*** START OF THE PROJECT GUTENBERG EBOOK 50640 ***
ELEMENTS OF SURGERY:
BY
ROBERT LISTON,
SURGEON TO THE NORTH-LONDON HOSPITAL, PROFESSOR Of CLINICAL SURGERY,
ETC., ETC., ETC.
FROM THE SECOND LONDON EDITION,
WITH
COPIOUS NOTES AND ADDITIONS,
BY
SAMUEL D. GROSS, M.D.,
PROFESSOR OF SURGERY IN THE LOUISVILLE MEDICAL INSTITUTE, SURGEON
TO THE LOUISVILLE MARINE HOSPITAL, ETC., ETC.
Illustrated
WITH NUMEROUS ENGRAVINGS.
Philadelphia:
ED. BARRINGTON & GEO. D. HASWELL.
NEW YORK—J. & H.G. LANGLEY: CHARLESTON, S. C.—WM. H. BERRETT:
RICHMOND, VA.—SMITH, DRINKER & MORRIS:
LOUISVILLE, KY.—JAMES MAXWELL, JR.
1842.
[Entered, according to Act of Congress, in the year 1842, by BARRINGTON
& HASWELL, in the Clerk’s office of the District Court for the Eastern
District of Pennsylvania.]
TO
WILLARD PARKER, M. D.,
Professor of Surgery in the College of Physicians and Surgeons
in the City of New York,
THIS EDITION OF MR. LISTON’S WORK
Is Inscribed,
AS A TESTIMONIAL OF RESPECT
FOR HIS UNTIRING ZEAL IN SURGICAL PURSUITS,
AND OF ESTEEM FOR HIS PRIVATE VIRTUES,
BY HIS FRIEND AND FORMER COLLEAGUE,
THE EDITOR.
5
PREFACE
TO THE AMERICAN EDITION.
The character of Mr. Liston’s work is too well established to render it
necessary for me to say anything in commendation of it. As an outline
of surgical science, which is all that can be claimed for it, it is
unrivalled in the English language. Written in a bold and graphic
style, the distinguished author never hesitates to express his opinion,
frankly and fearlessly, of what his judgment and experience have led
him to disapprove. In this, as well as in some other particulars, he
reminds one forcibly of that great and eccentric surgeon, John Bell.
There is no cringing to this man or that, no doubtful or equivocal
sentiment, no attempt to theorise or speculate; on the contrary, he
comes right out, and clearly tells us what he means. His work, full
of vigour and freshness, contains more originality than any other
similar publication that has been issued for a long time from the
British press. The hand of a master is discernible in every page; and,
notwithstanding an occasional incongruity, or outré expression, it is
impossible to read it without feeling that it is the production of a
great mind, thoroughly acquainted with the subject on which he treats.
Such a work is invaluable to the student; for, independently of
imparting sound surgical knowledge, it does more to form his judgment,
and to qualify him for the practical duties of his profession than all
the compilations in Christendom. Velpeau, with all his learning and all
his patience, has never furnished anything equal to it. His "Medicine
Operatoire" is nothing but a vast storehouse of research, to which
pompous doctors may resort for ancient lore, and prosing teachers for
materials for instruction. It details with endless minuteness the
operative methods of every surgeon, great or little, from the age of
Hippocrates to the present period, with their various modifications
and improvements, not forgetting the "appreciations" and labours of
the able professor himself. Such productions are well enough in their
way; they serve to give us an idea of the rise and progress of surgery,
and form good books of reference. Beyond this, however, they are of
comparatively little utility; the great mass of the profession is no
more benefited by them than if they had never been written; few read
them, and still fewer understand them. This6 attempt at erudition
pervades, if I mistake not, almost every recent publication on surgery
in the French language. Dupuytren is alone free from it. His writings
breathe throughout a different and more independent spirit: he speaks
like one accustomed to act and to think for himself; and the result
is, that he has accomplished more for French surgery than any other
Frenchman since the days of Ambrose Paré.
The first edition of the present Treatise was published at Edinburgh
in 1831, some time prior to the author’s removal to London. It was
originally comprised in three volumes. A second impression, of which
this is a reprint, appeared at London in 1840, in a revised and
improved form. The favourable reception which the publication has met
with in this country, and the desire I have felt to introduce it into
the school with which I am connected, as a text-book, have induced
me to prepare it for the American press with particular care. Among
the additions, properly so called, is an article on Strabismus, and
another on Club-foot; two subjects, the former of which was entirely
omitted in the English edition, and the latter discussed in a manner
altogether incommensurate with the existing state of our knowledge in
regard to it. The notes are designed to serve as further illustrations
of the text, or to supply deficiencies in relation to certain topics
which have been passed lightly over by the author. They might have
been extended to almost any number, and it would have afforded me no
ordinary gratification, had it been consistent with the views and
interests of my publishers, to present what might be considered as a
tolerably fair outline of American surgery. For such an object ample
materials are extant, highly valuable in themselves, and eminently
calculated, when they shall be properly embodied, to reflect credit
upon the talents, enterprise, and dexterity of our surgeons.
It need hardly be added, what is self-evident, that the editor of a
work is responsible to the public only so far as his own labours are
concerned. He adopts only in a general manner, without endorsing all,
the views and opinions of his author.
S. D. GROSS.Loui
LouiLouisville Medical Institute,
LouisvilleMay, 1842.
7
PREFACE.
The rapid advancement made in the pathology and treatment of surgical
diseases demands a perpetual revision and correction of the systematic
works devoted to this department of the healing art.
Accordingly, text books, various in merit and extent, have emanated
from the different schools. Several of these have, by successive
editions, kept pace with the science; whilst others have fallen into
disuse.
In this part of Britain, the systems of Latta, B. Bell, and Allan,
occupied the field; but it being now vacant, I venture to supply the
deficiency, by reducing the heads of my lectures into a compendium, or
guide, for those students who resort to this city.
It must appear superfluous to preface such a work by anatomical
descriptions, anatomy being now studied more generally, and with
greater zeal, than heretofore. Pathology also is more attended to,
and better understood. To which circumstances are to be ascribed the
improvements in surgical science, as well as in the art of operating.
The functions and structure of parts are more frequently preserved
uninjured—mutilation is more rarely required—and operations are
dispensed with. The wider the extension of pathology, the fewer the
operations will be—thus affording the best criterion of professional
attainment. Who will question, that there is more merit in saving one
limb by superior skill, than in lopping off a thousand with the utmost
dexterity?
