkaline.
(2) Cadaveric Rigidity or Rigor Mortis.—During this condition molecular death takes place; the muscles do not respond to stimuli, but fresh defibrinated blood passed through the muscles will restore the response to stimulation, and their reaction is markedly acid.
(3) Secondary Flaccidity.—Disintegration of the muscular elements takes place, no stimuli will provoke response, and the reaction again becomes alkaline.
Table showing the principal points to be noted in the period of accession of Cadaveric Rigidity and the causes which retard or hasten its appearance, or modify its duration:—
In what does it consist?—In a shortening and thickening of the muscles, particularly the flexors and adductors of the extremities, and elevators of the lower jaw.
Period of Invasion.—Generally in from eight to twenty hours after death. It has been known, however, to supervene within three minutes of death, but it may be delayed for sixteen or seventeen hours.
Period of Duration.—From one to nine days. Three weeks (Taylor).
Order in which the Muscles are affected.—Involuntary muscles, back of neck and lower jaw, muscles of the face, front of the neck, chest, upper extremities and then the lower extremities.
Order in which it disappears.—Back of neck, lower jaw, &c., following the course of its accession.
Effects of Exposure to Cold.—Prolonged by dry cold air, and by cold water.
Effects of Enfeebling Disease prior to Death.—Rapid in its invasion, and passing off rapidly.
Effect of a Robust Frame at Period of Death.—The accession may be prolonged; but, other things being equal, it is more strongly manifested, and continues longer.
Effects of Violent Exercise prior to Death.—Rapidly supervenes and rapidly disappears, as in soldiers killed at the end of a battle.
Effects of Poison.—Poisons which cause violent contractions for some time prior to death—strychnine, &c.—influence the rapid invasion of the rigor mortis, its short duration, rapidly followed by putrefaction. Where death in poisoning by strychnine is almost instantaneous, with a short convulsive stage, rigor mortis comes on rapidly and remains a long time.
11. Putrefaction.—the last of the phenomena which follow death—is the resolution of the organised tissues of the body to the inorganic state. It is a gradual process, and is the result of the action of micro-organisms, aided by moisture, air, and warmth.
Putrefaction is the only absolute sign of death having taken place.
The conditions which modify putrefaction are as follows:—
External Conditions.—1. Micro-organisms; 2. Air; 3. Moisture; 4. Warmth.
[Pg 50] Internal Conditions.—1. Age; 2. Sex; 3. Condition of the body—(a) Constitutional peculiarity; (b) State of the body. 4. Kind of death—(a) The result of disease; (b) The result of poisons.
1. Micro-organisms.—A fauna and flora of decomposition has been described in a paper by Hough on “The Fauna of Dead Bodies,” B. M. J., vol. ii. 1897, p. 1853, to which the reader is referred.
Many different forms of micro-organisms combine in the production of putrefaction, and the result of their action is inevitable, unless the body be guarded against their invasion by special means, or the tissues be rendered unfit for their use.
2. Air.—Exposure in the open air has a marked effect in promoting putrefaction; but garments fitting close to the body, and thus excluding air, have a contrary effect. Dry air, or air in motion, by assisting evaporation from the corpse, acts as a preservative. The composition of the soil in which the body is placed has also a more or less modifying effect. In light, porous soil, allowing of the free ingress of air, decomposition is more rapid than in close, compact soil, as clay; but in this we have to contend with another agent—moisture—which more or less counteracts the protective virtue of the closer earth.
3. Moisture.—Putrefaction cannot proceed without moisture. The body, however, contains sufficient water to enable this process to commence spontaneously. Organic substances artificially deprived of water do not putrefy. Cold and heat possess marked antiseptic properties—the former by freezing the fluids in the body, the latter by drying them up.
4. Warmth.—A temperature between 70° and 100° F. is found most favourable to decomposition. The effect of cold is shown by the fact that a body immersed in water during winter, at a temperature between 36° and 45° F., may be so well preserved as to present, ten or twelve days after death, well-marked signs of violence, which would in summer have been utterly obliterated in five or seven days. The preservative influence of cold water will, however, depend greatly on the depth at which the body has been submerged. Bodies so submerged, and then exposed to the air, putrefy with such rapidity that exposure for one day is said to work a greater change than three or four days longer retention of the body in the water. As an instance of the preservative power of cold, may be mentioned the mammoth found in Siberia embedded in a block of ice.
1. Age.—The bodies of young children, other things being equal, are said to putrefy rapidly. It should be remembered, however, that clothing possesses considerable power in retarding putrefaction, and that, in the hurry and anxiety to get rid of the infants, they are oftener exposed naked than clothed, which may, in some measure, account for their more rapid decomposition. [Pg 51]
2. Sex.—Sex, it would appear, has little or no influence either to retard or hasten putrefaction; but it has been remarked that females dying during or soon after child-birth, irrespectively of the cause of death, putrefy rapidly.
3. Condition of the Body.
(a) Constitutional Peculiarity.—It is generally admitted that persons of the same age and sex, dying similar deaths, and subjected to like conditions as to exposure to the air and interment in the same soil, exhibit marked differences as regards the accession and rapidity of putrefaction. The explanation may be difficult, but the fact still remains.
(b) State of the Body.—Fat and flabby corpses putrefy more rapidly than the lean and emaciated. Hence old people, who are generally thin, keep fresh for a comparatively long time. Bodies, also, which are much mutilated rapidly decompose—decomposition setting in first at the parts injured. In examining wounds and bruises said to have been inflicted during life, it is well to remember that the tendency of putrefaction is to make them appear more severe.
4. Kind of Death.
(a) Effect of Disease.—Healthy persons dying suddenly, other things being equal, are said to decompose more slowly than those who have died from exhausting diseases, as in the case of typhoid, phthisis, and dropsy, following organic disease, or of those diseases attended with more or less putridity of the fluids.
(b) Effects of Poisons.—Putrefaction rapidly supervenes in those who have died suffocated by smoke, by carbonic oxide, and by sulphuretted hydrogen. Narcotic poisoning is stated to accelerate this condition; but in poisoning by phosphorus or alcohol, and in cases of death from sulphuric acid, the putrefactive changes are greatly retarded. Arsenic, chloride of zinc, and antimony are reputed to possess antiseptic properties. The manner in which death takes place from the action of the poison greatly hastens or retards putrefaction. Thus, in the case of poisoning by strychnine, it is found that when death has occurred rapidly, without much muscular exhaustion, putrefaction sets in slowly; but that, when the muscular irritability has been greatly exhausted by successive fits, the contrary is the result.
One to Three Days.—Greenish coloration of the abdominal walls. Odour of putrescence is gradually developed, and, concurrently with this, the eyeball becomes soft and yielding to pressure.
Three to Five Days.—The green colour, of a deeper shade, has now passed over the abdomen, extending also to the genital organs. Patches of this green coloration also make their appearance somewhat irregularly on other parts of the body, such as the neck, back, chest, and lower extremities. A dark reddish frothy fluid about this time wells up from the mouth. [Pg 52]
Eight to Ten Days.—The patches of green colour have now coalesced, so that the whole body is discoloured. On some parts of the body the colour is of a reddish-green, due to the presence of decomposed blood in the cellular tissue. The abdomen is now distended with gases, the products of decomposition. In India this distension has been known to occur in less than six hours, the average period being a little over eighteen hours. Much depends upon the season of the year. The colour of the eyes has not disappeared, but the cornea have fallen in. Relaxation of the sphincter ani takes place, and the superficial veins appear like reddish-brown cords. The nails still remain firm.
Fourteen to Twenty Days.—The colour of the surface is now bright green, with here and there patches of a blood and brown colour. The epidermal layer of the skin is raised in bullæ of varying size, in some places the skin being more or less stripped off. The nails are detached, and can be easily removed. The hair can be pulled from the scalp with ease. The body is now greatly distended with gases, and the features cannot be recognised, owing to the swollen condition of the face. The body is generally covered with vermin. In determining the time at which death occurred, it will be necessary to take into consideration the season of the year, as it is found that an advanced stage of decomposition may be present in from eight to ten days, with the thermometer ranging between 68° and 77° F., which in winter, with a temperature of from 32° to 50° F., would require twenty to thirty days. “Bodies green from putridity, blown up and excoriated, at the expiry of one month, or from three to five months after death (cæt. par.), cannot with any certainty be distinguished from one another” (Casper).
Three to Six Months.—During the above period the stage of colliquative putrefaction has set in. The thoracic and abdominal cavities, due to the increased formation of gas, have burst. The bones of the cranium have more or less separated, allowing the brain to escape. The soft parts are more or less absorbed, and no recognition of the features is possible. The sex can only be positively made out by the presence of a uterus, or by the peculiar growth of hair on the pubes, which in woman only covers the pubes, but in man extends upwards to the navel.
Saponification.—Bodies exposed to the action of water, or buried in damp, moist soil, are apt to undergo certain changes, in the course of which they become saponified, and the formation of a substance known as adipocere is the result. Adipocere—adeps, lard, and cera, wax—is chiefly composed of margarate of ammonia, together with lime, oxide of iron, potash, certain fatty acids, and a yellow-coloured odorous matter. The melting-point is 126.5° F. Adipocere has a fatty, unctuous feel, is either pure white or of a pale yellowish colour, and with the odour of decayed cheese. It is highly resistant to putrefactive organisms, and is generally free from them. The formation of this substance “to any considerable extent is not likely to occur in less than three to four months in water, or six months in moist earth, though its commencement [Pg 53] may take place at a much earlier period” (Casper). The above-quoted authority mentions a case in “which the remains of a fœtus were found imbedded in adipocere, and which fœtus was proved to have been buried in a garden exactly six months and three-quarters.” Taylor also records the case of a bankrupt who committed suicide by drowning, in which the muscles of the buttocks were found converted into adipocere in five weeks and four days at the longest.
Although the above statements may be accepted with regard to the formation of adipocere as far as European countries are concerned, they do not seem to be applicable to India, where the change appears to be more rapid. Dr. S. Coull Mackenzie, in his valuable book on Medico-Legal Experiences in Calcutta, records a case of a young man whose body, recovered after seven days‘ immersion in the river Hooghly, “was found to be in an advanced state of saponification,” and the fleshy portions of undigested food in the stomach were converted entirely into adipocere. “Lastly,” he writes, “in the hot, steamy, rainy months of September and October, in three of the cases above mentioned, saponification was found in bodies immersed in water, both externally and internally, in from two days to eight days ten hours. In the soft and porous soil of Lower Bengal during the rainy seasons, even in a wooden coffin, the change is very rapid—three or four days.”
To explain the formation of adipocere, it has been supposed to be due to the decomposition of the muscular structures of the body, by which hydrogen and nitrogen are evolved, these combining to form ammonia, and this, coming in contact with the fatty acids of the fat, forms a soap. The process of saponification takes place most rapidly in young fat persons; next, in those adults who abound in fat, and in those whose bodies have been exposed to the soil of water-closets; more rapidly in running than in stagnant water; and lastly, in those who have been buried in moist, damp soil, especially if the bodies have been piled one on the top of the other, the lowest being first saponified. The muscular tissue appears to be the first to undergo this change. In water the process is said to be completed in about five months, but in soil a period of two or three years appears necessary.
Mummification is of no medico-legal interest, as the causes which produce it are unknown, and no reliable data can be obtained as to the period of its accession, or the time required for its production.
Table showing the order
in which the
Internal Organs undergo Putrefaction:
1. The Trachea, including the Larynx.—The rapid change in the trachea must be borne in mind, in order to avoid the error of attributing death to suffocation or drowning. An examination of the trachea should never be omitted.
2. The Brain of Infants up to the First Year.
3. The Stomach.—The first traces of putrefaction are seen in from four to six days after death. All the coats of the stomach are softened, but there is no excoriation, as is the case when corrosive poisons are taken. Emphysematous separation of the mucous coat may be present, but must not be confounded with the excoriation just mentioned.
4. The Intestines.—Casper declares that he does not remember any case in the course of his experience where the intestines were “found earlier putrefied than the stomach.” In the course of putrefaction they become of a dark brown colour, bursting, and allowing an escape of their contents; and they ultimately become changed into a dark pultaceous mass.
5. The Spleen.—This organ in some cases putrefies before the stomach and intestines; but, as a rule, it resists decomposition longer.
6. The Omentum and Mesentery.
7. The Liver.—This organ is not unfrequently found firm and dense some weeks after death. It putrefies earlier in new-born children than in adults. The convex surface first shows signs of putrefaction. The gall-bladder also remains for some time recognisable.
8. The Adult Brain.—The brain of newly-born children, as mentioned before, soon putrefies. This is not the case in the adult brain. Putrefaction sets in not on the surface, but at the base of the brain. A wound of the brain causes it to putrefy more rapidly than if no injury be present.
9. The Heart.
10. The Lungs.—Contemporaneously with the appearance of decomposition in the heart, the lungs also begin to show signs of putrefaction, though this condition may take place earlier.
11. The Kidneys.—These organs are long in yielding to the putrefactive process.
12. The Bladder.—Nearly all the other organs of the body are in a state of decomposition before this viscus becomes materially affected.
13. The Gullet.—This long remains firm, even after the stomach and intestines fail to be recognised.
14. The Pancreas.—The body must be far advanced in putrefaction before this gland becomes affected.
15. The Diaphragm.—This may be distinguished after the lapse of four to six months. [Pg 55]
16. The Blood-vessels.—The aorta may be recognised after the body has been interred for fourteen months.
17. The Uterus.—Of all the organs of the body, the uterus resists the putrefactive changes longer than any other organ.
Table showing some important Facts to be
noticed with regard To Putrefaction:
Does Lime hasten Putrefaction?—It is a very general opinion that it does. Careful experiment has, however, proved that lime neither retards nor hastens putrefaction, but that it prevents the escape of the gases produced during the process by absorbing them; it is, therefore, a good and safe deodoriser, and in this property its true value lies.
The following are some of the Instructions issued to Medical Inspectors by the Crown Office in Scotland, slightly modified:
13. When any portions of the body, or any substances found in or near it, are to be preserved for further examination, they ought never to be put out of the custody of the inspectors, or of a special law officer. They must be locked up in the absence of the person who keeps them. When they are to be transmitted to a distance, they should be labelled, and the labels signed by the inspectors; and after being properly secured and sealed, they should be delivered by the inspectors themselves, or the special law officer whose duty it is to see them delivered into the hands of the parties for whom they are intended.
14. Besides the ordinary instruments used in common dissections, the inspector should be provided with a foot-rule for measuring distances, and a glass measure graduated to drachms, for measuring the quantities of fluids, two or three stoneware jars of medium size, or when these cannot be had, a few clean bladders, for carrying away any parts of the body which it may be necessary to preserve for future examination, and in cases of possible poisoning, three or four bottles of eight, twelve, and sixteen ounces, with glass stoppers or clean corks, for preserving fluids to be analysed. The common square green glass pickle bottles are very suitable, and can generally be obtained. No bottle or jar should be used until it has been thoroughly washed under the supervision of one of the inspectors. In cases of infanticide a balance, having a flat scale-pan with a foot-rule painted on it, is of great use; on it the infant may be stretched, weighed, and measured at one operation. Paper, pens, ink, and sealing-wax should also be provided.
15. All distances, lengths, surfaces, and the like, whose extent may require to be described, ought to be accurately measured; and the same rule ought to be followed in ascertaining the volume of fluids. When large quantities of fluids are to be measured, any convenient vessel may be used, whose capacity is previously ascertained by the inspectors. Conjectural estimates and comparisons, however common, even in medico-legal inspections, are quite inadmissible.
16. The importance of the external examination, and the particulars to be chiefly attended to in performing it, will vary in different cases with the probable cause of death. It comprehends an examination—(1) Of the position of the body when found, as well as of all external injuries or marks presented by it. (2) Of the vicinity of the body, with a view to discover the objects on which it rested, or from or upon [Pg 57] which it may have fallen, marks of a struggle, signs of the presence of a second party about the time of death or after it, weapons or other objects the property or not the property of the deceased, the remains of poisons, marks of vomiting; and where marks of blood are of importance, and doubts may arise as to their really being blood, the articles presenting them must be preserved for further examination. (3) Of the dress, its nature and condition, stains on it of mud, sand, and the like, of blood, of vomit, of acids, or other corrosive substances, marks of injuries, such as rents or incisions; where injuries have been inflicted on the body, care should be taken to compare the relative position of those on the body and those on the clothes; and where stains, apparently from poison, are seen, the stained parts are to be preserved for analysis. (4) Ligatures, their material and kind, as throwing light on the trade of the person who applied them; the possibility, or impossibility, of the deceased having applied them himself; their sufficiency for accomplishing their apparent purpose, &c.
17. The inspectors will commence the examination of the body itself by surveying the external surface and openings. Before cleaning it they will examine it on all sides, not neglecting the back, as is often done, and look for marks of mud, blood, ligatures, injuries, stains from acids, and the like; foreign bodies, or injuries within the natural openings of the body, viz. the mouth, nostrils, ears, anus, vagina, and urethra. If there are impressions of finger marks, they will consider which hand produced them. If there be any doubt about stains being blood, the skin presenting them must be preserved for analysis. If there be acid stains, or other probable remains of poison, or any foreign matter, the nature of which may require to be determined by analysis, these must also be preserved. The ordinary places for the impressions of ligatures are the neck, the wrists, the ankles, and the waist. The degree of warmth of the trunk and extremities, the presence or absence of cadaveric rigidity, and whether it exists equally in the upper or the lower extremities, should be noted in this stage of the proceedings; in other cases the progress of putrefaction, as indicated by the odour of the body, the looseness of the cuticle, the colour of the skin, and formation of dark vesicles on it, the evolution of air in the cellular tissue, the alteration of the features, the softness of the muscles, the shrivelling of the eyes, the looseness of the hair and nails.
18. In this part of the examination it will sometimes be necessary to observe the particulars by which the body may be identified. These are numerous. But the most important are the stature, the age and sex, the degree of plumpness, the size and form of the nose and mouth, the colour of the eyes and hair, the state of the teeth, warts, nævi, deformities, scars of old abscesses, ulcers, and wounds, and, if a woman, marks of her having had one or more children.
19. The body is next to be washed, if necessary, and the hair of the head shaved, or at least closely cut; and a thorough examination of the whole integuments is to be made. At this stage the inspectors will look particularly for the appearance of lividity, noting its chief seat and its relation to the posture in which the body was found—for impressions on the skin of objects on which it had rested—for marks of injuries, more especially contusions, taking care to ascertain their real nature by making incisions through the skin—for marks of disease, such as eruptions, ulcers, and the like—for marks of burning—for marks of concealed punctures in the nostrils, mouth, external openings of the ears, the eyes, the nape of the neck, the arm-pits, the anus, the vagina, and beneath the mammæ or scrotum; in infants, also in the fontanelles and the whole course of the spine. At this stage, wounds and other injuries should be carefully examined according to the directions given in Division V. (infra). Where the injury may have caused loss of blood, the presence or absence of pallor of the skin, lining membrane of the mouth, and the gums ought to be noted. [Pg 58]
20. In commencing the dissection of the body, it must be laid down as an invariable rule that all the great cavities should be examined, and also every important organ in each, however distinctly the cause of death may seem to be indicated in one of them. It is right to examine the cavity of the spine, and at all events its upper portion, in any case where an unequivocal cause of death has not been discovered elsewhere.
21. In examining the organs situated in the several cavities of the body the inspectors must be guided in a great measure by their ordinary anatomical and pathological knowledge.
22. The inspectors should begin with that cavity over which there is a wound or other mark of injury. Or, if there be an injury on the extremities, the dissection ought to commence there. In the absence of any such guide, that cavity should be taken first where the circumstances of death, so far as they are ascertained, may lead the inspectors to expect unusual appearances. In other cases, the abdomen should be first opened but not dissected, and a general survey made of the parts exposed, without disturbing them materially, the position of the diaphragm being determined by examining it with the hand; then the thorax is immediately to be examined, unless there is good reason for doing otherwise. The reasons for this method of procedure are as follow: If the abdominal organs are removed, and the veins cut, the blood in the heart may drain away through the venæ cavæ, and error result. If, on the other hand, the thorax be first opened, the relation of the abdominal organs to each other cannot be clearly made, owing to the relaxation of the diaphragm, due to the severing of its thoracic connections. Again, if the thorax be first opened, the position of the diaphragm cannot be determined. The inspectors may begin with the head, which may be examined thoroughly in the first instance, afterwards the chest and belly, as above described; the spine being reserved till the conclusion. Wherever unusual appearances are discovered in the first cursory survey, the anatomical examination ought in general to be begun there.
23. In examining the several regions of the body it is to be observed that wherever a wound, or other obvious injury of the external parts, lies in the way of the ordinary incisions, that part must be avoided, so as to leave the external injury unaltered.
24. The most approved mode of opening the head in medico-legal cases is, after dividing the integuments from ear to ear, and reflecting the scalp over the forehead and occiput, to make the usual circular incision through the skull, about an inch above the orbits in front, and over the occipital protuberance behind, using the saw lightly and carefully after the outer table of the skull has been divided, so as to avoid injuring the membranes of the brain; and to raise the skull-cap from before backwards, taking care to detach the dura mater from the skull with the handle of the scalpel or a spatula where it adheres firmly. The chisel and mallet should never be used where there is any chance of finding a fracture of the skull; for how could it be distinguished from a fracture made with the mallet? Should the dura mater be firmly adherent to the skull-cap, the better practice is to divide it carefully, so as to remove both at the same time. Tearing the membrane and crushing the brain substance are thus avoided. In infants and young children this mode of procedure is most necessary, as in them the dura mater is, as a rule, adherent.
25. The ordinary mode of examining the membranes of the brain, and the brain itself, answers well in medico-legal dissections. Effusions of fluid within the skull should always be measured. After the brain is removed, the dura mater ought to be stripped from the base of the skull to facilitate the search for fractures there, which will, of course, [Pg 59] indicate external violence. After the removal of the brain, the upper part of the spinal canal should be examined through the foramen magnum before any part of its course be laid open; and search should be particularly made for dislocation or other injury in the region of the atlas and dentata. In cases of fatal fractures of the head, the strength of the bones should be attended to. In cases of extravasation within the head, the state of the coats of the cerebral arteries should be examined.
26. The best mode of opening the spine is, after having finished the examination of the brain, to cut through the integuments from the occiput to the coccyx—to lay the vertebræ thoroughly bare on each side by cutting away the muscles—to make an incision with the saw on each side of the skull, from the postero-inferior angle of the parietal bones into the lateral edge of the occipital hole—to remove the triangular portion of the occipital bone thus detached, and then to cut the rings of the vertebræ on each side with the bone-nippers or spine-knife, beginning with the atlas. In these cases preference should be given to the saw, by which the operation is not only more easily accomplished, but there is no risk of confounding previous fracture with that made in dissecting. Where there is reason to think that the bones are injured, the laying open of the canal should stop at the distance of two or three vertebræ from the injury, and the injured bones, with two or three adjacent vertebræ on each side, should be removed entire before the examination is extended farther down the spine.
27. The organs of the throat may be examined, either by dividing the lower jaw-bone at the chin, cutting the soft parts close to the inner surface of each half of the bone backwards, and then turning the two segments outwards; or by freely reflecting the skin of the throat, separating the soft parts from the inside of the lower jaw, the knife being carried parallel with and close to the bone, drawing the tongue out below the chin, and then continuing the dissection backwards.
28. The best mode of examining the organs situated in the throat is, after detaching the soft parts from the lower jaw, as advised in Sect. 27, to dissect the soft palate from the bone, and proceeding backwards, to detach the whole soft parts from the base of the skull and vertebræ down to the sternum, leaving them connected with the organs in the chest. Besides the ordinary points to be attended to in this part of the examination, the presence of venereal or other ulcerations is a matter requiring attention in some cases.
29. It is necessary to examine the pharynx and gullet, the larynx, trachea, and its greater ramifications, the lungs, the heart, and the great vessels with particular care, because here are most frequently found the causes of sudden natural death. In examining the heart each auricle and each ventricle ought to be laid open by an independent incision of its parietes; and this should not intersect any of the valvular openings or the septum cordis.
30. For laying open the chest and abdomen, the most convenient method is to make an incision down the fore part of the neck, chest, and abdomen to the pubes; then cutting from the peritoneum upwards, to dissect back the integuments and muscles of the chest, and examine the abdomen, as in Sect. 22; next, divide the cartilages of the ribs, and, cutting upwards, close under them, to raise the cartilages along with the sternum. In separating the sternum from the clavicles, care must be taken not to wound the subjacent vessels; and this may be avoided by the dissector moving each shoulder so as to show the exact position of the sterno-clavicular joints, and then dividing both joints cautiously. In dividing the cartilages of the ribs, the saw is sometimes necessary. The cartilages should be cut as far from the sternum as possible, to give free space for the subsequent examination. [Pg 60]
31. In inspecting the organs in the chest, a cursory examination should be first made by turning them over, ascertaining the nature and measuring the quantity of effused fluids, feeling for fractures of the ribs, tumours, or other diseases, and opening the pericardium to obtain a view of the heart. The most convenient course to pursue next is, without moving the heart from its place, to lay open its several cavities, in order to judge of the quantity and state of the blood in both sides of that organ. For this purpose the following incisions should be made: The first, beginning close to the base, is carried along the right border of the heart directly into the right ventricle towards the apex, care being taken not to cut the septum. This lays open the right ventricle. The second incision, opening up the right auricle, begins midway between the entrances of the venæ cavæ, ending just in front of the base. The third, for exposing the left auricle, commences at the left superior pulmonary vein, and ends just in front of the base, close to the coronary vein, care being taken not to wound it. The fourth, displaying the left ventricle, commences behind the base, and ends close to the apex. If the blood is in a fluid state, the quantity contained in the right auricle may be materially affected by the head being examined previously, as the blood may have escaped from the heart by the jugular veins. The whole of the organs in the chest—the lungs, heart, and gullet—together with the parts dissected downwards from the throat, should now be removed in one mass, in order to examine them in detail on a table. But previously two ligatures should be applied on the gullet, just above the cardiac orifice of the stomach, and the division made between them.
32. The organs in the abdomen ought to be turned over, like those of the chest, before any one of them is minutely examined, but before the thorax is opened, for the reasons given in Sect. 22. In the subsequent examination, that organ is to be first proceeded with in which there may appear to be disease.
33. In a post-mortem examination, the most approved mode of examining these injuries is, if they be situated over great cavities, to expose the successive structures in the manner of an ordinary dissection, observing carefully what injuries have been sustained by the parts successively exposed before they are divided. Wounds ought not to be probed, especially if situated over any of the great cavities. The depth of a wound is best ascertained by careful dissection and exposure of the parts involved; but after this is done, the thickness of the tissues penetrated may be measured by the probe.
34. The seat of the wounds must be described by actual measurement from known points, their figure and nature also carefully noted, and their direction ascertained with exactness.
35. Before altering by incisions the external appearances of injuries, which should never, if possible, be done, care must be taken to consider what weapon might have produced them, and if a particular weapon be suspected, it should be compared with them. The wounded parts should be cut out entire, and carefully preserved.
36. Apparent contusions must be examined by making incisions through them; and the inspectors will note whether there is a swelling or puckering of the skin; whether the substance of the true skin be black through a part or the whole of its thickness; whether there be extravasation below the skin or in the deeper textures, and whether the blood be fluid or coagulated, generally or partially; whether the soft parts below be lacerated, or subjacent bones injured; and whether there be blood in contact with the lacerated surfaces. By these means the question may be settled whether the contusions were inflicted before or after death. [Pg 61]
37. In the cases of wounds, too, the signs of vital action must be attended to, especially the retraction of the edges, adhesion of blood to their surfaces, or the injection of blood into the cellular tissue around, or the presence of the signs or sequelæ of inflammation. Hypostasis must not be mistaken for vascular injection.
38. When large arteries or veins are found divided, care must be taken to corroborate the presumption thus arising by ascertaining, in the subsequent dissection, whether the great vessels, lungs, liver, and membranous viscera of the abdomen be unusually free of blood.
39. In the course of the dissection of wounds, a careful search must be made for foreign bodies in them. When firearms have occasioned them, the examination should not be ended before discovering the bullet, wadding, or other article, if any, lodged in the body; and whatever is found must be preserved. When the article discharged from firearms, or when any other weapon had passed through and through a part of the body, the two wounds must be carefully distinguished by their respective characters, especially as regards their comparative size, inversion or eversion, smoothness or laceration, of their edges, their roundness or angularity, and the comparative amount of bleeding from each. In gunshot injuries, the presence or absence of marks of gunpowder should be noted.
40. When wounds are situated over any of the great cavities, they ought not to be particularly examined until the cavity is laid open; and in laying open the cavity, the external incisions should be kept clear of the wounds.
41. When the discoloured state of a portion of the skin is such as to render it doubtful whether it is due to injury or to changes after death, an incision should be made to ascertain whether there is blood effused into the textures, constituting true ecchymosis, or merely gorging of the vessels of the skin, or discoloration from infiltration of the colouring matter of the blood, which takes place in depending parts of a dead body. The term suggillation should be avoided, as it has been used in opposite senses by Continental and British authors. The respective expressions, “discoloration from extravasated blood,” and “lividity after death,” are preferable.
42. In examining a body in a case of suspected poisoning, the inspectors should begin with the alimentary canal, first tying two ligatures round the gullet, above the cardiac orifice of the stomach, two round its pyloric end, and a third at the sigmoid flexure of the colon, then removing the stomach and entire intestines; next dissecting out the parts in the mouth, throat, neck, and chest in one mass; and, finally, dissecting the gullet, with the parts about the throat, from the other organs of the chest. The several portions of the alimentary canal may then be examined in succession.
43. Previous to commencing the dissection in cases of supposed poisoning, the inspectors should make such inquiries as may enable them to form an opinion as to the class of poison to which the death may be traceable, and thus to guide them as to the conclusions to be come to from the presence, or it may be the complete absence, of any marked appearance explaining the cause of death.
44. The medical inspectors may afford most important aid to the law officers in investigating the history of cases of supposed poisoning. For this purpose minute inquiry should be made into the symptoms during life their nature, their precise date, especially in relation to meals or the taking of any suspicious article, their progressive development, and the treatment pursued. It is impossible to be too cautious in [Pg 62] collecting such information, and, in particular, great care must be taken to fix the precise date of the first invasion of the symptoms, and the hours of the previous meals. The same care is required in tracing the early history of the case, where the inspector happens to visit the individual before death; and if suspicions should not arise till his attendance has been going on for some time, he ought, subsequently to such suspicions, to review and correct the information gathered at first, especially as to dates. All facts thus obtained should be immediately committed to writing.
45. Besides inspecting the body and ascertaining the history of the case, the inspectors may afford valuable assistance to the law officers in searching for suspicious articles in the house of the deceased. These are—suspected articles of food, drink, or medicine; the vessels in which they have been prepared or afterwards contained; the family stores of the articles with which suspected food, &c., appears to have been made. All such articles must be secured, according to the rules in Sect. 13, for preserving their identity. In this examination the body-clothes, bed-clothes, floor, and hearth should not be neglected, as they may present traces of vomited matter, acids spurted out or spilled, and the like.
46. When a medical man is called to a case during life, where poisoning is suspected, he ought as soon as possible to follow the instructions laid down for securing articles in which poison may have been administered.
47. In the same circumstances, it is his duty to observe the conduct of any suspected individual, were it for no other reason than to prevent the remains of poisoned articles from being put out of the way, and to protect his patient against further attempts.
48. The whole organs of the abdomen must be surveyed, and particularly the stomach and whole tract of the intestines, the liver, spleen, and kidneys, the bladder; and in the female, the uterus and its appendages. The intestines should in general be split up throughout their whole length; and it should be remembered that the most frequent seat of natural disease of their mucous membrane is in the neighbourhood of the ileo-cæcal valve, and that, next to the stomach, the parts most generally presenting appearances in cases of poisoning are the duodenum, upper part of jejunum, lower part of ileum, and rectum.
49. In cases where the possibility of poisoning must be kept in view, and where matters may require to be procured for chemical analysis, it is essential to be sure that all instruments, vessels, and bladders used are scrupulously clean.
50. When any unusual odour is perceived, either in the blood in the course of making the dissection, or in the stomach when opened, it ought to be carefully observed, and if possible identified by all the medical men present. In this way alcohol, opium, prussic acid, oil of bitter almonds, and other odorous poisons may be recognised. The smell of the contents of the stomach ought always to be noted whenever it is opened, as the smell often alters rapidly.
51. The stomach and intestines should be taken out entire, and their contents emptied into separate bottles. If the stomach or part of the intestines present any remarkable appearance, examination may be reserved, if convenient, till a future opportunity; but in every circumstance it must be preserved and carried away, as it may itself be an important article for analysis. The throat and gullet may be examined at once, and preserved with their contents, which, if abundant, may be kept apart in a bottle. In addition to the alimentary canal and its various contents, portions of the solid organs of the body ought to be secured for analysis. The most important are the liver, spleen, and kidneys. A part of the liver, at least a fourth part, should be secured in every case of supposed poisoning; and in cases where the fatal illness has been of long duration, and therefore [Pg 63] only traces of the poison may remain in the body, the whole of the liver, the spleen, and both kidneys should be secured. A portion of the blood, especially when the odour of any volatile poison is perceived, should be at once put into a bottle, closed by a good cork or stopper.
52. No person ought to undertake an analysis in a case of suspected poisoning unless he be either familiar with chemical researches, or have previously analysed with success a mixture of organic substances, containing a small proportion of the poison suspected.
53. All persons undertaking an analysis should bear in mind that the opinion of some other person practised in toxicological researches may be required; and they should therefore take care, when practicable, to use only a portion of the several articles preserved for analysis. The identity of the subjects for analysis must be secured by the rules in Sect. 13.
54. In cases of suspected drowning, the inspectors will observe particularly whether grass, mud, or other objects be clutched by the hands, or contained under the nails; whether the tongue be protruded or not between the teeth; state of the penis; whether any fluid, froth, or foreign substances be contained in the mouth, nostrils, trachea, or bronchial ramifications; whether the stomach contains much water; whether the blood in the great vessels be fluid. Careful pressure should be made upon the lungs; any fluid contained in them in thus forced into the bronchial tubes and trachea, and its nature observed. When water with particles of vegetable matter or mud is found within the body, these must be compared with what may exist in the water in which the body was discovered, and should be preserved for further scientific investigation, if requisite. Marks of injuries must be compared diligently with objects both in the water and on the banks near it, and especial attention given to the question—whether any observed injuries had been sustained by the body before or after death.
55. In cases of suspected death by hanging, strangling, or smothering, it is important to attend particularly to the state of the face as to lividity, compared with the rest of the body; the state of the conjunctiva of the eyes as to vascularity; of the tongue as to position; of the throat, chin, and lips as to marks of the nails, scratches, ruffling of the scarf-skin, or small contusions; the state of the blood as to colour and fluidity; the state of the heart as regards the amount of blood in its several cavities; the state of the trunk and branches of the vena cava in the abdomen as regards distension with blood; and the state of the lungs as regards congestion, rupture of any of the air cells, and small ecchymoses under the pleura, or the pericardium. The mark of a cord or other ligature round the neck must be attentively examined; and here it requires to be mentioned that the mark is often not distinct till seven or eight hours after death, and that it is seldom a dark livid mark, as is very commonly supposed, but a pale greenish-brown streak, presenting no ecchymosis, but the thinnest possible line of bright redness at each edge, where it is conterminous with the sound skin. Nevertheless, effusions of blood and lacerations should be also looked for under and around the mark, in the skin, cellular tissue, muscles, cartilages, and lining membrane of the larynx and trachea. Accessory injuries on other parts of the body, more especially on the chest, back, and arms, must also be looked for, as likewise the appearance of blood having flowed from the nostrils or ears, and the discharge of fæces, urine or semen. In cases where death may be due to the emanations from burning fuel or other poisonous vapours, a small phial should be filled with the fresh blood, and securely corked for further investigation, if requisite. [Pg 64]
56. In supposed death by burning, the skin at the edge of the burns should be carefully examined for redness, or the appearance of vesicles containing fluids.
57. In suspected criminal abortion, when the woman survives, the chief points for inquiry are: The proofs of recent delivery, the ascertaining of facts tending to show that she has been subjected to manœuvres with instruments, and the occurrence of symptoms traceable to the action of any of the drugs reputed as capable of causing abortion.
When the woman has died, the points requiring special attention at the dissection are: The state of the womb, as regards its size and the condition of its lining membrane, in reference to the probable period of delivery; the condition of the intestinal canal, in reference to the action of irritant drugs; of the mucous membrane of the bladder, in reference to the action of cantharides; close inspection of the womb and vagina, in reference to mechanical injuries, especially punctured wounds; and any appearances that the death may have been caused by inflammation in the organs of the pelvis, or by bleeding from the wound.
58. In cases of suspected infanticide, certain specialities must be borne in mind. The cavity of the head should be laid open with a pair of scissors. In opening the abdomen, the navel should be avoided, so that the state of the vessels of the navel-string may be examined correctly. This is done by carrying two incisions from the ensiform cartilage to each of the anterior superior spines of the ilia, and by deflecting downwards the triangular flap thus formed.
59. The inquiry in cases of infanticide should be conducted with reference to the five following distinct questions: (1) The probable degree of maturity of the child? (2) How long it has been dead? (3) Whether it died before, during, or after delivery, and how long after? (4) Whether death arose from natural causes, neglect, or violence? and (5) Whether a suspected female be the mother of the child?
60. The points to be attended to for ascertaining the probable degree of maturity of the child are: The general appearance and development, the state of the skin, its secretions, and its appendages; the hair and nails; the presence or absence of the pupillary membrane; the length and weight of the whole body; whether the navel corresponds or not with the middle of the length of the body; the situation of the meconium in the intestines; the size of the testicles in the case of males, and in either sex the size of the point of ossification in the lower epiphysis of the thigh-bone. This is easily observed by making an incision across the front of the knee into the joint, pushing the end of the thigh-bone through the cut, slicing off the cartilaginous texture carefully until a coloured point is observed in the section, and then, by successive very fine slices, ascertaining the greatest diameter of the bony nucleus. This does not exist previous to the thirty-sixth week of gestation, and in a mature child is about one-fourth of an inch in diameter. Has the infant been washed? Absence or presence of vernix caseosa. Nature and character of the wrappings, if any, found on the child.
61. The points of chief importance in reference to the period which has elapsed after death are those specified in the last clause of Sect. 17—it being borne in mind that the bodies of infants are often concealed in ash-pits and dunghills, and that in these circumstances putrefaction is very rapid.
Plate.—Section
through the epiphysis
of the lower end of the femur showing
ossification centre, in a full-term fœtus.
[Pg 65] 62. The circumstances which indicate whether the child died before, during, or after parturition, and how long after it, are the signs of its having undergone putrefaction within the womb; the marks on the crown, feet, buttocks, shoulders, &c., indicating presumptively the kind of labour, and whether it was likely to have proved fatal to the child; the state of the lungs, heart, and great vessels, showing whether or not it had breathed; the nature of the contents of the stomach and of the intestines; the presence of foreign matters in the windpipe; the state of the umbilical cord, or of the navel itself, if the cord be detached.
63. In order to examine properly the state of the lungs, heart, and great vessels, with a view to determine whether or not the child had breathed, the inspection should be made in the following order: Attend, first, to the situation of the lungs; how far they rise along the sides of the heart; to their colour and texture; whether they crepitate or not. Then secure a ligature round the great vessels at the root of the neck, and another round the vena cava above the diaphragm. Cut both sets of vessels beyond the ligatures, and remove the heart and lungs in one mass, which must be weighed and put into water, to ascertain whether the lungs, with the heart attached, sink or swim. In the next place, put a ligature round the pulmonary vessels, close to the lungs, and cut away the heart by an incision between it and the ligature. Lastly, ascertain the weight of the lungs; whether they sink or swim in water; whether blood issues freely or sparingly when they are cut into; whether any fragments swim in the instances where the entire lungs sink; and in every instance of buoyancy whether fragments of them continue to swim after being well squeezed in a cloth.
64. The general question to be considered in relation to the cause of death is, whether the appearances are such as to be traceable to the act of parturition, or whether they indicate some form of violent death. The directions given in Divisions V., VI., and VII. apply to infants as well as adults; but the following points are specially to be noticed in cases of supposed infanticide:
In relation to wounds and contusions, the possibility of minute punctured wounds of the brain or other vital organs; in reference to injuries of the head, the effusion of blood under the scalp, not in the situation where it could have been produced during labour, or fracture of the bones not producible by compression of the head during labour, and not connected with defective ossification of the skull; in reference to the allegation that the head was injured by the child suddenly dropping from the mother, when not recumbent, the presence of sand or other foreign matters on the contused scalp, and the existence of more than one injury of the head; in relation to suffocation, the external and internal signs of this form of death—marks of compression of the mouth, and nose, and throat, and the presence of foreign matters in the mouth and throat, air-passages, gullet, or stomach, especially if the body be found in contact with similar substances; in reference to bleeding from the navel-string, a bloodless state of the body, without any wound to account for it; in reference to poisons, most commonly narcotics, the absence of any of the above appearances, with an otherwise healthy state of the body; in reference to starvation and exposure, emaciation of the body, absence of food from the stomach, and an empty, contracted condition of the intestines; in reference to the possibility of the child having been suddenly expelled, and having fallen on the floor or into privies, &c., the state of the navel-string is to be noted—whether long or short, whether remaining attached to the child and connected with the after-birth, indicating rapid labour, or, if divided, whether it had been cut or torn across. Nature of the ligature used, if any.
65. The circumstances noticed in Sects. 60, 61, 62, 63, 64, compared with the signs of recent delivery in the female, will lead to the [Pg 66] decision of the question whether the suspected female be the mother of the child. These circumstances may be shortly recapitulated as being the signs of the degree of maturity of the child—the signs on the body of the kind of labour, the signs which indicate the date of its death, and the interval which elapsed both between its birth and death, and between its death and the inspection.
It becomes necessary sometimes to exhume the bodies of persons who have been buried. The cases which generally call for this always unpleasant proceeding are those where a suspicion of poisoning or violence has arisen some little time after the burial of the supposed victim. Or the necessity may arise to show that the body buried is that of a person whose death it is absolutely necessary to prove. In the case of Livingstone, though this can scarcely be called a case of exhumation, yet an examination some months after death of the arm of the corpse alleged to be that of Livingstone, proved the existence of a badly united fracture which the deceased was known to have had.
In conducting the exhumation, it is necessary that the medical experts should be present to see the body removed from the coffin, and also any person or persons who may be in a position to speak as to the identity of the corpse—as, for instance, those who dressed it and prepared it for burial. The person who made the coffin may also be of assistance to speak as to its identity. As soon as the medical men are armed with the proper authority, no time should be lost in order to get the body as fresh as possible, and at once prove or disprove the accusation of the crime, which, in the case of innocent persons, cannot be too quickly removed. The best time to take up the body, if in the summer, is early in the morning; and, in all cases, the examination, if possible, should be made during daylight. Everything necessary for making a medical inspection should be taken, and also a table on which to place the body. Rubber gloves should be worn. A pail containing a solution of some disinfectant, for the inspectors to wash their hands after the exhumation is finished, should be close at hand. And it is as well to expose the body for a short time to the air before beginning the inspection. There is seldom any risk to health in removing a single body, yet certain precautions are necessary; thus it is as well to stand on the windward side of the corpse. Vaults should not be entered as soon as they are opened, but time allowed for their ventilation. Carefully note the amount of preservation of the coffin, and, if broken, if any of the surrounding earth is in contact with the body. This precaution is necessary in cases of suspected mineral poisoning (as in arsenic, &c.), and it is as well also to save one or two pounds of the earth immediately above the coffin for analysis. The body may then be examined externally, any hair left on head or face preserved for identification; and then an inspection of all the cavities made, the contents of the stomach and bowels being placed in dry earthenware jars or glass bottles, corked and capped with thin indiarubber skin, [Pg 67] and so tied and sealed that the string must be cut or the seals broken in order to open them. The ends of the string should be sealed in the presence of the authorities. In the examination, the instructions previously given should be carefully followed. All injured or diseased parts should be removed and preserved whenever this is practicable. Soft parts not intended for analysis may be preserved in a concentrated solution of salt.
Beyond what Period is it useless to Exhume a Corpse?—There is no scientific limit, for even the bones may show that violence has been used, or may point to the identity of a corpse, as in the case of Livingstone just mentioned. Pregnancy may be detected. The medical inspectors must proceed with the inspection unless they can positively say that the progress of decay is such as to render the examination nugatory in relation to its special objects. Casper mentions the case of a man whose body was three times exhumed for different purposes. In Scotland the law imposes a limit of twenty years, but in England the law is silent on the point; in France a limit of ten years from the date of the supposed crime; and in Germany, the limit is thirty years, if the offence is that punishable with death, the time varying from three to thirty years with the nature of the crime.
Assault.—Every act of attack upon the person of another is an assault in law, whether it injure or not; nor is it necessary that the act done take effect. Spitting on anyone is an assault. No provocation by word, whether written or spoken, can justify an assault, though it may mitigate the offence. If a medical man unnecessarily strip a female patient naked, under pretence that he cannot otherwise judge of her illness, it is an assault if he himself take off her clothes (R. v. Rosinski, 1 Mood C.C. 12). So, where a medical man had connection with a girl fourteen years of age, under the pretence that he was thereby treating her medically for the complaint for which he was attending her, she making no resistance solely from the bona fide belief that such was the case, this was held to be certainly an assault, and probably a rape (R. v. Case, 1 Den. 580; 19 L.J. [M.C.] 174). Such an act is now held to constitute a rape.
Battery.—This includes beating or wounding. A touch of the finger, however slight, is included under this term.
Homicide.—In Scotch law homicide is held to be committed only where a distinctly self-existent human life has been destroyed. Destruction of an unborn child, however short a time before delivery, may be criminal, but is not homicidal. In the same country criminal homicide is divided into two classes:
1. Murder is constituted in law by any wilful act causing the destruction of human life, whether plainly intended to kill, or displaying such utter and wicked recklessness as to imply a disposition depraved enough to be wholly regardless of the consequences. Murder may be the result of personal violence, poison, or by the committal of some other serious crime, as where anyone causes the death of a woman in the attempt to procure criminal abortion, rape, or by the exposure of an infant which results in its death. The use of weapons is not essential.
2. Culpable Homicide.—The name applied in law to cases where the death of a person is caused or materially accelerated by improper conduct of another, and where the guilt does not come up to the crime of murder:
(a) Intentional killing of another in circumstances implying neither murder on the one hand, nor justifiable homicide on the other—e.g. if a person exceed moderation in retaliation for an injury, or kill another when the danger to which he was exposed is passed.
Every charge of murder is held to conclude a charge of culpable homicide, and the jury, if they see cause, may find that culpable homicide only has been committed.
(b) Homicide, by the doing of any unlawful, or any rash and careless act, from which death results, though not foreseen as probable—e.g. using firearms in a public street, &c.
(c) Homicide, resulting from negligence or rashness in the performance of a lawful duty—e.g. a signalman on a railway forgetting to alter the points, and thus causing a collision, and loss of life. In England this would amount to manslaughter.
[Pg 69] Justifiable Homicide.—Self-defence; hanging a prisoner properly sentenced to death; killing another to prevent murder, if prevention can avail in no other way. In self-defence, the person killing must be in reasonable dread of death at the hand of his adversary.
In England there is—1. Murder; 2. Manslaughter; 3. Justifiable Homicide.
Murder, according to Lord Coke (3 Inst. 47), is constituted “where a person of sound memory and discretion unlawfully killeth any reasonable creature in being, and under the King‘s peace, with malice aforethought, either expressed or implied.”
In England the killing must be committed with malice aforethought. Malice may be expressed or implied.
In Scotland malice aforethought is not necessary (5 Irv. 525, and 40 S.J. 92, and 5 S.L.R. 20).
The law in both countries appears to differ more in terms than in practice. In England, if an injured party live for one year and a day, and then die, death is not attributed to the injury; but in Scotland, although no definite time is fixed, yet no case would I believe be entertained at any lengthened period after the commission of a homicidal act. The longest interval, according to Taylor, at which conviction has taken place from indirectly fatal consequences was nine months.
In the United States, as a rule, the crime of murder admits of two degrees: in the first, where the act is intentional or is the result of an attempt at burglary, rape, arson, or by poison; otherwise the crime falls under the second degree.
Legal Definition.—According to the statute (24 and 25 Vict. c. 100, sec. 18), the word “wound” includes incised, punctured, lacerated, contused, and gunshot wounds. But to constitute a wound within the meaning of the statute, the whole skin, not the mere cuticle, or upper skin, must be divided (R. v. M‘Laughlin, 8 C. & P. 635). But a division of the internal skin, e.g. within the cheek or lip, is sufficient to constitute a wound within the statute (R. v. Warman, 1 Den. C.C. 183). If the skin be broken, the nature of the instrument with which the injury is inflicted is immaterial, for the present statute extends to wounding, &c., “by any means whatsoever.” A wound from a kick with a boot is within the statute (R. v. Briggs, 1 Mood C.C. 318). Injuries, burns, and scalds—which, in accordance with the above definition of a [Pg 70] wound, are not wounds—are provided for under the clause, “or cause any grievous bodily harm to any person.”
Casper defines “an injury” to be “every alteration of the structure or function of any part of the body produced by any external cause.” Taylor proposed the following as the best definition which can be given to the word “wound,” whether in a medical or legal sense, viz. that it is “a breach of continuity in the structures of the body, whether external or internal, suddenly occasioned by mechanical violence.” This would include dislocations, fractures, either simple or compound, injury to the skin or mucous membrane, and to internal organs. Burns and injuries due to the action of corrosives are excluded from the category of wounds.
Concerning Wounds in general.—Great care must be taken to ascertain the exact site and course of the injury on the body, as this precaution will greatly assist in answering the questions: Is the wound dangerous to life? Does it cause grievous bodily harm? Is it suicidal, that is, inflicted by the person on himself; or homicidal, inflicted by another? The solution of the question of the dangerous character of the wound is left to the professional knowledge of the witness, who may be required to state his reasons for considering the wound dangerous to life. His mere assertion will not be accepted. “The safest course,” says Elwell, “for the witness, in regard to all these questions, is to give a true and plain account of the wound, describing it minutely, and the probable consequences that may attend it.” In relation to their danger to life (apart from so-called “simple” wounds which are not usually extensive, heal easily, and cause little trouble in their course), wounds may be considered dangerous to life when they are so extensive, or on account of their position and relation to important structures when they would prove fatal without the intervention of surgical skill; and when the danger is imminent. A mortal wound is one which is rapidly followed by death. Wounds, however, which in themselves could not be regarded as dangerous to life, may become so by intercurrent complications, such as erysipelas or other infective process. As a general rule, only those wounds in which the danger to life is imminent should be stated as dangerous to life. Compound fracture of the bones of the cranium, injury to any large arterial trunk, or to any of the internal organs, may be considered as “dangerous to life”; but where the danger is more remote, as in the probable supervention of tetanus, erysipelas, &c., the medical opinion must be more guarded. But the medical witness should always bear in mind that death may follow the slightest injury. A case is recorded of death in forty-eight hours after extraction of a tooth. The contrary also holds good, for the most fearful injuries have been followed with recovery.
The following suggestions may help the practitioner in the formation of his opinion as to the probable danger of a wound: [Pg 71]
1. The extent of the injury. 2. The character of the instrument used in the infliction of the wound. 3. The violence suffered by the parts. 4. The size and importance of the blood-vessels and nerves injured. 5. Is the wound healing or likely to heal well, and is the constitutional disturbance severe or slight? 6. Age of the sufferer. 7. Is there any constitutional taint likely to render even a slight wound more severe, or even dangerous to life? 8. Has the previous medical treatment been skilful or otherwise?
Should the injured party be found dead, a careful post-mortem examination will alone determine the probable part the injury bore in the production of the fatal result.
Points of Importance to be Noticed
in Examination of a Dead Body
found Wounded.
1. Note situation, extent, depth, breadth, length, and direction of wound. Take careful measurements, in order to determine the character of the weapon, and the organs of the body injured.
2. Is there any appearance of ecchymosis, or is the effused blood liquid or coagulated?
3. Examine wound as to presence of pus, adhesive inflammation, gangrene, or foreign bodies.
Why? Presence of pus, &c., will show that death must have taken place some time after the wound was inflicted.
4. In all examinations of wounds, be careful to disturb as little as possible their outward appearance, in order to compare the wound with the suspected weapon.
5. All notes should be taken during such examination, or immediately after.
6. Make a careful examination of all the important organs of the body.
Why? In order to disprove the suggestion that death was due to other causes—poison, disease, &c. This is important, as in the case of a girl who, dreading a whipping, swallowed some arsenic, from which she died, yet her father was tried for causing her death by the severity of his punishment.
7. Only facts should be stated in the Report; no inferences should be drawn or suggested.
8. In describing the appearance of wounds use simple untechnical language, and avoid superlatives and high-flown words to describe and explain simple facts.
9. In gunshot wounds, note position of body, state and contents of the hands, and the direction of the wound in relation to external objects.
Note also in all kinds of wounds the relationship of the wound to cuts or rents in the clothes of the deceased.
These may be either external, affecting the integuments; or internal, affecting the brain substance, &c. In the latter, as a rule, there are signs of external violence. An ecchymosed tumour of the scalp may impart a sensation of crepitation to the finger, and may thus be mistaken for a fracture of the skull. The tumour may also [Pg 72] pulsate if any large vessel be near it, giving one the idea that the pulsations are due to the movements of the brain. A large wound without fracture points to a more or less oblique blow, a small wound to direct violence. A blow with a heavy blunt weapon may make a clean incised wound, and often in these cases the seat of the bruise does not correspond with the centre of the cut. Dr. Ogston mentions the case of a young lady on whom a cricket ball inflicted a wound across the forehead, immediately above, and of the length of, one of the eyebrows, which he could not distinguish from a wound by a cutting instrument. All injuries to the head are more or less severe and dangerous, and great care is required in forming a prognosis with regard to the ultimate effect of an injury to the head. Inflammation of the brain does not, as a rule, supervene for about a week after the accident, and patients should not be considered safe from danger till two or three weeks after. Be it remembered also that in some cases the inflammatory action may proceed insidiously for some months without giving any distinct evidence of its presence till close upon a fatal termination. Scalp wounds are dangerous, from erysipelas, &c. They should be examined as to their extent, form, depth, and position.
Concussion of the brain may arise from falls on the nates, or from blows on the head. The face becomes pale, the pupils contracted, the pulse weak and small, the extremities cold, the respiration scarcely perceptible, and the sphincters relaxed. The tendency to death is from syncope. Reaction may then occur: the pulse quickens; the skin is hot and dry; there is great confusion of thought, from which the patient ultimately recovers; vomiting is present in most cases. Concussion often passes into compression, due to hæmorrhage from the lacerated cerebral vessels. Concussion and compression differ in this: in the former, the effects are instantaneous; in the latter, a short time elapses before the symptoms make their appearance; and these become more and more marked, whereas in concussion they gradually pass off. It is often a difficult matter to distinguish the effects of compression from those common to drunkenness or narcotic poisoning. The odour of the breath and the history of the case will assist in forming an opinion. Concussion of the brain may prove fatal without either fracture of the skull, effusion of blood within the cranium, or any other change being observed on dissection, death being caused by the shock given to the whole nervous organ, which, being unrelieved, speedily lapses into annihilation of function.
The symptoms of compression—a full, strong, and often irregular or slow pulse; normal heat of surface; muscular relaxation; dilatation, contraction, or inequality of the pupils; stertorous breathing, and paralysis—are not unfrequently retarded, and this consideration should render the opinion very guarded. Bryant records a case (Surgery, vol. i. p. 216) in which a man was thrown out of a gig on to his head. After a short period of insensibility he walked for half an hour, and then gradually again became insensible, and ultimately died. A large clot was found over the left cerebral hemisphere, the blood evidently [Pg 73] having flowed from the middle meningeal artery. The short period of insensibility probably arrested the flow of blood from the artery, which recurred on the sufferer walking. The structural form of the cranium may have much to do with the danger to be expected from blows—some skulls being thinner than others—and in a few rare instances the fontanelles may not have become ossified during life.
The possibility of an unhealthy condition—atheroma—of the arteries of the brain, or of disease of the heart, must be taken into consideration before venturing an opinion as to the tendency or ultimate cause of death.
It may be stated that the patient died of apoplexy. Apoplexy is a disease of old age, and seldom occurs in the young, although it is just possible it might occur. The arteries should, in every case, be examined for the presence or absence of disease. When violence is used, the effusion of blood is, as a general rule, on the surface of the brain; but two cases are given by Dr. Abercrombie of spontaneous bursting of a blood-vessel within the head, followed by effusion of blood upon the surface of the brain. “An external injury, coexisting with an extravasation of blood into the cerebral substance, does not necessarily imply cause and effect. The previous condition of the brain, or the outpouring of blood from diseased vessels, may, in fact, have been the cause of the accident” (Hewett). When, however, blood is found effused on the surface of the brain, especially between the dura mater and the skull, either beneath or opposite to an external wound, we may reasonably infer that the hæmorrhage is due to a direct blow. Hæmorrhage so severe as to produce dangerous pressure on the brain, as a rule, comes from a rupture of the middle meningeal artery.
Husband relates a case in the Edinburgh Infirmary in which there was a large clot over the left frontal lobes, accompanied with aphasia and right hemiplegia, with no rupture of the middle meningeal artery, or any signs of external injury. The man had just left the cells on a charge of drunkenness. The source of the hæmorrhage was not clearly made out, but it seemed to be due to the rupture of an artery in a pachy-meningitic patch. Blood may be found in the cavity of the arachnoid in the great majority of severe injuries to the head, and even in trifling cases where least expected. Rupture of the venous sinuses may take place without fracture of the skull. I have met with this in a fatality during a boxing match; a large effusion over the brain, and especially in the temperosphenoidal fossa, taking place from rupture of the left lateral sinus at the junction with the superior petrosal; there was also a vertical hæmorrhage into the pons. The effused blood may, after a time, become changed, and form a false membrane on the parietal arachnoid, seldom on the visceral surface. Blood cysts may even be formed, in the course of time, having all the appearances of a serous membrane. The blood may spread to parts remote from the seat of injury, and the extravasation does not always occur at the exact spot of the application of the blow, but often at a spot directly opposite. Two extravasations may be the result of one blow. [Pg 74]
Fits of passion have been advanced as a cause of apoplexy, but this cause is rare. Fracture of the cranial bones may be due to counter-stroke—contre-coup—or to falls on the nates, &c. Fractures of the skull are divided into two groups (Körber): (1) those produced by bilateral compression of the skull; and (2) those resulting from violence applied to one side only. In both groups the line of fracture runs parallel with the axis of compression. Fissures of the base from bilateral compression of the skull are always transverse. Punctured wounds of the cranium are always dangerous, but the patient may survive many days. Dr. Bigelow, Professor of Surgery in Harvard University, U.S.A., relates a case in which an iron bar, weighing thirteen and a quarter pounds, three feet seven inches in length, and one inch thick, was driven through the head, followed by recovery, the patient only losing the use of the injured eye.
Contusion and laceration of the brain may occur from injuries to the head, either at the seat of injury or by contre-coup at some other part. The contused area may exhibit local extravasation of blood, or in the diffuse form, extravasations may be multiple and also on the surface. The symptoms are those of cerebral irritation, coma, or restlessness, paralysis, tonic or clonic spasms. In slight cases recovery may follow, in others some degree of loss of mentality and paralysis may remain.
There is great danger of inflammatory complications. I have met with a case of severe comminuted fracture of the skull with laceration of the brain, the latter substance appearing on the surface of the scalp, with loss of brain substance, in a boy who made a complete recovery without any loss of intelligence or power following the injury.
For the detection of brain substance on weapons the microscope is alone reliable, and then only the cellular portion of the brain is of any use.
Injuries to the spinal cord may cause immediate death; cases, however, occur of life being prolonged for some days, or even longer, after injury to the cord. The symptoms are progressive paraplegia and paralysis of the bladder and rectum, ending in death. Bedsores and septic infection of the bladder and kidneys are complications which add to the gravity of the condition. Spicula of bone in the cord, dislocation of the vertebræ, or extravasation of blood in the membranes of the cord, may be found after death. The presence of blood upon the spinal cord is not necessarily the result of violence, as hæmorrhage may take place spontaneously. The spine should be examined in all fatal cases of supposed injury. Concussion of the spinal cord is a fertile source of differences of opinion in railway cases. In no case should a hasty decision be given as to the probable future result to the patient from the injury.
Wounds of the face are not generally dangerous, unless they penetrate the brain. There is always the possibility of injury to the eye causing detachment of the retina, or inflammation leading to blindness. Punctured wounds in the neighbourhood of the orbit may become septic and lead to secondary meningitis. [Pg 75]
Wounds of the throat are more or less dangerous, due to the possibility of severe hæmorrhage, emphysema, and bronchitis.
Wounds of the chest are dangerous, on account of the amount of the hæmorrhage which may take place, and the importance of the organs which may be injured. Death may result more from the mechanical action of the blood effused than from the depressing effect of the quantity evacuated. Penetrating wounds of the thorax injuring the lungs cause emphysema, pneumo-, pyo-, or hæmothorax, any of which may prove fatal; pleurisy and pneumonia may occur. A fracture of the ribs may give rise to injury of the lung substance or to inflammation of its coverings. Laceration of the lungs may take place without fracture of the ribs. The ventricles of the heart may be pierced, and yet life may be prolonged for one or two months, permitting of considerable locomotion during that period (Briand et Chaudé, Med. Leg., vol. i. p. 511). Wounds of the heart, however, are, as a rule, rapidly fatal. Rupture of valves may follow blows on the chest, and rupture of the heart may occur from crushes or violent blows. Rupture of the heart has taken place during violent exertion, and this is more likely to occur when the muscle is diseased. It is often difficult to make out the direction of the wound, as the lungs change their position during respiration.
Wounds of the abdomen, penetrating the intestines, although not necessarily fatal, may cause death from peritonitis, due to the escape of the intestinal fluids. Rupture of the intestine may follow blows or crushing; it is generally fatal from peritonitis unless early surgical treatment is carried out. Hernia may also follow wounds of the abdomen. Rupture of the liver is not of infrequent occurrence, and may occur without any external signs of the injury. The rupture is, as a rule, longitudinal, transverse lacerations being rare. It is often followed by pneumonia if not rapidly fatal. The cœliac plexus may be much damaged by a blow or kick on the stomach, especially if this organ be distended with food, and death may result without leaving any trace of the injury externally or internally. The bladder may be ruptured and death result from extravasated urine. Rupture of the bladder may occur from fracture of the pelvis without sign of external injury. Rupture of the kidney may be recovered from if slight, but when severe is fatal. Rupture of the spleen is usually fatal, and is more likely to occur when enlarged from any cause. Coagulable lymph, the effect of a wound of a serous membrane, may be thrown out in twelve hours or less.
Injuries to the abdomen may cause death by— [Pg 76]
1. Shock; without lesion of the internal organs, inflammation, or external signs of injury.
2. Hæmorrhage.
3. Lesion of the internal organs, but without inflammation. Death in these cases seems to be due to depression of the nervous system due to the intense pain following these injuries.
4. By inflammation without lesion of internal organs.
5. Inflammation from lesion of internal organs.
6. Destruction of the natural functions of the organs, and, as a result, malnutrition of the body.
Except in the first case, when death is instantaneous, wounds of the abdomen are not as a rule immediately fatal.
Wounds of the genital organs of the female may cause fatal hæmorrhage, which takes place from the plexus of veins which, in these parts, are devoid of valves. A kick from behind whilst the woman is stooping or kneeling may rupture the labial vessels and death supervene.
Blows and kicks upon the abdomen do not often injure the non-gravid uterus, but during gestation may produce abortion and hæmorrhage. If the pregnancy be advanced the uterus may be ruptured or the placenta separated. Penetrating wounds either through the abdominal wall, or per vaginam in the attempt to procure abortion, cause hæmorrhage and peritonitis with septic infection.
Unless they implicate some special structure, such as the brain and medulla, simple fractures are not considered dangerous to life. When compound, they may be complicated with hæmorrhage and infective processes.
Certain pathological conditions favour the spontaneous fracture of bones, or this occurrence with such slight violence as would not cause fracture in the normal may take place.
In old people bones are more liable to fracture from their brittle condition. Liability to easy fracture occurs in the insane, in nervous lesions as locomotor ataxia and general paralysis of the insane, when the bones are the seat of new growths, in fragillitas ossium, osteopsathyrosis; in the latter disease I have seen the femur fracture by the weight of the leg while resting the foot on a cushion. The liability to fracture depends upon the proportion of organic and inorganic constituents. In disease, the latter may be reduced and predispose to fracture; in the young, the bones are more liable to greenstick or incomplete fracture; and in the old, from excess of inorganic constituents causing brittleness.
A medical man may be required to express an opinion as to whether or not fractures are the result of direct violence, and especially when allegations have been made against attendants on the senile or insane.
The previous predisposing pathological conditions must always be taken into account, and also the amount, if any, of repair that has followed in relation to the time the alleged violence took place.
As the condition of a fracture of the bone of a limb may become a question of considerable importance in medico-legal investigations, the [Pg 77] following brief account of the process of repair in fractures is given:
From the First to the Third Day.—The period of inflammation and exudation. Ordinary signs of inflammation and laceration of the parts. Blood will be found extravasated round the fracture, also in the medullary canal mixed up with the fat.
From the Third to the Fourteenth Day.—Gradual subsidence of inflammatory action and growth of the soft provisional callus from the periosteum and surrounding structures, and internally in the medulla, forming a fusiform mass holding the broken ends of the bones together with some degree of firmness. This becomes firmer and almost cartilaginous in density. When the bones are kept immovable, or are impacted, the provisional callus may not be formed. In the case of the ribs the provisional callus is always formed, and Dupuytren‘s “ring of provisional callus” is constant. This may also occur in fractures of the clavicle.
From the Fourteenth Day to the Fifth Week.—Ossification of the provisional callus. The bone is first soft and spongy till the conversion of the soft callus is complete.
From the Fifth Week to some Months after the Injury.—Complete bony union of the fracture and absorption of the provisional callus.
Although the blood clot completely disappears from the immediate neighbourhood of the fracture at an early period, yet layers of dark coagulum may often be found beneath the superficial fascia for four weeks or more after the accident (Erichsen).
It may be of importance to remember this in medico-legal inquiries. The presence or absence of the signs of vital reaction will help to distinguish fractures caused before or after death.
A fracture taking place immediately after death cannot be distinguished from one immediately before death, but if a few hours after death, the differences are easily recognised, blood is not effused round the ends of the bones unless a large vessel be torn.
In the examination of bones for fracture in the living it is the duty of the examiner to have an X-ray plate taken of the injured bone, especially if the seat of injury is in close vicinity to a joint.
Previous fractures are easily recognisable after death even when the bone does not show manifestations externally; on longitudinal section the seat of fracture is rendered evident.
An attempt is made to answer this question by a consideration of the wounds in reference to their position, nature, extent, and direction.
In reference to their position it has to be borne in mind that one person may wound any part of the body of another, but that to the suicide certain parts only are accessible, and they have a predilection for wounding themselves in favoured regions; the front of the body and vital parts are chosen by the suicide, while wounds on the back point to homicide. Suicidal wounds on the head are generally in front or lateral, and on the neck in front or to one side, in cutting the throat. Accidental head injuries are more often on the vertex, and when [Pg 78] there may be no history of a fall on the occiput, wounds in this situation indicate homicide.
Suicides may choose unusual regions, such as cutting of a large vessel as the femoral artery in Scarpa‘s triangle, or by a limited incision, the carotid in the neck, the injury may be about the genitals, and the penis and scrotum have been amputated.
Accidental injuries may occur on any part of the body, but most commonly on exposed parts.
The nature and extent of the wounds does not afford much assistance; with the exception of contused wounds which are usually homicidal or accidental, any other form of wound, particularly incised or punctured wounds, may be suicidal or homicidal, and with regard to gunshot wounds, much depends upon their position and extent. As a rule, the suicide does not make several wounds, and the homicide may not only inflict several but of a greater severity than are necessary to carry out his purpose.
Suicides, especially when insane, may wound themselves severely and cause great injuries by leaping from buildings or similar high positions. In some cases suicides have inflicted several and varied wounds on their bodies.
The direction of suicidal wounds, when the person is right-handed, is generally from above downwards and inwards on the chest, and on the left side. An upward direction points rather to homicide.
Cut throat wounds, when suicidal and inflicted by the right hand, are generally oblique from left to right, beginning higher up than they end. They generally cross the thyroid cartilage, and the larger vessels may escape; if made below the thyroid cartilage they are generally smaller and horizontal. The skin is the last structure divided, and there may be several so-called “tentative cuts.” It has been held that when the large vessels are cut the suicide stops, but this is incorrect, as in some cases the wound has reached the spine and the vessels been quite severed. Suicides may try to decapitate themselves from behind, and failing this stab themselves. A homicidal cut throat wound, when made from the front with the right hand, commences on the right side and is carried to the left; they are often deep incisions to the vertebræ and the tissues “undercut” at the ends. A homicidal cut throat wound when made from behind the victim resembles a suicidal one. When wounds are present on the forearms, hands, and fingers, and if there are injuries on other parts of the body also, the inference would be that the hand wounds were received in guarding the throat or other efforts at defence from a homicidal attack.
Wounds produced by Firearms.—To distinguish between suicidal, homicidal, and accidental wounds is far from easy. If the weapon be held hard up or close to the body, as in suicide, the skin and hair would be scorched and blackened, as would probably the hand that held the weapon, but this has not occurred in every case. The grasping of the firearm by the hand in cadaveric spasm is certain evidence of suicide, as this cannot be simulated by an assailant placing the weapon [Pg 79] in the hand after death. Full investigation should be made by noting the bullet track and surrounding objects which may have been grazed in its course, in order to form a probable estimate of the direction from whence it came. Bullet wounds in the back are usually homicidal.
The surgeon should at once visit the wounded party, and proceed to examine the injury, for if this be done before swelling occurs, he will be better able to form an opinion of its nature, extent, and severity. If the wound has been dressed, he should, if possible, obtain the attendance of the person who applied the dressings, and who would be able to describe their nature, and the dangers to be avoided in their removal, should that be deemed necessary. In no case should a surgeon remove the dressings applied by a professional brother without his presence and assistance. The condition of the injured party should be carefully noted, and a minute description of the wound written down at the time. The statements of the bystanders are also useful and should be noted. The procedure in the examination of the dead body has been previously described (p. 60).
An important question here arises. Have the wounds found on the body been produced during life or after death? The answer is beset with difficulties, and considerable caution will be necessary, but tables will be given under the different kinds of wounds to assist the diagnosis. Signs of vital reaction are important, as showing the ante-mortem infliction of the wound; but these may, to some extent, be removed by the action of water, as in cases where the body is found in a pond. Under these circumstances the evident signs of drowning—water in the stomach, &c.—will assist the diagnosis. The presence of putrefaction also greatly obscures the diagnosis. The presence of coagulated blood between the edges of the wound is not a trustworthy indication of the ante-mortem infliction of the wound, as experiment has shown that as long as the body remains warm coagulation may take place. Coagulation even in contused wounds, effected before death, may be retarded from various unknown causes—disease, e.g. scurvy; mode of death, e.g. asphyxia. The amount of hæmorrhage on or around the body is, other things being equal, a safe criterion as to the time when the wound was inflicted; if in considerable amount, arterial blood points to ante-mortem injury; the presence of venous points blood to post-mortem injury.
Care should be taken to record and photograph the body in position where found, and its relation to surrounding objects. Careful note should be made of the surroundings and the character and presence of any blood-stains, footprints, &c. The question may have to be considered as to whether the body is in the place it was when the wounds were inflicted. Blood in any quantity in one place, and the body [Pg 80] found in another so seriously injured that locomotion would be impossible, point to the body having been removed.
Signs of a struggle, if any, should be recorded. If a weapon be found near to the body, its position should be noted, and if in the hand, the firmness of the grasp—cadaveric spasm—should be recorded. All clothing should be carefully examined, and the relation of cuts and body wounds noted. All blood-stains on the clothing should be examined and described.
Multiple bullet wounds denote homicide, but suicides have been known to inflict more than one wound. It is strong evidence of suicide if the gun or pistol has burst by the explosion, as suicides have a predilection for overloading the weapon employed.
How may wounds, alleged to have been the result of an assault, be shown to have been self-inflicted? This has to be done by considering:
(1) The character of the wounds: in these cases they are generally slight, and may consist in a series of small, superficial wounds.
(2) The parts of the body where they are, and those from which they are absent. They are never found on vital parts, but always where there is little danger of doing harm. They are present on parts accessible to the individual. The hands are seldom wounded, and if they be, not severely.
(3) The clothing may not be cut, and if it be, the cuts may not go right through, and if they do, they may not coincide with the position of the wounds. The person should be clothed in order to determine this. Blood-stains on the cuts in the clothing may be erratic in distribution, some being on the inner layer only, some on the outer, and rarely soaking through all, pointing to the probability of its having been artificially applied.
Such self-inflicted wounds are usually produced for the purpose of bringing a fictitious charge of assault, feigning self-defence or provocation on the part of the assailant when accused; and in order to divert suspicion, as in the case of a person who alleges he has received the injuries by an assailant who was committing robbery while he himself is guilty of it.
Wounds may prove fatal from results which are (1) directly due to injury—hæmorrhage, shock, or mechanical injury to some vital organ, e.g. the heart or lung; or (2) indirectly from complications which may supervene such as infective processes—erysipelas, tetanus, septic infections, gangrene,—exhaustion, or the effects of surgical operations; or (3) malum regimen (a) on the part of the patient, (b) on the part of the medical attendant. [Pg 81]
Hæmorrhage.—Hæmorrhage may be profuse and cause rapid death if a large blood-vessel, more especially an artery, has been injured. The hæmorrhage may take place internally, in which case it need not necessarily be profuse; it will depend upon the position; a small hæmorrhage into the pericardium or in the brain may prove rapidly fatal.
Shock.—Death from shock is generally associated with severe injury, either a single one, or from several smaller injuries, any of which alone would not be expected to prove fatal. Death may occur from shock when the visible injury may be slight, as in blows over the heart and abdomen, the latter causing fatal syncope from dilatation of the splanchnic vessels. Repeated lesser injuries as in flogging may cause death through shock; and fatal psychical shock may be caused by mental excitement, as, for instance, in an encounter when no physical injuries have been received.
Mechanical Injury to Viscera.—This causes rapid death, more especially when the viscus injured, as the heart or medulla, is necessary for the immediate functions of life; injuries to other organs may not be followed by immediate death unless very severe and with great shock. A wound of the lung may not be followed by death for some time.
In a healthy person the violence necessary to prove fatal ought to be greater than in one diseased, and pathological conditions may be found post-mortem, which were pre-existent to the injury, e.g. degeneration of blood-vessels, aneurysm, valvular disease of the heart, phthisical cavities which may have bled, gastric ulcer which may have ruptured. Such conditions might influence the findings of a jury, as, for example, it is not always possible to form the opinion that death has been directly due to violence when signs of injury are slight; a man may receive a blow on the head while in the act of falling in a fight, and post-mortem a cerebral hæmorrhage be found with diseased vessels, when it would be difficult to say with certainty that the hæmorrhage was directly caused by the blow or preceded it.
Fatal Complications.—In English law if death follow injury inflicted by a person within a year and a day, the assailant may be tried and punished; beyond that time the person is not held responsible for the death. The infective processes mentioned above may supervene at any time during the course of wounds with fatal result. Further, as a result of altered conditions left by injuries which in themselves have not proved fatal, and from the immediate effects of which the person has recovered, fatal complications may follow, e.g. a person may have received an abdominal wound which after healing may become the seat of hernia which may strangulate; or an injury to the spinal cord, which may cause death at a late date from bedsores and exhaustion.
Septic Processes.—These may cause death at an early date according to their nature and virulence and the power [Pg 82] of resistance of the person. In such cases the original injury need not have been dangerous to life. In other cases the infection may persist after the wound has healed, as infective endocarditis might conceivably do.
Surgical Operations.—Should a surgical operation be considered necessary for the treatment of the injury or in order to save life, and the person dies after it, the prisoner will be held responsible for the death. This holds good if the operation has been done in good faith and performed with reasonable skill and care. If, however, it can be shown that the operation was unnecessary, or performed unskilfully and death resulted, the prisoner would not be held responsible unless it can be proved that the injury apart from the operation could have caused death, when the jury might convict.
Where from improper treatment of an injury an operation is called for because of the improper treatment and the person dies, the prisoner would not be held responsible. The main points to be considered in reference to surgical operations for criminal injuries are:
(a) On the part of the Person Injured.—If the wound is not in itself sufficient to cause death, but by negligence in the care of it by the injured person, complications arise which cause death, then the punishment would probably be mitigated; but in law a person accused of criminally injuring another is held responsible for the immediate and remote results. “No man is authorised to place another in such a predicament as to make the preservation of his life depend merely on his own prudence.” If, however, it can be proved that death was largely due to the imprudence or recklessness of the deceased, it is probable that this would lessen the punishment.
(b) On the part of the Doctor.—A person accused of criminally injuring another being held responsible for the results immediate and remote, may plead that the latter, i.e. complications, or the death itself are not due to the injury directly, and endeavour to throw the responsibility on someone else, either the injured person through negligence, or on the doctor for unskilful treatment. In reference to the complications, the medical witness may be asked for his opinion as to the cause and effect of the complication, and how it might have been avoided. Having considered all the facts laid before him and made his deductions, he must give his opinion fairly, and leave it to the Court to decide in what way his opinion may influence its judgment and the amount of punishment for the offence.
When there is an allegation that the treatment has been unskilful or negligent, and contributory to complications and death, and a defence [Pg 83] raised accordingly, the prisoner has to prove this to the satisfaction of the Court in order to mitigate the offence and punishment. The medical man is expected to have exercised reasonable skill. If the person treating the injury is a registered medical practitioner, and has applied his treatment in good faith and for cure, even if the treatment were improper, the assailant would be held responsible.
The care which the medical man ought to exercise is that which everyone ought to exercise who has received the statutory education and passed the statutory examinations.
(1) Incised; (2) Punctured; (3) Lacerated and Contused; and (4) Gunshot.
Made by sharp instruments.
General Characters.—Incised wounds are somewhat spindle-shaped, their superficial extent being greater than their depth; the edges are smooth and slightly everted, and the wounds are always larger than the weapon which inflicted them—due to retraction of the divided tissues. If a wound be in a line with the fibres of a muscle, there will be less “gaping” than when the wound is directly or obliquely across the muscle. From muscular contraction, or the elasticity of the skin, an incised wound may assume a crescentic form. The cellular tissue is infiltrated with blood, and coagula are found at the bottom and between the edges of the cut. It must be borne in mind that a wound with smooth edges may be made by a blunt weapon over bones near the surface, as on the scalp and over the tibia or shin, but a certain amount of contusion may, in most cases, be detected by careful inspection a short time after the receipt of the injury.
It is often of importance to distinguish where the weapon entered, and where it was drawn out. The end where the weapon entered is usually more abrupt than the other, which is naturally more drawn out. But in some cases I have seen, when the weapon was simply drawn across the part, both ends of the wound alike.
The orifice is generally a little smaller than the weapon.
A stab may sometimes present the appearance of an incised wound; the depth will, however, help to distinguish the one from the other. The wound may not at all correspond with the shape of the weapon, and the same pointed instrument may produce very different-shaped wounds in different parts of the body. Much depends upon the movement of the instrument in the action of puncturing; in the case of a double-edged instrument the wound will most probably be fusiform or diamond-shaped. When made with a knife the wound may be wedge-shaped if the knife have a thick back. A circular weapon splits the skin and leaves a slit; broken glass and pottery act in a similar way, but the wounds may have [Pg 84] jagged edges and show signs of contusion in them. On dissection, two or more punctures may be found in the soft parts, with only one external orifice; these are due to the weapon being only partially withdrawn at each stab. Punctured wounds are always more dangerous than incised. They cause little, if any, hæmorrhage externally, unless a large vessel, such as the femoral artery, be injured, but they may cause internal hæmorrhage or penetrate a viscus, e.g. the lung or heart. These wounds generally heal by suppuration, and not infrequently an abscess is formed in and around the track of the wound. Perforating wounds generally have a large entrance wound with inverted edges, and a small exit with everted edges; if the weapon be rough, the reverse may be the case.
The edges of these wounds are never smooth, and generally do not correspond at all with the weapon. A considerable amount of contusion or bruising surrounds the solution of continuity of the part. Hæmorrhage from these wounds is usually slight. A point of considerable interest may arise in connection with this class of wounds; the defence may declare that the injury was the result of a fall, and not due to a blow. The history of the case, and the presence of a bruise where no theory of a fall can explain its existence, will often afford the only solution of the difficulty. Lacerated wounds heal by suppuration, generally with more or less sloughing, and leave a permanent scar. Scratches with the finger-nails may be considered as lacerated wounds, but the skin is merely abraded, not divided. They are never important as wounds, but often as a proof of a struggle in cases of rape, &e. Bites are also lacerated wounds. The diagnosis of lacerated and punctured wounds, whether inflicted before or after death, will depend on much the same grounds as those of incised wounds, hæmorrhage, vital reaction, &c.
Table of Differentiation Between
Ante-mortem and Post-mortem Wounds:
The appearance which gunshot wounds present will to a great extent depend upon the form of the projectile, and the distance at which the firearm was discharged. Round halls make a larger opening than conical. Small-shot, fired within a short distance of the body, make one large ragged opening. The scattering of the shot depends on the calibre of the gun, on the charge of powder, and essentially on the distance. A charge of ordinary (No. 5) shot, to make a single hole, must have been fired at less than one foot; but experiments should always be made with the alleged weapon. A patent cartridge would make a single hole at a considerable distance—five or six yards. Round bullets may split, but the conical ones seldom do. The edges of wounds produced by the discharge of firearms are always more or less ecchymosed; this condition appears in about an hour after the infliction of the injury. If the ball strikes obliquely, the edges of the wound may be much lacerated, or the opening may be valvular and of small size, if the skin over the part be in any way tightened, or if a conical ball has been used. The injury to bones is greater from conical than from round balls. The old round balls were easily deflected; the conical are not [Pg 86] so easily turned aside. The track of the ball widens as it deepens. This is the reverse of an ordinary punctured wound. The ball may either lodge in a part, or perforate it. Should it have lodged, it must be preserved and compared with the alleged firearm. Bits of clothing or wadding may be carried into the wound. The latter should be carefully kept, as they may prove important as a means of identification.
The aperture of entrance and exit must, if possible, be determined. On this point there is much difference of opinion. The wound of exit is always smaller than the wound of entrance (Casper). In this opinion Casper agrees with M. Malle, Olliver d‘Angers, and M. Huguier, but is opposed by Taylor, M. Matthysens, and others. “The characters of a gunshot wound,” says Assistant-Surgeon Neill, “are those of a contusion and laceration of all the tissues. Sometimes they are so simple as to bear resemblance to a punctured wound, particularly if a rifle-ball (conoidal), revolving on its long axis, has passed through the soft parts at a great speed, but within a few hours it resembles a contusion. The wound of entrance, as it has been termed, bears no comparison in size or shape to that of the exit when a rifle-ball has caused the injury. In the former you see the edges of the wound curving inwards, and the circumference small, with little or no hæmorrhage. In the latter, the wound is large, with torn and irregular edges projecting outwards, and perhaps only slight oozing of blood. In a short time, averaging an hour, round the entrance wound slight redness begins, gradually extending to about two inches round its orifice. Again, this colour changes to a blue- or greenish-black, and you see all the appearances of a severe bruise, with a small wound of the skin, its edges still curved inwards. In the exit wound the discoloration of the skin is not apparent.” The probable reason for the discrepancies in the statements of observers, as to the characters of entrance and exit wounds, may be found in the fact that experiments have been conducted with different-sized balls, different kinds of weapons, with varying quantities and qualities of the powder used, the character of the wads, and with varying velocities and distances. As pointed out by M. Roux, the two openings may be equal if the ball preserves the same velocity through the tissues as it possessed before entrance; the entrance hole is smaller than the exit, when the ball has lost much of its trajectile force, and enters the softer parts of the body first; the entrance is larger than the exit, when the ball first enters through the denser tissues of the body, and leaves through the softer.
The opening of entrance made by the ball has generally, but by no means always, inverted edges. The edges of the exit opening are everted, bloody, and raw; but both the entrance and exit wounds may be everted in fat persons, due to the protrusion of the fat; and this eversion may also result from the expansive power of the gases generated during putrefaction, should this condition be present. Wounds made by double shots, as from double-barrelled guns, or pistols, or from slugs fired from one barrel, diverge after their entrance into the body. [Pg 87]
Observations during the war in South Africa threw fresh light upon the results of gunshot wounds produced by modern projectiles. Of wounds produced by the Mauser bullet, one correspondent (The Physician and Surgeon, 1900, p. 49) states that “the aperture of entrance seldom shows any bruising of surrounding tissue; frequently it has been difficult to locate it, for where the skin is dense and elastic, there is seldom any bleeding. There is never any inversion of the edges, which are sometimes circular in form, and sometimes triangular like a leech-bite. The aperture of exit, where the bullet has not been distorted, is seldom any larger than that of entrance; there is no bruising of surrounding tissue, and no eversion of the edges; bleeding varies, of course, in accordance with the proximity of large, medium, or small blood-vessels in the track, but in the vast majority of cases it is slight.”
The late Sir William MacCormac, quoted by Sir William Stokes (B. M. J., vol. i., 1900, p. 1453), says: “I saw a large number of injuries inflicted by the Mauser bullet, which is remarkable for the small wound it produces. In three-fourths, if not a larger proportion, it was impossible to tell the exit from the entrance wound, they were so similar in appearance.”
In the examination of gunshot wounds we have to consider—
1. Direction in which the Gun was fired.—The track and position of the ball in the body, coupled with the relative position of the body to a window or door through which the gun may have been discharged, and the place where the ball is found, should it have passed through the body, may assist us in forming an opinion. It is often impossible to trace the course of the ball through the cavities of the body, but through the muscles and denser structures this is more easily accomplished. The effects of the ball on surrounding objects may assist very much in finding the direction of its course. Sir Astley Cooper, by a careful consideration of the above suggestions, once correctly determined that a left-handed man had fired the fatal shot.
2. Distance at which the Charge was fired.—In the case of wounds inflicted by a small shot, the scattering of the shot must be our guide. Dupuytren has related a case in which a fowling-piece charged with powder alone and fired at a distance of two or three feet from the abdomen made a round hole in it and killed the man. If the weapon be fired a short distance, e.g. a few inches from the body, the skin will be scorched, smoke-blackened, and tatooed with powder, the flame may singe the hair or clothing. If discharged quite hard up to the body, the edges of the wound are freely lacerated, ecchymosed, and burnt. Smokeless powder will not cause blackening of the skin. The absence of scorching, or marks made round the wound by the half-burnt powder, allows of the assumption that the shot must have come from some distance—rather more than four feet. The absence of any of the above, however, is not an absolute proof that the shot has come from a distance.
There is no means of deciding, from an examination of a pistol or gun, when the weapon was last used. In all cases, medical men, unless sportsmen and familiar with firearms, should hand over the weapon to a [Pg 88] gamekeeper or gunsmith, and not attempt to give an opinion on matters about which they know nothing. The following may be of use to students for examination purposes, but for nothing else: Among the products formed when gunpowder is exploded is the sulphide of potassium, but if exposed to the air some portion of this substance is converted into the sulphate of potash. If, then, the gun-barrel be washed out with distilled water, and the washings filtered, and, on the addition of a solution of acetate of lead, a black precipitate of sulphide of lead be formed, this is supposed to point to recent use; if, on the other hand, a white precipitate of sulphate of lead forms, to the use of the weapon at some more distant date than the period alleged.
It is important in medico-legal investigations to determine the nature of stains found on clothes, weapons, articles of furniture, &c. In the case of blood-stains note should be made of their incidence upon the body or in its vicinity. Blood-stains may vary in their character, incidence, and magnitude, as sprays, spirts, or jets, smears of various forms, or pools of blood.
Notes should be made of the relation of the direction of a spray of blood to the position of a wounded body when found. A plan with the position of the stains should be sketched upon the spot, and measurements taken carefully.
In the examination of blood-stains the purpose of the medico-jurist is not to demonstrate all the properties of blood, but to identify it. There is not much difficulty in ascertaining whether stains are due to blood or not; but when the question arises as to whether the blood be human or that of some other animal, the identification is more difficult and less certain.
Blood-stains vary in colour, according to the age of the stain, the quantity of blood in it—the thicker the stain the darker—and the nature and colour of the material upon which it is. Recent stains are reddish in colour, old stains brownish. This change of colour depends upon the free access of air and the presence or absence of chemical substances in the air, so that it is almost impossible to infer the age of a blood-stain by its colour. On dark-coloured materials the stains are rendered more visible by the aid of artificial light, such as candle-light; on light-coloured materials, on leather, wood, iron, and stone, they are more visible in good daylight. By reason of the coagulation and the albuminous composition of blood, dry stains stiffen the fabric when thin, and on thicker woollen materials the fine fibres become matted. On metals, such as iron or steel, they appear as dark shiny spots or smears, and when dried are often fissured or cracked. Rust may so alter blood as to produce a difference between the stains on the blade and handle of a knife. In quite recent blood-stains the general appearances are sufficient to give rise to a conclusion as to their nature, especially if the stains are large. The general features as seen by the naked eye are such that one may often recognise blood-stains as arterial by the comet shape they retain when falling slantwise on an object. Venous blood is not spurted in small jets like arterial, but blood from veins may become splashed upon objects and assume shapes similar to those produced from an arterial jet. [Pg 90]
The examination of blood-stains should be carried out in the following way:
1. Examine the stains carefully with a good pocket lens or a low power microscope lens. A fabric will show matting of its fibres, red filaments, and minute coagula in its meshes. In old blood-stains coagula may be absent and the fabric appear as if dyed. The characters of any fibres or hairs adhering to the stain and the nature of the substance upon which the stain is should be noted.
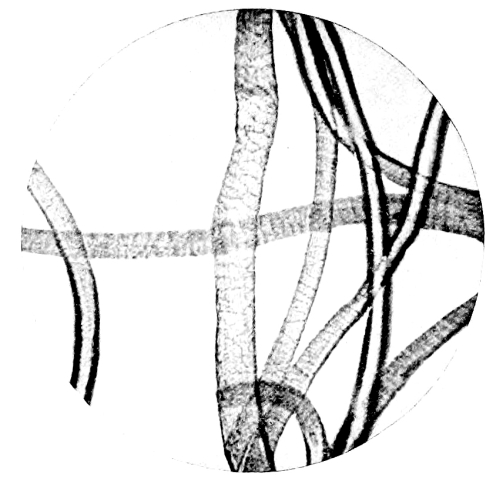
Fig. 4.—Photo-micrograph
of wool fibres, × 250.
(R. J. M. Buchanan.)
2. Make accurate notes of the position and shape of the stains on the material examined.
3. Take one stain, if there are several, or part if single, and note the solubility of it in water, or in a mixture of water and some other substance. The solubility of the colouring matter is greater if the stain be recent than if it be old. The older the stain the less soluble it becomes, as the hæmoglobin is gradually changed in course of time to insoluble hæmatin.
An endeavour should be made to obtain a solution for microscopical, chemical, and spectroscopical examination. The solvent, in order to obtain the blood corpuscles in as natural a form as possible, should approach in its specific gravity the liquor sanguinis.
The following solvents fulfil this purpose:
(a) Glycerine and water, 1 to 7 (sp. gr. 1030).
(b) Pacini‘s solution of chloral hydrate in water (1 in 10).
(c) Normal saline solution.
(d) Roussin‘s solution of glycerine 3 parts, sulphuric acid 1 part (by weight), and water so that the mixture shall have a sp. gr. of 1028.
(e) Saturated solution of borax in distilled water.
[Pg 91] If distilled water alone be used, the red corpuscles lose their hæmoglobin and become “laked” or “phantom” corpuscles; if the solution be of higher sp. gr. than liquor sanguinis, then the corpuscles become crenated and irregular in shape.
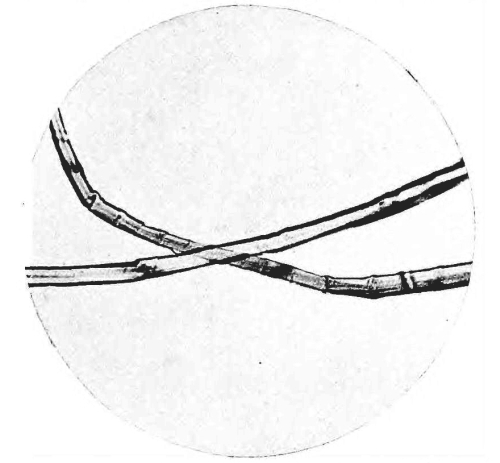
Fig. 5.—Photo-micrograph
of flax fibres, × 250.
(R. J. M. Buchanan.)
The technique of examination has to be varied in certain details, according to the material upon which the stain is. Stains may have to be examined upon cloth-fabrics, wood, plaster, metal, or leather. These will be taken separately, and the methods of examination described which will prove most reliable in each case.
1. Cloth-fabrics.—Cut out a stain, or part of one, and macerate it in a quantity of one of the solvents mentioned above, sufficient for the purpose. If the stain be very small, squeeze with fine forceps one or more drops upon microscope slides for microscopic, and keep the remainder of the solution for spectroscopic, examination. In dyed fabrics, which have been mordanted, the mordant may fix the blood-stain so as to prevent solution, and especially so when the attempts have been made to wash out the stain with soap and water.
To make a solution of the stain in such cases it is best to use distilled water to which a small quantity of ammonia or citric acid has been added; in one or other of these the colouring matter will dissolve.
2. Wood.—Note the kind of wood, cut off a thin shaving and treat with one of the solvents mentioned above. If on wood containing [Pg 92] tannic acid, such as oak or elm, the best solvent is a two per cent. solution of hydrochloric acid.