To treat surgical diseases as they ought to be treated, the
practitioner must be thoroughly acquainted with the healthy and morbid
structure; he must also have a mind vigorous and firm from nature, well
instructed in the best precedents, and matured by observation.
Years are not the measure of experience. It does not follow, that the
older the surgeon is, the more experienced and trustworthy he must be.
The greatest number of well-assorted facts on a particular subject
constitutes experience, whether these facts have been culled in five
years or in fifty.
It is only from experience, directed and aided by previous study, that
accuracy of diagnosis and celerity of decision can be acquired. Besides
knowing in what manner to proceed, the surgeon must know well wherefore
he acts, and also the precise time at which he should interfere. With
knowledge and confidence derived from experience, he will perform such
operations as are indispensable for the removal of pain and deformity,
or for the preservation of life, with calmness and facility—with safety
to his patient, and satisfaction to those who assist in, or witness,
his proceedings.
Attention to the apparatus is necessary. It should be in good order,
simple, and ample. The young surgeon should note down, previously to
an operation, whatever, on reflection, can possibly be required. "For
in most capital operations, unforeseen circumstances will sometimes
occur, and must be attended to; and he who, without8 giving unnecessary
pain from delay, finishes what he has to do in the most perfect manner,
and that most likely to conduce to his patient’s safety, is the best
operator."
It is seldom necessary to employ much preliminary treatment. From the
usual preparative course of bleeding, purging, cooling diet, etc.,
patients about to undergo capital operations, as lithotomy, suffer more
than they can gain.
It is of the utmost importance to attend to the state of the patient’s
mind and feelings. He ought not to be kept in suspense, but encouraged
and assured; and his apprehensions must be allayed. If this cannot be
effected—if he is dejected and despondent—talks of the great risk,
and of the certainty of his dying, it is better that the operation be
abandoned, or at least delayed. If, on the contrary, he is confident
in the resources of his constitution, and in the ability of his
attendant, and looks forward to the advantage to be derived from his
own fortitude, then should there be no delay.
A mild laxative may be given, when an empty state of the bowels is
desirable, or when they, by acting too soon afterwards, might put the
patient to inconvenience or pain, or interrupt the curative process.
Attention to after-treatment is of much greater importance. The
practitioner is not to rely on success, however well the manual part
has proceeded. He must consider his labour only begun, when the
operation has finished; the patient is yet to be conducted, by kindness
and judgment, through the process of cure.
It is thus only that difficult and unpromising cases can be brought to
a happy conclusion, and favour and lasting reputation gained.
In the present work an endeavour has been made, in the first place,
to lay down, correctly and concisely, the general principles which
ought to guide the practitioner in the management of constitutional
disturbance, however occasioned.
The observations introduced to illustrate the doctrines inculcated are
given as briefly as is consistent with an accurate detail of symptoms
and results. The descriptions of particular diseases have been sketched
and finished from nature; and, it is hoped, with such fidelity, that
their resemblance will be readily recognised.
To describe all the methods recommended and followed, in the different
surgical operations, would occupy more space than can be allotted in an
elementary work—would, without answering any good purpose, lead into
the wide range of the history and progress of surgery.
Such modes of operating are described as have been repeatedly and
successfully performed by the Author.
If by clear and simple description of the phenomena attendant on morbid
action, and of the changes which it produces,—if by plain rules for
the treatment of the diseases, and performing the operations for their
alleviation or cure,—he contribute to the progress of surgery, and the
consequent diminution of human misery, he will consider himself fully
rewarded for the time and the labour spent on this production.
9
CONTENTS.
| PART FIRST |
| Page |
| Inflammation | 13 |
| INFLSigns | 14 |
| Irritation | 20 |
| Termination of Inflammation | 25 |
| Termination of Adhesion | 25 |
| Termination of Suppuration | 29 |
| Termination of Mortification | 43 |
| Erysipelas | 55 |
| Furunculus and Anthrax | 62 |
| Inflammation of Mucous Membranes | 65 |
| Inflammation of Serous Membranes | 66 |
| Inflammation of Joints | 67 |
Hypertrophy and Atrophy of the Articular Cartilages, with Eburnation | 75 |
| Scrofulous Disease of Joints | 77 |
| Neuralgic Affections of Joints | 78 |
Growths from the Synovial Membrane and Loose Substances in Joints | 79 |
| Affections of Bursæ | 80 |
| Coxalgia | 81 |
| Alterations of Form in the Head of the Femur | 86 |
| Inflammation and Diseases of Bone | 94 |
| INFLSuppuration in Bone | 96 |
| INFLCaries | 96 |
| INFLNecrosis | 103 |
| Fragilitas Ossium | 110 |
| Mollities Ossium, Rachitis, &c. | 110 |
| Arterial System, Affections | 116 |
| Aneurism | 118 |
| Aneurismby Anastomosis | 127 |
| Inflammation of Veins | 130 |
| Tumours | 134 |
| TumoursAdipose | 137 |
| TumoursFibrous | 138 |
| TumoursEncephaloid | 139 |
| TumoursMelanoid | 142 |
| TumoursCarcinomatous | 142 |
| Fungus Hæmatodes | 147 |
| Painful Tubercle | 149 |
| Polypus | 150 |
| Encysted Tumours | 151 |
| Tumours of Bones | 153 |
| Osteosarcoma | 154 |
| Spina Ventosa | 157 |
| Aneurismal | 158 |
| Osseous | 158 |
| Hydatic | 161 |
| Wounds | 164 |
| Tetanus | 183 |
| Ulcers | 186 |
| Hospital Gangrene | 191 |
| Sloughing Phagædena | 191 |
| Malignant Pustule | 193 |
| Ulcers on the Genital Organs, with their Consequences | 195 |
| Scalds and Burns | 211 |
10
PART SECOND. |
| Injuries of the Head | 215 |
| InjuWounds of the Scalp | 215 |
| InjuWounds of the Temporal Artery | 216 |
| InjuConcussion | 218 |
| InjuCompression | 226 |
| InjuFractures of the Cranial Bones | 227 |
| InjuWounds of the Brain | 232 |
| InjuHernia Cerebri | 233 |
| InjuPerforation of the Cranium | 234 |
| InjuInflammation of the Scalp | 238 |
| InjuThickening of the Scalp | 239 |
| InjuTumours of the Scalp | 243 |
| Diseases of the Eye and its Appendages | 245 |
| InjuInflammation and Abscess of the Lachrymal Passages | 245 |
| InjuInflammation of the Lachrymal Sac | 246 |
| InjuFistula Lachrymalis | 248 |
| InjuEncanthis | 252 |
| InjuEncysted Tumours of the Eyelids | 253 |
| InjuClosure of the Eyelids | 253 |
| InjuEctropion | 254 |
| InjuEntropion | 255 |
| InjuTrichiasis | 255 |
| InjuPterygium | 256 |
| Diseases of the Eyeball | 257 |
| InjuOphthalmia | 257 |
| InjuPurulent Ophthalmia | 260 |
| InjuStaphyloma | 261 |
| InjuInflammation of the Cornea | 261 |
| InjuPustular Ophthalmia | 263 |
| InjuUlcers of the Cornea | 263 |
| InjuLeucoma | 264 |
| InjuHernia of the Iris | 264 |
| InjuAlbugo | 264 |
| InjuNebula | 264 |
| InjuOphthalmia Tarsi | 265 |
| InjuStaphyloma | 266 |
| InjuHydrophthalmia | 266 |
| InjuExophthalmia | 266 |
| InjuInternal Ophthalmia | 272 |
| InjuIritis | 272 |
| InjuHypopium | 273 |
| InjuChoroiditis | 274 |
| InjuAmaurosis | 275 |
| InjuGlaucoma | 277 |
| InjuCataract | 277 |
| InjuArtificial Pupil | 287 |
| Wounds of the Eyeball | 288 |
| Orbital Inflammation | 290 |
| Tumours in the Orbit | 290 |
| Strabismus | 292 |
| Nasal Polypi | 301 |
| InjuMalignant Polypi | 303 |
| Nose, and Nasal Cavities, Inflammation, &c. | 308 |
| InjuNoli me tangere | 310 |
| InjuOzœna | 310 |
| Rhinoplastic Operations | 312 |
| Inflammation of the Antrum Maxillare | 317 |
| Lips, Ulcers | 319 |
| InjuCongenital Deficiencies | 322 |
| Palate, Congenital Deficiencies | 322 |
| Soft Palate, Tonsils, &c., Inflammation, &c. | 326 |
| 11Tongue, Ulcers | 331 |
| InjuInflammation | 332 |
| InjuDivision of Frænum | 334 |
| Salivary Ducts, Diseases | 335 |
| InjuRanula | 335 |
| InjuGums, Diseases | 337 |
| InjuTeeth, Diseases | 338 |
| Injury Extraction of | 340 |
| InjuLower Jaw, Diseases | 341 |
| InjuDisarticulation | 345 |
| Wounds of the Face and Neck | 347 |
| Larynx and Trachea, Diseases | 354 |
| InjuForeign bodies | 363 |
| InjuTracheotomy | 364 |
| Pharynx, Diseases | 368 |
| InjuForeign bodies | 371 |
| Œsophagotomy | 372 |
| Ear, Diseases of | 373 |
| InjuForeign bodies | 375 |
| InjuPolypus | 375 |
| Deafness | 375 |
| Bronchocele | 377 |
| Glandular Tumours in the Neck | 379 |
| Hydrocele of the Neck | 381 |
| Distortion of the Neck | 382 |
| Venesection in the Jugular Vein | 384 |
| Ligature of the Carotid Artery | 385 |
| InjuArteria Innominata | 387 |
| InjuSubclavian Artery | 387 |
| InjuAxillary Artery | 392 |
| InjuBrachial Artery | 392 |
| InjuHumeral Artery | 394 |
| Wounds of the Palmar Arches | 395 |
| Paronychia or Whitlow | 396 |
| Onychia | 399 |
| Collections in Thecæ | 401 |
| Ganglia | 401 |
| Venesection, bend of the arm | 403 |
| Mamma, Diseases | 405 |
| InjuEncysted Tumours | 406 |
| Affections of the Chest | 409 |
| InjuHydrothorax | 410 |
| InjuEmpyema | 410 |
| InjuWounds | 411 |
| Affections of the Abdomen | 412 |
| InjuHernia | 412 |
| InjuCongenital Scrotal Hernia | 413 |
| InjuInjuHernia Infantilis | 414 |
| InjuHerniaInguinal | 415 |
| InjuHerniaCrural or Femoral | 416 |
| InjuAscites | 435 |
| InjuOvarian Dropsy | 436 |
| Bruises of the Abdomen | 438 |
| Lumbar Abscess | 441 |
| Spina Bifida | 444 |
| Affections of the Rectum and Neighbouring Parts | 445 |
| InjuHemorrhoids or Piles | 445 |
| InjuryDistinct Varieties | 445 |
| InjuInflammation of the Rectum | 447 |
| InjuFistula | 449 |
| InjuStricture | 450 |
| InjuSchirro-contracted Rectum | 452 |
| InjuProlapsus Ani | 453 |
| 12Pruritus of the Rectum | 460 |
| Neuralgia of the Rectum | 460 |
Affections of the Mucous Membranes of the Urinary and Genital Organs | 461 |
| InjuGonorrhœa | 462 |
| InjuHernia Humoralis | 467 |
| InjuInflammation of the Bladder | 469 |
| InjuIrritable Bladder | 470 |
| InjuStricture of the Urethra | 470 |
| InjuFistula in Perineo | 472 |
| Retention of Urine | 478 |
| Incontinence of Urine | 489 |
| Gonorrhœa Præputialis | 490 |
| Phymosis | 491 |
| Paraphymosis | 491 |
| Hypospadias and Epispadias | 495 |
| Chimney-sweeper’s Cancer | 495 |
| Hydrocele | 496 |
| Cirsocele | 501 |
| Hæmatocele | 503 |
| Sarcocele | 505 |
| Castration | 507 |
| Calculus Vesicæ | 508 |
| InjuLithotrity | 517 |
| InjuLithotomy | 519 |
| Calculus in the Female | 530 |
| Gonorrhœa in Females | 531 |
| Gonorrhœal Lichen | 532 |
| Retention of Urine in Females | 533 |
| Vesico-vaginal Fistula | 534 |
| Imperforate Vagina | 535 |
| Contracted Vagina | 535 |
| Inflammation of Vagina | 536 |
| Polypus Vaginæ | 537 |
| Diseases of the Uterus | 538 |
| Ligature of the Common Iliac Artery | 539 |
| Ligature of theInternal Iliac | 539 |
| Ligature of theExternal Iliac | 540 |
| Ligature of theFemoral | 541 |
| Aneurismal Varix in the Thigh | 542 |
| House-Maid’s Knee | 543 |
| Cartilaginous Bodies in the Knee-joint | 544 |
| Distortion of the Feet | 545 |
| InjuVarus | 547 |
| InjuValgus | 548 |
| InjuPes Equinus | 548 |
| InjuCalcaneal | 549 |
| Exostosis of Distal Phalanx | 551 |
| Fractures | 552 |
| Fracturesof the Cranium and Face | 558 |
| Fractures of theSpinal Column | 560 |
| Fractures of theThorax and Upper Extremity | 564 |
| Fractures of thePelvis and Lower Extremity | 574 |
| Disunited Fracture | 586 |
| Dislocations | 588 |
| InjuLower Jaw | 591 |
| InjuUpper Extremity | 592 |
| InjuLower Extremity | 600 |
| Sprain | 607 |
| Bruise | 610 |
| Amputation | 612 |
| Excision of Portions of Diseased Bones | 632 |
| Excision of Joints | 634 |
13
ELEMENTS OF SURGERY.