3. Plaster.—Scrape off some of the stained plaster, and treat as for cloth or wood.
4. Metal.—If the stain be upon a clean and unrusted metal, e.g. the clean blade of a knife, then gently heat the metal on the side opposite to the stain, when the latter, if recent, will peel off or can be easily detached. This requires some care and dexterity. It is easy, however, to scrape the stain off into a watch-glass, and this procedure is necessary when the metal is rusted and the stain mixed with the rust, or when the stain is thin.

Fig. 6.—Photo-micrograph
of silk fibres, × 250.
(R. J. M. Buchanan.)
If on iron and mixed with rust the borax solution may be used, with a drop or two of solution of ammonia; use a fine camel-hair pencil dipped in the solution, and brush the stain off into a watch-glass. Becker advises that stains mixed with rust should be digested with a weak solution of ammonia and common salt for a few hours; decant the solution and evaporate it upon a microscope slide to dryness, then test the residue by the “hæmin test.”
Ganttner‘s test should be used to a portion of a stain upon metal when thin or mixed with rust. It may be carried out upon the metal itself or upon a scraping of the stain in a watch-glass resting upon a black surface. Moisten the scraping in a watch-glass with a drop or two of distilled water rendered feebly alkaline, then add a minute drop of hydrogen peroxide. Wherever blood is present bubbles of gas develop, which give the material a white beaded appearance. The froth develops from the outside of the drop towards the centre when the stain is mainly composed of blood. In a scraping consisting of mixed particles [Pg 93] of rust and blood, the reaction only appears upon the particles of blood, and rust to which blood adheres; it does not take place on those particles of rust free from blood. Before adding the peroxide of hydrogen it may be necessary to dissipate any air-bubbles which may cling to the scraping in the alkaline water by gentle agitation with the point of a fine glass rod. Should the above reaction with peroxide of hydrogen not take place, then one can rest assured that no blood is present. The test, however, is a negative one; it is not a positive test for blood only; other fluids and exudations from the body, such as saliva and pus, give the reaction. The reaction will take place with blood-stains of any age.
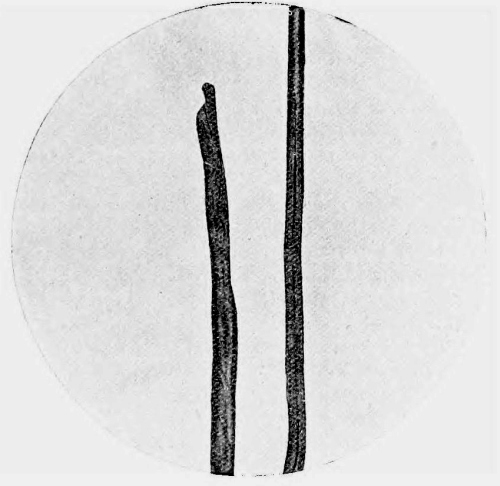
Fig. 7.—Photo-micrograph
of cotton fibres, × 250.
(R. J. M. Buchanan.)
In examining a clasp-knife or any hinged weapon for blood-stains, the instrument should be taken to pieces and all the hinges and recesses carefully examined, for in these places blood may be found, although the weapon had previously been wiped clean, and appear free from stains.
5. On Leather.—The tannic acid in leather forms a compound with blood which is insoluble in the solvents generally used. A thin shaving of the stained portion should be taken and folded, with the stained surface outwards, in the form of a loop. If the outer surface of the loop with the stain be made to touch the surface of the glycerine and water solution, at the same time taking care that the leather itself be not moistened, a recent stain may yield a sufficient quantity of colouring matter for the purposes of examination. Failing this, the shaving should be digested in a small quantity of a two per cent. solution of hydrochloric acid in distilled water (Sorby). [Pg 94]
The microscopical examination of blood-stains, for the purpose of identifying the presence of the red blood corpuscles, is especially applicable to recent stains. In these the corpuscles may retain, to a great extent, their normal characters; but their condition varies with the age of the stain; they become altered in appearance and irregular in shape with increasing age, until a stage is reached when they become completely disintegrated and unrecognisable. Having obtained a solution of a stain by one of the methods recommended, a few drops should be placed upon a clean microscope slide and covered with a No. 1 cover-glass. In a recent stain, where minute coagula are present, one may be placed on a microscope slide and moistened by breathing upon it several times, and then covering it with a No. 1 slip, or a drop of the glycerine solution may be allowed to act upon it on the slide until it be sufficiently moistened, when it should be covered in the same way. The preparation should be examined through the microscope with a good lens (preferably a ¹/₁₂th oil immersion), magnifying 300 to 400 diameters, and if any corpuscles be found, their characters should be carefully observed and noted.
All such specimens should be carefully preserved and labelled with a description of the method of preparation, the case to which they belong, the date of preparation, and the signature of the individual who has made and examined them. It is essential that the preparation and examination of the specimen should be made by the same individual. In certain cases the conditions may be sufficiently favourable to allow of the production of stained specimens, which can be mounted so as to retain their original characters permanently. In every case it is advisable to pursue the investigation with this object in view.
This process is especially applicable to recent blood-stains, in which, from preliminary examination, the presence of blood corpuscles has been determined; where complete disintegration of the blood corpuscles has taken place it would not be of any value.
It may so happen that by means of stained specimens the identity of blood corpuscles may be more easily established, when the result of examination is uncertain in a specimen not so prepared.
By the action of certain dyes upon the corpuscles their special features are rendered easier of recognition. Any of the approved methods of preparing blood films for general clinical purposes, which will suit the circumstances, may be employed. An easy and reliable method is as follows. A drop of the solution of the blood-stain properly prepared as previously recommended, or if obtainable a small coagulum moistened with normal saline solution, is placed on a clean coverslip and spread evenly over its surface with the aid of a fine glass rod. The film is allowed to dry in the air, covered with a watch-glass for protection against dust. When dry it is passed three times through the flame of a Bunsen burner, or placed in a mixture of [Pg 95] equal parts of absolute alcohol and ether, to fix it. After fixation it should be placed for a minute or more in an aqueous solution of eosin.
Any excess of stain should be removed by washing in distilled water, and the specimen allowed to drain by standing it on edge upon a piece of filter paper; it should then be allowed to dry, and then counterstained with a freshly prepared aqueous solution of methylene blue, hæmatoxylin solution, or other nuclear dye. Wash again in distilled water, allow to dry, and mount in Canada balsam. By this method the corpuscle will be stained pink, and if nucleated, the nucleus will be stained by the methylene blue, hæmatoxylin, or other nuclear stain which may have been used.
Leishman‘s stain may be used. This stain being a methyl-alcohol solution is used for fixing and staining at the same time. A few drops of the stain is placed on the dried film; after standing until evaporation is almost complete, distilled water is dropped on to the slide, and left to stand for two or three minutes, it is then drained off, and a few more drops of distilled water added until the film is pink in colour, then dried with filter paper. Red corpuscles are tinted red with the eosin, and nuclei of leucocytes or nucleated red cells violet or deep blue. The specimen may be examined direct with the oil immersion or mounted in Canada balsam.
When examining specimens prepared from blood-stains, it is necessary to search carefully for other cellular structures such as epithelial cells, spermatozoa, or fragments of hair.
It may be advisable, in certain cases where the amount of material submitted for examination is small, to centrifugalise some of the solution in a fine glass tube, in order to determine any cellular elements present to one spot. By making use of this concentrated portion containing the cellular elements for the preparation of a microscopic specimen, one not only facilitates the microscopical examination, but is able to place more reliance upon the results obtained.
The Results of Microscopical Examination of
Blood-Stains in Their Medico-Legal Relations.
As previously stated, the examination of alleged blood-stains from a medico-legal standpoint is pursued essentially for the purpose of testifying as to whether they have been produced by blood or not. Where the examination yields a negative result, further procedure is necessary with a view of identifying the true nature of the stain. Should, however, the result be positive, the question arises as to the possibility of distinguishing between human blood and the blood of other animals, and determining the exact animal from which the blood has been derived. Such an examination should be pursued in full recognition of its importance as a factor towards the establishment of truth essential to the administration of justice.
To fulfil this obligation the methods employed should be so selected as to produce results bearing testimony free from any possibility of doubt.
Certain differences exist, and may be detected by microscopical [Pg 96] examination, between the red corpuscles of human blood and those of some other animals sufficiently well marked to render differentiation possible. The differences are those of form and structure.
(1) In man the red corpuscles appear as circular biconcave discs, averaging ¹/₃₅₀₀ of an inch in diameter, and are non-nucleated.
The red corpuscles of mammals present the same features, with the exception of the
(2) Camel tribe, in which the corpuscles are oval in form, but non-nucleated.
(3) In birds, fishes, reptiles, and amphibians the red corpuscles are oval in shape, and possess a nucleus.
Guided by the above facts, one is able to testify whether or not the corpuscles exhibit the characters of mammalian blood.
Many attempts have been made with a view to establishing a reliable means of differentiation between the red blood corpuscles of man and other mammals (the camel excepted), and with a certain degree of success, such as might be expected, under select conditions favourable to histological research, but which do not obtain in medico-legal practice. Differences in size of the red corpuscles, as revealed by micrometric measurement, have been suggested as a possible means of distinguishing between the blood of different mammals. Of the common animals, the red blood corpuscles of the sheep present the most marked difference in size compared with those of man. The following table of the dimensions of red blood corpuscles is derived from measurements made by Treadwell, and quoted by White (The Medico-Legal Journal, New York, 1895):
| μ. | |
| Human | 7.940 |
| Dog | 6.918 |
| Rabbit | 6.365 |
| Ass | 6.293 |
| Pig | 6.101 |
| Horse | 5.503 |
| Cat | 5.463 |
| Ox | 5.436 |
| Sheep | 4.745 |
Menstrual blood contains no fibrin, has an acid reaction due to the vaginal mucus which keeps it fluid, and contains squamous epithelial cells. None of these characters can be differentiated on fabrics, especially when contaminated with urinary stains in addition. Hence, in cases of alleged rape, no distinction can be drawn between blood-stains on the underclothing of the female, which may have arisen from hæmorrhage the result of violence to the sexual parts, and those which might have arisen from the ordinary menstrual flow or metrorrhagia. The detection of spermatozoa, however, would add considerable value to the observation. [Pg 97]
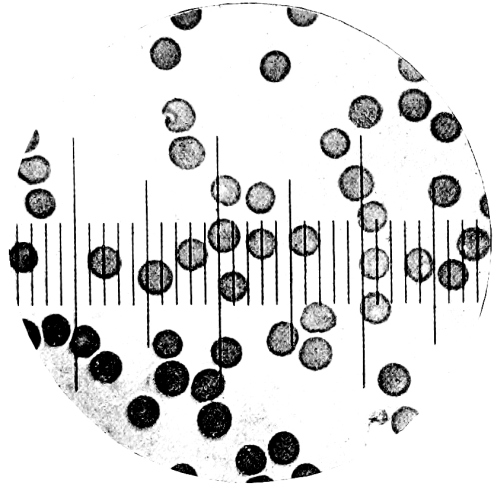
Fig. 8.—Measurement of Blood Corpuscles.
Photo-micrograph of human red blood corpuscles, × 800. Each corpuscle in diameter covers two divisions of the scale. Compare with sheep‘s blood, Fig. 9.
(R. J. M. Buchanan.)
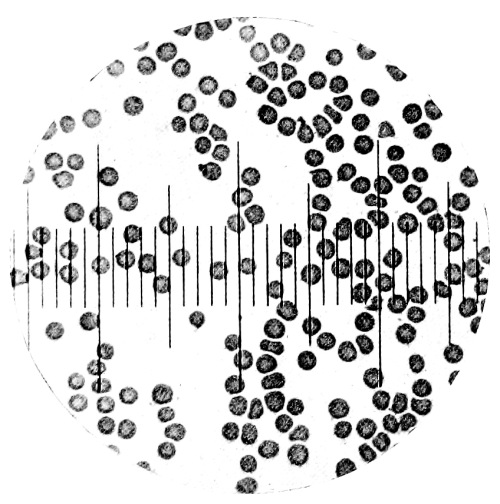
Fig. 9.—Measurement of Blood Corpuscles.
Photo-micrograph of red blood corpuscles from the sheep, × 800. The diameter of the corpuscle covers one division of the scale. Compare with human blood, Fig. 8.
(R. J. M. Buchanan.)
[Pg 98] Blood Crystals.—Professor Preyer of Jena pointed out many years ago that the hæmoglobin crystals from the blood of some animals differed in shape from those of man, and this fact has given rise to many attempts to trace the identity of the blood to the animal from which it has been derived. The results have not been of sufficient value to establish it as trustworthy for medico-legal purposes. Dr. Monckton Copeman (B. M. J., vol. ii. p. 190, 1889) has carefully investigated the subject, and his researches, partly confirmed by Professor Glaister of Glasgow, show that from the guinea-pig, rat, and squirrel, crystals of hæmoglobin may be easily obtained, but the solubility of human hæmoglobin renders it much more difficult to crystallise. Crystals may, however, be obtained in the following ways:
(a) By feeding leeches on human blood, crystals may be found, after some weeks, in the gastric dilatation of the alimentary canal.
(b) By diluting human blood with the fluid from hydrocele, ascites, or pleurisy when they have undergone decomposition.
(c) By adding crystals of glycocholate or taurocholate of soda to human blood.
(d) By adding a drop of cat‘s bile to human blood on a microscope slide, but the crystals are those of reduced hæmoglobin.
Crystals of human hæmoglobin appear in the form of rectangular plates, with a greenish or pale claret colour. On spectroscopic examination they exhibit the characters of reduced hæmoglobin, in contradistinction to the crystals derived from the lower animals, which produce the spectrum of oxyhæmoglobin.
The blood of the bullock, sheep, and pig is very difficult to crystallise. By the method adopted by Gamgee of adding to defibrinated blood one-sixteenth its volume of ether, shaking until the mixture becomes transparent, and allowing to stand in an ordinary temperature for 48 hours, crystals may be obtained from the blood of the following animals:
| 1. | Horse. |
| 2. | Bullock. |
| 3. | Sheep. |
| 4. | Pig. |
| 5. | Dog. |
| 6. | Cat. |
| 7. | Rabbit. |
| 8. | Squirrel. |
| 9. | Guinea-pig. |
| 10. | Rat. |
| 11. | Mouse. |
| 12. | Chicken. |
| 13. | Pigeon. |
Crystals from human blood are not easily obtainable by this process, but when they are, they always give the spectrum of reduced hæmoglobin, whereas those from the animals mentioned above give the spectrum of oxyhæmoglobin.
Having obtained a coloured solution from a supposed blood-stain, if sufficient in quantity, apply the following chemical tests to separate portions:
1. Add a few drops of a weak solution of ammonia in distilled water. The colour may remain unchanged, or, at the most, a slight heightening may take place, if it be due to blood. If the solution of ammonia be too strong, a brown colour may be produced if blood be present.
2. Heat to boiling, when the following changes take place if blood be present:
(a) The colour may disappear.
(b) Coagulation follows.
(c) A precipitate falls, dirty grey or brown in colour, depending upon the amount of colouring matter present.
On adding caustic potash to the precipitate it will dissolve, and the solution formed will appear greenish by transmitted and red by reflected light. This phenomenon is called the dichroism of blood. Authorities differ in opinion as to whether the colour is green by transmitted and red by reflected light, or vice versa. “As a matter of fact, the phenomenon is chameleon-like as regards colour, so that both sets of observers may be considered right or wrong” (Glaister).
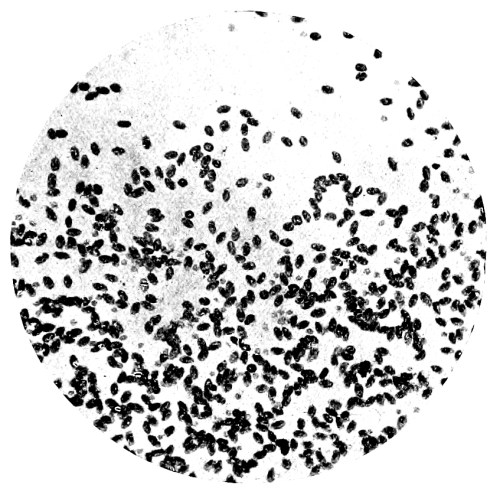
Fig. 10.—Photo-micrograph of red blood
corpuscles from domestic fowl, × 250.
(R. J. M. Buchanan.)
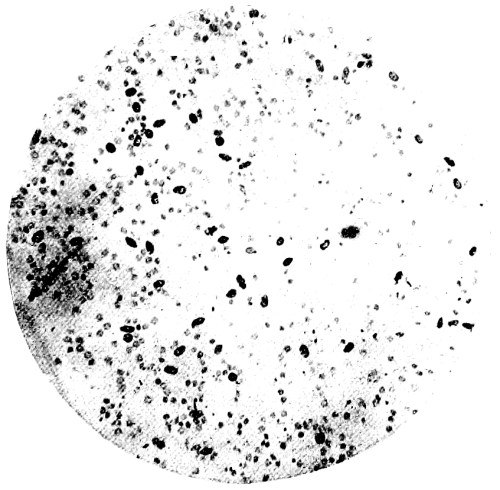
Fig. 11.—Photo-micrograph of blood
corpuscles of fish, × 250.
(R. J. M. Buchanan.)

Fig. 12.—Photo-micrograph of blood
corpuscles from a dried stain of the blood of a codfish, × 250.
(R. J. M. Buchanan.)
3. Add tincture of guaiacum, freshly prepared: an opaque, cream-coloured precipitate of the guaiac resin will form in the aqueous solution. On the addition of ozonic ether, turpentine, or peroxide of hydrogen, a blue colour will be produced at the junction of the fluids: proportionate to the amount of blood-colouring matter present, the blue colour will vary in intensity.
This test, known as Day‘s or Schönbein‘s, is extremely delicate, and reacts to no coloured substance except blood.
In cases where the blood-stain is small, the test may be applied as follows. Moisten a pure white filter paper with a drop of distilled water, or one of the solutions recommended in the section on physical examination, and touch the stain with the moistened portion. On adding a drop of tincture of guaiacum followed by a drop of ozonic ether to the wet filter paper the blue colour will be produced and easily recognised on the white surface.
The guaiacum test, although extremely delicate, can only be accepted as providing negative evidence. The absence of reaction proves the absence of blood, except in very old blood-stains, which may not respond [Pg 101] to the test. The blue colour produced indicates that the substance may be blood, but it cannot be accepted without corroboration. Gluten, raw potato, milk, bile, sweat (Ogston), and other oxidising substances give a blue colour with guaiacum and ozonic ether; some substances give the blue colour with guaiacum alone.
With blood, however, the test is sufficiently delicate to detect one drop in six ounces of water.
4. Nitric acid added to a portion of the solution of blood in distilled water produces a whitish-grey precipitate.
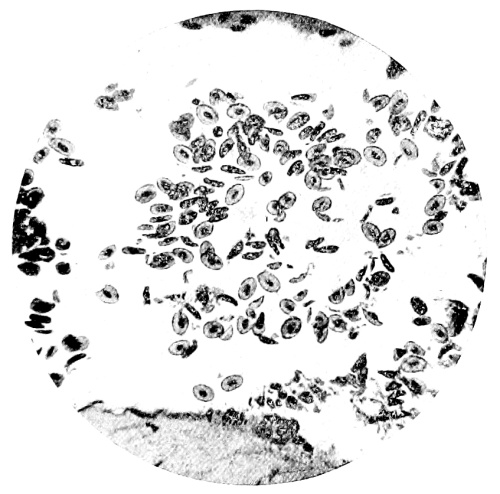
Fig. 13.—Photo-micrograph of
frog‘s blood showing oval nucleated red corpuscles, × 250.
(R. J. M. Buchanan.)
5. Hæmin Crystals.—Concentrate a portion of the solution upon a microscope slide, add to it a minute crystal of chloride of sodium and a few drops of glacial acetic acid. Heat gently to dryness or to a lesser degree under a coverslip; examine with the microscope; if blood be present, crystals of hæmin, or the hydrochloride of hæmatin, will be found. They are of a yellowish-red to brownish-black colour with a metallic lustre. They occur in rhomboidal prisms, or six-sided in shape, or in the form of “whetstones,” often in clusters; many of the crystals exhibit a lipped projection on one side. They are known as Teichmann‘s crystals. It is well to verify their origin from blood by placing upon them a drop of hydrogen peroxide, when they will give off bubbles of oxygen gas.
They are insoluble in water, alcohol, and dilute acetic and hydrochloric acids. They dissolve in boiling acetic or hydrochloric acids, and the caustic alkalies. They respond to the guaiacum test, and the ash produced by incineration shows the presence of iron by the red [Pg 102] colour produced on the addition of a drop of hydrochloric acid and a solution of potassium sulphocyanide.
The production, by the methods described, of such crystals affords conclusive proof of the presence of blood.
To a portion of the coloured solution, filtered if necessary, the spectroscopic tests should be applied. The following points must be remembered in carrying out a spectroscopic examination:
(a) The colouring matter of fresh blood is hæmoglobin, and it may exist in two states, according to the degree of its combination with oxygen.
In arterial blood it is present as oxidised hæmoglobin, and the same obtains in blood which has been exposed to the air under certain conditions and for a varying period of time.
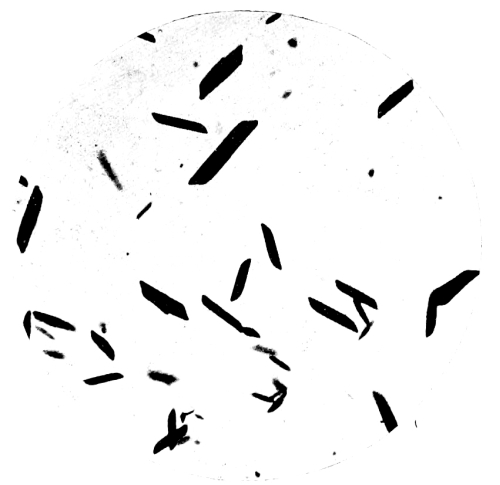
Fig. 14.—Photo-micrograph of
crystals of hæmin, × 250.
(R. J. M. Buchanan.)
In venous blood, especially when obtained under conditions preventing oxidation, as from the heart cavity of an animal newly asphyxiated, it is present as deoxidised hæmoglobin.
(b) In dry stains, especially if they have been subjected to the action of impure air containing the products of coal-combustion, the colouring matter becomes changed into methæmoglobin, or hæmoglobin in which its combination with oxygen has been altered in such a way that a current of a neutral gas, such as hydrogen or nitrogen, will not dissociate it, as it does with oxyhæmoglobin. Such stains have a brownish colour, and may give an acid reaction.
(c) In stains which have retained moisture, from having lain in damp places, the hæmoglobin becomes converted into hæmatin. The same change takes place in dry stains after a longer period of time. [Pg 103]
On examining the solution of the colouring matter from a blood-stain with the spectroscope, the spectrum will vary according to its condition and the nature of the solvent used.
The spectra of hæmoglobin and its derivatives are characteristic, and afford conclusive evidence of the presence of blood. The spectra must be recognised, however, in more than one condition. Other substances may yield spectra very similar to that of oxyhæmoglobin, but when subjected to certain tests they do not alter in the same way. They cannot be made to give the spectra of reduced hæmoglobin and reduced hæmatin, and any colouring matter which may be made to yield the spectra of reduced hæmoglobin and reduced hæmatin is derived from blood.
1. Oxidised hæmoglobin (O₂Hb) is characterised by the presence in its solar spectrum of two absorption bands between the D and E lines. The first band commences at the D line and extends a short distance towards the E. The second commences at a little distance from it, and terminates at the E line; it is about twice the breadth of the first. The band at D is more defined than the other (Fig. 15, 1).
2. Deoxidised or reduced hæmoglobin presents one broad band occupying almost the whole of the space between D and E slightly to the left of these lines (Fig. 15, 2).
3. Methæmoglobin presents two bands between D and E, in the same position as those of O₂Hb, but in addition a third band between C and D and near to the former (Fig. 15, 3).
A solution of oxyhæmoglobin or methæmoglobin may be reduced by the addition of a reducing agent, such as Stokes‘ reagent, consisting of ferrous sulphate with a small quantity of tartaric acid dissolved in water and rendered alkaline at the time of using with ammonia, or, better still, by the addition of ammonium sulphide. The spectrum will change to that of reduced hæmoglobin.
4. Acid hæmatin presents a spectrum with a band between D and E, commencing at a little distance from D and ending at E, also a narrower band between C and D and commencing at C. It is a difficult spectrum to obtain.
5. Alkaline hæmatin presents a spectrum with a single band between C and D near to the D line. It is more difficult to obtain than the spectrum of acid hæmatin.
It is not necessary, however, to obtain these spectra, viz. 5 and 6, but it is necessary to reduce solutions of either acid or alkaline hæmatin in order to obtain the spectrum of reduced hæmatin. To do so proceed as follows. To some of the solution of colouring matter obtained from the stain add a small quantity of a 20 per cent. solution of sodium hydrate; the solution will alter in colour, and the spectrum of O₂Hb or MetHb will disappear. On adding to this solution of alkaline hæmatin a few drops of ammonium sulphide, or Stokes‘ fluid, it becomes claret-coloured, and on examination with the spectroscope the spectrum [Pg 104] of reduced hæmatin will be seen. This is the most pronounced of all blood spectra. Its production can be hastened by gently warming the solution.
If the stain be old and already changed into hæmatin, its solution will yield the spectrum of acid hæmatin, and will give the spectrum of reduced hæmatin on the addition of ammonium sulphide or Stokes‘ fluid without previous alkalisation.
6. Reduced hæmatin presents a spectrum with a dark band about midway between D and E, and a broad but paler band commences near the E line and extends to the b line (Fig. 15, 4).
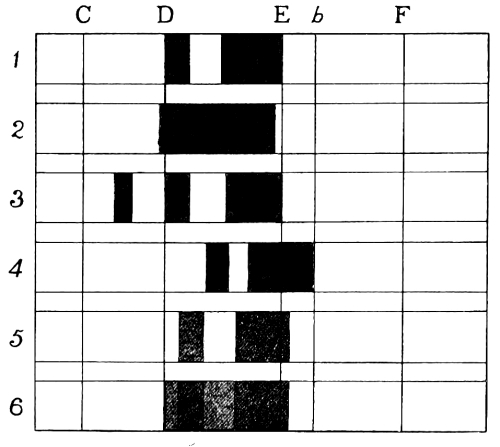
Fig. 15.—Blood Spectra.
| 1. Oxyhæmoglobin. | 3. Methæmoglobin. | 5. CO hæmoglobin. |
| 2. Reduced hæmoglobin. | 4. Reduced hæmatin. | 6. CO hæmoglobin and |
| reduced hæmoglobin. |
In cases of death by asphyxia, in which the hæmoglobin is in combination with CO₂, the blood, if removed and examined immediately after death, gives a spectrum of reduced hæmoglobin, but on exposure to the air it rapidly changes to oxyhæmoglobin. The period after death at which blood is usually submitted for medico-legal examination is sufficiently late to allow of this change, and so prevents the possibility of determining death by asphyxia by spectroscopic examination of the blood. Where death has been caused by the action of carbon monoxide, the blood is of a cherry-red colour, and it will retain this colour unchanged for a long time, in fact for years, due to a stable combination of the CO and hæmoglobin, called carboxyhæmoglobin. Such blood yields a very characteristic spectrum, with two bands similar to those of O₂Hb, but nearer to the violet end (Fig. 15, 6). Their position should be assured by accurate measurement and comparison with a spectrum of O₂Hb. The CO hæmoglobin, however, cannot be reduced; on the addition of ammonium sulphide or Stokes‘ fluid the bands remain unaltered. [Pg 105]
In cases where the amount of fluid obtainable for examination is very small, recourse must be had to the micro-spectroscope, using a Sorby‘s cell to hold the fluid, and substituting for the eye-piece of the microscope a specially constructed spectroscope arranged so as to throw the spectrum of a known solution of blood-colouring matter alongside of that yielded by the solution under examination. Artificial light should be used, and the D line located by placing in the flame a platinum wire carrying a salt of sodium.
The results of the experimental investigations of Friedenthal,[3] Deutsch,[4] Uhlenhuth,[5] Wasserman and Schutze,[6] Nuttall,[7] Tarchetti,[8] Grünbaum,[9] Metchnikoff,[10] and M‘Weeney[11] into “blood relationships” have led to the suggestion of a new method—the “biological test,” by which different kinds of mammalian blood may be distinguished one from the other. Their experiments show in a general way that the “serum from an animal which has been injected intraperitoneally with any given organic fluid will, if mixed in small quantity with a dilute solution of the fluid used for the injection, produce a more or less definite precipitate.” If human defibrinated blood be injected into the peritoneal cavity of a rabbit, the serum obtained from the rabbit‘s blood, when mixed with a clear solution of the blood of man or ape, will produce a precipitate, and agglutinate the red blood corpuscles if present: the same reaction will not follow if such serum be added to a solution of the blood of any other animal.
The introduction of substances of albuminous or proteid nature into the body of an animal, and which can be taken up by its cells as a food, produces in the body of the animal a series of substances called antibodies, of which one is designated precipitin from its power of producing a precipitate with the substance introduced. The organic substance introduced capable of producing antibodies is called the antigen. The precipitin is formed and present in the blood serum of the inoculated animal.
Metallic poisons, alkaloids and carbohydrates, do not produce antibodies; some vegetable proteids do.
The serum containing the precipitin is called the antiserum.
The precipitin in the antiserum is specific, and produces the effect only with its own antigen, not with that derived from another species of animal, but will act with one derived from a closely allied species, e.g. man and the higher apes, sheep, and goat. [Pg 106]
In order to eliminate this the antigen should be diluted to 1:1000.
The blood used as antigen may be dried and sterilised, thus it may be kept for a long time, and when required for use dissolved in normal saline.
The most convenient human antigen for general use is ascitic or pleuritic fluid, and may be kept in good condition when mixed with a small quantity of chloroform.
To produce the antiserum 3 to 10 c.c. of the antigen serum is injected into a vein or the peritoneal cavity of a rabbit, and repeated at an interval of four or five days until 25 c.c. have been injected. The serum of the rabbit is then tested with the antigen diluted 1:100. The injections are then continued until 70 to 80 c.c. have been administered. The animal is then killed, the blood collected, and stood in a refrigerator for the serum to separate. This is then drawn into sterile pipettes, sealed, and kept in the cold. For purposes of preservation one-tenth its volume of 5 per cent. phenol may be added before pipetting. The antiserum may be dried on slips of black paper for future use.
For medico-legal purposes, the antiserum should always be tested with its antigen to be sure of its efficacy.
The antigen to be tested should be diluted 1:1000 at least, as potent antisera may give reactions with strong solutions of antigens derived from other species of animals. Various antisera may be made by inoculating rabbits with the serum of different animals.
Metchnikoff has shown that intraperitoneal injection is not absolutely necessary in order to produce an antiserum, feeding a rabbit on the blood will act in the same way.
The procedure for testing a stain is as follows. First of all the stain must be proved to be blood by the usual methods; this because the antiserum will give reactions with other albuminous substances, e.g. mucus, pus, semen, milk, or albuminous urine derived from the animal providing the antigen.
Having proved the stain to be blood, a solution of it should be made in normal saline, sufficiently strong to give the HNO₃ reaction for albumin, or to foam when shaken up. If the amount of solution be small, the tests can be carried out in capillary tubes or pipettes. The solution of the stain must be cleared by filtration or the centrifuge.
The tests must be controlled by comparison with known human blood, and blood from several domestic animals. For this purpose the various antisera should be kept in stock.
Two sets, A and B, of six small tubes are used, into each of A is placed 0.05 c.c. of human antiserum from a sensitised rabbit. Into each tube of Set A is then added double the amount of diluted antigen, as follows:
| Set A — | 1. | Receives | extract | of known | human | blood | -stain. | |
| 2. | “ | “ | “ | ox | “ | “ | ||
| 3. | “ | “ | “ | horse | “ | “ | ||
| 4. | “ | “ | “ | sheep | “ | “ | ||
| 5. | “ | “ | “ | pig | “ | “ | ||
| 6. | “ | “ | “ | stain | under observation. | |||
Set B is now charged as follows: [Pg 107]
| Set B — | 1. | Receives | normal | rabbit serum | 0.05 | c.c. |
| 2. | “ | human | antiserum | 0.05 | “ | |
| 3. | “ | ox | “ | 0.05 | “ | |
| 4. | “ | horse | “ | 0.05 | “ | |
| 5. | “ | sheep | “ | 0.05 | “ | |
| 6. | “ | pig | “ | 0.05 | “ |
To each tube in Set B is now added about 0.1 c.c. of the extract of the suspected stain.
It will thus be seen that in Set A known antigen is added to known precipitin, with the exception of tube 6, which receives suspected antigen, while in Set B the suspected antigen is added to known antisera, with the exception of No. 1, which contains normal rabbit serum.
The tubes are observed in an hour and the results noted. Should the stain be human blood, positive reactions will be present in tubes 1 and 6 of stand A, and tube 2 of B.
The negative reactions in the other tubes in stand A prove that the antiserum used is specific, and will only react with its own antigen; in stand B that the stain is composed of specific human antigen, reacting only with its own antiserum.
Should the stain suspected be other than human, and derived from one of the other animals used for antiserum in stand B, then the positive reaction will occur in the particular tube.[12] The test is now recognised as very sensitive and reliable, and is also applicable to the detection of the flesh or fluids of animals, and has thus been used for the detection of meat stuffs.
Tarchetti advises the following procedure in the examination of blood-stains: Dissolve the stain in a few drops of a 0.9 per cent. aqueous solution of sodium chloride, filter, and divide the filtrate into two portions; to one (a) add 0.5 c.c. of the prepared rabbit serum (the so-called antiserum); to the other (b) serum from a rabbit which has not been injected with human blood. Both are to be placed in an incubator at 37° C. for an hour. By this time, if the solution of the stain be of human or anthropoid origin, the contents of the tube (a) will have become turbid, the contents of tube (b) will remain clear. From a series of experiments with blood-stains of man and other animals on a variety of materials, Tarchetti states that this method is reliable. Prepared rabbit “human antiserum” has been shown to have no such reaction with the blood of the pig, ox, calf, mouse, or rat.
From the result of his investigations Grünbaum points out that these reactions must be looked upon rather as “special” than “specific,” in view of the fact that his “chimpanzee antiserum” gave a slight but distinct turbidity after a few hours with horse blood. He also suggests a method for the microscopical application of the “biological test,” by using a 1 per cent. blood solution with a drop of [Pg 108] “antiserum.” This method has enabled him to distinguish between human and anthropoid blood, the reaction occurring earlier and being more complete when the “antiserum” is used on its own blood.
Certain vegetable colouring matters give spectra which may be mistaken for blood, from their close similarity. Of these cochineal dissolved in a solution of alum gives two bands similar to O₂Hb. On the addition of boric acid the bands move to the violet end of the spectrum, but they are unaffected if the colouring matter be blood. Lac-dye, alkanet root, madder, and others also give spectra resembling O₂Hb, but they are changed or disappear on adding ammonia or sulphite of potassium, while the spectrum of blood remains unaltered.
As stated previously, spectra of colouring matters other than blood are not capable of being altered by reducing agents, so that, however similar they may be to O₂Hb, they cannot be accepted as derived from blood unless the spectra of reduced Hb and reduced hæmatin can be obtained in the way described.
Cochineal, colours of certain roots and wood, turn crimson on the addition of ammonia, logwood bluish-black.
The colour of the rose and certain flowers turn green on adding ammonia.
Fruit-stains from mulberry, currants, gooseberries, &c., turn bluish-green with ammonia.
Vegetable stains have their colour heightened by the action of dilute acids.
Chlorine bleaches fruit-stains, but turns the colour of blood-stains to an olive-green.
Red dyes fixed by a mordant are not influenced by ammonia.
Iron stains are usually blackened by ammonium sulphide.
Red paint may contain red oxide of iron; digest with hydrochloric acid and test for iron, by adding ferrocyanide of potassium to obtain the Prussian blue. Iron stains may be of a reddish-brown or orange colour, and insoluble in water, so that HCl is used to dissolve them.
Citrate and malate of iron stains are soluble in water; the addition of ammonia to an aqueous solution produces no change; guaiacum will give a blue reaction if a persalt of iron be present. The addition of hydrochloric acid and ferrocyanide of potassium will give the Prussian blue reaction. A drop of nitric acid added to the solution will oxidise the iron to the ferric state, and on the addition of a few drops of fresh-made aqueous solution of sulphocyanide of potassium the port-wine colour of sulphocyanide of iron will be produced.
A control test must be made with distilled water to prove the purity of the reagents, and the two results compared with each other.
Aniline stains resembling blood are changed to greenish-yellow or yellow on the addition of dilute nitric acid. Eosin stains produce a [Pg 109] fluorescent solution when dissolved in water. Grease, tar, pitch, snuff, and paint may be mistaken for blood, especially on dark fabrics. They may be detected by two methods:
(a) The Wet Method.—Having failed to obtain a solution by the aid of the ordinary solvents for blood, other solvents must be used; ether or benzene for grease, paint, or tar. The solution obtained must be examined with the spectroscope.
(b) The Dry Method.—Place the cloth or other fabric stain down upon a clean white filter paper; then on pressing the cloth with a hot laundry iron, grease, tar, or pitch will stain the paper, paint or snuff will not.
Burns and Scalds are lesions characterised by a more or less marked destruction of the tissues of the body, caused by the action upon its internal or external surfaces of a temperature higher than that of the body itself, or by the action of corrosive chemical substances.
Burns are produced in the following ways:
By exposure to radiant heat.
By the direct application of flame.
By contact with heated solids.
By contact with solid bodies which have become liquefied by heat, such as metals in a state of fusion.
By friction.
By lightning, electricity, and X-rays.
By contact with corrosive chemical substances, solid or liquid.
Scalds are produced by the application of heated liquids, at or near their boiling-points, or in a gaseous form—as steam.
The injuries produced will depend upon the degree of temperature, the period of exposure to its action, and the extent of surface involved.
The danger to life depends more on the extent of surface injured than the intensity of the burn or scald upon a limited area, unless the position of the burn render it peculiarly dangerous. Even though the injuries be comparatively superficial, if they involve one-third or one half of the surface of the body they must be regarded as fatal. They may prove fatal by shock, by asphyxia, by constant and profuse discharge from the injured surface, from absorption of septic matter, from secondary inflammations of internal organs and serous membranes—pleurisy, peritonitis, meningitis, perforating ulcer of the duodenum. Children succumb more quickly than adults to burns and scalds—the simplest, in their case, often proving fatal.
The cause of early death from burns and scalds is looked upon as a disorder of the blood following injury to the red corpuscles by the heat, and that this is more easily brought about in children, because of the thinness of the skin, and the red corpuscles being less capable of resistance.
The following table gives the different degrees of burns:
1. Superficial inflammation, characterised by redness without blistering.
2. Acute inflammation, the epidermis raised, forming vesicles containing serum. [Pg 111]
3. Destruction of the superficial layers of the true skin.
4. Destruction of the true skin and subcutaneous cellular tissues.
5. The superficial and deep parts converted into a charred mass.
6. Entire carbonisation of the parts.
These will vary according to the extent of the injuries, the length of time the individual lived after receiving them, and the causative agent.
External Appearances.—1. Burns.—Radiant heat whitens the skin, flames blacken it, from deposit of carbonaceous material. The hair and clothing of the body are singed. Blisters may be present on various parts, and roasted patches of the skin or deeper parts may be present. The flame of an explosive, such as a mixture of coal gas and air, scorches and mummifies the skin. The skin is blackened by the explosion of gunpowder, and particles of the powder may be driven into it; similar results follow explosions in coal mines, but to a greater degree. Burns caused by red-hot solids or molten metals vary in appearance according to the length of time they have remained in contact with the surface: if short, there may be injury to the skin only, with blistering; if for a longer period, there will be roasting or charring of the part, and blisters may not be present.
All stages of burns may be present.
The uncovered parts of the body, as a rule, are more affected than the clothed, unless the clothes become ignited, when the converse would hold good. In cases where the clothes have been saturated with an inflammable oil like petroleum the burns are much more severe.
2. Scalds.—The appearances produced and the severity of the result will vary directly with the boiling-point of the liquid. Boiling water and steam produce vesication; the hairs are not affected. If the steam be superheated, blistering may be absent, and the skin appear sodden and devoid of elasticity. If the person survive the injuries for some days, the skin will present appearances of reaction. After exposure to great heat the bodies of the victims are usually contorted, with the limbs flexed and the arms fixed in a defensive attitude—the “pugilistic attitude.” This condition is due to heat rigidity.
Internal Appearances.—The brain is shrunk, usually without any alteration in form, the lungs also shrunk, and the larynx, trachea, and bronchi may contain carbonaceous material; their membranes may be injected and covered with frothy mucus. The kidneys may present reddish-brown markings from altered blood, and degeneration of the epithelium of the tubules and Malpighian bodies.
There may be a reddened appearance of the mucous membrane of the stomach and intestines, and in a certain number of cases, where death [Pg 112] has occurred some time after the injuries, ulcers may be present in the duodenum.
The uterus and testicles resist the action of fire in a marked degree, and may be changed but slightly, although the rest of the body has been almost consumed.
The blood of persons who have been exposed to the action of CO during a fire will present the usual cherry-red colour and the spectrum of COHb. A similar cherry-red colour of the blood is found in bodies of persons burnt to death which is not due to the action of CO. The cause is a physical one, the alteration in colour being due to the coagulation of the albumin in microscopical particles by the heat. In this condition the spectrum is that of O₂Hb, and can be reduced in the usual way. The same peculiar condition of the blood may be produced in corpses by exposure to a sufficiently high temperature.
If on the examination of the blood COHb is detected, it indicates that the person in whose body it is found was alive during the progress of the fire.
Corrosives.—The appearances produced by the application of corrosive chemical substances are peculiar to them, and depend upon their special actions upon the tissues. Sulphuric acid acts by rapidly extracting water from the tissues and producing local rise of temperature; nitric acid combines with the tissues to form picric acid; nitrate of silver acts upon the tissue by hyperoxidation, and combines to form albuminate of silver, nitric acid being liberated. A solution of phosphorus in carbon disulphide, known as Greek fire, by the rapid oxidation and burning of the phosphorus produces combustion of the tissues.
The diagnosis of lesions produced by corrosives from those by fire or heated fluid or steam rests upon the absence of vesication, the presence of the stains on the skin or clothing which they produce, and the chemical analysis of the stains. Sulphuric acid produces a grey or brownish-black eschar on the body; hydrochloric acid may leave a whitish-grey stain; nitric acid produces a yellow stain on the skin, and may produce sloughing.
Was the burn inflicted before or after death?—The answer to this question depends upon careful consideration of all the evidences afforded by the external and internal appearances, and upon the presence or absence of vital reaction in the lesions found.
Two characteristic appearances—redness and vesication—are present in burns inflicted during life when the surface of the body is not charred and the tissues destroyed. The redness affects the surface and entire substance of the true skin, which is dotted by the deep red openings of the sudoriferous and sebaceous ducts. This appearance cannot be produced after death. Blisters are formed by a temperature somewhat less than that of boiling water. Vesication, according to Orfila, is characteristic of a burn inflicted during life, and the late Sir Robert Christison found that in burns caused before and after death the vesicles in the former contained serum, the latter air. In anasarcous subjects, however, serous blisters may be formed, especially if the [Pg 113] heat employed be not too severe. A case is recorded by Taylor in which vesicles containing bloody serum were formed on the body of a man who had just been drowned and who had been put into a hot bath.
Ante-mortem vesicles in which vital reaction has taken place present the following characteristics:
(a) They contain serous fluid in which albumin and chlorides can be detected.
(b) An inflammatory red bounding line round the circumference.
(c) Inflammatory redness of the base, and the papillæ of the skin.
(d) The presence of pus, which would indicate that the person had lived at least thirty-six hours after the burn had taken place.
In burns produced after death, the surface and substance of the skin is of a dull white colour, dotted with grey openings of the sudoriferous and sebaceous ducts, and the subcutaneous tissues are uninjected. Vesicles produced by burns may have to be distinguished from the phlyctænæ, the result of advanced putrefaction. The latter possesses none of the characteristics of the former.
If a vesicle present the following characteristics it may be accepted as a post-mortem origin without doubt: if it be small and its contents scanty, if the fluid it contain be free from albumin and chlorides, if it contain air, and if there be no signs of inflammatory reaction.
Was the burning homicidal, suicidal, or accidental?—No general rules for guidance can be here laid down. In most cases the conditions under which the body is found will point less to suicide than to homicide or accident. In cases of murder, the body is often burnt in the attempt to destroy all traces of the crime. It must, however, be borne in mind that intense heat applied to the body may give rise to a wound on the surface like that caused by a cutting instrument. Casper mentions such a case, in which a wound was found over the liver, due to the application of intense heat to the body. The conjunction of robbery will greatly assist in helping to solve the difficulty. It may be very confidently stated that to dispose of a body by burning is no easy matter.
The possibility of “spontaneous combustion” occurring in bodies during life has been mentioned in the earlier writings on medical jurisprudence, and cases have been recorded in which it has been alleged to have taken place. Up to the present time no undoubted case of “spontaneous combustion” during life has been seen. On the other hand, the possibility of its occurrence is contra-indicated by the following facts: that the human body must consist of 75 per cent. of its weight of water, to be compatible with life, and that a dead body steeped in methylated spirit for many months or even years will never [Pg 114] be consumed, if set on fire, in the rapid and complete manner alleged as occurring in cases of so-called “spontaneous combustion.”
A case is recorded by Beatson (B. M. J., vol. i., 1886, p. 295) of a man, subject to foul eructations from the stomach, who got out of bed during the night and struck a match to see the time; while blowing out the light his breath took fire, producing an explosive noise sufficiently loud to awaken his wife. Such cases are very rare.
It is a fact that by the action of certain micro-organisms upon organic matter inflammable gases are produced. That such an occurrence is possible, in the dead human body, is supported by cases recorded by Gull (Med. Times and Gazette, 1885) and Reynolds (Med. Chron., 1891). In Gull‘s case inflammable gases escaped through punctures made into the abdomen, and they burned spontaneously on contact with the air. In Reynold‘s case no flames were seen, but extensive and deep marks of burning were present, especially on the trunk and thighs. It has been suggested that the habitual use of alcohol in excess during life renders the tissues of the body more inflammable, but the matter is not yet decided. Tissues steeped in alcohol are not rendered more inflammable.
Dr. Ogston, who cautiously avoids committing himself to the belief in “spontaneous combustion,” yet thinks that the subject of preternatural combustibility in certain conditions of the body may perhaps, to say the least of it, be set down as one still sub judice. “There is no evidence to justify the use of the word ‘spontaneous,’ but there can be no doubt that an extraordinarily high degree of combustibility occurs in rare instances, to which the term preternatural combustibility would more correctly apply” (J. Dixon Mann).
Over-exposure to the action of X-rays produces burns of a peculiar character, and in cases of unprotected skin exposed to the action of the rays in those who are constantly working with them, forms of dermatitis have arisen which are intractable and tend to become epitheliomatous in character.
The results of slight over-exposure, or repeated short exposures vary from a simple redness of the skin to severe dermatitis, the hair of the part being shed. When the over-exposure or dosage has been severe, the skin may vesicate and ulcerate. I have seen this in cases where the rays have been used for reduction of the spleen in leukæmia and Banti‘s disease. The burns heal with cicatrisation of radiate shape, the skin around the scar being permeated with numerous capillary vessels which produce the appearance of capillary nævi, and in other instances large stellate superficial vessels are formed. In addition, marked pigmentation of the skin may follow the burn. X-ray burns which have produced vesication and ulceration or sloughing take a long time to heal in comparison with ordinary burns.
In repeated exposure to the rays, even when little redness has been noticed at the time, the formation of capillary vessels may become evident some time after the exposures have been stopped. This may cause [Pg 115] disfigurement, by the formation of telangiectasis, especially if they appear on the face or neck. The falling out of the hair is produced by X-rays as a therapeutic measure in cases of ringworm, and due precaution must be taken to limit the effect and area of exposure by proper screening. The same precaution should be used to protect parts of the body other than the part which requires treatment or examination in other conditions.
With increasing knowledge of the effects of X-ray exposures, special precautions have been devised to prevent untoward effects, so that burns from over-exposure, and dermatitis amongst X-ray workers are prevented.
In the living these injuries are accompanied with swelling, pain, and more or less discoloration of the part affected. Among malingerers it is not an uncommon practice to bruise the body to imitate the spots of purpura and scurvy. In scurvy, the condition of the gums common to that disease, and the state of the general health, will point to the true nature of the spots. The diagnosis of purpura will be assisted by noting the diffusion of the spots over the body. In old people purpuric spots frequently extend round the limbs, chiefly on one of the lower extremities. Many blood diseases are associated with ecchymoses and purpuric eruptions. Some persons are very easily bruised, and a pinch, by no means severe, will cause on their arms a severe bruise. Discoloration—ecchymosis—may take place in the skin, cellular tissue, muscles, or internal organs as a result of external injury, or it may be due to sudden and powerful contraction of a muscle or group of muscles. Not infrequently the discoloration does not appear over the seat of injury, but at some distance from it; and when the effusion is deep-seated, days may elapse before any discoloration of the skin takes place, and then it is not blue, as in superficial parts, but of a violet, greenish, or yellowish hue. A deep-seated ecchymosis may give no external sign of its presence; hence in all cases deep incisions should be made before an opinion is ventured as to the entire absence of this occurrence. This is very noticeable among the deep-seated muscles of a limb. In these cases, forty or fifty days may elapse before the deep-seated bruise shows its existence on the surface, and then only as irregular, yellowish, green, or bluish spots over the part. A very slight contusion, as a sprain of the ankle, may give rise to extended discoloration of the leg. An ecchymosis is not necessarily situated directly under the seat of injury. A blow given during life may not appear as an ecchymosis till after death. The change of colour in bruises begins at the circumference, and travels inwards. During the first three days the colour of the bruise is blue, bluish-black, or black; greenish on the fifth or sixth day; and yellow from the seventh to the twelfth. The extent of an ecchymosis depends greatly on the looseness of the cellular tissue. A slight contusion [Pg 116] causes a slight redness and swelling, and may leave no mark on the dead body, unless death has taken place within thirty-six hours. Injuries of this kind sometimes leave a parchment-like hardness and discoloration of the skin. The part looks slightly depressed, due probably to the epidermis having been partly rubbed off, and the skin then drying. Similar marks are sometimes made by blisters. These marks may be produced on the dead body by friction and exposure to the air.
The diagnosis of ecchymosis from hypostasis has been given (see p. 46). A tolerably severe blow after death would be necessary to produce appearances similar to those produced by a slight one during life. In scourging, there are parallel ecchymosed lines, of small spots resembling petechiæ. An internal organ may be ruptured, and yet there may be no appearance of injury externally. The liver is the organ most commonly ruptured. The rupture is almost always longitudinal, and in some cases a portion of the gland is more or less detached. The spleen is also not infrequently ruptured; and this occurs most frequently in countries where ague prevails. Rupture of the lungs and brain is rare. When the pelvis is fractured, the bladder is frequently found ruptured.
Death in most cases is due to internal hæmorrhage or shock, when any of the internal organs are ruptured.
Can the appearance of a bruise be produced after death?—It is possible that the appearance of a bruise inflicted during life may be produced within two hours after death, and in some rare cases even after the lapse of three hours and a quarter (Christison); but these ecchymoses are limited in extent, and when large are due to a rupture in a vein which can be readily ascertained. The experiments of the late Sir Robert Christison, relating to this question, are detailed in the Edinburgh Medical and Surgical Journal, vol. xxxi. The amount of violence required after death to produce appearances like those made before death is such as would seldom, if ever, be inflicted on a corpse, and, therefore, where we find a well-marked bruise we ought to infer that it was made before death.
The following table, compiled from the experiments of Christison, may assist the diagnosis:
| During Life. | After Death. |
| 1. Swelling of the part. | 1. No swelling. |
| 2. Coagulation of the blood | 2. No such appearance, unless |
| effused into the adjacent | there is a rupture of a large |
| cellular tissue, with or | vessel in the neighbourhood |
| without tumefaction. | of loose cellular tissue. |
| 3. Incorporation of blood | 3. No such appearance produced |
| with the whole thickness | by a blow after death. |
| of the true skin, rendering | |
| it black instead of white. |
N.B.—Extensive effusion may occur without affecting the skin, but when the skin is so affected Christison thought it decisive of ante-mortem injury. [Pg 117]
The Size and Form of a Bruise should be noted.
Why?
1. In Hanging and Strangulation.—The mark due to pressure of the cord on the neck in hanging runs obliquely round the neck; in strangulation, the mark encircles the neck. The mark is frequently interrupted, and may present very varied appearances in different parts of the neck. The mark of the knot may be found under the chin.
2. In Throttling.—The pressure exerted on the throat of the deceased by the fingers of his assailant may leave marks which may point to the means used to cause death.
3. In other Cases of Death by Violence.—The impression made by the weapon used may lead to the identification of the murderer. The marks left by the wards of a large door-key once led to the identification of the assailant.
Death from suffocation is said to result from any impediment to the respiration which does not act by compressing the larynx or trachea.
Suffocation may therefore be caused by pressure on the chest, as in persons crushed in a crowd. It may also be due to the respiration of certain gases, or to the presence of pulverulent substances in the air, which act by choking up the air-passages. Imprisonment in any confined space may cause death from suffocation, and abscesses bursting into the trachea, or vomiting matters in drunken persons lodging in the windpipe, may be attended with a like result. Pressure on the umbilical cord whilst the child is in the maternal passages causes death from suffocation.
Signs of Death by Suffocation.—The first effect of arrest to the passage of air into the lungs is the stagnation of blood in the capillaries of the lungs. Non-arterial blood then goes to the brain and consciousness is soon lost. The respiratory sensation is then arrested by the circulation of venous blood. The left side of the heart becomes emptied, and then weak; the right side full and engorged. The great venous trunks are also more or less full, and the abdominal viscera, liver, spleen, and kidneys congested. The arrest of the heart‘s action is a secondary effect; the right side is paralysed by being too full, the left by being empty. These signs may be said to be typical, or, rather, are to be expected in death due to suffocation, but it must be distinctly stated that they are not always present. The right side of the heart is not in all cases engorged with blood; and Christison warns medical men against expecting “strongly marked appearances in every case of death from suffocation.” The heart, moreover, continues to contract after the lungs have ceased to perform their duty. Death is thus due to apnœa—that is, death beginning at the lungs—and not to syncope. Death in some cases is from neuro-paralysis or nervous apoplexy. In death by shock, which in most cases is instantaneous, both sides of the heart are equally filled. Death, the result of disease, may present all the signs of death from suffocation, and no suspicion may be aroused as to the cause of death from the post-mortem appearances, especially if putrefaction have set in. [Pg 119]
The following table is given as an aid to diagnosis in this form of death:
Points to be noticed in forming a
Diagnosis of Death by Suffocation
1. The Blood.—There is unusual fluidity of the blood found in death by suffocation, however produced. This condition is sometimes present in deaths due to certain diseases, fevers, &c., and in cases of narcotic poisoning. Even with the blood in this condition, the presence of coagula in the cavities of the heart is not infrequent. The colour of the blood is changed to a dark purple, but in suffocation by carbon monoxide it is red.
2. Animal Heat.—In persons who have died from suffocation the animal heat is long retained.
3. Cadaveric Rigidity.—Other things being equal, the rigor mortis is as well marked in this kind as in other forms of death.
4. The Lungs.—Hyperæmia of the lungs is rarely absent. In most cases both lungs are engorged in about equal proportions. Hypostasis—post-mortem stains—must not be mistaken for capillary engorgement.
5. The Heart.—Engorgement of the right side of the heart, the left being empty, or nearly so. It is advisable always to examine the heart first, and then the lungs. The pulmonary artery is also much congested.
6. Capillary Ecchymoses.—These appear as purplish-red spots on the pulmonary pleuræ, on the surface of the heart, aorta, in the thymus, and on the diaphragm. They may appear on the above-mentioned parts in a fœtus suffocated in utero by pressure on the cord. These ecchymoses are rarely seen on adults, most frequently on infants, due probably to the thinness of the coats of the capillaries, which are ruptured in the efforts made to breathe. They are not a positive sign of death from suffocation, as they have been seen in death due to cholera, typhus, and other diseases. They are present also where death is due to hanging, drowning, &c.
7. Condition and Appearance of the Trachea.—The mucous membrane of the trachea is injected, and appears of a cinnabar-red colour. This is present in every case of death by suffocation, and must not be confounded with the dirty cherry-red or brownish-red coloration due to putrefaction. Remember also that the trachea putrefies early. If suffocation be slowly produced, a quantity of frothy mucus may be found in the windpipe, and also in the smaller tubes of the lungs. Always examine, especially in cases of supposed infanticide, the trachea for foreign bodies, the presence of soot, &c. The presence of sand, ashes, &c., in the œsophagus and stomach in persons buried in these materials, is presumptive of the person having been placed in them prior to death.
8. Kidneys, Vena Cava, &c.—The quantity of blood in the kidneys is always considerable. The abdominal veins are all more or less congested, and the external surface of the intestines presents numerous traces of venous congestion.
9. The Brain.—Apoplexy of the brain, as secondary to the pulmonary apoplexy, may be more or less present, attended by its well-known appearances.
10. Face, Tongue, and Mouth.—The expression of the face is not characteristic of death by suffocation, and differs in no particular from that common to other forms of death, being more frequently pale than turgid; and the starting of the eyes, popularly ascribed to this form of death, is not often seen. The tongue may or may not be protruded beyond the teeth. The presence of froth about the mouth is not constant, and is of common occurrence in those dying from natural causes. The tympanum may be ruptured. [Pg 120]
Was the suffocation homicidal, suicidal, or accidental?—Suffocation may occur accidentally during the act of swallowing, and by foreign bodies placed carelessly in the mouth and then drawn suddenly into the windpipe, or by blocking the pharynx or œsophagus, also from being smothered by sinking into sand, grain, mud, and such-like, or by the bed-clothes in cases of epilepsy during a fit. Examine the lips for the presence of ecchymosis and other marks of violence. A man, some years ago, was accused of having caused the death of his wife by strangulation, for which he was indicted, and tried before the High Court of Justiciary in Scotland. The post-mortem examination revealed the cause of death as due to suffocation, and the following injuries were found on dividing the windpipe, which contained a quantity of frothy mucus: in the interior of the larynx there was a considerable extravasation of blood lying beneath the investing membrane, and passing up on both sides and behind, as far as the chink of the glottis, and above that opening into the ventricles of the larynx. There was here, also, a fracture of the right wing of the thyroid cartilage, by which its lowest horn was wholly detached, and the cricoid cartilage was broken in two places at opposite sides of its ring. The defence was that she had fallen accidentally while in a state of drunkenness, and had thus produced the fatal injuries.
The man was acquitted, the legal opinion in favour outweighing the medical opinion against the theory of accident. The above case created some discussion at the time, and induced Dr. Keiller to make several experiments as to the possibility of fracturing the cartilages of the larynx. The following are his conclusions:
1. That ordinary falls on the human larynx are apparently not capable of producing fractures of its cartilages, and even falls from a height with superadded force appear to be unlikely to do so.
2. That severe pressure applied from before backwards, so as strongly to compress the larynx against the vertebral column, or violent blows inflicted over the larynx by means of a heavy body, are sufficient to cause fractures of the larynx. Fractures so produced, however, will be most discernible on the internal surface, and generally in or near the mesial line.
3. Violent compression applied to the sides of the larynx (as in ordinary manual throttling or strangulation by grasping), is, of all applied forces, the most likely to produce fractures of the alæ of the thyroid cartilage, or even of the cricoid cartilage, and fractures so produced are most perceptible, as well as most extensive, on the external surface of the larynx. By this lateral mode of applying force, the hyoid bone is almost most readily broken.
4. That the condition of the larynx in regard to the absence or presence of ossific deposit materially influences its liability to fracture from external violence. If altogether cartilaginous, partial slits or splittings may be produced. If partly ossified, fractures may be produced by a comparatively moderate degree of applied violence, and if extensively or entirely ossified, extreme violence will generally be required to produce laryngeal fracture (Edinburgh Medical Journal, 1855-56).
Homicidal suffocation may be due to forcibly introducing foreign bodies into the air-passages, especially in children; adults suffocated thus are generally under the influence of alcohol or drugs, or enfeebled from disease. Suicidal suffocation by these means is generally limited to lunatics.
Fig. 16.—The pulse in this case became slower than normal. Five minutes after the drop the type reached that of bradycardia, then recovered itself, and even 14½ minutes after the drop was beating with normal frequency, but in the meantime had become very feeble.
Fig. 17.—The pulse in this case became accelerated and then fell again, but was feeble throughout.
Fig. 18.—In this case the pulse rate increased, and then fell to 72 per minute towards the end.
[Pg 121] Homicidal suffocation by compression of the chest has been effected in infants; in adults it is combined with the covering of the nose and mouth. The victims are generally old or enfeebled. Suffocation of infants may be homicidal, or accidental, due to “overlaying”; in the latter the greatest mortality is amongst the youngest infants. A child ten months old may struggle and free itself or awaken the mother.
In France a favourite mode of committing suicide by suffocation is the use of irrespirable gases—carbonic acid, carbon monoxide, and the like. Collateral circumstances must be taken into consideration, and will more or less help to point to the true cause of death.
The cause and nature of the death in all of its forms just mentioned are in general the same. Pressure on the trachea—thus arresting respiration—and also on the important vessels and nerves of the neck, results in death, which may be brought about in four different ways:
The following table will show the relative frequency of each form of death:
| Remer. | Casper. | ||
| Apoplexy | 9 | 9 | |
| Asphyxia | 6 | 14 | |
| Mixed | 68 | 62 | |
| 83 | 85 |
Traumatic asphyxia occurs when a heavy weight such as a fall of earth or masonry compresses the chest, and thoracic respiration is impossible. The head and neck appear ecchymosed, the purplish-blue lividity generally ending abruptly at the lower part of the neck or upper part of the thorax, about the level of the clavicles. The conjunctivæ are ecchymosed, and there may be epistaxis. This discoloration does not disappear on pressure by the finger, indicating its petechial character. If the person survive long enough, the discoloration gradually disappears, passing through the colour changes of an ordinary ecchymosis.
The effects on the eyes may be such as to be followed by changes in the retina, and optic atrophy leading to loss of vision.
Parts of the neck pressed upon by clothing may escape ecchymosis, and present a white mark of almost normal skin.
Death by hanging is caused by the more or less perfect suspension of the body by a cord applied around the neck, the weight of the body acting as the constricting force.
The body need not hang completely, partial suspension is sufficient to [Pg 122] cause death. The ligature surrounds the neck above the thyroid cartilage, the epiglottis is pushed against the back of the pharynx, the base of the tongue and the soft parts are pressed into the cavity of the pharynx, so that the obliteration of the naso-pharyngeal and the laryngeal passages is complete. Death is due to asphyxia and pressure on the cervical blood-vessels, even if the air-passages be not completely occluded; stoppage of the cerebral circulation being sufficient to cause death; in such a case the signs of asphyxia are absent.
Consciousness is quickly lost, due to pressure on the vessels, and, for this reason, in accidental or suicidal hanging the person is prevented from making any effort to save himself.
Post-mortem Appearances.—The external appearances are more or less those described under “Death from suffocation.” In the greater number of cases the face bears a quiet, placid expression, no turgidity or lividity being noticeable. The eyes are usually half open, but not protruded, and the condition of the pupils variable. The tongue may be protruded, but just as often not. The face may be pale or livid, and a bluish colour present on the free border of the lips. Cyanosis and swelling of the face are only present when the death agony has been long; they soon disappear.
Ecchymosis of the conjunctiva, and on the outer surfaces of the lids may be present. The escape of urine, fæces, and semen may take place, but are not characteristic, and are extremely rare.
Casper states that in not one of the many cases he had examined of persons hanged has he ever “found an erection of the male organ,” and he also asserts that the emission of semen is extremely rare. Seminal emissions take place more frequently in persons who have been shot, and also in those who have been poisoned by irrespirable gases or by hydrocyanic acid. As a test of strangulation, it is therefore worthless. Tardieu, however, only noticed the escape of urine and fæces in two out of forty-one cases; it is by no means a test of hanging, as it may occur after death if the body is shaken in a cart, or roughly used when first found. A fat person dying of apoplexy may have a mark round the neck as if strangled. Injury to the spinal cord due to fracture or dislocation of the cervical vertebræ is rare in suicidal hanging. Fracture of the spinal ligaments and of the hyoid bone is also rare. Rupture of the internal and middle coats of the carotid arteries sometimes occurs. But it appears that considerable damage is done to the soft parts of the neck by the present judicial mode of hanging with the “long drop.”
Dr. Dyer has recorded (New York Medical Journal, vol. iii., 1866) some experiments he made on the eyes of a man and some dogs killed by hanging. He found certain transverse fissures across the lens, which he is inclined to think are characteristic of this mode of death. Dr. R. F. Hutchinson states that an invariable sign of death from hanging is the flow of saliva out of the mouth, down the chin, and straight down the chest. The appearance is unmistakable and invariable, and could not occur in a body hung up after death, the secretion of saliva being a living act (Chevers). Death from hanging may take place although the toes or other parts of the body [Pg 123] rest on the ground. Death is complete in four or five minutes.
Marks of the Cord, &c.—The mark of the cord is nearly always present. It varies with the breadth and hardness of the ligature, but is often interrupted. Its irregularities are reproduced on the skin. It is sometimes only seen on one side. In strangling, the mark is low down, most frequently encircling the neck; in hanging, the mark is generally above or on the thyroid cartilage, and carried obliquely upwards. The mark of the cord may be of a dirty yellowish-brown colour, and, when cut into, feels more or less hard and leathery. In general appearance it is not unlike the mark left by mustard-plasters or blisters applied within a short time of death. This effect is probably produced by the rubbing off of the epidermis, and subsequent drying up of the cutis on exposure to the air. At other times the mark may be of a dirty reddish or bright blue colour; or, lastly, there may be little or no mark present, or the edges may assume a livid red coloration, being nothing more or less than a post-mortem stain.
May the mark of the cord be produced after death?—On this point Casper says: “That any ligature with which any body may be suspended or strangled, not only within a few hours, but even days after death, especially if the body be forcibly pulled downwards, may produce a mark precisely similar to that which is observed in most of those hanged while alive.” And the same authority also adds that “the mark of the cord is a purely cadaveric phenomenon.”
Accidental hanging is rare, and generally happens with children while playing at hanging, or by accidentally becoming entangled in a window-blind cord or swing rope, or by the neck-band of an article of clothing by which they may become accidentally suspended from the spike of a railing.
Homicidal hanging is rare, but the body may be suspended after death from violence, to simulate suicide; and it may have to be decided whether the hanging took place during life or after death.
The mark of the cord is of no assistance, rents in the carotids with extravasation into the coats of the vessels indicate ante-mortem suspension. The flow of saliva down the chin to the body indicates suspension before death. It is important to examine the body for injuries which could not be self-inflicted, and to remember the possibility of poison having been administered with suspension after death.
Suicidal hanging is the most common, as it is a favourite mode of death with suicides. The absence of marks of injury on the body found suspended, and the want of evidence as to a previous struggle having taken place, all point to suicide. The fact that the feet are found in contact with the ground does not militate against the probability of suicidal hanging; and it appears that in India the natives seldom hang themselves from any height, and are most frequently found with their feet on the ground. A person may take poison first, and hang himself before the poison has had time to prove fatal. [Pg 124]
Death is due to pressure made on the neck by any form of ligature carried circularly round the neck, without suspension. The cord in hanging is, as a rule, placed more obliquely than in strangling.
The mode of death is the same as in hanging. The post-mortem appearances are similar to those of hanging, practically those of asphyxia. The mark on the neck is the principal feature. In position it is generally horizontal and situated below or on a level with the thyroid cartilage. It more completely encircles the neck. It may be interrupted in places if an irregular ligature has been used, causing irregular pressure. Its character depends largely upon the nature of the ligature. If the constriction has been uniform a continuous depression is produced which may be marked by ecchymosis. If the skin has been abraded, the line dries, and has a brownish, parchment-like appearance and feeling. If the ligature has been removed before life is quite extinct, the depressed line may disappear or be but slightly evident.
A soft, broad ligature may leave no mark on the neck, if not applied too tightly, or for too long a time. Should the victim have been strangled in the recumbent posture, and dragged upwards and backwards by the ligature, the mark will be on a slant as in hanging. According to the amount of violence used injuries may be caused to the deeper structures of the neck, such as effusion of blood into muscles, fractures of the thyroid or cricoid cartilage; rupture of the tympanum and epistaxis may take place.
Accidental strangulation may occur when a cord suspending a weight on the back and passing across the chest slips and encircles or compresses the neck.
Falling out of bed, with entanglement in the clothes or nightdress, may cause strangling by tightening of the neck-band round the neck.
Homicidal strangling is as common as homicidal hanging is rare. It is difficult to hang a man, but easy to strangle him, because consciousness is rapidly lost, and the victim is unable to offer any resistance once the cord is tightened round the neck. In homicidal strangling the murderer generally uses a great deal more violence than is necessary, and so there is found after death much more local injury in such cases.
Severe local injuries, such as fracture of the laryngeal cartilages or hyoid bone, denote homicide, as they are rarely noticed in suicidal strangulation.
There may also be signs of general violence about the face, neck, chest, or other parts of the body. The position of the knot affords no material help, as the murderer may tie it in any position, but more than one knot, especially if in different positions, points to homicide. It must be remembered that finger-nails or other marks in the vicinity of the ligature may be present in cases of suicides, from the slipping of the cord or the determined attempts of the suicide to carry [Pg 125] out the act, or plucking at the cord involuntarily. When a person is first strangled, then hung, there would be two marks—one probably horizontal, the other slanting.
Suicidal strangulation is rare. The knot is generally adjusted at the front or side of the neck, the cord may encircle the neck several times. Injuries to the deep structures of the neck are absent. Signs of general violence are not necessarily present.
If there be two marks upon the neck, one due to an attempt at strangulation, the other to suspension, in a suicide, the first would be the less marked, the latter more pronounced, whereas in homicide the strangulation mark would be most distinct.
Throttling is strangling by means of the hand or hands alone, and is due to constant pressure of the fingers upon the throat. Very little pressure is required to occlude the glottis; it can be done with slight pressure of the thumb and forefinger on the side of the thyroid cartilage.
The impression of the fingers and thumb upon the throat have characteristic marks. They are usually to be seen on both sides of the throat. The thumb mark is on one side, and the marks of the fingers, separated from one another or clustered together, are on the other, the thumb mark being the highest. When grasped from the front by the right hand, the thumb mark will be on the right side of the throat. If the victim be throttled by the two hands at the same time, as when on the ground, the thumb marks are on the same side. If the assailant be left-handed, and has used this hand to grip the throat, the thumb mark will be on the left side of the victim. The finger marks are one above the other. The marks may appear as ecchymoses if the examination be made soon after death; if later, they may appear and feel like parchment, and of a brownish colour. Crescentic marks of finger-nails may be present, also other scratches in the vicinity. Other marks of general violence may be present, and should the victim have fallen to the ground, the head may be injured. Much blood is effused in the tissues of the neck and the laryngeal cartilages, and the hyoid may be found fractured; the carotids may escape injury, but not always.
The mucous membrane of the cheeks may be found lacerated. Where the victim is thrown to the ground and knelt upon, fracture of the ribs and ecchymosis of the chest wall may occur.
In a case examined by me of combined strangling and throttling, marks of the ligature and fingers were both present, and on the clavicles separate marks produced by the knuckles while tying the cord. These knuckle marks did not show up till some time after death. Effusions of blood were present in the tissues of the neck on each side of the larynx, and amongst the muscles on both sides, and in the sheath of the left carotid artery.
The hyoid bone was fractured in two places in its left half. The thyroid cartilage was fractured vertically on each side of the middle [Pg 126] line into three pieces, the central portion having fallen behind the other two into the cavity of the larynx. The right wing of the thyroid was comminuted. The cornua were fractured. The cricoid cartilage was also fractured posteriorly, and into three pieces in front. Effusions of blood in the fractured areas had formed beneath the mucous membrane. Effusion of blood was present on the front wall of the pharynx and the upper part of the œsophagus. The right carotid artery was atheromatous, and linear and star-shaped fissures were present, the latter surrounded by a ring of sub-intimal effusion of blood.
On the right side of the thorax the fifth rib was fractured at the junction with its cartilage, and on the left side the second, third, fourth, fifth, and sixth ribs were fractured close to their cartilages, and again from three to five inches further back. Blood effusions in the tissues of the chest wall and under the pleuræ were present in the region of the fractures.
A handkerchief was found tight on the neck and tied with two knots both fastened securely. It was probable that the handkerchief had been tied on after the throttling, as the knot ends were too short to allow a sufficient pull on them to cause the injuries. Throttling may be regarded as a homicidal act; although one or two instances of suicidal throttling have been recorded in the insane.
Judicial Hanging.—In judicial hanging the prisoner is suspended by a rope with a running noose around the neck, after a sudden drop of from six to eight feet according to the weight of the body. The noose may be arranged with the knot or slip-ring fixed at the side below the ear, or in front so as to jerk the head backwards. The sudden and severe strain upon the neck produces fracture or dislocation of the spinal column at the second or third cervical vertebra, with rupture of the spinal cord. Other local injuries occur, such as rupture of cervical muscles, fracture of the larynx, and even lacerated wounds of the neck. The head has even been severed completely from the body, and the deep structures of the neck have even been so lacerated that the body has hung by skin only, stretched to the thickness of two or three fingers. Death is said to take place from shock, pressure on the vagi, and asphyxia, probably also cerebral apoplexy. When death is instantaneous, the body hangs motionless, the head fallen over the side opposite the knot, and the neck stretched.
The heart may, however, continue to beat for a varying period after apparent death—in some cases even as long as 14½ minutes. The following interesting series of pulse tracings were taken by Dr. Llewellyn Morgan, of Liverpool, and kindly placed at my disposal. In No. 1 the heart beats could be recorded at the wrist for 14½ minutes after the drop; in No. 2 for 12½ minutes; and in No. 3 for 12 minutes. The frequency and character of the beat is variable, but in each case shows a practically normal rate towards the end. (See Figs. 16, 17, 18.)
Apart from the local injuries to the neck, the external appearances in judicial hanging are similar to those in other forms.
Death by drowning occurs when the breathing is arrested by watery or semi-fluid substances, blood, urine, or the muddy semi-fluid matter found in cesspools and marshes. It is not necessary for the whole body to be submerged. Death may result if the face alone be immersed, as in the case of a man in a fit of drunkenness being drowned in the water contained in the imprint of a horse‘s hoof left in the mud.
In addition to the changes in the internal organs, identical with those present in persons who have died from suffocation or hanging, water is found in the lungs or stomach.
Death may be due to—
Death from pure apoplexy is rare; and it may be affirmed that death from syncope never occurs in the drowned without leaving some signs of asphyxia.
It is more difficult to restore the drowned than those dying from mere stoppage of air from entering the lungs. Few if any persons recover who have been submerged four minutes, and even in cases where this time has been exceeded, followed by recovery, this result is probably due to the person fainting before entering the water.
In death from drowning, the lungs are distended and overlap the heart, and have a peculiar spongy feeling. They also contain a quantity of frothy fluid, which cannot be produced in the dead body, as it is the result of the violent efforts made by the individual to breathe in the act of dying. This frothy condition of the fluid in the lungs is an important sign of death by drowning, especially if the fluid corresponds with that in which the individual is said to have perished. It is just possible, however, that the person may have been first suffocated, and then thrown into the water, froth in the trachea being found in those suffocated; but in this case the froth is small in quantity, and not watery. The froth in the drowned is like that made with soap and water, and is not viscid, thus differing from bronchitic exudation. Water in the stomach is an important indication of death from drowning, especially if the water contained in the stomach can be shown to possess the same characters as that in which the body was found. Water in the intestines is still more important. In a great number of cases this, however, must be next to impossible; when it can [Pg 128] be identified, the value of this sign is enhanced by the fact that water does not enter the stomach in those submerged after death, unless putrefaction be far advanced, or the body has lain in very deep water. Casper concluded that a person had been drowned, by finding a small quantity of mud in the stomach after putrefaction had set in. Water, however, may be absent from the stomach if the person fall into the water in a state of syncope, and it may be present if the person has taken a draught of water before submersion.
The effect of season on putrefaction in water is shown in the following table:
| Summer. | Winter. | ||||
| 5 to 8 | hours | produce | as much change | as 3 to 5 | days. |
| 24 | “ | “ | “ | 4 to 8 | “ |
| 4 | days | “ | “ | 15 | “ |
| 10 to 12 | “ | “ | “ | 28 to 42 | “ |
| (Devergie.) | |||||
Of the external signs, the presence of sand, gravel, or mud under the nails may or may not be an important sign, for sand or mud may collect under the nails during the efforts to drag the body from the water; but weeds, &c., grasped in the hands show that there has been a struggle, and point to death from drowning. The cutis anserina—goose skin—present generally on the anterior surface of the body, and not, however, peculiar to death from drowning, is important as a sign of recent vitality. The face of those who have been drowned, and then quickly removed from the water, is pale, and in most cases not swollen; the eyes may or may not be closed; and not infrequently round the mouth there is more or less froth, especially when death is due to apnœa. In summer, however, after two or three days, and longer in winter, the face assumes a reddish or bluish-red coloration, putrefaction taking place about the head and upper extremities earlier than in other forms of death. The contraction or retraction of the penis is a well-marked sign of death by drowning, and Casper asserts that he has “not observed anything similar so constantly after any other kind of death.” Ogston states that he has met with two cases of erection of the penis in the drowned.
The question as to how long a body may remain in the water before it floats has given rise to considerable discussion, without, however, arriving at any very definite conclusion. It may be stated in general terms that, as floating depends to some extent on the rapidity in which putrefaction supervenes on submersion, bodies float earlier in summer than in winter, in salt than fresh water, clothed than naked. In India bodies have floated in twenty-four hours after immersion. Females and children float more readily than males. A body from various causes may float within a few hours of its submersion, especially if the body be that of a female, fat and clothed. The old idea that the body of a person thrown into water during life sinks, but that a dead body under like conditions floats, is a fiction now exploded.
Suicide or Homicide?—Homicide by drowning is rare, except in children. Accidental and suicidal drowning are common enough. [Pg 129]
The signs to be sought for in the drowned are—(1) Absence of any injury. (2) Cutis anserina and retracted penis. (3) Water and mud in the stomach. (4) Froth in the air-passages. (5) Distended lungs. (6) General signs of death by asphyxia.
It should be remembered that the fact of the hands being tied together, or to the feet, does not militate against suicide by drowning.
If wounds and other injuries be found on the body, the question arises as to whether the injuries were sufficient in themselves to cause death, and then as to whether they were caused during life. A person jumping from a height into the water may sustain severe injuries—dislocation of both arms, fracture of the skull and of the vertebræ, or even lacerated wounds of more or less severity. The absence of the signs proper to death by drowning, coupled with the presence of external injuries, would point to death by violence prior to immersion. The presence of signs of drowning, and injuries, sufficient to have caused death in themselves, would indicate that they had occurred after death.
The following considerations may assist in forming an opinion:
The time required to cause death by drowning is so short that persons seldom recover after submersion for three or four minutes; but the cessation of respiration is no guide to the extinction of life, and an attempt at resuscitation should always be made, for if the respiration be fairly restored the heart will soon act. Nay more, as pointed out before, in cases of so-called asphyxia, the heart may continue to act for several minutes after the entrance of air to the lungs has been arrested, and in judicial hanging it frequently happens that the pulse at the wrist can be felt for ten or twelve minutes after suspension. (See Figs. 16, 17, 18.)
1. In the Skin.—Rose-coloured patches may be present on the face and neck. The condition of goose skin—cutis anserina—is hardly ever absent even in summer. The cutis anserina is not, however, characteristic of drowning, as it may be present in other forms of violent death, and also in some persons during life. It is a vital act, the result of nervous shock, and does not depend upon the temperature of the water for its production; still, it points to recent vitality.
2. The Tongue.—The tongue is just as often found behind the jaws as between them (Casper).
3. The Hands and Feet.—The hands and feet acquire a greyish-blue colour when the body has lain in the water from twelve to twenty-four hours. The skin also becomes corrugated in longitudinal [Pg 130] folds. The greyish-blue condition of the hand is known as the “cholera hand.” The nails may contain particles of sand and weeds. “No corrugation or discoloration of the skin of the hands or feet is ever observed on the body of anyone drowned who has been taken out of the water within half an hour, within two, six, or even eight hours” (Casper). The same authority states he has produced these effects by laying the hands after death in water, or wrapping them in cloths kept constantly wet for a few days.
4. The Genitals.—Contraction of the penis and dartos is an almost constant symptom, and Casper has “not observed anything similar so constantly after any other kind of death.” It is due, probably, to the same cause as the cutis anserina, which Brettner attributes to “bundles of unstriped muscular fibres, lying in the upper stratum of the true skin, surrounding the sebaceous glands, and forcing them forwards by their contraction, thus making the cutis anserina. Precisely similar unstriped muscles are found in the subcutaneous cellular tissue of the penis; they run principally parallel to the long axis of the member, but very often large bundles run across it.” The action of cold and fright is to induce contraction of these cutaneous muscles, with a resulting contraction of the penis.
1. The Brain.—Cerebral hyperæmia is most rare in the drowned, but cerebral hypostasis is not infrequently mistaken for it.
2. The Trachea.—The mucous membrane of the trachea and larynx is always more or less injected, and is of a cinnabar-red, which must not be mistaken for the dirty, brownish-red colour, the result of putrefaction. A white froth, but seldom bloody, is also found in varying quantity in the trachea, and is a most important sign of vital reaction, but its diagnostic value is destroyed by putrefaction. Sometimes a portion of the contents of the stomach may be found in the trachea. When this occurs it is due to the act of coughing, induced by the admission of water into the lungs. The contents of the stomach are forced into the mouth, and then drawn into the lungs during the next attempt at inspiration. This indicates that the person entered the water during life. In cases where death has taken place from syncope little or no froth may be found in the trachea.
3. The Lungs.—The lungs are completely distended, almost entirely overlapping the heart, and pressing close to the ribs. They are spongy to the feel, and when cut into, a considerable quantity of bloody froth escapes. The froth found in the lungs is the result of the powerful attempts to breathe, and cannot be produced by artificial means. It adheres not to the sides of the bronchial tubes, as does the exudation of bronchitis or pneumonia. The distension of the lungs is due partly to an actual hyperæmia, and partly to inhaled fluid. Water is present in the pleural cavities.
4. The Heart and Great Vessels.—As is common to other forms of asphyxia, the left side of the heart is entirely, or almost entirely, empty; the right, on the contrary, is engorged. This condition of the heart is, therefore, not a diagnostic sign of drowning, and is absent in the drowned when death takes place by neuro-paralysis; in fact, in some cases of undoubted drowning, both sides have been found empty, probably, however, the result of putrefaction (Ogston). The same may be said of the accompanying congestion of the pulmonary artery.
5. The Blood.—As is common in all forms of death where respiration has been arrested, the blood is found to be remarkably fluid, and of a cherry-juice colour. M. Faure in his monograph on asphyxia states that he has found large and firm clots in the right side of the heart in the drowned who have not remained long under water. The blood is diluted with water, most marked in the left side of the heart. The amount of dilution is greater in slow drowning. [Pg 131]
6. The Stomach.—Casper considers that the presence of fluid in the stomach, corresponding to that in which the body is found, is “an irrefragable proof of the actual occurrence of death from drowning,” and that the swallowing of it must have been a vital act of the individual dying in the water. The absence of water from the stomach does not negative death from drowning. Water is not always present. It is possible for it to reach the stomach of a submerged body after death.
Water in the intestines is a more reliable sign of death from drowning, and indicates submersion during life. It is only after very long submersion and under great pressure that water finds its way into the intestines after death.
N.B.—Putrefaction in the drowned in most cases commences in the upper part of the body, and extends downwards. The face, head, and neck are first attacked. This is the reverse of putrefaction in air.
Death from starvation may be due to the total withdrawal of food, to prolonged insufficiency, defective quality, inability to swallow it, and inability to retain it.
Death from starvation may occur during famines, amongst ship-wrecked sailors, and persons entombed in mines or pits, and is due to sheer privation. It may follow criminal starvation, wilful refusal to take food as a form of suicide, and it has been noted in cases of hysteria and lunacy.
It may result from mechanical hindrance to the entrance of food into the body from ankylosis of the jaws, or its passage through the alimentary tract from stricture of the œsophagus or stomach, from cancer or cicatrisation after injury from swallowing corrosive substances. Amongst other diseases, tuberculosis, malignant disease, and diabetes mellitus are the chief which produce external appearances of starvation.
In the withdrawal or deprivation of food for criminal purposes the victims are usually old, helpless, or feeble-minded persons, or young children.
Symptoms.—These depend on the previous state of nutrition. Starvation may be regarded as acute when death occurs within fourteen days from the withdrawal of food, chronic when at a longer period.
The symptoms of hunger vary: they are said to pass off in forty-eight hours, but may last for several days acutely.
The body temperature falls below normal, and the fall may be two or three degrees before death. The pulse gradually increases in frequency day by day. The chief sign is loss of body weight. Chossat‘s experiments on pigeons showed that when they were totally deprived of food, the surplus fat of the body was lost first, then the fatty coverings of internal organs, the interstitial fat of muscles last of all; the muscles themselves also wasted. A peculiar odour like acetone emanates from those who have been starved, and towards and after death the odour is putrescent.
In addition to the above signs, there are anæmia, sunken, glistening eyes with dilated pupils, prominence of bony projections, pale and dry lips and tongue, parched mouth and throat, weakness of the voice, [Pg 133] sunken abdomen, wasted limbs, constipated bowels, urine scanty and turbid. There are pains in the abdomen, relieved by pressure; great thirst, a dusky, dry skin, occasionally purpuric eruptions, exhaustion, ultimately delirium ending in death.
Post-mortem Appearances.—There is emaciation of the whole body, dry, wrinkled skin of a brown colour; the muscles are flabby and wasted, the abdomen sunken, the eyes red and open; this appearance is not common in death from other causes. The mouth and throat are dry even to aridity. The heart, lungs, and blood-vessels are collapsed, and contain but little blood. The abdominal viscera are shrunken and without enveloping fat. The omentum is devoid of fat, and clear; the gall bladder is full of dark bile; the urinary bladder may be quite empty. The stomach and intestines are collapsed, contracted, and empty, and the walls extremely thinned.
Diagnosis.—The absence of any other cause of death—such as cancer of the stomach, stricture of the œsophagus, &c.—and the previous history of the case will assist in forming an opinion, care being taken not to confound the results of wasting disease with those due to starvation.
Legal Relations.—The question of death from starvation may be raised in a case of infanticide by omission. Although rare as an act of homicide, it must be remembered that the law does not require the absolute deprivation of food to be proved, but only that the necessary quantity and quality of food has been withheld; but malice at the same time must be proved. In cases of infanticide by starvation, the mother and not the father is responsible for the proper feeding of the child; but in the case of an apprentice, the master and not his wife is bound to supply proper food to such apprentice.
In questions of survivorship, and in criminal cases, the medical witness may be asked how long a person may survive after complete withdrawal of food. Little is known as to the length of time required to cause death by starvation, but it is certain that life may be prolonged for some time without food, if water be allowed. Starvation is less rapid in its effects if the body be kept warm. In a case recorded in the Lancet, a man who had been shut up in a coal-mine for twenty-three days, with only a little dirty water to drink, lived three days after his liberation, and then died of exhaustion. In adults the average is from seven to ten days without water. Tidy (Legal Medicine, vol. i. p. 392) is of the opinion that the young die first, then adults, and the aged last. Taking into account the enfeebled vitality of the aged, it is more probable that the young or middle-aged adult would survive the longest. Where water is freely obtainable, life may be prolonged to the fifty-eighth day (Foderé, vol. ii. p. 276) or even more.
Apart from age, account must be taken of the condition of the person in reference to bodily health prior to the withdrawal of food.
The following tables, showing the average weight and height of children up to twelve years of age, are from the Report of the British Anthropometric Committee (1883): [Pg 134]
Male Children
| Age. | Weight in Pounds. |
|
|---|---|---|
| At birth | 6.8 | |
| One month | 7.4 | |
| Two | months | 8.4 |
| Three | “ | 9.6 |
| Four | “ | 10.8 |
| Five | “ | 11.8 |
| Six | “ | 12.4 |
| Seven | “ | 13.4 |
| Eight | “ | 14.4 |
| Nine | “ | 15.8 |
| Ten | “ | 16.8 |
| Eleven | “ | 17.8 |
| Twelve | “ | 18.8 |
| Age. | Height in Inches. | Weight in Pounds. | |||
|---|---|---|---|---|---|
| Female. | Male. | Female. | Male. | ||
| One | year | 27.5 | 33.50 | .... | 18.8 |
| Two | years | 32.33 | 33.70 | 25.3 | 32.5 |
| Three | “ | 36.23 | 36.82 | 31.6 | 34.0 |
| Four | “ | 38.26 | 38.46 | 36.1 | 37.3 |
| Five | “ | 40.55 | 41.03 | 39.2 | 39.9 |
| Six | “ | 42.88 | 44.00 | 41.7 | 44.4 |
| Seven | “ | 44.45 | 45.97 | 47.5 | 49.7 |
| Eight | “ | 46.60 | 47.05 | 52.1 | 54.9 |
| Nine | “ | 48.73 | 49.70 | 55.5 | 60.4 |
| Ten | “ | 51.05 | 51.84 | 62.0 | 67.5 |
| Eleven | “ | 53.10 | 53.50 | 68.1 | 72.0 |
| Twelve | “ | 55.66 | 54.59 | 76.4 | 76.7 |
Table of Ages, Heights, and Weights
of Males and Females from
13 to 30-35 Years of Age
Recapitulation of the Post-mortem Appearances
of Death by Starvation
1. In the Body generally.—Marked general emaciation of the body. The skin is dry and shrivelled, sometimes more or less covered with unhealthy-looking pimples, the muscles soft, reduced in size, and free from fat. A peculiar fœtid acrid odour is given off from the body.
2. In the Solid Viscera of the Thorax and Abdomen.—The liver is small, the gall-bladder distended with bile, and the heart and kidneys deprived of any surrounding fat. All the internal organs are shrivelled and bloodless.
3. In the Stomach and Intestines.—The stomach in some cases is quite healthy, but more or less stained with bile; in others it is found collapsed, contracted, empty, and the mucous membrane more or less ulcerated. The intestines are thin, contracted, empty, and so shrunken that the canal is almost obliterated. According to the late Dr. Duncan, the intestines are frequently found inflamed and ulcerated.
This form of death is rare in England, but is more common in countries where the winters are severe. Anything that depresses the vital powers renders the individual more or less susceptible to cold; such, for instance, as drunkenness, previous illness, or deficiency in the amount of food. The following post-mortem appearances are given by Ogston, who holds that they point, in the absence of any other obvious cause of death, “if not with absolute certainty, yet with high probability,” to death caused by cold:
1. An arterial hue of the blood generally, except when viewed in mass within the heart; the presence of this coloration not having been noted in two instances.
2. An unusual accumulation of blood, as in Quelmalz and Cappel‘s cases, on both sides of the heart, and in the larger blood-vessels of the chest, arterial and venous.
3. Pallor of the general surface of the body, and anæmia of the viscera most largely supplied with blood. The only exceptions to this were moderate congestion of the brain in three cases, and of the liver in seven of them.
4. Irregular and diffused dusky-red patches—“frost erythems”—on limited portions of the exterior of the bodies, encountered in non-dependent parts, these patches contrasting forcibly with the pallor of the skin and general surface.
These signs are not so well marked in children as in adults. The late Sir Benjamin Brodie considered that the effect of cold is to destroy the principle of vitality equally in every part, and that it does not exclusively disturb the functions of any particular organ. The fact of a body being found frozen is no proof that death has been brought about by cold.
Symptoms.—Exposure to severe cold produces loss of energy, lethargy, followed by drowsiness, with an intense desire to sleep, which, if gratified, passes on to stupor and coma. There may be delusions before the coma. The primary cause of death is attributed to the lessened dissociation of oxygen from the hæmoglobin to the tissues, and a lessened power of the latter to utilise it. [Pg 136]
Diagnosis.—The general appearance of the deceased, and the absence of any other cause of death, together with the appearances just mentioned, will assist in forming an opinion on this difficult subject. The body lies as if in a deep and calm, sleep, without any external appearance to guide us as to the cause of death, except perhaps a swelling of the extremities, which has come on prior to death. If a body be found buried in snow, and putrefaction present, death did not in all probability take place from cold, provided that the cold has been severe and continuous. Death from cold is generally accidental, except in newly-born children, when it may be either accidental or homicidal, according to circumstances.
When freezing of the body has taken place prior to the onset of rigor mortis, the latter comes on after the body thaws. This, combined with the other post-mortem signs given above, affords evidence of the strong probability that death had resulted from exposure to cold. In view of the red colour of the skin being similar to that caused by poisoning with CO, a spectroscopic examination of the blood should be made.
The results from exposure to excessive heat manifest themselves in various ways. Any condition which may lessen the resistance of the body to external heat predisposes to heat-stroke; such as privation, fatigue, mental emotions, alcohol, over-eating, and especially previous attacks of the disease.
Sunstroke occurs in those who work under the direct rays of the sun, when the air is hot, still, and humid.
Heat-stroke or thermic fever affects those working in places which are excessively hot and confined, as in glass-works, foundries, stoke-holds, boiler-houses, sugar-refineries, paper-mills, &c.
Heat exhaustion and prostration are brought about in a similar manner, but the effects are not the same, and usually transient and less severe.