PART FIRST.
OF INFLAMMATION.
There are few accidents or diseases, to which the human body is liable,
which are not preceded or followed by incited action, increased
circulation, and accumulation of blood in the capillary vessels of
the part affected; and these phenomena require to be very attentively
studied, and correctly understood, by all who propose practising the
healing art. As all the salutary as well as diseased processes which
occur in the human body are more or less attended or affected by this
action, and as its regulation forms a principal part of the duty of the
surgical practitioner, this work cannot be more properly commenced than
by treating of its nature, consequences, and management.
Inflammation may be defined to be, an unnatural or perverted action
of the capillary blood vessels of an organ or part of the body,
attended with redness, throbbing, swelling, pain, heat, and disorder of
function, as well as with more or less disturbance of the system.
Every part of the body is liable to inflammation; and some writers have
divided this action into different kinds, according to the particular
tissue which it chiefly involves. But it appears to be always of the
same character, though modified by various circumstances, such as the
tissue in which it occurs, the state of the constitution, the exciting
cause, and the intensity of the action.
The usual division of the subject, into Acute and Chronic, is that
which it is here proposed to adopt. The term Chronic Inflammation is
more properly applicable to a consequence of the Acute: but it is at
the same time true, that morbid actions proceed more slowly in some
constitutions, and in some parts of the body, than in others; and that
changes of structure and morbid products, such as generally result from
inflammatory action, even occasionally occur, without the prominent
symptoms of inflammation being experienced by the patient or detected
by the practitioner.
The term Morbid is used in contradistinction to what is called
Healthy Inflammation; but inflammatory action is generally connected,
more or less, with a diseased or disordered state of some part14 of
the body. In many circumstances it is highly necessary that a certain
degree of incited action of the vessels should occur, and continue for
a certain time; as during the uniting of fractures, the adhesion of
wounds, and the healing of some sores—and thus far it is healthful:
when, however, the action becomes excessive, it must, for this
reason, be considered morbid, as it frustrates the natural reparative
process; if the action, in fact, proceeds farther than is necessary
for reparation, it becomes a disease, and leads to absorption or
destruction of parts. In animals possessing the greatest powers of
reparation, inflammation, it appears, does not take place at all, or is
very slight, and scarcely ever proceeds to suppuration.
Redness is the first sign of inflammation to be considered; this is
observed, in the living body, on the surface, or at the extremities
of those canals which terminate externally. The inflamed conjunctiva
affords a conspicuous example of this appearance. In a subject that
has suffered from an internal inflammatory attack, a good opportunity
is frequently afforded of observing the enlarged and injected state
of the vessels on which the red colour depends. But inflammation may
have existed to a certain degree, and yet the parts may be pale, from
the capillaries having emptied themselves into the veins immediately
after the patient’s death. The paleness may be also in part caused by
the influx of the red globules being impeded immediately after death,
or when the patient is in articulo mortis, in consequence of the
contraction of the vessels, which is well known to occur at that period.
It has been said that redness is not essential to inflammation; for
serous vessels may be altered in size and function by this action,
and yet not be sufficiently dilated to receive the red globules of
the blood. And, again, that serous vessels may be enlarged so as to
admit the red globules; and a part that is colourless when in the
healthy state may, in consequence, assume a highly red hue when in an
inflamed condition. This may be observed in the cornea lucida, which,
when violently inflamed, is pervaded by numerous vessels, visible to
the naked eye, distended with red blood, ramifying over the whole of
it, and freely inosculating with each other. Some have even supposed
that these vessels are newly formed, in consequence of inflammatory
action. This opinion is, however, erroneous; as the vessels existed in
the cornea previously, and are only increased in size, so as to admit
of the accumulation of a sufficient number of red particles to render
the vessels visible. The speedy, and, in many cases, instantaneous,
appearance of red vessels where they could not previously be observed,
decidedly overturns the opinion that new vessels are in such a case
formed. New vessels are seldom formed, unless after a breach of
structure, or in cases where morbid deposits become vascular. There is
no proof of the existence of mere serous vessels in the human body,
as any one may ascertain who is accustomed to examine the capillaries
with a good microscope. Vessels which are so small as to admit only a
very few, say one, or at most two rows of globules, would, of course,
appear colourless, and these are what have been called serous vessels.
The globules of blood are so small as to be invisible to the naked eye;
and vessels carrying only one series of15 them would appear colourless.
No vessels belonging to the sanguiferous system have ever been observed
less in character than a blood globule; and this, so far as I have
been able to observe, is, as nearly as possible, 1/3000 part of an
inch. They appear to be flattened discs; and whether those of the human
body have a central nucleus or not, seems, as yet, very doubtful. The
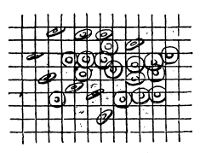 globules are here shown upon a scale of 1/4000 part of an inch, linear,
and in different positions. They are represented, as seen in the
greater number of microscopes, having a central nucleus. Whether, in
the blood of mammiferous animals, or not, this is an optical deception,
is not very clearly made out; but in that of reptiles the nucleus is
easily demonstrable. The redness then is not from error loci, or in
consequence of red particles flowing where none flowed before, but from
the capillaries becoming distended and dilated with an unusual quantity
of blood, which is stagnated in the central part of the inflamed
neighbourhood, the inflammatory focus.
globules are here shown upon a scale of 1/4000 part of an inch, linear,
and in different positions. They are represented, as seen in the
greater number of microscopes, having a central nucleus. Whether, in
the blood of mammiferous animals, or not, this is an optical deception,
is not very clearly made out; but in that of reptiles the nucleus is
easily demonstrable. The redness then is not from error loci, or in
consequence of red particles flowing where none flowed before, but from
the capillaries becoming distended and dilated with an unusual quantity
of blood, which is stagnated in the central part of the inflamed
neighbourhood, the inflammatory focus.
Throbbing, to a greater or less degree, is always felt in an inflamed
part by the patient; and it is frequently so distinct as to be readily
perceived by an attentive examination. This arises, probably, from
the stagnation of blood in the vessels of the part over-excited, and
principally affected by the disease or injury, causing an increase in
the collateral circulation; and it is this rapidly increased action
around that gives rise to the signs and symptoms, and constitutes,
in point of fact, what is known and recognised as inflammation. The
sensation of throbbing is not, however, produced entirely by the action
of the capillary vessels, but in consequence, also, of the larger
trunks in the neighbourhood sympathising with these capillaries,
and so having their action increased also. The obstruction of the
capillaries in the early stage of inflammation must necessarily cause
a greater force of the heart to be expended on the trunks leading to
such capillaries; hence the greater impulse and velocity of blood in
the circumferential and patent vessels. In fact, when the inflammatory
action is extensive or severe, or when the part affected is of much
importance to life, the whole circulating system is disturbed, and thus
arises the sympathetic excitement of the constitution.
The incited action of those vessels in the more immediate vicinity of
the inflamed part is well marked in cases of Paronychia. There the
digital, the radial, and ulnar arteries, with their branches, beat more
violently than usual; and with much greater force, though not more
rapidly, than the vessels in other parts of the body.
Swelling is caused by the enlarged and overloaded vessels relieving
themselves by effusion of part of their contents into the surrounding
cellular texture. The effusion varies in extent and consistence,
according to the degree of inflammatory action, and the species of
resistance offered; at first it is serous, then mixed with fibrin,
and consequently spontaneously coagulable. Cæteris paribus, the
greater16 the resistance, the less the effusion, and the more violent
the inflammatory action; the chance of its speedy and favourable
termination is also more diminished. Even the enlargement of the
bloodvessels produces a certain degree of intumescence previous
to effusion. The relief to the vessels by effusion giving rise to
swelling, when it occurs in loose cellular tissues, may be considered
as a beneficent provision of nature. But in vital organs it may be
productive of the most serious consequences; as in these, very slight
effusion will often endanger the structure of the organ, destroy its
functions, and not unfrequently be attended with fatal consequences.
The nature of the effused fluid varies according to the degree of
violence and advancement of the action, and is also modified by the
texture in which that action occurs. It may consist of serum, lymph,
blood, or pus. In inflammation, in short, exhalation, though at first
diminished, is soon much increased, whilst the powers of the absorbent
vessels are diminished, or at least do not maintain their usual
relation to those of the exhalants.
Pain is the next symptom enumerated. Here the very common error of
supposing that where there is pain there must always be inflammation
may be noticed. Some diseases attended with the most acute pain, as Tic
Douloureux and Cramp, are generally unattended with inflammation. Many
chronic diseases, too, are accompanied with violent and long-continued
paroxysms of pain, without excited circulation of the part.
This erroneous opinion often gives rise to highly prejudicial
proceedings, as—the exhausting, by copious depletions, the vital powers
of patients, already enfeebled by continued disease or treatment—the
consequent aggravation of the urgent symptoms—and, the then only
termination of the disease and of the practice, death.
Again, it is true that we must bleed, in some cases, with the view
of preventing the occurrence of inflammation; yet the prophylactic
treatment may be carried too far, as in cases of violent injuries, or
after severe operations. In these instances, the immediate abstraction
of blood, so far from being beneficial, expedites the dissolution
of the patient, or at least greatly retards the cure. Pains arising
from local irritations are often treated in a similar way, whilst the
removal of the cause would be much more likely to restore the natural
action of the parts.
Though inflammation does not always accompany the sensation of pain,
yet the latter, in a greater or less degree, attends inflammatory
action; and, perhaps, it is fortunate that it does so. Because, were
it not for the occurrence of pain, the patient’s attention would not
be directed to the disease; he would continue to use the part as if
in health, and the affection would thus be much aggravated. Whereas,
according to the existing provision of nature, pain is felt at the
commencement of the action, the presence of which the patient is
thereby made aware of; and he is compelled to employ such measures
for its removal as reason naturally dictates, of which none is more
effectual than disusing the affected part. The nerves are thus the
safeguards of the various parts of the body in health—their nurses
in disease. A part deprived of sensation may be used, even to the
de17struction of its texture, without producing any impression on the
sensorium, and consequently without the animal being conscious of it.
The presence of pain, as a symptom of inflammation, may be easily
explained. The connexion of the vascular with the nervous system
is very constant and intimate. Their ramifications accompany each
other, and are contained in the same cellular sheath; and without the
reciprocal influence of each, neither could perform its functions
perfectly. By injecting a limb soon after its separation from an
animal, and before its vital heat has departed, spasms of all muscles
are sometimes produced; showing the intimate connexion between these
two systems. This, however, is distinct from the contractions of the
muscular fibre produced by the application of stimuli. In the former
case, the contractions are universal, and induced through the medium of
the nerves. In the latter, the irritability of the fibre is excited.
When the circulation is excited, the nerves accompanying the affected
vessels are unusually compressed, and over-stimulated by the
circulating fluid, in which, probably, some change takes place, and in
this manner unnatural impressions are produced; the nerves themselves
are likewise the seat of disease, in consequence of the enlargement
of the minute capillaries which permeate them. Over-distension of the
coats of the vessels may also be supposed to give rise to painful
feelings, independently of any affection of the accompanying nervous
trunks.
The degree of pain is generally in proportion to the sensibility of
the part when in health; it also depends upon the distensibility
of the parts affected, and on the intensity of the inflammatory
action. When bones, tendons, &c., which in their uninflamed state are
nearly insensible, become inflamed, the pain and suffering are most
excruciating, owing to the resistance opposed to the dilatation of the
vessels, and the prevention of the effusion by which they naturally
relieve themselves.