Sunstroke or heat-stroke may occur in two forms, the asphyxial or apoplectic, and the hyperpyrexial; it is also classified as sthenic or asphyxial, and asthenic or syncopal.
Asphyxial sunstroke or heat apoplexy is probably the least frequent; prodromal symptoms are headache, vertigo, disturbances of vision, dyspnœa, and dry skin. In some cases sudden unconsciousness, with or without convulsions, may occur, and death rapidly follows.
The coma may not be profound; there may be nausea and vomiting of dark material, bounding pulse, stertorous breathing, contracted pupils, and frequent micturition. The body exhales a “mousey odour.” There may be involuntary dejection, with the same pungent odour, and very watery. Delirium is present in some cases. The temperature may be subnormal, or rise to 102° F., occasionally even to 106° F. When fatal, the coma deepens, the pulse becomes rapid and feeble, and there is Cheyne-Stokes respiration. [Pg 137]
In Hyperpyrexial cases the symptoms are similar to the asphyxial, but the temperature may reach 110-115° F., and in profound coma death takes place from asphyxia. A subconscious or automatic state, in which the person may go on working, may precede the “stroke.”
In cases which are not so rapid, pneumonia, meningitis, cardiac and respiratory paralysis may occur and prove fatal.
Heat exhaustion may be more gradual in its onset, or come on suddenly. Prodromal dizziness, faintness, nausea, headache, drowsiness, epigastric and lumbar pains may precede the prostration and muscular weakness. Fever supervenes, a rapid pulse, and in severe cases collapse. Consciousness is seldom completely lost, and in favourable cases is quickly regained. When there is marked prostration the heart may fail.
The condition known as heat prostration is a milder form, in which there is little or no fever, and the circulation remains good.
After suffering from an attack of heat-stroke certain sequelæ have been noted. The patients are rendered sensitive to slight elevations of temperature, and, during warm weather, experience chromatopsia, headaches, irritability, irascibility, and even delirium. Epilepsy and insanity may persist during life. Fiske from his investigations concludes that the habits of those working in hot atmospheres, and the degree of temperature, are not nearly so important as the absence of thorough ventilation as causative factors in the disease.
Post-mortem Appearances.—Rigor mortis comes on early, and is pronounced and disappears quickly. Putrefaction is early in onset. The brain and cord, the lungs and spleen and splanchnic area exhibit venous engorgement.
The blood is fluid, and the red corpuscles crenated. Extravasations of blood may be present in the skin, the serous membranes, and cavities, the superior sympathetic ganglia, and the vagi and phrenics. The left ventricle is markedly contracted, the right dilated and filled with blood.
Van Gieson records acute parenchymatous degeneration of the whole of the cerebro-spinal nervous system, with chromatolysis of the cells. Parenchymatous changes may be present in the liver and kidneys.
Death is not always immediate. Sometimes the clothes have been torn off the body with scarcely any personal injury. Metallic articles, especially steel, worn or carried about the person become magnetic and may be fused. The lesions which may be met with after lightning-stroke are varied, and may comprise wounds of almost any description; simple, compound, or comminuted fractures of bones; burns in the form of streaks, patches, lines, or arborescent markings; ecchymoses; singeing of the hair; impressions of metallic articles on [Pg 138] the skin. Apart from the lesions noted above, the following symptoms may be present: deafness, blindness, paralysis, loss of memory, delirium, and convulsions. Not infrequently those killed by lightning are found in the same position that they occupied during life. The question may arise as to whether the deceased died by lightning or violence. The presence of a storm at the time when death is stated to have occurred, and other attendant circumstances, will in most cases point to the true cause of death. Metallic articles should be examined with regard to their electric state. Dr. Honiball tenders this caution: “Be not too sure that in every body found dead after a thunderstorm, and where no marks upon it are found, that death was due to lightning-stroke, for it may happen that death was due solely to cardiac syncope owing to sudden and startling fright.”
Post-mortem Appearances.—Apart from the external injuries, when present, post-mortem rigidity comes on early. The head and neck may be purplish in colour, the eyes partially open and suffused, with variable pupils. The internal signs are not characteristic. The membranes and vessels of the brain may be hyperæmic. The blood has been said to be very fluid, but it may be coagulated. The internal organs may be torn, bones may be fractured, and blood-vessels ruptured.
With the increased use of electricity for motive power and illumination instances of injury and even death have occurred, and probably will become more frequent. One of the most important safeguards of the body against the effects of electricity is its high degree of resistance, especially if the body surface be dry. Moisture of the body surface lessens the resistance and increases the liability to injurious effects.
The body is a bad conductor; it is said to be three million times less than mercury, and fifteen million times less than copper; the nerves conduct like metals. The danger of electric shocks depends upon the amount of current passing through the body, the kind of contact, and the insulation of the body at the time. Moisture of the body or clothes will increase the effects of the shock. Much depends upon the quality, duration, strength, and density of the current, and the direction in which it passes.
The continuous current is less severe than the interrupted, and the alternating is the most powerful in its effects. An alternating current of 300 volts has caused death, and one of 1500 volts would certainly prove fatal, whereas for the continuous current it would take 3000 volts to prove fatal.[13] Cases are recorded when with good contact even so low as 65 volts has proved fatal. The Board of Trade forbids the introduction into dwelling-houses of currents of more than 250 volts, unless for special purposes and with special permission. [Pg 139]
As the current enters or leaves the body it may cause local injury. Tetanic muscular contractions with pain, and pain from stimulation of nerve endings in the skin with erythema may occur. Burns produced by electricity may be accompanied by much local destruction of tissue and slow healing.
There may be ascending neuritis from injury to nerves.
The shock may cause insensibility with pallor and stertorous breathing; the skin is moist, the eyes suffused, and the pupils dilated.
Death is due to (1) inhibition of the medulla oblongata, or (2) direct action on the heart muscle. According to the researches of Cunningham, currents which traverse the whole body transversely or longitudinally produce fibrillary contraction of the heart muscle. When the current passes through the brain, medulla, and upper cord it may cause death by respiratory paralysis. Those who have recovered from severe shock describe the sensation as peculiar rather than painful.
Post-mortem Appearances.—These include the local injury, if any, at the point or points of contact, some hyperæmia of the internal organs, œdema of the lungs, and fluidity of the blood. The general appearances are those of asphyxia. Kratter considers that external burns in association with subpericardial and subpleural ecchymoses, and especially subendocardial petechiæ, also the presence of congestion of the bronchi, strongly indicate death from electricity.
Minute hæmorrhages may occur in the meninges, and in the fourth and other ventricles. Changes have also been described in the cells of the central nervous system in experiments upon animals.
Treatment.—The current should be switched off at once; the patient should be removed from the conductor, the rescuer being protected with some insulating material, the attempt should not be made bare-handed.
Stimulation, warmth, and artificial respiration should be resorted to. After respiration has been re-established, friction should be applied to the body. The treatment should be persevered in for several hours. Signs of life may not be seen for two hours. Venesection may be desirable.
According to the Statute 24 and 25 Vict. c. 100, sec. 48, rape in England is defined as the “carnal knowledge of a woman against her will.” In Scotland rape is held to be “the carnal knowledge of a woman forcibly, and against her will, or of a girl below twelve years of age, whether by force or not” (Hume, i. 303). An Act passed in 1885 (48 and 49 Vict. c. 69) has materially affected the law on this subject as regards the age of females. To constitute the offence of rape, there must be penetration, but proof of the actual emission of semen is not now necessary. Before the Statute 9 Geo. IV. c. 31, sec. 18, it was also necessary to prove emission, which might be proved either positively by the evidence of the woman that she felt it, or it might be presumed from circumstances; as, for instance, that the defendant, after connection with the prosecutrix, arose from her voluntarily without being interrupted in the act. The slightest penetration of the male organ within the vulva will be sufficient, and the hymen need not be ruptured (R. v. Russen, 1 East P.C. 438, 439). The resistance of the woman must be to the utmost of her power. If, however, the woman yield through fear or duress, it is still rape; but of course much will depend upon the previous character of the woman, and her conduct subsequent to the alleged outrage. The party ravished is a competent witness to prove this and every other part of the case; but the credibility of her testimony must be left to the jury. The defendant may produce evidence of the woman‘s notoriously bad character for want of chastity or common decency, or that she had before been connected with the prisoner himself; but he cannot give evidence of any other particular facts to impeach her chastity (R. v. Hodgson, R. & R. 211). She may be asked if she has had connection with other men, but she need not answer (R. v. Cockcroft, 11 Cox, 410, per Willis, J.). If she deny connection with the men named to her, they cannot be called to contradict her (R. v. Holmes, L.R. 1 C.C.R. 334).
A rape, according to Scottish law, may be committed on a common strumpet; and in England the law goes even further, and admits the possibility of rape on the concubine of the ravisher (1 Hale, 729), “although such circumstances should certainly operate strongly with the jury as to the probability of the fact that connection was had with a woman against her will.” A husband may be guilty of rape on his wife if he hold her while another violates her, as in the case of the Earl of [Pg 141] Castlehaven, tried in 1637. Carnal knowledge of a woman by fraud, which induces her to suppose it is her husband, now constitutes a rape by the 48 and 49 Vict c. 69, which enacts that “whereas doubts have been entertained whether a man who induces a married woman to permit him to have connection with her by personating her husband, is or is not guilty of rape, it is hereby enacted and declared that every such offender shall be deemed to be guilty of rape.” It has also been decided that if a man get into bed with a woman while she is asleep, and he know she is asleep, and he have connection with her while in that state, he is guilty of rape (R. v. Mayers, 12 Cox, 311, per Lush, J.). The offence of rape is not triable at quarter sessions.
Upon an indictment for rape, there must be some evidence that the act was without the consent of the woman, even when she is an idiot. In such a case, where there was no appearance of force having been used to the woman, and the only evidence of the connection was the prisoner‘s own admission, coupled with the statement that it was done with her consent, the Court held that there was no evidence for the jury (R. v. Fletcher, L.R. 1 C.C.R. 39).
In another case, where the prisoner was caught in the act by the father of an idiot girl, the learned judge told the jury that if the prisoner had connection with the prosecutrix by force, and if she was in such an idiotic state that she did not know what the prisoner was doing, and if the prisoner was aware of her being in that state, they might find him guilty of rape; but if, from animal instinct, she yielded to the prisoner without resistance, or if the prisoner, from her state and condition, had reason to believe she was consenting, they ought to acquit him. The jury found that he was guilty of an attempt at rape (R. v. Barrat, L.R. 2 C.C. 81).
Where the prosecutrix, an apparent idiot, proved that the prisoner had had connection with her, but it appeared from her examination that though she knew he was doing wrong, she made no resistance, and the prisoner, on being apprehended and charged with committing a rape upon the prosecutrix “against her will,” said “Yes, I did, and I‘m very sorry for it,” it was held that there was evidence to go to the jury of a rape (R. v. Pressy, 10 Cox, 635).
In Scotland, in the case of Hugh M‘Namara (H.C. July 24, 1848, Ark. 521), where the woman was only one degree removed from idiocy, it was laid down that “if she had shown any physical resistance, to however small an extent, the offence would be complete, in consequence of her inability to give a mental consent.”
In future cases the above decisions will probably be set aside in the light of the present enactment.
In the case also of a quack doctor, who, under the pretext of performing a surgical operation on a young girl of nineteen years of age, had connection with her, she at the time resisting, but believing that she was undergoing an operation, it was held, on appeal, that he was guilty of the crime of rape, and the former conviction confirmed (R. v. Hattery, C.C.).
In England, and in Ireland, and also in Scotland, unlawfully and carnally knowing a girl under thirteen years of age constitutes a felony—the attempt in the former countries constitutes a misdemeanour; [Pg 142] in Scotland, a “crime and offence.” The child may be a witness if she understands the nature of an oath or understands the duty of speaking the truth, but her evidence must be corroborated by some other material evidence in support thereof, implicating the accused. The carnal knowledge of a girl above thirteen and under sixteen, or of any female idiot or imbecile woman or girl, under circumstances which do not amount to rape, but which prove that the offender knew at the time of the commission of the offence that the woman or girl was an idiot or imbecile, constitutes a misdemeanour. Above sixteen consent does away with the crime; and it shall be a sufficient defence for the accused to show that he had reasonable cause to believe that the girl was of or above the age of sixteen years. This defence does not apply to female idiots or imbeciles.
A boy under the age of fourteen was formerly in England presumed by law incapable of committing a rape (R. v. Groombridge, 7 C. & P. 582); but in Scotland there was no such provision, and a boy thirteen and a half years of age was committed for rape (Rob. Fulton, jun., Ayr, Sept. 20, 1841).
The recent Act before quoted provides that, instead of imprisonment, the offender, if under sixteen, may be whipped and sent to a reformatory school for not less than two or more than five years. Evidently age cannot now be pleaded as an incapability.
The crime of rape appears to be most frequently perpetrated against children, probably due to the popular idea that an attack of gonorrhœa may be cured by connection being had with a virgin or healthy female.
The following Table from Casper gives the result of his examination of one hundred and thirty-six cases of rape:
| From | 2½(!) | to | 12 | years | old | 99 |
| “ | 12 | “ | 14 | “ | 20 | |
| “ | 15 | “ | 18 | “ | 8 | |
| “ | 19 | “ | 25 | “ | 7 | |
| 47 | “ | 1 | ||||
| 68 | “ | 1 | ||||
| 136 | ||||||
In examination of a case of alleged rape, several points of interest will have to be considered, which, for the sake of convenience, will be placed in a tabular form:
1. An Examination of the Parts of Generation.
(a) More or less inflammatory redness and abrasion of the mucous membrane lining the parts, which is never absent in children, and may last for some weeks. “In adults, virgins up to the time of the commission of the crime, this appearance is either not found at all or only faint traces of it. In those previously deflowered it is never observed.” In the case of young children the genitals may be so injured as to cause death in a few hours. The parts may therefore present all varieties of injury, from slight bruising and redness to the most fearful lacerations.
Caution.—Inflammatory irritation due to catarrh may occur, and be apt to mislead.
(b) A muco-purulent secretion, from the mucous membrane lining the vagina, of a greenish-yellow colour, more or less viscid, and soiling the linen of the girl. This secretion, in colour and consistence, cannot be distinguished from that the result of gonorrhœa. The usual period of incubation of gonorrhœa is from three to eight days; among young girls, however, this period may be shortened. The incubatory stage of soft chancre is from three to five days (Diday); that of hard chancre somewhat longer, varying from fifteen to twenty days. Enlargement of the inguinal glands and the persistence of the discharge after the use of simple treatment will tend greatly to confirm the suspicion of venereal disease. The genital organs of the male may have to be examined as to the presence of gonorrhœa or syphilis. Syringing the urethra may remove for a time the gonorrhœal discharge; care must therefore be taken in forming an opinion.
Caution.—Unhealthy children, and those recovering from some debilitating diseases—fever, &c.,—may suffer from purulent discharges from the vagina. Small ulcers may also be present, and may be mistaken for syphilitic ulceration Infantile leucorrhœa is not uncommon. (Percival‘s Medical Ethics.)
(c) Hæmorrhage or Dried Blood about the Genital Organs.—(1) Frequently absent in young children. (2) Always found in adults, virgins at the time the rape was committed, when the vessels of the hymen are ruptured.
(d) Destruction of the Hymen.—Most frequently, and especially in young girls, one or more lacerations of the hymen may be seen. These lacerations must be looked for within five or six days of the alleged rape, as they soon heal up, and then no certain opinion can be given as to the date of their infliction. They may also be produced by any foreign body to substantiate a charge of rape.
(e) Dilatation of the Vagina.—This condition may be produced by the passage of hard bodies in order to substantiate a false charge of rape. Casper once examined a girl, only ten years of age, whose mother had gradually dilated her vagina with her fingers, in order to fit her for sexual intercourse with men.
(f) General Signs of Rape.—To the above are added certain [Pg 144] general signs, as a difficulty in walking, attended with an involuntary separation of the thighs, common to both children and adults; pain is also not infrequently present in passing water, and when the bowels are relieved. In determining the truthfulness of the statements made as to an alleged rape, the character of the woman, and the obvious inconsistencies of her statements must be taken into consideration. Moreover, if, in addition to the injuries found on the external genitals, spermatozoa be detected in the vagina, a presumption in favour of the injuries being due to sexual intercourse will be clearly made out, but the presence of spermatozoa in the vagina of a woman is no evidence of rape. Care, however, must be taken not to confound with spermatozoa an animalcule—Trichomonas vaginæ—described by M. Donné as being sometimes found in the vaginal mucus. The head of the animalcule is larger than that of a spermatozoon, and is surrounded by a row of cilia.

Fig. 19.—Hymen of child
of
four years—annular type.
The illustration also shows the
prominence of the
urinary portion of
the genitals.
In the case of young children, the anxiety on the part of the parents of the child to push the charge, and the story of the child and that of the parent heard apart, may assist in guiding the opinion. The lesson-like way in which the child tells her story, even to the minutest details, is always suspicious. The proof of a previous defloration negatives the pretended loss of virginity at the time of the commission of the deed for which the accused is being tried. In most cases, it is best to let the patient tell her own tale, and then cross-examine. An injudicious question may put her on her guard.
2. Examination of the Limbs and Body of the Female for Bruises, &c.—Little value is to be placed on injuries said to be inflicted on the person of a female the result of a struggle, as these may be produced by the woman on herself in order to substantiate her story. In children, for obvious reasons, they do not occur.

Fig. 20.—Virgin hymen,
with central slit.
3. Examination of the Linen.—In all cases a careful examination of the body linen of both parties should be made. With regard to the position of the stains on the chemise of the woman, M. Devergie insists that the stains on the front of the chemise are seminal, those on the back are due to blood. This distinction is too arbitrary to meet all the facts of these cases, for the position of the spots necessarily [Pg 145] depends on the respective positions of the parties at the moment of ejaculation; and, moreover, the woman is more likely to wipe the parts with the front than the back of her chemise. Mistakes may arise from—
1. The garments being intentionally soiled with blood. This is not infrequently done in cases of false accusations.
2. The menstrual discharge may be readily mistaken for that due to violence, as the two kinds of blood cannot be distinguished.
3. The red juice of fruits and grease spots have been mistaken for marks of blood and seminal stains on linen.
The identification of blood-stains is not difficult when the stain occurs on pieces of white linen; but when, as it not infrequently happens, they have to be detected on the coarse, dirty, often stinking linen of the poor, the task becomes somewhat more difficult. The same may be said with regard to seminal spots. As a means of diagnosis in stains due to semen, the appearance and smell of the stains are of no assistance whatever. The microscope will alone give any trustworthy evidence as to the nature of the stain; and even here a caution must be added—for the fact is beyond doubt that the semen even of a healthy young man varies much, and is scarcely ever twice alike, so that the absence of spermatozoa is no proof that the spot is not seminal in its origin.
The following are the tests used for the detection of semen:
1. Characteristic smell when the spot is moistened.—This test is of no use, for the reasons before stated.
2. Appearance when held to the light.—As uncertain as the preceding.
3. Doubtful spots upon cotton or linen—not upon wool, which usually contains sulphur—should be cut out and moistened with a few drops of oxide of lead, dissolved in liquor potassæ, and then dried at a temperature of 68° F. The stain in a few minutes becomes of a dirty yellow or sulphur-yellow colour. This change in colour proves that the mark is not a seminal stain. Semen does not contain albumen. This test only shows that the stain is not caused by albuminous compounds, which contain sulphur; but it does not follow therefore that the spot must be seminal, for marks made by gum, dextrine, and some other substances of a like nature are not changed in colour.
4. The Microscope.—This is by far the most reliable test, but care is required in its manipulation.
(a) The cloth must not be rubbed between the fingers, as the spermatozoa may be damaged by the operation.
(b) The suspicious spot on the linen should be carefully cut out and placed in a clean watch-glass or small porcelain vessel, and then moistened with a small quantity of distilled water. The cloth may be gently moved about in the water with a glass rod, and gentle pressure made so as to thoroughly wet the cloth, which, in most cases, will be accomplished in about a quarter of an hour. A single drop should now, by gentle pressure with the fingers, be squeezed on to a clean slide, and then placed under the microscope.
(c) Another method may be adopted. First determine the side of the cloth on which the stain is present, and cut out the stain, leaving a small strip of cloth attached to the main portion. Place the end of the strip in a little water in a watch-glass, so that the water by capillary [Pg 146] attraction may permeate the entire stain. With a thin-bladed knife gently remove the moistened stain and place it on a microscopic slide, and examine as before.
Fixing and Staining.—A drop of the watery extract of the stain may be placed on a microscope slide and allowed to dry in the air, covered to protect it from dust, and then fixed by heating the slide over a spirit or Bunsen flame or by the use of absolute alcohol. When fixed, the preparation can be stained with eosin and methylene blue, methylene violet, or other nuclear dye. The film may also be fixed and stained with Leishman‘s solution in one procedure, or fixed by heat first and then stained with Leishman. The procedure is the same as for blood, viz. to cover the film with a few drops of Leishman‘s stain, let stand for two or three minutes, then add a few drops of distilled water, in two or three minutes wash in distilled water, dry with filter paper, and examine with the oil immersion. The preparation may be mounted in Canada balsam and preserved for further reference. The head of the spermatazoon takes the nuclear dyes in ordinary use. The spermatazoa are best found in the centre of the stain. If the stain be small the watery extract may be centrifuged.
Florence‘s Reaction.—A useful chemical reaction has been introduced by Dr. Florence of Lyons. It depends upon the reaction between a concentrated solution of iodine in potassium iodide and human semen. A watery extract of the stain is made, and a drop placed on a microscope slide, by
| Potassium iodide | 1.65 | grms. |
| Iodine | 2.54 | “ |
| Distilled water | 30 | c.c. |
The drops are covered with a cover glass and examined; where the two drops unite, a precipitate is formed which consists of brown crystals, very similar to hæmin crystals. If there be sufficient material the precipitate may be obtained in a test tube. This test is extremely delicate, and is analogous in value to the guaiacum reaction for blood. A positive reaction does not absolutely prove that the stain is seminal, but a negative reaction proves that it is not. Dr. Florence holds the reaction is specific for human semen, as he has failed to obtain it with the seminal fluid of any other animal, or other fluids or tissues. He considers it due to the presence of an alkaloidal body in human semen, which he calls virispermin.
The crystals are said by Dr. Max Richter to form on the addition of the iodine solution to decomposition products of lecithin.
The author has found this reaction extremely delicate, even with minute traces. The crystals form rapidly and are easily recognisable. They, however, are evanescent and disappear on standing, so that they cannot be preserved as microscopic specimens.
The biological test.—This is carried out in the same way as the biological test for blood. Dr. C. G. Farnum, who proposed this test, uses semen or testicular emulsion for antigen, injecting 5 to 10 c.c. into the peritoneal cavity of a rabbit at intervals of from two to six days, on five or eight occasions. The antiserum is diluted from twelve to eighteen times with normal saline, and the semen four to twenty-five times. Human antiserum gives a precipitin reaction with the watery extract of human seminal stain, but not with testicular emulsions of the bull, dog, or goat, or with human blood serum.[14]
Can a Rape be committed by one man on a healthy, vigorous woman?—The answer to the question will, to a great extent, depend on the relative strength of the conflicting parties. Every case of rape [Pg 147] has to be judged on its own merits. In any case, the medical jurist has simply to state, from the examination of the parties, that sexual intercourse has taken place, leaving the jury to decide whether a rape or not has been perpetrated. A case is mentioned by Casper where a healthy, strong adult of twenty-five years old was violated by a single man.
Can a Woman be Violated during Sleep?—By this is intended natural healthy sleep, and not that induced by narcotics. In natural sleep, rape is scarcely possible in a virgin, especially if the hymen be found recently ruptured, though it may be possible in a woman accustomed to sexual intercourse.
Fig. 21.—Photo-micrograph
of human spermatozoa, × 1000.
(R. J. M. Buchanan.)
Can a Woman become Pregnant by an act of Rape?—The answer to this question is most decidedly in the affirmative. It is not necessary for a woman to experience any sexual pleasure during connection in order that she may conceive. A woman may become pregnant if fresh semen be injected into the vagina with a glass syringe.
Signs of Rape in the Dead.—In the case of a woman found dead, the question may arise as to her having been violated prior to death. The reply to the question is by no means easy. Severe injury to the genitals is a presumption in favour of rape, but cases are by no means rare in which men failing to accomplish coïtus have injured the parts with their fingers. The presence of spermatozoa in the vaginal mucus is good evidence of a recent coïtus, but is no direct evidence of a rape. Collateral evidence will in most cases decide the point. [Pg 148]
Physical Signs of Rape
in Adult and in Child
| In the Adult. | In the Child. |
| 1. If examined soon after the | 1. There may not be sufficient |
| commission of the offence, the | penetration to rupture the hymen, |
| hymen of the adult virgin may | consequently there will be |
| be ruptured, and the fourchette | no hæmorrhage. In other cases |
| may be lacerated, and the parts | the external organs will be |
| covered with blood. | bruised, and in many cases |
| severely lacerated, the lacerations | |
| depending on the amount of | |
| penetration and force used. | |
| 2. Difficulty in walking, in | 2. Same as in the adult, but |
| passing water, and sometimes | lasting for a longer time—from |
| when the bowels are relieved. | eight to fourteen days. |
| These signs in the adult pass | |
| off in a day or two. | |
| 3. Injuries on the person abused, | 3. For obvious reasons these |
| such as scratches and ecchymoses, | do not occur on children. |
| may be present as the result of a | |
| struggle. These may be self-inflicted. |
Directions as to manner of making a Medico-Legal
Examination in a Case of Alleged Rape.
1. Be careful to note everything, for it is in such cases as the one under discussion where apparently unimportant signs may become of the greatest moment.
2. Give the female no time for preparation, but make your visit, and at once proceed to an examination. The visit to be of any practical service should not be delayed beyond the third or fourth day after the alleged offence, “by which time the lacerations will have healed, the cicatrices disappeared, and the torn hymen be in such a state as to make it difficult to say whether it had been divided recently or at an earlier period.” But remember that you are not justified in using force; and in this, as in cases of suspected pregnancy, if you examine a woman against her will you render yourself liable for an action for assault, and may have to pay heavily for your enthusiasm.
3. Age, strength, and condition of the health of the complainant. Examine the wounds asserted to have been inflicted, and see if they correspond with the history given of their infliction.
4. Examine organs of generation.
5. Preserve any spots on linen, &c., for future examination. [Pg 149]
6. In case of death after violence—
7. Examine spot where the crime is stated to have taken place.
8. Examine person of the accused.
N.B.—The lapse of a few days may be sufficient to remove all traces of the violence done to the parts; and in most cases days, weeks, and even months may elapse before an examination is made of the alleged victim.
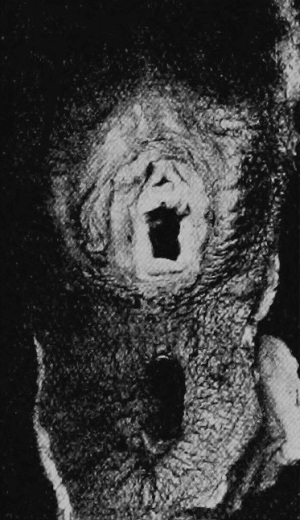
Fig. 22.—Deflorated hymen, after parturition, in adult woman.
There is no one sign which may be considered as an absolute test for virginity. The presence or absence of the hymen is of no probative value one way or the other. Its very existence has been denied by Paré, Buffon, and others. It may be absent as the result of disease, or as the result of a surgical operation to allow of the free discharge of the menstrual flow. Its presence is no bar to conception; and cases are on record where it has been found necessary to incise it, to allow of the passage of the fœtus into the world. In fact, women who have been prostitutes for years have possessed to the last uninjured hymens. The changes in the breasts which proceed from impregnation do not occur where only defloration has taken place. The rugose condition of the vagina is only affected by the first birth, and not by sexual intercourse.
What has been said of the above signs as tests for virginity may be said of a host of others which from time to time have, with varying success, been advanced as aids to the diagnosis. Casper, however, considers “that where a forensic physician FINDS A HYMEN STILL PRESERVED, EVEN ITS EDGES NOT BEING TORN, AND ALONG WITH IT—in young persons—A VIRGIN CONDITION OF THE BREASTS AND EXTERNAL GENITALS, HE IS THEN JUSTIFIED IN GIVING A POSITIVE OPINION AS TO THE EXISTENCE OF VIRGINITY, and vice versa.”
It not infrequently happens that a medical man is called upon to make an examination of a woman for legal purposes, in order to decide—(a) The existence of an alleged pregnancy. (b) The possibility of a previous pregnancy. (c) As to the existence of concealed pregnancy.
The following are some of the reasons why pregnancy may be feigned:
1. By a married woman, to gratify the desire of her husband for issue.
2. To influence the jury in a case of breach of promise of marriage as to the assessment of the damages.
3. To extort money from a seducer or paramour.
4. To produce a spurious heir to property.
5. By a single or married woman, to stay the infliction of capital punishment.
Pregnancy may be concealed—(a) In order to procure abortion. (b) In order to commit infanticide. (c) In the married and the unmarried, to avoid disgrace.
Besides the above, other important questions may arise with regard to this state:
1. Is pregnancy possible as the result of coïtus in a state of unconsciousness?—There appears no reason for doubting the possibility of this occurrence.
2. Can pregnancy occur before the appearance of the catamenia?—That pregnancy may occur before menstruation is undoubted; and it appears probable that the changes in the ovaries and uterus may go on at the regular monthly periods, and yet there may be no discharge of blood from the uterus, which, as pointed out by Bischoff, is only a symptomatic though usual occurrence. Hence, pregnancy is possible prior to menstruation.
3. What is the earliest and latest age at which pregnancy is possible?—In our climate (Britain), the earliest age at which pregnancy may occur is about the eleventh or twelfth year; but the youngest age at which this condition is reported to have occurred is nine years (Meyer). In hot climates—as in Bengal—mothers under twelve years of age are by no means rare. Cohabitation in marriage takes place much earlier in India than in Europe, but Chevers doubts if menstruation naturally occurs much sooner there than elsewhere, and Baboo Modusoodun Gupta believes that the catamenia appear sooner or later, according to the mode of living of the females, and the sexual excitement to which they may be subjected. Thomas mentions the case of a girl who menstruated regularly from the age of twenty-one months, and also of another at eight months. The limit to child-bearing appears to be between the fiftieth and fifty-second years; but even here considerable variation has been recorded, and women have been delivered of children at the age of sixty. Haller even reports one at seventy. As long as menstruation continues a woman may become pregnant; but even the cessation of this flow for some months is no bar to conception.
4. Is it possible for a woman to become pregnant eight weeks after [Pg 151] her last confinement?—This is undoubtedly possible, but it is of rare occurrence. It is also probable that a woman may abort at the end of the time above mentioned. Husband knew a woman, who for several years bore a child every ten months.
At common law, in cases of disputed inheritance, the following may occur, and give rise to the necessity for medical evidence on the subject: A woman who has just lost her husband may disappoint the expectant heirs to an estate by alleging that she is pregnant.
At criminal law, pregnancy may be used as a stay to the infliction of capital punishment.
In the first case, a jury of matrons is impanelled by a writ de ventre inspiciendo, to decide the existence of pregnancy, and if the fact be proved, to watch till such time as she be delivered.
In the second case, in England, the pregnancy must be proved, and also whether she be quick with child. In Scotland the pregnancy must be proved, but without reference to quickening, and the jury of matrons is unknown in that country. In the same country, if it can be shown that a woman is pregnant, and that her life or that of the child is endangered by her imprisonment, she may be admitted to bail till after delivery. A pregnant female also cannot be compelled to appear and give evidence, if on competent authority it be shown that her delivery will probably take place at the time fixed for the trial.
The diagnosis of early pregnancy in ordinary cases is by no means easy, especially before the third or fourth month of gestation; but to the medical jurist it is still more difficult, as he has to deal with cases where he can scarcely expect much candour. No opinion should, however, be given without taking into consideration the collective value of the signs, as no one sign will afford sufficient data on which to base an opinion. The signs furnished by auscultation are the most reliable, but the position of the fœtus may render the sounds of the fœtal heart and placental souffle difficult to detect.
The following may be taken as among the most important signs of pregnancy, given in the usual order of their occurrence:
1. Cessation of Menstruation.—The non-appearance of the catamenia, though a most valuable sign, is by no means a conclusive one, as menstruation may be arrested by diseases of various kinds; while, on the other hand, there are many well-recorded cases of women who have menstruated regularly during the whole period of their pregnancy. There have been also cases in which the menses only occurred during pregnancy; and in a few still more curious cases, women who have never menstruated have been known to have borne several children. In cases of concealed pregnancy, the woman may smear her linen with blood to imitate the menstrual flow.
2. Morning Sickness.—Nausea, often ending in vomiting, generally occurs soon after rising in the morning, and may commence almost immediately, but more frequently not till the expiration of the fifth or sixth week after conception. It is not a reliable sign, and is often very irregular in its occurrence. When present, it varies in degree, from a feeling of nausea to the most violent vomiting, very distressing to the patient.
3. Salivation.—The excessive secretion of the salivary glands, due to the irritation caused by pregnancy, was first mentioned by Hippocrates as a sign of this condition. “It is to be distinguished from ptyalism induced by mercury, by the absence of sponginess and soreness of the gums, and of the peculiar fœtor, and by the presence of pregnancy.” It is oftener absent than present.
4. Mammary Sympathies.—As the breasts may enlarge from various causes—such, for instance, as the distension of the uterus from hydatids, or, as is the case with some women at each menstrual period, when the catamenia are suspended, or after they have ceased—this is by no means a sign on which much reliance should be placed. The change in the colour of the nipple and areola, more apparent in women of dark complexions, is more to be relied on as a diagnostic sign of pregnancy. The first observable alteration, which occurs about two months after conception, is “a soft and moist state of the integument, which appears raised, and in a state of turgescence, giving one the idea that, if touched by the point of the finger, it would be found emphysematous. This state appears, however, to be caused by infiltration of the subjacent cellular tissue, which, together with its altered colour, gives us the idea of a part in which there is going forward a greater degree of vital action than is in operation around it; and we not infrequently find that the little glandular follicles, or tubercles as they are called by Morgagni, are bedewed with a secretion sufficient to damp and colour the woman‘s dress.”
During the progress of the next two months, the changes in the areola are in general perfected, or nearly so, and then it presents the following characteristics: “A circle round the nipple, whose colour varies in intensity according to the particular complexion of the individual, being usually much darker in persons with black hair, dark eyes, and sallow skin, than in those of fair hair, light-coloured eyes, [Pg 153] and delicate complexion. The extent of the circle varies in diameter from an inch to an inch and a half, and increases in most persons as pregnancy advances, as does also the depth of colour. In the centre of the coloured circle, the nipple is observed partaking of the altered colour of the part, and appearing turgid and prominent, while the surface of the areola, especially that part which lies more immediately around the base of the nipple, is studded over and rendered unequal by the prominence of the glandicular follicles, which, varying in number from twelve to twenty, project from the sixteenth to the eighth of an inch; and, lastly, the integument covering the part appears turgescent, softer, and more moist than that which surrounds it; while on both there are to be observed at this period, especially in women with dark hair and eyes, numerous round spots or small mottled patches of a whitish colour, scattered over the outer part of the areola, and for about an inch or more all around, presenting an appearance as if the colour had been discharged by a shower of drops falling on the part.” The value of the above changes in the nipple and areola as a diagnostic sign of pregnancy is greatly lessened by a previous pregnancy. It should also be remembered that milk may occur in the breasts of women who are not pregnant.
5. Enlargement of the Abdomen.—For the first four months of pregnancy the entire uterus is contained in the cavity of the pelvis; it then gradually rises, so that at about the fifth month it is midway between the pubes and umbilicus, which latter it reaches at the end of the sixth month; during the seventh month it may be felt half-way between the umbilicus and ensiform cartilage; at the end of the eighth month it is level with the cartilage, now quite filling the abdomen. Still increasing in size during the ninth month it does not ascend higher, the abdominal walls yielding to its increased weight, allowing it to fall somewhat forward. A caution is necessary with regard to this sign. The abdomen may enlarge from causes other than pregnancy. Pregnancy and ascites, or ovarian dropsy, may coexist in the same patient, and the diagnosis be rendered anything but easy. The enlargement of the abdomen may lead to unfounded suspicions detrimental to the happiness and health of the unfortunate object of them.
6. Condition of the Cervix Uteri.—The cervix softens during pregnancy, and the softening is present as early as the second or third week. It is an important sign. Hejar‘s sign or the softening at the junction of cervix and body and the lower uterine segment is valuable, but not always easily elicited. It is of most value from the second to the fifth months. At the sixth month it loses one-fourth of its length; at the seventh it is only half of its original length; at the eighth it loses another quarter; and at the ninth the neck is entirely obliterated. This shortening is more apparent than real, and its occurrence is denied by the late Dr. J. M. Duncan, except during the last few days of pregnancy.
7. Quickening.—The period at which quickening occurs varies from the fourth to the fifth month; and the term is understood to imply the first perception of the movements of the fœtus experienced by the [Pg 154] mother. Nervous women, anxious to have children, sometimes complain of sensations which they ascribe to quickening, pregnancy being absent. Pregnancy may occur without quickening.
8. Kiesteine.—This is no test of pregnancy, as it may be found in women not pregnant.
9. Jacquemier‘s Test.—A violet or port-wine colour of the vagina and inner surface of the vulva, due to venous congestion of the parts from pressure of the gravid uterus.
A flattening of the upper wall of the vagina, produced by the enlargement and anteversion of the uterus, which, forcing the os towards the sacrum, makes the anterior wall of the vagina tense, has been added by Dr. Barnes as a sign of pregnancy.
1. Ballottement.—This test of pregnancy is applied by causing the patient to stand upright; the finger of the right hand is then passed into the vagina and placed in the anterior fornix, the other hand being placed lightly over the abdomen in order to steady the uterine tumour. If the finger be now jerked upwards against the head of the child, it will be felt to float upwards in the liquor amnii, and then by its own weight gradually to return to its former position. Tumours in the uterus, attached to its walls by a pedicle, may give the same sensation. Scanty supply of liquor amnii, or malposition of the child, may sometimes prevent the adoption of the test.
2. Uterine Souffle.—Under this head are included the placental bruit, and the pulsations of the umbilical cord. Both these sounds require a skilled auscultator to detect them. The uterine murmur, or bruit placentaire, is heard best at the lower and lateral portions of the uterus, just above Poupart‘s ligament. It is isochronous with the pulse of the mother, and is heard most distinctly about the fourth or fifth month of utero-gestation; in some cases, however, it may be heard as early as the tenth week. The sound is intermittent, and varies in character, being sometimes hissing, whirring, or cooing, at others rasping.
3. Pulsation of the Fœtal Heart.—The sounds of the fœtal heart were first noticed by Mayar in 1818, and those of the placenta, or placental souffle, by Kergaradec in 1822. The sound of the fœtal heart is composed of a rapid succession of short, regular double pulsations, differing from that of the adult heart in rhythm and frequency. It can be heard more or less over the whole of the abdomen about the middle of the fourth month, and is not unlike the muffled ticking of a watch. In frequency it varies from 100 to 140. The auscultator should be careful not to hang his head down, or he may be apt to mistake the throbbing of his own arteries for sounds communicated from the patient.
4. Intermittent Contraction of the Uterus.—From the fourth to the tenth month of pregnancy, the uterus may be felt by the palpating hand to alternately contract and relax; the period of contraction and relaxation varies. It is present in pregnancy whether the fœtus be alive or dead. [Pg 155]
Pregnancy may be simulated by ascites, by fibrous tumours of the uterus, by ovarian dropsy, and by enlargement of the uterus from retention of the catamenia due to an imperforate hymen, &c. The breasts may also become affected by uterine tumours.
1. Pseudo-Pregnancy.—In the examination of cases of alleged pregnancy, the medical jurist should bear in mind the possibility of enlargement of the uterus and abdomen from the presence of tumours. The probable occurrence of pseudo-pregnancy should also be considered. Tumours and pseudo-pregnancy may occur in the married and unmarried; and as the latter is not infrequently accompanied with many of the signs and symptoms of pregnancy, an early diagnosis is of the utmost importance.
The diagnosis will consist in—
(a) A careful examination of all the symptoms present, when, in most cases, a break in their order of sequence may be observed, or certain signs may be added which do not occur in true pregnancy.
(b) Presence or absence of the hymen.
(c) If the patient be placed well under the influence of chloroform, the tumour, if the result of pseudo-pregnancy, will subside, gradually returning as the effects of the anæsthetic pass off. Whilst the patient is under the influence of the anæsthetic, the hand may be pressed on the abdomen at each expiration, and there retained, the pressure being continued during the inspirations.
2. Dropsy.—Use of the stethoscope; examination of the breasts for milk, and the urine for albumen.
3. Fibrous Tumours.—Absence of fœtal movements and other signs of pregnancy.
4. Ovarian Dropsy.—Tumour on one side of the abdomen; breasts unaffected, and auscultation giving negative results.
5. Retention of the Catamenia.—On examination, the hymen found perfect and bulging. This condition cured by a crucial incision.
This subject is best discussed under three heads: (1) Signs of Recent Delivery in the Living. (2) Signs of Recent Delivery in the Dead. (3) Signs of Previous Delivery.
(a) Transitory Signs; (b) Persistent Signs of Delivery
1. General Indisposition.—The face is pale or flushed; the eyes sunken, and surrounded by a dark areola; there is considerable debility, and a tendency to faint; the skin is warm and moist, and the [Pg 156] pulse quick. It must be borne in mind that a woman who is anxious to conceal her recent delivery may, by an effort of the will, to a great extent hide her real condition.
2. The Breasts.—The breasts feel firm and “knotty,” and on pressure yield a small quantity of colostrum or milk, which may be distinguished by the aid of a microscope.
3. The Abdomen.—The skin of the abdomen shows signs of recent distension; it is relaxed, and more or less thrown into folds, the lower part marked by irregular broken streaks of a pinkish tint, becoming white and silvery as time goes on.
4. The Lochia, or the “Cleansings.”—These consist in a discharge from the uterus, which, for the first three or four days after delivery, is more or less bloody. During the succeeding four or five days it acquires a dirty-greenish colour—“green waters,” with a peculiar sour, rancid odour. In a few days this is succeeded by a yellowish, milky-looking mucous discharge, which may continue for four or five weeks.
5. External Parts of Generation.—The labia and vagina bear distinct marks of injury and distension.
6. The Uterus.—The uterus is enlarged, and may be felt by the hand for two or three days after delivery, as a round ball, just above the pubes. The orifice of the uterus, if examined a few hours after delivery, appears as a continuation of the vagina. This condition completely disappears in about a week after delivery.
7. After-pains.—These are of no use from a diagnostic point of view, as we have no means of testing their presence or absence.
1. Entire obliteration of the hymen.—This is no proof of actual delivery.
2. Destruction of the fourchette.
3. The vagina dilated, and free from rugæ.
4. Dark colour of the areola round the nipples.—This varies among women; and cases are known where there was no areola either during pregnancy or after delivery.
5. Skin of Abdomen.—Due to the great distension of the abdomen, the skin appears streaked with silvery lines varying in breadth. These markings in some cases may be scarcely perceptible, especially if the female has worn a tight abdominal belt during her pregnancy. The same appearance may be produced by dropsy, or the prolonged distension of the abdominal walls, the result of other causes. Attention to the other signs present will assist the diagnosis. After the lapse of seven to ten days the recent delivery of a woman cannot be certainly proved by an examination of the living woman, especially if it be known that she had previously borne children. In primiparæ the pink-coloured streaks on the abdomen, and the transverse condition of the os uteri, may strongly point to recent delivery.
Should the woman die immediately after delivery, the external parts will present the same appearance as just described in the living. On [Pg 157] opening the abdomen, the uterus will be found fat and flabby, between nine and twelve inches long, and with the os uteri wide open. The cavity of the uterus may contain large bloody coagula, and its inner surface be lined by the decidua. The attachment of the placenta is easily detected by its dark colour, and by the semi-lunar openings of the arteries and veins on the surface of the uterus.
Of course all the appearances just described will be greatly modified by the time that has elapsed between delivery and death.
Delivery after Death.—The fœtus has been known to have been expelled from the uterus by the force of the gases generated by putrefaction. Dr. Aveling, in a paper published in the Obstetric Transactions, 1873, arrives at the conclusion that post-mortem delivery is possible even where no symptoms of parturition were noticed before death. He also thinks that the child may live in utero for some hours after the death of the mother.
Table showing the Size of the
Uterus at
Different Periods after Delivery
Two to Three Days.—7 inches long and 4 inches wide.
Seven Days.—Between 5 and 6 inches long and 2 inches wide.
Fourteen Days.—From 4 to 5 inches long and 1½ inches wide.
End of Second Month.—Normal size. 2½ inches long and about 2 inches broad at the fundus.
Table giving Weight of the Uterus
after Delivery
| Immediately after Delivery | 22 to 24 | ounces. |
| Within a Week | 18 to 21 | “ |
| End of Second Week | 10 to 11 | “ |
| End of Third Week | 5 to 7 | “ |
| End of Second Month | normal, 9 to 10 | drachms. |
| (Heschl.) | ||
1. Marks on the abdomen, consisting in shining silvery lines, due to the distension of the skin. These may result from distension other than that the result of pregnancy—tumours, dropsy, &c.
2. Marks on the breasts, similar to those appearing on the abdomen. These, in conjunction with the above, are important.
3. Peculiar jagged condition of the os uteri, felt by the finger. The condition may be the result of disease.
4. Marks of rupture of the fourchette or perinæum.
5. Dark colour of the areola round the nipple.
6. Negative evidence, from absence of any of the above.
Can a Woman be delivered unconsciously?—This question may arise in cases of infanticide. Setting aside cases of epilepsy (in a fit of which disease Husband once attended a woman who was confined during the fit without being aware that she had been delivered), cases of apoplexy, coma, and narcosis from chloroform, opium, &c., it may be [Pg 158] stated that delivery is possible during profound sleep. Husband once attended a woman who informed him that “she always had her pains during her sleep,” and only woke up just as the head came into the world. When it is borne in mind how easily some women pass through labour, it is quite possible that, after a busy day, sleep may be so profound as not to be disturbed by the pains of labour. In primiparæ the occurrence is more problematical. Women have often declared that they have been unconsciously delivered whilst at stool. This is also possible, but the circumstances of the case must be severely sifted.
[“Every woman, being with child, who, with intent to procure her own miscarriage, shall unlawfully administer to herself any poison or other noxious thing, or shall unlawfully use any instrument, or other means whatsoever, with the like intent: and whosoever, with intent to procure the miscarriage of any woman, whether she be or be not with child, shall unlawfully administer to her, or cause to be taken by her, any poison or other noxious thing, or shall unlawfully use any instrument, or other means whatsoever, with the like intent, shall be guilty of felony, and being convicted thereof shall be liable, at the discretion of the Court, to be kept in penal servitude for life, or for any term not less than five years, or to be imprisoned for any term not exceeding two years, with or without hard labour, and with or without solitary confinement.”—Statute 24 and 25 Vict. c. 100, sec. 58.]
The 59th section of the same Statute also takes into consideration the unlawfully supplying or procuring any poison, or other noxious thing, or instrument, or thing whatsoever for a woman, for the purpose of inducing abortion. The person so doing shall be guilty of a misdemeanour, and be kept in penal servitude for a term of five years, or be imprisoned for any term not exceeding two years, with or without hard labour.
It will be seen from the passages above quoted that there is no distinction between a woman quick or not quick with child. “The offence is to procure the miscarriage of any woman, whether she be or be not with child” (R. v. Goodhall, 1 Din. 187; 2 C. & K. 293). But although the law does not regard “quickening” in cases of abortion, yet the fact of having “quickened” may be pleaded as a bar to immediate capital punishment.
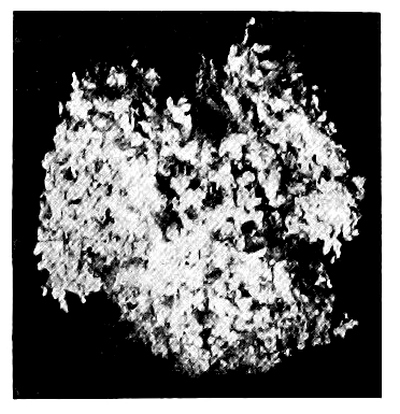
Fig. 23.—Abortion at fourth week.
(Glaister.)
It has been decided in Scotland that drugging or operating to procure abortion is criminal, though unsuccessful, but it is not certain whether the woman alone can be charged with taking drugs to procure abortion. Both in England and in Scotland, to make the procuring of abortion criminal, “there must be felonious intent,” for it may be necessary to cause abortion. It must be borne in mind that the law allows no discretionary power on the part of medical practitioners who, to save the life of the mother, may deem it advisable to induce premature delivery. This being the case, no medical man should attempt to induce premature labour without the consent of the relatives of the [Pg 160] woman, and the sanction of a medical colleague after consultation. This precaution is the more necessary as several medical men have been prosecuted, an event which would not have taken place had the precaution above suggested been observed. A medical man should also be very careful never to give any medicine “to bring on the courses” if he has the slightest suspicion of pregnancy, even as a “placebo” to satisfy an importunate patient, for should abortion be otherwise procured, his really harmless medicine may be accused with the result, and a grave suspicion be raised against him, to say the least.
The term abortion is understood in medicine to mean the expulsion of the contents of the fœcundated uterus before the sixth month of pregnancy, that is, before the child is considered viable. After this period it is said to be a premature labour.
In law, however, no distinction is made and the expulsion of the contents of the uterus at any period before the full time of pregnancy is considered an abortion; in popular language, a miscarriage.

Fig. 24.—Abortion between
sixth and eighth week.
(Glaister.)

Fig. 25.—Abortion at tenth
week.
(Glaister.)
Abortion, when not produced by criminal means, generally occurs at or a little before the third month of utero-gestation, and then usually in first pregnancies, or during the latter part of the period of child-bearing. It is also more frequent among the rich than among the poor. Of the two thousand cases of pregnant women examined by Dr. Whitehead of Manchester, the sum of whose pregnancies was 8681, or 4.38 for each, rather less than 1 in 7 had aborted.
When abortion is criminally induced, it generally takes place between the fourth and fifth months, that is, about the time the woman becomes certain of her condition.
The Causes of Abortion are—
(a) Maternal.—Among the maternal causes may be mentioned excessive lactation; any irritation of the rectum or bladder; loss of blood, which, by increasing the amount of carbonic acid in the blood, acts as an excitant to the spinal cord; excessive irritability and excitability of the uterus, &c. Certain states of the system conduce to [Pg 161] abortion—albuminuria, syphilis, certain fevers, scarlet fever, smallpox, &c. Abortion may become habitual in some women. Great joy or sudden sorrow have not infrequently been the cause of abortion. The tendency to abortion is greatest at the menstrual periods, that is, at the time when, had not the woman become pregnant, menstruation would have taken place. Slight causes acting at these times are very liable to produce abortion.
(b) Fœtal.—The death of the ovum, or a diseased condition of its uterine coverings, or of the placenta, probably of an inflammatory nature.
(a) Mechanical.—Under this head may be mentioned the passage of certain instruments into the cavity of the womb, and the rupture by violence of the membranes which surround the fœtus; also the injection of fluids into the uterus. A medical man practising in Yorkshire informed Husband that so great was the dread of large families, that he knew of several ladies who, if they went a day over their monthly period, passed a catheter into the uterus, with the desired result. “It was wonderful,” he added, “how clever they were.” In India a twig of the Euphorbium nivulia, anointed with assafœtida, is used for the same purpose. “The fœtus is never delivered alive, but there is said to be no great danger to the woman” (Chevers). Women may use hairpins, knitting-needles, and the idea is to pass the instrument “until blood comes,” which is accepted as a sign that abortion will be sure to follow. In some cases it is by no means easy to procure abortion, and women have been known to undergo a considerable amount of violence without abortion taking place. In some women, however, on the other hand, the slightest violence—such, for instance, as slipping from a step or low chair—will cause them to abort.
(b) Medicinal.—Certain drugs, among which may be mentioned ergot, savin, pennyroyal, rue, tansy, saffron, perchloride of iron, diachylon which contains lead, and others, have been used for the induction of abortion. In India unripe pineapple has a great reputation as an abortive (Medical Jurisprudence for India, Chevers). It is scarcely necessary to mention each drug individually, but it must be remembered that there is not one single internal medicament of which it can be consistently with experience asserted that, even when an abortion has followed its use, it must have produced this abortion, and that cause and effect are in such a case “indirect and necessary connection.” All the so-called abortives are most uncertain in their action, and their use is attended with considerable risk to the woman. In the case of diachylon profound lead poisoning may be the result. Be this as it may, they are more frequently used to induce abortion than mechanical procedure, from the fact that the latter requires some amount of anatomical knowledge and manipulative skill.
The dangers of abortion from any cause are hæmorrhage, sepsis, and peritonitis. In mechanical interference, especially where proper precautions have not been taken to prevent them, sepsis and peritonitis from local injury and perforation are prone to occur. [Pg 162]
A medical man may be required to—(1) Examine into the nature and characters of the substances expelled from the womb; (2) Examine the woman stated to have aborted.
1. Examination of the Substances expelled from the Womb.—The substances expelled from the womb often become the subject of judicial inquiry, and the medical man may be required to give his opinion as to their probable nature.
Dr. Gallard has called attention to the following:
1. During the last six months of pregnancy, abortion, even when it occurs spontaneously, goes through the two stages as at full time, i.e. the expulsion of the products of conception is, as a rule, preceded by rupture of the membranes, followed after a time by the expulsion of the placenta.
2. In the first three months this order of things is absent, for it is the rule to see the fœtus expelled entire en bloc without rupture of the membranes.
3. If, then, we find during the first three months of pregnancy the products of an abortion in which the membranes have been ruptured and the embryo expelled alone, we must look for a pathological cause for this infraction of a general rule; and if no disease of the embryo or of the mother is found, we are justified in attributing the abortion to mechanical means used directly against the products of conception. Charpentier has shown that this rupture of the membranes is not an absolute proof of criminal abortion; but in eighteen cases of spontaneous abortion M. Leblond only found rupture of the membranes in one, and in this the membranes presented an abnormal friability.
The questions may be asked—(1) Is it a fœtus?—(2) Is it a mole? If so, is a mole also a fœtus?—(3) Is it merely the coats of the uterus, and unconnected with pregnancy?
1. Is it a Fœtus?—The development of the fœtus is given on pp. 35, 36 et seq.
2. Is it a Mole?—This question gives rise to another: Is a mole a fœtus? To this the answer must be in the affirmative. Moles, being the diseased appendages of the fœtus, vary in character, and have been described by obstetrical writers under the following heads: (a) Hydatiginous; (b) Carneous; (c) Fatty Moles.
(a) Hydatiginous Moles are a result of a diseased condition of the villi of the chorion. The villi become dropsical, and hang in masses like a bunch of grapes.
(b) Carneous Moles.—These are the result of hæmorrhage into the chorion. The blood becomes organised, and a fleshy mass is formed, to which in some cases a withered fœtus is attached.
(c) Fatty Moles.—Death of the fœtus and fatty degeneration of the placenta, or fatty degeneration of the placenta and death of the fœtus, produces this variety of mole. A withered fœtus with a mass of fatty placenta are expelled.
3. Is it merely the Coats of the Uterus, and unconnected with Pregnancy?—Fleshy masses may be expelled from the womb, which may not be the result of sexual intercourse. The description just given of true moles will, it is hoped, assist in forming a correct diagnosis. [Pg 163] Considerable care will be required, for the honour of the woman accused depends upon the opinion given as to the nature of the substances submitted for examination. It must also not be forgotten that moles may be retained for many months in the uterus and be then expelled. The knowledge of this fact may rebut an accusation of infidelity against a wife. Polypi may be discharged from the womb; the presence of a pedicle will point to their true character. All substances expelled from the uterus should be carefully washed in water, and all clots removed. The examination of the woman may also help in the formation of the diagnosis. The absence of the signs of defloration or of recent delivery will be in her favour.
2. Examination of a Woman stated to have aborted.—This subject may be divided under two heads—(1) Has the woman been recently delivered? (2) What were the means used to procure the abortion?
It is by no means easy to answer the question whether an alleged abortion has really taken place or not. The signs of recent delivery are in most cases absent, for the woman can better hide her condition during the earlier than during the later months of utero-gestation; consequently suspicion may not have been aroused against her for some weeks or months after the event. The history of the case, with other attendant circumstances—milk in the breasts, change in the colour of the areola round the nipples, severe flooding, absence of the hymen, injuries to the os uteri, transverse condition of the os uteri in contradistinction to its circular form after delivery, &c.—will, in most cases, assist in forming a correct diagnosis; but it must be again repeated that few of the signs applicable to delivery at the full time are here available.
In all doubtful cases—
1. Examine into the general and present state of the health of the woman.
2. Find out if there are any reasons which would occasion a pretext to use drugs which are not usually given to women during pregnancy.
3. Learn if menstruation is regular and easy, or if the woman is in the habitual use of emmenagogues, for, if so accustomed, she may have used them ignorant of pregnancy.
4. If a woman ascribes her abortion to a fall, to an accident, or to violence used against her, carefully examine into the nature of these.
5. Examine into the general causes of abortion, and also inspect the expelled substances.
Where death is supposed to have followed the use of abortives, the alimentary canal must be examined for the signs of the action of irritants, or the presence of disease in the internal organs; but when death has resulted from an attempt to procure abortion by instrumental means, the neck of the womb is most frequently found covered by a number of small more or less irregular wounds, which may penetrate into the womb or lose themselves in the walls of the organ. Their course is indicated by infiltration, or a small extravasation of coagulated blood, the exact condition of which must, if possible, be ascertained, so as to decide when the wound was inflicted. [Pg 164]
The examiner must not forget that the wounds may extend to the fundus of the uterus, and in this case the autopsy shows that a blunt instrument, as a catheter or uterine sound, introduced through the os uteri into the retroverted uterus, glides by its own weight into the rent. The seat of the tear leads one to think that pregnancy was not far advanced when the attempt was made, and in fact the accident most frequently occurs in cases of suspected pregnancy. It must be remembered that the uterus is often punctured by the injudicious use of the uterine sound, but without any immediate dangerous symptoms. Wounds in the walls of the vagina indicate the use of instruments by an inexperienced hand; in the fundus of the uterus, to one at least accustomed to the introduction of instruments. Spontaneous rupture of the uterus is impossible during the early periods of pregnancy, just when the attempts at abortion are usually made. Rupture due to external violence is, as a rule, accompanied with outward signs of the violence used.
In all cases a careful examination of the structure of the uterus should be made. An examination of the ovaries for false or true corpora lutea should be made. The opinions on the character and differences of these bodies are so discordant as to destroy all confidence in their value as proof of conception or the reverse.
Taylor says: “The discovery of the ovum in the uterus in process of development could alone, in the present state of our knowledge, warrant an affirmative opinion on this point in a Court of Law, and this I believe to be the safest view at present of this much-contested question. On the other hand, the absence of a corpus luteum from the ovary would not in all cases warrant an opinion that conception had not taken place.”
Examine carefully for local sepsis and signs of inflammation of the uterus and its surrounding structures.
Recapitulation
In Medicine, Abortion occurs before the sixth month of pregnancy—premature labour after that period.
In Law, Abortion may take place any time before the full period of utero-gestation.
Abortion may be due to—
According to the present state of English law, infanticide—murder of a new-born child—is not regarded as a specific crime, but is treated and tried by those rules of evidence which are applicable in cases of felonious homicide, but with this difference, that the law requires proof that the child was born alive. An old Statute (21 Jac. I. c. 27) made the concealment of the birth of a bastard child conclusive evidence of murder. As far as the legal estimation of the crime is concerned, it matters not whether the child was killed immediately on its entrance into the world, or within a few days afterwards. A fœtus not bigger than a man‘s finger, but having the shape of a child, is a child within the Statute (R. v. Colmer, 9 Cox, 506; R. v. Hewitt, 4 F. & F. 1101). An English judge, at a late trial, stated that if the jury were of the opinion that the prisoner had strangled her child before being wholly born, she must be acquitted of murder. The law also, on the score of humanity, presumes that every child is born dead until direct evidence to the contrary, from medical or other sources, is given. The onus of the proof of live birth, therefore, devolves on the prosecution. It may also be difficult to decide as to the maternity, and the woman accused will have to be examined as to the possibility of her recent delivery.
Here let me repeat the advice given on page 148 as to the examination of a woman. Your duty is to request the woman to allow of the necessary examination, giving her the warning which every magistrate or coroner is bound to give to any person charged with a crime, before requiring an answer to a question which may be used in evidence against her at the subsequent trial. The innocent and the guilty may alike object to an examination, but the presumption is against the party declining, if several have voluntarily submitted. A young lady committed suicide rather than submit to an examination by two medical men under an order from the coroner. The medical men were guilty of a grave indiscretion, and both they and the coroner were acting ultra vires in attempting to force a woman to obtain evidence against herself (Taylor, vol. ii. p. 431).
The decision as to recent delivery will, to a great extent, rest on the condition of the mother, and the apparent age of the child found dead. The discovery of the body of the child is not necessary to conviction, but the medical evidence as to the signs of respiration, of course, depends on the body being found and examined. In most cases of alleged infanticide tried in England, juries appear more inclined to fall back [Pg 166] on the minor offence—concealment of birth—than to convict of the capital offence; and this appears to be the only alternative if the body cannot be found, for, as we have just said, in law every child is held to be born dead. It must of course be shown that the woman has been recently delivered. In case of failure to prove the murder of the child, the Act (24 and 25 Vict. c. 100, sec. 60) enacts that “if any woman shall be delivered of a child, every person who shall, by any secret disposition of the dead body of the said child, whether such child died before, at, or after its birth, endeavour to conceal the birth thereof, shall be guilty of a misdemeanour.” The mere avowal of the birth is not sufficient to convict her; she must be proved to have done some act of disposal of the body after the child was dead (R. v. Turner, 8 C. & P. 755).
In Scotland, concealment of pregnancy is a statutory crime, chargeable when the child born is found dead or is not found at all, and there is no proof of its having been murdered. Pregnancy, up to a period when a child might be born alive, must be proved, and the words “during the whole period of her pregnancy” do not imply that the pregnancy must have continued for the full period of nine months. All that is necessary is that there should be such proof of duration of pregnancy as made a living birth possible. If the accused can bring forward a witness to whom she communicated her pregnancy, or called for assistance at the birth, or (it is believed) can prove that the child was born dead, she is entitled to an acquittal.
It has also been said that a woman ought not to be convicted of “concealment of pregnancy,” if at the time of delivery the fœtus do not appear to have reached the seventh month of intra-uterine existence. The birth of a “child,” whether dead or alive, is essential; therefore, if the woman accused “can prove that that which she brought forth was not a ‘child,’ but an abortion, or a fœtus, which, from some accident, was in such a condition that, though there had been assistance, it could not have been in a condition to be called ‘a child,’ then the case is out of the Statute.” The Scotch Statute differs from the English on the “concealment of birth” in this, that so long as the woman makes known her pregnancy, the motive for doing so is not considered. Thus, if she make arrangements with anyone to conceal the birth, “the Statute is eluded by that very circumstance” (Alison). The Statute applies to married as well as to single women; but, in the former case, the penalty is seldom enforced unless foul play is suspected.
“The entire delivery of a child.” There must be an independent circulation in the child before it can be accounted alive (R. v. Enoch, 5 C. & P. 539). The entire child must be actually born into the world in a living state (R. v. Poulton, 5 C. & P. 329). But the fact of the child being still connected with the mother by the umbilical cord will not prevent the killing from being murder [Pg 167] (R. v. Reeves, 9 C. & P. 25). To kill a child in its mother‘s womb is no murder, because the person killed must be “a reasonable creature in being, and under the King‘s peace.” But if the child be injured in the womb, and yet be born alive, and then die as a result of such injuries, it may be murder in the person who inflicted them (R. v. Senior, 1 Mood. C. C. 346).
A distinction must be drawn between medical or physiological life and legal life. A child may have breathed, as it not infrequently does, before it is completely born into the world; and this might, in a medical point of view, be considered as a live child, but it is not one legally. The entire delivery of the child is necessary in law; and “it must also be proved that the entire child has actually been born into the world in a living state, and the fact of its having breathed is not a conclusive proof thereof.” The inference unfortunately follows from this ruling, that a mother may kill her child without fear of punishment, if she do so before the entire body has slipped from her.
The evidence of live birth in civil is somewhat different from that required in criminal cases. The viability of the child is determined in Scotland by its crying; in France, by its respiration; in Germany, “the LIVE BIRTH of a child is to be held proven when it has been heard to cry by witnesses of unimpeachable veracity present at its birth”; but in England, the pulsation of the child‘s heart, or any tremulous motion of the muscles, however slight, has been considered as satisfactory proof of live birth.[15]
According to Blackstone, “crying, indeed, is the strongest evidence, but it is not the only evidence”; and Coke remarks, “If it be born alive, it is sufficient though it be not heard to cry, for peradventure it may be born dumb.”
Signs of Live Birth prior to Respiration, and independent of it.—(1) Negative.—Signs of intra-uterine death, i.e. putrefaction, or “intra-uterine maceration,” or of such imperfect development that it could not have been born alive. (2) Positive.—Injuries to the child showing that it must have been born alive.
1. Negative.—Intra-uterine Putrefaction.—This condition differs in some remarkable points from putrefaction in air.
The body is extremely flaccid and flattened, the bones of the cranium moving easily on one another. The skin of the hands and other parts of the body bear the evidence of prolonged soaking in fluid. In parts, the skin is whitish, or of a reddish-brown or coppery-red colour, without any trace of green, which is always present when putrefaction takes place in the air. The cuticle may be raised in blisters, and be easily detached from the true skin. The denuded patches are moist and greasy, and exude a stinking, reddish-coloured serous fluid. The face [Pg 168] is flattened, and the features distorted. In one case that Husband attended of intra-uterine death of the fœtus in a primipara, and where putrefaction was far advanced, the scalp burst during delivery, and the brain was poured out. Should, however, the child be exposed to the air, it may soon acquire the appearances proper to putrefaction in that medium. If the child, immediately after birth, be thrown into water, the putrefactive changes would be like those of intra-uterine decomposition. In this case the lungs must be examined for the evidence of death by drowning.
2. Positive.—Evidence that injuries found on the body could not have been inflicted during birth, or accidentally after birth. On this subject it is scarcely possible to give an opinion one way or the other. All the medical witness can fairly state is, that, from the condition of the lungs, respiration has or has not taken place; that, in the former case, it is not easy to state whether the injuries were the cause of death or inflicted after death.
Appearances showing that a New-Born Child has breathed.—1. Walls of the Chest.—“The vaulting of the thorax is not of the slightest diagnostic value.” Casper quotes from Elsässer the following remarks: “It is irrefutable that the variations in the circumference of the thorax (and, of course, in its diameters) are so considerable that no certain normal mean for a thorax that has breathed, and for one that has not breathed, can be laid down. In most cases the measurements of the thorax are incapable of determining whether the lungs contain air or not. The reasons for these variations is, without doubt, to be referred to the congenital differences in the volume of the osseous thorax; partly, also, to the thickness of the soft parts, particularly of the subcutaneous fat and the thoracic muscles; partly, also, to the differences in the degree and amount of the dilatation of the thorax by respiration, with which the distension of the lungs also corresponds,” &c.
2. Diaphragm.—The position of the diaphragm may be considered as a good diagnostic sign; for it is found that, in children born dead, the highest point of the concavity is between the fourth and fifth ribs, whereas in those born alive it is between the fifth and sixth. The position of the diaphragm may be affected by the gases produced during putrefaction, and also, in children who have breathed, from distension of the stomach and intestines with gas.
3. Stomach and Intestines.—With regard to the stomach, Tardieu has suggested that the presence of air-bubbles in the glairy mucus usually found in that organ is a sign of live birth, as it can only have arisen from the swallowing of saliva and mucus, aerated by repeated attempts at respiration, probably lasting from five to fifteen minutes. Air in the duodenum is strong evidence of live birth. Breslau of Prague, who has further investigated this subject, states that, in children born dead, or who have undergone prolonged intra-uterine putrefaction, there is never any accumulation of gas in the stomach or intestines, and that the presence of gas in these organs is contemporaneous with respiration, and is independent of the ingestion of food. The intestines of newly-born children do not float [Pg 169] in water, but rapidly sink in that fluid. As respiration proceeds, the coils of the intestines become distended with gas.
4. Kidneys and Bladder.—The presence of crystals of uric acid in the pelvis of the kidneys and even in the bladder has been suggested as a sign of live birth. Uric acid infarction, as it has been called, usually occurs in from two to ten days after birth, at a period when there are more important signs of live birth than this, even if infarction did not occur, as it does, in still-born infants.
5. Lungs.
(a) Size.—In the fœtus, prior to respiration, the lungs do not fill the cavity of the chest, and the left lung is never found even partially covering the heart.
After respiration they fill the thorax more or less completely, the amount of distension depending, of course, upon the completeness of the respiratory acts on the part of the child.
(b) Consistence.—Before respiration has taken place, the lungs feel firm, compact, and resistant, and are of the consistency of liver.
After respiration they are spongy, crepitant, and yielding when pressed between the fingers. They also present a marbled appearance. These signs of respiration are more or less modified by disease, and the atelectasis pulmonum of Jörg, jun.
Casper denies the existence of atelectasis pulmonum as a distinct disease of newly-born children, and considers that “it is nothing else than the original fœtal condition, from which it differs in no anatomical respect”—an opinion supported by Meigs, who says “it, in fact, resembles exactly the fœtal lung.” It is simply the result of the child dying from some cause before respiration has had time to become fully established, and has possibly been confounded with hepatisation. It must also be remembered that cases are on record of infants having lived for some hours, and then died, yet the lungs sank as a whole, and when cut in pieces.
(c) Colour.—The colour of the fœtal lungs is “exceedingly various,” and it is by no means easy to convey the idea of colour by words. Speaking in general terms, the lungs of children who have not breathed are of a reddish-brown liver colour, this colour changing to a brighter red at their margins. In children who have breathed, the lungs are of a slaty-blue colour, more or less mottled with circumscribed red patches. This circumscribed mottling is never found in perfectly fœtal lungs. When the lungs are inflated artificially, they swell up and present a uniform cinnabar-red colour, destitute of insular marbling. The insular marbling of the lungs is characteristic of lungs that have breathed, and is due to the presence of blood in the arteries and veins surrounding the inflated lung tissue.
(d) Buoyancy in Water.—Lungs which have respired float in water.
But the objection may be raised that lungs that have not respired may yet float from—
[Pg 170] The value of these objections will be discussed in the following pages.
The following table is given by Tidy:
| Lungs that have not Breathed. | Lungs that have Breathed. |
| 1. Dark in colour (black-blue, | 1. Light in colour (rose-pink, |
| maroon, or purple), resembling | pale pink, light red, or crimson), |
| liver. No mottling. | mottled. |
| 2. Air-vesicles not visible | 2. Air-vesicles distinctly |
| to the naked eye. | visible to the naked eye, or a |
| lens of low power (say a two-inch, | |
| or even a common reading-glass). | |
| 3. When squeezed or cut, do not | 3. Crepitate or crackle freely. |
| crepitate or crackle. | |
| 4. Contain but little blood, | 4. Contain a good deal of blood, |
| therefore little escapes on section. | which escapes freely on section. |
| 5. The blood present is not | 5. The blood present is freely |
| frothy, unless there be | mixed with air, and therefore |
| putrefaction. | appears frothy. |
| 6. Sink in water, unless putrid, | 6. Float in water; or, at all |
| and often not then. | events, the parts which have been |
| events, the parts which have been | |
| expanded, or have breathed, float. | |
| If fully expanded, they will buoy | |
| up the heart. | |
| 7. Bubbles of gas arising | 7. The air cannot be squeezed |
| from putrefaction may be | out by pressure. |
| squeezed out, and as they | |
| escape are usually noted to | |
| be of large size. |
Hydrostatic Lung Test
(Docimasia pulmonum hydrostatica)
The value of this test, which is a test of respiration and not of live birth, is founded on the supposition that a lung in which respiration has taken place will float if placed in water, and that when this has not occurred it will sink. Admitting that a lung floats as a result of respiration, it has been objected that this is no proof of live birth, for respiration may take place in:
With regard to the two first objections, it will be sufficient to say that, in all the cases of so-called intra-uterine respiration, the respiratory acts have occurred in difficult or instrumental labours, where it is justifiable to suppose that, in the endeavour to remove the child, a certain amount of air may have been unavoidably admitted into the maternal passages. But the cases with which the medical jurist has to deal cannot be classed with these, for in all those brought under his notice delivery has been more or less rapid and unassisted.
To the last objection the same reply may be given, that rapid delivery in doubtful cases must be considered as the rule, and that the time [Pg 171] which elapses between the birth of the head of the child and its complete delivery is so short as not to lead to any great error in diagnosis. It is true that the woman may faint with the child half born, and that respiration may thus take place; and it has not yet been decided how many inspirations a child must make to entirely inflate its lungs, or the length of time required to do so.
N.B.—Any pressure exerted on the umbilical cord during the process of delivery gives rise to respiratory acts on the part of the fœtus. The presence of what Casper calls petechial ecchymoses beneath the pleuræ, upon the aorta, and even on the heart, are, as a rule, a proof that attempts at respiration have been made. These petechial ecchymoses are sometimes found on the same parts in the drowned. (See “Drowning.”)
How is the Hydrostatic Lung Test performed?
and What are the Objections to its Use?
As this test was first used, it consisted in placing the lungs, with or without the heart, in water, and then noting whether they sank or floated. A glass vessel, eighteen inches high and twelve in diameter, half filled with distilled water at 60° F., should be used. In summer, water at the ordinary temperature of the room will answer the purpose. To this rough test pressure is now added; the lung, or portions of it, are greatly compressed in a linen cloth, and then thrown into water as before. If the lungs thus compressed float, respiration is held to have taken place; should they sink, the contrary is presumed.
Pressure is used for the following reason: The air generated by putrefaction, and which may cause the lungs to float, is removed by pressure, but no amount of pressure, short of entirely destroying the lung tissue, will remove that which is the result of respiration or inflation; and between these the medical expert must decide from collateral evidence.
In performing the test: (1) Try if the lungs will float with the heart and thymus gland attached to them. (2) If they will float without the heart, &c. (3) Try if portions will float with or without pressure.
The following are the Objections to this Test:
1. That in consequence of disease the entire lungs, or portions of them, may sink, and yet respiration may have taken place. Disease of the lung may occur previously to birth or soon afterwards, but it is scarcely probable that the disease would attack every portion of the [Pg 172] lung. Parts, doubtless, small in proportion to the diseased part, may yet have been sufficiently inflated to float. The presence of disease is also not difficult of detection.
2. That respiration, even in healthy lungs, may be so imperfect that they may sink. This objection can scarcely be considered valid against the general application of the test, for in these cases there is no known test by which respiration or its absence can be determined. They are, therefore, out of the pale of the test, as they are out of every other mode of investigation.
3. Emphysema pulmonum neonatorum.—Emphysema is generally the result of excessive dilatation of the air cells of the lung, rupture of the cell walls, and infiltration of the intra-lobular areola tissue. This condition may be brought about by:
(a) Respiration. (b) Inflation.
The fact of the matter is simply this, that the so-called emphysema pulmonum neonatorum, or emphysema of new-born children, is nothing more or less than incipient putrefaction, induced by certain unascertained conditions.
Casper sums up his conclusions on this subject in the following words:
“That not one single well-observed and incontestable case of emphysema, developing itself spontaneously within the lungs of a fœtus born without artificial assistance, is known; and it is not, therefore, permissible in forensic practice to ascribe the buoyancy of the lungs of new-born children, brought forth in secrecy and without artificial assistance, to this cause.”
4. Putrefaction.—It must be admitted as proved that the lungs of new-born children in a state of decomposition will float in water. But this admission does not render the test valueless, for it must be remembered:
(a) That air generated by putrefaction is found in bubbles under the pleuræ, or in the fissures between the lobuli of the lungs, and not in the air cells of the lungs.
(b) That gas as a result of putrefaction can easily be removed by compressing the lungs, or portions of them.
(c) That crepitation in putrefied lungs is absent, owing to the fact stated under (a).
(d) That the lungs are among those organs which putrefy late.
(e) That negative evidence may be obtained, if the lungs, in a highly putrescent body, sink in water. The tendency of putrefaction, as above stated, is to cause them to float.
5. Inflation.—In the first place, it is to be remarked that to inflate the lungs is by no means an easy task. Elsässer states “that in forty-five experiments performed on children born dead, without opening their thorax and abdomen, only one was attended with complete success, thirty-four with partial success, and ten with none whatever; and it must also be remembered that these experiments were conducted without disturbance, and with the greatest care.” Professor Gross states his opinion on this subject thus: “We are decidedly of opinion that artificial inflation of the lungs is a very difficult matter; and we believe that the complete distension of these organs can only be [Pg 173] effected where a tube is introduced into the mouth of the larynx.” In the cases that come before the medical expert, the question naturally arises, Who would inflate the lungs? Surely not the mother. If not the mother, who else? It has been suggested that some malicious person might inflate them to sustain a charge of infanticide. Is this probable?
The following points may be noticed on this subject:
(a) Known difficulty in inflating the lungs.
(b) Absence on the part of the mother of any preparation to save the life of her child.
(c) Presence of air in the stomach and intestines, the result of attempted inflation.
(d) Bright cinnabar-red colour of the lungs, without trace of mottling.
(e) Absence of frothy blood when the lungs are cut into.
(f) When, therefore, we observe the following phenomena, a sound of crepitation without any escape of blood-froth on incision, laceration of the pulmonary cells with hyperæmia, bright cinnabar-red colour of the lungs without any marbling, and perhaps air in the (artificially inflated) stomach and intestines, we may with certainty conclude that the lungs have been artificially inflated.
It may be further noted that natural respiration is accompanied with, first, the distension of the air cells of the lungs with air; and, second, with an increased flow of blood into the organs, beyond that necessary for their nourishment and growth. They thus increase in absolute weight, while their specific gravity is lessened.
The objections just mentioned apply to the hydrostatic test as originally employed. It will now be necessary to notice those against the same test when modified by pressure. These are two in number:
1. That no amount of pressure, short of entirely destroying the lung tissue, can expel the air from a lung that has been inflated, or from one in which respiration has taken place.
2. Pressure is, therefore, no test of natural respiration or of artificial inflation.
In answer to the above, it will only be necessary to refer to what has been already said with regard to the difficulty of inflation, and the more probable event of the condition of the lungs being the result of respiration.
Casper thus sums up the result of his views with regard to the probative value of the docimasia pulmonaris:
“That a child has certainly lived
during and after its birth—
“1. When the diaphragm stands between the fifth and sixth ribs.
“2. When the lungs more or less completely occupy the thorax, or at least do not require to be sought for by artificial separation of the walls when cut through.
“3. When the ground colour of the lungs is broken by insular marblings.
“4. When the lungs are found by careful experiment to be capable of floating.
“5. When a bloody froth flows from the cut surface of the lung on slight pressure.” [Pg 174]
The Lung Test is unnecessary when—
1. The umbilical cord has dropped off, and cicatrisation has followed.
2. Where food is found in the stomach.
3. Where there are evident signs of putrefaction in utero.
4. Also in the case of the birth of monsters, or where, from congenital malformation, the possibility of live birth is excluded.
Besides the hydrostatic test, the following have been proposed:
Ploucquet‘s Test.—This test is based on the relative weight of the lungs, before and after respiration, to that of the entire body of the child. The variations found in practice between the relative weights render the test worse than useless.
Absolute Weight of the Lungs.—This test consists in a comparison of the weight of the lungs before and after respiration, and it may be stated here that the lungs, prior to respiration, vary in weight from about 400 to 650 grains; but so much depends on the maturity or immaturity of the child, and degree of respiration, that, like the last, the test is unworthy of confidence.
Wredin‘s Test.—Dr. Wredin, of Petrograd, states that the gelatinous substance found in the middle ear of infants before birth, gradually disappears, to be replaced by air on the subsequent establishment of respiration. Wendt, of Leipzig, from an examination of 300 cases, declares that the gelatinous substance can only be expelled by the establishment of full respiration. The value of this test has been questioned, as some observers have found that in different cases intervals of from a few hours to five weeks have occurred, before the replacement of the gelatinous material by air.
Table Showing the Signs of
Maturity of Child At Birth
As regards:
1. Average Length of Body.—Nineteen inches.
2. Average Weight of Body.—About seven pounds.
3. Eyes.—The pupillary membrane is not found in the mature child.
4. Navel.—Said to be exactly midway between the pubes and the ensiform cartilage.
5. External Genitals.—Testicles found in the scrotum, and the labia majora cover the vagina and clitoris.
6. Os Femoris.—Ossification of the inferior femoral epiphysis. The osseous nucleus measures from three-quarters of a line to three lines in diameter.
Death may be due to—
[Pg 175] I. Immaturity on the part of Fœtus.-From some cause or another, the child may die immediately after birth, in spite of every attempt to save it. In many of these cases no disease adequate to account for death can be detected.
II. Complications occurring during or immediately after Birth.—(1) Unavoidable or inherent in the process of parturition. (2) Induced with criminal intent, constituting “infanticide by commission.”
1. Unavoidable or Inherent in the Process of Parturition.—The immediate cause of death may be either maternal or fœtal. In the former, the presence of tumours in the pelvic passages, or disease of the bones, causing a narrowing of the canal, may lead to fatal compression of the head of the child. Death may also be due to protracted labour from debility on the part of the mother, or she may suddenly faint after delivery. A congested state of the brain may be present in these cases. In the latter (fœtal), pressure on the umbilical cord from malposition of the child during labour, or an abnormal increase in the size of the head, may cause death. There is also a greater mortality, both during and after delivery, among male than female children. The child may be also accidentally suffocated in the fæces of the mother, or in the fold of her dress; or it may be born while the woman is straining at stool, and be drowned in the contents of the pan. Husband once met with a case of accidental death of a child from suffocation in the drawers of the mother, who persisted, from motives of delicacy, in wearing those articles of dress during her confinement. Death may also result from strangulation, occasioned by the pressure of the funis round the child‘s neck. The death in this case can scarcely be considered as due to strangulation, as the child had never breathed, but it is probably the result of the arrest of the flow of blood along the cord, from the tightness of the folds round the neck. Some congestion of the brain may, however, be found resulting from the pressure on the vessels of the neck. Lastly, death may ensue from a fall on the floor in cases of sudden and quick labours, especially if the woman be in the erect posture at the time of delivery.
2. Induced with Criminal Intent.—Infanticide by commission: was the death due to violence? The answer to this question is by no means easy. In all doubtful cases the attendant circumstances must be taken into consideration. A woman may unintentionally injure her child in her efforts to drag it from her. The presence of respiration, more or less complete, is strongly presumptive against the death being the result of accident. But even here considerable caution is necessary, for the injury may not be immediately fatal, although accidentally inflicted, sufficient time elapsing between its infliction and the death of the child to allow of respiration. Foreign bodies found in the mouth and fauces are also corroborative of death by violence. A case is recorded in which the child‘s fauces, upper portion of the œsophagus, the larynx, and the trachea were closely packed with a coarse green sand, and yet the lungs sank when the hydrostatic test was applied to them. There was nothing to show when the packing of the fauces was effected. [Pg 176]
Strangulation may be produced by the constriction of the umbilical cord round the neck, and for this reason marks round the child‘s neck cannot always be ascribed to intentional violence. Of 327 cases collected by Elsässer, in which the cord was from one to four times round the children‘s necks, there was not in a single instance any mark of the cord perceptible, even though in some cases the cord had to be cut to permit the completion of labour. With regard to marks round the neck of a new-born child, Casper remarks that it is possible “to mistake the folds of the skin, produced by the movements of the head, and which remain strongly marked in the solidified fat, and are very prominent, particularly in short necks, for the marks of the cord.” The mark left by the funis is broad, corresponds with the breadth of the cord, runs without interruption round the neck, and is everywhere quite soft, and never excoriated. Ecchymoses may be present, irregularly following the line made by the cord. On the other hand, “a mummified, parchment-like, unecchymosed depression points in every case to strangulation by a hard, rough body,” and this more especially if there be any abrasion of the cuticle or laceration of the skin. Death, sometimes ascribed to strangulation, is probably the result of suffocation, and happens thus: any pressure exerted on the cord cuts off the blood from the placenta to the fœtus, and gives rise to respiratory attempts on the part of the child, the child dying from suffocation, or from the engorgement of the lungs with liquor amnii drawn into them at every effort to breathe. An infant may be poisoned. This cause of death is very rare, but deaths have resulted from the use of poisonous gases. While on this subject it may be advisable to state here that ulcerations have been found in the stomach and intestines more or less accompanied with a collection of dark brown or black bloody fluid, which have given rise to suspicions of poisoning in infants to all outward appearances quite healthy. An infant may be thrown into water and drowned. No traces of this mode of death would be discoverable in the infant unless respiration had taken place prior to its immersion. The plea of accidental drowning in a cesspool or water-closet pan may be put forward; it is therefore well to examine the cord. Has a ligature been placed upon it? Has it been cut by a sharp instrument? The nature and character of the fluid found in the stomach should be noted.
Fractures of the skull may happen—
1. In the Womb.—The parturient female may fall from a considerable height, and thus cause injury to her child. These cases are of no judicial importance, as the presence of intra-uterine putrefaction or an examination of the lungs will at once show that the child has not breathed. It must be borne in mind, however, that dislocations may take place in the womb, and this fact may be brought forward in defence. The history of the case, and the absence of any other signs of violence, will decide the truth or falsity of the plea.
2. During Labour.—Fracture of the cranial bones during labour generally occurs in difficult and protracted labours, which, from this [Pg 177] very cause, seldom become the subject of judicial inquiry. In some cases the defective ossification of the bones of the skull may give rise to fractures, which may lead to dangerous mistakes. This deficiency, in the process of ossification is thus described by Casper: “If the bone in question is held up to the light, this is seen to shine through the opening, which is closed only by the pericranium. When the periosteal membrane is removed, the deficiency in the ossification is seen in the form of a round or irregularly circular opening, not often more than three lines in diameter, though frequently less; its edges are irregular and serrated: these edges are never depressed, as is the case in fractures; and neither they nor the parts in their neighbourhood are ever observed to be ecchymosed.” The child in these cases may breathe for a short time, and then die without any apparent cause.
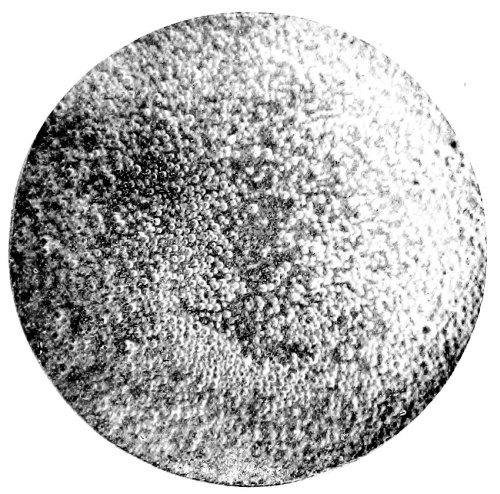
Fig. 26.—Photo-micrograph
of human milk, × 250.
(R. J. M. Buchanan.)
3. By Falls.—It is beyond doubt possible for a child to be born so precipitately as to fall on the floor and be severely injured, and that even fatally. In cases of alleged precipitate birth, to account for injuries found on the child, the following points should be remembered, and will assist in forming a diagnosis:
(a) Rupture of the umbilical cord. In all cases it would be advisable to measure the length of the cord, and then the distance of the vulva from the ground, allowing of course for the woman not being quite erect at the time of delivery owing to a separation of the legs. A disproportion between the two measurements may or may not account for the rupture of the cord. The following measurements may be taken: usual length of cord, eighteen to twenty inches; distance of vulva from the [Pg 178] ground, twenty-six inches, but allowing for stooping, two-thirds of the above. To the length of the cord must be added about nine inches, the distance from the navel to the top of the head of the child. Thus, a fall of about thirty inches will put no strain on the cord. A case is on record of a rupture of the cord taking place while the woman was in a recumbent position, but in that case the labour was precipitate, and the cord very short and small.
(b) Placenta not detached from the child.
(c) Fracture of the parietal bones; the fracture radiating into the frontal and squamous portion of the temporal bone. In experiments on twenty-five children dropped from a height of thirty inches, one parietal bone was found fractured in sixteen of the cases; both parietals, in six cases. The fractures in most cases occurred about the parietal protuberances. It must be remembered that the children were dead, and that it is easier to fracture the skull of a live infant than that of a dead one.
(d) Imperfect ossification of the bones of the skull.
(e) Absence of other injuries.
(a) The fact of the umbilical cord being divided by some sharp instrument and not torn. A caution must be here inserted, for Taylor mentions a case where rupture of the cord occurred in such a manner that it could not be decided whether it had been intentionally cut or torn.
(b) Extensive fracture of one or more of the bones of the cranium.
(c) Fracture and dislocation of the neck.
(d) Presence of incised wounds, and other evidence of violence.
N.B.—In all doubtful cases, a guarded opinion should be given, stating simply that the dissection does not reveal anything contrary to the statements offered as to the cause of death.
III. Congenital Disease in one or more of the Fœtal Organs.—In all cases the presence of congenital disease must be sought for.
IV. Neglect or Exposure, constituting “Infanticide by Omission.”—Under this head may be mentioned the following:
(a) Neglecting to place the child in such a position that it may breathe freely.
(b) Neglecting to protect the child from extremes of cold or heat.
(c) Neglecting to feed it with the food appropriate to its age. (See Signs of Death from Starvation, pp. 132 et seq.)
(d) Neglecting to tie the umbilical cord.
To give answers to these questions will in many cases be impossible, and each must be decided by such circumstances as present themselves in each individual case. For instance, if the body be found stiff, blanched, naked or nearly so, lying on the ground, the vessels of the interior gorged with blood, whilst the superficial vessels are contracted and can be seen only with difficulty; at the same time, the hydrostatic test shows that respiration has taken place, and in the absence of all external or internal causes—the probability is in favour of death by cold. In close relation with the present subject is the question—
Has the Infant bled to Death?—Fatal hæmorrhage from the cord [Pg 179] may occur, especially if it be divided by a sharp instrument close to the body of the child. As a rule, hæmorrhage does not occur from a ruptured cord. (The signs of death from hæmorrhage have been noticed, page 81.)
How Long did the Child survive its Birth?—The answer to this question is by no means easy, and the data on which a decision can be based are not very reliable. The presence or absence of the vernix caseosa should be noticed. In still-born children the closed eyelids, when raised, do not remain open; in the live-born, on the other hand, the eyes remain half open even after repeated attempts to close them. Another guide to the determination of the length of time the child survived its birth may be found in the absence or presence of the meconium in the intestines. The meconium—so-called from its resemblance to inspissated poppy juice—is found in the large intestine as a dark-greenish pasty mass, more or less filling that portion of the bowel. In the upper portions of the intestines it varies from a light-yellowish or greyish to a greenish-brown colour, till in the large intestine it assumes the colour and consistence above mentioned. It is generally discharged by the infant in from four or five to forty-eight hours after birth. In breech presentations it may be passed during the process of delivery, although the child be still-born; but its entire absence from the intestines is presumptive of existence for some days after birth.
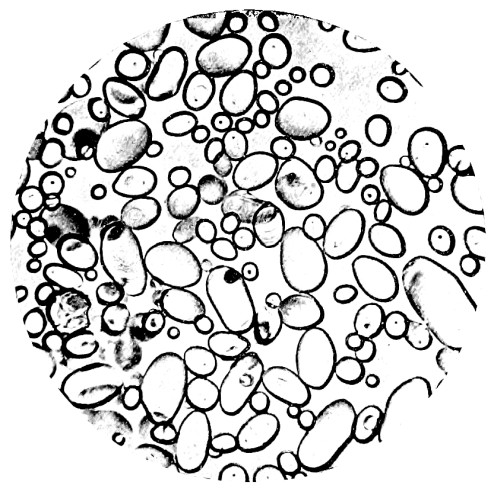
Fig. 27.—Photo-micrograph
of
starch granules, × 250 (potato).
(R. J. M. Buchanan.)
The following are some of the points to be considered in forming a diagnosis: (1) Changes in the skin. (2) Changes in the umbilical cord. (3) Changes in the circulatory system. [Pg 180]
Table showing how long a
New-born Child has Lived.
[Pg 182] 1. Changes in the Skin.—Exfoliation of the cuticle. The time at which this occurs is so variable as to be of little value in a medico-legal inquiry.
2. Changes in the Umbilical Cord.—Mummification of the cord is not of the slightest value as a proof of extra-uterine life; but the separation of the cord which occurs between the fourth and seventh day, especially when cicatrisation has taken place, is a sure sign that the child must have lived four or five days at least. Two other appearances of some value may also be noted, namely:
(a) In fresh bodies, the appearance of a bright red ring about a line in breadth, which surrounds the insertion of the cord, and which is formed within the uterus.
(b) A similar red ring, about two lines broad, around the insertion of the cord, accompanied with “thickening, inflammatory swelling of the portion of the skin affected, and slight purulent secretion from the umbilical ring itself.” This latter condition Casper considers as affording “irrefragable proof of the extra-uterine life of the child.”
3. Changes in the Circulatory System.
(a) Ductus Arteriosus.—Arterial duct. A contracted condition of this duct is of no value as a proof that a child has survived its birth; for the duct is liable to become contracted, and even obliterated, before the birth of the child.
(b) Ductus Venosus.—Nothing certain is known as to the exact time when this duct closes; the condition of the vessel is, therefore, of no assistance in determining the possibility of the child having survived its birth. The duct has been found closed in a still-born child; and in one child, which lived for a quarter of an hour, both the ductus arteriosus and the foramen ovale were found closed. Cases are also on record in which these fœtal channels were found open after thirty days of extra-uterine life.
(c) Foramen Ovale.—What has been said of the preceding may be said with regard to the foramen ovale.