The kind of pain also varies, in consequence of different modifications
in the action causing different impressions on the sensorium. Pain
is not always increased in proportion to the natural sensibility of
the part; for in some instances the sensibility is rendered much more
intense, while in others it is much obtunded.1
The last, and, according to some writers, the only unequivocal symptom
of inflammation, is Heat. In extravasation of blood into the cellular
texture, as under the conjunctiva, there is redness, swell18ing,
and occasionally pain; but at first, and unless the action of the
bloodvessels be excited, there will be neither heat nor throbbing.
In many internal inflammations heat is much complained of; and in
Enteritis it has been considered a pathognomonic symptom.2
The signs, symptoms, and consequences of inflammation—and amongst
others, heat—are modified by the distance of the affected part from the
centre of circulation. All actions, healthy as well as morbid, proceed
with more vigour in the superior extremities—in the head, the neck, and
the trunk, than in the more remote parts of the body; for to the former
the blood is transmitted more speedily, if not in greater quantity, and
is not so liable to be impeded in its return. Hence an arm may bear up
under a severe injury, which, to an inferior extremity, would prove
inevitable destruction. The heat, however, of an inflamed part, is
generally supposed to be much greater than it really is. The sensation
of heat is considerable to the patient, as well as to any observer,
whilst the absolute increase of temperature is very slight indeed.
It has been proved by the most decided experiments of Mr. Hunter, on
the mucous canals of animals, first when in health, and again after
violent inflammation had been excited, that little or no variation of
temperature can be observed. The elevation of temperature is probably
constant, though only amounting to a degree, or even less. As the blood
is the source of heat, wherever an increased quantity is circulated,
there should, to some extent, be increased heat.
The effects of an incited action of the vessels on the system at
large must now be adverted to; or, in other words, that general
disturbance in the system which attends inflammatory incitation, and
which occurs in a degree proportioned to the power of the exciting
cause, and the kind of texture primarily affected. The functions both
of the sanguiferous and nervous systems are deranged, producing a
state termed Symptomatic or Sympathetic Inflammatory Fever. From some
observations of my friend Mr. Gulliver, it is probable that this 19state
is frequently, if not generally, dependent on changes in the blood
consequent on inflammation. A sort of decomposition of part of the
fluid and vitiation of the remainder; the fibrin being separated and
effused into the injured part for the purposes of reparation, while the
blood globules are converted into pus in the capillaries, and mixed
with the circulating fluid. Thus the presence of pus in the blood may
become the proximate cause of fever; but if an outlet to the matter be
established, if it be discharged by the occurrence of suppuration in
a cavity or on a surface, the case is benefited and the constitution
relieved. This points to an important principle in practice. Nature
puts it in operation in small-pox, for example—how favourable it is for
the pustules to come out, and to what danger is not the patient exposed
if they are repelled.
During the paroxysm of inflammatory fever all the secretions and
excretions are diminished or suppressed; and hence the hot dry state
of the skin, the thirst with foul and dry tongue, the scanty and high
coloured urine, and the constipation of the bowels. This last symptom,
however, though it may arise partially from the diminished secretion
of mucus, yet is often dependent on disturbance of the functions of
the brain and nerves. The pulsations of the arteries become rapid and
strong, the sanguiferous system being unable to relieve itself by
effusion, in consequence of the obstruction of the exhalants.
If the extreme vessels are in any way obstructed, and the general
circulation in consequence much accelerated, the internal viscera
become oppressed, and are interrupted in their functions; and relief is
experienced only when relaxation occurs in the vessels upon the surface
of the body. Thus, in any violent and continued exertion, there is a
sense of oppression in the chest, and the functions of the encephalon
are somewhat disordered, but as soon as perspiration breaks out the
relief is instantaneous, and the animal can, without difficulty,
persevere in its exertions.
In inflammatory fever, the breathing is often difficult, and the
appetite declines; the patient is restless and watchful, and when he
does sleep, he is not thereby refreshed. In the more violent cases,
the sensorial functions are much disturbed; even delirium supervenes,
with violent muscular exertion and convulsions, and may be followed by
coma, should the local affection not subside. The delirium attendant
on violent diseases and accidents may often be considered a beneficent
effect of nature’s operations; for the patient, frequently losing all
consciousness of his situation, seems to be under the influence of the
most pleasing hallucinations, and is freed from the more lamentable
state of severe mental as well as bodily affliction.
Writers on Inflammation have expatiated at great length on
Sympathies; and these have been divided into, 1st, The Partial—the
Remote, the Continuous, and the Contiguous;—Remote, when parts
sympathise, though situated at a considerable distance from each
other;—Contiguous, when the sympathetic action seems to be produced, in
separate parts, merely from juxtaposition;—Continuous, when the action
extends in parts which are of similar texture, and conjoined with that
which is primarily affected.—2d,20 Universal, where the whole system
suffers along with parts of it. For instance, the whole system is often
disturbed by a deranged state of the alimentary canal, and, conversely,
the bowels, or the skin, the brain, the osseous or any other of the
textures, may suffer from a general disorder.
The system sympathises much more with some parts than with others;
and we accordingly find that disorder in one part will give rise to
alarming constitutional excitement, whilst in another, a much greater
derangement in function and structure will apparently be almost
entirely disregarded by the constitution.
Irritation is an effect of sympathy, and differs from inflammation,
inasmuch as the functions of the nervous system, and not those of the
sanguiferous, are disturbed;—the latter frequently supervenes on the
former. Irritation is local, or constitutional. As examples of the
strictly local species, may be mentioned that peculiar and dreadfully
annoying sensation produced in the alveoli by the presence of a
diseased tooth, or the irritation caused by ascarides in the rectum, or
by stone in the bladder.
But, from this action being dependent on the nervous agency, irritation
is frequently produced in a part remote from the source of the action.
Thus, if an irritating cause of any kind be applied to the origin
of a nerve, the effects of the irritation may be evinced in a part
supplied by its extreme branches; while, if the cause is applied
to the termination of a nerve, a similar action is produced at its
commencement, and in parts supplied by nerves from the same origin.
Thus, disease of the hip-joint causes pain in the knee, whilst
dentition in children not unfrequently produces fatal effusion at the
base of the brain; and again, irritation at the neck of the bladder
frequently gives rise to pain in the feet.
Local impressions, injuries, or irritations, though apparently of
little importance, frequently produce irritation which affects the
whole system, and is therefore termed constitutional. Syncope
sometimes follows the passing of a bougie along the urethra. We meet
with too many instances of constitutional irritation following severe
injuries or operations, especially if attended with much hemorrhage.