N.B.—To sum up, therefore, in the fewest words, any attempt at forming an opinion on the docimasia circulationis may result in a fatal error on the part of the medical witness, as it is impossible to determine with any accuracy by days the period of their closure. As a general statement, however, the following, according to Bernt and Orfila, is the order in which obliteration of the fœtal vessels takes place: (1) The umbilical arteries. (2) Ductus venosus. (3) Ductus arteriosus. (4) Foramen ovale.
Synopsis
1. Infanticide is not regarded as a specific crime.
2. To be tried by the same rules of evidence as apply to murder.
3. The law presumes that every child is born dead, till proof to the contrary is given.
4. Onus of proving live birth devolves on the prosecution.
5. The body need not be found in order to obtain conviction of the [Pg 183] suspected party, if not of infanticide, at least of concealment of birth.
The medical evidence, however, depends on the body being found and examined.
The medical witness may be examined on one or more of the following points:
6. In absence of proof of infanticide, the woman, in England, may be tried for concealment of birth, that is, disposing secretly of the body, whether the child be born dead or alive.
7. In Scotland, a woman may be tried for concealment of pregnancy when the child is dead or missing, if she do not call for or make use of help or assistance in the birth; but the case is quashed, if the child be shown alive by the mother to others.
This subject will be discussed under the following heads: (1) The child must be born alive. (2) The child must be born during the lifetime of the mother. (3) The child must be born capable of inheriting. (4) Tenancy by courtesy, and possessio patris.
1. The Child must be born alive.—This has been discussed in the preceding section.
2. The Child must be born during the lifetime of the Mother.—Death terminates the marriage contract. Would a child born after the death of the mother, and therefore not during marriage, be entitled to inherit?
On this point Lord Coke writes:—“If a woman, seised of lands in fee, taketh husband, and by him is bigge with childe, and in her travell dyeth, and the childe is ripped out of her body alive, yet shall he not be tenant by the curtesie, because the child was not born during the marriage nor in the life of the wife; but in the meantime her land descended.”
It appears from this that the husband is not entitled to the life-rent.
3. The Child must be born capable of inheriting.—Monsters cannot inherit according to law. Blackstone says: “A monster which hath not the shape of mankind hath no inheritable blood,” and cannot, therefore, inherit; but, “if it hath human shape, it may be an heir.”
Buffon classes monsters under three divisions: (a) Monsters by excess of organs. (b) Monsters by defect of organs. (c) Monsters by alteration or wrong position of parts.
A hermaphrodite inherits, or not, property according to the prevailing sex.
4. Tenancy by Courtesy and Possessio Patris.—“When a man marries a woman seised of an estate of inheritance, and has by her issue born alive, which was capable of inheriting her estate; in this case he shall, on the death of his wife, hold the lands for his life as tenant by the courtesy of England.”
There is yet another case bearing closely on this subject, known in law as possessio fratris. On this subject Mr. Amos writes: “In the event of a man twice married dying, and leaving a daughter by each marriage, his estate would be equally shared by the daughters of the two [Pg 185] marriages; but if we suppose that there is also a son by the second marriage, born in a doubtful state, the legal effect of his momentarily surviving birth would be to disinherit the daughter of the first marriage entirely, and transfer the whole of the estate to the daughter of the second marriage, she being sister to the male heir, while the daughter of the first marriage is only half-blood.”
In both of these cases proof of live birth, as before mentioned, is of the slenderest kind.
A fœtus in the womb (en ventre sa mère) may—(a) Have a legacy or estate made over to it. (b) A guardian assigned to it. That these conditions may take effect, it must be born alive. (c) Be an executor. To exercise this post partum function, the child must in England have attained the age of twenty-one.
Every child born in wedlock is presumed to have the husband of the woman as its father; but this presumption may be denied for the following reasons:
1. Absence or death of the reputed father.
2. Impotence or disease in the reputed father, preventing matrimonial intercourse.
3. In the case of a premature delivery in a newly-married woman.
4. Want of access.
5. The paternity of the child may be disputed when the woman marries immediately after the death of her husband.
In Scotland, a child is held to be legitimate if born ten lunar months after the death or absence of its alleged father; and the absence of the supposed father must continue till within six lunar months of the birth of the child, to prove its illegitimacy.
In the same country, a child born before marriage is rendered legitimate by the subsequent marriage of the parents. This is not the case in England.
A child born during wedlock is legitimate, although the date of conception may be before marriage. A child born after the death of its mother is held to be legitimate. A child may, as Taylor remarks, be conceived before marriage, and born after the death of the mother, and yet be legitimate, though neither conceived nor born in wedlock.
The Code Napoleon prohibits the contraction of a second marriage until ten months after the death of the first husband; and this is also the case in Germany. The Anglo-Saxon law prohibits remarriage for twelve months. In Britain no time is fixed by law.
Duration of Pregnancy.—The consideration of this subject is of importance in its relation to the legitimacy of a child.
The natural period of human gestation is usually stated at forty weeks, ten lunar or nine calendar months, or 280 days. In Prussia, the period is extended to 302 days, and in the Code Napoleon to 300; in Scotland, ten months is held as the limit.
The duration of human gestation is subject to considerable variation; in [Pg 186] some females it is always protracted; in others, always premature. Several modes of calculation are adopted by women:
1. Ascertained date of impregnation from one coïtus.
2. Supposed sensations of female at time of conception.
3. Suppression of the catamenia. This is open to the objection, that causes other than that of impregnation may arrest them. The catamenia may be stopped by cold or other causes for two or three months, and then, before their return, pregnancy may occur, thus upsetting all calculations. The usual mode of calculation is from two weeks after the last menstruation, and the period so fixed is corrected by the time at which quickening occurs.
4. Period of quickening. (a) Quickening supposed when pregnancy is absent. (b) Pregnancy without quickening. (c) Variations in the time of its occurrence.
Whichever may be the mode of calculation adopted, it may be stated that, as a rule, the period of human gestation is from 275 to 280 days, and that cases of alleged pregnancy beyond 300 days must be received with considerable caution.
The pregnancy of the Countess of Gloucester was held, in the reign of Edward II., to be legitimate, although her husband had been dead one year and seven months at the date of the application.
Premature Births.—The question may be asked, At what period of gestation may a child be born viable—that is, capable of living and attaining to maturity? Seven months, or 210 days, is considered as the limit; but cases have been recorded of children born at six months being reared. The Roman law admitted the legitimacy of seven-months’ children. (For the Signs of Immaturity, see “Table of the Development of the Embryo,” pp. 35, 36.)
Superfœtation.—The term is used to imply the conception of a second embryo in a woman already pregnant, and the birth of two children at one time, differing considerably in their maturity, or of two births, a considerable period of time elapsing between each. The possibility of this occurrence has been doubted.
Churchill, in his work on Midwifery, writing on this subject says: “In conclusion, I would say—(1) That the theory of superfœtation is unnecessary to explain the birth of a mature fœtus and a blighted ovum, of a mature and immature fœtus born together or within a month of each other, or of fœtuses of different colours, as they may reasonably be supposed to be the product of one act of generation, or of two nearly contemporaneous. (2) That, in cases of double uterus, it is possible for a second conception to take place, and—judging from the subsequent birth of the second child in the only case on record—at a later period than the first. (3) That, in the remaining cases, where one mature child succeeded the birth of another after a considerable interval, we have no proof of a double uterus in any, and positive proof that in one case it was single; and that to the explanation of these cases no theory as yet advanced is adequate, that of superfœtation being opposed by physical difficulties which are unsurmountable in the present state of our knowledge.”
The late Dr. Matthews Duncan has, however, shown that the mouth of the [Pg 187] womb is not completely closed by conception, and the communication between the vagina and ovary is not destroyed for some months after impregnation, and that there is no impediment to the ascent of the spermatozoa. Galabin[16] records an instance of extra-uterine and uterine pregnancy occurring at the same time, the extra-uterine fœtus being advanced in development as compared with that in the uterus, and regards the condition as one of superfœtation.
The late Dr. Milne, while admitting this form of pregnancy as possible, though very rare, remarks: “This variety we should not think due so much to mechanical hindrances as to the absence of proper ovules. It would imply extraordinary vigour were perfect ovulation to be achieved for any length of time after impregnation.”
Evidence in relation to the above subjects may be required in actions for nullity of marriage, divorce, legitimacy, inheritance, pregnancy, and criminal assault.
Impotence.—By impotence is meant the incapacity for sexual intercourse, and applies both to the male and female; but the term is more especially used in reference to the former.
Sterility.—Sterility denotes the incapacity for procreation of children; is also applicable to both sexes, but more usually in reference to the female. A person may be impotent without being sterile, although the former is usually regarded as implying the latter. On the other hand, a person may be sterile without being impotent, the former not necessarily denoting the latter. In reference to nullity of marriage, if natural sexual relations are not and cannot be consummated, the marriage will be declared null and void, provided that such inability of consummation was unknown to the person bringing the action for nullity before marriage. Impotence is sufficient ground for bringing an action for nullity, provided it was present at the date of the marriage, that it is irremediable, and that the person bringing the action was not informed of it previously. Should, however, the marriage have been consummated and impotence develop later, there will be no grounds for such an action.
Impotence and Sterility in the Male.—This may arise from some organic defect of the organs or functional disorder. In reference to the former there are certain abnormalities of the male organs which have to be considered. Monorchids, men in whom one testis is absent from the scrotum, are not necessarily impotent or sterile; nor are cryptorchids, where both testes are undescended. In many of these cases spermatozoa are absent from the seminal fluid with consequent sterility; on the other hand, procreation has taken place, proving that cryptorchids are not necessarily sterile.
Absence of the penis may be the result of want of development, injury, [Pg 188] disease, or operation. The penis may be present but attached in its whole length to the scrotum; this may be remedied by operation.
Epispadias, so often associated with ectopion vesicæ, as a rule renders an individual impotent and sterile. On the other hand, hypospadias does not necessarily bar procreation; it will depend largely upon the position of the urethral opening, and the possibility of its being remedied by operation.
Removal or destruction of both testes renders a man sterile eventually, but not necessarily impotent.
Functional disorder due to disease may give rise to impotence, although the organs may remain anatomically perfect. Diseases such as diabetes and influenza, neurasthenia, tabes dorsalis, myelitis, mumps, and orchitis, and injuries to the head may be causative factors in impotence.
The capacity for sexual intercourse is influenced to a varying degree by age. Sexual capacity is regarded as coincident with puberty. In judging the sexual capacity of a youth, age is of less moment than the degree of physical development. I have seen a male child of five years of age with as complete development of the sexual organs as an adult, and with a deep voice. At the other extreme of life it is impossible to lay down any definite limit to sexual capacity. Although it is regarded as diminishing with age, yet there are many instances of procreative power in men of an advanced age.
The principal points for consideration in reference to impotence and sterility in the male are: (a) Does the condition prevent the secretion of semen? (b) Does it prevent the conveyance of semen to the vagina?
Impotence and Sterility in the Female.—As in the male, these may be associated with organic defect or functional disorder. The external organs may be absent, with or without the internal. The vagina may be wanting through lack of development, or it may be obstructed by mal-development or the result of disease. Again, the external organs may be present, but the internal absent in whole or part. The hymen may be imperforate, or unusually tough. Diseases of the uterus often give rise to sterility. Vaginismus, in which attempts at coïtus cause painful spasm, may prevent intercourse. In reference to functional disorders are to be noted extreme debility, constant leucorrhœa, dysmenorrhœa, menorrhagia, and amenorrhœa, all of which may be associated with or causative factors in sterility. Emotional psychical conditions may prevent sexual intercourse in women. General diseases, however, do not necessarily prevent intercourse, as the woman may remain a passive agent, neither is bodily deformity always a barrier to the act.
The advent of sexual capacity in women is regarded as coincident with the onset of the menses, about fourteen years of age, but pregnancy has been known to take place prior to the first menstrual period. The age at which the menses first appear varies in no small degree. It has been known to occur during the first year of life, and pregnancy has been [Pg 189] known to occur as early as the eighth year. The menopause in women is regarded as coincident with loss of procreative power. Women as a rule cease to menstruate at forty-five years of age, but in not a few the function persists until fifty, in exceptional cases to a more advanced age. It is rare for a woman to bear children after the menopause, but exceptions have been known to take place.
In the case of a husband seeking a nullity of marriage on the grounds of impotence or sterility in his wife, the question at issue is not whether she can bear children, but can she permit sexual intercourse? Many conditions which cause sterility in the woman need not render her impotent, and unless the latter obtains a nullity of marriage would not be allowed. Further, the conditions which render the woman impotent must be permanent and irremediable.
The question of survivorship is not infrequently raised when a mother and her new-born infant are found dead, or where several persons have perished by a common accident. In the first case the mother is generally presumed to have lived longest; and this presumption may be borne out by the fact of the delivery being premature, or if there be considerable disproportion between the size of the child and the maternal passages. As pointed out before, important civil rights may depend upon the question as to the live birth of an infant; and the husband‘s rights to be tenant to the courtesy will, of course, depend upon the view taken as to the probable survivorship or not of the child.
With regard to the second question, much will depend upon the relative ages and strength of the individuals. Sex will also have to be taken into consideration. In the case of one or more persons found dead, either from wounds or other causes, the fact of some being warm and others cold, the presence of the rigor mortis in one and absence in the other, will point to the probable survivorship. The severity of the wounds and injuries to large arterial trunks must also be considered. (See test case, Underwood v. Wing, 1 Jur. N.S. 169.) In this case a man, his wife, and three children were washed overboard and drowned, one child, however, being seen alive a few minutes after the others were submerged. The question at issue was, Did the husband survive the wife, or the wife the husband? and on this Wightman, J., in summing up, said: “We may guess, or imagine, or fancy, but the law of England requires evidence, and we are of opinion that there is no evidence upon which we can give a judicial opinion that either survived the other; in fact, we think it unlikely that both did die at the same moment of time, but there is no evidence to show who was the survivor.” Verdict for the plaintiff.
A medical man is liable to a civil action for damages who, by a culpable want of care and attention, or by the absence of a competent degree of skill and knowledge, causes injury to a patient. And it is not [Pg 190] necessary that the patient should have employed or was to have paid him, provided always that there be no negligence or carelessness on the part of the patient. Lord Chief-Justice Tindall remarks: “Every person who enters into a learned profession undertakes to bring to the exercise of it a reasonably fair and competent degree of skill.” It has also been decided that if the defendant acted honestly, and used his best skill to cure, and it does not appear that he thrust himself in the place of a competent person, it makes no difference whether he was at the time a regular physician or surgeon or not (R. v. Van Butchell; R. v. Williamson, &c.). A surgeon does not undertake to perform a cure, nor does he profess to bring the highest professional skill into the consideration of the case; but he does undertake to bring a fair and reasonable amount. The degree of skill required by law is good common sense, or such knowledge as the operator had, joined with a good purpose to help the afflicted, even if such interference rendered the patient a cripple for life. “It would be dreadful,” says Hullock, B., “if every time an operation was performed an individual was liable to have his practice questioned.” “So, if a physician or surgeon give his patient a potion or plaster to cure him, which, contrary to expectation, kills him, this also is neither murder nor manslaughter, but misadventure.” A medical man is only liable for gross negligence, not for every slip he may make; but the distinction between criminal and actionable negligence cannot be defined; but it appears that the negligence must be so gross as to come under the legal meaning of the word “felonious.” (See p. 82.)
Human ingenuity is not wanting among those who, for private ends, pretend to be suffering from disease. The soldier or sailor, anxious to escape the dangers of active service, finds a ready means of evading his duties by shamming; the prisoner, in order to lighten the burden of his punishment, does the same. A man declares himself impotent to save the expense of keeping an alleged bastard child, or to avoid punishment for rape. Beggars appeal to the public by feigning some painful disease, and incautious benevolence becomes the dupe of the clever impostor.
Any attempt at classification is here out of the question, nor does it appear necessary to give a long list of diseases which have been feigned, or the means that have been employed by artists in deception. To give some general hints for guidance is all that will be attempted here, leaving matters of detail to the acumen of the medical examiner, who, if in active practice, will have many opportunities of testing his powers of discernment:
1. Never be satisfied with one visit, but pay a second at a short interval, and unannounced.
2. Have the patient carefully watched in the interval of your visits.
3. Examine each organ of the body separately, carefully comparing the state of each with the symptoms described by the patient. [Pg 191]
4. Note the discrepancies in the statements of the patient as to his symptoms and their known occurrence in real disease.
5. Sometimes ask questions the reverse of his statements, or take his statements for granted, when in all probability he will contradict himself.
6. Remove all bandages and other dressings.
7. The administration of sham physic, or the suggestion of some heroic mode of treatment; the application of the actual cautery may have a beneficial effect.
8. Pay little attention to the reports of bystanders, or of the culprit‘s fellow-prisoners.
9. Anæsthetics may be employed, if necessary, for the purpose of detection.
10. The motives of deception should be inquired into, and borne in mind, in the examination of all cases.
The existence of certain diseases may be claimed as a bar to active service, both in a civil and in a military capacity; and the opinion of a medical man may be required as to the fitness or unfitness of the individual for the service from which he claims exemption. In giving certificates of this nature, the medical practitioner cannot be too guarded in wording them; and each case must be treated on its merits, so that strict justice may be done.
Among the diseases which may incapacitate a man for active employment may be mentioned—syphilis; hernia; phthisis; affections of the eyes, attended with dimness of vision, or colour blindness; varicose veins; and some other diseases.
Although a medical man, as a rule, should refuse to draw up a will, still there are occasions when his doing so may save much litigation and expense. The following directions may therefore be of use:
1. Let the wishes of the testator be expressed in the plainest and simplest words, avoiding all expressions that seem to admit of another meaning than the one intended.
2. All alterations in the will should be initialled.
3. Do not scratch out a word with a knife, and no alteration must be made after the will is executed.
4. Two witnesses are necessary, who must both be present and sign the following attestation at the end of the will, or on each sheet if more than one sheet of paper be used: “Signed by the testator (or testatrix, as the case may be) in the joint presence of us, who thereupon signed our names in his (or her) and each other‘s presence.”
5. Add address of witnesses.
6. A clause appointing an executor should be inserted thus: “And I appoint J. B. executor of this my will.”
7. Begin, “This is the last will of me, W. B. of S.”; and end, “and I
revoke all former wills and codicils.”
Dated this ___________ day of
______________ one thousand, &c.
In the whole range of medical jurisprudence there is no subject more interesting, more difficult, or more important than the diagnosis of insanity, and its relation to the criminal responsibility of individuals. It is impossible, in the short space at our disposal, to do more than to offer a few remarks which may assist the student in the elucidation of some of the most important cases which may engage his attention.
Legal Definitions.—Three forms of mental disorder are recognised in law:
1. A nativitate, vel dementia naturalis—idiocy or imbecility.
2. Dementia accidentalis, vel adventitia—acquired general insanity, either temporary or permanent, lunacy.
3. Dementia affectata, acquired madness
from intoxication, &c.
(See “Delirium Tremens,” p. 205.)
Under the term lunacy are included the mania, monomania, and dementia of medical writers. Another term frequently used in legal proceedings, the meaning of which it is not easy to give, is “non compos mentis,” unsoundness of mind. According to the late Forbes Winslow, “unsoundness of mind is not lunacy” in the legal acceptance of the phrase. This term was first used in a Statute passed in the reign of Henry VIII., relating to the punishment of treasonable offences, and is defined by the early law text-books to be strictly one who gaudet lucidis intervallis—a definition not psychologically exact. The phrase “unsoundness of mind” was first used by the late Lord Eldon to designate a state of mind not exactly idiotic, and not lunatic with delusions, but a condition of intellect occupying a place between the two extremes, and unfitting the person for the government of himself and the management of his affairs.
The above definition has been acted upon by other judges—Lyndhurst, Brougham, &c. As a rule, a medical witness will consult his own interest in not attempting to define insanity, bearing in mind the philosophic caution of Polonius, who, when addressing Hamlet‘s mother, says—
Since the trial and acquittal of MacNaughton on the ground of insanity, the doctrine of the knowledge of abstract right and wrong has been changed to a knowledge of right and wrong in relation to the particular act of which the person is accused, and also at the time of committing it.
It has also been held that, on the assumption that a person labours under partial delusion only, and is not in other respects insane, he must be considered in the same situation as to responsibility as if the facts, with respect to which the delusion exists, were real. For example, if, under the influence of delusion, he supposes another man to be in the act of attempting to take his life, and he kills that man, as he supposes, in self-defence, he would be exempt from punishment. If his delusion were that the deceased had inflicted a serious injury on his character and fortune, and he killed him in revenge for such supposed injury, he would be liable to punishment. “Here,” says Maudsley, “is an unhesitating assumption that a man, having an insane delusion, has the power to think and act in regard to it reasonably, ... that he is, in fact, bound to be reasonable in his unreason, sane in his insanity.” Yet this was the doctrine laid down by the judges in answer to certain questions propounded by the House of Lords after the acquittal of MacNaughton (see Maudsley‘s Responsibility in Mental Disease, pp. 88 et seq.).
As laid down by English lawyers, madness absolves from all guilt in criminal cases. Where the deprivation of the understanding and memory is total, fixed, and permanent, it excuses all acts; so, likewise, a man labouring under adventitious insanity is, during the frenzy, entitled to the same indulgence, in the same degree, as one whose disorder is fixed and permanent (Beverley‘s Case, Co. 125, Co. Litt. 247, 1 Hale 31). “But the difficulty in these cases is to distinguish between a total aberration of intellect and a partial or temporary delusion merely, notwithstanding which the patient may be capable of discerning right from wrong; in which case he will be guilty in the eye of the law, and amenable to punishment.”[17]
Lord Hale, who first pointed out the distinction to be drawn between total and partial insanity, offered the following as the best test he [Pg 194] could suggest: “Such a person, as labouring under melancholy distempers, hath yet as great understanding as ordinarily a child of fourteen years hath, is such a person as can be guilty of felony.” (On this subject, see R. v. Ld. Ferrers, 19 St. Tr. 333; R. v. Arnold, 16 St. Tr. 764, &c.)
To excuse a man from punishment on the ground of insanity, it appears that it must be distinctly proved that he was not capable of distinguishing right from wrong, and that he did not know, at the time of committing the crime, that the offence was against the laws of God and nature (R. v. Offord, 5 C. & P. 186).
I shall here quote from Macdonald‘s Criminal Law of Scotland: “Insanity or idiocy exempts from prosecution. But there must be an alienation of reason such as misleads the judgment, so that the person does not know ‘the nature of the quality of the act’ he is doing, or if he does know it, that he does not know he is doing what is wrong. If there be this alienation, as connected with the act committed, he is not liable to punishment, though his conduct may be otherwise rational. For example, if he kill another when under an insane delusion as to the conduct and character of the person—e.g. believing that he is about to murder him, or is an evil spirit,—then it matters not that he has a general notion of right and wrong. For, in such a case, ‘as well might he be utterly ignorant of the quality of murder.’ He does the deed, knowing murder to be wrong, but his delusion makes him believe he is acting in self-defence, or against a spirit. Nor does it alter the effect of the fact of insanity at the time, that the person afterwards recovers.... But the alienation of reason must be substantial. Oddness or eccentricity, however marked, or even weakness of mind, will not avail as a defence. Even monomania may be insufficient as a defence, where the delusion and the crime committed have no connection, or where the person, though having delusions, was yet aware that what he did was illegal.”
Mere moral insanity—where the intellectual faculties are sound, and the person knows what he is doing, and that he is doing wrong, but has no control over himself, and acts under an uncontrollable impulse—does not render him irresponsible (R. v. Burton, 3 F. & F. 772). Some medical writers contend that there are two forms of insanity—moral and intellectual. The law only recognises the latter, owing probably to the difficulty of distinguishing between so-called moral insanity and moral depravity. Taylor says: “Further, until medical men can produce a clear and well-defined distinction between moral depravity and moral insanity, such a doctrine, employed as it has been for the exculpation of persons charged with crime, should be rejected as inadmissible.”
The day may not be far distant when the term “moral depravity” will be unknown, and future generations, ceasing to believe in absurd superstitions, will come to look on crime as the result of disease of the brain, and learn to treat, instead of to punish, the morally diseased. (For a full discussion of this subject the reader is referred to the works of Dr. Henry Maudsley.)
The fact of the sanity or insanity of the prisoner at the time the crime was committed is left to the jury to decide, guided by the [Pg 195] previous and contemporaneous acts of the party; and it has been laid down by Lord Moncreiff in Scotland, and Lord Westbury in England, that the mental soundness or unsoundness of any individual is to be decided by the jury on the ordinary rules of every-day life, and that on these principles they are as good judges as medical men. The whole tendency of legal practice, when dealing with the plea of insanity, is to entirely ignore the medical evidence. On the question of medical evidence in cases of insanity, Doe J., of New Hampshire, remarks: “At present, precedents require the jury to be instructed by experts in new medical theories, and by judges in old medical theories,” and that in this “the legal profession were invading the province of medicine, and attempting to install old exploded medical theories in the place of facts established in the progress of scientific knowledge. If the tests of insanity are matters of law, the practice of allowing experts to testify what they are should be discontinued; if they are matters of fact, the judge should no longer testify without being sworn as a witness, and showing himself qualified to testify as an expert.”
Lunacy—What Constitutes? (8 and 9 Vict. c. 100, secs. 90 and 114).—Imbecility and loss of mental power, whether arising from natural decay, or from paralysis, softening of the brain, or other natural cause, and although unaccompanied with frenzy or delusion of any kind, constitute unsoundness of mind, amounting to lunacy within the meaning of 8 and 9 Vict. c. 100 (R. v. Shaw, 1 C.C. 145).
The above is the last definition of lunacy up to 1875; but as the law on this subject is so constantly changing, the student will find it best to consult the Law Reports from time to time. (See the account in the case of R. v. Treadaway, Law Reports. Also the Lancet, on the same case, vol. i. 1877.)
For some valuable remarks on the subject of the irresponsibility of madmen, the student is referred to the works of Maudsley, Pritchard, Ray, Hoffbauer, Georget, and others.
The following suggestions are offered for consideration on this subject:
1. Was the act an isolated event in the life of the culprit? Has it the appearance of spontaneity, or was it the culminating point of a life spent in so-called criminal acts?
2. Absence of a motive for the committal of the deed.—The absence of an apparent motive is no proof of an unsound mind; the moving principle may be “the conscious impulse to the illegal gratification of a selfish desire.”
3. The presence or absence of a well-concerted plan of action is a diagnostic sign of little value.—Casper remarks that “only in one case can the examination of the systematic planning of the deed afford any information, and that is when these plans and preparations themselves evince the stamp of a confused intellect, and betray the hazy consciousness, the mental darkness, in which the culprit was involved.” [Pg 196]
4. A dominant delusion may be so concealed as to be for a time undiscoverable.—The case of the man who gave no indication of his madness till he was asked to sign the order for his release, when he signed Christ, is an example how carefully a delusion may be concealed even during a most careful examination. Questions directed to this point showed that he laboured under all the errors which such a delusion might suggest.
5. It may “easily be conceived that insane persons, whose unreason affects only one train of thought more or less restricted, yet labour in other respects under disorders of feeling which influence their conduct and their actions and behaviour without materially affecting their judgment: and that many of such deranged persons, who often conduct themselves tolerably well in a lunatic asylum, and while living among strangers with whom they have no relations, and against whom they have no prejudices or imaginary reason of complaint; subjected, besides, to the rules of the house and to an authority that nobody attempts to dispute; would, nevertheless, if restored to liberty and residing in the midst of their families, become insupportable, irritable at the slightest contradiction, abusive, impatient of the least remark on their conduct, and liable to be provoked by trifles to the most dangerous acts of violence. If, under such circumstances, a lunatic should commit any act of injury or serious damage to another, would it be just to punish him; because it cannot be made apparent that the action has any reference to, or connection with, the principal delusion which is known to cloud his judgment, it being apparent that his moral faculties have undergone a total morbid perversion?”
6. Insanity with Lucid Intervals.—Haslam, Ray, and others appear to deny the possibility of lucid intervals; but M. Esquirol, on the other hand, fully recognises the existence of this form of insanity. In a legal sense, a temporary cessation of the insanity constitutes a lucid interval, but the cessation must be complete, and not merely a remission of the symptoms. The interval must be of some duration; and when continuous insanity has been proved, the onus of proving a lucid interval in civil cases rests with the party trying to support the validity of a deed executed during the alleged interval. “If you can establish,” says Sir W. Wynne, “that the party afflicted habitually by a malady of the mind has intermissions, and if there was an intermission of the disorder at the time of the act, that being proved is sufficient, and the general habitual insanity will not affect it, but the effect of it is this—it inverts the order of proof and presumption; for, until proof of habitual insanity, the presumption is that the party agent, like all human creatures, was rational; but when an habitual insanity in the mind of the person who does the act is established, then the party who would take advantage of the fact of an interval of reason must prove it.” In civil cases the law recognises the validity of wills made during lucid intervals, and has even taken the reasonableness of a will as a proof of a lucid interval.
7. Have measures been taken by the culprit to escape punishment? [Pg 197]
The classification of insanity adopted here is that given by Ray, and is sufficient for all practical purposes:
| I N S A N I T Y. |
Defective development of the faculties. |
Idiocy | 1. Resulting from |
| congenital defect. | |||
| 2. Resulting from an | |||
| obstacle to the | |||
| development of the | |||
| faculties supervening | |||
| in infancy. | |||
| Imbecility | 1. Resulting from | ||
| congenital defect. | |||
| 2. Resulting from an | |||
| obstacle to the | |||
| development of the | |||
| faculties supervening | |||
| in infancy. | |||
| Lesion of the faculties subsequent to their development. |
Mania | 1. Intellectual— | |
| (a) General. | |||
| (b) Partial. | |||
| 2. Affective— | |||
| (a) General. | |||
| (b) Partial. | |||
| Dementia | 1. Consecutive to mania, | ||
| or injuries of | |||
| the brain. | |||
| 2. Senile, peculiar to | |||
| old age. |
Under this heading may be included idiocy, cretinism, imbecility, feeble-mindedness, and moral imbecility.
Idiocy is congenital, and was defined by Esquirol thus: Idiocy is not a disease, but a condition in which the intellectual faculties are never manifested, or have never been developed sufficiently to enable the idiot to acquire such an amount of knowledge as persons of his own age, and placed in similar circumstances with himself, are capable of receiving. Idiocy commences with life, or at an age which precedes the development of the intellectual and affective faculties, which are from the first what they are doomed to be during the whole period of existence. Since the days of Esquirol, much improvement has been made in the care and treatment of the idiot; and it appears that he is capable of some, though in most cases slight, mental culture. The cases in which improvement takes place probably belong to imbecility, leaving the idiot in the same condition as described by Esquirol.
Cretinism differs from idiocy in being endemic; it is also more curable, or at least more susceptible of improvement, than the latter. In the idiot the malady is congenital; the cretin, on the other hand, may to all appearances be free from disease for a time. “Every cretin is an idiot, but every idiot is not a cretin; idiocy is the more comprehensive term, cretinism is a special kind of it.” The enlarged thyroid gland, high-arched palate, and brown or yellow colour of the skin, are characteristic of the cretin. Local causes are at work in the production of cretinism; e.g. defective function of the thyroid gland.
The idiot is usually cunning, mischievous, and dirty in his habits. [Pg 198]
The derivation of the word idiot, from the Greek, ίδιώτης— a private person, or an ill-informed ordinary fellow—is peculiar. A person suffering from any form of mental unsoundness, and thereby rendered incapable of taking care of himself or of his property, was formerly called by English law “an idiot,” and this word was not infrequently joined with “fatuus” in old writs.
Imbecility.—This is a minor form of idiocy, and may or may not be congenital. It admits of considerable degrees of intensity. Imbeciles exhibit mental defection, rendering them incapable of managing themselves or their affairs, and imbecile children are incapable of being taught to do so.
Feeble-mindedness is a lesser degree of mental defection than imbecility. It may exist from birth or an early age. Such persons require care and control for the protection of themselves and others. They may be incapacitated from acquiring the knowledge imparted in ordinary schools.
Moral imbeciles exhibit moral defects which render them vicious in behaviour, and they often exhibit criminal tendencies, which are not affected by punishment.
The Mental Deficiency Act of 1913 provides for their care. Such a person may be either sent to an institution or placed under special guardianship by the parent or guardian, if an idiot or imbecile; or by the parent when, though not an idiot or imbecile, the person affected be under the age of twenty-one years. If in addition to being a defective, the person is neglected, abandoned, or without means of support; or cruelly treated, guilty of a criminal offence, or liable to be sent to an industrial school, or under imprisonment, detained in an industrial school, inebriate reformatory, or institution for lunatics, or habitual drunkard within the meaning of the Inebriates Act; or in whose case proper notice has been given by the Local Education Authority; or who is in receipt of relief at the time of giving birth to an illegitimate child, or pregnant of such child.
Certificates required.—In the case of a parent or guardian who desires to place a mentally defective person under guardianship, two medical certificates are necessary, one of which must be from a medical man approved by the Local Authority or Board. If the person be not an idiot or imbecile, the certificates must be signed by a Judicial Authority, after such inquiry as he thinks fit. A defective to be dealt with otherwise than by parent or guardian, is so under an order by a Judicial Authority on a petition presented under the Act, an order of a Court if guilty of a criminal offence, or an order of the Secretary of State if detained in prison, a criminal lunatic asylum, or reformatory.
The order of a Judicial Authority may be obtained by petition of any relative or friend, or an officer of the Local Authority authorised under the Act for the purpose. Two medical certificates must accompany the petitions, one of which must be signed by a medical man approved by the Local Authority or Board; or, when a medical examination cannot be carried out, a certificate to that effect must be presented, and a [Pg 199] statutory declaration made by the petitioner and one other person, who may be one of the medical certifiers, stating the class to which the defective belongs. Upon receiving the certificates the Judicial Authority interviews the defective. When the petition is presented by a parent or guardian, the Judicial Authority, if satisfied, may issue an order for the defective to be placed in an institution or appoint a guardian. If the petitioner be not parent or guardian, consent in writing of one or other must be obtained, without which the order must not be made, unless the parent or guardian withhold their consent unreasonably or are not to be found. If the Judicial Authority be not satisfied, he may postpone the order, or refuse it.
When the order is made by a Court, the Court must be satisfied, on medical evidence, that the person is a defective.
Two medical certificates are necessary when the Secretary of State makes an order.
The order remains in force for a year, may be renewed for a second year, and then for periods of five years.
The onset of insanity may be gradual or sudden. More commonly the onset is gradual, and manifested by alterations of emotion and conduct, which may for a considerable period precede any impairment of intelligence. Periods of depression may alternate with periods of excitement. Irritability and instability of temper manifest themselves, and lead relatives and friends to become suspicious of the change that is the herald of serious mental impairment. Lack of interest in environment, business, or the usual pleasurable pursuits, also a tendency to personal seclusion manifest themselves, and changeability of the affections, more often to those nearly related, are not uncommon. Sooner or later the capacity to conduct business and allied pursuits becomes enfeebled, and the power of judgment lessened; depression begets apprehension and a dread of impending ruin in this world or in the world to come. Marked indecision and vacillation of action is quite common. Delusions follow, mostly of persecution, in the form of attempts to cause ruin or poisoning. Delusions associated with the special senses are common, particularly of hearing, supposed voices urging the committal of certain actions, or expressive of derision; of vision, by which objects are seen which are non-existent; of taste, imparting the idea of poisoning; of touch and pain, invoking peculiar sensations; of smell, conveying the idea that food, the body, &c., exhale disgusting odours.
Associated with the onset of insanity, and remaining permanently, are three special distortions of perceptions—viz. illusions, hallucinations, and delusions. So long as the first two can be reasoned upon and rejected, judgment remains. At one or other time the afflicted person becomes so affected by them that they become realities, and are accepted as true and existent; then the judgment is perverted, and the person is said to suffer from a delusion.
Illusions.—An illusion is a false perception, a perversion of [Pg 200] the senses, a mockery, false show, counterfeit appearance. The false perception is, however, invoked by some external appearance.
Hallucinations.—Hallucinations are perverted sensations and perceptions, for the production of which no external impulse is present. The person may complain of seeing horrible reptiles around, which are not present. So long as the reasoning faculties are capable of dispelling the alleged reality of the hallucination and rejecting it, it remains but an hallucination.
If, however, it becomes accepted as a reality and the person becomes obsessed thereby, it becomes a delusion.
Delusions.—A delusion is a chimerical thought, an affection of the mind. It implies a disordered intellect. Delusions generally concern the insane person, his power, soul, &c. A delusion is a perverted idea of the mind in which there is belief in non-existent things or occurrences. Delusions may be based upon previous hallucinations, or arise out of erroneous conceptions.
Mania is the result of a morbid condition of the brain, and to express which “the term raving madness may be used with propriety, as an English synonym for mania. All maniacs display this symptom occasionally, if not constantly, and in greater or less degree.” Like other diseases, mania observes the same pathological laws. There is a period of incubation, during which the true state of the patient is in most cases misunderstood, or not appreciated. Mental exaltation may exist from the first onset of the disease, or the attack may be ushered in by a stage of gloom or despondency. The general health shows signs of impairment, the liver becoming sluggish, and the bowels confined or relaxed. In some cases a febrile condition of the system is among the premonitory symptoms of an attack of mania. The physical health is not usually much affected during the paroxysm.
Dr. Conolly remarks that “even acute mania is not always accompanied by the ordinary external signs of excitement. It would seem as if we had yet to learn the real symptoms of cerebral irritation. Certainly, in recent cases of mania—cases which have lasted more than six weeks, and in young persons in whom I have seen the maniacal attack pass into dementia—I have known the most acute paroxysms of mania exist, rapid and violent talking, continual motion, inability to recognise surrounding persons and objects, a disposition to tear and destroy clothes and bedding, without any heat of the scalp or of the surface, without either flushing or paleness of the face, with a clean and natural appearance of the tongue, and a pulse no more than eighty or eighty-five.”
This may occur in some cases, but in the majority there is always some amount of physical derangement; the system, however, gradually becoming tolerant of the undue excitement to which it is subjected.
Following the classification adopted, Intellectual Mania will now be briefly considered under its two divisions—General and Partial. [Pg 201]
General Intellectual Mania.—By many medical writers general intellectual mania is divided into mania and melancholia. The mind in the former type of the disease is involved in the most chaotic confusion possible, and there is also considerable bodily derangement. The moral faculties become more or less affected, and the patient‘s social and domestic relations are greatly altered. At one time he is subject to violent fits of immoderate laughter, at another he is gloomy and taciturn; sometimes quiet and tractable, at others wild and excited, necessitating close confinement. He is haunted by wild delusions, which at times take entire possession of him, and under the influence of which he acts in the most extraordinary manner. In the latter—melancholia, or mania with depression—delusion may be absent, or, rather, for a time undetectable. The sufferer is gloomy, and troubled with unhappy thoughts, which sometimes lead him to self-destruction. He is sleepless, and rejects his food as unnecessary. He may be aroused for a short time by questions addressed to him, his replies to which are usually given correctly, most frequently in monosyllables; but the moment his questioner leaves him he relapses into his former gloomy state.
Partial Intellectual Mania.—The term monomania, first suggested by Esquirol, is now generally given to this variety of insanity. The patient, in the simplest form of this disorder, becomes possessed of some single notion, which is alike contradictory to common sense and to his own experience. Thus, he may fancy himself made of glass; and influenced by this idea, he walks with care, and in dread of being broken by contact with other bodies. In the case of an inmate at the City of London Asylum, the presence of a weasel in the stomach was stated by one woman. Esquirol mentions the case of a woman with hydatids in her womb, who believed that she was pregnant with the devil. Most of these strange fancies appear to be dependent on errors of sensation.
Monomaniacs are ready enough to declare their predominant idea; yet at times, and that without the occurrence of a lucid interval, they will as carefully conceal it. “In the simplest form of monomania, the understanding appears to be, and probably is, perfectly sound on all subjects but those connected with the hallucination. When, however, the disorder is more complicated, involving a longer train of morbid ideas, we have the high authority of Georget for believing that, though the patient may reason on many subjects unconnected with the particular illusion on which the insanity turns, the understanding is more extensively deranged than is generally suspected.”
Pinel first drew attention to this form of madness. Pritchard defines it as “consisting in a morbid perversion of the natural feelings, affections, inclinations, temper, habits, and moral dispositions, without any notable lesion of the intellect or knowing and reasoning faculties, and particularly without any maniacal hallucinations.” [Pg 202]
It is divided into—General Moral Mania. Partial Moral Mania.
General Moral Mania.—“There are many individuals,” says Pritchard, “living at large, and not entirely separated from society, who are affected in a certain degree with this modification of insanity. They are reputed persons of a singular, wayward, and eccentric character. An attentive observer will often recognise something remarkable in their manners and habits, which may lead him to entertain doubts as to their entire sanity; while circumstances are sometimes discovered on inquiry which add strength to this suspicion. In many instances it has been found that a hereditary tendency to madness has existed in the family, or that several relatives of the person affected have laboured under other diseases of the brain. The individual himself has been discovered to have suffered, in a former period of life, an attack of madness of a decided character. His temper and disposition are found to have undergone a change, or to be not what they were previously to a certain time; he has become an altered man, and the difference has perhaps been noted from the period when he sustained some reverse of fortune which deeply affected him, or the loss of some beloved relative. In other instances, an alteration in the character of the individual has ensued immediately on some severe shock which his bodily constitution has undergone. This has been either a disorder affecting the head, a slight attack of paralysis, or some febrile or inflammatory complaint, which has produced a perceptible change in the habitual state of his constitution. In some cases, the alteration in temper and habits has been gradual and imperceptible; and it seems only to have consisted in an exaltation and increase of peculiarities which were always more or less natural and habitual. Persons labouring under this disorder are capable of reasoning, or supporting an argument upon any subject within their sphere of knowledge that may be presented to them; and they often display great ingenuity in giving reasons for the eccentricities of their conduct, and in accounting for, and justifying, the state of moral feeling under which they appear to exist. In one sense, indeed, their intellectual faculties may be termed unsound—they think and act under the influence of strongly excited feelings; and persons accounted sane are, under such circumstances, proverbially liable to error, both in judgment and conduct.” (For interesting cases of this form of madness, see Ray‘s Jurisprudence of Insanity.)
Partial Moral Mania.—In the case of the unfortunate sufferers from this malady, one or two only of the moral powers are perverted.
This division admits of several subdivisions:—
Kleptomania.—A marked propensity to theft. “There are persons,” says Rush, “who are moral to the highest degree as to certain duties, but who, nevertheless, lie under the influence of some vice. In one instance, a woman was exemplary in her obedience to every command of the moral law except one—she could not refrain from stealing. What made this vice more remarkable was, that she was in easy circumstances, and not addicted to extravagance in anything. Such was the propensity [Pg 203] to this vice that, when she could lay her hands on nothing more valuable, she would often, at the table of a friend, fill her pockets secretly with bread. She both confessed and lamented her crime.”
Pyromania.—This consists in an insane impulse to set fire to everything—houses, churches, and property of every kind and description.
Erotomania and Nymphomania.—This is known as amorous madness, and consists in an inordinate and uncontrollable desire for sexual intercourse. The unfortunate victims of this disease often express the greatest disgust and repugnance for their conduct.
Homicidal Mania—In this form of madness the propensity to homicide is very great, and in most cases uncontrollable. In the case of the notorious Deeming, hanged in Australia in 1892 for the murder of his wife, an appeal was made from the finding of the Colonial Court by which he was tried to the Privy Council, on the ground of his being affected with homicidal mania. The plea was not sustained. (See the case of Henrietta Cornier, given by Pritchard, Ray, and others.)
The following suggestions may be of assistance in forming a diagnosis as to the existence or non-existence of this form of madness:—
1. Previous history of the individual.—Melancholy, eccentric, morose, &c.
2. Absence of motive.—Gain, jealousy, revenge, hatred, &c.
3. A number of victims are often sacrificed at one time.—The murderer, on the other hand, seldom sheds more blood than is necessary for his success.
4. Proceedings of the murderer before and after the crime.—Absence of attempts at concealment or escape on the part of the madman.
5. Character of the victims.—Not infrequently, in the case of madmen, their victims are those whom, when sane, they loved most, and to whom they were most attached.
Suicidal Monomania, or the Propensity to Suicide.—Much discussion has arisen on this subject. Suicide is not always the result of unsoundness of mind. Some, like M. Esquirol, are inclined to consider suicide as always a manifestation of insanity. In the present day, the dislike of coroners‘ juries to bring in any other verdict but that of “suicide whilst in a state of unsound mind” is proverbial.
This condition is associated with mental depression and delusions. In its simple form, marked depression of spirits, apprehension of evil, sleeplessness, loss of appetite, and impaired alimentation with constipation are evident.
Delusions of ruin, of the committal of acts contrary to the laws of God and man—“the unpardonable sin”—a marked inaptitude to carry on the ordinary duties of life, indecision, and often unutterable misery, are commonly exhibited. The delusions are fixed and may be multiple. They may comprise persecution, by friends or others; that things are happening which powerfully influence the person‘s life and body, or, as is often the case, concern religious matters, and everlasting punishment.
Suicidal tendencies are often present, and depend largely upon the [Pg 204] misery associated with the condition. Melancholics often conceal this tendency, or may exhibit it in varied ways so as to hide the method which has been definitely decided upon. Thus a person so afflicted may be found in possession of poison at one time, a pistol at another, a knife at another, when the real intention is that of drowning. Thus it is necessary to keep an extremely careful watch on melancholics. Homicidal tendencies are not common. In some cases the melancholia is combined with marked agitation. The face depicts misery, the eyebrows raised, and the person moves about incessantly, picking up objects and replacing them, moaning and uttering the same phrases expressive of misery and hopelessness, wringing the hands, and rocking the body to and fro.
In other cases stupor is predominant, and the person sits in silence and in the same attitude. Some resent interference, others are easily persuaded by their attendants to do certain acts, but when done relapse again into stupor. They manifest extreme apathy. Suicidal tendencies are a pronounced feature of such cases.
Melancholia and mania may alternate periodically, with lucid intervals intervening. The term circular insanity has been applied to this alternate character of the disease.
Dementia consists in a failure of the mental faculties, not congenital, but coming on during life. “A man,” says Esquirol, “in a state of dementia is deprived of advantages which he formerly enjoyed. He was a rich man who has become poor. The idiot, on the contrary, has always been in a state of want and misery.” In this state there is always more or less coherence, and maniacal paroxysms are not infrequent. In mania, incoherence may be present, but then it is characterised by sustained and violent excitement. In dementia, on the other hand, there is apparent torpor and exhaustion of the mental faculties. Closely allied to this form of mental unsoundness is that interesting disease known as “general paralysis of the insane,” or perhaps a better term, progressive paralysis of the insane. It is considered by some to precede the psychical derangement, a contrary opinion being held by others. General paralysis may accompany any of the forms of mental derangement, but it is generally preceded by a stage of melancholy. As the paralytic affection becomes more marked, there is a concurrent loss of memory and incapability of mental association, and all sense of duty is lost; the patient becomes careless as to his person, and dirty in his habits. He expresses himself as possessed of great property, and boasts of the wonderful deeds that he can or has accomplished. Gradually he sinks into a state of complete mental and physical decay. He cannot give expression to his thoughts, and has to be fed, the food being pushed into his mouth. The symptom which first attracts the attention, and which is perhaps the first order of sequence, is a modification in the articulation. “This is neither stammering nor hesitation of speech. It more closely [Pg 205] resembles the thickness of speech observable in a drunken man. It depends upon loss of power over the co-ordinate action of the muscles of vocal articulation.” If the tongue be now examined, it will be found that when it is protruded it is not inclined to one side, but that it is tremulous, and is protruded and withdrawn in a convulsive manner. Griesinger was the first to call attention to the fact, and his statement has since been confirmed, “that this motory disorder is at the commencement not so much paralytic as convulsive in its nature.” The gait becomes unsteady, the patient walks stiffly, and stumbles over the slightest unevenness in the floor. Step by step the paralysis progresses, till at last the unfortunate sufferer takes to his bed, on which he may lie for months. Sometimes, especially during the earlier stages, he may suffer from terrible delusions, from maniacal paroxysms, or from epileptic fits, the latter possessing certain peculiarities. The tongue during the fit is seldom bitten, which is so commonly the case in epilepsy; and the convulsions are not so general, being limited more to one side than to the other. It is also remarkable that each fit is in most cases followed by an increase of the mental derangement.
Pritchard recognises four stages of dementia or fatuity:—
First Stage.—Forgetfulness and impaired memory. This is common to old age. In most cases passing events produce little, if any, impression, whilst the past is remembered with tolerable freshness.
Second Stage.—Incoherence and unreason, characterised by a total loss of the reasoning faculty.
Third Stage.—Incomprehension. The person so affected is quite incapable of comprehending the meaning of the simplest question; and should he attempt to reply, his answer is generally remote from the subject.
Fourth Stage.—Inappetency. The animal instincts are lost. The unfortunate sufferer lives, and that is all, being scarcely conscious of life. Organic life is all that is left.
Delirium Tremens.—A temporary form of insanity, the result of excessive indulgence in spirituous liquors. The drunkard, under the effects of intoxication, “can derive no privilege from a madness voluntarily contracted, but is answerable to the law equally as if he had been in full possession of his faculties at the time” (1 Hale 32; Co. Litt. 247). The intoxication of the defendant may be taken as a mitigating circumstance, showing that the deed was unpremeditated. A person rendered incapable of using his reason by intoxication brought about by others, is not liable for his actions.
Simple Delirium.—Acts performed during attacks of certain diseases—fever, sunstroke, &c.—accompanied with delirium, do not render the individual liable to punishment; and wills made during the continuance of the disorder, if they contain no statement inconsistent with the known wishes and desires of the party during health, are valid, the law looking more to the good sense of the will as a proof of a lucid interval, than to the proved existence of such lucid interval. [Pg 206]
Somnambulist, &c.—This is an abnormal mental state, closely allied to that artificially produced and known under the names of mesmerism, hypnotism, electro-biology, &c. It is commonly known as “sleep-walking.” In this condition the mind appears to become enslaved by one train of ideas to the exclusion of all others; the somnambulist, thus deeply bent on the accomplishment of a definite end, takes no heed of those objects which are in no way connected with the dominant ideas in his mind. Hence, he walks safely past dangers which, when awake, would disconcert his judgment and weaken his will. Somnambulism appears also to be closely connected with epilepsy. In 1878, a man named Fraser was tried in Glasgow for the murder of his child by beating it against the wall. He was acquitted on the ground of being unconscious of the nature of his act by reason of somnambulism. He had sprung from an epileptic and insane stock; his mother died in an epileptic fit, and some of his other relatives were insane. Thus it appears, if the somnambulism be proved, the accused is exonerated from any responsibility connected with the act for which he is being tried. So also, if a person be suddenly aroused from a deep sleep—somnolentia or sleep-drunkenness—the question may be raised as to his responsibility for an act committed at the moment of awakening (R. v. Milligan). There cannot be a doubt but that if a person be suddenly aroused whilst dreaming, he may unconsciously commit acts, the outcome of his dream, which, unless the possibility of this condition be recognised, may entail severe punishment on him. This state is closely allied to that mental condition which sometimes occurs in epileptics immediately after a fit. But in this, as in cases of somnambulism, the facts of the case would have to be most carefully scrutinised.
The following hints may be of use as a guide in determining the responsibility or not of the accused:—
1. The person must be shown to have a general tendency to deep and heavy sleep, out of which he can only be aroused by a violent and convulsive effort.
2. Are there any circumstances which, happening before the individual went to sleep, would produce a train of disturbed thought not entirely composed by sleep?
3. Did the act occur during the usual hours for sleep?
4. Was the cause of the awakening sudden, and does the act bear throughout the character of unconsciousness?
5. What were the subsequent acts of the accused in relation to the deed? Did he try to evade responsibility? This must not have too much stress laid upon it, for the wretchedness of the sudden discovery may so overcome him, that he may seek to shelter himself from the consequences of an act for which he is legally but not morally responsible.
No person can be put under restraint unless the conditions required by the Lunacy Acts are fulfilled. The Acts of Parliament for this purpose [Pg 207] are the Lunacy Act of 1890 (53 Vict. c. 53) and that of 1891 (54 and 55 Vict. c. 65). Lunatics may be put under restraint by the following procedures, according to the particular case:—
Reception Order on Petition.—This is usually the procedure for private patients. The order for petition may be obtained from a specially appointed Justice of the Peace, Judge of County Courts, or Magistrate. A petition for the order must be presented to the Judicial Authority by the husband, wife, or relative of the alleged lunatic; if any other person apply, the reasons for this must be given. A petitioner must be twenty-one years of age or over, and must have seen the alleged lunatic within fourteen days before its presentation. A statement of particulars and two medical certificates must accompany the petition. The proceedings are private, and no one except the petitioner, the alleged lunatic, and any one person appointed by him, and the two medical men who have signed the certificates, may be present, unless by permission of the Judicial Authority. If the Judicial Authority be satisfied, he may make the order at once, even without seeing the patient, or he may appoint a time within seven days for inquiries and consideration. He may visit the alleged lunatic.
At the time of consideration of the petition he may adjourn it for not more than fourteen days, or he may make the order at the time. He may summon further witnesses, or dismiss the petition, giving his reasons for so doing in writing.
A reception order is valid for seven days from its date, unless the lunatic is certified by a medical man to be unfit for removal, when the order is extended until a medical certificate of fitness for removal is obtained, which is valid for three days.
The medical men signing the certificates must not be in partnership, as principal and assistant, or have any direct or indirect interest in the patient or his keeping (16 and 17 Vict. c. 96, sec. 4). They must make separate visits at different times for the purpose of examination. Each medical man must have examined the person within seven clear days before the presentation of the petition.
Each medical man must write clearly and in the proper place on the certificate: (1) The facts observed by himself as evidence of insanity, and (2) the facts observed by others as evidence of insanity. The name of his informant must be given.
One of the certificates should, whenever practicable, be under the hand of the usual medical attendant (if any) of the alleged lunatic. If not practicable, the reason must be given by the petitioner to the Judicial Authority. [Pg 208]
Neither of the certifying medical practitioners may be the father or father-in-law, brother or brother-in-law, sister or sister-in-law, partner or assistant of the other of them.
Great care should be taken to follow carefully the marginal directions on the certificate form. The most trivial omission will invalidate the certificate. The omission of the name of the street and number of the house is sufficient to set it aside. A medical man should remember that, although his certificate may have passed the scrutiny of the Commissioners, it is liable to be made the subject of discussion in a Court of law, and in cross-examination he will have to support the statements therein made.
The following certificate properly filled up by Dr. Millar of Bethnal House Asylum, is given in his book on Hints on Insanity, and may be taken as an example of a correct certificate at that time, the present form being slightly different:—
MEDICAL CERTIFICATE
PROPERLY FILLED UP
| 1. Here set forth the | I, the undersigned, |
| qualification entitling the | John Millar, being a (¹) |
| person certifying to practise | Licentiate of the |
| as a physician, surgeon, or | Royal College of Physicians, |
| apothecary. | Edinburgh, |
| and being in actual practice as | |
| 2. Physician, surgeon, or | a (²) Physician, hereby certify |
| apothecary, as the case | that I, on the third day of |
| may be. | November, One thousand eight |
| hundred and eighty-eight_, a | |
| 3. Here insert the street and | (³) 600 - Cambridge Road, |
| number of the house (if | Bethnal Green, in the county of |
| any), or other like particular. | Middlesex, separately from any |
| other medical practitioner, | |
| personally examined | |
| James Thompson, sen., of | |
| 4. Insert residence, and | (⁴) 600 Cambridge Road, |
| profession or occupation | Bethnal Green, gentleman, |
| (if any). | and that the said James Thompson, |
| sen., is a person (⁵) | |
| 5. Lunatic, or an idiot, | of unsound mind, and a proper |
| or a person of unsound mind. | person to be taken charge of, and |
| detained under care and treatment; | |
| and that I have formed this opinion | |
| upon the following grounds, viz.:— | |
| 6. Here state the facts. | 1. Facts indicating insanity |
| observed by myself (⁶)— | |
| He is incoherent in his | |
| conversation, violent in his | |
| conduct, and quite unable to | |
| take care of himself. | |
| 7. Here state the information, | 2. Other facts (if any) |
| and from whom. | indicating insanity |
| communicated to me by | |
| others (⁷)— | |
| His son, James Thompson, jun., | |
| informs me that he has | |
| threatened to commit suicide, | |
| and has twice attempted it with | |
| a razor. | |
| (Signed) Name—JOHN MILLAR | |
| Place of abode—Bethnal House, Bethnal Green. | |
| Dated this third day of November, One thousand eight hundred and eighty-eight. |
|
Table relating to “Facts” of Insanity,
(compiled from Millar.)
| Facts offering no Evidence of Insanity. |
| 1. Refuses to take her medicine and resists |
| in every way; closes her teeth; threatens |
| to strike every one near her; obliged to |
| use the strait-waistcoat. |
| 2. Violent in her temper, and very abusive. |
| 3. Moody and irritable temperament, and of |
| weak memory in many particulars. |
| 4. General restlessness of manner; considers |
| himself heavily involved in debt to many |
| thousand pounds; says he has been ruined |
| by the Government, and that he intends |
| prosecuting the Admiralty for £5000 damages. |
| Vague and Irrelevant Facts. |
| 1. She is suspicious of her husband; says he |
| keeps bad company; she is most irritable and |
| jealous, and takes stimulating drinks to a |
| dangerous and exciting extent. |
| 2. Obstinate; has the manner and appearance |
| of an insane person; complained of her head; |
| refused her food, and would not go |
| downstairs; melancholy. |
| 3. He has imperfect sight; good hearing and |
| taste; he is unable to speak; his gait is |
| ape-like, and the skull-bones seem to have |
| fallen together from the want of cerebral |
| development. He will occasionally slap his |
| face and strike his hands; sometimes makes |
| a howling noise. |
| 4. She is very good-tempered; but day and |
| night she talks almost incessantly; |
| occasionally sings. She says she comes from |
| Otaheite, and relates stories of thos |
| around her doing absurd things. |
| Good Facts. |
| 1. She states that she is a lost person and |
| without hope of forgiveness; that she will |
| be taken to prison, and die a miserable |
| death; that the devil whispers in her ear |
| that she has committed the unpardonable sin. |
| 2. Great taciturnity; complete seclusion |
| from society; aversion to cleanliness; |
| wandering about the streets at improper hours. |
| 3. He states that he is a Prince of France; |
| that he possesses a palace, and has recently |
| had two fortunes left him (he cannot tell by |
| whom)—one of £400,000, the other of |
| £600,000; that he is going to Liverpool, a |
| distance of 150 miles, with a horse and |
| cart, which will take him four hours to go and |
| eight to return. |
| 4. Inability to hold any rational |
| conversation; her manner and conduct are |
| totally at variance with her usual habits. |
[Pg 210] The following are examples of “Facts” sent back to be amended by the Commissioners—the emendations in italics:—
1. Incoherence, perversion of facts, delusion. Fancies that he possesses large amounts of money which people have secreted from him.
2. Says her sister lives in Chiselhurst, and she fears she is dying. She took great notice of my feet, and remarked that they were very large. Query by Commissioner—Are these delusions? Her sister does not live at Chiselhurst, and is perfectly well; my feet are not large.
3. General restlessness of manner; considers himself heavily involved in debt to many thousands of pounds, whereas his debts do not amount to a few hundreds; says he has been ruined by the Government, whereas he has only been dismissed from his appointment on account of his incapacity; and he intends prosecuting the Admiralty for £5000 damages, he having no real ground of action. (This was twice sent back for correction, the first correction being—By these statements I was satisfied that the patient was of unsound mind, and by his general conduct during examination. Finally amended as given above.)
(a)—a Justice of the Peace for ____, or His Honour the Judge of the County Court of ____, or ____ Stipendiary Magistrate for ____.
(b) Full postal address and rank, profession, or occupation.
(c) At least twenty-one.
(g) Some day within 14 days before the date of the presentation of the petition.
(h) Here state the connection or relationship with the patient.
(k) Full Christian and surname.
53 Vict. c. 5.—Sched. 2, Form 1.
PETITION FOR AN ORDER FOR RECEPTION
OF A PRIVATE PATIENT
In the Matter of_______________________________
a person alleged to be of unsound mind.
To (a)____________________________________
____________________________________
____________________________________
The Petition of__________________________________________
of (b)______________________________________________
______________________________________________
in the County of_________________________________________
1. I am___________(c) years of age.
2. I desire to obtain an Order for the Reception of
________________________________________________
as a person of unsound mind, in the Haydock Lodge Licensed House,
situate at Newton-le-Willows, Lancashire.
3. I last saw the said__________________________________
at______________________________________________________
on the (g)_______day of________________ 19_______
4. I am (h)_______________________________ of the
said________________________________________________
(or if the Petitioner is not connected with or related
to the or Patient, state as follows:)
I am not related to or connected with the said_________________
________________________________________________________
The reasons why this Petition is not presented by a relation
or connection are as follows:
The circumstances under which this Petition is presented by
me are as follows:—
[Pg 211]
5. I am not related to or connected with either of the persons
signing the certificates which accompany this petition as (where
the petitioner is a man) husband, father, father-in-law, son,
son-in-law, brother, brother-in-law, partner, or assistant (or
where the petitioner is a woman) wife, mother, mother-in-law,
daughter, daughter-in-law, sister, sister-in-law, partner, or assistant.
6. I undertake to visit the said_____________________________
__________________________personally, or by some one specially
appointed by me, at least once in every six months while under
care and treatment under the order to be made on this petition.
7. A statement of particulars relating to the said________________
______________________________________accompanies this petition.
If it is the fact, add: 8. The said_____________________
has been received in the Haydock Lodge Licensed House,
Newton-le-Willows, under an Urgency Order dated the____________
________________________________________________________
The petitioner therefore prays that an order may be made in
accordance with the foregoing statement.
Signed (k)_______________________________________
Date of Presentation of the Petition, this____________
day of___________________ 19_________
53 Vict. c. 5, s. 31.
When neither Certificate is signed by the
Usual Medical Attendant.
(a) Name
of
Patient.
I, the undersigned, hereby state that it is not practicable to
obtain a Certificate from the usual Medical attendant of (a)
__________________________________________________________________
for the following reason, viz.:—
(b) To be
signed
by the
petitioner.
(Signed) (b)______________________________
_______________ 19____________
Form 2.
STATEMENT OF PARTICULARS REFERRED
TO IN THE ANNEXED PETITION
If any particulars are not known the fact is to be so stated.
[Where the patient is in the petition or order described
as an idiot,
omit the particulars marked ►]
| The following is a Statement of Particulars | __________________ | |
| relating to the said | __________________ | |
| Name of patient, with Christian name at | __________________ | |
| length | __________________ | |
| Sex and Age | __________________ | |
| ► Married, single, or widowed | __________________ | |
| ► Rank, profession, or previous occupation | __________________ | |
| (if any) | __________________ | |
| ► Religious persuasion | __________________ | |
| Residence at or immediately previous to | __________________ | |
| the date hereof | __________________ | |
| ► Whether first attack | __________________ | |
| Age on first attack | __________________ | |
| When and where previously under care | __________________ | |
| and treatment as a lunatic, idiot, or | __________________ | |
| person of unsound mind | __________________ | |
| ► Duration of existing attack | __________________ | |
| Supposed cause | __________________ | |
| Whether subject to epilepsy | __________________ | |
| Whether suicidal | __________________ | |
| Whether dangerous to others, and in | __________________ | |
| what way | __________________ | |
| Whether any near relative has been | __________________ | |
| afflicted with insanity | __________________ | |
| Names, Christian names, and full postal | __________________ | |
| addresses, of one or more relatives | __________________ | |
| of the patient | __________________ | |
| Name of the person to whom notice of | __________________ | |
| death to be sent, and full postal | __________________ | |
| address, if not already given | __________________ | |
| ‡Name and full Postal Address of the | __________________ | |
| usual Medical Attendant of the Patient | __________________ | |
| ‡When the Certificate is not signed by the
usual Medical Attendant, the Certificate on the other side must be filled out. |
||
| Signed (a) | |
| Name, with Christian | |
| Name at length | ____________________________________ |
| Rank, Profession or | |
| Occupation (if any) | ____________________________________ |
| How related to, or | |
| otherwise connected | |
| with the Patient | ____________________________________ |
53 Vict. c. 5. s. 7 (4).
When a previous Petition has been dismissed.
(a) Name of
Patient.
(b) Name
of asylum,
hospital,
licensed
house,
or single
charge.
(c) Justice
of the
Peace
for ——,
or Judge of
County
Court
of —, or
Stipendiary
Magistrate
for ——
I, the undersigned, hereby state that a former Petition for
Reception of (a)___________________________________________
into (b)__________________________________________________
was presented to __________________________________________
(c)______________________________________________________
in the month of________________ 19_______, and dismissed.
Herewith is a copy
(furnished by the Commissioners in Lunacy)
of the statement sent to them of the reasons for its dismissal.
Note.—This Copy is to be obtained from the Commissioners
in Lunacy by the Petitioner at his own expense.
An Order for Reception of a Lunatic is to be obtained upon a private application by Petition to a Judge of County Courts, or Stipendiary Magistrate, or Metropolitan Police Magistrate, or specially appointed Justice of the Peace. The petition is to be presented, if possible, by the husband or wife, or by a relative (i.e. a lineal ancestor or lineal descendant, or lineal descendant of an ancestor not more remote than great-grandfather or great-grandmother) of the Lunatic, and is to be accompanied by a Statement of Particulars and two Medical Certificates on separate sheets of paper. One of the Medical Certificates accompanying the Petition must, if practicable, be by the usual Medical Attendant of the Lunatic; if not by him, the reason must be stated (see Form above). If a previous Petition has at any time been dismissed, the facts relating to its dismissal are to be stated in the fresh Petition (see Form above); and the Petitioner must obtain from the Commissioners in Lunacy a Copy of the Statement sent to them of the reasons for its dismissal, and present this copy with his Petition. The Reception Order (which will not remain in force for more than seven days after its date), the Petition, the Statement of Particulars, and the Medical Certificates must be sent to the Superintendent or Proprietor of the Asylum, Hospital, or House where the Patient is to be received. [Pg 214]
(a) Insert residence of patient.
(b) County, city, or borough, as the case may be.
(c) Insert profession or occupation, if any.
53 Vict. c. 5.—Sched. 2, Form 8.
CERTIFICATE OF MEDICAL PRACTITIONER
In the Matter of_________________________________________
of (a)___________________________________________________
in the (b)_____________________ of_________________________
(c) _____________________________________________________
_______________________________________an alleged lunatic.
I, the undersigned, ________________________________________
do hereby certify as follows:
1. I am a person registered under the Medical Act, 1858,
and I am in the actual practice of the medical profession.
(d) Insert the place of examination, giving the name of the street with number or name of house, or should there be no number, the Christian and surname of occupier.
(e) County, city, or borough, as the case may be.
(f) Omit this where only one certificate is required.
(g) A lunatic or an idiot, or a person of unsound mind.
(h) If the same or other facts were observed previous to the time of the examination, the certifier is at liberty to subjoin them in a separate paragraph.
(i) The names and Christian names (if known) of informants to be given, with their addresses and descriptions.
(k) Strike out this clause in case of a patient whose removal is not proposed.
(l) Insert full postal address.
2. On the_______________________ day of ________________ 19__
at (d) _______________________________________________
in the (e)___________________ of _____________________
_________________(separately from any other practitioner) (f)
I personally examined the said ___________________________________
and came to the conclusion that ____ he is (g) ____________
and a proper person to be taken charge of and detained under
care and treatment.
3. I formed this conclusion on the following grounds, viz.:—
(a) Facts indicating insanity observed by myself at the
time of examination (h), viz.:—
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
(b) Facts communicated by others (i), viz.:
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
4. The said __________________________________________________
appeared to me to be[18] ..................in a fit condition of
bodily health to be removed to an asylum, hospital, or licensed house (k).
5. I give this certificate having first read the section of the
Act of Parliament printed below.
Dated this __________ day of ________ 19__
53 Vict. c. 5, ss. 4, 11, 16, 28, 29.
Extract from section 317 of the Lunacy Act, 1890.
Any person who makes a wilful misstatement of any material
fact in any medical or other certificate or in any statement or
report of bodily or mental condition under this Act, shall be
guilty of a misdemeanour.
(a) A Justice for —, specially appointed under the Lunacy Act, 1890, or the Judge of the County Court of —, or the Stipendiary Magistrate for—
(b) Address and occupation.
(d) Name of petitioner.
53 Vict. c. 5.—Sched. 2, Form 3.
ORDER FOR RECEPTION OF A PRIVATE PATIENT, TO BE MADE
BY A JUSTICE APPOINTED UNDER THE LUNACY ACT, 1890,
JUDGE OF COUNTY COURTS, OR STIPENDIARY MAGISTRATE
I, the undersigned _______________________________________________
being (a) _________________________________________________
__________________________________________________________________
upon the petition of _____________________________________________
of (b) ____________________________________________________
in the Matter of _________________________________________________
a person of unsound mind, accompanied by the Medical Certificates
of _______________________________________________________________
and ______________________________________________________________
hereto annexed, and upon the undertaking of the said (d)
__________________________________________________________________
to visit the said ________________________________________________
personally or by some one specially appointed by the said (d)
__________________________________________________________________
once at least in every six months while under care and treatment
under this Order, hereby authorise you to receive the
said _____________________________________________________________
as a patient into your Licensed House (e).
And I declare that I have [or have not] personally
seen the said ____________________________________________________
before making this Order.
Dated this __________________ day of ________________ 19___
Urgency Orders.—Where it is urgent that an alleged lunatic (not a pauper) must be put under restraint as soon as possible, he may be received upon an urgency order, without petitioning a Judicial Authority, accompanied by a statement of particulars and one medical certificate. The order should be made by the husband, wife, or a relative of the alleged lunatic; if this be not possible, the reasons must be stated. It may be signed before or after the medical certificate, and before or after a petition order has been made. If before, it must be noted in the petition; if after, a copy must accompany the petition. No person may sign an urgency order if under twenty-one years of age, and must have seen the alleged lunatic within two days before the date of the order.
The urgency order remains in force seven days from its date, during which period the procedure for a “Judicial Order on Petition” is carried out. If the petition has been presented and the order is for [Pg 216] some reason or other deferred, then the urgency order remains in force. The medical examination for certification must have been made not more than two days before reception, and reasons must be given why “it is expedient” that the alleged lunatic should be put under control “forthwith.”
53 Vict. c. 5.—Sched. 2.
FORM OF URGENCY ORDER FOR THE RECEPTION OF
A PRIVATE PATIENT, WITH MEDICAL CERTIFICATE
AND STATEMENT ACCOMPANYING URGENCY ORDER
Forms 4, 2, 8 and 9.
(a) House, or hospital, or asylum, or as a single patient.
(b) Name of Patient.
(c) Lunatic, or an idiot, or a person of unsound mind.
(d) Some day within two days before the date of the order.
(e) Husband, wife, father, father-in-law, mother, mother-in-law, son, son-in-law, daughter, daughter-in-law, brother, brother-in-law, sister, sister-in-law, partner, or assistant.
(If not the husband or wife, or a relative of the patient, the person signing to state as briefly as possible—1. Why the order is not signed by the husband or wife, or a relative of the patient. 2. His or her connection with the patient, and the circumstances under which he or she signs.)
(f) Superintendent of ____ the ____ asylum, ____ hospital or resident licensee of the ____ house (describing the asylum, hospital, or house by situation and name.)
Lunacy, Nos. 4 & 2.
(33 Vict. c. 5, s. 11.)
I, the undersigned, being a Person Twenty-one years of age,
hereby authorise you to receive as a Patient into your (a)
House (b) _______________________________________________
_______________________________________________________
as a (c) __________________________________whom I last saw at
________________________________________________________
on the (d) __________________ day of_______________ 19______
I am not related to or connected with the Person signing
the Certificate which accompanies this Order in any of the
ways mentioned in the Margin. (e) Subjoined (or annexed)
hereto is a Statement of Particulars relating to the said ____________
Name and Christian Name _______________________
at length_______________________
Rank, Profession, or Occupation ___________________
(if any)_______________________
Full Postal Address _____________________________
How related to or connected _____________________
with the patient___________________________
Dated this _______________ day of __________ 19____
Form 2.
STATEMENT OF PARTICULARS REFERRED
TO IN THE ANNEXED ORDER
If any particulars are not known the fact is to be so stated.
[Where the patient is in the petition or order described
as an idiot,
omit the particulars marked ►]
| The following is a Statement of Particulars | __________________ | |
| relating to the said | __________________ | |
| Name of patient, with Christian name at | __________________ | |
| length | __________________ | |
| Sex and Age | __________________ | |
| Married, single, or widowed | __________________ | |
| ► Rank, profession, or previous occupation | __________________ | |
| (if any) | __________________ | |
| ► Religious persuasion | __________________ | |
| Residence at or immediately previous to | __________________ | |
| the date hereof | __________________ | |
| ► Whether first attack | __________________ | |
| Age on first attack | __________________ | |
| When and where previously under care | __________________ | |
| and treatment as a lunatic, idiot, or | __________________ | |
| person of unsound mind | __________________ | |
| ► Duration of existing attack | __________________ | |
| Supposed cause | __________________ | |
| Whether subject to epilepsy | __________________ | |
| Whether suicidal | __________________ | |
| Whether dangerous to others, and in | __________________ | |
| what way | __________________ | |
| Whether any near relative has been | __________________ | |
| afflicted with insanity | __________________ | |
| Names, Christian names, and full postal | __________________ | |
| addresses, of one or more relatives | __________________ | |
| of the patient | __________________ | |
| Name of the person to whom notice of | __________________ | |
| death to be sent, and full postal | __________________ | |
| address, if not already given | __________________ | |
| Name and full Postal Address of the | __________________ | |
| usual Medical Attendant of the Patient | __________________ | |
| Signed (a) | ____________________ | |
When the Petitioner or person signing an Urgency Order is NOT
the person who signs the Statement, add the following particulars
concerning the person who signs the Statement.
| Name, with Christian | |
| Name at length | ____________________________________ |
| Rank, Profession or | |
| Occupation (if any) | ____________________________________ |
| How related to, or | |
| otherwise connected | |
| with the Patient | ____________________________________ |
(a) Insert residence of patient.
(b) County, city, or borough, as the case may be.
(c) Insert profession or occupation, if any.
(d) Insert the place of examination, giving the name of the street, with number or name of house, or should there be no number, the Christian and surname of occupier.
(e) County, city, or borough, as the case may be.
(f) A lunatic, an idiot, or a person of unsound mind.
(g) If the same or other facts were observed previous to the time of the examination, the certifier is at liberty to subjoin them in a separate paragraph.
(h) The names and Christian names (if known) of informants to be given, with their addresses and descriptions.
Lunacy, Nos. 8 & 9.
(53 Vict. c. 5, ss. 11, 28, 29, 32 and 33.)
53 Vict. c. 5.—Sched. 2, Form 8.
CERTIFICATE OF MEDICAL PRACTITIONER
In the Matter of ___________________________________
of (a) _____________________________________________
in the (b)________________________ of ________________
(c) ________________________________________________
an alleged lunatic.
I, the undersigned __________________________________
do hereby certify as follows:—
1. I am a person registered under the Medical Act, 1858,
and I am in the actual practice of the medical profession.
2. On the _____________ day of _____________ 19 ____
at (d) ____________________________________________
in the (e) ________________ of ______________________
I personally examined the said ________________________
and came to the conclusion that ______ he is (f)___________
and a proper person to be taken charge of and detained under
care and treatment.
3. I formed this conclusion on the following grounds, viz.:—
(a) Facts indicating Insanity observed by myself
at the time of examination (g), viz.:—
______________________________________________
______________________________________________
______________________________________________
______________________________________________
(b) Facts communicated by others (h), viz:—
______________________________________________
______________________________________________
______________________________________________
______________________________________________
(i) If an urgency certificate is required, it must be added here.—Form No. 9.
53 Vict. c. 5.—Form 9.
(i) STATEMENT ACCOMPANYING
URGENCY ORDER
I certify that it is expedient for the welfare of the said
_______________________ (or for the public safety, as
the case may be) that the said ________________________________
should be forthwith placed under care and treatment.
My reasons for this conclusion are as follows: __________________
_______________________________________________________
_______________________________________________________
_______________________________________________________
_______________________________________________________
(k) Strike out this clause in case of a private patient whose removal is not proposed.
4. The said ___________________________________
appeared to me to be [‡ _____________] in a fit condition
of bodily health to be removed to an asylum, hospital,
or licensed house(k).
(‡) Or not to be.
5. I give this certificate having first read the section of the Act
of Parliament printed below.
Dated this ________________ day of ________________
One thousand nine hundred and ______________
(l) Insert full postal address.
Extract from section 317 of the Lunacy Act, 1890.
Any person who makes a wilful misstatement of any
material fact in any medical or other certificate,
or in any statement or report of bodily or mental
condition under this Act, shall be guilty of a misdemeanour.
[Pg 220] Orders after Inquisition.—This constitutes a legal investigation as to whether or not a person is capable of managing his or her own affairs, and whether restraint is necessary. It is conducted before a judge, with a jury if the alleged lunatic demand one, unless the judge is satisfied by personal examination that the lunatic is not mentally competent to understand the demand for a jury. In such a case the medical man is only concerned as a witness.
According to circumstances the alleged lunatic may be kept under restraint, or remain at liberty with the control of his or her affairs under a “Committee of Estate”; or, if declared sane, set free and with control of his estate.
Summary Reception Orders.—When a lunatic is not under proper control, and if without relations or friends, and there be no one who will sign a petition for detention, or when a lunatic is uncared for, cruelly treated, and is found so by a medical practitioner, his duty is to inform a constable, relieving officer, or overseer of the parish of the fact. The official will then make a statement on oath to a Judicial Authority, who will direct two medical practitioners to make the necessary examinations, and if satisfied he will issue an order for the removal of the individual to an asylum. The procedure followed will then be the same as for a “petition for reception.” Under a summary reception order the Judicial Authority may place the person under the care of a relation or friend, or the visitors of the asylum in which the person is intended to be, or is placed.
Lunatics Wandering at Large.—Every constable, relieving officer, or overseer of a parish who knows of a person, whether pauper or not, who is deemed to be a lunatic and wandering at large, shall apprehend and take such person before a Justice, or if the Justice receive information on oath, he may have the person apprehended and brought before him. The Justice has the person medically examined, and if certified a lunatic to the satisfaction of the Justice, he may issue an order for detention; if the medical man certify that the person is not fit for removal, the removal is postponed until the person is certified fit for it.
The above proceedings are not necessary if it be considered a matter of public safety and for the good of the alleged lunatic that immediate detention be carried out. The constable, relieving officer, or overseer of the parish may remove such person to the workhouse of the union in which the person is, and detain him for not more than three days. Before the expiration of that time the necessary proceedings under the Lunacy Act must be taken.
Reception Order by two Commissioners.—Any two or more Commissioners in Lunacy may visit a pauper lunatic or an alleged lunatic not detained in a workhouse or lunatic asylum, and if satisfied after certification by a medical man that the person is a lunatic, order removal to an asylum.
Pauper Lunatics.—A medical officer of a Poor Law Union who has knowledge that a pauper within his district is alleged to be a lunatic, [Pg 221] shall notify the relieving officer or overseer of the parish where the pauper resides of the fact, who within three days shall notify a Justice, who will interview the alleged lunatic and call in a medical practitioner to examine and certify. If the Justice be satisfied that the person be a lunatic, he makes an order for removal to an asylum. One medical certificate only is necessary.
Escape of Lunatics.—An escaped lunatic may be retaken at any time within fourteen days without a fresh order.
Discharge of Lunatics.—The reception order remains in force for periods of one, two, and three years, and then for periods of five years. At the end of any of these periods the Lunacy Commissioners may continue the detention of the lunatic, if satisfied by certification from the medical man of the institution, or the usual medical attendant of the lunatic, that the patient remains of unsound mind and further detention is necessary.
The petitioner of the reception order may request the discharge of a patient. The discharge may be refused if the medical man in charge certifies the lunatic dangerous and unfit to be at large, unless two of the visitors to the asylum or the Commissioners visiting the asylum or house give their consent in writing.
Two Commissioners—one medical, the other legal—may order the discharge of any patient.
When a patient recovers, the medical attendant of the institution notifies this to the petitioner or person responsible for the payment on account of the patient. Should the patient not be removed within seven days of such notice, the patient may be discharged “forthwith.”
PROCEDURE IN SCOTLAND
Idiots and imbeciles under eighteen years of age may be received into training schools without the legal procedure which obtains in England and Wales. They are sent to these institutions as lunatics, however, under the usual legalities, in order that the Government grant may be obtained. When over eighteen years of age, if sent to institutions other than training schools, they are classed as lunatics, and the necessary legal procedure is followed.
Insane persons whose malady is not confirmed may be cared for privately for a period not exceeding six months. The certificate of one medical practitioner only is required.
Insane persons, pauper or not, can be placed in an asylum by order of the Sheriff, by petition and two medical certificates. The inspector of the poor acts as petitioner for paupers.
In cases of urgency a certificate of emergency from one medical practitioner is required, along with a request from the petitioner, to the superintendent of the asylum.
A person who is prodigal or facile can be restrained from alienating his property by guardians appointed by the Court.
When a lunatic is found to be incapable of administering his or her estate, the Court appoints a Committee of Estate. [Pg 222]
PROCEDURE IN IRELAND
The procedure differs in pauper and private cases.
Pauper patients, not dangerous.—In order to detain such a pauper there must be a declaration of insanity and destitution, with the names and addresses and descriptions of two relatives of the person, given before a magistrate. A magistrate and a clergyman or poor-law guardian must certify that they have personally inquired into the case. One medical certificate is necessary. The applicant must remove the patient when called upon.
Paying patients who are not dangerous, for admission to a district asylum, are under more stringent regulations. A declaration that they are unable to pay the expenses necessary for support in a licensed house must be made before a magistrate; further, that there is no friend who can undertake this; and a statement of the length of time the patient has resided in the country. A magistrate and clergyman must certify that they have investigated the case. One medical certificate must be signed by two practitioners. A guarantee for the payment must be given, and also to remove the patient when called upon. The sanction of an inspector of lunatics must be given.
For admission into licensed houses, charitable institutions, and single care, an order by a relative or connection of the lunatic is required with two medical certificates, unless urgent, when one is sufficient, but a second must follow within fourteen days.
A medical practitioner is bound to certify as to the sanity of a person. If, however, he undertakes to fill up the certificates necessary for the detention of an alleged lunatic, he becomes responsible to the authorities for the correctness of the certificates, and if he make a wilful misstatement of facts he is guilty of a misdemeanour. The medical practitioner may have an action brought against him by the lunatic when recovered or discharged. The most vindictive feelings may be entertained against the medical man. In such a case, if the medical man proves his “good faith” and the exercise of “reasonable care” in his examination and certification, he receives the protection of the Court.
In the case of Nottidge v. Ripley and Nottidge, the Lord Chief Baron having been understood to intimate an opinion that no person ought to be so confined unless he is dangerous to himself or others, the Commissioners pointed out that the scope of the Lunacy Acts is not thus limited. They said:
“The object of these Acts is not, as your Lordship is aware, so much to confine lunatics, as to restore to a healthy state of mind such of them [Pg 223] as are curable, and to afford comfort and protection to the rest. Moreover, the difficulty of ascertaining whether one who is insane be dangerous or not is exceedingly great, and in some cases can only be determined after minute observation for a considerable time.
“It is of vital importance that no mistake or misconception should exist, and that every medical man who may be applied to for advice on the subject of lunacy, and every relative and friend of any lunatic, as well as every magistrate and parish officer (each of whom may be called upon to act in cases of this sort), should know and be well assured that, according to law, any person of unsound mind, whether he be pronounced dangerous or not, may legally and properly be placed in a county asylum, lunatic hospital, or licensed house, on the authority of the preliminary order and certificates prescribed by the Acts.
“Upon the whole, it appears that the power to restrain and confine a lunatic is limited at common law to cases in which it would be dangerous, either as regards others or himself, for the lunatic to be at large; but that the power to place and detain a lunatic in a registered hospital or licensed or other house, under an order and medical certificates duly made and obtained in accordance with the Lunacy Acts, is not so limited.”
The terms of the Lunacy Act, 1890, are as follows:
“Subject to the exceptions in this Act mentioned a person shall not be received or detained as a lunatic, as a single patient, unless under a reception order by a judicial authority.” “Every person who, except under the provisions of the Act, receives or detains a lunatic or an alleged lunatic in an institution for lunatics, or for payment takes charge of, receives to board or lodge, or detains a lunatic or alleged lunatic in an unlicensed house, shall be guilty of a misdemeanour, and in the latter case shall also be liable to a penalty not exceeding fifty pounds.” “Except under the provisions of this Act, it shall not be lawful for any person to receive or detain two or more lunatics in any house, unless the house is an institution for lunatics or a workhouse.” “Any person who receives or detains two or more lunatics in any house except as aforesaid shall be guilty of a misdemeanour.”
It is therefore unlawful to receive a lunatic or alleged lunatic except by reception order. Only one can be received into a private house, and a reception order is required. No medical man should receive a lunatic into residence without the necessary reception order. All the statutory regulations are demanded for a single case, and the private house is subject to visitation and inspection.
It is also important to remember that if any one receive a person not insane at the time, but who subsequently becomes insane, he renders himself liable to prosecution, unless he procure the necessary medical certificates and order (R. v. Wilkins).
Is a Lunatic a competent Witness?—Mr. Fitzjames Stephen maintains (Criminal Law) that madmen are competent witnesses in relation to testimony as in relation to crime. If they understand the nature of an oath, and the character of the proceedings in which they [Pg 224] are engaged, they are competent witnesses whatever be the nature or degree of their mental disorder. An idiot shall not be allowed to give evidence (Co. Litt. 6 b; Gilb. Ev. 144); a lunatic during a lucid interval may do so (Id. Com. Dig. Testm. {A}). When a lunatic is tendered as a witness, it is for the judge to examine and ascertain whether he is of competent understanding to give evidence, and is aware of the nature and obligation of an oath; if satisfied that he is, the judge should allow him to be sworn and examined (R. v. Hill, 2 Den. 255; 20 L.J. [M.C.] 222).
The Civil Rights of Lunatics.—If an individual be suffering from such mental disease as to render him incompetent to manage his own affairs, the law steps in to protect him and his property from injury. But the power so used does not necessarily imply that he is deprived of his personal freedom, but merely such restraint as is necessary for his protection.
Many lunatics, under the protection of the Court, live in their own houses with large establishments. A person so protected by the law is said to be subject to an “interdiction.” In these cases a commission is usually granted by the Court of Chancery, and a writ known under the name of “de lunatico inquirendo” issued, after certain legal matters of detail are settled, and affidavits from medical men certifying to the insanity of the party have been filed.
The tests of insanity in these cases differ from those required in criminal cases, where the knowledge of right from wrong is imperatively demanded. The mental defect must not be the result of ignorance or want of education, and at one time commissions were only issued when it was shown that lunacy and idiocy alone existed, imbecility or mere weakness of mind not being deemed sufficient to deprive a man of his civil rights, or to place him under the protection of the Court.
To so great an absurdity did this lead, that the man suffering from a delusion sufficient to be comprehended under the legal term “lunacy” was protected, whereas the feeble-minded were left without interference, though needing it more. The cost of these commissions sometimes reached almost fabulous sums. The expense has been somewhat lessened by recent enactments, and the process simplified—the Lord Chancellor having it in his power to direct an inquiry before two Commissioners, thus dispensing with a jury. (See the 16 and 17 Vict. c. 70, and 25 and 26 Vict. c. 86.)
In Scotland, however, the law is far more simple. The cognition proceeds on a brieve or writ addressed to the Lord President of the Court of Session, and directs him to inquire “whether the person sought to be cognosced is insane, who is his nearest agnate, and whether such agnate is of lawful age.” “And such person shall be deemed insane if he be furious or fatuous, or labours under such unsoundness of mind as to render him incapable of managing his affairs.” “The trial is before a judge of the Supreme Court and a special jury. If the insanity be proved, the nearest agnate—relation by the father‘s side—is by law entitled to the guardianship.” No one not a near relative can institute these proceedings.
In Scotland also, the trial by jury may be avoided by applying by petition to the Court of Session for the appointment of a judicial [Pg 225] factor or curator bonis. Of this appointment the alleged lunatic is informed, which, if he please, he may oppose; medical evidence is received, and on this the Court rests its decision—the usual course being to remit the case to some competent person to make inquiry, take evidence, and report. The Commissioner is usually the Sheriff.
Examination of the Insane.—A few words of caution need here be said. Medical men will consult their own dignity and that of their profession by remembering that in cases of alleged insanity, as in fact in all other cases when their opinion is sought, they are not justified in taking sides. Their evidence will be the more valuable in proportion to the care they take in examining into the facts of the case, and the good sense and judgment shown in their examination of the patient. To distinguish between the mistakes, the result of ignorance and want of education, and those the result of a feeble mind, is of primary importance. It is no sign of insanity in an uneducated farmer that he knows not the pons asinorum. All cases should be tested by considering the surroundings and possible degree of culture of a person placed under like conditions as the party under examination. Has he shown himself capable of an average amount of culture? or is his mental condition inferior to what one might legitimately expect under the influences to which he has been subjected? The medical examiner should also direct his attention to this important point, setting aside all legal and medical theories of insanity, viz.—“Is the case of such mental disorder as to create an incapacity for managing affairs.”
A medical practitioner may be called upon to give evidence as to the capacity of a testator to make a valid will. An ordinary person witnessing a will does so to fact only, but if a medical man do so it implies that he was of the opinion that the testator was fit to make a will and of a sound and disposing mind. In making an examination of a person for fitness to make a will, the medical man must endeavour to find out if the testator understands the nature of his action, and all the details associated with it; also if he knows the nature and amount of his property, and the claims or otherwise of those who may become beneficiaries under it. Further, has he such a delusion as may influence his will in disposing of his property, and bring about a disposal of it which, if the mind had been sound, would not have been made.
A person may have a delusion or delusions without interfering with the making of a will. If the “disposing mind” be left intact, testamentary capacity is upheld. In severe illness and old age the mind may be so disturbed, without true insanity being present, that a person is rendered incapable of making a will. In all such cases the medical man should be sure of his ground before granting, if requested, that the patient is capable or otherwise. It is a good plan, when examining a patient as to testamentary capacity, to have the will produced, and [Pg 226] privately read it out to the person and ask if it be correct, then to have the person repeat the dispositions of the will, and see if they coincide with the contents of the document.
People who are aphasic may make wills which are valid. Difficulties arise in cases of sensory aphasia.
An habitual drunkard, as defined by law, is “a person who, not being amenable to any jurisdiction in lunacy, is notwithstanding, by reason of habitual intemperate drinking of intoxicating liquor, at times dangerous to himself or herself, or to others, or incapable of managing himself or herself or his or her own affairs.”
Before placing such a person under restraint in a licensed retreat the person‘s consent must be obtained. The patient must make an application to a Justice of the Peace, and supported by a declaration from two persons stating that the applicant is an habitual drunkard within the meaning of the Act. If the justice be satisfied, he can make out an order for detention. The order is valid for any time mentioned in the application not exceeding two years. The patient can be detained, forcibly if necessary, and if escaped may be arrested and taken back.
DEFINITION OF A POISON—SALE OF POISONS—CLASSIFICATION OF POISONS—ACTION OF POISONS—GENERAL EVIDENCE OF POISONING—GENERAL TREATMENT IN CASES OF POISONING —GENERAL METHODS OF EXAMINATION FOR POISON
Toxicology is that division of Forensic Medicine which takes into consideration the modes and actions of poisons upon the living body, the treatment of their effects upon the body, and the methods of detecting them when occasion requires.
Definition of a Poison.—Neither the law nor medicine defines a poison. The popular definition is to be avoided, viz., that, a poison is a substance capable of acting injuriously on the body when taken or administered in a small dose.
Husband defined a poison as “any substance which, introduced into the system or applied to the body, is injurious to health and destroys life, irrespective of temperature or mechanical means.”
Taylor and Stevenson define a poison as “a substance which when absorbed into the blood is, by its direct action, capable of seriously affecting health or destroying life.”
There are substances, however, which do not require absorption into the blood in order to exert their deleterious action, e.g. the corrosive acids and alkalies; but, although the chief action is a local one in most cases, some absorption does take place and is evidenced in systemic effects, and are so classified as poisons differing from powdered glass, which acts mechanically only and is not a poison in the true sense of the word.
Winter Blyth considers that “a substance of definite chemical composition, whether mineral or organic, may be called a poison if it is capable of being taken into any living organism, and causes, by its own inherent chemical nature, impairment or destruction of function.”
According to Luff a poison is “a substance which, either by its direct action upon the skin or mucous membranes, or after its absorption into the blood, is capable of injuriously affecting health or destroying life.”
Letheby defines a poison as “anything which otherwise than by the agency of heat or electricity is capable of destroying life, either by chemical action on the tissues of the living body, or by physiological action from absorption into the system.” [Pg 228]
The law does not recognise the manner in which the substance acts, nor the result; the legal standpoint is the intent of the administrator qua administrator. The law is as follows: “Whosoever shall administer or cause to be administered or taken by any person any poison or other destructive thing with intent to commit murder shall be guilty of a felony” (24 and 25 Vict. c. 100, sec. 11).
Section 22. “Whosoever shall unlawfully apply or administer to or cause to be taken by, or attempt to apply or administer to, or attempt to cause to be administered to or taken by, any person, any chloroform, laudanum, or other stupefying or overpowering drug, matter, or thing, with intent, in any of such cases, thereby to enable himself or any other person to commit, or with intent, &c., to assist any other person in committing any indictable offence, shall be guilty of felony.”
Section 23 enacts that, “Whosoever shall unlawfully administer to, or cause to be administered to, or taken by any other person, any poison or other destructive or noxious thing so as thereby to endanger the life of such person, or so as thereby to inflict upon such person any grievous bodily harm, shall be guilty of a felony.”
Section 24. “Whosoever shall unlawfully or maliciously administer to or cause to be administered to or taken by any other person any poison or other destructive or noxious thing with intent to injure or aggrieve or annoy such person shall be guilty of a misdemeanour.”
Section 25. “If upon the trial of any person charged with the felony above mentioned the jury shall not be satisfied that such person is guilty thereof, but shall be satisfied that he is guilty of the misdemeanour above mentioned, then, and in every such case, the jury may acquit the accused for such felony and find him guilty of a misdemeanour.”
Administration of Noxious Drugs.—The law throws on the medical witness the responsibility of the definition of a noxious thing, and whether it was given in excess, or liable to cause annoyance or injury to health. At a Bodmin Assize, Lord Chief-Justice Cockburn, after consultation with Mr. Justice Hawkins, delivered an important judgment on the subject. A man was charged with having administered cantharides with criminal intent. The judges ruled that there must not only be an administration of a noxious drug with a guilty intent, but the drug must have been administered in such quantities as to be noxious, whereas the dose here given was too small to be seriously deleterious. Distinction was drawn between a drug like cantharides, which is only noxious when given in excess, and strychnine, a well-established poison. Acquittal was therefore directed. In the case of R. v. Cramp, the prisoner was charged with having administered half an ounce of oil of juniper with intent to procure abortion. He was convicted, but appealed on the legal ground that the substance must be noxious in itself, and not only when given in excess. Lord Coleridge ruled that “if a person administers with intent to produce miscarriage something which as administered is ‘noxious,’ he administers a ‘noxious thing.’”
The Sale of Poisons.—The law, by the Pharmacy Act, 1868, and its amendments, restricts the sale of poisons to pharmaceutical [Pg 229] chemists, chemists and druggists, and registered medical practitioners. The Acts define and indicate by schedule “Poisons within the meaning of the Act.” The Schedule of Poisons, as amended in the “Poisons and Pharmacy Act, 1908,” and “Additions to Schedule 1913,” is:
SCHEDULE OF POISONS
[As amended by Orders in Council]
Part I
Arsenic, and its medicinal preparations.
Aconite, aconitine, and their preparations.
Alkaloids.—All poisonous vegetable alkaloids not specifically
named in this schedule, and their salts, and all
poisonous derivatives of vegetable alkaloids.
Atropine, and its salts, and their preparations.
Belladonna, and all preparations or admixtures (except belladonna
plasters) containing 0.1 or more per cent. of belladonna
alkaloids.
Cantharides, and its poisonous derivatives.
Coca, any preparation or admixture of, containing 1 or more
per cent. of coca alkaloids.
Corrosive sublimate.
Cyanide of potassium, and all poisonous cyanides and their
preparations.
Emetic tartar, and all preparations or admixtures containing 1 or
more per cent. of emetic tartar.
Ergot of rye, and preparations of ergots.
Nux vomica, and all preparations or admixtures containing 0.2 or
more per cent. of strychnine.
Opium, and all preparations or admixtures containing 1 or more
per cent. of morphine.
Picrotoxin.
Prussic acid, and all preparations or admixtures containing 0.1 or
more per cent. of prussic acid.
Savin, and its oil, and all preparations or admixtures containing
savin or its oil.
Part II
Almonds, essential oil of (unless deprived of prussic acid).
Antimonial wine.
Cantharides, tincture and all vesicating liquid preparations orCarbolic acid, and liquid preparations of carbolic acid,
and its homologues containing more than 3 per cent.
of those substances, except preparations for use as
sheep wash or for any other purpose in connection with
agriculture or horticulture, contained in a closed
vessel distinctly labelled with the word “poisonous,”
the name and address of the seller, and a notice of the
special purposes for which the preparations are intended.
[Pg 230]
Chloral hydrate.
Chloroform, and all preparations or admixtures containing more
than 20 per cent. of chloroform.
Coca, any preparation or admixture of, containing more than 0.1
per cent. but less than 1 per cent. of coca alkaloids.
Diethyl-barbituric acid, and other alkyl, aryl, or metallic
derivatives of barbituric acid, whether described
as veronal, proponal, medinal, or by any other
trade name, mark, or designation; and all poisonous
urethanes and ureides. [Added March 12, 1913.]
Digitalis.
Mercuric iodide.
Mercuric sulphocyanide.
Oxalic acid.
Poppies, all preparations of, excepting red poppy petals
and syrup of red poppies (Papaver rhœas).
Precipitate, red, and all oxides of mercury.
Precipitate, white.
Strophanthus.
Sulphonal, and its homologues, whether described as trional,
tetronal, or by any other trade name, mark, or
designation. [Added March 12, 1913.]
All preparations or admixtures which are not included in
Part I. of this schedule, and contain a poison within
the meaning of the Pharmacy Acts, except preparations
or admixtures the exclusion of which from this
schedule is indicated by the words therein relating to
carbolic acid, chloroform, and coca, and except such
substances as come within the provisions of Section 5
of this Act.
Memorandum.—Special importance attaches to the last paragraph of Part II. of the schedule, as the effect of that paragraph is to include in Part II. many preparations and admixtures of vegetable drugs which contain poisonous alkaloids, although the drugs containing them are not specified in the schedule.
With those in Part I. a registration of the sale is compulsory, the purchaser must be known to or introduced by some person known to the vendor, and the purpose for which the poison is required, the date, the name and amount of the poison sold, the name and address of the buyer, and the entry must be signed by the purchaser and introducer. All substances in Parts I. and II. must be labelled by the vendor with a label bearing the name of the poison, the name and address of the seller, and the word “Poison”; but with those in Part II. no registration as in Part I. is required. In the sale of arsenic both the seller and purchaser must sign the entry, and the introducer must witness it. No arsenic can be legally sold to a person under the age of twenty-one years; nor may it be sold in quantities of less than 10 lbs. unless mixed with soot or indigo—one ounce of the former, or half an ounce of the latter, to each pound of arsenic. If quantities of over 10 lbs. be sold, and the soot or indigo would render it unfit for use in the way desired, then they may be omitted (Arsenic Act, 1851).
Classification of Poisons.—A good and scientific classification [Pg 231] of poisons is still wanted. The following simple general division, depending upon the chief effect, may be taken as guides by the student:
| (a) Corrosives—Local corrosion. | ||
| (b) Irritants—Gastro-intestinal irritation. | ||
| (c) Neurotics—Altered action of the nervous system. | ||
| 1. INORGANIC |
||
| Corrosive—Sulphuric acid, &c. | ||
| Irritant—Arsenic, &c. | ||
| 2. ORGANIC |
||
| Irritant—Savin, Cantharides. | ||
| Affecting Brain—Opium. | ||
| Affecting Spinal Cord—Strychnia. | ||
| Affecting Heart—Digitalis. | ||
| Affecting Lungs—Carbonic acid. | ||
| (Guy.) | ||
| IRRITANTS |
||
| Mineral | Acid poisons—Sulphuric acid, &c. | |
| Alkaline poisons—Caustic soda, &c. | ||
| Non-metallic—Phosphorus, Iodine, &c. | ||
| Metallic—Arsenic, Antimony, &c. | ||
| Vegetable—Savin, Elaterium, &c. | ||
| Animal—Cantharides. | ||
| NEUROTICS |
||
| Cerebral—Opium, Hydrocyanic acid, Alcohol. | ||
| Spinal—Strychnia, Nux vomica. | ||
| Cerebro-spinal—Conium, Belladonna, Aconite. | ||
| Cerebro-cardiac—Calabar bean, Digitalis. | ||
| (Taylor.) | ||
The subjoined classification is based upon that adopted by the late Professor Sir Douglas Maclagan. Where the poison acts in such a manner as to place it in two or more groups, I have fully described it in one, merely drawing attention to it under the others:
Action of Poisons.—Amid the difficulties which surround this subject, three points appear to have been clearly made out: (1) That it is necessary for all poisons to enter the blood before their specific action can be produced. (2) That poisons possess an elective affinity for certain tissues and organs. Thus, arsenic, however introduced into the system, as a rule attacks the stomach; and this peculiarity of action closely allies it to the poisons of typhoid, scarlet fever, smallpox, &c., which appear to have, respectively, an elective affinity for the glands of the intestines, the throat, and the skin. (3) That the habitual use of a poison in medicinal doses does not ensure a perfect toleration on the part of the system with regard to the action of the poison, for sooner or later a complete cachexia is produced, showing that the poisonous effect of the drug is not arrested.
Besides the above, there are also certain conditions connected with the action of poisons: (1) The poison is absorbed and distributed by the blood. (2) A portion is eliminated by the fluid secretions and excretions. (3) Another portion is for a time deposited in the tissues and organs of the body. These processes are of necessity simultaneous.
The channels of entrance and exit are as follows: Of entrance we have—(1) The blood-vessels as a result of wounds—more important in a physiological than a medico-legal question. (2) The skin and cellular membrane.—Absorption by the skin is modified by the condition of the part, and also by the form in which the drug is applied. Thus the skin of the arm-pits and groins is more absorbent than the palms of the hands. Watery solutions are not so effective as oily preparations, and the application of the drug in fine powder is more effectual than a watery solution of it. This is explained by the presence of a natural oily, unctuous substance on the skin, which prevents the direct contact of the watery solution, but if the solution be allowed to evaporate on the part, the substance thus left in minute division is then readily absorbed. The danger of allowing strong solutions of corrosive sublimate to evaporate on the head in the treatment of certain skin eruptions is thus explained. (3) The lungs and air-passages.—Absorption by these organs is most active, hence the intense rapidity in the action of aerial poisons. (4) The stomach and intestines.—Poisons introduced into the stomach or intestines take longer to arrive at the special organs on which they act than by the other channels of entrance. They are absorbed by the capillaries into the mesenteric veins, and before passing to the heart, [Pg 233] by which they enter the general circulation, they pass through the liver, where they are in part excreted in the bile or deposited in the gland. The absorbing power of the stomach is modified by its fulness or emptiness, and poisons not soluble in water may be rendered so by the gastric secretion.
The avenue of entrance may materially modify the action, and some poisons which act rapidly when entering by a wound, are inert when taken into the stomach. Snake poisons when given by the mouth are entirely harmless. Hydrogen sulphide is more toxic when inhaled than when taken in solution. This, though true in some cases, does not always occur; and the inertness of these poisons, it has been suggested, may be due to the elimination of them being as rapid as their absorption, so that a poisonous dose never enters the circulation. The intestines absorb more rapidly than the stomach, and this must be borne in mind when administering powerful drugs per anum.
Of the channels of exit we have: (1) The kidneys. (2) The lungs. (3) The bile. (4) The milk. (5) The saliva. (6) Mucous membrane. (7) The skin.
We know not the cause, but certain poisons appear to select a particular route for their exit—thus iodide of potassium leaves by the urine; mercury and its salts by the saliva; arsenic and eserine, the active principle of the Calabar bean, in small quantities, by the stomach, &c. We are, however, prepared to show that all poisons must enter the blood before they produce their effects, and that almost simultaneously with the entrance of the poison into the blood a process of elimination begins, and that fatal effects depend upon absorption taking place more rapidly than elimination. On the amount also of the poison absorbed do its fatal effects depend, and not on the quantity actually taken. Whilst absorption and elimination are both going on, some of the poison is being deposited in the organs and tissues of the body. As proofs of these statements it has been shown that poisons have been detected in the blood, and that urine, saliva, and milk, fluids secreted from it, may contain portions of the poison taken, and produce dangerous symptoms when given to other animals. Poisons applied to the brain tissue, or to nerve trunks, do not produce symptoms, and the action of a poison may be arrested for a time by compressing by a ligature the main vessels of the limb under the skin of which the poison has been injected. After death no trace of the poison may be detected, the quantity taken being just sufficient to produce a fatal result, or elimination may be so rapid that, although death was directly due to the poison, any remains of its existence cannot be made out. This occurred in the case of Dr. Alexander, who died from an accidental dose of arsenic, all the arsenic being eliminated in seventeen days—in another fatal case, in seven days. (Taylor)
As evidence of the diffusion of poisons the following table may be of use: [Pg 234]
| Physiological. | |
Dilatation of the pupil in poisoning by | |
| belladonna, hyoscyamus, &c. | |||
| Contraction of the pupil in poisoning by | |||
| opium, Calabar bean. | |||
| Physical. | |
Taste.— | Bitter taste of the secretions. Strychnia, |
| picrotoxin. The milk of animals fed on wormwood | |||
| may become bitter; on colchicum, poisonous. | |||
| Smell.— | Prussic acid, tobacco, conium, &c. | ||
| Colour.— | Skin blackened by nitrate of silver, given | ||
| internally. | |||
N.B.—By the aid of the spectroscope the salts of lithium and thalium have been detected in the liver and other tissues.
Recapitulation of the Mode of Action of Poisons,
and the Causes which Modify their Action.
| MODE OF ACTION | ||
|---|---|---|
| I. LOCAL | ||
| 1. Corrosion of the part | |
Strong acid, alkali, &c. |
| to which the poison | ||
| is applied. | ||
| 2. Inflammation as the | |
Arsenic, cantharides, &c. |
| result of irritants | ||
| applied to a part. | ||
| 3. Effects on the nerves | |
Dilatation of the pupil by belladonna, |
| of motion and sensation. | tingling of the tongue and skin by | |
| aconite, paralysis by conium. | ||
| II. REMOTE | ||
|---|---|---|
| 1. Common—not to be distinguished from the effects of | ||
| injury or disease. | ||
| 2. Specific—peculiar to the poison itself. | ||
| (1) General—affecting the whole system.—Antimony. | ||
| (2) Partial—acting on a particular organ.—Antimony | ||
| MODIFYING CAUSES |
||
| 1. Quantity. | |
1. Quantity of the poison increases its rapidly |
| fatal action. | ||
| 2. Action changed by the size of the dose. Thus, | ||
| oxalic acid in large doses acts as a corrosive; in | ||
| small doses on the heart, brain, or spinal cord. | ||
| 2. Form. | |
Solubility increases the activity of poisons. |
| Chemical Combinations.—Baryta is poisonous, | ||
| sulphate of baryta is inert. | ||
| Mixture.—Dilution may retard or accelerate | ||
| the action of a poison.[19] | ||
| 3. Point of application—Skin, lungs, mucous and serous membranes. [Pg 235] | ||
| 4. Condition of the body. |
|
Habit—generally lessens the action of |
| poisons, e.g. arsenic-eater, morphine | ||
| taker, morphine taker. | ||
| Idiosyncrasy—increases or may lessen the | ||
| action of poisons. | ||
| Disease—generally lessens, but in some | ||
| cases increases the action of poisons. | ||
It will now be necessary to consider briefly the general evidences of poisoning, in order to determine whether a death alleged to be due to poison is not really the result of disease. For convenience of description, this subject will be divided into five sections:
1. Evidence from the Symptoms.—As a general rule the symptoms come on suddenly while the person is in apparent health, except in cases of slow poisoning, when the poison may be so administered by frequently repeated and small doses as to simulate disease, and the physician is more easily misled than when a single large dose is given. In cases of suspected homicide this suddenness in the accession of the symptoms is particularly to be noticed, and we may have to decide as to the probabilities of accident, suicide, or homicide. Here collateral evidence must be our guide. The slowness, obscurity, and irregularity of the symptoms are more in favour of homicide than either accident or suicide. But it must also be borne in mind that the invasion of many diseases is sudden, as is the case with cholera, gastritis, and some others.
Certain conditions of the system more or less modify the effects of some poisons. Thus, sleep delays the action of arsenic; and this may also be the case with other poisons. Intoxication has also been said to exert a retarding power over the action of certain poisons. This is probably more apparent than real, the fact being that the symptoms in the cases observed are masked.
Much more important, however, is the influence of disease. Large doses of opium are well borne in mania, delirium tremens, dysentery, and tetanus; whereas it is well known that even small doses of mercury in cases of Bright‘s disease of the kidney, or in children recovering from any of the eruptive fevers, have produced dangerous salivation.
The symptoms of poisoning go on from bad to worse in a steady course; but there may be remissions, followed, under treatment, by their entire disappearance, no ill effect remaining. Remissions are most likely to [Pg 236] occur in slow poisoning with the metallic irritants, from fear of detection or cunning on the part of the poisoner to imitate the progress of disease. In nervous affections, all the symptoms must be taken into consideration, and these will be found to differ from those of any known poison. The history of the case should also have due attention paid to it.
In poisoning, the symptoms appear soon after food or drink has been taken. This is open to the objection that apoplexy has occurred immediately after a meal. The probative value of the above statement is, however, increased if several persons have been similarly affected after partaking of the same dish, especially if the symptoms followed within a short time—under four hours—of the meal. But it must also be remembered that all persons are not affected alike by the same poison. Again, the diagnostic value is weakened if it can be proved that the person or persons affected have taken nothing in the way of food for two or three hours previously.
The flesh of animals poisoned by accident, or intentionally, may seriously affect those who eat it.—As a case in point may be mentioned the injurious effects produced in some persons who had partaken of the Canadian partridges imported to this country some years ago, and which had probably eaten some poisonous berries during the severe winter of that year.
Poisons may be introduced into the system otherwise than by the mouth; that is, they may be placed in the vagina or rectum, or inhaled when volatile poisons are used. Sometimes a poison has been introduced into the medicine, or a poisonous draught substituted for the one prescribed. In any case, where suspicious symptoms suddenly occur, the poison has most probably been taken in from half an hour to an hour previously, and it is of special importance to note the period of time that may have elapsed between the accession of the symptoms and the last meal, or administration of medicine.
When called in to a case of suspected poisoning, and in many cases where no suspicion at the time arises, the medical attendant should pay attention to the following points:
1. The time of the occurrence of the symptoms, and their character.
2. The time that has elapsed between their commencement and the last meal, dose of medicine, &c.
3. Have the symptoms continued without intermission or remission, and in an aggravated form, till death?
4. The order of their occurrence.
5. The previous health or illness of the patient.
6. Have the symptoms any relation to a particular meal or article of food, &c.?
7. If patient has vomited, have the vomited matters, especially the first, been carefully preserved?
8. Preserve all vomited matters, food, medicines, &c.
9. How many were at the meal, and was what was taken common to all, or only taken by a few?
2. Evidence from Post-mortem Appearances.—The morbid [Pg 237] appearances found in cases of poisoning will be treated more in detail when each poison, or group of poisons, comes to be separately considered. A caution may be given here against allowing the post-mortem signs of disease or external injury to exclude the idea of poisoning; for death may to all appearance be the result of disease or injury, and yet be caused by poison. An attention to the post-mortem appearances is important in all cases; for in many instances, where the symptoms were unknown to the experts at the time the inspection was made, they were subsequently found to correspond with the morbid changes which the autopsy revealed. The normal appearance of the stomach is white or nearly so, except during digestion, when it is reddened; yet we may sometimes come across cases in which the mucous membrane of this organ may be found so reddened as to lead to a suspicion of poisoning. The knowledge of this fact, and the absence of symptoms, will prevent an error in diagnosis. Ulceration from disease and from irritant poisoning must be distinguished. In that due to disease, the ulcers formed are, as a rule, small and circumscribed; in those from poison, there is diffused inflammatory redness over other parts of the stomach, and even in the intestines; and the poison, as in the case of arsenic, may be found adhering to the sides of the ulcer. Ulceration is more frequently the result of disease than of the action of poisons. Perforation of the stomach or intestines may be due to ulceration or to corrosion. The condition of the mouth and gullet will help the diagnosis. The appearance of the ulcer and the parts around it, together with the hints just given, must guide the diagnosis. Of post-mortem softening little need be said, beyond stating that it very rarely occurs, and is of course not preceded by symptoms. (For the diagnosis between inflammatory redness of the intestines and post-mortem staining, see page 45.)
3. Evidence from Chemical Analysis.—The objects of a chemical analysis are to determine: (1) The presence and nature of the poison. (2) The proportion or quantity of the poison taken. (3) The solution of certain questions connected with the administration of the poison.
The detection of poison in the body is of course the most important proof of poisoning; but it may be suggested that the poison was introduced after death, which, to say the least, is a most ingenious line of defence, but which, at the same time, must be held to be highly improbable, and impossible if found deposited in one or more of the solid organs. Again, granting that poison has been taken, is it the cause of death? This question may arise when injuries are found on the body, and it then becomes a matter of importance to know something of the symptoms which preceded death, and the morbid appearances found after death. The case of the girl who took arsenic to escape a beating by her father is a case in point. The father was tried for causing the death of the girl by undue severity, but it was subsequently shown that arsenic self-administered was the true cause of death. The poison may disappear from the body. This disappearance may be effected by vomiting, purging, or by the urine, or the poison may become absorbed [Pg 238] and decomposed. The person poisoned may live sufficiently long to allow of the entire elimination of the poison, and yet die of the induced exhaustion. (See case of Dr. Alexander, ante.)
Some poisons, especially those which are sparingly soluble, are with difficulty removed from the stomach, even by the most incessant and violent vomiting. This is notably the case with arsenic, which adheres to the mucous coat of the stomach with considerable tenacity. But even after all traces of the poison have left the stomach, it may be detected in the solid viscera.
Temporary deposit of poison in the organs or tissues (Taylor): (1) The Liver. (2) The Kidneys. (3) The Spleen. (4) The Heart. (5) The Lungs. (6) The Muscles. (7) The Brain. (8) The Fat. (9) The Bones.
With regard to arsenic, the following table, taken from Taylor, is of importance, as showing the amount of the poison which may be found in the liver at certain intervals:
| After taking the Poison. | Total Weight of Arsenic. | |
| In | 5½ to 7 hours | 0.8 grains. |
| 8¾ hours | 1.2 | |
| 15 hours | 2.0 | |
| 17 to 20 hours | 1.3 | |
| 10½ days | 1.5 | |
| 14 days | 0.17 | |
| 17 days | nil | |
Is it necessary that the poison should be found in the body or in the evacuations to lead to a conviction for poisoning? On this point, Christison was of opinion that if the symptoms, post-mortem, appearances, and moral evidence are very strong, it is not necessary that the poison be found in order to establish a charge of poisoning. This opinion was also supported by the late Dr. Geoghehan, Professor of Medical Jurisprudence in the Royal College of Surgeons, Ireland, and was also virtually acted upon in the case of Palmer, where the non-detection of strychnia was strongly dwelt upon by the counsel for the defence, but without success. Many of the vegetable poisons almost defy detection, except by the symptoms, post-mortem appearances, and some experiments on animals of doubtful value. The detection of poison in the food taken, or in the vomited matters, is of great importance; but it is of still greater importance if it can be found in the urine, drawn from the bladder, this being a proof that it has passed through the system. Here again a caution is necessary—for it must be remembered that poisoning may be feigned or imputed—the poison being mixed with the food and evacuations, and an innocent person accused.
The following suggestions should be carefully considered by every analyst when substances are sent to him for examination:
He should carefully note when and from whom the substances were received; in what state they were received—secured, or exposed—the number of articles, and whether properly labelled. He must make the [Pg 239] analysis himself, and state where it was made. The character and nature of the substances examined should be noted, and he must be prepared to give an outline of the methods or processes used for their determination. He must also be able to guarantee the purity of his reagents, and be prepared to answer the following questions:
The analyst may have the following submitted to him for examination: (1) Substances found on the accused, or in the room, or on the person of the deceased. (2) Articles of food. (3) Vomited matters, urine, &c. (4) Contents of the stomach. (5) Solid organs of the body.
He may also have his results called in question for the following reasons: (1) Purity of his reagents. (2) Faulty processes. (3) Hasty conclusions. (4) Experiments on animals.
Death may undoubtedly be due to the action of a poison, and yet its presence may fail to be detected, due to—(1) The nature of the poison-strychnia, hydrocyanic acid, &c. (2) Vomiting and purging. (3) Absorption and elimination. (4) Decomposition—phosphorus, chloral hydrate, chloroform. (5) Smallness of the dose.
(For directions for conducting a post-mortem examination in cases of poisoning, see page 61.)
4. Evidence from Experiments on Animals.—The evidence derived from experiments on animals with the contents of the stomach and vomited matters must not be too implicitly trusted, as these may give rise to vomiting and other symptoms when no poison is present. All animals are not alike affected with man by the same poisons; and it appears that the dog and the cat are the only animals that at all approach man with regard to the effects produced. Experiments on the lower animals are useless to decide—(1) The fatal dose of any poison. (2) The rate of absorption, deposition, or elimination of poisons. (3) The rapidity of the action of certain poisons.
In the case, however, of some vegetable poisons, the effects produced on animals by a portion of the substance taken by the person suspected of having been poisoned, may afford corroborative evidence of poisoning. In the case of Lamson, executed for poisoning his brother-in-law with aconite, experiments on animals formed the chief evidence against the accused.
5. Moral Evidence.—The moral evidence of poisoning is generally furnished by the common witnesses of the Crown; but the value of this kind of evidence, in many cases, can only be fully appreciated by a medical witness. To render this part of the subject as complete as possible, a few remarks may not be out of place. The suspicious conduct of the prisoner before and after the event, the recent purchase of [Pg 240] poison, the mode of administration, the object of the prisoner in getting rid of his supposed victim, and the fact of several persons being alike affected, should be carefully noted down. The anxiety evinced during the illness of the deceased, and the hurry in the funeral arrangements, showing an over-anxiety to remove all traces of his guilt, are suspicious. The probability of suicide is weakened by the state of the mind and the nature of the dying declarations of the deceased. In the case of a person indicted for poisoning, evidence to show motive in another case is admissible. (R. v. Geering, 18 L.J. [M.C.] 215; R. v. Heeson or Johnson; R. v. Garner, 3 F. & F. 681.)
Lastly, it remains to be considered—
What is the duty of a Medical Man who suspects the Action of Poison in a Patient on whom he is in attendance?
In the case of R. v. Wooler, Baron Martin, who tried the case, in his charge to the jury, stated that, in his opinion, the medical men in attendance ought, “when the idea of poisoning struck them, to have communicated their suspicion to the husband, if they did not suspect him; and if they did suspect him, they ought to have gone before a magistrate.” Suppose they had acted as the learned judge suggested, and spoken to the husband, who, had he been guilty, would in all probability have desisted from his terrible design for a time, then a great criminal would have been let loose on society, and without punishment. Then, again, had they applied to the magistrates, the delay caused by the indecision of the magistrates how to act in so delicate a case would have allowed the criminal to remove all traces of his design, and the means of testing their suspicions would have been lost; and, along with this, would have been lost the professional character and fortunes of the authors of the investigation. “There is a third course,” said the late Sir R. Christison, “and in my opinion it is the fittest of all: When the medical attendant is satisfied of the fact of poisoning, he should communicate his conviction to the patient himself. His predicament, in every other way, is so embarrassing, that he ought not to be deterred by the chance of injury to his patient from making so dreadful a disclosure.” (See an account of the same course being adopted in the case of Mr. Blandy by his physician, Dr. Addington, reported in Howell‘s State Trials, vol. xviii.)
Table giving the names of Diseases, the Symptoms of which resemble those the result of Irritant Poisons, together with such points of difference as may assist in distinguishing the one from the other:
Irritant Poison.—Symptoms of violent irritation in one or more portions of the alimentary canal. Pricking and burning of the tongue and mouth, and intense thirst, frequently accompanied with great constriction in the throat. Great abdominal pain and tenderness. Vomiting and purging are also usually present. The skin is hot and cold at intervals; the pulse small, frequent, and irregular. In the last stage the skin may become icy cold. An acrid, metallic, or burning taste in the mouth precedes the vomiting. The vomit and alvine discharges are generally mixed with blood. Death occurs in from six hours to two days and a half. [Pg 241]
Cholera.—Extreme and sudden prostration. The breath is cold to the hand in the last stages. The body is cold, shrivelled, and livid, or of a leaden hue. Vomiting and purging are present; the former is never bloody, the latter resembling rice-water. The thirst is intense, and in this particular alone resembles the effects of irritant poison. Death in from one to two days, or even less.
Summary of the General Evidence of Poisoning,
in a Tabular Form
| Poison. | Natural Causes. |
| 1. The symptoms come on suddenly, | 1. Many diseases come on |
| and rapidly progress. | suddenly—cholera, gastritis, |
| &c—and run a rapid course to | |
| a fatal termination. | |
| 2. The symptoms begin while | 2. Some acute diseases begin |
| the person is in sound health. | under like circumstances. |
| 3. The symptoms of poisoning | 3. This is also the case with |
| go on from bad to worse in a | many common diseases. |
| steady increase. | |
| 4. Uniformity in the nature of | 4. The uniformity of the symptoms |
| the symptoms. | is common to many diseases; |
| but in some cases the absence | |
| of uniformity may be a proof | |
| of disease. | |
| 5. The symptoms come on | 5. Apoplexy, colic, cholera, and |
| immediately after a meal. | some other diseases may follow |
| a meal. But the fact that some | |
| hours have elapsed since the | |
| last meal is against the | |
| probability of poisoning. | |
| 6. Several persons are attacked, | 6. As a general principle it may |
| after partaking of the same | be stated that there is no |
| meal, with the same symptoms. | disease likely to attack |
| several persons at once, but | |
| there are cases on record of | |
| this having occurred. | |
| 7. Poison found in the food, | 7. Poison may be mixed with food, |
| vomited matters, urine, &c. | &c, in cases of imputed poisoning. |
English Cholera.—In this disease all the symptoms of irritant poisoning are present. Pain in the belly, and vomiting. But in this disease the vomit and alvine discharges are never bloody, most frequently bilious. An acrid taste in the mouth and throat succeeds the vomiting. This is due to the acrid nature of the vomited matters. The stools contain bile in English cholera; in irritant poisoning, sometimes blood. Death is rare within three days.
Gastritis.—Acute idiopathic gastritis is so rare in this country as scarcely to need description. Most of the cases recorded of acute gastritis have been found to be due to irritants. We must, therefore, consider the period and order of the occurrence of the symptoms in relation to the last meal. Costiveness of the bowels would point to the presence of gastritis or enteritis, violent purging and vomiting to irritant poisoning.
Enteritis.—Though more common than gastritis, enteritis is a rare disease. The bowels are generally confined. Tubercular and[Pg 242] aphthous inflammation of the intestines may simulate irritant poisoning, especially chronic poisoning by arsenic. The post-mortem and a chemical analysis will reveal the true cause of death.
Peritonitis.—In the early stages of the disease vomiting is rare, and constipation is the rule, with marked tenderness over the whole abdomen. The morbid appearances in the peritoneum are seldom caused by irritants.
Perforation of the Stomach.—The symptoms supervene immediately after a meal; the pain, which is very acute, gradually extending over the abdomen. In most cases the patient has suffered for some time previously from dyspepsia.
Hernia.—Examine the seat of pain, the cause will be soon detected. But an omental hernia may be present, giving rise to twisting pain at umbilicus.
Intussusception of the Bowels.—Pain, sudden and confined to one spot below the stomach. Vomiting is present without purging, thus differing from diarrhœa and cholera. After a time the vomit becomes fæcal.
Colic.—May be confounded with poisoning by the salts of lead. If lead be taken in large doses, it produces the symptoms common to irritant poisons added to those of colic. In chronic lead poisoning, the blue line round the gums, the aspect of the patient, and history of the case, will point to the true cause of the symptoms. Lead colic is also generally accompanied with extreme depression of spirits.
Rupture of Internal Organs.—Rupture of the stomach, duodenum, gall-bladder, and impregnated uterus, is of rare occurrence. The autopsy will show the true cause of death.
Table giving the names of Diseases the Symptoms of which resemble those the result of Narcotic Poisoning, together with such points of difference as may assist in distinguishing the one from the other:
Narcotic Poisoning.—Giddiness, headache, drowsiness, and considerable difficulty in keeping awake. Paralysis of the muscles, convulsions, ending in profound coma and death. The symptoms of narcotic poisoning begin not later than an hour, or at most two hours, after the poison is taken, except in the case of poisonous fungi and spurred rye, when a day or two may elapse. The symptoms of narcotic poisoning advance gradually. The person may, in most cases, be roused from the deepest lethargy. The pupil in opium poisoning is, as a rule, contracted. Recovery seldom occurs after twelve hours; in most cases, death takes place in six or eight hours—the shortest time being three hours.
Apoplexy.—In some cases apoplexy is preceded by warning symptoms—headache and giddiness. As a rule apoplexy is a disease of old age, and of stout, plethoric people. If the symptoms do not come on for some hours after food or drink has been taken, this disease is to be suspected; but it may occur at or immediately after a meal, too soon to be the result of the action of narcotics—ten to thirty minutes always elapsing before these poisons act. Apoplexy generally comes on suddenly, coma at once present. It is seldom possible to rouse the person when the sopor of apoplexy is fully developed. The pupils in apoplexy are usually unequal or dilated; but should the effusion of blood take place into the pons Varolii, the pupils may be contracted, hence closely simulating opium poisoning. Apoplexy may last for days, or death may occur in an hour.
Epilepsy.—Loss of consciousness and presence of convulsions mark this disease; and in these it resembles poisoning by prussic acid. Epilepsy is in most cases a chronic disease. Warnings—aura epileptica—are often present. The fit begins violently and abruptly. The paroxysm generally lasts for some time, and death rarely occurs during the first attack. [Pg 243]
Table showing Points
of Difference in the Action of
Corrosive and Irritant Poisons
| Corrosives. | Irritants. |
| 1. Destruction of the parts to | 1. Irritation of the parts to |
| which they are applied. No | which they are applied |
| remote action on the system. | producing inflammation. |
| Remote action present in | |
| most of the irritants. | |
| 2. Symptoms supervene immediately | 2. Symptoms may rapidly |
| they are swallowed, and consist | supervene after they are |
| of a burning, scalding pain | taken, or some delay may |
| elt in the mouth, gullet, and | occur, due to the state of |
| stomach. | concentration or dilution |
| of the poison. Pain in | |
| the stomach and bowels, | |
| more or less severe, is | |
| always present with the | |
| other signs of irritation. | |
| 3. Death may result from— | 3. Death may result from— |
| (1) Shock. | (1) Shock. |
| (2) Extensive destruction of | (2) Irritation, causing |
| the parts touched. | |
| (3) Starvation. | (3) Protracted suffering. |
| (4) Suffocation, the result of | (4) Starvation. |
| œdema, or spasms due to | |
| acid in larynx. | |
| 4. Post-mortem appearances: | 4. Post-mortem |
| corrosion and extensive | appearances: irritation |
| destruction of tissue. | and signs of inflammation, |
| ulceration, &c. |
The principal modes of procedure are as follows:
1. To remove the poison from the digestive tract, or neutralise it or render it insoluble by the administration of suitable antidotes.
2. To overcome the effects of that which has been absorbed.
3. To promote its elimination.
4. To alleviate dangerous symptoms, and endeavour to keep the patient alive until the effects of the poison have passed off.
To forcibly empty the stomach, emetics may be administered or other means used to induce vomiting, or the stomach pump or tube may be employed.
Suitable emetics are sulphate of zinc in thirty-grain doses dissolved in warm water, a dessert-spoonful of mustard in half a pint of warm water, ipecacuanha wine in tablespoonful doses, copious draughts of hot water. Tartar emetic and sulphate of copper should be avoided, except in cases of phosphorus poisoning, when the latter may be used. The hypodermic injection of ⅒ grain of apomorphine is a very useful emetic, especially in cases of narcotic poisoning. Irritation of the fauces with the finger or a feather promotes vomiting, and may be useful in the absence of an emetic.
The stomach tube or pump is most useful in that it is under the control of the operator and enables him to thoroughly wash out the stomach. [Pg 244] After passing the tube, previously lubricated with vaseline or glycerine, through the œsophagus down to the stomach, a pint of warm water should be first injected before withdrawing any of the contents. By alternate injection of water and its withdrawal, the stomach may be efficiently cleansed, and at the same time solutions of suitable antidotes may be passed into it. It must be remembered that neither the stomach pump, syphon tube, nor emetics, are to be used in cases of poisoning with corrosives, with the exception of carbolic acid. The tube should be used with great caution in cases of irritant poisoning.
Antidotes are remedies which counteract the effects of poisons. They act mechanically, e.g. flour and water, chalk mixture; chemically, as magnesia and chalk in mineral acid poisoning, alkaline sulphates in lead and barium poisoning; and physiologically, as antagonists, such as morphine and atropine, atropine and physostigmine, strychnine and chloral hydrate.
To counteract the effects of the portion of the poison absorbed, special treatment is necessary: purges and diuretics may be called for; artificial respiration may be necessary; cardiac depressants require cardiac stimulants; the cold douche as a restorative and external warmth are desirable in certain cases. Sedatives may be administered to alleviate convulsive seizures. Tracheotomy may be required in cases with laryngeal complications; and pain, exhaustion, excessive vomiting or purging are to be treated by appropriate remedies.
The number and condition of the vessels received should be noted and copies made of any affixed labels.
The appearance, smell, colour, and reaction to test paper of the contents should be noted, and their weights and volumes determined. All jars, wrappers, labels, and seals should be preserved for future reference.
The stomach contents should be carefully examined in reference to their nature, colour, and smell, and the presence or absence of any abnormal constituents. The mucous membrane of the stomach should be examined with the naked eye and by the aid of a lens, the surface washed with distilled water, and the washings added to the contents.
There is often some clue as to the nature of the poison afforded, and the investigation should be made for it first; the presence or absence of other poisons, however, must be determined. If there be no clue, then a systematic examination must be carried out. The poison must be looked for not only in the contents of the stomach, but in the viscera as well; it must be remembered that poison may be introduced into the stomach after death.
Volatile poisons, such as alcohol, chloroform, prussic acid, may be separated by distillation after acidulation with tartaric acid. Arsenic is best separated by drying the organic material, and distilling after adding strong hydrochloric acid. [Pg 245]
Other metallic poisons may be tested for, with or without destruction of organic matter. To destroy the organic matter, the moist method is the one in general use: After reducing the contents of the stomach or the viscus to a pulp, they are mixed with distilled water to the consistency of thin gruel, and placed in a flask with some crystals of potassium chlorate—half an ounce to each pound of the liquid. Pure hydrochloric acid is added, and the flask gently heated on a water bath, a mixture of chlorine and oxides of chlorine is given off and gradually breaks up the organic matter, converting at the same time any mineral poison present into the chloride. This procedure is followed until the material becomes quite limpid, more chlorate or hydrochloric acid may be added if necessary. It is then transferred to an evaporating dish and heated on the water bath until the smell of chlorine disappears. It is then filtered while hot, to allow chloride if present to pass through; a stream of sulphur dioxide is passed through the filtrate when cold, to reduce any metals present to a lower state of oxidation. Silver chloride will not pass through the filter in this process, so it has to be dealt with in a special manner.
In making a systematic analysis, volatile poisons must be tested for first, then ascertain the presence or absence of alkaloids, after which the inorganic poisons must be dealt with.
General Characters.—The mineral acids have no remote effects on the system; their action is purely local. They are seldom used for the purpose of homicide, except in the case of young children. By suicides they are more frequently employed.
The Symptoms common to the action of these acids supervene immediately the acid is swallowed, and consist in a sensation of burning in the mouth and gullet. Dreadful pain is felt in the stomach, attended with constant eructations, and vomiting of a brownish or blackish matter, mixed with blood. Mucus, together with, in severe cases, portions of the mucous membrane of the stomach, may be detected in the vomited matters, which have an intensely acid reaction, changing the colour and destroying the texture of cloth or other material on which they may fall. The act of swallowing is attended with intense pain, and not infrequently is rendered quite impossible. The thirst is intense, the bowels are confined, and the urine is diminished in quantity. The pulse is small and weak, and the skin clammy and cold. Respiration is performed with difficulty, and the countenance expresses the most intense anxiety. Sometimes, when the upper part of the windpipe is implicated, there is more or less cough and difficulty of speech. Death may even result from suffocation—the skin, in this case, presenting a cyanosed appearance. The mouth is excoriated, the lips shrivelled and blistered. In children, when the acid has been poured far back into the mouth, by forcing the bottle backwards before emptying it of its contents, the mouth may more or less escape injury, and the signs in it of corrosive poisoning be absent. The teeth may become loose, and fall out of the mouth. The mental faculties remain clear, death generally coming on suddenly, the patient dying convulsed or suffocated. The period at which death ensues is very variable, and considerable power for locomotion may be retained by the sufferer, though, as a rule, he is found writhing in exquisite agony on the floor or elsewhere. Some cases recover, leaving the coats of the stomach more or less injured, and the general health greatly impaired.
Post-mortem Appearances.—The body externally is healthy. The lips and external parts of the body, which have come in contact with the acid, are charred. The mucous membrane of the mouth, shrivelled and eroded, is whitish, yellowish, or brownish, sometimes [Pg 247] appearing “as if it had been smeared with white paint” or thin arrowroot. Many of the appearances above described will depend upon the rapidity with which death has followed the swallowing of the poison. The mouth, gullet, and trachea may alone show any signs of the corrosive action of the poison, and it is important to remember that death may be due to sulphuric acid, and yet the acid may never have reached the stomach. In one or two cases where the poison was poured into the mouth during sleep, and in the case of children in whom the mouth was held open, there were no signs of the poison on the lips, and the mouth even escaped in one or two cases. The stomach, in some cases more or less contracted and perforated by the corroding action of the acid, may contain a dark grumous liquid, the acidity of which will depend upon the treatment adopted, or the length of time that may have elapsed from the swallowing of the acid to the fatal termination. The stomach also appears as if carbonised, this being due to the action of the acid on the effused blood; no such appearance being produced when sulphuric acid is poured into the dead stomach. Corrosive action may be found in the duodenum. In cases where the patient has survived from sixteen to twenty hours, the small intestines have been found inflamed. The blood, Casper states, is never fluid in acute poisoning by sulphuric acid, but always “syrupy at least, and sometimes ropy; it has a cherry-red colour, and acid reaction.” Sulphuric acid is also said to possess powerful antiseptic properties, and that bodies of those who have died from its effects remain long fresh.
There are two things which may render the diagnosis difficult—(1) Gastric ulcer. (2) Post-mortem digestion of the stomach.
Gastric ulcers vary in size from that of a threepenny-piece to that of a florin, or larger. In shape they are round or oval, and present the appearance of shallow but level pits, with sharp, smooth, vertical edges—appearing as if they had been punched out. The peritoneal opening is smaller than that on the internal surface of the stomach. The absence of injury to the mouth and gullet will distinguish gastric ulcer and post-mortem softening from the action of corrosive poisons.
General Treatment.—Chalk, carbonate of magnesia, bicarbonate of soda, the plaster from the walls or ceiling of the apartment stirred in water, and followed by diluent drinks—barley water, linseed tea, &c. The use of the stomach pump is contra-indicated.
Forms.—Sulphuric acid occurs in two forms—concentrated and diluted.
Characters.—Concentrated sulphuric acid or oil of vitriol (specific gravity, 1.800 to 1.845), as it is found in commerce, is a heavy, oily, colourless, or slightly brownish-coloured liquid, not fuming when exposed to the atmosphere; but, when added to water, causing a rapid increase of temperature, which may crack the glass [Pg 248] vessel in which the mixture is made. Sulphuric acid chars and destroys the texture of organic bodies placed in it. Dilute sulphuric acid is a colourless, strongly acid liquid, reddening litmus, and charring paper dipped into it when subsequently dried, care being taken not to scorch the paper.
Symptoms, &c.—The symptoms and post-mortem signs have been already described, p. 246.
Chemical Analysis and Tests.—The acid will have to be examined under the following heads: (1) Simple, concentrated acid. (2) Dilute acid. (3) Mixed with organic liquids, food, vomit, &c. (4) On the clothes of the person injured.
I. Concentrated Acid
1. Chars Organic Matter.—A piece of wood or paper placed in the strong acid rapidly becomes blackened.
2. Heat when added to Water.—Equal quantities of acid and water added together produce intense heat.
3. Evolution of Sulphurous Acid.—When boiled with chips of wood, copper cuttings, or mercury, fumes of sulphurous acid are evolved, detected by their sulphur-like odour, and by their power of first bluing and then bleaching starched paper dipped in iodic acid.
II. Dilute Acid
1. Chars Paper.—This only occurs when the paper is dried by the aid of heat, subsequently to moistening it in the dilute acid.
2. Precipitation of Sulphate of Barium.—A solution of the nitrate or of the chloride of barium is precipitated by sulphuric acid in the form of a white insoluble powder, unaffected by nitric or hydrochloric acid, even when heat is applied. This test is so delicate, that a liquid containing ¹/₂₅₀₀₀th part by weight of the acid is precipitated by either of the test solutions.
3. Action of Heat.—The dilute acid is entirely volatilised by heat.
III. Mixed with Organic Liquids, &c.
In tea, coffee, or beer the mode of applying the tests are the same, the mixture being previously filtered, or the acid separated from the organic mixture by dialysis, or the following cautions are necessary:
Objection A.—Alum, or any acid sulphate, would give all the reactions with the nitrate and chloride of barium.
Answer A.—Evaporate a portion of the doubtful liquid; if pure acid, there will be no residue, sometimes only the slightest trace of sulphate of lead.
Objection B.—Erroneous estimation of free sulphuric acid, in consequence of the presence of some saline or neutral sulphates.
Answer B.—Evaporate as before. The free sulphuric acid separated by warming the liquid is then added to a known weight of powdered carbonate of baryta until effervescence ceases. The resulting precipitate when weighed, represents the free sulphuric acid present. [Pg 249]
Calculate in the following manner—
In the above equation, 98 parts of H₂SO₄ take the place of 44 parts of CO₂. If, therefore, 100 grains of BaCO₃ renders the liquid neutral, the amount of free SO₄ present will be represented by the increased weight of the precipitate in the proportion of 54 to 98, the difference between 44 and 98 the equivalent of CO₂ + SO₄.
To extract the acid from organic mixtures, digestion with alcohol is required: filter and neutralise the filtrate with caustic potash, evaporate to dryness, and dissolve the residue in distilled water acidulated with hydrochloric acid; the previous tests may then be applied. Extraction with alcohol leaves behind combined acid in the form of sulphates. The presence of free acid in the filtrate or original mixture may be detected by the change of tropæolin solution from yellow to crimson or ruby colour when added to it; or on adding a few drops of the mixture or filtrate to a solution of potassio-tartrate of iron B.P. in water, so as to make it of a yellow tinge, and to which potassium sulphocyanide has been added, the liquid changes from a yellow to a port-wine colour.
IV. Stains on the Clothes, &c.
1. The strong acid changes the colour of black woollen cloth to a dirty brown, the edges of the spots assuming a reddish tint after a few days. The dilute acid on the same cloth produces a red stain, which in time becomes brown.
2. The spots made by the strong acid remain damp for some time—strong sulphuric acid, having a great affinity for water, continually absorbs moisture from the atmosphere.
3. The spot should be cut out, boiled in distilled water, or digested with alcohol, filtered and tested for free sulphuric acid.
4. A portion of the cloth not touched by the acid should be tested, in order to show that the sulphuric acid found is not due to sulphates present in the cloth.
5. An acid sulphate—bisulphate of potash—gives a reddish stain to black cloth like that produced by the dilute acid. Test for this salt by incineration.
Fatal Period.—Average time before death ensues is from two to twenty-four hours. The shortest time was one hour, but in children death may be instantaneous. Life, however, may be prolonged for some weeks, or even months.
Fatal Dose.—One drachm in a healthy adult has proved fatal; on the other hand, however, four ounces have been swallowed without being fatal.
Treatment.—As before mentioned.
N.B.—This acid in past years has given rise to several actions, it having been employed to disfigure the person by throwing it in the face. [Pg 250]
Forms.—Strong nitric acid, and dilute nitric acid.
Characters.—This acid is commonly known as aqua fortis, or red spirit of nitre. It is seldom used as a poison.
The strong acid varies in colour from a pale yellow to a deep orange. The colour is due to admixture with peroxide of nitrogen. On cloth and articles of dress it produces yellow stains, which are darkened by the application of an alkali. If poured on copper cuttings, reddish fumes of nitrous acid are given off. Dilute nitric acid is a colourless acid liquid, not precipitated by nitrate of barium or nitrate of silver, showing absence of sulphuric and hydrochloric acids. All its alkaline salts are soluble in water.
Symptoms.—The symptoms have been before described, and are similar to those produced by sulphuric acid, though not quite so severe. The vapour of this acid has caused death in eleven hours by congestion of the bronchial tubes and lungs; care should, therefore, always be taken not to inhale the fumes given off by the acid in the manufacture of gun-cotton, &c.
Post-mortem Appearances.—Same as the mineral acids generally, but the tissues touched are turned yellow, and if bile be in the stomach it is turned green. The stomach is rarely perforated.
Chemical Analysis.—Nitric, like sulphuric, acid will be examined under four heads; but being a volatile acid, easily decomposed, and also having its nature changed by contact with organic substances, its presence on clothes may fail to be detected after a few weeks. The colour of the stain on cloth may also remain, although the acid has been entirely removed by washing. 1. Strong, concentrated acid. 2. Dilute acid. 3. Mixed with organic liquids, &c. 4. On the clothes of the person injured.
I. Concentrated Acid
1. Volatility.—When exposed to the atmosphere, strong nitric acid gives off colourless or orange-coloured acid fumes. Heated in a watch-glass, it is evaporated without residue.
2. Action on Organic Matter.—The acid leaves on woollen clothes a yellow-coloured stain, which is darkened by the addition of an alkali. The colour of the stain is due to the formation of picric acid.
3. Action on Metals.—Gently heated in a test tube with copper filings, orange-coloured fumes are given off, which redden but do not bleach litmus paper. Starch paper treated with iodide of potassium becomes purple.
4. Solution of Gold.—If a small portion of gold leaf be put into the acid, no effect is produced; but on the addition of concentrated hydrochloric acid, the metal is rapidly dissolved.
II. Dilute Acid
1. Absence of sulphuric and hydrochloric acids, proved by no precipitate being formed with nitrate of barium and nitrate of silver. [Pg 251]
2. It does not char paper when the paper is heated, as is the case with sulphuric and hydrochloric acids.
3. If a piece of filtering paper be dipped into a solution of the acid saturated with carbonate of potash, dried and ignited, it will burn like touch-paper.
4. The acid liquid, saturated with carbonate of potash and evaporated, deposits fluted prisms which do not effloresce or deliquesce on exposure. Neutralised with soda, the crystals are of a rhombic form.
5. A crystal, so formed, moistened with distilled water on a plate, and then heated with strong sulphuric acid and allowed to cool, gives with—
(1) A piece of green sulphate of iron—a dark green ring round the crystal.
(2) A small portion of morphia—a rich orange colour, a yellow liquid being formed.
(3) A small portion of brucine—a blood-red colour.
6. If an aqueous solution of diphenylamine be added to a solution containing nitric acid, in a test tube, and pure sulphuric acid be poured down the side of the tube to form a layer at the bottom, a blue colour forms at the junction of the two liquids.
III. Mixed with Organic Liquids, &c.
Due to the measures employed by way of treatment the vomited matters may be neutral and yet nitric acid be present. The method adopted with viscid and turbid organic mixtures is to dilute them with pure water, and then filter. If the filtrate be acid, it is neutralised with carbonate of potash, evaporated, and then set aside to crystallise, and the crystals purified by digesting them in ether or alcohol. The crystals are again dissolved and re-crystallised. The tests just mentioned should then be employed. It should be remembered that nitric acid has a strong tendency to combine with solid organic structures, and to become decomposed. The parts of the body stained by the acid should, therefore, be digested in water at a gentle heat, the liquid cooled, filtered, and neutralised with carbonate of potash, and then examined for nitre.
IV. Stains on the Clothes, &c.
Macerate the piece of cloth in distilled water by the aid of heat. If the solution be acid, neutralise with carbonate of potash, and filter. Test the solution as before mentioned.
The action of the dilute solution of caustic potash on the following stains on cloth is characteristic: Nitric acid stain becomes of a clear orange tint. Iodine stain disappears. Bile stain remains unchanged.
Fatal Period.—Death may take place in an hour and a half, or life may be prolonged for some months. [Pg 252]
Fatal Dose.—Two drachms; recovery has taken place after half a fluid ounce of the strong acid has been taken.
Treatment.—As before mentioned when speaking of the acids generally.
Forms.—Strong and the dilute acid. It is known as muriatic acid, or spirits of salts.
Characters.—Strong hydrochloric acid is either colourless or has a bright yellow tint, due to the presence of the perchloride of iron. It fumes in the air, and gives rise to dense white fumes when a glass rod moistened with ammonia is held over the surface of the acid. The dilute acid is colourless.
Symptoms.—Poisoning with muriatic acid is so rare that the symptoms have not been well studied, but they do not appear to differ much from those produced by the action of the other acids. It does not stain the skin, but may darken the mucous membranes. The fumes are apt to attack the air-passages.
Chemical Analysis.—The acid will have to be examined under the following heads: 1. Simple, concentrated acid. 2. Dilute acid. 3. Mixed with organic liquids, food, &c. 4. On the clothes of the person injured.
I. Concentrated Acid
1. Action on Organic Matter.—The strong acid tinges most organic tissues, when immersed in it, a yellow colour. The stains on black cloth are at first distinctly red, becoming reddish-brown after a few days.
2. Action on Metals.—This acid does not act on copper or mercury, even when boiled with them, and this distinguishes it from the other acids.
3. Hydrochloric acid, added to peroxide of manganese and then warmed, gives off chlorine gas, detected by its greenish-yellow colour and suffocating odour. The vapour thus produced bleaches litmus paper, and causes a blue coloration on starch paper moistened with iodide of potassium.
II. Dilute Acid
1. Decomposes alkaline carbonates, chlorides being formed which, when heated in the solid state with strong sulphuric acid and peroxide of manganese, evolve chlorine gas, known by the before-mentioned tests.
2. Precipitation of Chloride of Silver.—A white curdled precipitate of chloride of silver is thrown down when a solution of nitrate of silver is added to hydrochloric acid. This precipitate becomes grey on exposure to light. If a portion of the precipitate be added to ammonia it will dissolve; another portion, when boiled with nitric acid, is unaffected; and a third portion, ignited in a capsule, becomes converted into a horny mass. [Pg 253]
In any case where there is a doubt as to whether the hydrochloric acid exists in the free state, or is only present in the form of chlorides, the following test should be resorted to, which will not only discriminate between the two forms, but give the relative amount of each present:
Take two equal measures of the acid liquid. Precipitate one with nitrate of silver, after the addition of nitric acid, and weigh the precipitate. Evaporate the second portion of the acid liquid to dryness, and dry the residue in a water bath; dissolve this residue in distilled water, and treat the solution with nitrate of silver as before, weighing any precipitate which occurs. The weight of chloride of silver obtained from the first portion of the liquid will give all the hydrochloric acid present, both in the free state and in combination; while the weight of the silver precipitate in the second portion of liquid only gives the chlorides, all free—hydrochloric acid having passed off during the process of evaporation.
III. Mixed with Organic Liquids, &c.
The suspected acid liquid should be filtered, and then distilled almost to dryness. The portion of the distillate which comes over at first may be thrown away; but the latter portion will give all the reactions before described for hydrochloric acid, if that be present. Distillation is adopted in the case of this acid, as it is more volatile than either sulphuric or nitric acid. It may be objected that the acid found in the vomited matters is from the gastric juice. In answer to this, it may be stated that the free hydrochloric acid in normal gastric juice is only about five grains in sixteen ounces, an amount which would give but slight reaction with the tests.
IV. Stains on the Clothes, &c.
The spots produced by the action of the acid on black cloth are at first of a bright red colour, changing in ten or twelve days to reddish-brown. These spots may be cut out and macerated in warm water; the liquid thus obtained then tested by nitrate of silver and the other tests before noticed. Another portion of the cloth should be treated in the same manner, and the resulting liquid tested, as a control against the objection that the acid might have been present in the cloth. Hydrochloric acid has been used to erase writing from paper in attempts at forgery, &c. The paper must be treated in the same manner as mentioned for the cloth, and the tests used. Sometimes oxalic acid is employed for a like purpose, in which case the nitrate of silver will give a precipitate; but the oxalate of silver is soluble in nitric acid; the chloride is not soluble even when boiled.
Fatal Period.—From two or five hours to thirty hours or more.
Fatal Dose.—One fluid drachm to one ounce; recovery has taken place after swallowing two fluid ounces.
Treatment.—The same as for the other acids. [Pg 254]
Table showing the Colour produced by
the Action of
the Mineral Acids
on the Skin and on Cloth
| Skin. | Cloth. | |
|---|---|---|
| Sulphuric acid. | Brown colour. | Dirty-brown edges becoming |
| red after a few days from | ||
| absorption | ||
| Nitric acid. | Bright yellow, due to | Yellow, orange-red, or brown. |
| the formation of | ||
| picric acid. Colour | ||
| heightened by | ||
| alkalies. | ||
| Hydrochloric acid. | Greyish-white. | Bright red changing after some |
| days to reddish-brown. |
A dark blue liquid formed by dissolving indigo in strong sulphuric acid. Used as a dye. The symptoms are much the same as those detailed under sulphuric acid, with the additional bluing of the mouth and lips. It may be detected with the tests given under sulphuric acid, the blue colour being first discharged by boiling it with nitric acid.
Phenol. Phenic Acid. Coal-tar Creosote. Oil of Tar
Carbolic acid is obtained in the dry distillation of coal, and forms the acid portion of coal-tar oil, from which it is subsequently extracted by shaking the crude coal-tar oil with a mixture of slaked lime and water. After allowing the mixture to stand for some time, the watery portion is separated from the undissolved oil, the former treated with hydrochloric acid, and the resulting oily fluid purified by careful distillation. Up to the year 1900 no restrictions were put upon the sale of carbolic acid, but owing to the large number of suicidal and accidental deaths from its use, it was by Act of Parliament scheduled as a poison, and all preparations containing more than 3 per cent. of it, cresylic acid, or their homologues, must be sold as poisons.
Pure carbolic acid forms long, colourless, prismatic needles, which melt at 35° C. into an oily liquid. It boils at 180° C., and greatly resembles creosote, for which it is very frequently substituted in commerce, but from which it differs in the following characters: It does not affect polarised light as creosote does; it forms a jelly-like [Pg 255] mass with collodion, and is soluble in a solution of potash, whereas creosote is unaffected by collodion, and is insoluble in a solution of potash. It possesses a penetrating, characteristic odour; burning taste; is slightly soluble in water, but freely so in glycerine, ether, and alcohol; and gives no acid reaction to test paper. When undiluted, it attacks the skin, which it shrivels up.
Creosote is obtained from wood-tar, which imparts to it its caustic properties.
Carbolic acid acts as a corrosive and anæsthetic on the skin and mucous membranes, and as a narcotic on the brain. Its poisonous properties are exerted whether it be swallowed or merely applied to the skin, especially if a wound be present.
Effects on the Skin, &c.—Strong carbolic acid, when applied to the skin, corrugates, hardens, and destroys its sensibility, and is said to whiten it; though in one case, in which the crude acid had been taken with a suicidal intent, there was after death a dark brownish ring about half an inch wide surrounding the mouth; and in another, that of a child who, in climbing to a shelf, poured over its face and neck about half a saucerful of diluted acid, the colour of the skin touched by the acid was yellowish-white and yellowish-brown, dry and parchment-like. The action of the acid on the mucous membranes is similar to that on the skin, but the corrugation is more marked, and considerable softening and peeling may also take place.
Effects on the Nervous System.—Rapidly supervening stupor, total muscular relaxation, anæsthesia, and stertorous breathing are among the most prominent symptoms. Nearly all the sufferers die comatose. Carbolic acid appears to act principally on the central nervous ganglia at the base of the brain and on the spinal cord. The evidence is more in favour of its action on the brain than on the spinal cord, and not at all on the periphery of the nerves. The muscles contract vigorously after death, in response to galvanic stimulation applied either to the nerves or to the muscles themselves.
Effects on the Circulation.—The action of carbolic acid on the circulation has not yet been fully worked out, but it appears to be a cardiac depressant, the heart being arrested in diastole.
General Symptoms.—As soon as the acid is swallowed, the patient complains of intense burning pain in the mouth, throat, and stomach, the pupils are contracted, the conjunctiva insensible to touch, the skin cold and clammy, the temperature rapidly falls, and the pulse becomes weaker and weaker, till it is almost imperceptible. The breathing is laboured, and, as the fatal issue approaches, becomes stertorous; vomiting of frothy mucus occurs in some cases. The invasion of the symptoms is most rapid, and many of the patients have been in an insensible condition when found. The above symptoms have even supervened when the strong acid has been used for dressing wounds.
Dr. J. Hamilton records a case where the acid was used as an application to a wound four inches long, in a child four and a half years of age. Direct contact of the acid with the wound was prevented. [Pg 256] About an hour after the dressing was applied he saw the patient, who was then supposed to be suffering from the effects of chloroform used during the operation on the child‘s arm. She was suffering from symptoms like those before described. On removing the dressing, some of the carbolic acid, it was found, had melted and run into the wound, and to this Dr. Hamilton attributed the symptoms. The child ultimately died. (See British Medical Journal, 1873, vol. i. p. 226.)
The urine and fæces, when passed, are of a dark colour, and it has been frequently noticed that the urine passed by the assistants in surgical hospitals, who, under the antiseptic methods adopted, are constantly washing their hands in solutions of carbolic acid, is of an olive-green colour. This shows that absorption takes place readily through the skin. Bilroth, in his work on Clinical Surgery, gives several instances of absorption in this way. Nephritis with casts in the urine may occur. The hypodermic administration of carbolic acid, twelve to twenty-four grains in a day, has failed in five cases under my observation to be followed by carboluria.
Post-mortem Appearances.—If the poison has been drunk, a dark brownish horny rim may be found soon after death round the lips; the mucous membrane of the mouth and stomach is whitened, corrugated, and softened, and looks as if smeared with white lead—in some cases, horny in patches; inflammatory signs being absent or only slightly visible. The blood is uniformly fluid, becoming a bright red on exposure. The smell of carbolic acid is detected in the stomach, and sometimes in the small intestine, and even in the spleen, liver, and kidneys. In Dr. Ferrier‘s case, the urine found in the bladder after death had a slight olive-greenish tint with a peculiar mixed odour, which gave the usual reactions to the tests for carbolic acid. The dark colour of the urine is not due to the presence of hæmin, as the urine, in poisoning by carbolic acid, does not contain more than a normal amount of iron; the colour is, therefore, probably due to some product formed by the partial oxidation of the acid as hydroquinone. Signs of nephritis may be present. The left ventricle of the heart is, in most cases, found contracted, the right flaccid. The lungs are congested, and this may also be the case with the vessels of the brain; but there may be an entire absence of any post-mortem signs to point to the probable cause of death, where the poison has gained entrance through a wound when the acid has been used as a surgical dressing.
Chemical Analysis.—Carbolic acid may be separated from mixture with organic substances by distillation with dilute sulphuric acid, from urine by agitation with ether. Bromine water, as recommended by Landolt, gives a bulky yellowish precipitate of tribromo-phenol. The precipitate should then be collected, well washed, and gently warmed in a test tube with sodium-amalgam and water. The liquid poured into a dish and acidulated, will, if phenol be present, give the characteristic odour of that substance, and it may be seen floating in the liquid as an oily fluid. By this test, one part of phenol in 43,700 of water may be detected. It must be remembered that, according to Landolt, carbolic acid is normally present in the urine, but Hoppe [Pg 257] Seyler contends that it is not originally present in urine, but is formed by the action of sulphuric acid, probably from indican. Carbolic acid urine, treated with nitric acid, and then with potassæ, and concentrated, becomes blood-red, brown-red, and then changes from pea-green to violet. Carbolic acid mixed with urine does not give the above reactions (Schmidt‘s Jahrbücher, Bd. clxiv. p. 144).
A solution of carbolic acid, mixed with one-fourth of its volume of ammonia and a few drops of bleaching powder solution (1 in 20 of water), and then warmed, but not boiled, assumes a blue colour (green in very dilute solutions), becoming red on the addition of sulphuric or hydrochloric acid. The perchloride of iron gives a violet colour with carbolic acid.
Fatal Period.—Death has occurred in three minutes; also delayed to sixty hours; usually three to four hours.
Fatal Dose.—One drachm has caused death in twelve hours. A child six months old died from the effects of a quarter of a teaspoonful of a solution of one part of the acid to five of glycerine. Recovery has taken place after an ounce of 90 per cent. strength liquefied acid, also after four ounces of the crude acid; after six ounces of the crude acid, 14 per cent. strength; and in a child of two after half an ounce of crude acid of 30 per cent. strength.
Treatment.—Stomach pump. Wash out the stomach with equal quantities of alcohol and water mixed—whisky, brandy, gin, or rum will do until absolute alcohol or rectified spirit be obtained. The washing should be repeated every 5 to 15 minutes from four to eight times; apomorphine hydrochlorate gr. ⅒ should be given hypodermically at the commencement, and the administration of demulcent drinks. Emetics are of little or no use, owing to the anæsthesia of the mucous membrane of the stomach. The sulphate of soda, Glauber salts, has been proposed as an antidote. Any soluble sulphate may be tried. Oil or vinegar is the best outward application to the skin, after washing with spirit of wine or methylated spirits.
This is a powerful corrosive and cardiac poison, but on account of its strongly acid taste it is ill-adapted for the purposes of the murderer. Deaths have not infrequently followed the accidental substitution of this substance for Epsom salts—sulphate of magnesia—which it somewhat closely resembles.
The ordinary crystals of oxalic acid are in the form of four-sided prisms, colourless, transparent, odourless, or with a slight acid smell, very acid taste, and not deliquescent in the air. It is largely used in the arts, by brass-polishers, straw-bonnet makers, book-binders, and others. The acid is also used to remove writing-ink from parchment, paper, &c., for the purposes of forgery, &c.
Symptoms.—These present many strange anomalies. In a large dose—an ounce or more—oxalic acid acts as a corrosive; in a smaller, as an irritant; and in a still smaller dose, as a cardiac sedative. [Pg 258] Death has been known to occur so rapidly as to prevent any attempt at treatment. When the dose is large, an acid taste is experienced during swallowing, followed by burning pain in the throat and stomach. Vomiting then sets in, and in most cases continues till death, which may, however, occur when this symptom has existed from the first. The vomited matters may be simply mucus, mucus and blood, or dark coffee-grounds-looking matter. Unless the case is protracted, the bowels are rarely much affected, though purging and tenesmus have been noticed. Occult blood may be present in the fæces. Collapse now sets in; the pulse becomes feeble and scarcely perceptible, the skin cold and clammy, showing the action of the poison on the heart probably through the central nervous, as well as through the intra-cardiac ganglia. Should the treatment adopted prove successful, and life be prolonged, the patient complains of tenderness of the mouth, soreness of the throat, and painful deglutition. Pressure over the abdomen causes pain. Vomiting and purging are also frequently present; and if recovery takes place, convalescence is generally very gradual. The urine may contain a large quantity of albumen, casts are numerous, and oxalates in crystal form are present.
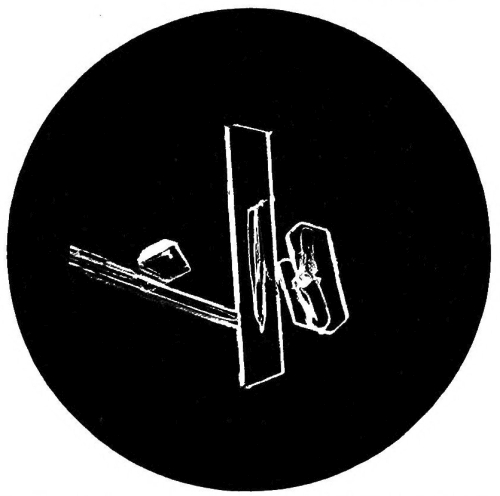
Fig. 28.—Photo-micrograph
of crystals of oxalic acid, × 50.
(R. J. M. Buchanan.)
Oxalic acid acts as a poison when applied to a wound in any part of the body; and although this substance undoubtedly acts on the brain through the medium of the blood, it is a remarkable fact that it cannot be detected in that fluid, even when injected into the femoral vein of an animal which died in thirty seconds (Christison). Leeches, it is recorded, have been poisoned by the blood drawn by them from persons suffering from oxalic acid poisoning. The blood does not appear [Pg 259] to undergo any physical change. Unlike the mineral acids, oxalic acid is still poisonous even when its corrosive and irritant properties have been destroyed by dilution.
Post-mortem Appearances.—The mucous membrane of the mouth, tongue, and throat is corrugated, white, and softened. The tongue is sometimes of a brownish colour, and sordes appear on the teeth. The stomach is in some cases pale, soft, and very brittle, and contains a dark, grumous, acid liquid; at other times it presents several semi-gelatinous spots, looking as if they had been boiled. Enlarged blood-vessels filled with dark-coloured blood are also seen ramifying over the internal surface of the organ. Perforation is of rare occurrence. The intestines generally escape with some slight inflammatory redness, unless the case is unusually prolonged. In some cases the stomach is quite healthy, no morbid appearance being found in any portion of the alimentary canal.

Fig. 29.—Photo-micrograph
of crystals of oxalic acid, × 50.
(R. J. M. Buchanan.)
Chemical Analysis.—From organic mixtures the acid may be separated by dialysis, and the tests applied, or it may be obtained in crystals by precipitating it from the boiled and filtered organic mixture with acetate of lead. The precipitate washed is then decomposed by sulphuretted hydrogen and filtered, the filtrate concentrated to drive off excess of sulphuretted hydrogen, and then set aside to crystallise, which, if the acid be present, it does in slender prisms. From the contents of the stomach the acid may be separated by partial drying over a water bath, extraction with hot alcohol acidulated with a little hydrochloric acid, filtering the alcoholic solution, evaporating to dryness, and dissolving the residue in water. Should, owing to the treatment adopted, oxalate of lime in white chalky masses be found in [Pg 260] the stomach, these should be washed and then boiled with pure carbonate of potash. A partial decomposition takes place, insoluble carbonate of lime and soluble oxalate of potash are present in the liquid, which, when filtered and neutralised with nitric acid, may be tested with the following reagents:
1. Nitrate of silver gives a white precipitate, soluble in cold nitric acid; the precipitate dried and heated on platinum foil is dissipated in a white vapour with slight detonation.
2. Calcium chloride or sulphate produces a white precipitate with oxalic acid; the test is more delicate if the acid be first neutralised with ammonia. The precipitate is immediately dissolved by hydrochloric or nitric acid, but not dissolved by oxalic, tartaric, acetic, or other vegetable acid. Lime-water should not be used as a test, as it gives precipitates with other acids; the sulphate largely diluted is not open to this objection.
3. Lead acetate gives a white precipitate soluble in nitric acid. On clothes, parchment, &c., the spot or spots must be well boiled, and the above tests applied to the solution. The stains may vary from a brownish-red to orange-red colour.
Fatal Dose.—Three drachms have caused death in one hour; sixty grains caused the death of a boy sixteen years of age, but recoveries have been known to take place after an ounce and an ounce and a half had been swallowed.
Fatal Period.—Death has resulted in ten minutes from a dose of one ounce. The shortest period has been three minutes. The time varies with individuals, even when the same quantity is taken. In the case of two girls who each swallowed an ounce of oxalic acid, one died in ten minutes, and the other in thirty minutes. Death usually takes place within from half an hour to an hour, although it has been delayed for five days.
Treatment.—Water should not be given, as it increases the solubility of the acid, and thus assists in the more extensive absorption and diffusion of the poison. The carbonates of potash and soda should be avoided, as the oxalates of these alkalies are themselves poisonous. The stomach tube should not be used. Lime is the best antidote, as the oxalate of lime is insoluble, and may be given in the form of common whiting; a pint of saccharated lime water may be given. Vomiting should be promoted. In the stage of collapse the case must be treated on general principles.
The binoxalate of potash or salt of sorrel, or, as it is more commonly known, salt of lemons, occurs as a constituent of many plants. The common sorrel—Rumex acetosa—contains it in large quantities.
Symptoms.—Those of poisoning by oxalic acid, on which its poisonous properties depend.
Post-mortem Appearances.—Inflammation of the stomach and intestines. Other appearances as in oxalic acid. [Pg 261]
Chemical Analysis.—See oxalic acid. The incinerated salt leaves a white residue of potassium carbonate; oxalic acid leaves no residue.
Fatal Period.—Eight minutes in the case of a lady recently confined, who took half an ounce of the salt by mistake for cream of tartar.
Fatal Dose.—Half an ounce.
Treatment.—The same as recommended for poisoning by oxalic acid.
Table showing Symptoms, Post-mortem
Appearances,
Fatal Dose, Period of Death, and
Treatment of Poisoning by
| Sulphuric Acid. | |
| Symptoms | Burning pain in the mouth, |
| throat, and gullet. Constant | |
| vomiting of brownish or blackish | |
| matter containing blood. | |
| The lips shrivelled, blistered, | |
| and excoriated; and the corners | |
| of the mouth show signs | |
| of the corrosive action of the | |
| poison. Collapse and death. | |
| Post-mortem Appearances | Presence of the signs of powerful |
| corrosion; perforation of the | |
| stomach, which is blackened | |
| and softened. | |
| Fatal Dose | One drachm. |
| Fatal Period | One hour. Average about ten hours. |
| Treatment | Magnesia, chalk, whiting, soap suds, |
| milk, and mucilaginous drinks. | |
| Hydrocyanic Acid. | |
| Symptoms | Giddiness, insensibility, difficult |
| respiration, dilated pupil, | |
| tetanic spasms, and convulsions. | |
| In acute cases, death by shock; | |
| in those more prolonged | |
| suffocation ends the scene. | |
| Post-mortem Appearances | Face pale and countenance composed; |
| congestion of the brain, and traces | |
| of inflammation in the stomach | |
| and bowels. Odour of prussic acid | |
| may be detected in most cases in the | |
| stomach and other parts of the body. | |
| Fatal Dose | About 45 minims of the |
| Pharmacopœia acid. | |
| Fatal Period | Two to five minutes. |
| Treatment | Chlorine in vapour and in water, and |
| the mixed oxides of iron. Cold | |
| affusion to the head and face, | |
| galvanism, artificial respiration, &c. | |
| Oxalic Acid. | |
| Symptoms | Burning pain in the mouth and |
| throat, vomiting of greenish-brown | |
| or grumous matter. Collapse sets | |
| in; skin cold and clammy; | |
| frequent pulse, and respiration | |
| hurried. Delirium and convulsions | |
| end in death. Effects depend on | |
| size of dose. Well diluted, it acts | |
| on brain, spine, and heart. | |
| Post-mortem Appearances | Lining membrane of mouth and |
| fauces white, shrivelled, and easily | |
| removed. Perforation of stomach | |
| rare. The post-mortem appearances | |
| depend on dilution of acid. | |
| Fatal Dose | One drachm in a boy; in another |
| case, half an ounce. | |
| Fatal Period | Less than ten minutes. |
| Treatment | Chalk and water. Promote vomiting. |
| Magnesia, lime water, and oil. | |
| Mucilaginous drinks. |
In the glacial form this acid acts as a corrosive, the dilute acid as an irritant. Cases have been recorded of poisoning by the glacial acid.
Symptoms.—The parts with which the acid has come in contact are softened and rendered yellowish-white in colour. The larynx is commonly affected by the acid, as it is very volatile.
Post-mortem Appearances are those of corrosive poisoning with inflammatory action in the upper air-passages.
Fatal Period is variable but rapid.
Fatal Dose.—One drachm caused death in a child, but recovery has taken place in an adult after taking six fluid ounces.
Chemical Analysis.—Separate the free acid from organic matter by distillation, if in combination it should be liberated by adding phosphoric acid. With ferric chloride and ammonia to neutralisation a red colour is produced, turned yellow by hydrochloric acid.
Treatment.—Magnesia should be given to neutralise the acid and vomiting produced. The laryngeal symptoms will require treating on general principles; tracheotomy may be necessary.
POTASH. SODA. AMMONIA
Poisoning by the use of the alkalies is very rare. For the sake of convenience, and as the symptoms produced by the caustic preparations of soda and potash, taken in large doses, do not greatly differ, one description will do for both:
Potash is found in commerce as (1) caustic potash, either solid or in solution; (2) carbonate and bicarbonate; (3) pearl-ash and soap-lees.
Soda is found as (1) caustic soda; (2) carbonate (washing soda) and bicarbonate; (3) soap-lees, carbonate of soda mixed with caustic alkali.
General Characters.—Like the inorganic acids, the alkalies destroy the animal tissues with which they come in contact. Their action is local, no specific remote effects being produced. They are seldom, if ever, used for the purpose of homicide; the deaths caused by them are in most cases the result of accident or suicide. When injected directly into the veins of animals, the toxic action of potash and soda [Pg 263] appears to differ, the former arresting the action of the heart in diastole, whereas the latter, according to Podocaepow and Guttman, does not, even in large doses, affect the heart or temperature—Guttman, moreover, asserting that soda has no influence upon the nerve centres, the peripheral nerves, or the muscles. It is difficult to understand how, with this asserted negative action, soda, like potash, causes death.
Symptoms.—During the act of swallowing, the patient complains of a caustic taste, accompanied with a sensation of burning in the mouth and throat, extending into the stomach. Vomiting may or may not be present; but in severe cases, when it does occur, the vomited matters may be mixed with blood. The surface of the body is cold, and bathed in a cold sweat. Purging is generally present, accompanied with intense pain and straining. The pulse is weak and quick, and the countenance anxious.
The post-mortem appearances are inflammation and softening of the mucous membrane of the mouth, gullet, and stomach, which may also be covered with chocolate-coloured or black spots. When life has been prolonged for some months the stomach may become contracted, the pyloric orifice scarcely admitting the passage of a fine probe.
Chemical Analysis.—The caustic alkalies are known from their carbonates by giving a brown precipitate with nitrate of silver; whereas their carbonates give a white, and also effervesce on the addition of an acid.
The following table will show the reaction of these alkalies with reagents:
To distinguish Caustic Potash from Caustic Soda
| Potash. | Soda. | |
|---|---|---|
| Bichloride of platinum. | A canary-coloured | No precipitate. |
| precipitate | ||
| in solutions | ||
| acidulated with | ||
| hydrochloric acid. | ||
| Strong solution of | Precipitate in granular | No precipitate. |
| tartaric acid. | white crystals. | |
| Colour given to flame. | Rose or lilac tint. | Yellow tint. |
| Neutralised with | Crystallises in long, | Crystallises in |
| nitric acid. | slender, fluted prisms. | rhombic plates. |
In Organic Mixtures.—If the mixture be strongly alkaline, filter and test as above.
Fatal Period.—From three hours to as many years.
Fatal Dose.—About half an ounce of the caustic alkali. The smallest fatal dose recorded of caustic potash is forty grains.
Treatment.—Water freely; drinks containing citric or acetic acid, vinegar, lemon juice, oil, linseed tea, and other demulcent drinks. The stomach tube should be avoided.
In vapour, in solution, or solid.
Symptoms.—The vapour may cause death by producing inflammation of the larynx and lungs. The symptoms to which it gives rise are a feeling of choking, and a suspension of the power of breathing. Intense heat and pain are felt in the throat, which may remain for some time. When ammonia is swallowed in solution, the symptoms produced are not unlike those the result of the action of soda or potash, only more intense. Dr. Patterson records the history of a case of a poor man who drank about an ounce of the liquid ammonia. When seen, his lips were livid, breathing stridulous, aspect anxious, extremities cold, pulse 100; inside of mouth, tongue, fauces, as far as visible, red, raw, and fiery-looking. He died suddenly, nineteen days after the accident, of laryngeal spasm. Albuminuria occurred in one case.
The post-mortem appearances are those found in most cases of poisoning by corrosives.
Chemical Analysis.—Ammonia can be separated from organic mixture by distillation. Putrefaction must not have taken place. The vapour of ammonia is easily set free and recognised by its pungent odour. The carbonate effervesces when an acid is added to it, and gives a white precipitate with salts of lime. Dense white fumes are given off in the presence of hydrochloric acid. Nessler‘s reagent gives a reddish-brown colour or precipitate.
Fatal Period.—Death has been known to occur in four minutes, but life may be prolonged for some time, the person dying of some thoracic trouble.
Fatal Dose.—A teaspoonful of the strong solution.
Treatment.—Vinegar and water, lime-juice and oil, and leeches to the throat if the inflammatory symptoms be severe. The rest of the treatment will depend upon the symptoms present. Tracheotomy may be necessary.
Chloride of antimony (butter of antimony) is a corrosive liquid. The colour varies from a light yellow to a dark red. Though a powerful poison, it is seldom taken for that purpose. It has been taken by mistake for ginger beer. On the addition of water, the white oxychloride is precipitated.
Symptoms.—The symptoms produced by swallowing this substance are those of corrosive poisoning. The mouth and throat are excoriated, the skin cold and clammy, and the pulse feeble and quick. Severe pain is felt in the stomach, and vomiting is incessant.
Post-mortem Appearances.—Those found after corrosive poisoning.
Chemical Analysis.—When poured into water, the chloride is precipitated; the precipitate, soluble in tartaric acid, becomes [Pg 265] orange-red on the addition of hydrogen sulphide. The supernatant liquid will give a white precipitate with nitrate of silver, showing the presence of hydrochloric acid. The salts of bismuth are precipitated by the addition of water, but the precipitate is, unlike the antimonial, insoluble in tartaric acid, and is blackened by hydrogen sulphide.
From organic liquids, the antimony may be obtained by boiling them with tartaric acid, filtering, and then applying the tests for antimony.
Treatment.—Milk, magnesia, and infusions containing tannin.
This substance is a powerful corrosive. It is employed as a disinfectant, and is sold to the public under the name of “Sir W. Burnett‘s Fluid.” This preparation, which is a strong solution of the chloride of zinc, has caused death by being mistaken for “fluid magnesia,” for “pale ale,” and in one case, on board one of the American steamers, for “mineral water.” Chloride of zinc is also used in the treatment of cancer and other tumours as an external application.
Symptoms.—The symptoms come on immediately after the poison is swallowed. Chloride of zinc acts as a powerful corrosive, accompanied with all the symptoms which have been before described when speaking under the head of corrosive poisons. The nervous system is also powerfully affected.
Post-mortem Appearances.—Those of corrosive poisoning in its most violent form. The mouth, throat, stomach, and intestines are often found hardened, white, opaque, and corrugated.
Chemical Analysis.—Ammonium sulphide gives a white precipitate, which is insoluble in caustic alkalies. Hydrogen sulphide gives a white precipitate in neutral solutions, but no precipitate when the free mineral acids are present. Potassium ferrocyanide gives a white precipitate. Test for chlorine with nitrate of silver.
Treatment.—White of eggs, emetics, followed by demulcent drinks.
This metal requires but little notice; but the two chlorides—protochloride and the perchloride—form a mixture used in the arts, and known as Dyer‘s Mixture. They act as irritant poisons, but are seldom used as such.
The only preparation of silver requiring notice is the nitrate—lunar caustic, or lapis infernalis. It acts as a powerful corrosive. If administered for some time in small doses it is deposited in the skin, which acquires a permanent dark colour. It does not appear to be eliminated by the urine, and has been discovered in the liver five months after its administration was discontinued. [Pg 266]
The symptoms come on immediately, the vomited matters becoming blackened on exposure to light. The dark spots on the skin will also help to point to the nature of the poison. A dose of salt and water may be given by way of treatment.
GLASS, ENAMEL, AND NEEDLES
None of the above can be considered as poisons; but should they be taken, they give rise in most cases to irritation of the stomach and bowels. Pins and needles have been swallowed without doing much harm. Mixing ground-glass in food is a favourite mode of killing adopted by the West Indian negroes.
Poisoning by this substance is more common in France than in England. In England, the deaths due to this poison are more frequently the result of accident, from the incautious use of phosphorus paste for the destruction of vermin. These pastes generally contain from 3 to 4 per cent. of phosphorus. Children have also been poisoned by sucking the heads of lucifer matches. In one case, that of a child, death followed from sucking about forty matches. It has most frequently been employed as a means of suicide, but seldom for the purpose of homicide. One case, however, occurred at the Bodmin Assizes in 1857. Kopf relates a case of a young woman, aged twenty-four, who died on the fourth day after swallowing the heads of six packets of lucifers (Allg. Wien. Med. Ztg., No. 47, 1819; Schmidt, vol. cv. p. 296). The size of the packets is not stated. In this case the bowels were confined, and the post-mortem revealed only the redness of inflammation in the stomach and bowels. Death has followed inunction of phosphorus paste.
General Characters.—There are two kinds—ordinary waxy, crystalline phosphorus, and a peculiar form known as red allotropic or amorphous phosphorus, prepared by heating waxy phosphorus to a temperature of 240° C., in an atmosphere free from oxygen. The ordinary yellow phosphorus is poisonous, the red or amorphous non-poisonous. As found in the shops, phosphorus is preserved in water in the form of translucent white or slightly yellow-coloured cylinders. It is sparingly soluble in oil, alcohol, and other hydrocarbons, but greatly so in bisulphide of carbon. White vapours are given off when it is exposed to the air, these consisting of phosphorus and phosphoric acids.
Symptoms.—Phosphorus acts as an irritant poison, but some days may elapse after the poison is taken before the injurious effects become apparent. The symptoms occur in three stages.
First stage: The patient complains of a garlic-like taste in the mouth, peculiar to poisoning by this substance. This is followed by a burning sensation in the throat, accompanied with severe pain in the stomach, and intense thirst. The belly becomes swollen, and there is vomiting, in some cases, of blood from the stomach, which may continue till death. The vomited matters are of a dark green or black colour, [Pg 268] with an odour of garlic, and sometimes appearing phosphorescent in the dark. This condition may also be observed in the motions passed. There is intense thirst. The pulse is feeble, the countenance anxious, and the surface of the body bathed in a cold sweat. In males, priapism is not infrequent. The nervous and muscular debility is intense, and the patient may die in a state of collapse or during a fit of convulsions.
Second stage: This is a stage of intermission of the symptoms which may last for three days or more, the patient seems as if going to recover, and only suffers from general malaise. A case is recorded where the intermission lasted nine weeks. In cases proceeding to a fatal termination the intermission is followed by the third stage.
Third stage: Jaundice is the most notable symptom and rapidly increases; the liver becomes much enlarged and the abdomen distended; epigastric pain is severe and there is vomiting of grumous black material consisting of altered blood; purging may be present and the motions contain blood. There is a marked tendency for hæmorrhages to occur from the mucous membranes and subcutaneously, producing purpuric spots. The urine is diminished, high coloured, contains bile pigments, albumen, blood, and casts. There are great prostration, a quick weak pulse, sleeplessness, coldness of the surface, gradually increasing weakness, apathy, convulsions, and coma, followed by death about the fifth or sixth day.
The liver may diminish in size before death. It is rare for recovery to take place after enlargement of the liver and jaundice have supervened. It is by no means always easy to diagnose acute yellow atrophy of the liver or malignant jaundice from phosphorus poisoning. In phosphorus poisoning, the early symptoms, those of acute gastritis, are more severe, are developed more rapidly, and run their course more quickly than in acute atrophy, and there is a marked interval between these and the appearance of the jaundice; in acute yellow atrophy this interval is wanting, and from the beginning, on the contrary, there are gradual malaise, slight gastric catarrh, and jaundice. The jaundice and suffering, together with the increased action of the heart in phosphorus poisoning, are wanting in malignant jaundice, but the cerebral symptoms are more marked in the latter than in the former. Acute yellow atrophy most frequently occurs in women, especially during pregnancy. In acute atrophy leucin and tyrosin are present in the urine; in phosphorus poisoning they may occur, but generally in the urine voided just before death.
Chronic poisoning, accompanied with all the symptoms just mentioned, may result from the action of the vapour on those engaged in the manufacture of phosphorus or of lucifer matches. In persons thus employed, necrosis of the jaws and caries of the teeth are not of infrequent occurrence. The lower jaw is more commonly affected. Mr. Lyons states that this form of necrosis cannot attack persons who have perfectly sound teeth, but only those whose teeth are carious (St. Bartholomew‘s Hospital Report, vol. xii.). [Pg 269]
Post-mortem Appearances.—Those of acute irritant poisoning, including extensive destruction of the coats of the stomach, by softening, ulceration, and perforation, terminating in gangrene. The stomach may contain a quantity of white vapour, having a strong smell of garlic. This white vapour has been noticed to pass from the vagina and anus of those poisoned by phosphorus. The blood appears to be thoroughly disorganised; the blood-cells are colourless and transparent, their colouring matter being dissolved in the uncoagulated liquor sanguinis; hæmorrhages may be present beneath the serous membranes and in the pleural and pericardial cavities, and thromboses are frequently present, due to a tendency for the blood-cells to agglutinate. In a case recorded in the British Medical Journal, 1873, fatty degeneration of the liver and kidneys was found a week after the poison was taken. In phosphorus poisoning, the liver is enlarged, of a dull appearance, doughy, uniformly yellow, with the acini well marked; in acute atrophy, the liver is diminished in size, greasy on the surface, leathery, of a dirty yellow colour, with traces only of the obliterated acini. In the former, also, the hepatic cells are either filled with oil globules or entirely replaced by them; in the latter, the cells are filled with a fine granular detritus, and their structure replaced by newly-formed connective tissue. Putrefaction rapidly supervenes on death. Hæmorrhages may be found on the surface of the brain and spinal cord, and the grey matter of the cortex and basal ganglia rose-pink in colour. Fatty changes have been found in the walls of the capillaries and the large cortical cells.
Chemical Analysis.—The smell of phosphorus is characteristic, as is also its luminosity when exposed in the dark. The following process, suggested by Mitscherlich, may be adopted for its detection:
To render the suspected matter quite fluid water is added, previously acidulated with sulphuric acid, in order to neutralise any ammonia present. The liquid is then transferred to a glass retort, fitted with a long condensing tube passing into a receiver containing solution of nitrate of silver. Distillation is conducted in the dark, when the minutest trace of phosphorus may be detected by the luminous appearance of the vapour during condensation. Other modifications of this process have been suggested, in order to increase the space occupied by the phosphorescence.
By the above process, one part of phosphorus may be detected in 100,000 parts of substance. Another method for the detection of this poison in very minute quantities is that proposed by Dussart (Compt. Rend., xliii. 1126), and modified by Blondlot (Compt. Rend., lii. 1197). The test is based on the fact that when phosphorus is exposed to the action of nascent hydrogen in a Marsh‘s apparatus, it burns with an emerald-green flame. In order to avoid the yellow colouring of the flame produced by the sodium in glass, Blondlot recommends the use of a platinum jet. As the green colour is more or less interfered with by the presence of organic matters, he passes the gas through a solution of nitrate of silver; the resulting precipitate [Pg 270] is then placed in another hydrogen apparatus, as just mentioned, and the colour of the flame of the issuing gas noted. Phosphorus may become decomposed in the body; and as phosphoric acid is taken in most articles of food, the only satisfactory evidence of phosphorus having been taken is to produce it in its free state, or at least to exhibit its luminosity. The detection of the colouring matter of lucifer matches in the stomach or vomited matters will point to the probable nature of the poison, and whence it was derived.
Scherer‘s Test is based on the reducing action of phosphorus on nitrate of silver, which it blackens. The suspected material should be placed in a flask or in a Dowzard‘s apparatus for Gutzeit‘s test for arsenic, lead acetate is added to the material to fix the H₂S, and some lead acetate solution placed in each cell. A little ether is added to the mixture, and the flask or top of the apparatus capped with paper moistened with nitrate of silver, and set aside for some hours in a dark place. If phosphorus be present the paper will be blackened from deposition of metallic silver.
Fatal Period.—From half an hour to twenty days or more.
Fatal Dose.—One grain and a half. The smallest fatal dose recorded for an adult is one-eighth of a grain. An infant five weeks old died from sucking a single match head, which probably contained one-fiftieth of a grain of phosphorus. Recovery has taken place after four and six grains have been taken.
Treatment.—The stomach pump or syphon tube should be used as soon as possible, and the stomach well washed out with warm water containing a drachm of old oil of turpentine to the pint. If the turpentine be not readily obtained, “sanitas” should be used with the water, or a 1 per cent. solution of permanganate of potash. After washing the stomach, the old oil of turpentine, or the French oil of turpentine, or “sanitas” may be administered in half to one drachm doses in mucilage and water every fifteen minutes for several doses, and afterwards three or four times daily. The 1 per cent. solution of potassium permanganate may be administered in copious drinks.
According to some observers, turpentine is said to be of no value; but this failure in the use of turpentine has been shown to be due to the employment of different varieties of oil. The crude acid French oil, of the three kinds met with in commerce, appears to be the only one that acts as described below. With turpentine, phosphorus forms a spermaceti-like mass consisting of turpentine phosphorus acid. It has an acid reaction, and is converted, on exposure to the air, into a resinous substance smelling like pine-resin. With earths and metallic oxides it forms insoluble salts. The acid is not poisonous; doses of 0.03 to 0.3 gram may be given to dogs and rabbits without any other effect than that of lowering of the body temperature. To the formation of this compound, the antidotal properties of turpentine in phosphorus poisoning are attributed (Kohler a. Schempf Dingl., pol. Jcxcix.). Turpentine is said by some to be valueless if not given within twelve hours. Emetics of sulphate of copper may be administered, but the salt is liable to cause severe gastro-enteritis. Further [Pg 271] treatment may consist of mucilaginous drinks containing magnesia and opium to relieve pain. Oils or fats should not be given because of their solvent action upon phosphorus.
Synopsis of the Effects due to
Poisoning by Phosphorus
1. Which variety of phosphorus is poisonous?—The ordinary yellow phosphorus usually kept in water. The allotropic form is inert.
2. What quantity is sufficient to kill an adult?—One grain and a half.
3. Symptoms as regards—
(1) Alimentary Canal.—Pain in the stomach and belly, eructation of gas smelling like garlic, vomiting, and sometimes purging, with other signs of irritation.
(2) Circulatory System.—Tendency to hæmorrhage from the mouth, stomach, lungs, bladder, &c. Petechiæ and ecchymoses may occur on all parts of the body. If the case be prolonged, anæmia may be present. Pulse small, weak, and scarcely perceptible.