In general, there is considerable prostration of strength; the patient
is anxious and restless; his sleep is disturbed; the pulse is weak and
fluttering, occasionally intermittent; the tongue is white and loaded;
the appetite is gone; the stomach rejects the little food which the
patient is able to take; he is startled and annoyed by the slightest
external impression. At this period of the disorder, rigors generally
occur, and are followed by a sense of heat, and by perspiration; then
the above symptoms gradually decrease, and the patient recovers; but in
certain instances his breathing becomes quick and somewhat oppressed,
attended with a peculiar spasmodic elevation of the nostrils; all the
secretions are diminished, the intellectual functions become impaired,
and there are occasional convulsive twitchings; coma supervenes,
preceded by a low muttering delirium, and followed by death.
This action, as well as every other, is much modified by the importance
of the part which is the source of the action, and by the21 constitution
of the patient. It is more severe in children than in adults. The
affection will be more fully detailed, when treating of local injuries,
and the management of patients after severe operations.
The Causes of Inflammation come next to be considered; and first, of
the proximate cause or theory. The different states of the Vessels, in
their healthy and in their incited condition, have given rise to much
discussion. In the first place, considerable difference of opinion
exists as to the relative share which the heart, the larger arteries,
and the capillaries, have in propelling the circulating fluid in a
state of health. Some physiologists are inclined to attribute the
principal power to the heart, the blood being propelled and returned,
according to them, almost entirely by the vis a tergo; while they
suppose that the arteries possess merely a degree of elasticity or
tonicity. Considering the arteries as elastic tubes, performing an
indispensable part in the propulsion of the blood, we will now briefly
consider their state in inflammation.
Passing over the different theories of error loci, spasm, &c., which
have at various times been entertained, let us first examine the
condition of the capillary vessels, for these are primarily and
principally concerned. In inflammation, the balance of the circulation
is destroyed, but a diversity of opinion has existed as to the precise
nature of the change which occurs. It has been supposed, and perhaps
correctly, that the circulation is, in the first instance, much
accelerated in the capillary vessels of an inflamed part; but it has
been satisfactorily proved by experiment, that, after inflammation
is fairly established, the blood circulates more slowly than in the
healthy state of the vessels. There appears, in fact, to be, as
insisted upon by some writers on the subject, a state of excitement,
then of collapse, followed, if the life of the part is not destroyed,
by reaction. When a part is stimulated, the circulation is accelerated,
and a greater quantity of blood is transmitted by its vessels: if
the excitement is speedily removed, they recover themselves, though
perhaps a little dilated, and no inflammation ensues. If, for instance,
a foreign body of any kind gets entangled betwixt the upper eyelid
and the bulb of the eye, and it is permitted to remain a few moments
only, redness of the whole surface of the conjunctiva takes place,
but it is transitory, and disappears entirely some short time after
the extraction of the foreign body. If, however, it is permitted to
continue longer in contact with this sensible surface, the membrane
reddens more and more, and becomes thickened. Violent pain, with
discharge of tears, and alteration of the secretion from the mucous
surface, take place, ophthalmia is, in fact, established. If the
exciting cause is applied for a sufficient length of time, the extreme
vessels lose their contractility, they are weakened, become dilated,
and the contained blood circulates slowly. When inflammation is fairly
established in a part, the capillaries become considerably dilated,
and the blood is often completely stagnated in the inflammatory point.
In the circumference of this focus, it is accelerated as formerly
noticed: the blood is probably stagnated for two or three days in the
capillaries and in the contiguous cellular tissue, when the action
is at all violent. It,22 however, begins to move again; it loses its
colouring matter, while stagnated; the fibrin is assimilated to the
neighbouring parts, or rather effused, so as to cause the thickening,
and the blood globules have possibly undergone a change, and been
converted into those of pus. If the disease be of a limited extent,
and without breach of surface, they are carried into the circulation
very gradually, and in such small numbers as not to produce injury
to the health; otherwise the contamination of the blood by a large
quantity of pus causes inflammatory fever. It is probable that the
permanent dilatation occurs in consequence of the larger vessels in the
immediate vicinity being incited, and propelling more blood into the
minute capillaries than they can readily return into the corresponding
veins; and in consequence of so great a degree of distension being
produced, the vessels are incapable of again speedily contracting;
the blood, also, from being stagnant, becomes of a darker colour. The
larger trunks propelling blood into the distended and comparatively
inert capillaries, which are incapable of transmitting into the veins
the same quantity of fluid which they receive, will cause the throbbing
or pulsating sensation. The blood circulating in the parts around is
sometimes apparently changed in quality; it is redder, flocculi appear
floating in it, and the globules disappear. These last may have been
broken down, or partial decomposition may have taken place from a loss
of vital power in the vessels themselves.
The blood globules are, perhaps, merely compressed; for whenever motion
is produced in the fluid, they speedily reappear. Fresh globules
also find their way into the affected capillaries from neighbouring
vessels. The alteration in the component parts of the blood has been
supposed to depend upon the previous state of the inflamed vessels
in which it is contained: it is said soon to reassume its natural
appearance, when brought into a healthy vessel, and reference is made
to experiments on the web of the frog’s foot. When once altered, it
is, however, questionable if the blood ever reassumes its natural
appearance; of course the blood which takes the place of that which
was stagnated in the capillaries will be natural. If there have been
extensive inflammation, and therefore much altered blood, one of two
things will happen, viz., inflammatory fever and its consequences, or
the discharge of the offending matter (the altered blood) as pus. We
may also conclude that the blood of an inflamed part undergoes chemical
changes; for when the part becomes gangrenous, the blood then loses its
red colour, and assumes a yellowish-brown hue, from the absorption of
its colouring matter, which necessarily implies an alteration in its
chemical constitution. It seems not unlikely, that the change which is
early observed in the appearance of the blood of an inflamed part is
the commencement of a chemical process, which, if the vessels do not
regain their contractile power, terminates in the total destruction of
the ordinary properties of that fluid. It is probable that the more
modern speculators in medical science have paid too little attention
to the state of the fluids, and to the fact that, when diseased
action occurs in a part, its secretions and supplying fluid are very
considerably changed.