(3) Nervous System.—Cramps, creeping sensations in the limbs, delirium, convulsions, paralysis, and extreme nervous prostration.
(4) Period of Invasion of the Symptoms.—Obscure and insidious; some hours or even days may elapse before the appearance of the symptoms.
(5) Period of Fatal Termination.—In some cases as short as four hours.
4. Post-mortem Appearances—
(1) Alimentary Canal.—Signs of irritation and inflammation in the stomach and intestines. Gangrene and perforation have been noticed. Strong smell of garlic when the abdomen is laid open. Appearances not unlike scurvy may be found.
(2) Cellular Tissue.—Ecchymoses may be present in the cellular tissue of the abdomen, chest, and other parts of the body.
(3) Muscular Tissue.—Fatty degeneration in the heart and other organs of the body has been noticed in several cases.
(4) Liver.—Fatty degeneration of the gland.
(5) Blood entirely disorganised, the cells transparent, and their contents dissolved in the uncoagulated liquor sanguinis. The colour, cherry-red.
5. Name special affection produced by phosphorus in lucifer match makers—Necrosis of the jaws, usually of the lower jaw. The disease begins in a decayed tooth.
6. Name a natural disease which phosphorous poisoning has been supposed to resemble—Acute yellow atrophy of the liver.
Iodine is seldom used as a poison, owing to the difficulty experienced in disguising its colour. In the form of a strong solution it has been, however, employed for throwing on the person with intent to cause grievous bodily harm, as in this form it is corrosive, and destroys the part which it touches.
General Characters.—Iodine is a dark grey solid, with a bright metallic lustre. It melts at 107° F., boils at 175° F., and gives off at the ordinary temperature a faint odour not unlike chlorine. But slightly soluble in pure water, it is, however, readily dissolved when a soluble iodide is added to the water. [Pg 272]
Symptoms.—Those produced by irritant poisons generally; the severity of the symptoms being increased by the strength of the solution, iodine possessing corrosive as well as irritant properties. The vomited matter will be stained with the iodine, and starchy material turned blue or black.
Post-mortem Appearances.—Those the result of acute irritant poisoning.
Fatal Period.—Two days.
Fatal Dose.—One fluid drachm of the tincture has proved fatal; recovery has taken place after taking one fluid ounce of the tincture.
Treatment.—The stomach should be emptied by the aid of the stomach pump, and then diluent drinks—arrowroot and barley water—may be given.
Chemical Analysis.—Add bisulphide of carbon to the suspected mixture, and shake them together. The sulphide will dissolve out the iodine, which may be obtained on evaporation and sublimed. The characteristic reaction of iodine, the development of a blue colour on the addition of a small quantity of starch, will be conclusive evidence of its presence. If chloroform be added to iodine in aqueous solution and shaken up, the chloroform is coloured crimson by the iodine, and falls to the bottom as the mixture is allowed to settle.
This salt is largely used in medicine; and though poisonous effects may be produced, due probably to some constitutional idiosyncrasy, it has seldom been used as a poison. It must, however, be placed among noxious irritant substances.
General Characters.—Iodide of potassium—hydriodate of potash—occurs in cubical crystals of a white or faint yellow colour, very slightly deliquescent when pure, and with a feeble odour of iodine.
Symptoms.—Iodide of potassium acts as an irritant in large doses, producing also many of the symptoms which attend a violent catarrh, with profuse discharge from the nose, lachrymation, and swelling of the eyelids, also pustular eruptions like acne on the face and body generally. Small doses—three to five grains—have produced in some persons most unpleasant and even alarming symptoms. In chronic poisoning, certain glands, the mammary and testicles, are said to waste away. Salivation is not infrequently present. I have seen the administration of the salt produce a severe bullous and hæmorrhagic eruption, simulating hæmorrhagic smallpox, with sloughing. (See also the account in British Medical Journal, 1878, of a case of purpura in a child five months old, after a dose of two and a half grains of the salt.)
Treatment.—The use of emetics and the stomach pump, starch, &c.
Chemical Analysis.—In solution, iodide of potash gives the following characteristic reactions:
| 1. With a salt of lead | Bright yellow precipitate. |
| 2. With corrosive sublimate | Bright scarlet precipitate. |
| 3. With strong nitric acid and starch | A blue colour. |
[Pg 273] In organic mixtures the mode of detecting it is more complicated.
Sulphuretted hydrogen should be first passed through the mixture in order to convert any free iodine into hydriodic acid. The excess of the gas is then driven off by the application of heat, and potash added, the resulting liquor filtered, and the filtrate evaporated to dryness. To get rid of any organic matter, the residue left after evaporation is charred at a low red heat, reduced to powder, and dissolved in water. This solution is then concentrated, and strong nitric acid and solution of starch added, when, if iodine be present, the blue colour will be developed.
Arsenic is found as metallic arsenic, as arsenious acid, in the form of two sulphides—realgar and orpiment, and as a constituent of several ores—iron, copper, &c.
Metallic arsenic is of a steel-grey colour, brittle, and sublimes at a temperature a little below 400° F., without, however, previously fusing. The vapour of the metal has a peculiar garlic-like odour, which is not possessed by any of its compounds.
Arsenious Acid
Arsenious anhydride—white arsenic—the most important of all the compounds of arsenic, is colourless, odourless, and almost devoid of taste. As found in commerce, it occurs under two forms—as a white powder, and as a solid cake, which is at first nearly transparent, but soon becomes opaque, and then resembles white enamel. At a temperature of about 380° F. it sublimes, but is again deposited on cool surfaces in the form of octahedral crystals. It is but slightly soluble in cold water, only about half a grain to a grain being taken up by an ounce of water. Stirred in boiling water, and then allowed to cool, from a grain to a grain and a quarter is dissolved in the same quantity of water; but when it is boiled for an hour, about twelve grains are dissolved in the ounce of water. This solubility is, however, diminished by the presence of any organic matter in the liquid. It is therefore less soluble in infusions of tea or coffee than in pure water. A teaspoonful of powdered arsenic is said to weigh 150 grains, and a pinch 17 grains.
Arsenious acid is used in the arts in the manufacture of certain green colours, in dyeing, and in calico printing. A weak solution is employed in medicine in the treatment of certain diseases of the skin, in ague, and in other diseases.
It has been proposed to use arsenious acid, on account of its caustic properties, as an application for cancerous tumours. The employment of this substance for this purpose is by no means new; but its use has been revived from time to time by the charlatan. In the year 1844, a man was tried at the Chester Winter Sessions (R. v. Port) for the murder of a woman whom he pretended to cure of a cancer by the use of an arsenical plaster. In another case, recorded by M. Flandin, where death occurred, the quack declared that he had not applied more than four or five grains to the woman‘s breast. The powder used for this purpose is generally composed of arsenious acid, realgar, [Pg 275] and oxide of iron. The above cases, to which many more might be added, attest to the danger which attends the application of arsenic to the surface of the body; it should, therefore, never be used, especially as a more safe and potent caustic for this purpose is found in the chloride of zinc. Some years ago, in London, several cases of severe arsenical poisoning were due to the presence of arsenic in some cheap violet powder. In one case the navel and scrotum of a baby were fearfully excoriated, due to the use of this powder.
Farmers employ arsenious acid (white arsenic) for destroying vermin: for steeping corn in order to destroy any spores of fungi; and it also forms an ingredient in the wash for sheep. Injurious effects have followed the accidental use of the corn thus treated, and those employed in washing the sheep have suffered more or less severely.
By an Act of Parliament (14 Vict. cap. xiii. sec. 3), it is ordered that if sold in small quantities, it must be mixed with the sixteenth part of its weight of soot, or the thirty-second part of its weight of indigo, ten pounds being the smallest quantity allowed to be sold unmixed.
The presence of this admixture must be remembered, as a medical man may be led into an error when the vomited matters are coloured blue, black, or green, from the mixture of bile with the indigo. Arsenic is not, as a rule, a corrosive poison. One case is, however, on record where it acted as a corrosive, but the purity of the arsenic in that case has been questioned. Its action is that of an irritant, causing inflammation in the stomach and bowels of those who have taken it; and it appears that fatal effects are produced whether the poison be swallowed or introduced into the system in any other way—e.g. by injection into the rectum or vagina, or applied to the surface of the body.
Some observers hold that arsenic cannot be considered in the light of an accumulative poison, others that it is so to a certain extent, and that its elimination is not so rapid as was previously thought. Given in medicinal doses, it is eliminated in from fifteen to twenty days. Hence, in cases which have survived the immediate action of the drug, no arsenic may be found in the body fifteen days after its fatal administration. This is a fact of considerable importance. In the case of Pierre Emile L‘Angelier, for whose murder Madeline Smith was tried, Dr. Penny found 88 grains in the stomach, although the deceased survived eight or ten hours after the probable period of taking the poison, and vomited repeatedly during that time. At the above trial, the question was suddenly raised, that if such a large quantity was found after death in the stomach, it was scarcely possible to infer the administration of a much larger quantity; and thus, that the quantity must have been larger than another party could have secretly administered, or naturally would attempt to administer. Drs. Mackinlay and Wylie, of Paisley, obtained 60 grains, and Sir R. Christison 30 grains more, from the stomach of a man poisoned by arsenic administered in whisky-punch sweetened, the arsenic being kept in suspension by constant stirring. [Pg 276]
Symptoms of Arsenical Poisoning
Acute.—The rapidity and virulence of the symptoms are more or less modified by the form (e.g. solution) and the dose taken. From half an hour to an hour is the usual time which elapses before the symptoms of poisoning present themselves. In one case, in which the poison was in solution, the symptoms came on immediately after it was swallowed; in another, after the lapse of ten hours. The patient first complains of a feeling of faintness and depression, followed by intense burning pain in the stomach, increased by the slightest pressure. Nausea and vomiting, the latter increased by the act of swallowing, now occur. The vomited matters may be dark brown, black, or bilious; or they may be greenish from the indigo mixed with the arsenic coming in contact with the yellow colouring matter of the bile. Blood may also be vomited. Purging, accompanied with straining at stool, and cramps in the calves of the legs may occur—the purging, like the vomiting, being incessant, and affording no relief to the sufferer; the stools may contain blood, or resemble those of cholera. The thirst is intense, and there may be a feeling of throat irritation, the pulse feeble and irregular, and the skin cold and clammy. The urine may or may not be suppressed. As a rule, the symptoms in this form of poisoning are continuous; but cases occur in which there are distinct remissions, and even intermissions. Coma, paralysis, or tetanic convulsions may supervene before death closes the scene.
Certain anomalies may occur.—The pain may be absent or but slight. Vomiting and purging do not occur in all cases, nor is thirst, a most common and persistent symptom, always present. In some cases the symptoms resemble those which accompany an attack of cholera. In others, signs of collapse first make their appearance, from which the patient may rally, or he may die outright. These variations in the symptoms do not appear to be due to the form or quantity of the poison taken. It should also be remembered that arsenic may produce symptoms closely resembling those the result of narcotic poisoning.
Chronic.—In whatever way the poison be exhibited in small and repeated doses, there follows a peculiar and characteristic train of symptoms, associated with (a) the general nutrition of the body, (b) the facial appearance, (c) irritative disturbance of the alimentary canal, (d) skin eruptions, and (e) implication of the nervous system.
(a) The nutrition of the body is altered, there is gradual loss of flesh with ragged growth of the finger-nails and falling out of the hair. There may be œdema and jaundice in some cases.
(b) The face presents a peculiar appearance, the eyes are inflamed and watery, the conjunctivæ reddened and congested, there is excessive secretion from the nose resembling coryza.
(c) The disturbance of the digestive organs is revealed by the dryness of the mouth and occasional excoriation of the tongue, which may be reddened or covered with white fur and silvery in appearance; [Pg 277] salivation may be present instead of dryness of the mouth; there may also be irritation of the throat; symptoms of gastro-enteritis, e.g. nausea and vomiting, anorexia, diarrhœa, or alternating diarrhœa and constipation.
(d) The skin eruptions are of various kinds, and comprise eczema, herpes, urticaria, erythema, keratosis, marked pigmentation and exfoliation.
(e) The nervous symptoms are those of peripheral neuritis, numbness, formication, hyperæsthesia, and tenderness, especially of the soles of the feet, the latter presenting appearances of erythro-melalgia; there is some amount of paresis, in some cases amounting to absolute paralysis of the limbs affected. The hands may be anæsthetic, while the feet are hyperæsthetic and hyperalgesic, and the perspiration much increased. Mental symptoms are not common, but there may be hebetude, or delusions.
In the Maybrick case, tried at the Liverpool Assizes in 1889, the following symptoms arose from repeated administration of arsenic during a period of probably about fourteen days. On April 27 Mr. Maybrick was seized with vomiting after taking tea. On the next day the vomiting continued, with foulness of the tongue, and he complained of stiffness in the lower limbs. On May 1 he complained of feeling unwell after taking luncheon, and he was sick on the following three days, and complained of a tickling sensation in the throat, with retching. On May 7 he was still suffering from vomiting, diarrhœa had commenced, and the throat was very dry and inflamed. On May 8 the diarrhœa was accompanied by tenesmus. On May 9 the tenesmus was distressing, and he died on May 11.
Dr. Prosper de Pietra Santa describes a disease to which workers in manufactories of paper coloured with Schweinfurt-green are liable, characterised by the appearance of vesicles, pustules, plaques muqueuses, and ulcerations on the exposed parts of the body, fingers, toes, and scrotum. Arsenical poisoning has been mistaken for nettle-rash, scarlet fever, and Addison‘s disease. In cases of slow poisoning the symptoms resemble very much those of gastritis and ulcer of the stomach, and death due to the action of arsenic has been referred to “spontaneous inflammation of the bowels.”
It must be remembered that in some cases of acute arsenical poisoning, when the acute symptoms have passed away, the nervous system exhibits its effects at a later period; in one case paresis came on on the fifth day, in another at the end of a week, and in a case recorded by Seeligmüller four weeks elapsed before the onset of nervous symptoms.
Post-mortem Appearances.—The appearances found after death depend upon the quantity of the dose and the length of time which supervenes between the taking of the poison and death. Inflammation of the stomach is a marked effect of the action of this substance on the system; and this condition is in most cases present whether the poison be swallowed, sprinkled on an ulcerated surface, or rubbed into the skin. The inflammatory redness, which may assume the appearance of crimson velvet, may be found in cases where death has taken [Pg 278] place in two hours. It is sometimes found spreading over the entire surface of the stomach; at others, at the cardiac end only. The red colour is increased on exposing the stomach to the air. When the poison has been swallowed, the stomach may be found covered with white patches of arsenic, embedded in dark-coloured thick mucus, mixed with blood. Dr. Paterson thus describes the condition of a stomach he examined: Its lining membrane was generally very red and injected; but in addition there were very numerous stellated patches of vivid red, leading to a darker tint; in the centre of some of them was noticed a minute clot of blood; in others, an exceedingly rough particle of a crystalline substance, which was afterwards found to be arsenious acid. Perforation of the stomach is extremely rare, if it has ever occurred, but ulceration of the same organ has been observed in a person who died from the effects of arsenic in five hours (Christison, on Poisons, p. 340). In opposition to all the statements just made it has been shown that arsenic may prove fatal without leaving any sign of inflammatory action (R. v. M‘Cracken; R. v. Newton).
The mouth, pharynx, and gullet are generally found free from any inflammatory action. The small intestines may or may not be affected: in most cases the duodenum alone shows any signs of irritation. The rectum is that part of the large intestine most prone to inflammation. I have seen marked ulceration of the colon after death from inhalation of arseniuretted hydrogen. The other internal organs—the liver, spleen, and kidneys—do not appear to be appreciably affected by arsenic.
Due probably to the antiseptic properties of arsenic, the stomach and intestines retain for a long period after death the appearances of irritant poisoning. In two cases, this was so well marked as to be visible—in the one case, twelve months, and in the other, nineteen months after interment. In suspected cases portions of the liver should always be preserved and examined for arsenic.
The Period after Death when
Arsenic may be Detected
Arsenic is an indestructible poison, and may be found in the body after many years. In one case it was detected after the lapse of fourteen years. Arsenic has the power, to a certain extent, of arresting putrefactive changes; the stomach may, therefore, be found well preserved, and with the signs of inflammatory action present after the lapse of many months, and after putrefaction has far advanced in other parts of the body. When a person is suspected of having been poisoned with arsenic, and nothing but the skeleton is left for investigation, the arsenic should be looked for specially in the bones of the pelvis and the neighbouring vertebræ (Watt‘s Dictionary of Chemistry, Sup.).
In reference to the preservative action of arsenic upon the tissues of those poisoned by it, the appearances of the bodies of the victims of Flannagan and Higgins, recorded by Whitford (B. M. J., 1884, vol. i. p. 504), are interesting. Arsenical poisoning having been established in one of three victims, the bodies of two others, Mary [Pg 279] Higgins, aged ten years, and John Flannagan, aged twenty-four years, were exhumed and examined. The abdominal viscera of Mary Higgins yielded one grain of arsenious acid, and although the body had been interred for about thirteen and a half months, it was well preserved. A remarkable state of preservation obtained in the body of John Flannagan, who had been interred for thirty-seven and a half months; the face and body generally could be easily identified. Three and a half grains of arsenious acid were found in the abdominal viscera. In these cases a peculiar appearance was found in the stomach and intestines, consisting of a golden-yellow pigment or coating of the mucous membrane of the parts. It was thought by some observers to be composed of arsenic sulphide, but Campbell-Brown, and Davies of Liverpool, as a result of their analysis of it, found that it did not contain any appreciable amount of arsenic, but consisted mainly of bile pigment.
In trials for arsenical poisoning, where an exhumation has been made, the question may arise whether the arsenic found in the body has been carried into it from the earth surrounding the coffin.
In reply, the following points must be kept in mind:
1. Arsenic may occur in certain calcareous and ochrey soils.
2. In these soils no arsenical compound soluble in water has been found.
3. The arsenic of these soils is dissolved out by hydrochloric acid, proving their previous insolubility.
4. The arsenic is, therefore, probably in the form of an arsenite or arseniate of iron, lime, &c.
5. Careful experiments have rendered it evident that even “under the most favourable circumstances the dead human body does not acquire an impregnation of arsenic from contact with arsenical earth” (Taylor).
6. It has been suggested that the arsenical compound in the soil may be rendered soluble by the ammonia formed during putrefaction.
This last suggestion is negatived by the following facts:
1. The production of ammonia ceases before the body arrives at that stage of decomposition when it is at all likely to be exposed to the action of the soil of the cemetery.
2. The production of hydrosulphuret of ammonia during decomposition would tend to the production of sulphuret of arsenic forming yellow patches in the substance of the organs, thus rather fixing the arsenic on particular parts than allowing it to percolate through the tissues of the body from external application.
Analysis of the Suspected Earth.—About two pounds of the earth should be boiled for some time in water; supernatant liquid should then be poured off from the insoluble residue, and filtered. The filtered liquid, after concentration, may then be examined by the tests about to be described. If no arsenic be found, the earth may now be boiled with dilute hydrochloric acid, filtered, concentrated, and then tested as before. The first process shows that no compound of arsenic soluble in water is present; the second shows that the arsenic is in a state of combination, and therefore not likely to impregnate the body. [Pg 280]
The Detection of Arsenic
General Directions.—In cases of suspected poisoning by arsenic or antimony, the contents of the stomach should be mixed with distilled water acidulated with hydrochloric acid and filtered, and the filtrate placed in a stoppered bottle lettered or numbered “A” or “1.” The liver should be cut into pieces, some of which should be bruised in a mortar with distilled water acidulated as above mentioned, pressed and filtered, and the filtrate placed in a bottle marked “B” or “2.”
The kidneys and portions of the other solid organs may also be treated as above. Each solution so obtained may be then tested by the processes about to be described. By these means the amount of poison in each organ may be estimated.
Before subjecting the organic mixture to Marsh‘s or Reinsch‘s processes, Brande and Taylor strongly recommend a modified course of procedure.
The contents of the stomach, vomited matters, &c., and the solid organs, finely divided, must each be separated and thoroughly dried in a water bath, then mixed with an excess of strong hydrochloric acid in a flask, and slowly distilled by means of a sand bath, the distillate carried into a receiver containing a little pure distilled water, and the process continued nearly to dryness.
If arsenic be present, the distillate contains the arsenic as chloride, and can be at once subjected with great facility to the usual tests for the presence of that metal. This mode of proceeding both facilitates and expedites the ordinary methods of testing, as it separates the arsenic present from the complex organic mixtures with which it is associated, and presents it in a comparatively pure form for identification. The process also admits of the residue left in the retort being examined for lead and the other metallic poisons.
Before the following processes are applied, some of the sediment from the contents of the stomach, or the vomited matters, may be collected and well washed. If this is boiled in distilled water and filtered, the following tests, known as “the liquid tests for arsenic,” may be applied to the filtrate:
1. Ammonia Nitrate of Silver, prepared by adding a weak solution of ammonia to a strong solution of nitrate of silver, gives with arsenic a yellow precipitate of arsenite of silver soluble in nitric, citric, acetic, and tartaric acids, and ammonia.
2. Ammonia-Sulphate of Copper, prepared by adding ammonia to a dilute solution of sulphate of copper, gives with arsenic a green precipitate of arsenite of copper. This precipitate is soluble in the mineral and vegetable acids and ammonia, but is not affected by soda or potash. The precipitate, dried and heated in a reduction tube, yields octahedral crystals of arsenious acid.
3. Sulphuretted Hydrogen.—The suspected liquid should be first slightly acidulated with pure hydrochloric acid before the sulphuretted hydrogen gas is passed into it, when, if arsenic be present, a yellow precipitate is formed, known to be such by the following tests: [Pg 281]
(1) Insoluble in water, ether, alcohol, the vegetable acids, and dilute hydrochloric acid, but decomposed by strong nitric and nitro-hydrochloric acids.
(2) Dissolved, if no organic matter present, forming a colourless solution, when potash, soda, or ammonia is added.
(3) The yellow precipitate dried and heated with soda and cyanide of potassium yields a sublimate of metallic arsenic.
N.B.—None of the above tests should be applied in the presence of organic matter. The soluble salts of cadmium and per-salts of tin give yellow-coloured precipitates with sulphuretted hydrogen.
(4) If stannous chloride dissolved in strong hydrochloric acid be added to a solution of arsenic in hydrochloric acid, metallic arsenic is thrown down as a precipitate. This is a fairly delicate test.
The following Table
gives the differences between the
Yellow Precipitates formed with
Sulphuretted Hydrogen
and Arsenic, Cadmium, and Per-Salts of Tin:
| Arsenic. | Cadmium. | Per-Salts of Tin. | |
|---|---|---|---|
| Colour. | Yellow. | Yellow. | Dirty yellow. |
| Action of ammonia. | Soluble. | Insoluble. | Insoluble. |
| Action of hydrochloric acid. |
Insoluble. | Soluble. | |
| With cyanide flux. | Sublimes as metallic arsenic. |
Sublimes as brown oxide. |
No sublimate. |
Marsh‘s Process.—This method for the detection of arsenic is founded on the fact that the several compounds of arsenic, except the sulphide and metallic arsenic itself, form a gaseous compound with nascent hydrogen, from which it may be readily separated by appropriate treatment. The solution to be tested should, therefore, be prepared as proposed by Brande and Taylor, given on a preceding page.
Precautions.—(1) Absolute purity of reagents. (2) The sulphuric acid should be diluted with five times its weight of water, and allowed to cool. (3) The suspected fluid should be added gradually. (4) Generate the gas regularly. (5) If no stain be at once produced, keep a portion of the exit tube red-hot for at least one hour.
The usual form of the apparatus is that of a U-shaped glass tube, about one inch in diameter and eight inches high, supported in a vertical position on a wooden stand. One end of the tube is fitted with a tap, and terminates in a glass tube drawn to a fine point; the other end is closed with a cork.
The apparatus is used as follows: A piece of pure zinc is dropped into the tube, and shaken into such a position that it occupies the bottom of that limb of the tube which is furnished with the tap. Water is then added, and subsequently sufficient pure sulphuric acid to cause a moderately brisk evolution of hydrogen. The production of hydrogen gas from pure zinc and pure sulphuric acid is sometimes slow, and may be facilitated by adding a few drops of platinic chloride solution to the contents of the flask previous to the addition of the sulphuric acid. The gas being allowed to [Pg 282] accumulate for a short time, the tap is then partially turned on, and the gas ignited; if, on depressing a piece of white porcelain momentarily in the flame, no deposit or discoloration occur, the reagents used may be taken as pure. By the use of Thorpe‘s apparatus for Marsh‘s test, in which the hydrogen is obtained by the electrolysis of water, the absence of arsenic in the reagents and apparatus is ensured. The tap is now connected with a tube of thin, hard glass, drawn out to a fine point at the end and having a constriction in the middle. The liquid to be tested being now placed in the apparatus, the gas is again ignited, and a piece of white porcelain momentarily depressed in the flame, when, if arsenic be present, a black, circular, metallic-looking stain will appear, which has the following composition. In the centre is the unoxidised metal, round this is a mixed deposit, and outside this the zone of arsenious acid. While the gas is passing, the exit tube should be heated to redness a little behind the constricted part, when a dark ring will appear if arsenic be present. The black deposit on the porcelain may be either arsenic or antimony, but may be distinguished as follows:
| Arsenic. | Antimony. | |
|---|---|---|
| Nature of the stain. | Metallic brilliancy | Absence of metallic lustre. |
| Effect of heat. | Volatile. | Non-volatile. |
| Heated with a little | Dissolves. | Oxidises to a white |
| nitric acid. | insoluble powder. | |
| Warmed with a strong | Dissolves immediately. | Slowly dissolved. |
| solution of chloride | ||
| of lime. | ||
| Treated with | Detached but not dissolved, | Soluble: on evaporation, |
| bisulphide of | but if heated to drive off | orange-yellow sulphide |
| ammonium. | ammonia yellow sulphide | formed. |
| formed. | ||
| The nitric acid | A brick-red precipitate | No reaction, but if |
| solution evaporated | soluble in ammonia | ammonia and potash |
| to dryness gives | are added, a black | |
| with nitrate of silver. | precipitate is ultimately | |
| formed. |
The portion of the tube on which the dark ring has been deposited is now cut off, broken into fragments, and heated in a small, hard glass tube—when, if arsenic be present, a white sublimate will be obtained of well-defined octahedral crystals. If the sublimate be treated with sulphide of ammonium, it is detached but not perfectly dissolved, and on evaporation of the solution to dryness, a residue of the yellow sulphide of arsenic will remain, which, if heated with strong nitric acid, and evaporated again to dryness, will give a brick-red precipitate with nitrate of silver solution, soluble in ammonia. The [Pg 283] process of Marsh may be used quantitatively by passing the issuing gas through a glass tube, dipping into a strong solution of argentic nitrate. A portion of the tube is kept at a red heat, when, if arsenic be present, it is deposited in the metallic form in the cool portion. The glass tube containing the stain is cut with a file and weighed. The stain is then removed by strong nitric acid, the tube dried and weighed: the difference in weight equals the amount of metallic arsenic. The nitrate of silver solution is now treated with pure hydrochloric acid, filtered, and the filtrate neutralised with sodium carbonate, titrated with standard solution of iodine. By dipping the end of the issuing tube into a fresh solution of argentic nitrate, the absence of colour will show that all the arsenic has been obtained.
Instead of the U-shaped tube a Wolff‘s bottle or Erlenmeyer‘s flask may be used, and the exit tube carrying off the gas bent twice upon itself and connected with a glass bulb containing calcium chloride. From this bulb the long, hard glass tube proceeds, pointed at the end to form a gas jet; the gas is lighted at the end, and if a Bunsen flame be applied at a short distance from the end, a deposit of the arsenic, if present, will form on the distal side of the point at which the flame is applied.
Reinsch‘s Process.—First obtain a clear solution by filtration or otherwise, and then proceed as follows: Strongly acidify the liquid with hydrochloric acid, introduce some pieces of copper foil, and heat to near the boiling-point of the liquid. Both the acid and metal must be previously tested to ensure their freedom from arsenic. Any arsenic present will then be deposited on the copper in the metallic state, either in the form of a black lustrous deposit when the arsenic is present in any quantity, or else as a steel-grey coating when a minute quantity only is present. In either case, the copper foil, after remaining for some time in the suspected fluid, is taken out, cut into small pieces, introduced into the bottom of a hard glass tube, and heated to low redness, when the arsenic will sublime as arsenious acid in octahedral crystals, forming a ring in the cooler portion of the tube. The deposit is identified as arsenious acid by the form of the crystals, and by its deportment with the various reagents, as in the treatment of similar sublimates mentioned under Marsh‘s Process. Two precautions have to be taken in applying this test: do not use too large a portion of copper foil at first, and do not remove the copper too quickly from the boiling fluid. A solution containing arsenic acid or an alkaline arsenite, mixed with sulphuric acid, does not produce any deposit on metallic copper even after long boiling, unless the quantity of the arsenic present be considerable; the deposition may, however, be ensured by adding sulphurous acid or a sulphite, whereby the arsenic is reduced to arsenious acid (G. Werther, J. Pr. Chem., lxxxii. 286; Jahresb., 1861, p. 851).
Objections to Reinsch‘s Process.—The chief objection to Reinsch‘s process is the possible impurity of the reagents used—both these reagents, even when supplied as pure, being liable to contain traces of arsenic. As met with in commerce, both hydrochloric acid and metallic copper invariably contain minute quantities of arsenic, the [Pg 284] former generally containing the larger quantity of that impurity. Although, by purchasing the purest possible reagents, specially prepared for analysis, it may be possible to ensure their freedom from arsenic, yet in all cases they should be tested before using them. Some of the hydrochloric acid should be diluted with distilled water, and gently heated with the copper foil. If no tarnishing or deposit of any kind occur on the metal after a lapse of several hours, the reagents may be taken as pure and the trial of the suspected substance at once made.
Professor Abel has proposed the following process to ensure the purity of the copper and acid: Boil together equal portions of strong hydrochloric acid and a solution of perchloride of iron. While the mixture is boiling immerse the copper foil, which, if pure, will be merely brightened in colour; if impure, a black deposit on the metal is formed.
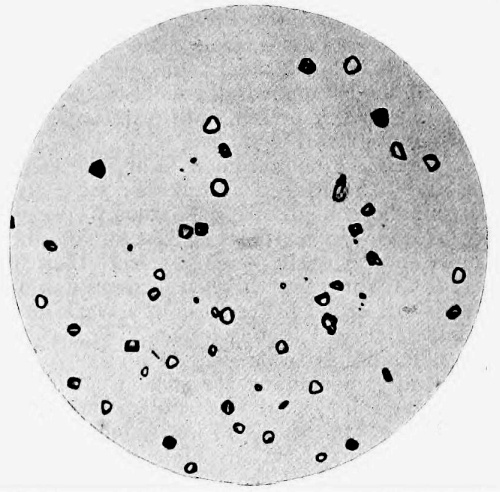
Fig. 30.—Photo-micrograph
of
sublimate of arsenious acid obtained
by Reinsch‘s process, × 250.
(R. J. M. Buchanan.)
Bloxam‘s Method for the Detection of Arsenic.—The late Professor Bloxam suggested an admirable and delicate process for the detection of small quantities of arsenic. The method is, like that of Marsh, founded on the property possessed by nascent hydrogen of forming a gaseous compound with arsenic; but, instead of the hydrogen being generated by the action of dilute sulphuric acid on zinc, Bloxam generates the gas by an electric current.
The wires from the extremities of a battery terminate in small plates of platinum foil, which are plunged into the liquid to be tested, the apparatus being so arranged that the hydrogen gas evolved from the negative pole is collected. The issuing gas is tested in a similar manner to that obtained in Marsh‘s process. [Pg 285]
This method of Bloxam‘s is exceedingly delicate, and possesses one great advantage, that no zinc being used, there is no danger of contamination by the use of impure metal; while, as nothing foreign is introduced during the process of testing, the liquid under examination is left pure for the application of other tests if necessary.
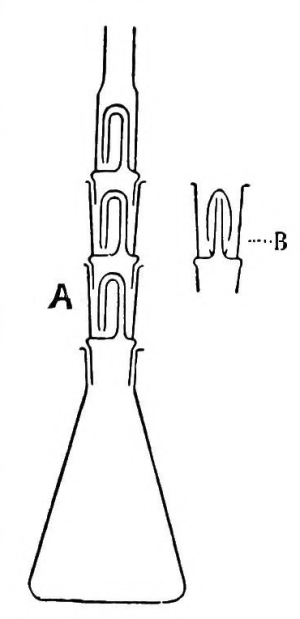
Fig. 31.—Dowzard‘s apparatus for Gutzeit‘s test for
arsenic. A and B indicate glass cells or traps which contain
solutions of lead acetate and copper chloride for the purpose of
fixing H₂S and PH₃ which otherwise would react upon the mercuric
chloride spot on the filter-cap. The cells are fitted into one another,
as shown in the figure.
Gutzeit‘s Test.—This test is more sensitive to the presence of minute quantities of arsenic than that of either Reinsch or Marsh. The apparatus devised by Dowzard should be used (Journ. Chem. Soc., vols. lxxix. and lxxx. 463, p. 715), which consists of an Erlenmeyer‘s flask fitted with superimposed cells, containing solutions which will wash or neutralise those gases which would interfere with the accuracy of the result. The following is Dowzard‘s description of the method of using the apparatus:
“A weighed or measured portion of the sample is mixed with 5 c.c. of pure HCl (if the sample is alkaline it must be neutralised first), four drops of a 15 per cent. solution of cuprous chloride in hydrochloric acid are then added, and the mixture made up to 30 c.c. with water; if it is not convenient to work with such a small bulk as 30 c.c. this quantity may be doubled or trebled, but the same proportion of acid should be used. A rod of pure zinc, 3 cm. long and 5 mm. in diameter, is first placed in the flask, the above mixture is then introduced and the first cell placed in position; lead acetate solution 5 per cent. is now poured into the cell until it is about half full. The second and third cells are filled in a similar manner; a small tuft of cotton wool is introduced into the neck of the top cell, and its mouth capped with mercuric chloride paper, which may be held in position by an elastic band or a glass collar made from a piece of glass tubing. After forty minutes or more the cap is removed and examined in full daylight. A minute trace of arsenic is indicated by a lemon-yellow spot, which varies in tint according to the amount present; and a heavy trace by an orange-brown spot. The mercuric chloride paper is prepared as follows: one drop of a 5 per cent. solution of mercuric chloride is allowed to fall on the centre of a piece (4 cm. square) of thin Swedish filtering paper, such as Muncktell‘s No. 1 F.; the paper is dried before using.” The lead acetate in the cells absorbs any H₂S gas given off, and if additional cells contain a 15 per cent. solution of cuprous chloride in hydrochloric acid, PH₃ is also prevented from passing and causing a stain. By this method arsenic can be detected in the presence of 2500 [Pg 286] times its weight of antimony. The presence of selenium and tellurium compounds does not interfere with the usefulness of this method.
Fleitmann‘s Test.—Detects arsenic in the presence of antimony, but does not detect arsenic as arsenic acid. When zinc or aluminium is heated with excess of potassium or sodium hydroxide in a mixture containing arsenious anhydride, arseniuretted hydrogen is evolved. The gas may be led into 4 per cent. nitrate of silver solution, or a test tube the top of which is covered with filter paper wet with nitrate of silver. The gas reduces the silver salt, and a black precipitate is produced in the solution, or a black spot on the paper.
Fatal Dose.—Two grains in solution have been known to cause death. Recoveries have, however, occurred after an ounce or more of the poison has been taken. Much will depend upon the fulness or emptiness of the stomach at the time the poison is taken, and also upon the vehicle in which the poison is administered. Vomiting and purging are more urgent when the dose is large, probably assisting to get rid of the arsenic before its fatal action is produced.
Fatal Period.—From twenty minutes to two or three weeks, and even later from the secondary effects of the poison. Any thick medium, cocoa or soup, will of course delay the action of the poison.
Treatment.—Vomiting should be promoted, and diluent drinks largely given. The stomach pump, if it can be procured without much delay, should also be employed to empty the stomach. Emetics of sulphate of zinc should be given without delay—followed by the administration of milk, lime-water, and albumen. Symptoms as they occur must be treated on general principles.
The hydrated sesquioxide of iron, the hydrated oxide of magnesia, and animal charcoal have been proposed and used as antidotes. The sesquioxide of iron can be prepared ready to hand by saturating the tincture ferri perchloridi with ammonia or washing soda. It should be given freely. Drachm doses of dialysed iron in water may be administered. Reputed antidotes are useless when the poison is in the solid state. The diarrhœa, tenesmus, collapse, pain, and nervous symptoms should be treated on general principles.
Other Poisonous Compounds of Arsenic
Arsenical Vapour.—The vapour from the flues of the copper and arsenic smelting-works in Cornwall, escaping into the air, may cause death to cattle, and the destruction of vegetation. The workmen in these works not infrequently suffer from eruptions on the skin, and from great constitutional derangement; but, on the whole, taking into consideration the dangerous nature of their employment, the men appear to enjoy average health. Actions for damage and nuisance have resulted from the escape of this vapour from the factories.
Arsenite of Potash.—A solution of arsenite of potash, mixed with the tincture of red lavender (the solution contains four grains of arsenious acid in one ounce)—better known as Fowler‘s Solution, or as Fowler‘s Mineral Solution or [Pg 287] Tasteless Ague Drop. It is probably a solution of arsenious acid in carbonate of potash, and not a true arsenite of potash. This preparation has been much used as a domestic remedy for ague in the Fens of Cambridgeshire. Death from its use is rare; but it is, nevertheless, too dangerous a medicine to be used recklessly. Idiosyncrasy has much to do with the action of the drug, some persons taking even large doses with impunity, whilst, in others, the smallest medicinal dose has produced alarming symptoms. It is stated that the Styrian arsenic-eating peasant is capable of taking without injury five grains of arsenious acid for a dose; and in one case of suspected murder in Styria, the prisoner was acquitted as the deceased was known to be an arsenic-eater.
Donovan‘s Solution.—A solution of hydriodate of arsenic and mercury. Now officinal, and much used by many practitioners.
Sheep Dip.—The mixture used for washing sheep, composed of tar-water, soft soap, and arsenic, has caused death in twenty-four hours. The men engaged in dipping the sheep may suffer both locally and constitutionally from the effects of the arsenic in the solution.
Treatment.—As before described.
Analysis.—See p. 280 et seq.
Arsenite of Copper.—Scheele‘s green, and the aceto-arsenite of copper, Schweinfurt-green, are met with in commerce and the arts as green pigments. Among workmen they are familiarly known as emerald-green, Brunswick-green, or Vienna-green. In France, the term vert Anglais or English green has been given to them. Scheele‘s green contains about 55 per cent. of pure arsenious acid; the other, Schweinfurt-green, about 58 per cent.
These colours are employed for various purposes, among which the following may be mentioned:
The employment of emerald-green in the colouring of wall-papers is so extensive, that in the year 1860 an English paper-stainer stated that he used two tons of arsenic weekly. In 1862 the amount of this colour manufactured during the year was from 500 to 700 tons. Numerous cases of chronic arsenical poisoning have resulted from the presence of arsenic in the form of Scheele‘s green and Schweinfurt-green in wall-papers and other articles. As the colour is only loosely applied to the surface by means of a weak solution of size, it is easily brushed off, and may so impregnate the air of a room as to produce injurious effects on those who inhabit the apartment. By fermentation of the starch paste used for fastening the paper to the walls, nascent hydrogen is liberated, and, combining with the arsenic to form arseniuretted hydrogen, passes into the air of the room and is inhaled. [Pg 288] This gas is extremely poisonous, and small quantities suffice to produce serious results. Certain moulds are endowed with the power of living in materials containing arsenic, and of decomposing arsenious acid or its salts into the gaseous form known as diethylarsine; there are altogether ten such moulds, and the most active is the Penicillium brevicaule.
In the case of ladies‘ dresses, the following method is adopted:
The colouring material is made by thoroughly stirring together a mixture containing, in definite proportions, the green pigment, cold water, starch, and gum arabic, or some similar substance which shall give the colour consistence and adhesiveness. Not infrequently in this process the hand and forearm are freely used in the liquid to expedite the work. Of this mixture, properly prepared, the workman takes a quantity in his fingers and roughly spreads it over the muslin or fine calico. The fabric is then beaten and kneaded between the hands until it is uniformly coloured. The longer this process is continued, the more perfect is the result. The cloth is now fastened to a frame for drying. In all this process of colouring, the hands, forearms, and frequently also the face of the operative must become soiled with the green colour. It will be also observed that the colour is but loosely applied, no mordant being used, as in calico printing, to fix the pigment in the texture of the cloth.
Symptoms.—All the effects produced by arsenic may result from the use of articles coloured with these pigments. Chronic inflammation of the stomach and bowels, and irritation of the eyes, accompanied in some cases with extreme nervous debility and prostration, are by no means uncommon in those employed in the manufacture of this “cheerful,” but poisonous colour. The skin of the hands, arms, and scalp is often attacked by a vesicular eruption or an erythema. When it is borne in mind that, according to the analysis of Hoffman, a single twig of twelve artificial leaves may contain as much as ten grains of pure arsenic, it is not to be wondered at that the most serious results have occurred from the reckless use of these colours. In Prussia and France the use of the arsenical colours is prohibited.
Analysis.—Scheele‘s green is insoluble in water, but is soluble in ammonia, the solution having a blue colour, from the separation of the arsenious acid from the oxide of copper. If a few drops of the blue ammoniacal solution be poured on some crystals of nitrate of silver, the yellow arsenite of silver is formed. The blue ammoniacal solution, if acidified with HCl and boiled with pure copper foil, deposits arsenic on the copper, which, if cut into strips and placed in a small reduction tube and heated, sublimes and is deposited in octahedral crystals on the cold portion of the tube. The tests before described are applicable for the detection of this substance.
Orpiment
Orpiment, or yellow arsenic, one of the sulphurets of arsenic, has been used occasionally as a poison. It is also largely employed in the arts [Pg 289] for paper-staining and for colouring toys. In cases of arsenical poisoning, it is this compound that is commonly found adhering to the stomach and intestines. It is formed by the sulphuretted hydrogen, the result of decomposition, acting on the white arsenic swallowed.
Realgar
Realgar, or red arsenic, is another of the sulphurets of arsenic, and, like orpiment, is largely used in the arts as a colour. It is also employed, like orpiment, as a depilatory, fatal results having followed its use for this purpose. The colour of this substance prohibits its frequent use as a poison.
Both of these compounds owe their poisonous properties to the amount of free arsenious acid which they contain, and which may be as much as 30 per cent.
Symptoms.—The symptoms produced by these substances are similar to those caused by arsenic. The fatal dose will depend on the amount of free arsenious acid which they may each contain.
Treatment.—Emetics and demulcent drinks.
Metallic Arsenic, &c.
Metallic arsenic, fly powder, arsenic acid, largely used in the manufacture of magenta, aniline red, or fuchsine, and the arseniates of potash and soda, are all poisonous. The papier moure of the shops consists of blotting-paper steeped in a solution of arseniate of potash. Macquer‘s neutral arsenical salt is the binarsenate of potash.
Symptoms.—The symptoms are those of arsenical poisoning.
Treatment.—When metallic arsenic has been taken, vomiting must be promoted by the use of proper emetics. Tartar emetic should never be used. In the treatment for poisoning with arsenic acid, or of the arseniates of potash and soda, the hydrated oxide of iron, or of the acetate of iron, should be used, as the arseniates are precipitated by the iron.
Arsenic Acid
No case of poisoning by this substance has been recorded, for, although poisonous, it is better known in the laboratory than in the shops. It differs from arsenious acid in being only partially volatilised by heat, in its solubility in water, and in being precipitated of a brick-red colour by nitrate of silver. With sulphuretted hydrogen a yellow precipitate is slowly formed, insoluble in hydrochloric acid.
Arseniuretted Hydrogen
This gas has proved fatal in several cases. It is generated in the process known as Marsh‘s process for arsenic, and is so poisonous that a very small quantity, not sufficient to be detected by its odour, has [Pg 290] caused death. In most cases death has been the result of accident.
Symptoms.—Giddiness, fainting, constant vomiting, pain in stomach, and suppression of urine, with rapid destruction of the red blood corpuscles, associated with hæmorrhages from all the mucous membranes and jaundice, are among the most prominent symptoms.
The post-mortem appearances are inflammation of the stomach, with softening of its coats. The liver and kidneys are also more or less affected, and have been found of a deep indigo colour.
Analysis.—This has been described when speaking of Marsh‘s process for arsenic.
Cacodylic acid and the cacodylates are poisonous. The acid dissolves easily in water and alcohol, and it unites with many metals and organic substances to form salts. Although it is held by some to be non-poisonous, Murrell asserts that the administration of cacodylate of sodium produces symptoms “far more severe than those which follow the exhibition of arsenic in its ordinary forms” (B. M. J., 1900, vol. ii. p. 1823; 1901, vol. i. p. 120).
Professor Fraser of Edinburgh, on the other hand, from clinical observation and chemical tests, affirms that cacodylic acid and the cacodylates are extremely stable bodies, and the arsenic in them is with such great difficulty set free that it passes through the body in combination as an inert substance (B. M. J., 1902, vol. i. p. 713).
Arsenical Contamination of Food Stuffs
Arsenic is found associated with many other substances in nature, particularly copper and pyrites. Arsenic is commonly present in commercial sulphuric acid manufactured from pyrites containing the metal, and when such acid is used with common salt for the production of hydrochloric acid, the latter also becomes contaminated. It may be safely stated that commercial sulphuric acid, hydrochloric acid, copper and zinc, free from arsenic, do not exist in the market. Hence in the detection of arsenic by the toxicologist the absolute purity of these reagents, which he uses, must be established.
In the manufacture of glucose, arseniferous sulphuric acid has been the means of contaminating it. Ritter and Blyth pointed out the danger, by this means, of conveying arsenic into beer, confectionery, syrup, and other food stuffs. Glucose made with such acid, and used in the manufacture of beer, was the cause, in the year 1900, of a widespread and serious epidemic of arsenical poisoning in Manchester and Liverpool, in which several thousand persons suffered. Arsenic may also contaminate grain during malting by the use of anthracite coal or sulphur bar in the kilns. [Pg 291]
Recapitulation of the Leading Facts
with regard to
Poisoning
with Arsenic
Antimony, the Stibium of the ancients, is obtained from the native sulphide. Metallic antimony is of a bluish-white colour, crystalline and brittle. It melts at about 840° F., and is slowly volatilised at a white heat.
Two compounds of antimony—tartar emetic and chloride of antimony—are alone of any toxicological interest.
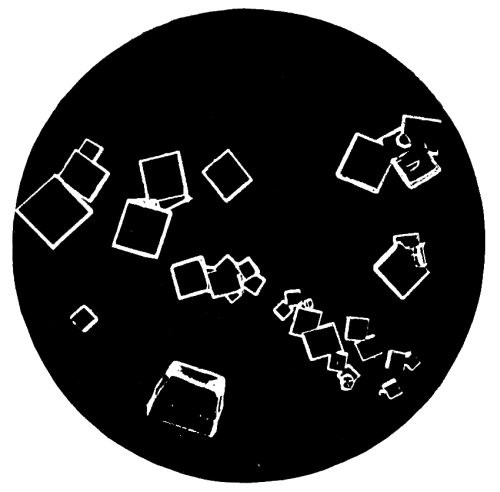
Fig. 32.—Photo-micrograph
of crystals
of tartarated antimony, × 50.
(R. J. M. Buchanan.)
Antimonium Tartaratum. Tartarated Antimony
Tartar emetic occurs as a white powder; sometimes, however, with a yellowish tint. It is soluble in about three parts of boiling water and fifteen of cold, and insoluble in alcohol.
The vinum antimoniale of the Pharmacopœia contains two grains of the salt in an ounce of wine.
Before 1856 poisoning by antimony was of rare occurrence, but since that year several cases of chronic poisoning have occurred, giving to this substance considerable importance.
Symptoms of Antimonial Poisoning
Acute.—Tartar emetic is an irritant poison, but possesses slight corrosive properties. When taken in large doses, two or three drachms, it gives rise to a metallic taste in the mouth, which is not easily removed. In most cases, violent vomiting follows immediately after the poison is swallowed, the vomiting continuing even after the [Pg 293] stomach is emptied of its contents. In a few cases, however, even when a large dose has been taken, vomiting may be absent. Burning pain is felt at the pit of the stomach, accompanied with cramps in the belly and purging. There is considerable difficulty in swallowing, and the patient complains of tightness and constriction in the throat. The mouth and throat in some cases are excoriated, or covered with whitish aphthous-looking spots, which ultimately become brown or black. In some cases the thirst is intense; in others, absent or nearly so. Cramps in the lower extremities, almost amounting in some cases to tetanic spasms, followed by extreme depression, are generally the precursor of a fatal termination. The urine may be suppressed, as is the case in arsenical poisoning; in some cases it has even been increased. On this point, however, the statements of observers differ. Trousseau says that the urine is suppressed; Huseman that it is never suppressed. The skin is in some cases covered by a pustular eruption, not unlike that of smallpox. Dobie has recorded a case of poisoning by tartar emetic in which a comatose condition was present. In antimonial poisoning, even in the most desperate cases, there is always greater hope of recovery than in arsenical poisoning.
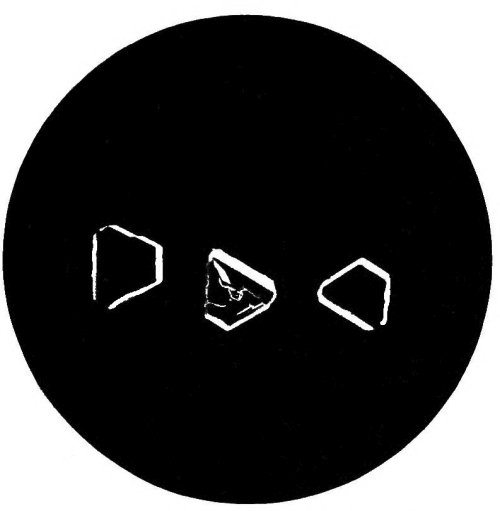
Fig. 33.—Photo-micrograph
of crystals
of tartarated antimony, × 50.
(R. J. M. Buchanan.)
Chronic.—The symptoms which mark the chronic form of poisoning differ chiefly in being less intense and less rapid than in the acute. Chronic poisoning by small repeated doses is that form of poisoning which appears most in vogue of late years—as certain diseases, enteritis, etc., can be simulated by the administration of repeated small doses. The unfortunate victim complains of constant nausea and [Pg 294] retching, with great depression. Food is objected to, as it only increases the vomiting. The matters vomited are at first merely mucus, but after a time they become mixed with bile. Each time the poison is repeated, the symptoms become aggravated. Emaciation gradually sets in, and the person dies from complete exhaustion, or from the effects of a larger dose than usual. Chronic poisoning has given rise to several errors in diagnosis, and the histories of recorded cases should put medical men on their guard. In all doubtful cases examine the urine.
Post-mortem Appearances.—The mucous membrane of the throat, gullet, and stomach is inflamed, and in some places softened and corroded. Aphthous-looking spots are not infrequently found on the mucous membrane of the stomach, and these may also be observed on the throat and on the small intestines. The liver has been found in some cases of chronic poisoning, where the fatal termination has been for some time retarded, enlarged, and its structure so soft as to be easily broken down. Fatty degeneration of the internal organs has been found after protracted fatal administration of the drug. It is stated that in Brunswick the fatty livers of the geese are produced by the judicious administration of antimony. The appearances above detailed may be more or less absent or present, according to the time that may have elapsed from the swallowing of the poison to the time at which death has occurred.
At the post-mortem examination on the body of Mr. Bravo, poisoned with tartar emetic in 1876, the mucous surfaces of the stomach and duodenum were found pale and yellowish. Ulcers were present in the cæcum, and the rest of the large intestine blood-stained, but not ulcerated. Stevenson records the post-mortem appearances of the bodies of three women poisoned by tartar emetic (B. M. J., 1903, vol. i. p. 873). They are of peculiar interest in reference to the preservative action of antimony upon the bodies of those poisoned by it. In the case of M. E. Marsh, upon whose body the examination was made eight days after death, there was no odour of putrefaction, the bowels were in a condition of acute catarrh and streaky congestion without ulceration.
The body of Bessie Taylor had been buried for twenty-one months; ordinary putrefactive changes were absent, and with the exception of the integuments, it was in a remarkably good state of preservation. The alimentary canal showed acute non-ulcerative gastro-enteritis, the stomach and duodenum were of a cinnabar-red colour, the jejunum also in patches. The ileum was covered with orange-red mucus in its lower portion, and there was an orange-coloured patch twelve inches above the ileo-cæcal valve. The patch on analysis was proved to contain antimonious sulphide. Similar orange patches were present in the colon and upper portion of the rectum. There were no ulcerations, but the mucous membrane of the intestines was of a dull cinnabar-red colour.
The body of Mary J. Spink was exhumed five years after burial, and presented a life-like aspect; there was no putrefactive odour, and no larvæ present. The stomach and intestines were of a cinnabar-red colour; there were no ulcerations; the intestines contained orange-coloured mucus. [Pg 295]
Elimination of Antimony from the System
Antimony, taken in a large dose, or in small doses frequently repeated, appears to be rapidly absorbed, and then eliminated from the system by the kidneys. Dating from the time at which the poison was swallowed, it will be found in the organs of the body in the following order:—
1. Stomach and bowels, but slightly in the liver.
2. Absent from the stomach, but present in the liver, spleen, and kidneys—traces in the blood.
3. Present in the fat and bones, with traces in the liver, fæces, and urine.
4. The period required for its complete elimination from the vital organs varies from fifteen to thirty days.
In other words, the presence of antimony in the stomach and intestines points to the recent administration of the poison; and its absence from those organs, and presence in the others above mentioned, to a more remote period of administration. It has been suggested that in some cases the poison may be eliminated by the mucous membrane of the stomach. This assumption has been proved to be correct, for it has been shown that antimony may be found in the stomach after the inhalation of antimoniuretted hydrogen.
Fatal Dose.—It is impossible to state with certainty the exact amount of antimony—tartar emetic—which may prove fatal, as recoveries have taken place even after an ounce had been taken. Large doses are uncertain in their effects, as the severe vomiting which they produce generally helps to get rid of the poison. In small doses, death may result from the depressing action which it exerts over the heart.
Fatal Period.—From a few hours to several weeks, and even months.
Treatment.—Promote vomiting by the administration of warm water, or warm greasy water, or the stomach may be washed out with a syphon tube, unless the chloride of antimony is the poison, and then give tannic acid in drachm doses in warm water, or any vegetable infusion containing tannin—viz., tea, oak bark, or cinchona bark. Demulcent drinks may be administered, and warmth applied. Opium may be given to relieve pain, and stimulants for the depression.
The Detection of Antimony
Prepare the solutions of the liver and other solid organs, and also the contents of the stomach, as described under the detection of arsenic, using tartaric acid instead of hydrochloric acid. Through a portion of one of the solutions, obtained by filtration or dialysis, pass a current of sulphuretted hydrogen, which will produce, if antimony be present, an orange-coloured precipitate of the sulphide of antimony. The precipitated sulphide is dissolved by hot hydrochloric acid with the evolution of sulphuretted hydrogen; and if the resulting solution [Pg 296] be poured into water, a white precipitate is formed of oxychloride of antimony, soluble in tartaric acid. Chloride of bismuth is precipitated when poured into water, but the precipitate is turned black by sulphide of ammonium, the antimonial orange-red; the precipitate of bismuth is not soluble in tartaric acid, the antimonial is soluble.
Marsh‘s and Reinsch‘s processes may also be used for the detection of antimony. The former is, however, open to the objection that antimony, when present in any quantity, rapidly precipitates on the zinc in the form of a flocculent black deposit, while the issuing gas is found to contain only traces of the metal.
Reinsch‘s process is, however, very delicate, and its application is in every respect similar to that in use for the detection of arsenic. The acid liquid should, however, be boiled down to a small bulk with the copper, before a conclusion is drawn as to the entire absence of the metal.
Table giving the Characteristic Reactions
of Antimonial and Arsenical Deposits
on Copper.
| Antimony. | Arsenic. | |
|---|---|---|
| The colour of the | Lustrous, with a violet hue. | Dark steel-grey colour, |
| deposit on copper | and lustrous. | |
| by Reinsch‘s | ||
| process is— | ||
| The coated copper | No effect, or only a | Well-marked sublimate |
| heated in the end | trifling white sublimate, | of octahedral crystals; |
| of a small tube. | non-crystalline, | is readily volatile. |
| non-volatile. If the | ||
| sublimate be dissolved | ||
| in solution of tartaric | ||
| acid and sulphuretted | ||
| hydrogen passed | ||
| through the solution, | ||
| the orange antimonious | ||
| sulphide is thrown down. |
It may be noted that mercury likewise yields a deposit on copper with Reinsch‘s process; but the coating is in this case either of a grey colour or white, and silvery on the application of friction. When the coated copper is heated in a glass tube, there is a sublimate of metallic mercury readily aggregating into globules on being rubbed with a glass rod. If the deposit is trifling in quantity, a magnifying-glass should be used to identify the metallic globules. This test at once distinguishes a deposit on copper due to mercury from that produced under similar conditions by arsenic or antimony.
Quantitative Analysis.—Take a measured quantity of the suspected liquid and precipitate thoroughly with sulphuretted hydrogen. Wash, dry, and weigh precipitate. One hundred parts equal 202.78 parts of crystallised tartar emetic. [Pg 297]
Recapitulation of the
Leading Facts
with regard to Poisoning
with Antimony.
Metallic mercury possesses no toxicological interest, as it appears to be almost inert, even in very large doses. If applied to the skin in a finely-divided state, as in mercurial ointment, or internally, as blue pill, its toxic effects may be produced. The vapour given off from the metal is highly poisonous, producing salivation, emaciation, and death. A singular accident of poisoning by mercurial vapour occurred on board H.M.S. Triumph in 1810, owing to the bursting of bladders containing large quantities of the metal; in three weeks 200 men were affected with salivation, etc., nearly all the cattle on board died, as well as the mice, a dog, and a canary-bird.

Fig. 34.—Photo-micrograph
of crystals of corrosive sublimate, × 50.
(R. J. M. Buchanan.)
Corrosive Sublimate
This is the most important of the preparations of mercury. It occurs either in crystalline masses of prismatic crystals or as a white powder. It is now known among chemists as the perchloride, though it is frequently spoken of as the bichloride, chloride, and oxymuriate of mercury. It has a powerful metallic and styptic taste, and is soluble in about sixteen parts of cold water and three of boiling water. Alcohol and ether readily dissolve it, the latter having the power of abstracting it from its solution in water. This property of ether is of importance as a means of separating corrosive sublimate from its solution in other liquids. It is important to remember that corrosive sublimate is soluble in alcohol (R. v. Walsh). The liquor hydrargyri perchloridi of the Pharmacopœia contains half a grain [Pg 299] of the salt to a fluid ounce of water. Half a grain of the muriate of ammonia is added to increase the solubility of the mercurial salt. Applied externally to the unbroken skin, corrosive sublimate has caused death in several cases, the symptoms being almost identical with those which follow the entrance of the poison into the stomach. Toxic symptoms have followed intra-uterine or vaginal injections of solution of perchloride of mercury, also when it has been used to wash out abscess cavities. Acute poisoning, in some cases fatal, has resulted from the external application of corrosive sublimate to ulcers and tumours.
Symptoms of Poisoning by
Corrosive Sublimate
Acute.—The symptoms come on almost immediately the poison is swallowed. A strong metallic coppery taste in the mouth is experienced, and a choking sensation in the throat. Pain of a burning character is felt, extending from the mouth to the stomach, followed by nausea and vomiting of stringent mucus, more or less tinged with blood, and violent purging, the evacuations being also mixed with blood and mucus. The pulse is feeble, quick, and irregular; the countenance flushed or pale, and the tongue white and shrivelled. This appearance of the tongue is not present in all cases. Broncho pneumonia may occur. The skin is cold and clammy, and the functions of the kidneys are altered and albuminuria present, there being in many cases complete suppression of urine. As is the case with other irritant poisons, the symptoms and effects produced admit of considerable variation. Thus, there may be no pain in the stomach, and no purging. Salivation is present in some cases, but chiefly in those in whom the fatal termination is somewhat prolonged. This sign is not infrequently absent. Poisoning with corrosive sublimate differs from arsenical poisoning in the following particulars:—Corrosive sublimate has a distinct metallic taste, arsenic is almost tasteless; the symptoms in the former supervene immediately the poison is swallowed, in the latter there is a short delay. The discharges in corrosive sublimate are more frequently bloody than in arsenic poisoning.
Chronic.—The symptoms present in this form of poisoning are modified by the size of the dose, and the interval allowed to elapse between each dose. Nausea, followed by occasional vomiting, and pains in the stomach, are complained of by the patient. There is general constitutional disturbance, with anæmia and cachexia, and consequent mental depression. Salivation, as might be expected, is a more prominent symptom than in acute poisoning; but the salivation may be intermittent—that is, it may cease and then reappear, even after the lapse of months, without an additional dose of mercury having been given in the interval. Salivation may also come on in the course of certain diseases, attacking the salivary glands, and it may also be produced by other causes—pregnancy, etc. The glands of the mouth become swollen and painful, the gums tender, and the teeth loosened fall out of the mouth. Periostitis of the jaw may occur. The breath has [Pg 300] a peculiar, offensive smell, the bowels are irritable, and diarrhœa is not infrequently present. It must be borne in mind that in certain diseases—granular disease of the kidney—the smallest dose of any mercurial preparation may produce profuse ptyalism. And the toxicologist must be careful not to mistake the affection known as cancrum oris, or “the canker,” most common in delicate, ill-fed children and adults, for the effects of mercury. The nervous system is more or less affected, neuralgic pains and mercurial tremors being present in many cases. The tremors commence in the tongue and face and spread to the arms and legs—they are similar to those of paralysis agitans; at first they are invoked by exertion, finally they become continuous; they cease during sleep. Paralysis may also occur, especially in those exposed to the vapour of mercury. Habit appears to exert some influence on the action of corrosive sublimate, if we may accept the story of the old man of Constantinople, who for thirty years took large doses till his daily allowance was a drachm, and then died at the respectable age of one hundred years.
Post-mortem Appearances.—The morbid appearances are chiefly confined, as is the case with arsenic, to the stomach and bowels; but the corrosive action of the mercurial sublimate is more marked. Inflammation more or less intense is always present in the stomach, the mucous membrane of which may be found of a slate-grey colour, corroded, and so soft as to scarcely admit of the removal of the organ without tearing it. The cæcum and rectum are also sometimes found inflamed, and the mucous membrane softened. Perforation of the stomach is very rare, only one case having been recorded in which this was present. The mouth, throat, and gullet may also present signs of the action of the poison similar to those just described as seen in the stomach. Patches of pneumonia are present in the lungs of some cases, and the kidneys show coagulative and desquamative nephritis.
Fatal Dose.—The smallest dose was two grains in the case of a child, but the exact amount to cause death in an adult has not been accurately determined. Recovery has taken place after one hundred grains has been taken.
Fatal Period.—From half an hour to five days. No exact time can be stated. In one case death took place on the twelfth day after swallowing seventy grains of the perchloride.
Treatment.—Vomiting, if present, must be encouraged; if absent, it must be produced by emetics—zinc sulphate or cupric sulphate, followed by copious draughts of warm water. The hypodermic injection of ¹/₂₀ to ⅒ grain of apomorphine may also be used to produce vomiting. Albumen, the white of egg, or vegetable gluten produced from flour by washing it in a muslin bag, should be given. The albuminate of mercury so formed should be quickly removed by an emetic or lavage by means of a soft tube and funnel in mild cases, as it is soluble in excess of albumen, and may be digested or absorbed. The rapid removal of the poison from the stomach, however, is the end to which all our exertions must tend. The forcible use of the stomach pump should not be employed [Pg 301] if it can possibly be avoided, as it may greatly injure the softened mucous membrane of the gullet and stomach. Opium may be given to relieve pain, and opium enemata to relieve purging and tenesmus.
Calomel
Calomel, or the subchloride of mercury, is not used as a poison. In large doses it may act as an irritant poison, and death has not infrequently occurred even from comparatively small doses. Profuse salivation and gangrene of the mouth have resulted from its use, and cases are recorded of death resulting from these. In many cases idiosyncrasy appears to modify, more or less, the action of this preparation of mercury. The poisonous effect of calomel has been attributed to—(1) Adulteration with corrosive sublimate. (2) Conversion of the calomel into corrosive sublimate by the action of the hydrochloric acid of the gastric juice.
N.B.—The free acid of the gastric juice is probably in too small a quantity to materially alter the composition of the calomel.
Ammonio-Chloride of Mercury
White precipitate may, if taken in large doses, produce alarming effects, but it cannot be regarded as an active poison. Pavy‘s experiments on rabbits indicate that it is a more powerful poison than was formerly thought to be the case. Its action is that of an irritant, accompanied with, in some cases, severe salivation.
Red Precipitate
Red oxide of mercury possesses poisonous properties, but it is seldom employed as a poison. The symptoms most frequently present are vomiting, coldness of the surface of the body, stupor, pain in the abdomen, and cramps of the muscles of the lower extremities. The vomited matters are generally mixed with some of the red oxide.
Cinnabar. Vermilion
A compound of sulphur and mercury in the form of a dark red crystalline mass is known as cinnabar; and to the same substance reduced to a fine powder the name vermilion has been given. It is used as a red pigment. It can scarcely be considered as a poison, Orfila asserting that it is not poisonous. The vapour of this substance appears, however, to be capable of producing severe symptoms, and in one case, profuse salivation resulted from the application of the vapour to the body.
Cyanide of Mercury
This substance, though an active poison little inferior to corrosive sublimate, is seldom used as such, probably from its being better known to chemists than to the general public. It differs from corrosive [Pg 302] sublimate in having no local corrosive action. It has been supposed, but proof is wanting, that its injurious effects are due to its decomposition by the acids of the stomach and the formation of prussic acid. Death has occurred in nine days from a dose of ten grains. It acts as an irritant. The sulphocyanide of mercury is used in the manufacture of the toy known as Pharaoh‘s serpents.
Turbith Mineral
A powerful irritant poison, but seldom used. A drachm has caused death in a boy sixteen years of age. Coldness of the surface, burning pain in the stomach and bowels, with other symptoms of irritant poisoning, were present. After death, the mucous membranes of the throat, stomach, and bowels were found considerably inflamed.
Nitrates of Mercury
These substances—the nitrate and sub-nitrate—are used in the arts for various purposes. They act as powerful irritant poisons, with symptoms and post-mortem appearances not unlike those before described when speaking of corrosive sublimate and other irritants.
Chemical Analysis:
Table showing the Reaction of Mercuric and
Mercurous Salts with Reagents
Detection of Mercury in the Tissues and
in the Contents of the Stomach.
Mercury is particularly liable to be absorbed by the tissues; it also readily combines with various organic substances, gelatine, albumin, &c.
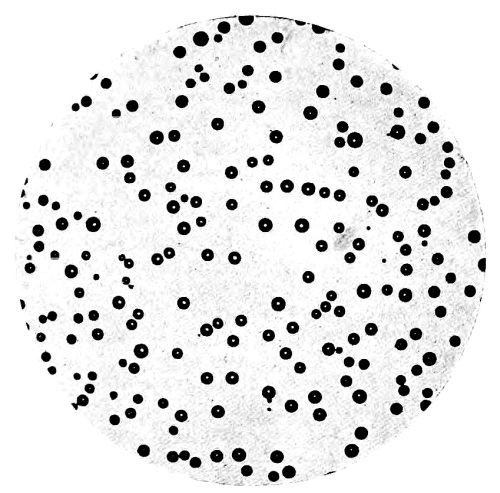
Fig. 35.—Photo-micrograph
of globules of
mercury obtained by Reinsch‘s process, × 50.
(R. J. M. Buchanan.)
A.—If the contents of the stomach are under examination, they should be diluted with distilled water, filtered, and the residue pressed and reserved for further examination.
The liquid thus obtained may be concentrated, and, while still warm, slightly acidified with hydrochloric acid. A slip of zinc foil, with a piece of gold foil twisted round it, is then introduced. If mercury be present, the gold will, sooner or later, lose its yellow colour, and its surface become white and silvery, while the zinc is wholly or partially dissolved. The gold being removed, separated from the zinc, washed first with water and then with ether, is divided into two equal parts. One half may be heated in a reduction tube, when it will yield a sublimate of metallic mercury, identified by the spherical form of the globules under a magnifying-glass, and their metallic reflection and complete opacity. The other half of the gold may be treated with nitric acid and heated, which will dissolve off the mercury. The resulting solution, after expelling the excess of acid by evaporation, will give a scarlet precipitate with iodide of potassium soluble in excess; and, with protochloride of tin, a black precipitate of metallic mercury.
B.—For the detection of mercury in the insoluble form, the [Pg 304] residue from A is dried; or, if the tissues are under examination, they should be finely divided, and freed from superfluous moisture. In either case, the substance is boiled in moderately strong nitric or hydrochloric acid (about one part of acid to four of water). After digestion for some time, the liquid is filtered, concentrated, and tested as in A. When there is reason to infer the presence of corrosive sublimate in considerable quantity in an organic liquid, advantage may be taken of the solubility of the salt in ether, and the power possessed by this liquid of abstracting it from its aqueous solutions. The liquid is agitated with an equal volume of ether, the ethereal solution poured off and allowed to spontaneously evaporate, when the corrosive sublimate will be left in white silky prisms, yielding all the characteristic reactions of the salt. In obscure cases of salivation, the saliva should be examined as follows: Take about two drachms of the saliva, acidulate with pure hydrochloric acid, and immerse in the mixture a very small piece of copper gauze attached to a platinum wire, and set aside in a warm place for some hours. If mercury be present, the copper will be covered with a white coating; this should be washed and heated in a reduction tube, when globules of mercury will be formed, and examined with a lens.
C.—Mercury in solution may be detected by Reinsch‘s process. On boiling with pure copper foil after acidifying the solution with hydrochloric acid, the mercury is deposited on the copper in the metallic state, as a whitish silvery film, which can be polished to a silvery mirror surface. On washing the film in water, ether, and absolute alcohol and allowing it to dry, then subliming it in a reduction tube by the aid of heat, the mercury deposits on the cool part of the tube in the form of minute globules, which may be easily recognised through the microscope. If a small crystal of iodine be now placed in the tube and gently warmed so as to volatilise it, but not the mercury, and the tube be left to stand for a short time, the iodine combines with the mercury to form the scarlet iodide, the colour of which renders it easy of recognition.
According to Bonnewyn, the presence of an extremely small quantity of corrosive sublimate (¹/₅₀₀₀₀) in calomel may be detected by immersing a clean knife blade, moistened with alcohol or ether, in the suspected calomel. A black spot is formed on the steel very difficult of removal. No spot is formed when the calomel is pure.
Metallic lead is not poisonous; but it appears probable that when it is acted upon by the acids of the intestinal secretions, it may become so changed as to produce unpleasant symptoms. Any salt of lead is poisonous when in a condition to be absorbed into the system.
Sugar of lead and white lead are alone important, and will therefore be briefly considered. [Pg 305]
Sugar of Lead
Acetate of Lead. Subacetate. Goulard‘s Extract
General Character.—The acetate of lead, better known as sugar of lead, is not unlike loaf-sugar in its general appearance. It is usually met with in the form of solid crystalline masses of a white or brownish-white colour. To the taste it is sweet, a metallic astringent taste being left in the mouth. Acetate of lead is soluble in water and in alcohol. The subacetate is a more active poison than the neutral acetate. Sugar of lead is popularly considered as an active poison, but this does not appear to be the case. Sir R. Christison gave eighteen grains daily in divided doses for eight or ten days with no other unpleasant symptoms than slight colicky pains in the abdomen. Lead is probably eliminated from the system by the urine, and also by the milk; but there is reason to believe that when once deposited in the body, some considerable time is required for its complete elimination. Dr. Wilson is of opinion that in chronic lead poisoning the lead is more largely deposited in the spleen than in any other organ of the body. This organ should therefore always be carefully examined in suspected cases of poisoning by this metal.
Goulard‘s Extract is a solution of the subacetate of lead. It may be of a reddish colour, from the employment of common vinegar in the place of pure acetic acid in the manufacture.
Goulard‘s Lotion is the extract diluted with water.
White Lead
White lead, carbonate of lead, ceruse, or kremser white, is used as a pigment. It is generally in the form of white, heavy chalky masses, insoluble in water, and, when taken in large doses, poisonous. It is this substance which, in the majority of cases, causes chronic lead poisoning, or painter‘s colic.
The chloride and nitrate, the oxides, litharge and red lead, are all poisonous; but the sulphate, due probably to its insolubility, appears to be inert.
Lead poisoning may result from—
1. Constant contact with lead and its salts in manufactories.
2. Its use in the arts and as a pigment. The injurious effects of this substance are strikingly seen among painters, the makers of glazed cards, and the workmen engaged in preparing Brussels lace—this material being whitened by beating white lead into it. All thus employed are liable to suffer more or less from chronic poisoning.
3. Its application to the surface of the body in the form of ointment, plasters, cosmetics, and hair-dyes.
4. Drinking water impregnated with lead, from being stored in leaden cisterns or conveyed in leaden pipes.
“The action of water upon lead is much modified by the presence of saline substances. It is increased by chlorides and nitrates, and diminished by carbonates, sulphates, and phosphates, and especially by carbonate of lime, which, held in solution by excess of carbonic acid, [Pg 306] is a frequent ingredient of spring and river water. But water highly charged with carbonic acid may become dangerously impregnated with lead, in the absence of any protecting salt, in consequence of its solvent power over carbonate of lead. In general, water which is not discoloured by sulphuretted hydrogen may be considered as free from lead; but there are few waters which have passed through leaden pipes, or have been retained in leaden cisterns, in which a minute analysis will not detect a trace of the metal; and were it not for the great convenience of lead, iron pipes and slate cisterns would, from a sanitary point of view, be in all cases preferable.
“Another case of contamination by lead may arise from electric action, as where iron, copper, or tin is in contact with or soldered into lead; and in these cases, owing to the action of alkaline bases as well as of acids upon the lead, danger may occur when it is thrown into an electro-negative as well as into an electro-positive state.
“Cisterns are sometimes corroded and their bottoms are perforated by pieces of mortar having dropped into them, the lime of which has caused the oxidation of the metal and a solution of the oxide.”
5. Lead may also find its way into the system by means of the food. Farinaceous foods, chocolate, and tea may become contaminated if lead wrappers be used; and confectionery from the use of lead chromate as a colouring agent. The use of leaden vessels in the manufacture of cider is attended with danger, and also the keeping of pickles in glazed earthenware jars. The celebrated “Devonshire Colic” was the result of cider-making in leaden vats. Beer may be contaminated with lead if allowed to stand in leaden pipes overnight. Rum has been known to have been dangerously impregnated with lead, leaden worms having been used attached to the stills. Many tobacconists are in the habit of using lead foil to wrap up their tobacco and snuff; this practice has resulted in several cases of chronic lead poisoning. Soda and Seltzer waters may contain lead when kept in syphons with leaden caps or valves.
6. Acute and subacute cases of poisoning occur from the taking of lead in the form of diachylon pills to procure abortion.
Symptoms of Poisoning by Lead
Acute.—A metallic taste in the mouth, accompanied with dryness in the throat and intense thirst, is experienced by the patient soon after the poison is swallowed. In some cases, however, two or more hours may elapse before the effects of the poison begin to show themselves. Vomiting may or may not be present. Twisting colicky pains are felt in the abdomen, relieved in some cases by pressure. The paroxysms of pain may be separated by intervals of ease. The bowels are, as a rule, obstinately confined, and the fæces are of a dark colour, from the formation of the sulphuret of lead. The skin is cold, the pulse quick and weak, and there is considerable prostration of strength. In some cases the patient suffers from cramps of the calves of the legs, and sometimes, in protracted cases, paralysis of one or more of the extremities may supervene. The effect on the nervous [Pg 307] system, headache, temporary blindness, is marked by giddiness, and stupor, in some cases delirium even resembling acute mania, terminating in coma, or convulsions and death. Albuminuria may occur.
Chronic.—This form of poisoning generally occurs among painters, manufacturers of white lead, pewterers, and others. The early symptoms are those of ordinary colic, only more severe. The patient generally complains, in the first instance, of feeling unwell, and of general debility. He then suffers from pain of a twisting, grinding nature, felt in the region of the navel, the abdomen being retracted and hard. The bowels are obstinately confined. The appetite becomes capricious, and may be entirely lost. The mouth is parched, the breath fœtid, the countenance sallow, the skin dry, and general emaciation sets in. A nasty sweetish metallic taste in the mouth is present in most cases. Not infrequently the subjects of lead poisoning experience a peculiar form of paralysis of the upper extremities, well known as “dropped hand.” It appears that this condition is the result of paralysis of the extensor muscles of the wrist, the long supinator escaping. In other cases the muscles of the shoulder girdle or pelvic girdle and legs may be affected. Acute general paralysis has occurred in workers with lead, and may prove fatal. Optic neuritis and optic atrophy occur in some cases. Persistent headache may be present in others. The muscles undergo a form of fatty degeneration. The lead appears to act primarily on the muscles, then on the nerves, and lastly on the nerve centres. The absorption of lead causes marked anæmia with degeneration of the red corpuscles, which show marked punctate basophilia. One other symptom of importance has yet to be noticed. The gums, at their margins where they join the teeth, present a well-marked blue line, absent where a tooth has been removed. This is not present in all cases, but it should be looked for. Chronic lead absorption produces cardiovascular changes with arterio-sclerosis, valvular degeneration, cardiac hypertrophy, and chronic renal changes with albuminuria. Closely associated with these conditions are saturnine arthritis and gout. The effects upon the vessels may predispose to cerebral hæmorrhage or lead encephalopathy. Cicconardi suggests as a method of diagnosis in lead poisoning, where the cause of the colic is uncertain, to paint the skin with a 6 per cent. solution of sodium sulphite. If lead be the cause the painted part will become darkened in colour.
N.B.—The symptoms produced by white lead—carbonate of lead—are those of colica pictonum, or painter‘s colic, described under the head of Chronic Lead Poisoning.
Post-mortem Appearances.—In acute poisoning the mucous membrane of the stomach and intestines is inflamed, and is in some cases covered by layers of white or whitish-yellow mucus, more or less impregnated with the salt of lead swallowed. Corrosion of the mucous membrane may occur if the dose be large, and this condition is more frequently present when the neutral salt is taken.
In chronic poisoning there are no constant post-mortem appearances. [Pg 308] The muscles of the paralysed extremity are usually found flaccid, of a cream colour, and the subject of fatty degeneration.
Fatal Dose.—Sugar of lead is not an active poison, recovery having taken place after one ounce had been swallowed.
Fatal Period.—Uncertain.
Treatment.—The stomach should be emptied by means of the pump or syphon tube, followed by the free administration of the sulphates of soda and magnesia. The carbonates should not be given, the carbonate of lead being poisonous. Vomiting should be promoted, and a powerful cathartic administered. Albumen and milk should also be given, as these precipitate the oxide. In the chronic form of poisoning, the iodide of potash and aperients, notably the sulphate of magnesia, should be administered. Dixon Mann does not consider that iodide of potash is of any value as an eliminator of lead, as the latter forms a stable compound with the tissues. Sulphur baths are also useful in removing the lead from the system. Lately the galvanic bath has been tried with great success. By way of prophylaxis, it has been recommended that all those engaged in lead manufactories, or who are obliged to handle this metal frequently, should partake largely of lemonade made with sulphuric acid, should not take their meals in the factories, or without well washing the hands.
Chemical Analysis.—When the solid acetate is heated on platinum foil, it melts, then solidifies, becomes dark in colour, and gives off fumes of acetic acid.
The following are the liquid tests for lead in solution:
1. Dilute sulphuric acid gives a white precipitate of the sulphate, which is insoluble in nitric, but soluble in hydrochloric acid, in excess of caustic potash solution, and in ammonium acetate solution.
2. Solution of potassium iodide gives a yellow precipitate, soluble in boiling water and caustic potash solution.
3. Sulphuretted hydrogen, or ammonium sulphide, gives a black precipitate.
4. Potassium bichromate a yellow precipitate.
Detection of Lead in Organic Mixtures
The contents of the stomach or vomited matters must be diluted with water and filtered. The residue left on the filter, washed with distilled water, should be set aside for further examination; the filtrate and washings acidified with nitric acid. A current of sulphuretted hydrogen passed through the solution will then throw down the whole of the lead, should any of that metal be present, in the form of a brownish-black sulphide, which may be collected on a small filter and dried. The sulphide, boiled with dilute nitric acid, is partly converted into insoluble sulphate, and in part dissolved as nitrate. The carefully neutralised solution may be either tested at once or carefully concentrated. In either case, the production of a bright yellow precipitate, with a solution of bichromate of potash, and a similar one with a solution of iodide of potassium, may be taken as [Pg 309] conclusive of the presence of lead. The portion of lead deposited as sulphate will be found to be soluble in a solution of pure potash, the resulting liquid giving a brown-black precipitate on the addition of sulphide of ammonium.
The insoluble residue left on the filter should be incinerated in a porcelain crucible, either with or without nitric acid, care being taken not to raise the temperature more than is necessary to produce the desired effect: the carbonised mass boiled with dilute nitric acid evaporated to dryness, extracted with distilled water, and then filtered, the filtrate tested as before mentioned. It is often useful, as a preliminary test for the presence of lead in a soluble form, to dip a piece of bibulous paper into the clear liquid obtained by submitting the contents of the stomach or vomited matters to filtration, and then exposing the paper to the action of a current of sulphuretted hydrogen. If lead be present, blackening of the paper will take place.
To detect the lead in the urine and fæces, Dixon Mann advised the urine to be evaporated to the consistency of gruel, and the fæces to be mixed with distilled water to a similar consistence; the organic matters are then to be destroyed with hydrochloric acid and chlorate of potash with the aid of heat, and the solution filtered. The filtrate is then placed in a cell with a parchment bottom, and this into another cell containing distilled water acidulated with sulphuric acid. Two pieces of platinum foil are now placed in the inner and outer cells, separated by the parchment; that in the inner cell is connected with the cathode, that in the outer with the anode of four Grove cells, and the current closed for several hours. The lead, if present, is deposited on the platinum connected with the cathode.
The magnesium method (Marsden & Abram) is useful. A strip of pure magnesium is placed in the urine, to which has previously been added ammonium oxalate, about 1 gramme to 150 c.c. Lead, if present, is deposited on the magnesium in about half an hour, but it may take some hours. The strip is washed in distilled water and dried—warmed with a crystal of iodine the yellow iodide will form; or the deposit may be dissolved in HNO₃ and tested in the usual way.
Goadby recommends inoculating the urine with bacillus coli, which during its growth produces H₂S; this precipitates any lead as sulphide. After filtering, the filtrate is dissolved in a small quantity of 10 per cent. nitric acid and tested by the usual methods.
Recapitulation of the Leading Facts with
regard to Poisoning by Lead
Metallic copper, like metallic lead, is not poisonous, but its oxides are; it should, therefore, not be swallowed, as it is rapidly acted on by the intestinal secretions and poisonous compounds formed. An alloy of copper is used for ornamenting ginger-bread, &c. All the salts of copper are poisonous. The most important are, however, the sulphate, blue-stone, or blue vitriol, and the subacetate or verdigris.
Copper is eliminated to a slight extent by the urine. It has been found in the stomach, liver, and intestines eight months after its administration had been discontinued. It has also been detected more readily in the bronchial secretion than in the urine.
Symptoms of Poisoning by Copper
Acute.—The primary action of the sulphate of copper in from five- to fifteen-grain doses is that of a quick emetic; in larger doses, a powerful irritant; but when absorbed, it appears to act chiefly on the brain and nervous system. Its irritant action is marked by nausea, vomiting, griping pain in the belly, which is greatly distended, and increased flow of saliva. The vomited matters are of a bluish or greenish colour, and the discharges from the bowels greenish and containing blood. The vomited matters become blue on the addition of ammonia. The above-mentioned symptoms usually follow immediately after the poison is swallowed, and rapidly increase in severity. After a time, the remote effects supervene, marked by headache, giddiness, laboured breathing, quick irregular pulse, coma or convulsions, paralysis, and death. [Pg 311]
In poisoning by this substance, the convulsions are most violent, and wild incoherent delirium not infrequent.
The subacetate of copper or verdigris produces symptoms not unlike those just described. Jaundice and suppression of urine may result when either this or the sulphate is taken.
Chronic.—Constant and troublesome irritation of the stomach and bowels; vomiting and purging, attended with considerable straining at stool; loss of appetite, loss of power, and general emaciation set in. The patient is subject to frequent trembling of the limbs, which may end in paralysis. The mouth is unpleasant, and a coppery, metallic taste is experienced. Cramps or colicky pains in the belly are not infrequently present. Jaundice is sometimes present. The vomited matters are greenish; but the practitioner must not be led away, and thus mistake the colour of the vomited matters which occur in some morbid states of the bile, for the result of poisoning by a salt of copper. A form of chronic poisoning affecting workers in this metal has been described by some French pathologists as “copper-colic.” A cachectic condition of the system, accompanied with one or more of the symptoms already detailed, marks this form of poisoning. A purple line along the margins of the gums is present in some cases.
Copper poisoning may result from—
1. Its introduction into the system by using, for culinary purposes, copper vessels not properly tinned. An interesting account of poisoning from this source may be found in the second volume of the Medical Observations and Inquiries by a Society of Physicians in London, published 1764. The cases there recorded occurred on board ship, with most alarming symptoms.
2. By constant application of the metal to the surface of the body, necessitated by certain processes in its manufacture and in its application for industrial purposes. M. Michel Levy, however, says in his work, Traité d‘Hygiène, Publique et Privée, that workmen in copper may pass green-coloured urine and yet be as robust and as long-lived as other workmen.
3. The use of certain preparations of this metal as pigment.
4. The use of German silver—an alloy of copper, zinc, and nickel—may be rendered dangerous by the action of acid food upon the compound.
5. The use of a salt of copper to give a green fresh colour to certain tinned vegetables and fruits, peas, &c., now introduced into this country from France.
Post-mortem Appearances.—The mucous membrane of the stomach is inflamed, the inflammation extending sometimes into the gullet. The intestines may be found perforated. The lining membrane of the whole alimentary canal presents a deep green colour, distinguished from that the result of a morbid condition of the bile by being turned blue on the addition of ammonia.
Fatal Dose.—Nothing certain is known as to the exact quantity that may prove fatal, as the evidence of the poisonous action of copper [Pg 312] is somewhat contradictory. It appears to be more dangerous in small doses than in large ones. Half an ounce of verdigris or subacetate has proved fatal to an adult.
Fatal Period.—The shortest time on record is four hours.
Treatment.—Induce vomiting, and assist the emetic action of the copper salts by the free use of warm water, milk, or any demulcent drink. The stomach tube may be used if vomiting does not occur. As an antidote, large quantities of albumen and iron filings have been given, of which the former appears to be most efficacious.
Chemical Analysis.—The following are the liquid tests for copper in solution:—
1. Ammonia gives a bluish-white precipitate soluble in excess, forming a blue solution.
2. Sulphuretted hydrogen and ammonium sulphide give a chocolate-coloured precipitate.
3. Ferrocyanide of potassium gives a port-wine colour, or reddish-brown precipitate.
4. If a bright steel needle be introduced into an acid solution of copper, the metal is deposited on the needle.
5. If a piece of zinc bound with platinum wire be placed in a solution of a copper salt, the metal is deposited on the platinum; it is turned violet on exposure to the vapour from sulphuric acid mixed with potassium bromide.
Detection of Copper in Organic Liquids
A.—The finely-divided tissue, or the contents of the stomach, diluted with water, are thrown on a filter, and the insoluble portion set aside for further treatment. (See B.)
The filtrate and washings may now be concentrated, acidified with sulphuric acid, and a polished needle inserted in the liquid; and should no immediate deposition of metallic copper occur, it may be allowed to remain for several hours. The colour of the metallic deposit is highly characteristic of copper. As a corroborative proof, the concentrated liquid may be placed in a platinum capsule with some fragments of zinc, when the copper will be deposited on the platinum capsule at the parts in contact with the zinc; the liquid poured off, and the excess of zinc adhering to the platinum removed by dilute hydrochloric acid. The copper may now be dissolved off the platinum by nitric acid, the excess of acid driven off by heat, and the solution subjected to the wet tests given above.
B.—The insoluble portion from A is incinerated in a porcelain crucible. The ash thus obtained is digested in hydrochloric acid with the aid of heat, and evaporated nearly to dryness. The residue, dissolved in distilled water, may be tested as under ‘A.’
The sulphate and the chloride of zinc are alone important. Poisoning by the chloride of zinc has been described (p. 265). [Pg 313]
Sulphate of Zinc
White vitriol or white copperas.
Symptoms.—The sulphate of zinc acts as a pure irritant. Violent vomiting, accompanied with pain in the abdomen, and purging, are the symptoms which first make their appearance. These may be followed by symptoms which betoken collapse, viz. coldness of the limbs, paleness of the face, irregular pulse, and fainting.
Post-mortem Appearances.—Presence of inflammatory action.
Fatal Dose.—Uncertain.
Fatal Period.—Death has occurred in four hours.
Chemical Analysis.—Distinguished from oxalic acid by remaining fixed when heated on platinum foil.
In Solution:
1. Ammonia gives a white precipitate soluble in excess.
2. Ferrocyanide of Potassium, a white precipitate.
3. Sulphuretted Hydrogen or Ammonium Sulphide, a milky-white precipitate in a neutral pure solution.
4. Nitrate of Baryta, a white precipitate showing the presence of sulphuric acid.
5. Caustic potash or soda, a white precipitate soluble in excess.
In Organic Mixtures pass sulphuretted hydrogen, collect the sulphuret, and decompose it with boiling hydrochloric acid, then test for zinc.
Treatment.—Tea, coffee, milk, warm water, albumen, and in some cases enemata of gruel and other emollients.
The preparations of iron which are of importance are the sulphate and the muriate.
Sulphate of Iron
Copperas or Green Vitriol—has been administered as a poison, but more frequently to procure abortion. An ounce has been taken with no other serious effect than the production of violent pain, purging, and vomiting. Constant application of this substance to the body has produced vomiting, pains in the belly and limbs. These symptoms disappear on treatment.
Chemical Analysis.—(1) Hydrosulphuret of ammonia gives a black precipitate. (2) Ferrocyanide of potassium added to it, in solution, gives rise to a greenish-blue precipitate, becoming dark blue on exposure. (3) Chloride of barium will point to the nature of the acid present.
Muriate of Iron
Better known as the Tincture of Sesquichloride of Iron, or the Tinctura Ferri Perchloridi.—The tincture acts as a corrosive and irritant poison, death having followed in five weeks after an ounce and a half had been swallowed. It is sometimes used as an abortifacient. Recovery has, however, taken place after three ounces had [Pg 314] been swallowed. The symptoms present in most cases observed were those of a corrosive and irritant.
Chemical Analysis.—(1) The addition of nitrate of silver, causing a white precipitate insoluble in nitric acid, points to the presence of chlorine. (2) The peroxide of iron, indicated by the formation of Prussian blue on adding a solution of the ferrocyanide of potassium.
The preparations of this metal act as irritant poisons, death having occurred from a dose of two drachms of the sub-nitrate. Dr. Trail (Outlines of Medical Jurisprudence, p. 116) mentions the ease of a patient of his who took six drachms in three days in divided doses. The symptoms were vomiting, extreme pain in the abdomen and throat, a weak, feeble pulse, and much anxiety about the præcordia. Recovery took place. A case of severe vomiting during pregnancy, ending fatally, was mistaken for arsenic poisoning. The error arose from mistaking a greyish powder on the walls of the stomach for arsenic. It turned out on further inquiry that it was bismuth, given medicinally to prevent the vomiting. Bismuth carbonate mixed with gruel or bread and milk is given in large quantities for the purposes of radiography of the alimentary canal without any untoward effects.
Nitrate of Potash
This substance is well known as nitre, saltpetre, and sal prunella. In large doses it acts as an irritant, and cases are recorded in which it has been used to poison children. In one case, the presence of crystals of the salt in some of the dried vomited matter on the child‘s shoe, led to an explanation of the cause of death.
Symptoms.—Those of a pure irritant, to which death must be referred, and not to any constitutional action of the drug. The nervous symptoms, which are sometimes very marked, are, as is well known, common to the action of many pure irritants. In some cases there is suppression of urine.
Post-mortem Appearances.—Those produced by irritants generally.
Chemical Analysis.—Separate the poison by dialysis, evaporate, and test the crystals as directed under nitric acid.
Fatal Dose.—About an ounce.
Fatal Period.—Two hours.
Treatment.—The same as for other irritants; demulcent drinks. Promote vomiting.
Sulphate of Potash
Sal Polychrist, Sal de Duobus, or sulphate of potash, acts as an irritant poison, being largely used in France as an abortive. The symptoms and the post-mortem appearances are much [Pg 315] the same as those produced by the nitrate. A like treatment may also be adopted. In the detection of this substance, the nitrate of baryta will point to the acid present, and bichloride of platinum to the presence of potash.
Chlorate of Potash
This salt acts as a poison when taken in large doses, producing symptoms which might be mistaken for poisoning with arseniuretted hydrogen, or for such diseases as hæmoglobinuric fever.
Symptoms.—These comprise pain in the stomach and bowels with vomiting, collapse and stupor, cyanosis, jaundice; diminution of the urine, which contains hæmoglobin, casts, and albumen. It is a question whether the jaundice is hæmatogenous or hepatogenous. Chlorate of potash destroys the red corpuscles, the hæmoglobin is dissolved out and is set free in the liquor sanguinis.
Fatal Dose.—45-50 grains proved fatal to a child three years old. For an adult 390 grains to an ounce and a half.
Fatal Period.—From five hours to several days.
Treatment.—The stomach should be washed out through the syphon tube. Venæsection may be useful, with subsequent transfusion of fresh blood. The nephritis and other symptoms must be treated generally.
Post-mortem Appearances.—The mucous membrane of the stomach may be inflamed and submucous hæmorrhages may be found. The blood is chocolate in colour and gives the spectrum of methæmoglobin. The spleen is enlarged and chocolate-coloured, and the kidneys acutely inflamed.
Chemical Analysis.—Chlorate of potash may be separated from organic material by dialysis.
1. If to a solution of the salt a few drops of indigo sulphate be added, and then a few drops of strong sulphuric acid, the indigo-blue is bleached.
2. If a small crystal of the chlorate be heated in a test tube with a drop of strong sulphuric acid, it explodes with detonation.
The chloride, nitrate, and carbonate of barium are all irritant poisons. But besides their irritant action, the salts of barium also appear to act on the nervous system and the heart, arresting its action in systole. The symptoms, post-mortem appearances, and treatment are the same as for the other irritant poisons. Sulphate of magnesia, or other soluble sulphate, should be given to form an insoluble sulphate of baryta. Sulphate of barium is also used like bismuth carbonate for radiography.
Chemical Analysis.—Sulphuric acid or alkaline sulphate gives a white precipitate with solution of chloride of baryta, insoluble in nitric acid. The salts impart to flame a greenish-yellow colour. The chlorine is detected by nitrate of silver. Dissolve the carbonate in hydrochloric acid, and test as above. [Pg 316]
Two compounds of this metal are largely used in the arts for dyeing purposes—the neutral chromate and the acid bichromate of potash. The bichromate of potash is a powerful poison, and death may occur from its direct action on the nervous system, without the development of any of the signs of irritation; in other cases, however, well-marked irritant symptoms have been present. Applied externally, it produces deep fistulous sores, especially on the mucous membrane of the septum of the nose, in the workmen who are engaged in its manufacture. These sores are prevented to some extent by taking snuff. Dyers not infrequently suffer severely on their arms when using it in the course of their trade. Death has resulted in four hours after its administration.
Chemical Analysis.—A solution of the bichromate of potash, added to a solution of acetate of lead, gives a yellow precipitate; with nitrate of silver, a red. The salt boiled with hydrochloric or sulphuric acid and alcohol, gives a green liquid.
Treatment.—Emetics, magnesia, chalk, demulcent drinks, &c.
Mode of Action.—The general effects produced by the somewhat large class of vegetable irritants are—
1. Severe abdominal pain, accompanied with vomiting and purging.
2. Absence in most cases of any cerebral or nervous symptoms.
3. The irritant properties appear to reside in an acrid oil or resin. In colchicum, stavesacre, and some others, the presence of an alkaloid may account for their active properties.
4. In medicinal doses, the vegetable irritants act as safe purgatives.
5. The post-mortem appearances found in the alimentary canal betoken inflammation, the result of irritation.
6. Applied externally, they produce inflammation, pustular eruptions, and sometimes unhealthy callous sores.
The leaves and tops of this plant, Juniperus Sabina (N.O. Coniferæ), yield an acrid volatile oil, to the presence of which the poisonous properties are due. The oil is colourless or pale yellow, with a peculiar terebinthinate odour. It is used in medicine both internally and externally, and is supposed to possess emmenagogue properties. The dried powder is less active than the fresh tops. Savin is seldom used as a poison, more frequently to procure abortion. Its use for this purpose is mentioned in the old ballad of “Marie Hamilton”:
Symptoms.—Those of irritant poisoning. Violent pain in the abdomen, followed by vomiting, and in some cases salivation and strangury. Purging is not always present. When taken to procure abortion, death often takes place before the object for which it was taken is attained.
Post-mortem Appearances.—The stomach, gullet, and intestines are found congested and inflamed. The stomach may in places be seen corroded, and a green powder adherent to its coats. The powder washed and dried, and then rubbed, gives off the odour of savin. [Pg 318]
Chemical Analysis.—When an infusion or decoction of the leaves has been taken, chemical analysis is of no assistance. The oil may be separated from the contents of the stomach by subjecting them to distillation, and then shaking the distillate with ether, when the oil is dissolved out. On the evaporation of the ether, the oil is left for examination. When the powder is taken the contents of the stomach are not unlike green pea-soup. If a small portion of the green liquid be taken, and diluted with water, the green chlorophyll, being insoluble, will sink; but if the colour be due to bile, the liquid will remain of a uniform green colour. If a portion of the green matter be collected, dried, and then rubbed in a mortar, the characteristic odour of savin will be given off. The microscope may detect bits of the twigs.
The oil, on the addition of strong sulphuric acid, gives a brown colour. On diluting the coloured liquid with water, a dense white precipitate forms.
The oil expressed from the seeds of Croton tiglium (N.O. Euphorbiaceæ).
The seeds, when taken, produce violent pains in the stomach and purging. Pereira has described the case of a man who suffered severely from inhaling the dust of the seeds. The dose of the oil is from half a minim to a minim. Dr. Trail mentions the case of a delicate lady patient who took three drops for a dose without inconvenience. Dr. Adam records a case (Edinburgh Medical Journal, 1856) of a man who, in mistake, drank three drachms of a liniment containing about fifty drops of croton oil. After the most alarming symptoms, the patient ultimately recovered. Two drachms and a half have caused death (Journal de Clinic Médicale, 1839, p. 509). The poisonous properties depend upon the presence of a fatty acid.
A medical friend informed Husband that in Shetland six drops in as many colocynth pills have, in cases there, only produced “a comfortable ‘aisement’ of the bowels.” This is attributed to the dura ilia, resulting from a constant fish diet.
Symptoms.—Pain in the abdomen, vomiting, and purging, followed by exhaustion and collapse. In some cases, when the dose is large, the pain is hot and burning, and may be felt from the mouth downward.
Chemical Analysis.—Separate the oil from the contents of the stomach by means of ether, and then drive off the ether by means of heat. The oil then warmed with nitric acid becomes of a brown colour, and nitrous acid vapours are given off.
The poisonous properties of Colchicum autumnale, Meadow Saffron (N.O. Melanthaceæ) reside in an alkaloid Colchicine, chiefly found in the corms, but also present in other parts of the plant. The seeds have caused death. [Pg 319]
In June 1875 an epidemic of gastric irritation among the inhabitants of Rione Boego was traced to the use of the milk of goats which had accidentally eaten the leaves of colchicum.
Symptoms.—Colchicum, in medicinal doses, increases the activity of the liver, and bile is freely secreted. The action of the kidneys and of the skin is also increased. The heart is more or less affected, and its frequency diminished. In large doses, all the symptoms of irritant poisoning are present, and in some cases have been likened to those observed in Asiatic cholera.
Post-mortem Appearances.—Death may result from its use without leaving any morbid appearances. In other cases, however, the usual signs of inflammation were present. Casper describes the colour and condition of the blood in those poisoned by colchicum as dark cherry-red, with the consistency of treacle. A marked congestion of the vena cava may also be present.
Chemical Analysis.—Colchicine, obtained by Stas process, added to concentrated nitric acid, becomes of a violet colour, changing to blue and brown. The violet solution changes to yellow on dilution with water, then to red on adding caustic soda. Tincture of iodine precipitates colchicine of a kermes brown colour, platinum bichloride yellow, and tannic acid white, the precipitate being soluble in alcohol, acetic acid, and alkaline carbonates. Strong sulphuric acid gives a yellow colour with colchicine, which changes to green, violet, and reddish-brown on the addition of nitric acid.
Fatal Dose.—One ounce of the tincture.
Treatment.—Stimulants and opium should be given to counteract its depressing effects. Tannin is said to be an antidote.
Like savin, ergot is more frequently used to procure abortion than as a poison. When taken in a large dose it causes vomiting, purging, intense thirst, hurried breathing, and irregularity of the heart‘s action. Ergot appears to act powerfully on non-striated muscular fibre wherever it exists in the body; hence the vessels contract powerfully, and the peristaltic action of the intestinal canal is greatly increased. On the pregnant uterus its action is uncertain, as it does not appear to have any marked power in inducing labour, but on the parturient uterus its effects are most marked. A case is recorded in the Lancet (vol. ii. 1882) in which ergot had been taken for some time to procure abortion, but this end not being accomplished, the patient took “two hands full” of the powdered ergot to expedite matters, which caused the following fatal symptoms: There was some amount of jaundice, and the expression of the face was anxious. Occasionally fits of stupor occurred, and the general condition of the patient was maudlin, but there was no smell of alcohol in the breath; but during the course of the case, which ended fatally, a distinct etherish smell could be perceived. The pulse was so quick that it could not be counted, and it had also a peculiar jerky feeling under the finger. Attempts were made [Pg 320] to induce labour by passing a bougie-a-boule, but the patient died collapsed before delivery could be effected.
Where the drug has been taken for some time in the form of rye-bread made from the diseased grain, the symptoms in some cases are referable to the nervous system; in others, the blood appears to undergo certain changes; and hæmorrhages into the internal organs, as in the case just mentioned, have been frequently noticed. Gangrene of one or more of the extremities has also been known to occur. To chronic poisoning by this drug the term Ergotism has been applied, and may occur under two forms—the spasmodic and the gangrenous; the former marked by convulsions, giddiness, delirium, dimness of vision, and tetanic spasms; the latter, as a rule, by dry gangrene of the nose or extremities.
Chemical Analysis.—Ergot has a peculiar, slightly fishy odour, which is increased by rubbing up the powder with liquor potassæ and heating the mixture. At the same time it turns a reddish colour. The production of this odour, and the appearance under the microscope, are the only tests yet known for this substance in powder. From organic mixture it may be extracted with hot alcohol acidulated with sulphuric acid. The solution is red in colour, and shows two bands in the spectrum, one in the green, and a second, broader and more marked, in the blue.
Treatment.—Wash out the stomach, and give inhalations of amyl nitrite.
This plant, Helleborus niger—Black Hellebore—(N.O. Ranunculaceæ), known as the Christmas rose, is the melampodium of the old pharmacopœias. All parts of the plant are poisonous.
Symptoms.—Purging, vomiting, pain in the bowels, and cold sweats. Death is generally preceded by convulsions and insensibility.
Post-mortem Appearances.—Those common to the action of other irritants.
White Hellebore, Veratrum album (N.O. Melanthaceæ), acts very much in the same manner as the black hellebore, but is more powerful. The powder causes violent sneezing. The alkaloid Veratria appears to be the active principle. The symptoms and post-mortem appearances are analogous to those produced by black hellebore.
Gamboge is the gum resin of Garcinia Morella. It is an active ingredient in certain quack “vegetable pills.” One drachm has caused death by its irritant action. Owing to the imperfect pulverisation of gamboge in quack pills, they have caused violent irritation of the bowels, straining at stool, and prolapsus uteri, due to the irritating action of small pieces of this substance. [Pg 321]
Jalap, the powder obtained from the tubers of Exogonium Purga. The active properties of the drug reside in a resin. It is a drastic purgative; twelve grains have killed a dog.
Scammony is obtained from the dry root of Convolvulus Scammonia. Like the last mentioned, it is a powerful purgative, and may cause death if given in large doses to debilitated individuals.
The oil expressed, with or without the aid of heat, from the seeds of Ricinus communis. A girl, eighteen years of age, died in Liverpool in 1837 from eating a few of the castor-oil seeds.
Cuckoo-pint, Wake-robin, or Lords and Ladies, is one of the most acrid of indigenous vegetables. The active property of the plant appears to be lost by drying, and by distillation in water. Children have been poisoned by its leaves.
The twigs and fruit of Taxus baccata act as irritant poisons, producing also symptoms which point to cerebro-spinal mischief. A case is recorded of poisoning by yew leaves, in which only five grains of the leaves were found in the stomach; yet death took place within an hour from the time the symptoms commenced (British Medical Journal, 1876, vol. ii. p. 392). In the above-mentioned case, vomiting and other signs of gastric irritation were absent. The chief symptoms present were—pallor of the face, faintness, an almost imperceptible pulse, facial convulsions, foaming at the mouth, stertorous breathing, loss of consciousness, ending in death. The symptoms are due to an alkaloid toxin. Several children have died after eating the fruit. Post-mortem signs of irritation of the alimentary canal.
Cytisus Laburnum, or common Laburnum, the seeds, bark, and wood of which are poisonous. They contain a narcotico-acrid, crystallisable alkaloid—Cytisine—producing vomiting, foaming at the mouth, convulsions, and insensibility. Recovery took place in two cases mentioned by Trail, from the use of emetics and ammonia.
Æthusa Cynapium has been mistaken for parsley. Nausea, vomiting, giddiness, and severe abdominal pains are among the most common symptoms of poisoning by this plant. [Pg 322]
Two plants are included under this name, Bryonia dioica, white bryony (N.O. Cucurbitaceæ), the only indigenous cucurbitaceous plant, and the Tamus communis, black bryony (N.O. Dioscoreaceæ). Both the bryonia dioica and the tamus communis possess active irritant properties. They are of importance from the fact of their growing wild, and the possibility of the fruit being eaten by children.
Elaterium, the inspissated juice of Ecballium officinarum, or Squirting Cucumber. It is a powerful drastic purgative, one grain having given rise to alarming symptoms in man.
ANIMAL IRRITANTS
Cantharides—Cantharis vesicatoria (N.O. Coleoptera)—is seldom given as a poison, but is most frequently employed to procure abortion, or for its supposed aphrodisiac properties.
Cantharides is a pure irritant. Applied externally, it produces vesication; and if absorbed, strangury.
Cantharidine—the active principle of Cantharides—is insoluble in water and bisulphide of carbon. It is but slightly soluble in alcohol, but it is dissolved by chloroform, ether, and some oils. Four parts of cantharidine have been procured from a thousand parts of the flies.
Symptoms.—An acrid taste is first experienced in the mouth, followed by a burning heat in the throat, stomach, and abdomen. There is constant vomiting of bloody mucus, and the stools also contain blood. The patient complains of intense thirst, pains in the loins, and an incessant desire to void urine, which is frequently mixed with blood. Salivation in some cases is a prominent symptom. Strangury may result from the external application of cantharides as a blister, &c. Priapism is often obstinate and painful, and the fatal termination is generally ushered in by violent convulsions and delirium. In pregnant women, abortion may take place as a result of the general irritation and disturbance of the system, there being no proof that the uterus is particularly affected by the drug. The vomited matters may contain shining green particles, the presence of which indicates the nature of the poison taken. The invasion of the symptoms may in some cases be retarded.
Post-mortem Appearances.—Those of powerful irritation. The mucous membrane of the whole alimentary canal, from the mouth to the rectum, has been found in a state of acute inflammation. The uterus, kidneys, and internal organs of generation share also in the general irritation, ulceration of the bladder having been met with in some cases. Portions of the wings and elytra are sometimes found adhering to the coats of the stomach. [Pg 323]
Fatal Dose.—One ounce of the tincture has caused death in fourteen days. This is perhaps the smallest fatal dose on record. Six ounces have been stated to have produced no dangerous symptoms. The worthlessness of the preparation may account for this result.
Treatment.—Vomiting should be promoted and warm mucilaginous drinks given. If vomiting be absent, emetics should be administered. Oil should not be given, as it dissolves out the active principle. Opium may be given with advantage.
Chemical Analysis.—The contents of the stomach should be concentrated and then treated with chloroform, filtered, and the filtrate allowed to spontaneously evaporate. A portion of the residue should then be placed on the skin, and the presence or absence of vesication noticed. Examined under the microscope, portions of the wing-cases may be detected. No change of colour is produced in cantharidine by the action of sulphuric or nitric acid, thus distinguishing this substance from any of the vegetable alkaloids.
The processes by which complex and highly organised substances are broken up into their primary elements are largely synthetical. The putrefactive processes brought about by the action of bacteria result in the formation of special products, some of which combine with certain mineral and vegetable acids to form definite chemical salts; in this respect they correspond with inorganic and organic bases. These products are called ptomaines, a name suggested by an Italian toxicologist, Selmi, and it is derived from the Greek word πτῶμα, a cadaver or corpse.
On account of their basic properties, resembling the vegetable alkaloids, they are called putrefactive or bacterial alkaloids. They have been called animal alkaloids, but some ptomaines may be produced by the action of bacteria upon vegetable proteids; so this term is not strictly applicable, and should be restricted to those basic bodies or “leucomaines” that result from metabolism of the tissues in the animal body.
The essential element of their basic nature is nitrogen, and in this they resemble the vegetable alkaloids. Some contain oxygen, like the fixed alkaloids, while others do not, like the volatile alkaloids nicotine and conine. The kind of ptomaine formed depends upon the nature of the bacterium, the material upon which, and the conditions under which, it grows; the amount of oxygen present; the temperature and the period of growth. All ptomaines are not necessarily poisonous. Albumin is the origin from which all alkaloids, vegetable or animal, are derived. The following is a list of the principal ptomaines: [Pg 324]
Methylamine, CH₃NH₂.—Found in herring brine and decomposing fish—non-poisonous.
Dimethylamine, (CH₃)₂NH₂.—From putrefying gelatine, yeast, fish, and sausage—non-poisonous.
Trimethylamine, (CH₃)₃N.—Various decomposing animal and vegetable tissues, ergot—poisonous in large quantities.
Ethylamine, C₂H₅NH₂.—Beet-sugar, wheat-flour—non-poisonous.
Diethylamine, (C₂H₅)₂NH₂.—Putrid fish and sausage—non-poisonous.
Triethylamine, (C₂H₅)₃N.—Putrid fish and sausage—non-poisonous.
Propylamine, C₃H₇NH₂.—From cultures of bacteria of fæces—non-poisonous.
Butylamine, C₄H₁₁N.—From cod-liver oil. Diaphoretic and diuretic—in large doses causes vomiting and stupor.
Iso-amylamine, (CH₃)₂·CH·CH₂CH₂NH₂.—Decomposing yeast and cod-liver oil—active poison, causes convulsions and death.
Caproylamine, C₆H₁₅N.—Called septicin by Hager.
Collodine, C₈H₁₁N.—The first ptomaine obtained in a chemically pure condition—from putrid horse flesh, pancreas, gelatine, and mackerel.
Hydrocollodine, C₈H₁₃N.—Putrefying horse flesh and mackerel—highly poisonous.
Parvoline, C₉H₁₃N.—Putrid horse flesh and mackerel.
Unnamed base, C₁₀H₁₅N.—From decomposing fibrin and jelly-fish. Like curare in its action.
Putrescine, C₄H₁₂N₁₂.—From human corpses—feebly poisonous.
Cadaverine, C₅H₁₆N₂.—From human corpses—causes suppuration.
Neuridine, C₅H₁₄N₂.—Common product of putrefaction—quite inert.
Neurine, C₅H₁₃NO.—From human corpses, intensely poisonous—resembles muscarin in its action.
Choline, C₅H₁₅NO₂.—From putrefying animal and vegetable substances—feebly poisonous; by giving up one molecule of water it changes to neurine—this may be brought about by bacteria or chemical agencies.
Muscarine, C₅H₁₃NO₂.—From putrid fish and horse flesh. The active principle of poisonous mushroom.
Gadinine, C₇H₁₆NO₂.—From putrefying codfish, haddock, and gelatine, in pure cultures of proteus vulgaris—poisonous in large quantities.
A Base (?), C₇H₁₇NO₂.—From decomposing horse flesh—its action is like curare: causes loss of temperature, rigors, convulsions, and general paralysis: the heart stops in diastole.
Mydaleine.—Composition not determined—from human corpses—actively poisonous.
Even after prolonged periods and with access of air, any putrefactive alkaloids which may form do so in very small quantities, and they are very unstable. In their chemical reactions they respond to many of the group-tests used for alkaloids, but they differ in their reaction to the special tests used for vegetable alkaloids. There is no test that will differentiate between putrefactive and vegetable alkaloids, as a class; at the same time no putrefactive alkaloid will give the same chemical reactions, and have the same physiological properties, as any one of the vegetable alkaloids.
Neurine was first obtained by Liebreich by boiling protagon with concentrated baryta. Since then it has been extracted from putrefying animal tissues. The free base is strongly alkaline, and gives a white cloud with the vapour of hydrochloric acid. It is intensely poisonous, resembling muscarine in its action. Very small quantities cause complete paralysis in frogs. Respiration ceases first, and the heart beats become more and more feeble, until it stops in diastole. If atropine be now injected the heart begins to beat again. [Pg 325]
As a defence set up in cases of poisoning, when one or other of the rarer alkaloids has been used, it has been suggested that the poison discovered in the body of the deceased was due to the processes of putrefaction of the tissues themselves. In view of this it is important to know the toxic power of such putrefactive alkaloids as may be found in the human cadaver.
Two only of these are actively poisonous—neurine and mydaleine; others are toxic in so small a degree that large amounts would be required to produce lethal effects, far more in proportion to the body weight than any vegetable alkaloid for which it may be alleged they have been mistaken.
Neurine does not appear before the fifth or sixth day after death, mydaleine not until the seventh day, and only in traces; it does not appear in amount sufficient for quantitative analysis until the end of the second or third week.
At the period after death when a medico-legal analysis has generally to be made, choline is the only alkaloid present, and it is but feebly poisonous.
In rabbits neurine causes marked salivation and increased flow of secretion from the eyes and nose. The heart beats more quickly at first, but gradually slows down and stops in diastole. There is increased peristalsis of the intestines with profuse diarrhœa. There is narrowing of the pupil both after injection or local installation. Clonic spasms and violent convulsions occur, and are followed by paralysis first of the hind then of the fore legs, ending in death. The symptoms are prevented or relieved by atropine.
If atropine be injected first the poisonous effects of the neurine do not show themselves.
Mydaleine was discovered by Brieger in putrefying cadaveric organs. Small doses injected into guinea-pigs cause profuse lachrymation and coryza.
The pupils dilate and then become motionless. The temperature rises from 1° to 2° Centigrade. There is somnolence at this stage, with increased intestinal peristalsis. The pulse and respirations are quickened; later these with the temperature return to the normal, and the animal recovers. Large doses cause death with the heart in diastole and the intestines contracted.
Clonic spasms and stupor precede death.
The Extraction of putrefactive alkaloids from organic matters may be carried out by the process for alkaloid extraction (vide p. 335 et seq.).
Amongst the attempts made to distinguish the putrefactive from vegetable alkaloids by chemical reactions one method was based on the rapid reduction of potassium ferricyanide to the ferrocyanide. After converting the alkaloid to a sulphate, a solution of it is mixed with a drop of potassium ferricyanide and a drop of ferric chloride added: the deep blue colour of Prussian blue is produced if reduction to the ferrocyanide has taken place. However, certain vegetable alkaloids, viz. morphine, aconitine, eserine, and hyoscyamine act rapidly as reducing agents upon the ferricyanide. Emetine, igasurine, nicotine, [Pg 326] colchicine act less rapidly. Brieger considers that when the reaction occurs with putrefactive alkaloids it is due to impurities present in them. Brouardel and Boutmy have suggested making use of the action of alkaloids upon photographic silver bromide paper as a means of distinction. The paper is written upon with a solution of the alkaloid and kept light free for half an hour; it is then fixed in a solution of sodium hyposulphite and washed in water. The putrefactive alkaloids are said to reduce and blacken the silver compound, while the vegetable alkaloids do not. Neither of these processes is to be relied upon for medico-legal purposes.
Leucomaines or animal alkaloids are basic substances which originate from the metabolic processes taking place in the animal body. They closely resemble the vegetable alkaloids, and some are found in plants as well as animals. It is probable that some of them may have originated primarily from the putrefactive processes in the intestines and been absorbed into the system. The following is a list of the principal leucomaines resulting from the metabolism of the tissues of the animal body:
Adenin, C₅H₅N₅.—From thymus gland, from all tissues animal or vegetable which are rich in nucleinic acid—poisonous in large doses.
Sarkine or hypoxanthine, C₅H₄N₄O.—From urine and flesh—causes increased reflex excitability and convulsive seizures.
Guanine, C₅H₅N₅O.—From flesh and guano—it is inert.
Xanthine, C₅H₅N₄O₂.—From flesh and urine—acts as a muscle stimulant.
Heteroxanthine, C₆H₆N₄O₃.—From urine.
Methylxanthine, C₆H₆N₄O₂.—From urine.
Paraxanthine, C₇H₈N₄O₂.—From urine—destroys spontaneous muscular action, lessens reflex excitability.
Carnine, C₇H₈N₄O₃.—From fresh meat.
Gerotine, C₅H₁₄N₂.—From liver and kidneys, an isomer of cadaverine—exerts a paralysing action upon the nerve centres and cardiac ganglia.
Spermin, C₂H₅N.—From semen, testicles, ovaries, breast, thyroid, pancreas, and spleen, normal bone marrow. Poehl states that it has a tonic effect on the nervous system.
Creatinine, C₄H₇N₃O.—From urine.
Crusocreatinine, C₅H₈N₄O.—From fresh meat.
Xanthocreatinine, C₅H₁₀N₄O.—From fresh meat—causes depression, fatigue, somnolence, defæcation, and vomiting.
Betaine, C₅H₁₁NO₂.—From urine.
Mytilotoxine, C₆H₁₅NO₂.—From poisonous mussels.
The Relation of Leucomaines
to Disease
It will be necessary in considering the relation of leucomaines to disease to give the term a wider significance than that relative to the chemistry of these bodies. Autogenous diseases may be looked upon as having their origin in altered metabolism of the tissue cells, apart from the introduction of foreign cells or poisons. “It is certainly true that if we should drink only chemically pure water, take only that [Pg 327] food which is free from all adulteration and infection, and breathe the purest air free from all organic matter living and dead, yet our excretions would contain poisons. It is true that the excretions of all living things, plants, and animals contain substances which are poisonous to the organisms excreting them” (Vaughan). Bouchard estimates that the amount of a certain poison formed in the intestines of a healthy man in twenty-four hours, if absorbed, would prove fatal. Unless free elimination takes place, elevation of temperature may follow.
The products of imperfect digestion, if absorbed, may give rise to serious disturbances. Hildebrandt has shown by his experiments that subcutaneous injection of pepsin into dogs is followed by elevation of body temperature, which he calls “ferment fever.” The fever reaches a maximum within a few hours and may last several days. Rigors are frequent. The animals suffer from trembling in the limbs, uncertainty of gait, vomiting, dyspnœa, and coma followed by death. On post-mortem examination there are found degeneration of the heart, muscles, liver, and kidneys, abundant hæmorrhages into the intestine, Peyer‘s patches, the mesenteric glands, and occasionally into the lungs. The blood is at first lessened in coagulability, afterwards increased, and thrombi formed which have been found in the lungs and kidneys.
Excessive formation of these poisonous substances within the body or insufficient elimination of them produces serious disturbances. Fatigue fever is an example. A considerable rise of temperature may follow excessive and prolonged exercise, the appetite is impaired, and insomnia is present from excitation of the brain and the senses being rendered more acute. There may be rigors simulating malaria. This fatigue fever occurs particularly amongst recruits in armies subjected to prolonged marching. From his observations of this disease in the Italian army, Mosso states that it is due to the absorption of poisonous substances into the blood from the tissues, which, if injected into the circulation of healthy animals, produces symptoms of exhaustion. The fever of prostration or exhaustion is similar but less in degree, it is more likely to be produced by prolonged exertion with insufficient food, it may resemble typhus fever, delirium may be present, and loss of muscular control over the bowels; death may result. In non-fatal cases weeks may elapse before recovery takes place.
Rachford has pointed out that an excess of paraxanthine in the blood is followed by migraine, and it may give rise to epileptic seizures, gastric neurosis, and asthma; and by injecting paraxanthine into the blood of mice and rats he has produced symptoms of certain forms of epilepsy, and others similar to the nervous symptoms of chronic lead poisoning.
Instances have occurred from time to time of serious illness attacking individuals either separately or collectively shortly after the ingestion of food. The food may be rendered poisonous in the following ways:
1. A poisonous substance may have been added to it, intentionally or accidentally.
2. Grain may become infected with poisonous fungi, e.g. ergot.
3. Plants or animals may feed upon materials harmless to them, but which render them poisonous to man—birds that have fed on mountain laurel are said to have proved poisonous to man.
4. During periods of physiological activity of certain of their glands, the flesh of some animals becomes poisonous to man; some fish, for example, are poisonous during the spawning season.
5. Food may carry infection by contamination with germs, e.g. typhoid bacilli in milk.
6. The animal may suffer from a specific disease, and it may be transmitted to man, e.g. tuberculosis.
7. Foods may be contaminated with bacteria which produce poisons either before or after the food has been eaten.
8. The food may be infected with parasites or their ova, and which develop in the individual who partakes of it, e.g. trichiniasis.
In cases in which the poison has been added or preformed, the symptoms of poisoning come on almost immediately or within a short space of time; there may, however, in the latter, be a delay in the appearance of the symptoms in instances where the bacterial poison is formed subsequent to the ingestion of the food. This delay is bordering on the nature of a true infection. In those cases when the bacteria have been present in the animal before, or develop in it subsequent to its death, and which develop in the person who eats it as food, symptoms may not come on for some time; the condition is a true infection, and there may be an incubation period over six or seven days.
Apart from those cases of poisoning following the ingestion of food to which poison has been added, or from meat affected by parasitic disease, there have occurred outbreaks of serious illness following the partaking of meat. Vaughan, in the Twentieth Century Practice of [Pg 329] Medicine, vol. xiii. p. 20, holds that “there can scarcely be any difference of opinion on the following points: (1) With fresh food to act upon and with normal gastric juice to act, the process of peptic digestion proceeds without the formation of any harmful substance. (2) With putrid food, containing poisons to start with, the most active digestion does not guarantee the destruction of those poisons. (3) With even the best of food, peptic digestion may proceed so slowly and imperfectly that during the process poisons may be formed by bacterial agencies.” During the process of decomposition of meat and other albuminous foods by bacterial agency, certain poisonous substances are formed prior to the production of the ptomaines or bacterial alkaloids. These are known as toxalbumoses and enzymes; they are unstable bodies, they cannot be obtained in a crystalline form, and their composition is not fully understood. They give certain reactions with a few group reagents, but they are recognised only by their effects upon living animals. As decomposition advances the more stable alkaloids are formed, but those which are poisonous, like the toxalbumoses, are readily converted by further processes of putrefaction or by chemical means into innocuous bodies. Toxins is the general term used in toxicology for these poisonous substances formed from animal tissues.
It is not necessary that complete putrefaction should have taken place for meat to prove poisonous. In fact many of the severest cases are those in which it has not fully putrefied. The most poisonous toxins are present during the early stages of decomposition, and the changes are not recognisable by the senses—smell or taste—which would ensure the rejection of the meat as food.
The poisonous effects are rarely due to the ingestion of bacterial products alone; those cases in which no bacteriological investigation of the food has been made cannot be taken into consideration. The toxalbumoses are destroyed by a few minutes‘ exposure to a temperature at boiling-point, 212° F. (Durham, B. M. J., 1898, vol. ii. p. 797).
In reference to the toxic action of the alkaloids, these have been noted only from the results following subcutaneous injection; their effects when taken per orem have not been established by experiment. In all instances where the necessary bacteriological investigation has been properly carried out a true infection has been proved to have taken place.
In cases of meat poisoning the principal bacteria concerned are not the ordinary putrefactive organisms. The Bacillus enteritidis of Gärtner, which has been found associated with twelve epidemics, and the Bacillus botulinus of Ermengem are the most important causative agents.
The Bacillus enteritidis is killed by proper cooking. It is destroyed in one minute at a temperature of 180° F. At 41° F. it will not grow, but, in meat kept at 68° F. for seventy-two hours, it flourishes abundantly. Freezing will not kill it. In meat which has been infected with the bacilli post-mortem they do not penetrate the meat more [Pg 330] than 1 cm. in ten days. Roasting or boiling will sterilise it. In those instances in which poisoning has taken place after cooking, the bacilli have either been present in the meat beforehand, and the temperature has not been sufficiently high or the cooking sufficiently prolonged, to ensure their destruction in the deepest portions; or the meat after cooking has become contaminated, and been insufficiently warmed up again after keeping it for a day or so. Exposure to sewer gas will not affect meat and contaminate it with the Bacillus enteritidis. The chief symptoms due to the Bacillus enteritidis are vomiting and diarrhœa, herpes labialis, rashes on the skin followed by desquamation in about fourteen days, jaundice, and great thirst. The onset is sudden, with nausea, headache, pains in the back and limbs, rigors, fever lasting a few days, general weakness, and, in cases which recover, convalescence extending over a period of from three to six weeks.
The symptoms of botulismus, due to the Bacillus botulinus of Ermengem, and associated with sausage poisoning, are, as a rule, dryness of the mouth, constriction of the fauces, nausea, vomiting, purgation, vertigo, dilatation of the pupils, with dimness of vision and diplopia, and a sense of suffocation. Marked muscular weakness and nervous prostration are prominent symptoms. In fatal cases there is weakness of the pulse and cyanosis, with coldness of the surface and perspiration. The temperature is raised at first and may reach 103° F., but ultimately falls below normal. Delirium comes on late, followed by coma and death.
In dangerous cases obstinate constipation may follow after a few hours of watery stools.
On post-mortem examination of the bodies in fatal cases the following appearances have been noted: a white, dried, parchment condition of the mouth, fauces, throat, and gullet; hyperæmia of the mucous membrane of the stomach and intestines with submucous extravasations of blood. The abdominal and thoracic viscera have been found engorged with blood, with enlargement of the spleen; the former are due to failure of the heart, and cannot be regarded as characteristic of sausage poisoning. Some stress has been laid on the observation that putrefaction is unusually delayed, but Müller has shown that no reliance can be placed upon it; he says that in forty-eight autopsies it has been noted that in eleven of them putrefaction had developed rapidly.
The symptoms of meat poisoning are grouped by Dixon Mann into two divisions: (1) those due to a true infection, (2) those due to simple poisoning.
In (1) the symptoms are those of an infectious disease—they include headache, anorexia, rigors, constipation followed by diarrhœa, pains in the back and limbs, photophobia, delirium, skin eruptions, meteorism, and enlargement of the spleen. The post-mortem appearances greatly resemble those of enterica—infiltration, ulceration, and sloughing of Peyer‘s patches; hæmorrhage into the bowels, enlargement of the spleen, with possibly some pus depots. [Pg 331]
In (2) the symptoms are those of acute gastro-enteritis—violent vomiting, purging, prostration, cramps in the legs, and collapse; the temperature is generally subnormal, but may be elevated. The post-mortem appearances are those produced by gastro-enteritis, with hæmorrhages into the intestinal mucous membrane; the spleen is frequently enlarged, and Peyer‘s patches may be infiltrated.
Meat poisoning has usually been most frequently associated with the ingestion of pork, veal, beef, meat pies, potted meat, tinned meat, sausages, and brawn. The more finely divided the meat, the more easily and completely it may become infected and poisonous. Cases of poisoning from the ingestion of canned meats are not uncommon. In some instances they may be due to metallic poisoning, in the great majority they are due to putrefactive changes having taken place in the meat. Ungefug reports a case confirmed by the celebrated chemist Heinrich Rose, in which sulphate of zinc had been used as a preservative instead of saltpetre. In some the canning may have been imperfect, and putrefaction taken place before reaching the consumer; in others decomposition may have begun after opening the can. The meat may have been taken from diseased animals, or decomposed prior to canning.
Poisoning by tinned provisions with the metal used for tinning is more likely to occur with fruits than meat. The malic acid of the juice probably dissolves the solder and forms a malate of tin. Cherries, apples, pineapples, and tomatoes are the most likely to do this.
In 1890 Luff investigated four cases of tin poisoning due to the consumption of tinned cherries. Some of the material left was analysed, and the juice contained malate of tin in solution equivalent to two grains of the higher oxide of tin per fluid ounce. It was estimated that the symptoms were produced by doses of two to four grains of malate of tin. Two of the patients nearly died from the diarrhœa and collapse.
Sulphate of copper is used to give a full green colour to peas, olives, and pickles, or it may contaminate preserved fruits if they be left in copper vessels. The copper combines with the phyllocyanic acid of the chlorophyll, and although insoluble in the surrounding liquor, is set free and absorbed by the process of digestion.
Fish may cause poisoning in two ways: in one the poison is a physiological product of certain glands of the animal, and is quite independent of bacteria; the other is due to the poisonous products of bacterial growth. The fish that are inherently poisonous as a rule occupy tropical waters: several of them exist in Japanese waters. Mackerel, carp, barbel, and herrings may become poisonous at times; some of these, especially mackerel, may rapidly become unfit for food [Pg 332] after they are dead. Caviare and the roe of herrings have caused poisoning. Shell-fish, especially mussels, also may prove poisonous.
The symptoms of fish and shell-fish poisoning are variable. In some cases disturbance of the nervous system predominates, with delirium, convulsions, and paralysis. There may be dryness and constriction of the throat, dyspnœa, disturbed vision, vertigo, jerky speech or aphonia, rapid pulse, loss of co-ordination, numbness, formication, coldness of the limbs, dilated pupils, paralysis, and collapse, followed by death in a few hours. Other cases exhibit symptoms of severe gastro-intestinal irritation, with nausea, vomiting, pain, tenesmus, mucous and bloody stools; in the most dangerous cases the bowels are constipated. Cases exhibiting the nervous type of symptoms resemble poisoning by atropine, and an alkaloid—ptomatropine—is regarded as the cause. It has never been obtained in the pure state, and nothing is known of its composition. It must not be mistaken, in toxicological examination, for atropine; its presence can only be recognised by its action on the pupil.
Many cases of fish poisoning are accompanied by erythema, urticaria, and severe itching of the skin. In probably all cases there is an elevation of the body temperature.
Tinned fish has caused poisoning on many occasions. In one case of tinned salmon poisoning, which proved fatal, parts of the stomach and intestines were almost gangrenous from the intensity of the inflammation.
Stevenson (Brit. Med. Journ., 1892) records a case of sardine poisoning which proved fatal, and in which the tissues post-mortem were found to be emphysematous. He extracted an alkaloid from some of the sardines, and the stomach contents; it was highly toxic and proved fatal to rats.
It is most probable in poisoning by tinned fish that the contents of the tins have become contaminated with bacteria before being sealed up.
Shell-fish may become contaminated with bacteria and cause true infections in people who eat them. Typhoid fever has been carried in this way by oysters, and probably cockles. The fish may develop toxins and prove poisonous, and as an example of this mussels produce a powerful toxin—mytilotoxine—while they are alive, which gives rise to a serious illness termed mytilotoxismus. There are three quite different classes of symptoms induced by poisonous mussels. In one the symptoms are principally those of acute gastro-enteritis; in another skin eruptions are the principal feature; and the third is known as mytilotoxismus paralyticus, in which there is great disturbance of the cerebro-spinal nervous system, with paralysis. The two former groups of symptoms are due to putrefactive processes in the mussels, but the third or paralytic group is due to the alkaloid mytilotoxine, which is not a product of putrefaction, as it is not found in mussels that have been allowed to decay.
There is nothing to evidence the idea that mussels absorb metallic poisons—e.g. copper—from the bottoms of vessels. [Pg 333]
The term milk poisoning or galactotoxismus is used here to indicate the results following the drinking of milk infected with saprophytic toxicogenic bacteria, and which are mainly responsible for the high mortality from “summer diarrhœas” of artificially-fed infants. One of the products of these bacterial infections of milk is the alkaloid tyrotoxicon. It has been isolated by Vaughan from cheese, and has also been found in ice-cream, frozen custards, and cream puffs. Vaughan, however, asserts that it is not the one most frequently present, nor is it the most actively poisonous. There are others which he considers are poisonous albumins (Vaughan, Twentieth Cent. Pract. Med., vol. xiii.).
The symptoms of poisoning by tyrotoxicon are mainly those of acute gastro-enteritis, and comprise constriction of the fauces, nausea and vomiting, sharp griping intestinal pains, headache, thoracic oppression, chilliness, dizziness, and purging. In severe forms exhaustion, subnormal temperature, coma, collapse, and death may follow.
This disease is due to the introduction of the Trichina spiralis into the human body. The encysted worm is found embedded in the fibres of all the striped muscles of the trunk and limbs, and even in the heart, where it appears in the form of white ovoid bodies or capsules, the capsules being sometimes calcareous. The worm passes the greater part of its existence in the chrysalis state in the muscular system of one animal, and only reaches its mature condition in the stomach of another. Virchow and Zenker assert that the trichina not only frequently presents itself in the human organism, but that this organism is most favourable for its full development. Once in the stomach, the period of incubation is about three to eight days, and then propagation rapidly begins and continues, so that Dr. Kellen estimates that in about seven days after the ingestion of half a pound of meat the stomach and intestines may contain thirty millions of the worms. The worms when introduced into the stomach leave their capsules, become free, produce young, and these leave the stomach through its coats for the muscles, where they become encysted. The trichina is most frequently found in pork, seldom in sheep, horses, or oxen—the last being the most free.
Symptoms.—Intestinal irritation, loss of appetite, sickness, malaise, general weakness of the limbs, and diarrhœa. The eyelids swell as well as the joints, the skin is bathed in cold, clammy sweat, and a low form of fever sets in. Death may be due to peritonitis, paralysis of the muscles—the result of their destruction—or to irritative fever. During the perforation of the coats of the stomach and bowels by the worms, the mucous membrane becomes inflamed, pus is formed on the surface, and the stools become bloody. [Pg 334]
Under this head may be classed all those effects produced by the sting or bite of various insects and reptiles, and also by the bite of the mad dog and wolf.
No medico-legal question is likely to be raised on this subject, at least in this country, where, with the exception of the common viper or adder, all our reptiles are harmless enough.
Vegetable alkaloids may be classified in three groups: (1) derivatives of pyridine, e.g. atropine, conine; (2) derivatives of quinoline, e.g. cinchonine, narcotine; (3) substituted amines and amides. The majority of the vegetable alkaloids belong to the first two groups. They are for the most part solid, crystalline, and colourless; a few, such as conine, nicotine, and pilocarpin, are liquid. They combine with acids to form salts, and the salts are more soluble in water than the free alkaloid. Alkaloids possess certain properties in common, amongst which is that of being precipitated from their solutions by certain reagents, which are called alkaloidal grouping reagents. Some are precipitated by all the group reagents, others only by a few.
1. Iodine dissolved in solution of Potassium Iodide—Wagner‘s reagent.—Gives a reddish-brown precipitate with most alkaloids.
2. Phosphomolybdic Acid—Sonnenschein‘s reagent.—Made by dissolving phosphomolybdate of soda in water containing one-tenth its volume of strong nitric acid. It gives a yellow precipitate with most of the alkaloids; it also precipitates ammonium salts and ammonia derivatives, also salts of lead, silver, and mercury unless there be sufficient acid to keep them in solution.
3. Potassio-mercuric Iodide—Mayer‘s reagent.—Made by adding a solution of potassium iodide to one of mercuric chloride until the red precipitate first formed be just dissolved. This solution precipitates most of the alkaloids. The solution to be tested must contain acetic acid.
4. Phosphotungstic Acid—Scheibler‘s reagent.—This acts in a manner very similar to phosphomolybdic acid.
There are several methods recommended for the isolation and detection of the vegetable alkaloids, and their separation from the contents of the stomach or from the membranes and tissues of the body. The process, however, most generally pursued is that of Stas, which may be briefly described as follows:
(a) The substance to be examined is mixed with twice its weight of absolute alcohol, to which from ten to thirty grains of tartaric or oxalic acid—preferably the former—have been added, and the mixture subjected to gentle heat in a flask, 70° to 75° C., or 158° to 167° F. [Pg 336]
(b) If the membranes or organs have to be examined, they are finely divided, treated with absolute alcohol, squeezed, and again treated with fresh alcohol as in (a).
In either case, the mixture, when quite cold, is filtered, and the alcoholic solution is concentrated by evaporation, either in vacuo or in a current of air not exceeding 95° F. or 35° C.
The liquid residue is now passed through a moistened filter, which separates the fat and other insoluble matters. The filtrate is evaporated to dryness over sulphuric acid or in vacuo, and the acid residue of this evaporation dissolved in the smallest possible quantity of distilled water. The acid liquid is then gradually neutralised with the bicarbonate of potash or soda until effervescence ceases, and afterwards shaken in a flask with four or five times its bulk of pure ether, and allowed to settle. When the ether has become quite clear, a small portion of it is decanted into a small glass capsule, and allowed to spontaneously evaporate in a dry place. If during evaporation streaks of liquid appear on the side of the capsule, running together at the bottom, a liquid volatile alkaloid is probably present. If none of these manifestations occur, the alkaloid is in all probability solid and non-volatile.
| The Alkaloid is Volatile. |
The Alkaloid is Non-Volatile. |
|---|---|
| To the original mixture in a flask | To the original mixture in a |
| add a moderate quantity of a strong | flask add strong caustic potash or |
| solution of caustic potash or soda, | soda solution, and agitate with |
| mixed with ether; agitate, and allow | successive portions of pure ether |
| the mixture to settle. Pour off the | allowing it to completely settle |
| ethereal solution, and re-shake | each time. The ethereal solutions, |
| residue with a fresh quantity of | being mixed, are evaporated, leaving |
| ether; decant, and mix both solutions. | the alkaloid in an impure state. |
| The ethereal solution is now shaken | To purify it, the solid residue left |
| with a mixture of four parts of water | on evaporation is treated with a |
| and one of sulphuric acid, which | small quantity of dilute sulphuric |
| withdraws the alkaloid from its | acid, which dissolves the alkaloid, |
| solution, leaving any fatty matter | leaving any fatty impurities behind. |
| dissolved in the ether. The acid | The acid liquid is evaporated to |
| solution is now mixed with strong | three-quarters of its bulk over |
| potash or soda solution in excess,[20] | strong sulphuric acid, and then a |
| agitated with ether, the ether poured | saturated solution of carbonate of |
| off, and then evaporated at as low | potash or soda added. The absolute |
| a temperature as possible,[21] | alcohol will then dissolve out the |
| leaving the pure alkaloid with all its | pure alkaloid, giving it, on in the |
| characteristic chemical and | crystalline form, and in evaporation, |
| physical properties. | a state to show its characteristic |
| reactions. |
If morphine has to be sought for, the liquid should be shaken with ether immediately after being neutralised with carbonate of sodium, and [Pg 337] the ether poured off as quickly as possible; for if the alkaloid have time to separate in the crystalline form, scarcely any of it is dissolved by the ether (Otto).
The method of Stas is based upon the fact that the salts of the alkaloids, as a class, are soluble in water and alcohol, but are insoluble in ether; and that these salts when in solution are readily decomposed by the mineral alkalies with the elimination of the alkaloids, which, in their free and uncombined state, are more or less readily soluble in ether.
Otto‘s Method.—Otto‘s modification of Stas‘s process is simpler, and at the same time equally accurate. Instead of numerous treatments and evaporations which have to be gone through in the original process, Otto converts the alkaloid into a salt, such as the sulphate, by the addition of acid, and after solution in a small quantity of water, agitates with successive quantities of ether, which remove all foreign fatty matters, leaving the solution of the alkaloid comparatively pure, and from which the alkaloid may be obtained in a state of great purity, by first rendering the solution alkaline and then using ether to dissolve the alkaloid.
R. Wagner‘s Method.—The presence of alkaloids in organic liquids—strychnia in beer, for example—may, according to R. Wagner (Zeitschr. Anal. Chem., vol. iv. p. 387), be detected by mixing the liquid, diluted with two vols. water (½ to 1 litre), with about 5 c.c. of a solution of iodine in potassium iodide (12.7 grains iodine to the litre) and a few drops of sulphuric acid. The precipitate separated from the supernatant liquid is dissolved in a dilute solution of sodium hyposulphite, and again precipitated by means of the iodine solution. If this new precipitate be now dissolved in aqueous sulphurous acid, the solution will leave, on evaporation, the pure sulphate of the base.
Dragendorff‘s Method.—This is intended for the purpose of separating alkaloids from each other when more than one are in aqueous solution, by using different solvents in sequence. Some solvents take up certain alkaloids to the exclusion of others. The process consists of extracting the aqueous acid solution of the alkaloids successively with petroleum spirit, benzene, chloroform, and amyl-alcohol, then alkalising it and repeating with the same solvents.
1. From the acid solution benzene removes caffeine, colchicine, santonin, digitalin, cantharidin. Chloroform removes papaverine, colchicine, narceine, picrotoxin.
2. From the alkaline solution petroleum ether removes strychnine, brucine, aconitine, veratrine, conine, nicotine, lobeline, emetine, and aniline. Benzene removes atropine, hyoscyamine, physostigmine, codeine, narcotine, and further quantities of strychnine, brucine, aconitine, veratrine, and emetine. Chloroform removes morphine, narceine, papaverine, strychnine, and brucine. Amyl-alcohol removes morphine, solanine, and narceine.
The Stas process cannot be recommended for the detection of opium in organic liquids, for two reasons. Firstly, that it altogether fails to indicate the presence of meconic [Pg 338] acid; and, secondly, because morphine is almost insoluble in ether. Dragendorff recommends the use of benzole for separating the alkaloids, but in this substance morphia is nearly insoluble. It is, however, applicable to strychnine, aconitine, conine, and atropine; but for the two last, on account of their volatility, ether is preferable.
Rodger‘s and Girdwood‘s Method.—Extraction with dilute hydrochloric acid and the use of chloroform instead of ether. Chloroform is a much better solvent of most alkaloids than ether. Particularly useful for the isolation of strychnine and for most alkaloids, but there is a little danger of hydrolysis of the alkaloid in the use of a mineral acid, e.g. hyoscine.
Stevenson‘s Modification of the Otto-Stas Process.—The material to be examined, if solid, is finely divided, and digested for twenty-four hours with twice its weight of rectified spirit at 35° C.; if fluid, with twice its volume. The clear liquid is decanted and the residue again digested with fresh spirit; this is again decanted, and mixed with the first alcoholic solution. The residue is now digested with spirit faintly acidified with acetic acid; this is decanted, and the residue digested with two or three lots of unacidified alcohol. The alcoholic extracts obtained before acidification are mixed together and rapidly raised to 70° C. for a moment or two. They are quickly cooled and filtered, and the filter washed with spirit. The acidified extract and those after it are mixed and treated in the same way. The extracts are then separately evaporated at a temperature not above 35° C. to the consistency of a syrup, the excess of acid being neutralised with soda; these are extracted with absolute alcohol, and the extracts evaporated to a syrup as before. The syrupy extracts are now diluted with a small quantity of water, filtered, the filters washed with water, and the filtrates mixed. The liquid will contain the whole of the alkaloids, and will be free from albuminoids, which have been coagulated while the extracts were at 70° C. The liquid containing the alkaloids is extracted several times with washed ether, which removes fatty acids or oils, but does not remove alkaloidal salts. The ether should be washed with water to which a few drops of sulphuric acid has been added, and the water kept: this has to be done because some alkaloidal salts are slightly soluble in ether. The acid liquid and the acidified aqueous washings of the ether are mixed together, rendered alkaline with sodium carbonate, and exhausted firstly with a mixture of one volume of chloroform to three of ether, and lastly three or four times with ether alone.
The alkalisation with sodium carbonate liberates the alkaloids from their salts, and these are soluble in the chloroform-ether and ether. These ethereal extracts are then washed with water acidified with sulphuric acid, and water alone, and the washings mixed. The water acidulated with sulphuric acid converts them into sulphates, which are insoluble in the ether and chloroform, and are removed by the acidified water, while impurities are left behind. The mixed aqueous and acid extracts are again washed with ether, the ether removed, and the liquid re-alkalised with sodium carbonate and then re-extracted with chloroform-ether and ether. [Pg 339]
The ethereal solutions are removed and are washed with water slightly alkalised with sodium carbonate. The ethereal solution is filtered through a dry filter, the filtrate evaporated to dryness first at 35° C. then at 100° C., and cooled over sulphuric acid. The residue is weighed and represents the weight of the alkaloids. A test quantity should be evaporated to see if there be any oily odorous residue, i.e. a volatile alkaloid, nicotine or conine. If so, the chloroform and ether extracts should be mixed with a little pure ether and strong hydrochloric acid; the alkaloids are thus changed into non-volatile hydrochlorides, which are left behind after evaporation of the chloroform and ether. Any alkaloid found should be converted into the hydrochloride, dissolved, and tested by special tests. Morphine cannot be extracted except in very minute amounts by this method. To obtain it, the first alkaline solution from which the other alkaloids have been removed should be extracted with acetic ether and ether, in which morphine is soluble.

Fig. 36.—Photo-micrograph
of crystals
of hydrochloride of morphine, × 50.
(R. J. M. Buchanan.)
Taylor‘s method for the extraction of morphine may be briefly described as follows:
The liquid—porter, &c.—to be examined is acidified with acetic acid; or, if a solid organ is to be tested, it must be cut into thin slices and placed in distilled water acidified in a similar way. In either case the liquid is digested for one or two hours at a gentle heat, and filtered. Acetate of lead is now added to the filtrate until no further precipitation occurs; the liquid is then boiled and filtered. The meconic acid remains on the filter as meconate of lead, while the filtrate contains the morphine as acetate. The liquid is freed from excess of lead by passing through it a current of sulphuretted hydrogen, filtered to remove the precipitated sulphide of lead, and the [Pg 340] resulting liquid evaporated to an extract on a water bath, and treated with alcohol. The alcoholic solution on evaporation gives acetate of morphine, which may then be tested.

Fig. 37.—Photo-micrograph
of meconic acid
crystallised from aqueous solution, × 50.
(R. J. M. Buchanan.)
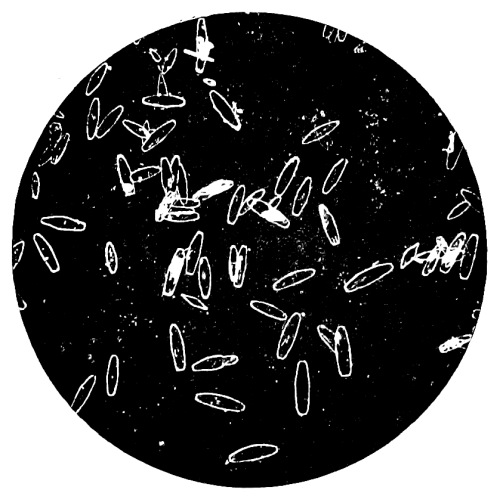
Fig. 38.—Photo-micrograph
of meconic acid
crystallised from an alcoholic solution, × 50.
(R. J. M. Buchanan.)
The meconate of lead which remains on the filter is decomposed by [Pg 341] treating it with dilute sulphuric acid, and gently boiling the mixture. The filtered liquid should be neutralised before the tests for the presence of meconic acid are applied.
The reactions of both morphine and meconic acid are best seen from the following Table:—
| Morphine—Solid | |
|---|---|
| Treated with strong nitric acid. | Dissolves with effervescence and |
| the production of ruddy fumes, | |
| forming a rich orange-coloured | |
| solution not changed by the | |
| addition of stannous chloride. | |
| Mixed with a little iodic acid | A blue colour, due to the |
| and starch paste. | liberation of iodine. |
| Dissolved in cold strong | Bright-green colour. |
| sulphuric acid, and a drop of | |
| strong solution of bichromate | |
| of potash added. | |
| Rubbed with sulphomolybdic acid | A violet colour changing to |
| (Frohde‘s reagent). | green, and then sapphire-blue. |
| Morphine and Meconic Acid in Solution | ||
|---|---|---|
| Morphine. | Meconic Acid. | |
| Tested with litmus paper. | Slightly alkaline. | Very distinctly acid. |
| A little perchloride | An inky-blue colour, | Deep red colour, not |
| of iron, rendered | destroyed and changed | easily destroyed by |
| of nearly neutral | to orange-red by | a solution of |
| as possible. | nitric acid. | corrosive sublimate or |
| dilute mineral acids. | ||
The characteristic tests for morphine are its reactions with nitric acid, iodic acid and starch, and perchloride of iron. The reaction with the perchloride of iron is also characteristic of meconic acid. This last-mentioned test is a very conclusive one for meconic acid, when certain precautions are taken; for the property of striking a deep red with a persalt of iron is shared equally by sulphocyanides and alkaline acetates. The colour produced by sulphocyanic acid is instantly bleached on the addition of corrosive sublimate. The question thus lies between acetic and meconic acid. To distinguish the one from the other, the solution to be tested should be boiled for a short time after the addition of a few drops of sulphuric acid. Any acetate present is decomposed and the acetic acid is expelled by the boiling; so that if, after allowing the solution to cool, it still gives the red colour with perchloride of iron, the reaction may be taken as conclusive of meconic acid. By these means morphine and meconic acid may be detected in porter and other liquids. [Pg 342]
Table showing the Characters and
Tests of the Following Poisons
| Morphine. | Strychnine. |
|---|---|
| 1. Crystallises in colourless | 1. Crystallises in white |
| transparent prisms, belonging | four-sided prisms, terminated |
| to the trimetric system. | by four-sided pyramids. |
| 2. Sulphuric acid and | 2. Treated with cold sulphuric |
| bichromate of potash give | acid, no reaction; on |
| a bright-green coloration. | the addition of a crystal of |
| potassium bichromate, an | |
| intense purple colour is | |
| produced, becoming | |
| crimson and then light red | |
| 3. Strong colourless nitric acid, | 3. Strong nitric acid usually |
| added freely to a cold | produces a yellow or |
| solution, produces a deep | yellow-brown colour. |
| orange-red coloration, not | |
| changed by stannous chloride. | |
| Brucine. | Narcotine. |
| 1. Crystallises in oblique rhomboidal | 1. Crystallises in right rhombic |
| prisms, sometimes agglomerated | prisms, or in needles |
| mushroom-like heads. | grouped in bundles. |
| 2. Sulphuric acid gives a | 2. Sulphuric acid a bright |
| rich rose-pink tint; on the | sulphur-yellow colour, |
| addition of potassium | potassium bichromate added a |
| bichromate, none of the | green colour as with morphine, |
| reactions of strychnine | but slower in production. |
| are observed. | |
| 3. Strong nitric acid produces a | 3. Strong nitric acid forms |
| blood-red colour, changed | a colourless fluid, becoming |
| after warming and diluting | yellow on heating. |
| with distilled water to purple | |
| by stannous chloride; | |
| ammonium sulphide gives | |
| a similar but less marked | |
| reaction. Excess of stannous | |
| chloride discharges the | |
| blood-red colour in the cold. |
Opium is the inspissated juice of the Papaver somniferum, the garden or opium poppy. The plant is a native of Egypt and Syria, cultivated in England.
Opium is sometimes taken in its crude state as a poison, but more frequently one of its preparations is thus employed—notably the tincture, better known as laudanum.
The poisonous properties of this drug reside in an alkaloid, morphine—in combination with an acid, meconic acid. The several varieties of opium vary considerably in the quantity of morphine which they contain, the amount varying from 2 to 9 per cent.
Opium, or its alkaloid, morphine, forms an important ingredient in Dalby‘s Carminative, Winslow‘s Soothing Syrup, Godfrey‘s Cordial, Chlorodyne, Nepenthe, &c.
Of all forms of poisoning, that by opium and its preparations is the most frequent; and it is stated that three-fourths of all the deaths from opium occur among children under five years of age.
Symptoms.—The rapidity with which the symptoms of poisoning by opium make their appearance will depend upon the form in which the poison is taken—solution, of course, increasing the activity of the drug. In most cases, an interval of from half an hour to an hour elapses after the poison has been swallowed before any evil effects become apparent. Christison, however, mentions a case in which stupor did not show itself for eighteen hours. During the first stage of poisoning by opium, the patient may become slightly excited; this state is, however, soon followed by giddiness and drowsiness. The eyes are kept open with difficulty. Stupor and insensibility now supervene, from which he may, in most cases, be temporarily aroused by a loud noise or a smart blow. As the case progresses, coma and stertorous breathing occur, and it becomes almost impossible to rouse him at all. The pulse, at first small, quick, and irregular, becomes slow and full as the coma increases. The breathing, hurried in the early stages, is now slow and stertorous. The pupils are contracted in the early stages, and may be in the later stages dilated; the former condition is most frequently present, together with insensibility to light. The pupils may be contracted in cases of hæmorrhage into the pons Varolii, and [Pg 344] this disease has been mistaken for opium poisoning. In uræmic coma, coming on in the course of Bright‘s disease, the pupils may also be contracted; the nature of the case will be explained by the history and presence of dropsy. All the secretions, except that of the skin, are suspended, and the bowels are usually obstinately confined. The breath may be impregnated with the odour of opium. Certain anomalies in the symptoms may occur; thus, there may be vomiting and purging, convulsions (the last most frequent in children), delirium, tetanic spasms, one pupil dilated and the other contracted, paralysis, and anæsthesia. It must be borne in mind that remissions sometimes occur in the symptoms, the patient dying after an attempt at recovery.
A question of some importance may arise as to the amount of volition and power of locomotion which may exist for some time after a poisonous dose has been taken. Death may be due to causes other than the effect of poison. It must, at least, be admitted as possible, that a person, after swallowing a quantity of opium sufficient to cause death, may yet be able to walk and move about for one or two hours.
Opium-eating.—If opium be taken for some time in small doses, the system becomes tolerant of it, so that a dose which would be poisonous to most people only produces a slight and pleasurable excitement. De Quincey was in the habit of taking daily nine ounces of laudanum. The habitual opium-eater generally suffers from disorders of the digestive organs, dyspepsia and its train of unpleasant symptoms; the body becomes thin, the countenance attenuated, the eyes sunken and glassy, the gait halting, and the body bent. The craving for the drug, which becomes greater and greater, is only temporarily satisfied by larger and larger doses. The opium-eater seldom attains a great age, usually dying before forty. This is perhaps a somewhat exaggerated picture of the ill effects of opium-eating. Christison, after quoting the results of his observations in twenty-five cases of confirmed opium-eaters, concludes as follows: “These facts tend on the whole rather to show that the practice of eating opium is not so injurious, and an opium-eater‘s life is not uninsurable, as is commonly thought, and that an insured person, who did not make known his habit, could scarcely be considered guilty of concealment to the effect of voiding his insurance. But I am far from thinking (as several represent who have quoted this work) that what has now been stated can with justice be held to establish such important inferences; for there is an obvious reason why, in an inquiry of this kind, those instances chiefly should come under notice where the constitution has escaped injury—cases fatal in early life being more apt to be lost sight of, or more likely to be concealed.”
Effects of External Application.—The application of opium to the surface of the body is not usually attended with dangerous symptoms; but, in a few cases, due probably to some idiosyncrasy, alarming effects, or even death, have resulted from the external application of the drug. Orfila has tried to show that opium is readily absorbed by the coats of the rectum, and that it acts more rapidly than [Pg 345] when taken into the stomach. This statement does not appear to be correct, for the dose administered by enema is usually twice that given by the mouth.
Post-mortem Appearances.—As might be expected, the appearances found after death are not very characteristic. The vessels of the brain are congested, and serous effusions in the ventricles or between the membranes are not uncommon. Engorgement of the lungs is most frequently present in those cases in which convulsions have occurred. The stomach is in most cases found quite healthy. The bladder may be full of urine, due probably to the person being unable to empty it from loss of consciousness.
Fatal Period.—From three-quarters of an hour and upwards.
Fatal Dose.—Four grains is about the smallest fatal dose of opium in an adult; but cases of recovery, where an ounce or more of laudanum has been taken, are not very rare. Children are very susceptible to opium. The smallest dose of morphine that has proved fatal to an infant is one-twelfth of a grain of the hydrochloride. Half a grain of the acetate has proved fatal to an adult, one grain of morphine or its salts has proved fatal on several occasions. With prompt treatment recovery has taken place after much larger doses, even as much as seventy-five grains.
Chemical Analysis and Tests.—These have been described on p. 339 et seq.
Treatment.—The stomach pump should be used without delay, and the stomach thoroughly washed out. The washing water should contain about ten to fifteen grains of permanganate of potash to the pint, and the washing repeated at short intervals, as the permanganate destroys the morphine. If the stomach tube be not at hand, the patient should be made to drink the permanganate solution if possible. This treatment should be carried out even when morphine has been administered hypodermically, as it is excreted by the stomach. Emetics should also be given if the patient can swallow; if unable to do so, a hypodermic of ⅒ grain of apomorphine may be given. The administration of strong coffee or tea, the application of ammonia to the nostrils, flagellation of the soles of the feet, and keeping the patient constantly walking about (a procedure of doubtful value) are among the measures usually adopted by way of treatment. Galvanism and artificial inflation of the lungs have done good service even in the most hopeless cases. The student is referred to some important cases recorded by Dr. Burgess and others in the Medical Press and Circular, vol. i. p. 369, for the year 1892. Dr. Burgess strongly recommends prolonged artificial respiration, the interrupted current, and the administration of stimulants, externally, internally, and hypodermically. Dr. Finny is of opinion that, while opium may be useful in cases of atropine poisoning, atropine is of little use in opium poisoning; in this opinion Dr. Burgess concurred. The state of the respiration is a better test than the condition of the pupil when atropine is used as an antidote. If the administration of atropine does not quicken the respiration it should be discontinued, and other methods tried. Vinegar should not be given, [Pg 346] as it dissolves the morphine and renders it more easy of absorption. Death is rare in those cases in which proper remedies have been resorted to before the stage of stupor has commenced.
Synopsis of the Effects of Opium
upon the System
1. The Mental Faculties.—The first effect noticed when opium is taken in small doses is a primary exaltation of the mental faculties; the imagination is rendered brilliant, and the passions exalted; after a time drowsiness supervenes, followed by deep sleep. A dose of thirty drops of the tincture caused in one experimenter an exhilaration of the mental faculties, and an aptitude for study; the subsequent drowsiness being removed by a dose of a hundred drops or more, when the greatest mental excitement was the result.
2. The Respiration.—The frequency of the respiration is diminished, and the oxidation of the blood impaired.
3. The Pulse.—The first effect on the circulatory system is that of a stimulant, and then sedative. By the administration of repeated small doses, the force of the circulation may be maintained for some time.
4. The Eyes and Countenance.—The pupils, when the patient is powerfully under the influence of opium, are contracted even to a point. Dilatation, has, however, been noticed in some cases, especially when death approaches. In apoplexy of the pons Varolii, the pupils are contracted. The countenance is placid, pale, and ghastly; the eyes heavy, and the lips livid.
5. The Cutaneous System.—The skin, although cold, is not infrequently bathed in profuse perspiration.
6. The Alimentary Canal.—Sometimes there is vomiting and even purging; but, as a rule, the secretions along the whole alimentary canal are diminished, and constipation is the result. According to Dr. Walter Smith, of Dublin, morphine is mainly excreted into the stomach and bowels, and so cast out in the fæces. Very little goes out in the urine.
7. The Average Commencement of Symptoms.—Much depends upon the size and form of the dose. In most cases the first appearance of the symptoms is seldom delayed beyond an hour after the poison is taken.
8. The Average Period of Death.—Seven to twelve hours. [Pg 347]
Table showing some of the Symptoms and Effects
of Opium and Belladonna
| Opium. | Belladonna. |
|---|---|
| 1. Slight excitement, coma, | 1. Active, busy delirium preceding |
| lethargy, and no return of the | the coma, followed by delirium, |
| excitement should the patient | if recovery takes place. |
| recover. | |
| 2. Coma is of shorter duration than | 2. Coma is of longer duration than |
| in poisoning by belladonna. | in poisoning by opium. |
| 3. Pupils contracted. | 3. Pupils dilated. |
| 4. Local application to the eye | 4. Dropped into the eye, the pupils |
| does not affect the pupil. | are dilated. |
| 5. Bowels as a rule confined. | 5. Bowels not affected. |
| 6. Acts powerfully on children. | 6. Well borne by children. |
Table showing the Points
of Distinction between
Apoplexy and Narcotic Poisoning
Table showing the Condition of the Pupils in—
| Ordinary sleep | The eyes turned upwards; pupils contracted. |
| Chloroform narcosis | When the liquid is taken, coma; pupils |
| dilated; eyes suffused or glistening, and | |
| turned upwards. When the vapour is | |
| inhaled, pupils first contracted; when coma | |
| supervenes, dilated. | |
| Apoplexy | Pupils dilated; insensible to light. Sometimes |
| unequal. Apoplexy of pons Varolii, | |
| pupils contracted. | |
| Alcoholic coma | The pupils dilated or variable, and not affected |
| by a bright light placed before them. | |
| Poisoning by opium | Contracted in some cases to a pin‘s head; as |
| death approaches, the pupils dilate. | |
| Carbolic acid | Contracted and insensible to light. |
| Calabar bean | Powerful contraction of the pupils. |
| Hyoscyamus or atropine | Dilatation of the pupils. |
| Strychnine | In some cases the pupils, during the |
| paroxysms, are dilated, and contracted | |
| during the intermissions. | |
| Aconite | Sometimes contracted; but in 17 out of 20 |
| cases recorded by Dr. Tucker, dilatation | |
| was present. |
Under this head will be noticed those poisons whose action on the animal economy is characterised by delirium, illusion of the senses, and marked dilatation of the pupil. In some cases there is considerable irritation of the digestive organs, accompanied with a difficulty in passing water, sometimes ending in complete suppression of urine. The mydriatic alkaloids atropine, hyoscine, hyoscyamine, daturine, duboisine, scopolamine, are practically identical in chemical composition and action, and produce similar symptoms.
The following are among the most important poisons of this group:—
Those of less importance are Œnanthe crocata or Dropwort, Camphor, Salicylic Acid, and Yew—the last already described among the Vegetable Irritants.
Symptoms.—Taken internally or applied externally, belladonna, Atropa Belladonna (N. O. Solanacea), or its alkaloid atropine, causes dryness of the mouth and throat, with intense thirst. Nausea and vomiting are present in most cases, accompanied with giddiness, double or indistinct vision, active delirium, convulsions, ending in stupor and coma. In the majority of cases an erythematous rash appears on the skin, with elevation of temperature resembling scarlet fever. A very marked characteristic of poisoning by solanaceous plants is dilatation of the pupil, the iris in some cases being reduced to a mere line round the pupil. The symptoms in some cases which have been recorded are almost identical with those of delirium tremens. In other instances there has been little or no delirium, the patient at once passing into fatal lethargy. Alarming symptoms have followed from drinking a decoction of belladonna leaves, which were mistaken and supplied for those of the ash. Accidental poisoning has also frequently occurred among children from their eating the ripe berries of the belladonna plant. Slight symptoms of poisoning are sometimes met with from the use of belladonna plasters to remove the [Pg 350] milk from the breasts of women delivered of still-born children, or in cases where the child has died soon after birth. In these cases the patients complain of intense dryness of the mouth, dimness of vision, and itching of the skin. The removal of the plasters will at once arrest the unpleasant symptoms.
In the Gazette des Hôpitaux, July 1859, a case is recorded of poisoning by the outward application of belladonna in the form of the following liniment: Camphorated oil of henbane, ten ounces; extract of belladonna, four scruples. The patient was seriously ill for some days, but ultimately recovered.
Poisoning has also resulted from the use of a solution of atropine (four grains to one ounce) dropped into the eye in the treatment of iritis. (See British Medical Journal, 1876, vol. i.)
Post-mortem Appearances.—Congestion of the vessels of the brain, sometimes with fluid blood, at other times with thick black blood. The stomach may or may not be congested; but in cases where the ripe berries have been taken, the mucous lining may be seen deeply dyed by the juice of the berries. The pupils are usually found dilated.
Fatal Dose.—One teaspoonful of belladonna liniment and one drachm of tincture have proved fatal. Recovery has taken place after half an ounce of liniment and extract. Children are less affected than adults. Of atropine half a grain has proved fatal. Recovery has taken place after five grains of the sulphate.
Fatal Period.—Twelve hours to several days.
Chemical Analysis.—From organic mixtures the alkaloid may be obtained by Stas‘s process, and treated according to Vitali with a little fuming nitric acid, and then dried in a water bath: when cold, it must be moistened with a drop of potassæ dissolved in absolute alcohol. A violet colour changing to red is produced, the violet being characteristic, as strychnia when treated as above gives a red colour. The physiological action on the pupil must also be noted. When the berries are taken, the mucous membrane of the stomach may be found dyed of a purple colour, turned green by alkalies and red by acids. Fragments of the berries may also be found in the stomach.
To a small quantity of solid atropine add a drop or two of strong sulphuric acid, then a crystal of sodium nitrite; a yellow colour is produced, which alcoholic solution of potash changes to reddish-violet and then pale rose.
Free atropine gives a red colour with phenolpthalein; the colour is discharged with alcohol, but reappears on evaporating it.
Gerrard‘s Test.—Mercuric chloride dissolved in alcohol gives a red colour.
Blyth‘s Test.—To the solid alkaloid add strong solution of baryta, evaporate, to dryness, and heat the residue, when the smell of hawthorn blossom is given off.
Wormley‘s Test.—An alcoholic solution of bromine gives a crystalline yellow precipitate.
Treatment.—Wash out the stomach and give hypodermic injections [Pg 351] of one-third of a grain of pilocarpine, which is the best antidote. Emetics and purgatives, castor-oil and animal charcoal may be administered. The symptoms as they present themselves must be treated on general principles.
N.B.—Belladonna has been stated to act in antagonism to opium, and its administration recommended in poisoning by that drug.
Hyoscyamus, Hyoscyamus niger, or henbane (N.O. Solanaceæ), alkaloids hyoscine, hyoscyamine, taken in large doses, produces symptoms not unlike those due to belladonna. There is the same affection of sight—double vision; the same dilatation of the pupils, delirium, confusion of thought, insensibility, and coma. Hyoscine has a hypnotic effect in comparison to the deliriant action of belladonna. But its action varies very much on different people. A form of mania, with wild hallucinations, has sometimes been observed to follow the administration of this drug.
The peculiar property of henbane is marked by its tendency to produce a general paralysis of the nervous system. The root has been eaten by mistake for parsnips, when all the foregoing symptoms were present. The seeds are more poisonous than the roots, the leaves being the least poisonous part of the plant.
Post-mortem Appearances.—The morbid appearances are not unlike those which result from poisoning with belladonna.
Fatal Dose.—Nothing certain can be stated as to the amount required to cause death. Alarming symptoms are said to have followed the administration of ten minims of the tincture, repeated every six hours. Twenty of the seeds have caused active delirium. Idiosyncrasy may have something to do with this result. Half a drachm of the tincture is often given to an adult, and repeated every four hours, without any unpleasant result.
Treatment.—As for belladonna, emetics and purgatives, to expel the poison from the system.
The Thorn Apple, Datura Stramonium (N.O. Solanaceæ), possesses powerful poisonous properties. These are marked by the production of giddiness, impairment of vision, and syncope. Furious delirium is not infrequent; and in one case where this state was present there was loss of speech. The face is usually flushed, the eyes glistening and restless, and the pupils dilated; in short, the countenance is that of one intoxicated. Taken together, the symptoms are not unlike those produced by belladonna.
Poisoning by stramonium seeds is a favourite mode of procedure among the Hindoos; but as the poison is most frequently given to facilitate robbery, death seldom results from its use. In India, the seeds are mixed with the boiled rice so commonly eaten there, and as they closely resemble the seeds of the common capsicum, the dangerous nature of the [Pg 352] mixture is not readily detected. The seeds of the datura can be distinguished by the taste, which is slightly bitter, whereas that of the capsicum is hot and pungent. The outward application of the leaves may give rise to all the appearances of poisoning.
The active principle of stramonium is the alkaloid Daturine, which crystallises in colourless quadrangular prisms, with a bitter acrid taste. It resembles atropine and hyoscyamine in chemical properties.
Post-mortem Appearances.—Congestion of the vessels of the brain and its membranes, with some slight gastric irritation.
Treatment.—As for belladonna, emetics and purgatives, to get rid of the portions of the plant swallowed.
Some other solanaceous plants—Solanum Dulcamara, Bittersweet or Woody Nightshade, Solanum nigrum, or Garden Nightshade, and the Solanum tuberosum, or Potato—possess poisonous properties. They, like the other members of the order to which they belong, give rise to symptoms characterised by giddiness, dimness of sight, trembling of the limbs, and delirium. The water in which the potato has been boiled is sometimes used by the vulgar as an application to favus of the scalp.
The active principle of these plants resides in an alkaloid, Solanine, which is not a very powerful poison. A rabbit has been killed in a few hours by two grains of the sulphate of solanine.
Hemlock-Dropwort, or Dead-tongue, is a poisonous indigenous, umbelliferous plant.
Accidental poisoning by this plant has occurred, the root having been mistaken for parsnip. The symptoms in one of the cases which have been recorded were those of delirium tremens; in another, which terminated fatally, vomiting of blood was followed by convulsions. First contraction and then dilatation of the pupil, spasmodic respiration, and an almost imperceptible pulse were the effects noticed. Death may take place in a few hours.
Post-mortem Appearances.—Congestion of the vessels of the brain, and gastric irritation. The face has sometimes a bloated expression, and blood may escape from the ears and mouth.
Treatment.—Purgatives and emetics, to evacuate the bowel and stomach, and thus get rid of the poison.
Camphor is a concrete vegetable oil obtained from Camphora officinarum (N.O. Lauraceæ). Its employment for the purpose of homicide is rare, but several cases of accidental poisoning from the use of the homœopathic solution have been recorded (British Medical Journal, 1873, vol. ii. p. 617).
The symptoms are—languor, giddiness, delirium, foaming at the mouth, [Pg 353] vomiting of blood-tinged fluid, convulsions, gastric irritation, and great abdominal pain. In one case—that of a young lady aged twenty, who took twenty-five drops of “Epps‘ Concentrated Solution of Camphor” for a sore throat—all the above-mentioned symptoms were present; she was also unconscious for several hours, and partially paralysed for several days—perfect recovery from the nervous symptoms not taking place for more than six months.
The homœopathic solution (Rubini‘s) is stronger than that of the British Pharmacopœia in the proportion of 7.2 to 1. For its detection in organic fluids, it may be removed by chloroform; and from fixed oils, by distillation. Water precipitates it from its alcoholic solution.
Post-mortem Appearances.—Those produced by irritants.
Treatment.—Purgation and emetics, to empty the bowel and stomach.
This substance, prepared by acting on a mixture of carbolic acid and sodium with carbonic acid at a moderate heat, is used largely for acute rheumatism. In some cases premonitory symptoms of poisoning have demanded a cessation in the administration of the drug. The most usual of these are noises in the ears, difficulty of hearing, amblyopia, delirium, and profuse perspiration. There may be hæmorrhages from the mucous membranes, and into the retina. When the drug is discontinued the symptoms pass off. The symptoms are held by some observers to be due to the artificial and not the natural acid.
The poisons grouped under this head are characterised by causing delirium, followed by narcotism. Recovery is not infrequently slow, the system suffering more or less severely from the effects of the poison.
In the case of alcohol, loss of appetite, accompanied with considerable gastric irritation, are among the after-effects of the poison.
The chief of this group are—Alcohol, Cocculus Indicus, Poisonous Fungi, Nitro-Benzene.
Others of less importance will be briefly considered.
It will be necessary to consider poisoning by this substance under two forms—acute and chronic. So many anomalies present themselves that it is difficult to give a clear outline of the symptoms.
Acute.—In most cases the symptoms come on within a few minutes after the poison is swallowed. Giddiness, confusion of ideas, and a difficulty in walking straight are among the first effects produced, these being followed by stupor and coma. Nausea and vomiting are the early signs of recovery. In some cases there may be no premonitory symptoms, sudden and complete stupor supervening some time after a large dose of alcohol has been taken.
The patient not infrequently recovers from the first symptoms. A relapse takes place; he becomes insensible, and dies convulsed. The countenance wears a vacant expression, the face flushed and bloated, the lips livid, and the pupils dilated and insensible to light. The pupils may be contracted, but dilate on irritating the skin by a pin-prick or pinch. The sensibility of the pupil to the action of light should be regarded as a favourable symptom. The rapidity with which alcohol acts is not so great as to prevent the individual from walking some distance and performing certain acts of volition. The rapidity with which the symptoms show themselves will depend upon the previous habits of the individual, and the strength and quantity of the alcohol taken. Alcohol, when diluted, induces a preliminary stage of excitement, followed by stupor; but when concentrated, stupor may come on almost immediately after the spirit is swallowed.
The vapour of alcohol may act as a poison, giving rise to the symptoms above mentioned.
Congestion of the lungs or brain, or both together, is in most cases the cause of death in acute poisoning by alcohol.
Chronic.—The habitual dram-drinker suffers from many diseases. [Pg 355] The appetite becomes impaired; there is considerable irritation of the stomach and bowels, marked by vomiting and purging. Then follows a long list of organic diseases. The structure of the liver becomes changed; it may increase in size, become lighter in colour and cirrhotic, being then known as “hobnailed” or dram-drinker‘s liver. Jaundice and dropsy may be present as the result of this altered condition of the gland. The kidneys also suffer from granular degeneration. Then follow a long series of nervous complaints: congestion of the brain, paralysis, delirium tremens, and insanity. Sudden death by coma not infrequently ends the career of the drunkard.
Delirium tremens is one of the most common results of the habit of drinking; and this affection, it is stated, may be induced by the sudden discontinuance of alcohol in those who are habitually given to its use.
Post-mortem Appearances.—The stomach may present the usual signs of inflammation, due to the irritant action of alcohol. The colour of the mucous membrane of the stomach may be bright red, dark red, brown, or quite pale. The brain and its membranes are sometimes congested, and the intracranial vessels gorged with blood. The odour of alcohol may be present in the contents of the stomach; and alcohol may, in some cases, be detected in the lungs, brain, and other organs of the body. The lungs are not infrequently found congested, and the right cavities of the heart full of dark-coloured blood. Casper examined a case in which the cavities of the heart were empty. The blood is remarkably fluid, and of a dark colour. “Lymphatic exudation between the cerebral meninges, so that the pia mater upon the cerebral hemispheres is seen here and there whitish as if varnished, is not a result of death from drinking, but is the result of the chronic irritation of the brain by habitual drunkenness, and is therefore a very common appearance in the bodies of all drunkards, from whatever cause they have died.” One other condition occurring in those dying from the effects of alcohol, is the remarkably long continued presence of the rigor mortis, and perfect freedom from putrefaction, even up to the ninth day, in an atmosphere by no means unfavourable to early decomposition. A condition of the skin known as cutis anserina, or “goose skin,” was present in some of the cases examined by Casper.
Absorption and Elimination.—From experiments on animals, it has been shown that alcohol is rapidly absorbed, and then eliminated from the system, and that all traces of alcohol may disappear in a few hours, and yet death be the result of its action. Alcohol is supposed to be decomposed in the body, but the exact changes it undergoes do not appear to be very clearly made out.
Fatal Period.—Death has occurred in a few minutes after a large dose of alcohol had been swallowed. The average fatal period is about twenty-four hours. Death may also be an indirect result of the action of alcohol on the system.
Fatal Dose.—Uncertain. The age and habits of the individual must be considered. Between three and four ounces proved fatal to a boy seven years of age. [Pg 356]
Table showing the Points of Distinction between Concussion
of the Brain, Alcoholic Poisoning, and
Poisoning by Opium.
| Concussion of the Brain. | Alcoholic Poisoning. | Poisoning by Opium. |
|---|---|---|
| 1. Marks of violence on | 1. The absence of | 1. Same as under |
| the head. | marks of violence, | alcohol. |
| unless the person has | ||
| fallen on the ground. | ||
| The history of the | ||
| case will help in | ||
| forming an opinion. | ||
| 2. Stupor comes on | 2. Excitement | 2. The symptoms |
| suddenly. | previous to the | slow in appearing; |
| stupor, which comes | drowsiness, stupor, | |
| on suddenly. | lethargy. Muscles | |
| relaxed, and | ||
| locomotion impossible. | ||
| The patient may be | ||
| roused by a sharp | ||
| question. | ||
| 3. Face pale and cold; | 3. Face flushed; and | 3. The face pale, |
| the pupils sluggish and | pupils generally | pupils contracted. |
| insensible to light | dilated. | |
| sometimes dilated. | ||
| 4. Remissions are | 4. Partial recovery | 4. Remissions are, as |
| rare, the patient | may take place, | a rule, rare in this |
| recovering slowly, | followed by death | form of poisoning. |
| and with some | after the lapse | |
| confusion of ideas. | of some hours. | |
| 5. Absence of the | 5. Presence of the | 5. Odour of opium |
| odour of alcohol in | odour of alcohol in | in the breath. |
| breath; if present, | the breath. | |
| it is probably due | ||
| to the treatment of | ||
| bystanders. |
Chemical Analysis.—Tests for Alcohol:
1. Characteristic smell.
2. It dissolves camphor.
3. Treated with dilute sulphuric acid and a strong solution of bichromate of potash, the green oxide of chromium is set free, and the vapour of aldehyde may be detected by the smell.
4. Burnt under the mouth of a test tube, moistened with solution of baryta or lime-water, a deposit is formed in the tube of carbonate of baryta or lime.
5. If a few drops of a solution of iodine in iodide of potassium be added to alcohol, and then sufficient caustic potash be added to decolourise it, a crystalline precipitate of iodoform with its characteristic odour will be formed.
6. If copper turnings be added to a solution containing alcohol, then some strong nitric and sulphuric acid, and the mixture warmed, the odour of sweet spirit of nitre will be given off.
7. On warming with sodium or lead acetate and sulphuric acid the odour of acetic ether is evolved.
[Pg 357] Alcohol in the Contents of the Stomach or in the Tissues.—The contents of the stomach, or the tissues bruised and macerated in distilled water, should be carefully distilled in a water bath. It will be necessary to neutralise the liquid prior to distillation. The distillate should be mixed with chloride of calcium or anhydrous sulphate of copper, and re-distilled. The liquid thus obtained is shaken with dry carbonate of potash, and allowed to settle. The alcohol rises to the top of the mixture, whence it may be removed by the aid of a pipette, and tested as before mentioned.
Treatment.—Immediate use of the stomach pump and emetics; to empty the stomach a hypodermic injection of apomorphine may be given. Affusion of cold water to the head, or the injection of cold water into the ears, may be tried. The administration of ammonia, and the employment of galvanism, have been of service in some cases.
Cocaine is an alkaloid obtained from the Erythroxylon Coca. It produces a paralysing effect upon the endings of sensory nerves, and is used as a local anæsthetic. When absorbed into the blood it paralyses the vagus and causes increased rapidity of the pulse. Applied to the eye it causes dilatation of the pupil. It first has a stimulating action on the centres of the brain and spinal cord, finally paralysing them. It produces death by paralysis of respiration, according to Mosso, by causing tetanus of the respiratory muscles.
Symptoms.—The symptoms produced are pallor, cyanosis, faintness, and cold sweats, pain in the precordial region, rapid pulse, intermittent heart beat, laboured respiration. The pupils are dilated. Speech becomes incoherent, there may be trismus of the jaws, the ideas are confused, and there may be delirium. Tetanic spasms of muscles may occur, and convulsions, also loss of consciousness.
Chronic poisoning, following the cocaine habit, produces a long series of symptoms which are manifestations of mental and physical degeneration, which in extreme cases may pass on to insanity, with hallucinations and delusions.
Fatal Dose.—Half a grain injected into the gum of an adult has caused alarming symptoms, and two-thirds of a grain has caused death. Recovery has taken place after forty-three grains were taken by the mouth.
Fatal Period.—Death has occurred in twenty minutes after three and a half grains by hypodermic injection.
Chemical Analysis.—The alkaloid may be separated from the stomach contents or viscera by the usual procedure for extraction of alkaloids.
1. On the addition of strong nitric acid and evaporating to dryness, the residue when treated with alcoholic solution of potash gives off an odour like peppermint or meadow-sweet.
2. Goeldner‘s Test.—Strong sulphuric acid and resorcin when mixed with cocaine gives a blue colour, changing to rose-pink on [Pg 358] addition of caustic potash. Goeldner considers this a reaction peculiar to cocaine.
3. Metzer‘s Test.—If a few drops of a 5 per cent. solution of chromic acid in water be added to a solution of cocaine hydrochloride, each drop gives a yellow precipitate which redissolves. The addition of strong hydrochloric acid produces a yellow precipitate of chromate of cocaine. Metzer considers this reaction peculiar to cocaine.
4. When applied to the tongue or lips a feeling of numbness is produced; it is rendered more effectual if a solution of sodium bicarbonate be first applied to the mucous membrane.
Treatment.—Wash out the stomach and encourage vomiting. Stimulants and ammonia should be given freely, and if convulsions occur chloroform should be inhaled. Tannic acid or gallic acid in thirty-grain doses have been recommended, also iodine one grain with potassium iodide ten grains, in a wine-glassful of water between the stomach-washing or emesis. Oxygen inhalations and artificial respiration may be resorted to in failure of the respiration.
The fruit of Cocculus Indicus, Anamirta paniculata (N.O. Menispermaceæ), is poisonous, and is frequently used by poachers to capture fish. The berries are ground to powder, mixed with bread, and then thrown into the water. When taken by the fish, they become stupefied, float to the surface, and are then taken.
The poisonous properties are due to a crystalline alkaloid, Picrotoxin. Fraudulent publicans have used this drug for the adulteration of beer. The strength of the beer is first reduced by the addition of salt and water, and then the cocculus indicus is added, to give to it an intoxicating property. The effect produced on the unfortunate customers is a strong desire to sleep, with more or less wakefulness. Loss of voluntary power is present, but consciousness is not lost, the sufferer lying in a state bordering on nightmare. Cocculus is not used in medicine or the arts, and yet a large quantity is imported, and mysteriously disappears in this country.
Symptoms.—The symptoms which have been noticed in poisoning by this substance are—nausea, vomiting, severe abdominal pains, stupor, and intoxication. Two deaths at least have been reported as resulting from it. In the case of R. v. Cluderay, “the defendant administered to a child two cocculus indicus berries, entire in the pod, with intent to murder the child.” The kernel is a poison; the pod is not, and will not dissolve in the stomach; and they were therefore harmless. This was held to be administering poison with intent to murder, within the section of the Statute.
Picrotoxin, the alkaloid, is in fine white crystals, intensely bitter to the taste, soluble in boiling water, slightly so in cold. Alcohol and ether readily dissolve it. Strong nitric acid dissolves it, [Pg 359] without change of colour; and sulphuric acid produces an orange-yellow colour, changed to pale yellow by dilution. In organic liquids it might be mistaken for sugar, or vice versa, as it precipitates the oxide of copper when boiled with the sulphate of copper and potash. In examining beer supposed to be adulterated with picrotoxin, the beer should be acidulated with hydrochloric acid, and then shaken up with ether. On spontaneous evaporation of the ether, the picrotoxin is left in crystals.
Treatment.—Stomach pump, emetics, apomorphine subcutaneously; then chloral and the bromide of potassium. Chloroform may be inhaled. Paraldehyde is said to be a specific antidote.
The seeds of Lolium temulentum, or common darnel, are poisonous. Cases of poisoning have occurred from these seeds being accidentally ground with wheat or rye, and then made into bread.
Symptoms.—Gastric irritation, nausea, and vomiting followed by giddiness, deafness, loss of vision, and, in some cases, delirium. Not infrequently the symptoms resemble those produced by ergot. No death has been recorded as resulting from the use of these seeds. Three ounces of paste made from darnel flour, given to a dog, did not cause death.
Accidental poisoning by mushrooms is by no means rare. The Agaricus campestris, and a few others, are edible; but it is a fact worthy of notice that the poisonous properties of mushrooms are modified by climate and the seasons of the year at which they are collected. Idiosyncrasy may have something to do with the injurious effects produced on some persons by the fungi.
The Agaricus campestris, or common mushroom of this country, is sometimes poisonous; and in some countries—Italy and Hungary—it is usually avoided. In Russia and in France certain fungi are eaten which are regarded as poisonous by us.
Bentley gives, in his Botany, the following table, by which edible and poisonous mushrooms may be known:
| Edible. | Poisonous. |
|---|---|
| 1. Grow solitary in dry airy | 1. Grow in clusters in woods |
| places. | and dark damp places. |
| 2. Generally white or brownish. | 2. Usually with bright colours. |
| 3. Have a compact, brittle | 3. The flesh tough, soft, and |
| flesh. | watery. |
| 4. Do not change colour by the | 4. Acquire a brown, green, or |
| action of the air when cut. | blue tint when cut and |
| exposed to the air. | |
| 5. Juice watery. | 5. Juice often milky. |
| 6. Odour agreeable. | 6. Odour commonly powerful |
| and disagreeable. | |
| 7. Taste not bitter, acrid, salt, | 7. Have an acrid, astringent, |
| or astringent. | acid, salt, or bitter taste. |
[Pg 360] Symptoms.—Two sets of symptoms may follow the use of mushrooms as food—those of irritant and those of narcotic poisoning. In the latter class, giddiness, double vision, and even delirium, have been present. Nausea, vomiting, purging, and convulsions characterise those of the former class. In some cases the individual has presented all the appearances of intoxication.
Post-mortem Appearances.—These will depend to a great extent upon the character of the symptoms prior to death. If signs of irritation have been present, inflammation of the stomach and bowels will most probably be found; but if, on the other hand, narcotic symptoms were predominant, congestion of the vessels of the brain will most likely be present. Arsenic and other poisons have been mixed with mushrooms with intent to kill; the probability of this occurring should be borne in mind, and a rigid examination of the contents of the stomach made in all doubtful cases.
Treatment.—Castor-oil and emetics, atropine hypodermically.
This substance, prepared by acting on benzene by nitric acid, is largely used for flavouring sweets, &c. Nitrobenzene is a heavy, yellow, oily substance with a strong odour of bitter-almond oil, from which, however, it differs by undergoing no change of colour when agitated with strong sulphuric acid. The natural oil acquires a fine crimson colour when treated with strong sulphuric acid.
Symptoms.—These may not make their appearance for three or four hours after the poison is swallowed or inhaled. The vapour is more powerful than the liquid. In some cases which have been described, the patient has complained of feeling drunk, with pain in the head, giddiness, faintness, distorted vision, drowsiness, ending in coma and death. The face is flushed, the jaws sometimes spasmodically closed, and the lips livid. Vomiting then supervenes, the vomited matters having the odour of bitter almonds. Symptoms not unlike those produced by prussic acid or the essential oil of bitter almonds have been noticed in one or two cases; but, as a rule, the insensibility is not immediate, as in prussic acid poisoning, and in this fact lies the distinction between the two substances. Rapidly fatal cases might be mistaken for apoplexy, but the odour betrays the cause of death.
Post-mortem Appearances.—Nothing very characteristic is found after death due to this poison. The blood is sometimes black and fluid and gives the spectrum of acid hæmatin, the lungs congested, and the liver of a purple colour. The blood, contents of the stomach, and even the tissues, may smell strongly of this substance.
Chemical Analysis.—Nitrobenzene may be separated by distilling the organic mixture with sulphuric acid, when the distillate will contain the poison if present. It is converted into aniline by heating it with acetic acid and iron filings. (See test for aniline, infra.) On account of its odour, the only substance with which it can be confounded is the essential oil of bitter almonds, which owes its poisonous properties to the prussic acid it contains. [Pg 361]
The following Table may assist in its Detection.
| Nitrobenzene. | Oil of Bitter Almonds. | |
|---|---|---|
| Strong sulphuric acid. | No change of colour. | A rich crimson colour. |
| Proto-sulphate and the | No blue colour. | Prussian blue. |
| persulphate of iron, | ||
| liquor potassæ, and | ||
| hydrochloric acid. | ||
| Solution of sulphate | Insoluble. | Soluble. |
| of soda. |
Treatment.—Stomach pump, emetics, stimulants, cold douche, artificial respiration.
This substance is a solid of a yellow colour, and is used in the manufacture of roburite, bellite, and sicherite, explosives used in coal mines for blasting. Poisoning by it occurs amongst the workmen who come in contact with it in factories where it is used, by inhaling either the vapour or fine particles, and by handling it may become absorbed through the skin.
Symptoms.—In acute cases these are similar to poisoning by nitrobenzene. In chronic poisoning there is a marked and peculiar pallor of the face, with a livid blue colour of the ears, lips, fingers, and toes. Nausea and vomiting occur, with weakness, giddiness, and staggering. Amblyopia is a common symptom, with concentric contraction of the visual field and central scotoma. The blood resembles that of pernicious anæmia, and the urine is brown or blackish, due to some pigments of the aromatic series.
Post-mortem Appearances.—The blood has been found chocolate-coloured, and ecchymoses have been noted in mucous membranes.
Treatment.—As for nitrobenzene.
Aniline is a colourless oily liquid gradually changing to brown on exposure to air. The various aniline dyes are obtained by oxidation of aniline. Aniline is produced by reduction of nitrobenzene. It is slightly soluble in water, freely so in alcohol or ether. It can be absorbed through the unbroken skin as well as by the lungs and mucous membranes. It is used in the manufacture of marking inks. It has very toxic properties.
Symptoms.—The symptoms come on rapidly—nausea and vomiting, with giddiness and drowsiness; the lips, face, ears, fingers, toes, conjunctivæ, and mucous membranes become cyanotic. The respirations are slow and laboured. The pulse may be full and slow, or small and [Pg 362] irregular. The body surface is cold, the pupils react sluggishly to light. The blood is chocolate-coloured, and is said to give the spectrum of methæmoglobin. The blue colour is held to be due to pigment changes, and not to true cyanosis. Convulsions and coma may come on in fatal cases.
Buchanan met with a case of aniline poisoning in a man who by mistake swallowed about half an ounce of marking ink. Vomiting came on early, with giddiness and staggering gait. The body became changed in colour very rapidly—the colour being between a slate and leaden hue. The eyeballs were of the same colour but of a lighter shade, the mouth and tongue exhibited the colour most markedly. The temperature was subnormal, the pulse quick and feeble, and the breathing occasionally interrupted with sighing respirations. The blood failed to give the spectrum of methæmoglobin. The symptoms passed off within twenty-four hours. During the illness, the man passed several green-coloured motions. The vomit was of a purplish-black colour—from the marking ink—and on analysis gave the reactions of aniline. Some of the ink was procured, and on being analysed was found to consist of hydrochloride of aniline and chloride of copper. The treatment consisted of stomach lavage and inhalations of oxygen, which gave the patient much relief.
Cases have been recorded of aniline poisoning in infants from absorption of the material from linen napkins, which were stamped with marking ink. Buchanan has seen lividity arise from the dry hydrochloride of aniline having been carried in a paper parcel in the waistcoat pocket for two or three days.
Post-mortem Appearances.—None characteristic.
Fatal dose.—Six drachms have proved fatal, probably less might do so.
Chemical Analysis.—Aniline may be separated from organic matter by alkalising and distilling the mixture.
1. If chloride of lime (bleaching powder) be added slowly to an aqueous solution of aniline, a deep purple colour is produced, which changes to brownish-red.
2. If strong sulphuric acid be added to aniline in a porcelain capsule it forms a dirty-white mass; on adding water and then potassium bichromate a bronze-green colour is produced, which changes rapidly to blue and then black.
3. If aniline be dissolved in excess of aqueous solution of phenol, and bleaching powder dropped into the mixture, a yellow streak changing to blue follows each drop.
4. Heated with corrosive sublimate a rich crimson colour is produced.
5. If aniline be mixed with a little chloroform and alcoholic solution of potash and heated, the peculiar odour of phenyl-isocyanide is given off.
Treatment.—As for nitrobenzene.
Fusel-oil, Amylic Alcohol, Potato-Spirit.—Fusel-oil, also known as amylic alcohol, is known by its unpleasant odour and burning taste; it acts like alcohol as an inebriant, giving rise to headache, giddiness, &c. [Pg 363]
Nitro-glycerine.—In liquid or vapour, violent headache and throbbing in the temples are produced by this substance, which is used in the treatment of angina pectoris.
These substances are used extensively as antipyretics. They have been known to cause poisoning when administered in large doses.
Symptoms.—The symptoms are principally those of depression, impairment of sight, vertigo, sleepiness, and unconsciousness; collapse, cyanosis, and loss of body temperature; the pulse and respiration are lowered. Antipyrin causes tumultuous action of the heart, and there may be erythematous or herpetic eruptions on the skin. Aniline derivatives, like sulphonal and other synthetic drugs, tend to destroy the red corpuscles of the blood, and decompose hæmaglobin, producing hæmatoporphyrin which appears in the urine.
Chemical Analysis.—Antifebrin may be extracted from an acid solution by chloroform; for antipyrin the solution should be alkaline.
Antifebrin gives the phenyl-isocyanide reaction on warming with alcoholic solution of potash and chloroform. Bichromate of potassium dissolved in strong sulphuric acid gives a red colour, changing to brown and dirty green; sodium nitrite and strong hydrochloric acid give a yellow colour, changing to green and blue; on evaporation the residue is orange, and turns red on addition of ammonia.
Antipyrin.—Heated with strong nitric acid and the liquid allowed to cool, a purple colour is produced; if water be added a violet precipitate is thrown down, and the filtered liquid will be purplish-red. Ferric chloride gives a blood-red colour, destroyed by a mineral acid. An aqueous solution of potassium nitrite and strong sulphuric acid gives a green colour.
Phenacetin is coloured yellow by nitric acid, the colour persisting when heated. It dissolves in sulphuric acid without change of colour. Boiled with hydrochloric acid, then diluted with water and chromic acid solution added, gives a deep red solution.
Cardiac
The common foxglove, Digitalis purpurea, (N.O. Scrophulariaceæ), grows wild in the hedges in the South of England. All parts of the plant are poisonous, from the presence of a glucoside digitalin, and in addition it also contains the glucosides digitoxin, digitonin, and digitalein; according to Kopp, digitoxin is six to ten times more toxic than digitalin.
Symptoms.—Nausea, salivation, vomiting, purging, and severe abdominal pains are first noticed. The patient then complains of pain in the head, giddiness, and a gradual loss of sight. The eyes protrude, the pupils are dilated and insensible to light, and the sclerotics, according to Tardieu, are of a characteristic blue colour; the pulse weak, slow (forty in the minute) and jerky, sometimes intermittent. The surface of the body is cold, and bathed in perspiration. An aggravation in the symptoms takes place whenever the patient attempts to leave the recumbent position; hence, in all cases of poisoning, and in those where the therapeutical action of the drug is sought, the patient should be warned of the danger of leaving the recumbent posture. A marked depression in the action of the heart is a characteristic effect of this poison. The effect on the heart may be divided into three stages: (1) diminution in the frequency of the pulse, and rise of arterial pressure; (2) both of these become abnormally low; (3) frequency of pulse abnormally high, arterial pressure abnormally low. Convulsions have sometimes been noticed, and syncope and stupor are not uncommon.
Post-mortem Appearances.—Congestion of the brain and its membranes, and some inflammatory redness of the mucous membrane of the stomach. The blood is fluid.
Fatal Dose.—Uncertain. Large doses of the infusion and tincture have been given without any untoward results. Thirty-eight grains of the powdered leaves, and nine drachms of the tincture, have proved fatal. One-quarter to half a grain of digitalin might prove fatal to an adult.
Fatal Period.—From three-quarters of an hour to twenty-four hours.
Chemical Analysis.—If the leaves in an infusion be taken, these must be sought for and examined. The glucoside may be extracted by [Pg 365] first removing the impurities by means of petroleum ether, then acidifying with acetic acid and extracting with chloroform.
The following are the tests for digitalin:
1. An almost amorphous, white, or fawn-coloured inodorous substance.
2. Almost insoluble in water.
3. Decomposes nitric acid, with the evolution of nitrous acid fumes. An orange-yellow-coloured solution is formed, which, in a few days, assumes a golden-yellow tint.
4. Sulphuric acid dissolves it, changing it to a reddish-brown colour, changed to violet by bromine vapour.
5. Hydrochloric acid with it at first forms a yellow solution, which, when heated, changes to a bright green colour.
The physiological test may be employed by injecting a solution of a carefully prepared extract of the contents of the stomach or vomited matters under the skin of a frog, dog, or rabbit.
Treatment.—Purgatives and emetics should be given, followed by infusions containing tannin, green tea, oak bark, galls, strong coffee, and other stimulants. The patient should be kept in the recumbent posture, and on no account allowed to sit up.
The consumption of tobacco, Nicotiana Tabacum (N.O. Solanaceæ), has greatly increased of late years. In some countries its use was prohibited by stringent laws. In Russia amputation of the nose was the punishment. Several Popes have excommunicated those who smoked in St. Peter‘s at Rome; and in some parts of Switzerland it was ranked on the tables next to adultery. Amurath IV made smoking tobacco a capital offence. Be this as it may, the moderate use of tobacco does not appear to lead to injurious results; and it is found that workmen engaged in the manufacture of tobacco do not suffer from any diseases other than those affecting the generality of mankind.
Nicotine—the alkaloid—is a colourless or slightly amber-coloured, oily, volatile liquid. It is to this principle that the poisonous activity of the drug is due. It differs from the other oily alkaloid, conine, in appearing of a green colour when a drop is placed on the surface of white enamelled glass—conine having a pink colour. They both leave a greasy stain on paper. Nicotine has been detected by Stas‘s process in the tongue, stomach, lungs, and liver. A ptomaine not unlike nicotine has been discovered.
Symptoms.—Symptoms of poisoning by tobacco are by no means uniform, and have been variously described by observers. As a type of the effects produced, the following may be noticed as occurring to the tyro after his first or second “pipe”: The pulse is primarily quickened; then follow nausea and faintness, accompanied with an intense feeling of sinking. The face is blanched, the pulse slow; perspiration stands on the forehead, and ultimately he vomits, and then gradually recovers. Cold air blowing on the face, or sponging the face [Pg 366] with cold water, materially hastens a return to comfort. Sometimes, as in the case related by Dr. Marshall Hall of a man who smoked two “pipes,” nausea, vomiting, and syncope occurred, followed by stupor, stertorous breathing, general spasms, and insensibility of the pupil. After an interval of a few hours, the above symptoms again returned, but from which the patient ultimately recovered. Death has resulted as a sequence to excessive smoking. Gruelin records two cases—one from seventeen, the other from eighteen, pipes smoked at a sitting. The symptoms after taking nicotine are more acute, and are a burning acrid taste in the mouth and throat, nausea, vomiting, unconsciousness, shock, sighing respirations, delirium, convulsions; the pupils first contracted then dilated.
The filthy habit of snuff-taking has also been accredited with one or two deaths. Santeuil, the French poet, died in two days from the effects of snuff mixed with his wine as a practical joke.
In animals, the symptoms are—nausea, vomiting, purging, convulsions, stupor, and death. The heart becomes paralysed. One drop of the empyreumatic oil on the tongue of a cat killed it in two minutes, the animal dying in convulsions.
Post-mortem Appearances.—These are by no means uniform or characteristic. If much vomiting precedes death, the vessels of the brain may be engorged with blood. Inflammation of the stomach and intestines is also present in some cases. The odour of nicotine may be detected in the vomit or the stomach contents.
Fatal Period.—The symptoms soon make their appearance, and death has occurred in three-quarters of an hour, or even less—in three minutes after taking the nicotine, in fifteen minutes after enema of tobacco.
Fatal Dose.—One to three drops of nicotine would probably kill an adult in a few minutes; an enema containing half a drachm of the leaves has proved fatal.
As an enema, tobacco should be used with extreme care.
Chemical Analysis.—Nicotine obtained by the usual process for alkaloid extraction, and mixed with water, may have the following tests applied after solution in dilute hydrochloric acid:
1. Chloride of platinum gives an orange-yellow crystalline precipitate.
2. Corrosive sublimate, a white crystalline precipitate.
3. Arsenio-nitrate of silver, a yellow precipitate.
4. Caustic potash added to the hydrochloride and warmed causes a strong odour of tobacco.
5. Solution of iodine in ether added to ethereal solution of nicotine is followed by the production of long needle crystals after some hours.
Treatment.—Promote vomiting, wash out the stomach, cold water douches, and stimulants. Inject strychnine hypodermically.
Lobelia, or Indian Tobacco, Lobelia inflata (N.O. Lobeliaceæ), is extensively employed in North America in the treatment of asthma. The plant is officinal in the British Pharmacopœia. In small doses it possesses expectorant properties. [Pg 367]
Symptoms.—Nausea, vomiting, giddiness, cold clammy sweats, and great depression. The pulse becomes irregular, and very feeble. Taken together, the symptoms are not unlike those produced by tobacco.
Fatal Period.—One to two days, or more.
Fatal Dose.—One drachm of the powder.
Chemical Analysis.—The alkaloid is fluid and may be extracted like nicotine; with it (1) strong sulphuric acid gives a red colour; (2) sulphomolybdic acid gives a violet colour.
Treatment.—The same as recommended under tobacco. Stimulants should be given, ether hypodermically or alcohol per rectum.
The alkaloid Veratrine is obtained from the dried fruit of Asagrœa officinalis (N.O. Melanthaceæ).
The alkaloid is in the form of a white amorphous powder, bitter and acrid to the taste. It acts as a powerful errhine, causing violent sneezing. Insoluble in water, it is readily dissolved by alcohol, ether, and chloroform. When gently heated on a plate with strong sulphuric acid, it first turns yellow, then crimson. Veratrine is entirely dissipated by heat.
Two grains of the alkaloid killed a cat in one minute; a dog being destroyed in two hours by a dose of three grains. The one-sixteenth of a grain (?) of veratrine in a pill caused alarming symptoms in an adult woman, for whom it was ordered by a medical man.
Symptoms.—Acrid burning sensation in the throat and down the œsophagus to the stomach, vomiting, great thirst, diarrhœa may occur with tenesmus. The pulse is feeble and respiration slow. The pupils may be dilated or contracted. Collapse and twitching of muscles, loss of consciousness and convulsions, or delirium and stupor may come on.
Post-mortem Appearances.—Are the same as in poisoning by any of the vegetable irritants.
Treatment.—Stomach pump, and emetics. Astringent infusions should be given, and alcohol and opium administered if the condition of the patient seems to require them.
Chemical Analysis.—Extract in the usual way for alkaloids.
1. Strong sulphuric acid produces a yellow colour, changing to red, produced rapidly if heated.
2. Strong hydrochloric acid and heat produces a red colour.
3. Sulphomolybdic acid produces a reddish colour, changing to dirty brown, greenish, and finally blue.
These tests should be done with the solid veratrine.
Hydrocyanic acid is a compound of cyanogen and hydrogen. It was first obtained by Scheele in 1782, but it was not until 1815 that Gay-Lussac [Pg 368] pointed out its real nature. Anhydrous hydrocyanic acid may be obtained by passing over cyanide of mercury, gently heated, a stream of dry sulphuretted hydrogen. It is now made by mixing ferrocyanide of potassium with dilute sulphuric acid, and applying heat, when the acid is distilled over and collected in a cooled receiver.
Dilute hydrocyanic acid, the only important form of the acid from a toxicological point of view, is a colourless, feebly acid liquid, with a peculiar odour, like that of bitter almonds or peach kernels (specific gravity, 0.997). The Pharmacopœial acid contains 2 per cent. of anhydrous acid; that of Scheele 5 per cent. According to Taylor, however, the percentage of the acid varies from 1.3 to 6.5. Taking into consideration the smallness of the dose, and the shortness of the time before death occurs, it is the most deadly of all known poisons. Prussic acid is not regarded as a cumulative poison—that is, it does not gradually accumulate in the body and then break out with dangerous or fatal violence.
Symptoms.—These will be more or less modified by the quantity of the dose, and in some cases closely resemble an attack of epilepsy. In most cases, the symptoms of poisoning are seldom delayed beyond one or two minutes; and if the dose be large, the symptoms of poisoning may come on while the person is drinking. Giddiness, followed by almost complete insensibility, mark the accession of the symptoms. The eyes are fixed, staring, and glassy; the pupils are dilated, and insensible to light. The muscles of the extremities are relaxed, and the limbs flaccid. A white or bloody froth surrounds the mouth, and the jaws are fixed. The surface of the body is cold and clammy to the touch; the respiration is sometimes long-drawn and spasmodic; and the pulse so reduced as to be almost imperceptible. The breathing is sometimes stertorous in character. This is an important fact; for, in ignorance of the occasional presence of this symptom, it was argued that Walter Palmer, whose breathing was stertorous, died of apoplexy, and not from prussic acid as was alleged. When the dose is small (between twenty and thirty drops of the dilute acid), the patient complains of nausea, giddiness, and a feeling of constriction round the head. The mind is confused, the pulse hurried, and the breathing irregular. Salivation may also be present. Tetanic spasms and involuntary evacuations precede the fatal termination. When the dose is from ten to twenty drops, the patient complains of nausea, giddiness, and a feeling of impending suffocation. These symptoms under treatment may soon pass off, or leave the patient more or less confused and listless. In most cases, where the dose is very large, death takes place suddenly, without convulsions; but the period of death does not appear to be as short in man as in the lower animals.
External Application.—Applied to the unbroken skin, prussic acid does not appear to have caused any alarming symptoms; but it should be used with the utmost caution where the skin is at all abraded or ulcerated.
Post-mortem Appearances.—In making an inspection, care should be [Pg 369] taken; for, if the dose be large, the vapour from the corpse on opening it has been known to produce giddiness and fainting. Externally, the skin is pale, livid, or of a violet colour. The hands are clenched, and the nails blue. The jaws are firmly set, and there is usually some froth around the mouth. The internal organs are greatly congested, and the venous system gorged with fluid dark-coloured blood. The stomach and intestines are sometimes inflamed, but in many cases they present no material alteration in colour.
The appearances, when only a small dose has been taken, are not unlike those of asphyxia. The detection of the odour of hydrocyanic acid in the body is of importance; but this may be absent from the following causes:
1. Smallness of the quantity of the acid present.
2. Volatilisation from exposure of the corpse to the air.
3. The smallness of the dose, and its absence the result of absorption and elimination, if death has not rapidly taken place.
4. The amount of dilution of the poison.
5. Concealed by other odorous substances.
In some cases, the smell may be detected in the stomach seven or eight days after death. The viscera should, in all cases of suspected poisoning, be placed in a glass-stoppered jar, and the stopper covered by bladder and tinfoil. Hydrocyanic acid is so volatile that, unless the greatest care be taken, all traces of it may vanish; and thus the guilty person may be allowed to escape.
Fatal Period.—From a few seconds to as many minutes. Under active treatment, if a patient survive forty minutes, he will generally recover.
Fatal Dose.—Thirty minims of the dilute acid of the Pharmacopœia. This contains six-tenths of a grain of the anhydrous acid. Recovery has, however, taken place even after comparatively large doses. The strength and age of the individual, and also the emptiness or fulness of the stomach at the time the poison is swallowed, will materially affect the issue.
Experiments on Animals
Numerous experiments on animals have been made to ascertain the rapidity with which prussic acid kills. The late Sir R. Christison found that three drops projected into the eye acted on a cat in twenty seconds, and killed it in twenty more. The same quantity dropped on a fresh wound in the loins acted in forty-five, and proved fatal in one hundred and five seconds. In the cases where death did not occur so rapidly, there were regular fits of violent tetanus; but in the very rapid cases, the animals perished, just as the fit was ushered in, with retraction of the head. In rabbits opisthotonos, in cats emprosthotonos, were the chief tetanic symptoms.
As a proof that the acid acts equally on the brain and spinal cord, may be noticed the presence of coma and tetanus in some cases of poisoning by this substance. [Pg 370]
In the experiments on animals certain effects were noticed, which are as follows:
Expulsion of the Fæces and Urine.—In some cases only the fæces, in others the urine alone, was involuntarily expelled; and in some other cases neither the one nor the other was present.
The Shriek or Cry.—This cry, though a common, is by no means a constant symptom.
Convulsions.—These are sometimes present.
Acts of Volition.—Only slight acts are possible; in the case of one of the dogs experimented on by Mr. Nunneley, the animal “went down, came up, and then went down again the whole flight of a steep, winding staircase.”
The Post-mortem Appearances were not well marked in the animals subjected to experiment. In chronic cases, Mr. Nunneley states that both sides of the heart were distended with black blood. The pure acid is stated to completely destroy the irritability of the heart and voluntary muscles, galvanism producing no effect whatever. “In eight experiments on cats and rabbits with the pure acid, the heart contracted spontaneously, as well as under stimuli, for some time after death, except in the instance of the rabbit killed with twenty-five minims, and one of the cats killed by three drops applied to the tongue. In the last two the pulsation of the heart ceased with the short fit of tetanus which preceded death; and in the rabbit, whose chest was laid open instantly after death, the heart was gorged, and its irritability utterly extinct.”
Detection of Hydrocyanic Acid
in Cases of Poisoning
The “Vapour Tests” are those most readily applied to organic mixtures; but in some cases it may be necessary to make a distillation of the suspected substance, in order to isolate the poison.
The first point to be noticed is, whether any odour of the acid can be perceived in the substance under examination. In any case, the contents of the stomach or finely-divided tissues should be mixed with water, and examined as to the reaction with test paper. If the mixture be found to be alkaline, it must be neutralised by the addition of tartaric acid; if, on the contrary, it be acid, carbonate of soda must be carefully added to neutralisation. A state of neutrality is always necessary previous to distillation, for the following reasons:
An alkaline state of the liquid would, on the one hand, prevent, or, at all events, retard, the evolution of the hydrocyanic acid; whilst, on the other, the existence of any free acid would decompose any cyanide which might be present, and thus give rise to an evolution of hydrocyanic acid not existing as such in the mixture.
The organic mixture is then placed in a flask, and the contents distilled at as low a temperature as possible by the aid of a water bath.
Should hydrocyanic acid be present, the distillate will yield all the characteristic reactions of the dilute acid.
1. Nitrate of silver will give a curdy-white precipitate, insoluble in cold but soluble in boiling nitric acid. A portion of the precipitate, on the addition of some liquor potassæ, sulphate of iron, ferric chloride and hydrochloric acid, forms Prussian blue. In this test, which may be taken as quite conclusive, the hydrochloric acid decomposes [Pg 371] the cyanide of silver; and on the addition of the sulphate of iron, Prussian blue is formed.
2. If a portion of the dry precipitate formed by the nitrate of silver be heated in a test tube, cyanogen gas will be evolved, known by its characteristic odour of peach blossoms, and by its burning at the mouth of the tube with a rose-coloured flame.
3. To the solution containing hydrocyanic acid add a few drops of potassium nitrite, two or three drops of ferric chloride solution and dilute sulphuric acid until a yellow tint is obtained; heat to boiling, cool, precipitate excess of iron with ammonia, filter, and add one or two drops of a very dilute solution of colourless ammonium sulphide. A very minute quantity of hydrocyanic acid gives a violet-red colour, changing to blue, green, and finally yellow.
4. If a solution of starch be tinged blue with iodine, the colour will be discharged by a minute quantity of hydrocyanic acid.
Vapour Tests.—There are three tests for the presence of hydrocyanic acid when present in organic mixtures, which have the advantage of being applicable without the addition of anything extraneous to the mixture to be tested. They are all dependent on the volatile nature of hydrocyanic acid, and may be applied as follows, the suspected mixture being divided into three portions:
1. Iron or Prussian Blue Test.—The liquid mixture to be tested is placed in a small beaker glass, and covered with a glass plate the centre of which is smeared with a mixture of potash and proto-sulphate of iron. The whole is now left undisturbed for some time. The glass is eventually removed, and the mixture of potash and iron treated with hydrochloric acid, which, should hydrocyanic acid be present, will cause the development of Prussian blue.
2. Sulphur Test, or Liebig‘s Test.—A second portion of the original mixture is placed in a beaker, and a watch-glass containing a few drops of bisulphide of ammonium is suspended over the liquid, the mouth of the beaker being closed. A short time is allowed to elapse; the watch-glass is then removed, and its contents evaporated to dryness at a low temperature. A blood-red colour is developed on the addition of a little perchloride of iron to the dry residue. This effect is due to the absorption of the hydrocyanic acid vapour by the bisulphide of ammonium—sulphocyanide of ammonium being formed, which, on the addition of perchloride of iron, gives the blood-red colour of the sulphocyanide of iron, which is bleached by corrosive sublimate.
3. Silver Test.—This is the most successful of the vapour tests, a single apple pip yielding all the reactions. If a watch-glass containing a few drops of nitrate of silver solution be suspended in a beaker (as in 2), the silver solution will become white and opaque, from the formation of cyanide of silver; examined under the microscope it is seen to consist of small prismatic crystals. The cyanide as formed, treated with hydrochloric acid, liquor potassæ, and sulphate of iron, will give Prussian blue.
The Quantitative Analysis.—Use the precipitate of cyanide of silver, 100 grains being equal to 20.33 of pure anhydrous acid.
Treatment.—The treatment of poisoning by prussic acid is now to [Pg 372] be considered. As part of the general treatment, the stomach pump should be at once employed, and the stomach emptied and then washed out with water.
Ammonia.—The use of this substance was first advocated by Mr. John Murray of London, and is no doubt a valuable remedy if given early. Care should be taken that the mucous membrane of the air passages and alimentary canal be not inflamed by using too strong a solution.
Chlorine.—Recommended by Riauz in 1822. Water impregnated with the vapour of chlorine may be given internally, and the gas may be breathed under proper precautions.
Cold Affusion.—First proposed by Dr. Herbst of Göttingen. Its success is most to be looked for when it is employed before the convulsive stage of the poisoning is over. The cold water should be poured on the head and down the spine.
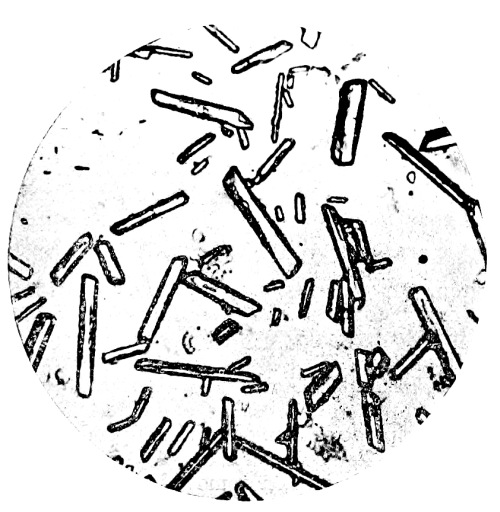
Fig. 39.—Photo-micrograph
of crystals of cyanide
of silver obtained by the vapour test, × 50.
(R. J. M. Buchanan.)
Bleeding from the Jugular Vein.—In one case treated by Magendie, bleeding from the jugular vein was attended with success.
Chemical Antidotes.—The administration of a solution of carbonate of potash, followed by a solution of the mixed sulphates of iron, has been suggested. The formation of Prussian blue is the result. The only objection to this treatment is, that prussic acid is so rapidly absorbed that death may result from the already absorbed acid before the antidote can be given.
Atropine.—This should be given hypodermically.
Peroxide of hydrogen should be given freely by means of the stomach tube. [Pg 373]
Cobalt nitrate 0.5 to 1 per cent. solution has been advocated hypodermically.
Sodium thiosulphate, in 10 per cent. solution, repeated hypodermically.
Cyanide of Potassium
This substance is used largely by photographers and electro-platers. It acts as a poison in a similar manner to hydrocyanic acid, and the symptoms are the same. As a commercial preparation it frequently contains undecomposed potassium carbonate, and may exert a corrosive action on the mucous membranes of the mouth and stomach, leading to the production of blood-stained mucus in the stomach.
Post-mortem Appearances.—These are the same as those described under hydrocyanic acid, with the addition of the corrosive effects.
Fatal Dose.—Five grains have proved fatal in a quarter of an hour; recovery has taken place after forty grains.
Chemical Analysis.—Same as for hydrocyanic acid.
Treatment.—As for hydrocyanic acid.
PREPARATIONS CONTAINING
HYDROCYANIC ACID
The following plants contain prussic acid, and are therefore more or less poisonous in proportion to the quantity of the acid which they severally contain:
Bitter Almonds
The essential oil of bitter almonds is very poisonous. “The oil does not, like common essential oils, exist ready formed in the almond, but it is only produced when the almond pulp comes in contact with water. It cannot be separated by any process whatever from the almond without the co-operation of water—neither, for example, by pressing out the fixed oil, nor by the action of ether, nor by the action of absolute alcohol. After the almond is exhausted by ether, the remaining pulp gives the essential oil as soon as it is moistened; but if it is also exhausted by alcohol, the essential oil is entirely lost. The reason is, that alcohol dissolves out a peculiar crystalline principle named Amygdalin, which, with the co-operation of water, forms the [Pg 374] essential oil by reacting on a variety of the albuminous principle in the almond, called Emulsin, or Synaptase.
The essential oil of bitter almonds may contain from 6.0 to 14.33 per cent. of hydrocyanic acid. Deaths from the incautious use of this oil for flavouring articles of confectionery are not infrequent. As the flavour is not in the least injured, it has been suggested to subject the oil to repeated distillation with caustic potassæ, by which means the oil is purified from prussic acid.
Symptoms in Man.—Nausea, vomiting, and diarrhœa, due to gastric irritation, have occurred when the dose has been small, as is the case when confectionery owes its flavour to the use of the essential oil. Idiosyncrasy may have something to do with these effects, for cases are on record where a single almond has produced a state resembling intoxication, followed by an eruption not unlike urticaria or nettle-rash. Taken in large doses, the symptoms produced are identical with those described under poisoning by prussic acid. The breath is usually strongly impregnated with the odour of bitter almonds.
Symptoms in Animals.—Vomiting, trembling, weakness, paralysis, tetanic convulsions, and coma.
Post-mortem Appearances.—These are identical with those seen in poisoning by the pure acid.
Fatal Dose.—The essential oil is from four to eight times as strong as the acid of the Pharmacopœia. From twenty to thirty drops have proved fatal. Death may take place in half an hour or less.
Treatment.—The same as that recommended under prussic acid.
Cherry-Laurel
The cherry-laurel, Prunus Laurocerasus—the leaves of which have been used for flavouring custards, &c.—contains prussic acid, and is therefore poisonous.
In the British Pharmacopœia there is an Aqua Laurocerasi—laurel water—prepared from the leaves. It contains 0.1 per cent. of hydrocyanic acid. It should be used with extreme caution, as the amount of hydrocyanic acid contained in the leaves is uncertain. Death has frequently resulted from its use. The most important case, however, is that of Sir T. Broughton. His mother, who gave him his usual draught on the morning of his death, observed that it had a strong smell of bitter almonds. Two minutes after he took it she observed a rattling or gurgling in his stomach; in ten minutes more he seemed inclined to doze; and five minutes afterwards she found him quite insensible, with the eyes fixed upwards, the teeth locked, froth running out of his mouth, and a great heaving at his stomach, and gurgling in his throat. He died within half an hour after swallowing the draught. No light was thrown on the case by the carelessly conducted post-mortem; but the suddenness of his death, the improbability of apoplexy occurring at so early an age, and the odour of bitter almonds observed by his mother, pointed out clearly enough the true cause of death.
All parts of this plant, the Aconitum Napellus (N.O. Ranunculaceæ), are poisonous. The poisonous properties depend upon the presence of an alkaloid—aconitine—chiefly found in the root.
Poisoning by the alkaloid came before the public mind in the case of Dr. Lamson, executed for the murder of his brother-in-law. The symptoms noticed in that case were very much as detailed below. When any part of the plant is chewed, a sensation of tingling is experienced in the mouth, and burning in the throat. Many of the aconites are, however, inert. The root, having been taken by mistake for horse-radish, has led to several cases of accidental poisoning.
| Aconite | Horse-Radish |
|---|---|
| General Characteristics.— | General Characteristics.— |
| Root conical; dark brown externally, | Root cylindrical, of nearly the same |
| and with numerous twisted rootlets; | thickness down its whole length. |
| internally, the colour is whitish. | Externally, buff-coloured; |
| internally, white. | |
| Taste.—Produces a tingling | Taste.—Sweet and pungent. |
| and numbing sensation in the mouth. |
Symptoms in Man.—The patient complains, within a short time after the poison is taken, of dryness of the throat, accompanied with tingling and numbness of the mouth and tongue. He then complains of nausea, vomiting, pain in the epigastrium, and distressing dyspnœa, of a sensation of formication or tingling, with numbness in his face and limbs, which appear to him heavy and enlarged. In attempting to walk he staggers, his limbs losing their power of supporting his body. He becomes giddy, his pupils dilated, and his sight and hearing imperfect; but he is seldom unconscious till near death. His pulse irregular, gradually becomes weaker, and at last almost imperceptible; his skin cold and clammy; his features pale and bloodless; and his mind clear: then suddenly he dies, in some cases from shock, in others from asphyxia; or he may die from syncope, especially after some exertion.
Symptoms in Animals.—Weakness of the limbs and staggering, the respiration slow and laboured, loss of sensation, paralysis, dimness of vision, increasing difficulty in breathing, convulsions, and death by asphyxia.
Delirium is present in some cases, and dilatation of the pupil has also been noticed. In a case recorded in the British Medical Journal, 1877, vol. i. p. 258, two ounces of the tincture of aconite were drunk in mistake for Succus Limonis; recovery took place, but not before alarming symptoms had taken place, and death at one time appeared imminent.
Post-mortem Appearances.—General venous congestion. The brain and its membranes are, in most cases, found congested and the stomach and intestines inflamed. [Pg 376]
Fatal Period.—The symptoms may come on immediately, or may be delayed for an hour or two. In the case mentioned in the British Medical Journal the patient walked about five miles after swallowing two ounces of the tincture, which he drank at 11 o‘clock, returning home at 2.30 P.M. An excise officer, who died in about four hours, was able to walk from the Custom House over London Bridge. Death has taken place in so short a time as one hour and a quarter.
Fatal Dose.—About two grains of the extract, and one drachm of the tincture. Much will depend upon the amount of the alkaloid present. One drachm of the scraped root is said to have proved fatal. One-fifteenth of a grain of aconitine has proved fatal.
Chemical Analysis and Tests.—The alkaloid must be isolated from the contents of the stomach by the process of Stas. The physiological test consists in placing a small portion of the extract, or the alkaloid so obtained, on the tongue or lip, and noting if tingling be produced. To the pure alkaloid, nitric acid added produces no change of colour. Officinal phosphoric acid added, and the mixture carefully evaporated, a violet colour is produced; this reaction is due to impurities in the aconitine.
Kundrat‘s Test.—A solution of ammonium vanadate in strong sulphuric acid produces a coffee colour with aconitine.
Treatment.—Emetics, stomach lavage, castor-oil, and animal charcoal should be given. The administration of digitalis in aconite poisoning has been attended with good results. (See British Medical Journal, 11th December 1872.) The drug may be given hypodermically as an antidote. Stimulants will be required; and friction down the spine, together with galvanism and artificial respiration, may be tried.
Synopsis of the Action of Aconite
1. On Nervous System.—Giddiness, numbness, and tingling in the limbs is a primary effect, followed by gradually increasing paralysis of the muscles, and insensibility of the surface of the body to pinching and pricking. Dr. Fleming asserts that it produces a powerful sedative effect on the nervous system. At any rate, it now seems to be proved that aconite paralyses the sensory nerves, commencing at their peripheral endings.
2. On Vascular System.—Extreme depression of the circulation is produced by doses large enough to cause death. The pulse may become imperceptible at the wrist. In medicinal doses, aconite lowers the heart‘s action; in poisonous doses, it causes fatal syncope.
3. On Digestive System.—Some have denied the irritant action of aconite on the alimentary canal, but Sir R. Christison states that he was deterred from the use of aconite “by two patients being attacked with severe vomiting, griping, and diarrhœa.”
The symptom most characteristic of these poisons is the marked anæsthesia which they produce when their vapours are inhaled. The hydrate of chloral, though placed under the above heading, is more closely allied in its action to opium than to ether or chloroform.
Ether, when taken in its liquid form, produces symptoms and post-mortem appearances not unlike those caused by alcohol.
Fatal Dose.—No death having been recorded, the fatal dose of this substance is unknown.
Ether Vapour.—The vapour of ether has caused death. Entering the blood through the lungs, it acts with great rapidity, a state of lethargy being quickly induced.
The early symptoms are noticed in a modification of respiration, the breathing becoming slow, prolonged, and stertorous. The face is pale, the lips bluish, and the surface of the body cold and exsanguine. The pulse, at first quickened, becomes slower, as the inhalation of the vapour is continued. The pupils are dilated, and the eyes glassy and fixed. The voluntary muscles of the body become flabby and relaxed, the patient still, however, having the power to move the limbs. The involuntary muscles are not affected; as an instance, the uterus contracts and expels its contents with ease. If the inhalation of the vapour be pushed too far, the pulse sinks, and coma ensues, from which the patient can only with difficulty be aroused; but if in an early stage the ether be discontinued, the patient quickly regains consciousness, due to the rapid elimination of the ether by the lungs. A marked peculiarity in this form of poisoning is the complete anæsthesia or paralysis of the nerves of sensation.
Post-mortem Appearances.—These are chiefly found in the brain and lungs, which in most cases are greatly congested. The cavities of the heart have been found full of dark-coloured liquid blood. A marked effect noticed in poisoning by ether is the congestion of the vessels of the upper portion of the spinal cord. The liver, kidneys, and spleen are sometimes congested.
Chemical Analysis.—The contents of the stomach and tissues must be treated and distilled, as described under alcohol. [Pg 378]
Tests:
1. The vapour passed into a solution of bichromate of potash, and sulphuric acid added, gives the reactions of alcohol.
2. The vapour burns with a smoky flame, depositing carbon on any cool surface placed above the flame.
3. It is but sparingly soluble in water, on which liquid it floats.
Treatment.—When the pulse becomes weak, and the breathing laboured and stertorous, the inhalation should be discontinued, and cold water dashed in the face—free ventilation being also allowed. Galvanism and artificial respiration should also be tried.
The effects produced by chloroform when swallowed are not unlike those occasioned by alcohol. Four ounces have been taken without causing death; it is, therefore, not an active poison in this form.
Chloroform Vapour.—The symptoms occasioned by chloroform when inhaled are not unlike those caused by ether, with this exception, that insensibility and general relaxation of the muscles are more rapidly produced.
Symptoms.—The symptoms of poisoning when chloroform is taken by the mouth are similar to those following inhalation, with irritation of the mucous membrane of the stomach and intestines. Vomiting generally occurs, the person becomes unconscious and comatose, the face cyanosed and the skin moist. The pupils are dilated and insensitive to light. The breathing is slow and stertorous, the pulse small and feeble. Death is due to respiratory paralysis first, and paralysis of the heart in addition, or the latter, according to some observers, may be the primary cause. On recovery diarrhœa may follow, with occasionally enlargement of the liver and jaundice.
Post-mortem Appearances.—Congestion of the vessels of the brain, and also of the lungs, is generally found. The cavities of the heart are usually empty; but, in some cases, the right side of the heart is found distended with dark-coloured fluid blood. Congestion of the spleen, liver, and kidneys is not of infrequent occurrence.
Fatal Period and Dose.—In one or two cases where the vapour was inhaled, death took place in from one to two minutes. Thirty drops thus taken destroyed life in one minute, and even fifteen drops have proved speedily fatal. It has thus destroyed life in a smaller dose, and more rapidly, than any other known poison. When swallowed, one fluid drachm has proved fatal in a boy, about four fluid drachms in an adult. Recovery has taken place after four fluid ounces. Three hours is the shortest fatal period after swallowing chloroform.
Chemical Analysis.—In searching for the presence of this substance in the blood or tissues, the examination should be made as [Pg 379] speedily as possible, as chloroform is thought by some observers to have a great tendency to pass into formic acid, and thus to escape recognition.
1. The substance to be examined should be placed in a flask, to which is adapted a glass tube bent at right angles. A piece of blue litmus paper, and another portion of paper moistened with iodide of potassium and starch paste, are inserted into the end of the glass tube. The flask and its contents should now be placed in a water bath heated to a temperature of 161° F. (72° C.), and a portion of the glass tube just past the bend heated to redness. Any chloroform vapour evolved from the contents of the flask is decomposed during its passage through the heated glass tube into free chlorine and hydrochloric acid, the presence of the former being indicated by the starch paper becoming blue; while at the same time the reddening of the litmus paper reveals the presence of the acid. As a further corroboration, the exit tube may be made to dip into nitrate of silver solution, when a precipitate of the curdy-white chloride of silver will take place, insoluble in nitric acid, but dissolving on the addition of ammonia. Every 100 parts of chloride of silver formed, equals 27.758 of chloroform. By this process chloroform has been detected four weeks after death in putrid organs.
2. Chloroform may be separated from organic mixtures by distillation. If aniline and alcoholic solution of potash be added to chloroform and heated, the peculiar odour of phenyl-isocyanide is given off.
3. A solution of β-naphthol dissolved in caustic potash, when added to chloroform and heated, gives a blue colour.
4. Chloroform reduces Fehling‘s solution.
Treatment.—The same as recommended with regard to ether. M. Nelaton recommends inversion of the body, and ascribes the recovery of one patient to his suddenly lifting him up and throwing him over his shoulder with his head hanging down.
This substance is largely used in certain industries, as it dissolves oils, fats, caoutchouc, gutta percha, &c. It is very inflammable, burns with a blue flame, evolving sulphur dioxide. The odour, when this substance is impure, is very disagreeable. If taken internally, it produces an intense burning sensation in the throat, headache, and giddiness. In chronic poisoning from the vapour in manufactories where it is used, there appear to be two stages—one of excitement, and one of depression. In the former, there are more or less persistent headache, irritability of temper, tinnitus aurium, and even mania; in the latter, anæsthesia of the skin, even affecting the mucous membranes, patients complaining that their tongues feel as if tied in a cloth. Paralysis of the limbs has been noted in prolonged cases of chronic poisoning. The post-mortem appearances do not differ [Pg 380] much from those found after death from the inhalation of chloroform. Carbon bisulphide may be separated from organic liquids by distillation, and detected by its odour, and by a black precipitate of sulphide of lead when heated with nitrate of lead and potash.
This substance is prepared by acting on alcohol by chlorine. It is used extensively as a hypnotic, and, owing to its indiscriminate use, many fatal cases have been recorded. Care should be taken when large doses are given not to repeat them too quickly, as there appears to be a tendency to accumulation, and sudden and dangerous action of the drug.
Symptoms.—Chloral, in moderate doses, acts on the brain as a powerful hypnotic, the early symptoms being gradual drowsiness, followed by deep sleep. With a dose of about 30 grains, the patient can, however, by walking about, ward off sleep. In large doses the narcosis becomes completely uncontrollable, and the poison then acts as a depressant to the basal ganglia of the brain, and on the spinal cord; and, as a result, there is weakness of the heart‘s action, with ultimate diastolic arrest, slowing of the respiratory movements, and general muscular weakness, with some anæsthesia. Under these circumstances the patient has all the appearance of a drunken person, the face is flushed, and the deep sleep may pass imperceptibly into death without any marked change. In some cases delirium precedes the condition of sleep. The pulse in some cases is quickened, and the face flushed; but, in other cases, the pulse becomes slow and almost imperceptible, the heart being ultimately arrested in diastole. In these cases the face is pale, and the breathing performed at long intervals. The motor paralysis present, when a poisonous dose is taken, is due to the action of the drug on the spinal cord, and not on the nerves. During the sleep produced by chloral, the pupils are contracted, but dilate on the person awakening. In a case described by Dr. Levinstein, and reported in the Lancet, 21st February 1874, the patient took six drachms with intent to commit suicide. The face was at first flushed, the veins swollen, and the pulse 160 per minute; he then became livid, the pupils contracted, and at times the circulation appeared to be entirely arrested. The temperature varied from 32.9° C. to 38.7° C. (89.6° F. to 100.4° F.). This case recovered under treatment by the subcutaneous injections of strychnine (.03 to .04 grain), and the use of faradisation in thirty-two hours after the poison had been taken. Chronic chloral poisoning, “chloral-drinking,” has unfortunately become far too common of late years, in which the mental faculties suffer severely, so that in our asylums, cases of mania and melancholia are rightly (or wrongly) attributed to the habit. A peculiar eruption, not unlike that produced by shell-fish, and followed by desquamation, sometimes occurs when this substance has been given for some time in medicinal doses.
Post-mortem Appearances.—These are not unlike those of asphyxia, the vessels of the brain being engorged, and the ventricles [Pg 381] containing an abnormal quantity of fluid. The mucous membrane of the larynx may be injected, and in some cases œdematous. The right side of the heart is engorged and the left empty, together with congestion of the lungs. Chloral is very little decomposed into chloroform by the blood. W. H. Roberts has in several cases recovered it as chloral from the blood.
Fatal Dose.—The fatal dose cannot be accurately stated, but children, as in the case of belladonna, are said to bear the drug better than adults. A child a year old died in ten hours from a dose of three grains. Ten grains proved fatal to an old lady seventy years of age. Twenty grains has caused death in an adult in half an hour, and in one case thirty grains. As a rule, any quantity over two drachms may be considered a dangerous, if not a fatal dose, although recovery has been stated to have occurred after one ounce. Dr. Richardson considers 120 grains, distributed over twenty-four hours, as a safe dose for an adult. Death may take place suddenly, or after the lapse of several hours.
Fatal Period.—From fifteen minutes, which is the shortest time on record, to thirty-nine and a half hours, which is the longest period recorded.
Chemical Analysis.—Chloral may be extracted from the stomach contents by digestion with absolute alcohol acidified by sulphuric acid. The alcoholic extract is filtered and evaporated. The residue is treated with petroleum ether to remove fatty substances, and finally shaken with pure ether to remove the chloral. On evaporating the ether the chloral hydrate is left. From urine it may be extracted by first acidifying with sulphuric acid and then treating it with petroleum ether and ether. Chloral hydrate in solution gives the following reactions:—
1. On agitation with solution of caustic potash, and gently warmed if necessary, chloroform is evolved, which can be detected by its odour. From a strong solution the chloroform may separate in the form of minute globules.
2. If one drop of ammonium sulphide be added to a solution of chloral hydrate and gently heated, a peculiar opalescent milky reddish-yellow precipitate forms. This test is extremely delicate, and differentiates chloral hydrate from chloroform.
3. Alcoholic solution of potash and aniline when added to chloral hydrate solution, shaken up and warmed, produces the peculiar odour of phenyl-isocyanide. This is due to the formation of chloroform on the addition of the caustic potash.
4. If β-naphthol dissolved in caustic potash solution be added to a solution of chloral hydrate and the mixture warmed, a blue colour is produced.
5. Chloral hydrate reduces Fehling‘s solution.
To separate chloroform in the stomach contents from chloral hydrate they should be acidified with tartaric acid and distilled, when the chloroform which was free in the stomach will pass over to the receiver. If the residue be now rendered alkaline with caustic potash and again distilled, any chloroform which then comes over must have been derived from chloral hydrate in the stomach contents. [Pg 382]
Treatment.—The treatment consists in washing out the stomach, the administration of emetics, or hypodermic injection of apomorphine, in the use of galvanism, friction, mustard-plasters to the calves of the legs, artificial respiration, and the hypodermic injection of a solution of nitrate of strychnia or injection of atropine. The warmth of the body must be carefully maintained in all cases by suitable external applications. Oxygen inhalations are said to be beneficial.
Sulphonal is a product of the oxidation of mercaptol, obtained from acetone and mercaptan; it occurs in tasteless, odourless, colourless crystals or powder, was introduced into medical practice in 1888, and has since caused many accidental deaths. The habit of taking it may be acquired. It has a tendency to accumulative action when taken for some time without interruption. A serious feature in most of the cases of poisoning is that usually those taking it have been apparently benefited by the drug up to the time of the appearance of toxic symptoms.
Symptoms.—In medicinal doses (15-30 grains) it has an action similar to that of paraldehyde, it causes sleep with little depression of the circulation and respiration. Larger doses produce variable symptoms, mental confusion with nervous ataxic manifestations, stupor, and insensibility; less frequently excitement and convulsions. Skin eruptions may follow a large dose or from its long continued use. In severe cases there is marked cyanosis, feeble pulse, and stertorous and irregular breathing. Death usually results from failure of respiration, or the urine may be suppressed and fatal coma supervene. Albuminuria and hæmatoporphyrinuria are common features, especially in chronic cases. The deep pink colour of the urine was attributed to hæmatoporphyrin, and indicating extensive destruction of the red blood corpuscles. It is a grave symptom. That the colour of the urine is due to hæmatoporphyrin is questionable, for on removing the hæmatoporphyrin the colour remains the same. The cumulative action is due to slow elimination by the kidneys. A case published by Drs. Taylor and Sailer, and reported in the Lancet, February 1900, was that of a woman aged fifty-two years, unmarried, and presenting symptoms of hysteria. On inquiry it was discovered that she had been in the habit of taking sulphonal for some time, the dose being fifteen grains per diem. She was informed of the evil results likely to follow the continued use of the drug, and she discontinued its use for some weeks. After this she resumed taking the drug, and began speedily to exhibit all the symptoms of sulphonal poisoning: viz. mental confusion, marked insomnia, difficulty of speech, and a peculiar sighing dyspnœa. The urine was tinged a deep pink colour (hæmatoporphyrinuria), and a stiffness and paralysis of both legs soon developed. The control of the sphincters was lost. Cutaneous sensibility was not affected. The paralysis spread rapidly upwards, and death resulted from cardiac failure. Spectroscopic examination of both urine and blood disclosed the presence of [Pg 383] hæmatoporphyrin. At the necropsy the following conditions were revealed: fatty degeneration was present in the heart, liver, and kidneys. The spleen was filled with a greenish pigment, both free and within the lymphoid corpuscles, the fibrous trabeculæ were greatly increased in size, and the lymphoid follicles were extremely well developed. Excessive pigmentation was found also in the lymphatic glands of the body and in the lungs. No morbid changes could be found in the spinal cord or brain.
Fatal Dose.—This is very uncertain, depending upon idiosyncrasy. Thirty grains has caused death in a woman in forty hours, while a case is reported in the Lancet, January 1904, of recovery after the taking of 365 grains. In many cases death has followed the daily use of moderate doses (10-20 grains) for several months.
Fatal Period.—May occur in a few hours, or days, or after months; also after the use of the drug has been discontinued.
Chemical Analysis.—Sulphonal is very stable, and is unaffected by boiling alkalies or by concentrated nitric or sulphuric acids. From its solution in concentrated sulphuric acid it may be recovered by dilution. It is easily recovered from the body after death, as its stability prevents its decomposition. It is isolated from organic matter by treatment with alcohol, evaporation, and extraction of the residue with hot water, evaporation and final extraction with ether.
Tests.—1. Heated in a test tube with powdered charcoal, sulphonal forms mercaptan, acetic acid, formic acid, and sulphur dioxide. The offensive odour of mercaptan may be noted, and the vapours will change blue litmus paper. Sulphur dioxide may be shown by its bleaching action on a piece of filter paper moistened with blue starch iodide and suspended in the mouth of the tube.
2. When melted with potassium cyanide, sulphonal develops a mercaptan odour, and potassium sulphocyanate is formed at the same time. A blood-red colour is therefore produced on the addition of ferric chloride to a solution of the residue in water. Great care must be exercised in the carrying out of this test, as it is somewhat dangerous to the experimenter.
Treatment.—The stomach should be washed out in order to remove any drug unabsorbed. Diuretics, purgatives, and general stimulants given, such as strychnine, hot coffee, &c.
These compounds are very similar in both their chemical and physiological properties to sulphonal, but both have a bitter taste. Both have caused fatal poisoning, the symptoms being very similar to those caused by sulphonal.
Veronal, a synthetic compound, is a white crystalline powder about four times as powerful as sulphonal, very slightly soluble in water, more soluble in hot water, and in alkaline solutions, and absorption takes place from the intestine. [Pg 384]
Symptoms.—In moderate doses it produces sleep without subsequent depression, and does not affect temperature or respiration. In larger doses it may cause erythema and constipation, with alternating semi-coma and delirium. During the last few years fatal cases of poisoning have become rather frequent.
Details of a fatal case by Dr. Durrant reported in Taylor, p. 616, are, briefly: A man aged thirty-three, a heavy drinker, to whom veronal had been prescribed, in fifteen-grain doses, with chloral hydrate and bromide of ammonium, had gradually increased the dose from 15 to 30 grains, or even 60 grains. Five weeks before death he had taken 100 grains, and had recovered in three days. Nine hours after taking 120 grains of veronal with 20 grains of chloral and 40 grains of ammonium bromide he was found deeply comatose, with surface warm, respirations 32, pulse 102, pupils dilated, corneæ insensitive, reflexes absent. Next day not so deeply comatose, he could be made to wince by slapping the face, the pupils were still dilated, temperature 102° F., pulse 110, reflexes still absent. Later he was still constipated, and the breathing impeded by mucus. On the third day he spoke when roused; the temperature, bowels, and pupils the same. With slight remission he became worse, and on the fourth day, in a comatose condition, with muscular flaccidity and absence of reflexes, temperature 104° F., respirations over 40, and the pulse 150, death took place. Post-mortem.—Nothing was found except intense congestion of the lungs, liver, spleen, and brain, due, no doubt, to the asphyxial form of death. The mucous membrane of the alimentary canal was congested, but otherwise normal.
Chemical Tests.—1. Heated dry with sodium carbonate, ammonia is evolved. If held in the mouth of the tube red litmus paper turns blue, turmeric paper brown.
2. A saturated solution acidified with nitric acid gives a white precipitate with Millon‘s reagent soluble in excess.
Treatment.—As for sulphonal.
The common or spotted hemlock, Conium maculatum (N. O. Umbelliferæ), is indigenous. It must be distinguished from the Myrrhis temulenta, another indigenous, umbelliferous plant, which has also a spotted stem, but which is covered with hairs—the stem of the hemlock being smooth. Several cases of poisoning have occurred, hemlock having been mistaken for parsley, fennel, asparagus, and parsnip. The leaves of the plant have a peculiar mousy odour, which is intensified when they are rubbed in a mortar with some caustic potash. The poisonous properties reside in an alkaloid, conine. The activity of the plant appears to depend upon the time of the year when it is gathered, being most powerful in May. The ready decomposition of the alkaloid by heat or age renders the extract of conium a very uncertain preparation, the conine being converted into an inert resinoid matter.
Conine the alkaloid is a colourless volatile oil, lighter than water, with an odour of mice. It is strongly alkaline, soluble in diluted acid, but its salts have not yet been crystallised. It has been suggested that a ptomaine not unlike conine may be formed in the body by the combination of one molecule of butyric acid and one molecule of ammonia with separation of water, thus:
| Butyric Acid. | Ammonia. | Conine. | |||
| 2C₄H₈O₂ | + | NH₃ | - | 2H₂O = | C₈H₁₅N |
Conine is a deadly poison, killing all animals, death resulting from asphyxia. Neutralised with an acid, its activity is increased, and it becomes more soluble in water. Almost instant death resulted in a dog from injecting two grains of conine, neutralised with hydrochloric acid, into the femoral vein.
Symptoms in Man.—The symptoms in some cases resemble those of poisoning with opium; in others, the patient complains of dryness and constriction of the throat, and drowsiness. There is dilatation of the pupil, with closure of the eyes or ptosis, and loss of power in the muscles of the extremities, so that the patient falls on attempting to walk. The paralysis does not appear to be due to any direct influence upon the muscles, but upon the motor nerves, and especially on their extreme peripheral ends, and in this differs from Calabar bean, which acts on the spinal cord. Gradual loss of power in the respiratory [Pg 386] muscles is the cause of death. Giddiness, coma, and convulsions were the typical symptoms of two cases of accidental poisoning recorded by Dr. Watson.
Symptoms in Animals.—“Palsy, first of the voluntary muscles, next of the chest, lastly of the diaphragm—asphyxia, in short, from paralysis, without insensibility, and with slight occasional twitches only of the limbs; and the heart was always found contracting vigorously for a long time after death” (Christison).
Post-mortem Appearances.—Congestion of the vessels of the brain and lungs. The blood is very fluid, and of a dark colour, the fluidity due probably to the mode of death—slowly induced asphyxia. There may be some redness of the mucous membrane of the alimentary canal.
Fatal Period.—The symptoms may come on in from ten minutes to an hour, or more, after the poison has been taken. Death usually takes place in about four hours.
Fatal Dose.—Uncertain. Thirty grains of the extract carefully prepared killed a rabbit in five minutes. A single drop of conine dropped into the eye of a rabbit killed it in nine minutes.
Chemical Analysis.—Conine may be extracted from organic mixture by the general process for extracting alkaloids. The following tests may then be applied:
1. The odour of conine, when diluted with water, resembles that of mice. Harley states that a mixture of caustic potash with organic substances may evolve a similar odour even when conine is absent.
2. On warming conine with sulphuric acid and potassium bichromate butyric acid is produced, and can be recognised by its peculiar odour.
3. If conine be added to a solution of alloxan a reddish-purple colour is produced in a few minutes, and white needle-shaped crystals form on standing. These crystals if dissolved in caustic potash solution produce a purple colour, and the odour of conine is given off.
Treatment.—Emetics, stomach pump, castor-oil, followed by ammonia and other diffusible stimulants. Artificial respiration should be resorted to and kept up for a long time.
A strong emulsion of Calabar bean, Physostigma venenosum (N.O. Leguminosæ), is used on the West Coast of Africa as a test of innocence in cases of suspected witchcraft. In 1864 some children in Liverpool were poisoned by eating some of these beans, which had been swept out of a ship from Africa on to a heap of rubbish. The poisonous alkaloid is physostigmine or eserine.
Symptoms.—Vomiting, giddiness, irregular action of the heart. The mental faculties are unaffected. The eyes are bright and the pupils contracted; in which latter it differs most strikingly from atropine, hyoscyamine, and daturine, where dilatation of the pupil is the rule. The late Sir R. Christison considered that its primary action is on the heart, causing paralysis of that organ, and that the insensibility and coma are only secondary. Dr. Harley considers that it [Pg 387] is not a cardiac, but a respiratory poison. Later experiments have shown that the paralysis produced is due to the action of the drug on the spinal cord and not on the nerve trunks. It appears also that death is due to a failure of the respiration, for the heart in animals has been found still beating for one and a half hours after death. The contraction of the pupil, when locally applied, is probably brought about by its paralytic action on the peripheral sympathetic nerve fibres of the iris; and it is stated that when very large doses of physostigmine are given, the pupils dilate, pointing to oculo-motor palsy. A few drops of the extract placed in the eye cause powerful contraction of the pupil.
Fatal Dose.—Six beans produced death in a boy six years of age.
Chemical Analysis.—The alkaloid eserine should be extracted in the usual way, benzene being used as a solvent in the place of chloroform and ether.
Eserine gives the following chemical reactions:
1. If an aqueous solution of the salt be boiled and then strong nitric acid added, the solution turns a yellowish-orange colour, changed to violet on addition of caustic soda in excess; the violet is discharged on acidulation, but returns on re-alkalising the solution.
2. A solution of eserine in ammonia solution gives a blue residue on evaporation to dryness. Dilute acids produce a red-coloured solution with it, which is fluorescent by reflected light.
3. Bromine water produces a red turbid solution with eserine, which clears on heating.
4. The physiological test—eserine solution instilled into the eye of an animal produces contraction of the pupil.
Treatment.—The stomach should be emptied and washed out by means of the syphon tube, or emetics administered. One-fiftieth to one thirtieth of a grain of atropine sulphate should be administered hypodermically and repeated until the pupils dilate. The tincture of belladonna may be given by the mouth. Stimulants should be given and artificial respiration carried out if required.
NUX VOMICA STRYCHNINE
Some of the most poisonous known plants belong to the genus Strychnos (N.O. Loganiaceæ).
The Java poison, Upas Tieuté, is a watery extract of S. Tieuté; the basis of the poison used in Guiana, and known as Wourali, Ourari, Urari, or Curare, is the juice of S. toxifera. S. nux vomica, the Koochla tree, produces the nux vomica seeds of commerce; and the bark of the tree has been accidentally substituted for cusparia, or angustura bark, hence it is known as false angustura bark. The substitution is attended with considerable risk, on account of the strychnine which the false bark contains. It may be known by its being quilled, externally covered with white lichenous spots, and the internal surface becoming blood-red when touched with nitric acid. This reaction, which depends upon the presence of an alkaloid, brucine, does not occur when true angustura bark is thus treated.
The Seeds of S. Nux Vomica
The British Pharmacopœia contains an extract and a tincture. The alkaloid strychnine is the active principle of the seeds and other parts of the plant. Another alkaloid, brucine, is also found, and is poisonous.
The symptoms and post-mortem appearances and treatment will be detailed under the head of strychnine. The brown powder of the seeds may, in some cases, be seen adhering to the mucous membrane of the stomach.
Strychnine is very slightly soluble in cold water to the extent of one part in 8300; in boiling water one part dissolves in about 2500. It is more soluble in alcohol, and very soluble in chloroform or ether and chloroform mixed.
It has a bitter taste, so intense, that one part in 70,000 of water can be detected by the taste. Strychnine is not easily decomposed—it resists the action of warm strong sulphuric acid, and is not altered by putrefactive processes when present in viscera. It has been discovered in the body 322 days after death in one case, 368 days in another. [Pg 389]
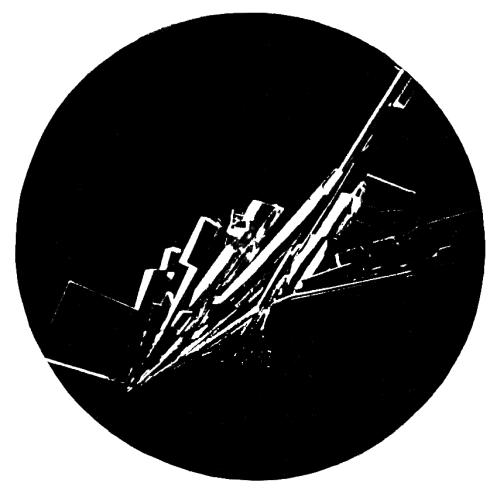
Fig. 40.—Photo-micrograph
of crystals of
strychnine sulphate from aqueous solution, × 50.
(R. J. M. Buchanan.)
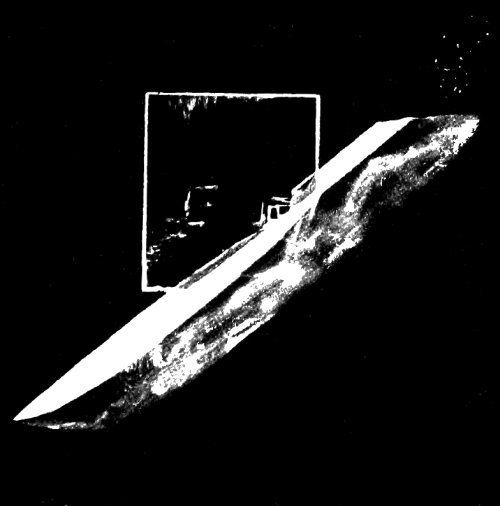
Fig. 41.—Photo-micrograph
of crystal of
strychnine sulphate from aqueous solution, × 50.
(R. J. M. Buchanan.)
[Pg 390] Allen detected strychnine in the residue of some viscera from a person who had died of strychnine poisoning, and which he had kept in a jar for six years. Richter found the alkaloid at the end of eleven years in putrid tissues which had been exposed to the air all that time in open vessels.
Symptoms.—Should the poison be in solution, the patient complains of a hot and intensely bitter taste during swallowing. The effects of the poison depending to a great extent on the mode of administration, become manifest in from a few minutes to an hour or more after it is taken. The earliest symptoms are a feeling of suffocation and great difficulty of breathing. These come on suddenly, without any premonitory warnings. Twitching of the muscles rapidly pass into tetanic convulsions of nearly all the muscles of the body, which are simultaneously affected. The head after several jerks becomes stiffened; the neck rigid; the body curved forward, quite stiff, and resting on the back of the head and heels. The face is congested, and the countenance expresses intense anxiety; the eyes staring, the mouth open, and the lips livid. The throat is dry, the thirst great; but when an attempt is made to drink, the jaws are spasmodically closed, and a piece of the vessel may be bitten out. During the intervals of the paroxysms the intellect is usually clear, and the patient appears conscious of his danger, frequently exclaiming, “I shall die!” He is also conscious of the accession of the paroxysms, telling those around him of their approach, and asking to be held. In the case of J. P. Cook, poisoned by Palmer, those about him tried to raise him, but he was so stiff that they found it impossible. He then said, “Turn me over,” which they did, and he died in a few minutes. Intense pain is felt, due to the powerful contractions of the muscles. After the lapse of a minute or two, the spasms subside, a sudden lull takes place, during which the patient feels exhausted and his skin is bathed in sweat.
In poisoning by strychnine, the jaws are slightly, if at all, affected, trismus is a late symptom, and occurs only during a convulsive seizure.
In tetanus the result of disease, the locking of the jaws is an early and a marked symptom.
As death approaches the fits become more frequent, and the patient dies from exhaustion or suffocation.
Post-mortem Appearances.—There is no characteristic appearance found after death. The blood is fluid, the heart empty, with some congestion of the membranes of the brain. Absence of all cause for so violent and sudden a death. Rigor mortis is prolonged for some time.
Fatal Period.—The rapidity in the accession of the symptoms and fatal termination will, to some extent, depend upon the form in which the poison is taken—i.e. in solution or in pill. In most cases the symptoms appear in from three or four minutes to an hour or more after the poison is swallowed, death following in from ten minutes to six hours. As a rule, if the person lives for two hours after the onset of symptoms recovery may be expected. [Pg 391]
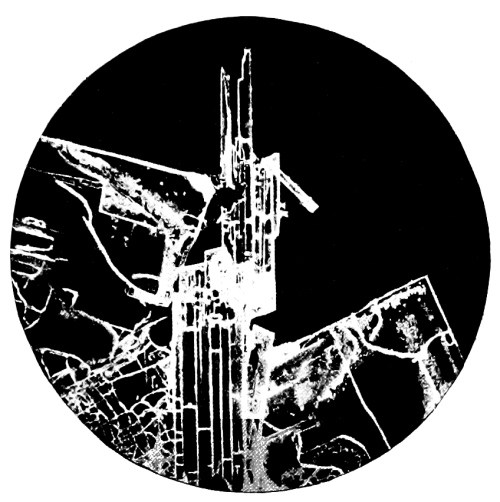
Fig. 42.—Photo-micrograph
of strychnine sulphate,
film preparation from chloroform solution, × 50.
(R. J. M. Buchanan.)
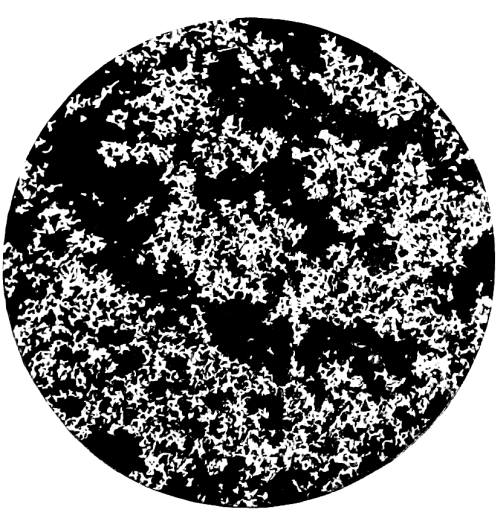
Fig. 43.—Photo-micrograph of
chromate of strychnine, × 50.
(R. J. M. Buchanan.)
[Pg 392] Fatal Dose.—A quarter to half a grain; but large doses have been taken, followed by recovery.
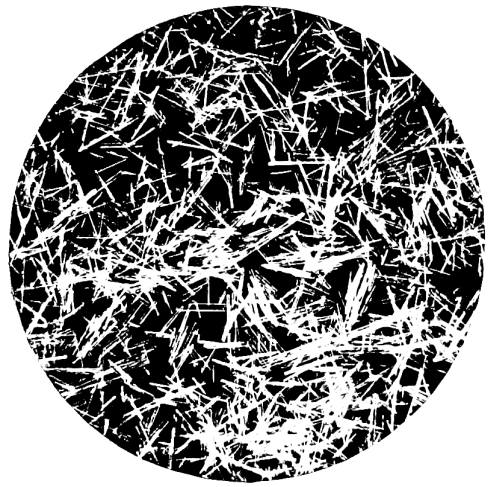
Fig. 44.—Photo-micrograph
of
sulphocyanate of strychnine, × 50.
(R. J. M. Buchanan.)
Chemical Analysis.—The poison may fail to be detected, and this link in the scientific evidence may be wanting, as was the case in Palmer‘s trial. In that case the strychnine had been administered in pills; and when after death the stomach had been cut open, and the contents lost, there was little hope of discovering the poison. The non-discovery of the poison was made a strong point on the part of the defence, ignoring at the same time the fact that the stomach had been tampered with and the contents spilt. The alkaloid abstracted from the tissues or contents of the stomach by the process generally used for extraction of alkaloids, may have the following tests applied to it:
1. Scarcely soluble in water, but readily soluble in acidulated water.
2. Intensely bitter taste.
3. Not affected by sulphuric acid; but when a little peroxide of lead, or peroxide of manganese, or bichromate of potash, or ferricyanide or permanganate of potassium is added, a magnificent purple-blue colour, changing to crimson, and finally to a light red tint, is the result. The ¹/₂₀₀₀₀ part of a grain of strychnine has been stated to give this reaction.
4. The physiological test consists in introducing a small quantity of the suspected substance under the skin of a frog, and noting whether or not the animal suffers from tetanic spasms.
5. The Galvanic Test.—Place a solution of strychnine, say one part of strychnine in 15,000 of water, in a slight depression in a piece of platinum foil, and allow the mixture to [Pg 393] evaporate. When dry, moisten the spot with sulphuric acid, connect the foil with a positive pole of a single-cell Grove‘s battery, and then touch the acid solution with the negative pole. A violet colour will be at once produced, remaining permanent.
6. Bloxam‘s Test.—To the solid alkaloid in a porcelain dish a drop or two of strong nitric acid is added and gently heated; on adding a small quantity of potassium chlorate a scarlet colour is produced. Ammonia changes this colour to brown and a brown precipitate falls. If the mixture he evaporated to dryness it leaves a dark green residue forming a green solution in water, changed to orange-brown with caustic potash and green again with nitric acid. This test distinguishes strychnine from any of the alkaloids which commonly occur in cases of poisoning.
7. Potassium bichromate when added to a solution of a salt of strychnine, produces a yellow crystalline precipitate of chromate of strychnine: the reaction can be done on a microscope slide and the crystals examined. On drying the crystals and then touching them with a drop of strong sulphuric acid, the purple colour changing through red to green is produced.
8. Picric acid gives a yellow crystalline precipitate of the picrate.
9. Ammonium or potassium sulphocyanate produces crystalline precipitates.
10. Ferri-cyanide of potassium produces a crystalline precipitate with solutions of salts of strychnine.
Strychnine may not be found in the body, even after death from poisoning by it, for the following reasons:
1. Smallness of the quantity taken.
2. The time which has elapsed after taking the strychnine until the symptoms commence.
3. If the careful preservation of the stomach and its contents has been overlooked.
4. The alkaloid may have been eliminated from the body before death.
Treatment.—Evacuation of the stomach by emetics and the stomach pump, under anæsthesia, and then the administration of animal charcoal, iodide of potash, tannic acid, and tea; bromide of potassium in large doses (half an ounce), and repeated in smaller doses. Chloral should be given in five-grain doses hypodermically every ten minutes, until the convulsions are subdued. Chloroform should be inhaled for some time. Urethane is said by Anrep to be more useful than chloral, and should be given in drachm doses.
This alkaloid is present along with strychnine in Nux Vomica seeds and the Ignatius bean. Cases of poisoning by it seldom occur, as the alkaloid is but little known by the public.
Symptoms.—It resembles strychnine in its action but is much less poisonous. It produces death by convulsions when injected subcutaneously, but according to Brunton does not so often produce convulsions when taken into the stomach. [Pg 394]
Differential Diagnosis of Strychnine Poisoning from
Tetanus, Hysteria, Epilepsy, and other
Poisons causing Tetanic Spasms.
| Tetanus. | Tetanus from Strychnine. |
|---|---|
| 1. The presence of a wound. | 1. Some solid or liquid |
| Symptoms have no connection | taken within a short time |
| with any liquid or solid | of commencement of symptoms. |
| swallowed. | Not connected with any |
| peculiarity of constitution. | |
| 2. Gradual accession and | 2. Symptoms sudden and |
| progress of the symptoms; | violent. All the muscles are |
| difficulty in swallowing; | affected at one and the same |
| stiffness of the jaws, neck, | time. Arms affected and |
| trunk, legs, and arms. The | hands clenched at the same |
| hands not generally affected. | time as the body and legs. |
| Jaw only affected or fixed | |
| during efforts to swallow. | |
| 3. Curving of the spine forwards | 3. Opisthotonos an early |
| not primarily present; | symptom, generally |
| generally comes on after some | appearing in a few minutes. |
| days of previous illness. | |
| 4. Symptoms may undergo | 4. Intervals of complete |
| abatement, but there is no | intermission. |
| perfect intermission. | |
| 5. Death after the lapse of | 5. Death usually occurs in |
| several hours or days. Direct | two hours, or even less |
| injury to spinal cord may give | than a quarter of an hour. |
| rise to tetanus and death in | Recovery in a few hours. |
| a few hours. Recovery slow. |
| Hysteria. | Epilepsy. | Tetanus occurring During the Action of other Poisons. |
|---|---|---|
| 1. Connected with | 1. Previous | 1. The presence of |
| a peculiar | history of | other symptoms of |
| constitution. | epilepsy. | poisoning peculiar |
| to certain poisons. | ||
| 2. The presence of | 2. Presence of the | |
| known stigmata | aura epileptica. | |
| of hysteria. | The tongue bitten; | Obs.—Arsenic, |
| and insensibility | antimony, and | |
| lasting for | other irritant | |
| some time. | poisons may | |
| 3. The spasms | 3. Alternate | sometimes cause |
| frequently | contraction and | tetanic spasms; |
| convulsive, and | relaxation of | but other symptoms |
| alternating with | the muscles. | are present which |
| stiffness of the | point to the nature | |
| muscles. Loss | of the poison. | |
| of consciousness. | ||
| 4. | ||
| 5. Never fatal. | 5. Seldom fatal | |
| Recovery very | during first | |
| rapid. | attack. |
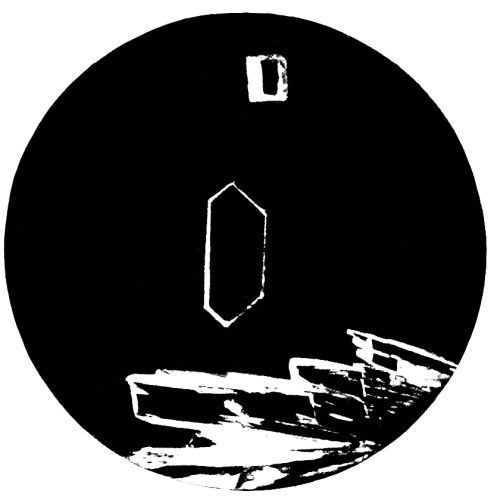
Fig. 45.—Photo-micrograph of
crystals of brucine sulphate, × 50.
(R. J. M. Buchanan.)

Fig. 46.—Photo-micrograph of
crystals of brucine sulphate, × 50.
(R. J. M. Buchanan.)
[Pg 396] Chemical Analysis.—The alkaloid may be extracted from organic admixture by the usual methods. Its reactions to special tests are as follows:
1. If nitric acid be added to the solid alkaloid, or in aqueous solution, a bright red colour is produced which changes to yellow on heating. The addition of stannous chloride or sulphide of ammonium to the acid solution after cooling changes it to violet; the colour is discharged by excess of the stannous chloride. If the red acid solution be largely diluted with water, a yellow precipitate falls, soluble in dilute hydrochloric acid. If the filtrate from the yellow precipitate be neutralised by ammonia and calcium chloride added, a precipitate of calcium oxalate forms, insoluble in acetic but soluble in hydrochloric acid. This reaction is peculiar to brucine.
2. With sulphuric acid and potassium bichromate a deep orange-red colour is produced.
3. Sulphomolybdic acid gives an orange-red or purplish-red colour, changing to blue.
4. Blyth‘s Test.—If methyl iodide be added to a solution of brucine in strong alcohol, circular rosettes of crystals form in a few minutes. Strychnine does not give this reaction.
Treatment.—Same as for strychnine.
Circumstances under which it occurs accidentally.—Death may result where several persons are sleeping in the same room, and the ventilation is imperfect; from the admission of the vapour of charcoal into a room from an adjoining vent; or from incautiously sleeping in a brewery close to a vat in which fermentation is going on. Many deaths have occurred from this gas, due to the incautious descent into wells. It must also be borne in mind that death may result from the presence of this gas in an atmosphere which will permit the combustion of a candle. For a candle will burn in an atmosphere containing 25 per cent. of CO₂, whereas 5 per cent. will cause death. The burning of a candle is therefore no test of security from danger in an atmosphere where the presence of carbonic acid is suspected. Carbonic acid does not, as is generally supposed, sink to the lower portions of a room; and Dr. Taylor, from his experiments, states “that in a small and close room persons are liable to be suffocated at all levels, from the very equal and rapid diffusion of carbonic acid during combustion.”
Symptoms.—When the carbonic acid is pure, that is, unmixed with other gases, spasm of the glottis at once occurs, and the sufferer falls down insensible, and death is almost immediate. When the gas is diluted the early symptoms are a feeling of weight and fulness in the head, accompanied with giddiness, throbbing of the temporal arteries, drowsiness, palpitation of the heart, gradually increasing insensibility, stertorous breathing, ending in death from asphyxia or apoplexy. Sometimes the victim dies convulsed, at other times a deep sleep quietly merges into death. The symptoms will, of course, depend upon the quantity and purity of the gas present in the apartment.
Action on the Animal Economy.—The opinions of observers vary greatly—Berzelius maintaining that an atmosphere containing 5 per cent. was not injurious to life; Allen and Pepys, on the other hand, stating that 10 per cent. of the gas would cause death. Bernard considers that it is not poisonous, as it can be injected into the bodies of animals without injury, and that its action is purely negative; it is irrespirable in the same sense as pure hydrogen or nitrogen is—simply, therefore, causing death by suffocation. Whatever may be the true explanation of its action, it is enough for all practical purposes to know that death follows when it is breathed, even when mixed with a normal amount of oxygen. [Pg 398]
Post-mortem Appearances.—The face may be pale and composed, or swollen and livid. The vessels of the brain are frequently greatly congested, and the heart and great vessels gorged with black fluid blood. The blood in some cases, however, is of a cherry-red colour. This may probably be due to the presence of carbon monoxide, which appears to have the power of preventing the change of arterial into venous blood, the opposite effect to that of carbon dioxide. The tongue may or may not be protruded beyond the teeth; in most instances the latter is the case. Animal heat is long retained after death, and the rigor mortis occurs as in other forms of death.
Treatment.—Bleeding from the arm, cupping from the nape of the neck, and the employment of cold affusion to the head. The patient should be removed without delay into the open air. Artificial respiration and galvanism have been successfully employed in some cases, and inhalations of oxygen should be used if possible.
How the proportion of Carbon Dioxide may be estimated.—The air to be examined is drawn into a vessel capable of holding one and a half gallons, to which is added a clear solution of lime or baryta. The vessel, after being well agitated, is allowed to remain untouched for from eight to twenty-four hours. The carbonic acid is absorbed by the lime or baryta, and the difference in the causticity of the lime solution before and after it is placed in the vessel gives the amount of carbonic acid present in the air. A simple method of collecting the air in a mine is by lowering a bottle full of fine sand, so arranged that at any depth it may be turned upside down, and the sand allowed to run out, its place being taken by the air of the mine. The bottle may now be quickly drawn up, corked, and reserved for examination.
How may an Apartment, Well, or Mine be cleared of it?—Free ventilation in the first case. In the case of a well, a basket of slaked lime may be let down; but in mines a steam fanner or a jet of steam must be blown through the mine. No one, of course, should be allowed to enter the well or mine until it has been cleared of the carbonic acid.
This gas is formed in a variety of ways, one being the oxidation of carbon at a very high temperature in a limited supply of oxygen. It is given off by iron stoves at a red heat. It is one of the chief ingredients of the vapour of burning charcoal.
To this gas is due the suffocating quality of air in which coke or charcoal is burnt. It is inodorous, hence the dangerous insidiousness with which it produces its fatal results. It is said that 0.5 per cent. will cause death, and even 0.1 per cent. is injurious. The vapours from brick kilns and “burnt ballast” heaps are injurious to health, and the owners of them may be indicted for causing a nuisance.
The fumes from burning charcoal are taken advantage of for purposes of suicide, a method frequently used on the Continent, but almost unheard [Pg 399] of in England. The suicide generally shuts himself up in a room, which he has closed against any ventilation, and in which he has placed a receptacle containing burning coke or charcoal.
Poisoning by carbon monoxide occurs in two forms—acute and chronic.
Symptoms: Acute.—The first symptoms may be those of excitation, which are quickly followed by intense headache, giddiness, throbbing of the temples, and nausea followed by vomiting. Muscular weakness occurs, sensation and the reflexes are lost, drowsiness and coma follow, and in fatal cases convulsions often come on before death. The pulse becomes imperceptible at the wrist. The conjunctivæ become hyperæmic, the eyes staring, the pupils dilated and insensible. The voluntary and involuntary muscles are relaxed, the skin cold and cyanotic, and the lips covered with froth.
Chronic.—The symptoms are headache, neuralgic pains, anæmia, shortness of breath, and wasting; when advanced they are those of peripheral neuritis and mental disturbances.
The less severe symptoms of chronic carbon monoxide poisoning are not uncommon, and occur in those who occupy small and badly ventilated rooms, in which there may be a heating stove, gas stove, or imperfect gas fittings; the last are especially dangerous when water gas is used for illuminating purposes, as it contains a high percentage of carbon monoxide.
It is a very powerful gas, speedily causing death by acting chiefly on the nervous system, the symptoms being those produced by a pure narcotic.
The post-mortem signs are redness of the face, with reddish patches on different parts of the body. The blood—and this is chiefly characteristic of carbon monoxide poisoning—is cherry-red, due to a chemical compound formed by the action of the gas on the colouring matter of the blood, thus paralysing the oxygen-carrying power of the blood corpuscles. The gas is supposed to combine with the hæmoglobin forming a fixed compound, the spectroscopic examination showing the two absorption bands of the hæmoglobin nearer to the violet end of the spectrum than under normal conditions. (See Blood Spectra, p. 103.)
These bands resemble those of O₂Hb, so their position must be compared with a spectrum of O₂Hb, the two spectra being side by side.
There is another important difference, however, determined by the action of a reducing agent such as ammonium sulphide. The bands of COHb are unaltered, while those of O₂Hb are reduced. Death frequently takes place before all the Hb has been changed into COHb, so that the blood contains a mixture of COHb and O₂Hb, and on the addition of a reducing agent the spectrum is a composite one of COHb and reduced Hb. Only the broad band of reduced Hb is to be seen if the amount of COHb present be less than 28 per cent. In an atmosphere containing a large percentage of carbon monoxide death may occur before the blood contains sufficient COHb to give the characteristic spectrum.
The treatment consists in the removal of the sufferer into the [Pg 400] fresh air, artificial respiration, venesection, and the transfusion of arterialised defibrinated blood. Oxygen inhalations should be given. In two cases subcutaneous injections of nitro-glycerine were followed by recovery.
This gas is prepared by passing steam through incandescent carbon, and is a compound of nearly equal parts of carbonic oxide and hydrogen. It owes its dangerous properties to the first-named gas. When water gas, pure and simple, is supplied for heating purposes, its leakage cannot be detected, as the gas possesses no odour. When used for lighting and carburetted, its escape is more readily detected by the smell, but even then it is more dangerous than coal gas as the proportion of CO is higher. Several deaths have resulted from the use of water gas for heating and lighting purposes, and also for steel smelting in Leeds. The symptoms of poisoning are those of carbon monoxide.
Sulphuretted hydrogen is a gas possessing a powerful odour of rotten eggs. It is largely used as a test for most of the metals; and its presence may be detected by filter paper, moistened with a salt of lead, becoming black.
Symptoms.—When the gas is moderately diluted the symptoms produced are giddiness, throbbing of the temples, pain and oppression of the stomach, nausea, and vomiting; delirium and convulsions sometimes occur, together with laborious respiration and an irregular pulse. When the gas is but slightly diluted, the person becomes suddenly weak and insensible, and rapidly dies.
Post-mortem Appearances.—Fluidity and blackness of the blood, loss of muscular contractility, and a tendency to rapid putrefaction. The bronchial tubes are reddened, and the internal vascular organs may appear almost black.
Treatment.—This will consist in the immediate removal of the person into fresh air, and the administration of stimulants, together with the respiration of chlorine gas evolved from bleaching powder by the action of an acid.
Coal gas is composed of several hydrocarbons, the chief of which is marsh gas, together with free hydrogen, carbon monoxide and carbon dioxide, ammonia, hydrogen sulphide, and sulphides of carbon, which give to it its peculiar odour. The poisonous properties of coal gas are due to the carbon monoxide, 7.5 per cent. being present in ordinary gas as supplied for illuminating purposes. It can be detected by passing the coal gas through an acid solution of cuprous chloride, which [Pg 401] becomes black by the formation of a compound CuCOCl. A dangerous explosive compound is formed when the gas reaches the proportion of 1 in 10 of the atmosphere. Poisoning by this gas is, as a rule, accidental.
Symptoms.—Headache, nausea, vomiting, giddiness, ending in coma. Stertorous breathing is noticed in some cases. Should the sufferer be removed from the gas, the breath smells strongly of the gas. The murderer Chantrelle tried to cover his crime by admitting gas into his wife‘s bedroom, but the attempt failed. The pupils are, as a rule, dilated before death.
Post-mortem Appearances.—Cherry-red colour of the blood, redness of the pulmonary tissue, and froth in the air-passages. The vessels of the brain are engorged, and rose-coloured patches appear on the thighs.
Treatment.—This consists in removing the patient into the fresh air, artificial respiration, oxygen inhalations, &c., as in carbon monoxide.
Toxic effects have been produced by inhalation of the gases caused by explosives. The principal gases are carbon dioxide, carbon monoxide, and nitrogen. Gunpowder yields a considerable amount of CO and sulphuretted hydrogen. Nitro-glycerine, dynamite, and gun-cotton yield a large amount of CO. Tonite yields very little CO, and roburite none. Smokeless powders give off CO.
The manufacture of “roburite” and “sicherheit,” which contain dinitro-benzine, is fraught with danger from this substance, causing, in acute cases, cyanosis of the face or the whole body, headache, vertigo, paresis, coldness, quick pulse, dyspnœa, shallow breathing with long intervals, and coma. Vomiting may occur, and the blood becomes a chocolate colour. A chronic form of poisoning produces lividity and cyanosis, with gastritis, hepatic enlargement and jaundice, paræsthesia, numbness, and cramps in the muscles, amblyopia with concentric contraction of vision-fields, and central scotoma. The blood is like that of pernicious anæmia, and the urine brown or blackish.
This gas has a peculiar odour of geranium. It is a product of the incomplete combustion of hydrocarbons, and is formed when lamps or gas jets are burned with insufficient air, e.g. a Bunsen burner which has “lighted back,” also from the use of oil stoves, and gas cooking and heating apparatus. It is used for illumination, and formed by the action of water on calcium carbide. It forms a highly explosive mixture with air. It is not a potent poison. Continued exposure to it causes anæmia, malnutrition, and nervous symptoms. On animals it produces narcosis. It does not combine with hæmoglobin, but acts as an indifferent gas. [Pg 402]
This is known as laughing gas; it has a sweetish taste and smell. When breathed in small quantities it produces tingling sensations and induces laughter, hence its name. When breathed for anæsthetic purposes the skin becomes livid, the blood pressure raised, and unconsciousness follows. It acts first upon the higher nerve centres, then upon the spinal cord, medulla, and heart. If pushed too far it causes death by asphyxia. In ordinary use for anæsthesia, the latter is rapidly produced, and recovery follows quickly when the administration is stopped. It has peculiar effects upon certain people, who may not only show the symptoms of hilarity, but, in some cases, become extremely violent.
Petrol fumes produce toxic effects upon those who breathe them, comprising perverted taste, dysphagia, headache, giddiness, cyanosis, insensibility, mania and imbecility. Maniacal outbreaks occur during recovery. Peripheral neuritis may follow.
This causes poisoning when swallowed or inhaled, e.g. glove cleaning, waterproofing, &c. Death has taken place in either way.
Symptoms.—In acute poisoning there is excitement, flushing of the face, cyanosis, dilated pupils, headache, slow breathing, stupor and coma, with gastro-intestinal irritation.
Hallucinations and delirium may occur amongst workers in it; idiosyncrasy plays a part. Women may become intoxicated, excited, and hysterical. It may cause headache, vertigo, narcosis, and inability to walk, with vomiting. Small hæmorrhages may occur. Rapid coma and death may occur when the vapour is concentrated.
Treatment.—When swallowed, the stomach tube should be used and ether and strychnine given hypodermically. When overcome by vapour, removal to the open air, artificial respiration, oxygen inhalations, and restoratives are required.
This is an irrespirible gas with the odour of burning sulphur. It is a preservative and bleaching agent, is used for disinfection, and occurs in certain industries.
The inhalation of the fumes causes a feeling of suffocation, with spasm of the glottis, and irritation of the nose, trachea, and bronchi, producing sneezing and cough; opacity of the cornea, dyspnœa, cyanosis, and convulsions may occur. [Pg 403]
The gas is used for disinfection and bleaching. In chemical works chronic poisoning may occur causing anæmia, emaciation, gastritis, dental caries, bronchitis, and emphysema. If concentrated, it causes dyspnœa, violent cough, hæmoptysis, stupor, and syncope.
Treatment.—Fresh air, steam inhalations, and the general treatment of the lung conditions.
This is a very poisonous gas. Deaths have occurred on board ships carrying cargoes of electrolytic ferrosilicate containing calcium phosphide. It reduces the oxyhæmoglobin. It may produce rapid, followed by slow and laboured breathing and convulsions. [Pg 404]
Footnotes:
[1] Monthly Journal of Medical Science, 1851.
[2] Edinburgh Medical Journal, February 1876.
[3] Friedenthal, Archiv für Anatomie und Physiologie, 1900, p. 494.
[4] Deutsch, Bulletin Medical, Sept. 8, 1900; and Centralblatt für Bakteriologie, Band xxix. p. 661.
[5] Uhlenhuth, Deutsch Medicinische Wochenschrift, 1901, Nos. 6, 17, 45.
[6] Wasserman and Schutze, Berlin Klin. Wochenschr., Feb. 21, 1901.
[7] Nuttall, Jour. Hygiene, vol. i., 1901, p. 367; B. M. J., vol. i., 1901, p. 669.
[8] Tarchetti, Gazz. degli Osped., May 19, 1901; B. M. J., vol. i., 1901.
[9] Grünbaum, Lancet, Jan. 18, 1902.
[10] Metchnikoff, Centralblatt für Bakteriologie, April 18, 1901.
[11] M‘Weeney, Jour. State Med., vol. ix. No. 7, p. 378. Lancet, June 18, 1910.
[12] M‘Weeney, Lancet, June 18, 1910.
[13] Cunningham, New York Med. Journ., 1890, p. 287.
[14] Journ. Amer. Med. Assoc., 1901, p. 1721.
[15] Fyshe or Fisher v. Palmer, in 1806.
[16] Manual of Midwifery, 1886.
[17] Archbold‘s Criminal Cases.
[18] Or not to be.
[19] Dilution lessens the activity of some poisons, by prolonging the time necessary for their absorption; but in the case of powerful irritants, which act through the blood, moderate dilution increases their activity, by enabling them to enter the vessels more easily. Oxalic acid is an example of the effect of dilution as a modifying agent in its action. A small concentrated dose acts as an irritant; diluted, it is soon absorbed, and quickly causes death.
[20] The sulphates of alkaloids are insoluble in ether; hence they must be decomposed by an alkali.
[21] The temperature should be low, or the greater part of the conine will be evaporated with the ether.
Transcriber’s Notes:
Antiquated spellings were not corrected.
The illustrations have been moved so that they do not break up paragraphs and so that they are next to the text they illustrate.
Typographical and punctuation errors have been silently corrected.