But the blood in inflammation also undergoes a change, observable23
after its removal from the circulation, and especially when the system
sympathises with the part affected. The blood, it is generally believed
and stated, does not coagulate so quickly as in the natural state,
or else, it is said, the red globules, being increased in specific
gravity, fall rapidly to the lower part of the containing vessel, so
that a yellowish crust appears on the surface of the crassamentum
or clot; and this appearance is termed the inflammatory or buffy
coat. The blood extracted from the veins of a patient labouring
under inflammatory fever often appears to coagulate very quickly;
but it contains an unusual proportion of fibrin. In certain states
of inflammation, this crust is also much contracted, so that its
marginal circumference is at a considerable distance from the sides
of the containing vessel; its margins also are elevated and inverted;
its upper surface is smooth, whilst the under adheres firmly to the
coagulum; and in this state the blood is said to be cupped, as well
as buffed. The appearance of the buffy coat is not peculiar to the
inflammatory state, but is apparently dependent on hurried circulation,
however occasioned. It frequently presents itself in blood removed
from the circulation during pregnancy, and in several other conditions
of the system, apparently altogether unconnected with inflammatory
excitement. In these circumstances, however, the contracted or cupped
appearance of the coagulum is hardly ever observed. An ignorance
of the above fact leads to dangerous practice, inasmuch as certain
practitioners will bleed, and continue to bleed, for very equivocal
inflammatory symptoms, conceiving themselves fully warranted in so
doing by the presence of the buffy coat. This coat is often not so
apparent in the blood first drawn as in that afterwards abstracted.
In inflammation, as was formerly remarked, a greater quantity of blood
not only flows into the capillary vessels, but it also escapes from
them, or is extravasated. This may occur with or without rupture of the
vessels, and to a greater or less extent, according to the violence of
the action, and the texture of the part.
When local inflammatory action exists to a considerable degree, the
general circulation is more or less disturbed. The heart, and the
larger vessels supplying the capillaries, which are more immediately
concerned in the local action, subsequently sympathise with the part
affected, and, acting with greater vigour than usual, propel the blood
into the extreme branches; so that the inflammatory excitement may be
said to be gradually communicated by the continuous sympathy, till the
whole sanguiferous system becomes subject to its influence. The degree
of this general excitement depends greatly on the texture and function
of the part primarily affected.
The term Passive Inflammation has been applied to that state in which
the larger vessels are not excited, or have ceased to sympathise with
the capillary branches. The term Chronic Inflammation is properly
limited to the consequence of the acute inflammatory action, the part
remaining turgid and swollen, the vessels over-distended with dark
blood, but with little or no pain, and without heat or throbbing.
Congestion is also employed to denote fulness of the vessels,
large as well as small, when no sign of excited circulation, or of
decided inflammatory action, has occurred. It is most fre24quently
used, however, when describing the condition of an internal organ. An
over-distention of a particular set of vessels may certainly exist
(as a consequence of inflammation, or altogether unconnected with
it), unattended with inflammatory action. These two states ought to
be carefully distinguished from a similar condition of the vessels,
attended with inflammation; for practice, which would be beneficial
in the one case, is highly prejudicial in the other, and lamentable
examples of the non-attention to this distinction are every day
observed.
It may here be mentioned, that some have denied the existence of
vitality in the blood; and to some minds it may, perhaps, be difficult
to conceive how a fluid should be possessed of this principle. But
no one can either doubt or deny that the blood, in its distribution,
in its manner of receiving increase, in the secretions furnished by
it, and in its various morbid changes, is governed by certain laws
and principles which cannot be explained by those of chemistry or
mechanics, but must belong to some other power. It is allowed, and has
been promulgated by all authors, that the blood is one of the most
active agents in the animal economy—in repairing waste, in affording
peculiar fluids necessary in that economy, in supplying organs with
materials for carrying on their functions, &c.; and yet all this,
according to some, is accomplished by a dead animal fluid; no one
can plausibly object to the laws by which the blood is governed
being referred to the power of life, and to their being called Vital
Principles.
Certain circumstances give rise to inflammation, and have been called
its Exciting or Immediate Causes. Among the external applications
producing inflammation, stimulants bear a conspicuous part; the
effects of which, in causing this action, are well shown by many
experiments that have been performed on the lower animals: by the
application of ammonia, spirits of wine, or common salt, for example,
to the diaphanous web of a frog’s foot. As stimulants usually causing
inflammatory action, by their being applied to the surface of the body,
may be enumerated acids, alkalies, certain salts, animal substances,
such as cantharides, the juices of many plants, many poisons, an
excessive degree of heat, &c. Any solid substance, though by no means
acrimonious in its quality, may act as an exciting cause, as by
pressure or friction.
Wounds also, especially when of considerable size, and occurring whilst
the constitution is in an unhealthy condition, give rise to local, and
occasionally general, inflammatory action.
This action is besides frequently produced by injury from an obtuse
body causing a bruise or fracture; by the lodgement of extraneous
substances, or of decayed portions of the system,—such as portions of
bones, tendons, &c.; or by irritating matter generated in the system
itself,—by concretions, tumours, vitiated secretions, &c.
One of the most frequent causes of inflammation is cold; the action of
which, however, cannot always be readily explained. In some instances,
it appears to act directly on a part, as in inflammation of the mucous
membrane lining the organs of respiration: in others, its action is
indirect, probably by disturbing the equality of the circulation, the
inflammation occurs in a part distant from the surface the25 temperature
of which had been diminished. In the great majority of instances in
which inflammation has occurred, in consequence of very intense cold,
it is produced by the sudden application of heat whilst the temperature
of the part is greatly below the natural standard, as will afterwards
be more particularly illustrated. But the inflammatory action may be
produced, even though no heat be afterwards applied directly to the
part, by its vessels being too rapidly brought into a degree of action
similar to that of the surrounding parts which are in their natural
condition. Sudden and general diminution of temperature seems to act
as an exciting cause, by producing an instantaneous suppression of
the transpiration. Another exciting cause of the inflammation, is
the retention of the secreted fluids, causing unnatural distension
of canals or cavities, and is exemplified by cystitis occurring in
consequence of retention of urine. Certain states of the constitution
are justly supposed to excite inflammation, in particular textures.
Other exciting causes of inflammation might be enumerated, but these
will be more naturally explained, and more fully considered, whilst
treating of inflammation of the various tissues and organs. Their
effects are various and diversified, according to the intensity of the
cause, the structure, function, and sympathies of the part affected,
and the state of the system. And it is also to be remembered, that not
unfrequently inflammatory action appears, whilst we can assign no cause
for its production.
Inflammation is said to terminate in Resolution, Suppuration, and
Mortification. The application of the word termination, however,
is injudicious; for in general the inflammatory action, though much
abated, is not extinguished by the occurrence of suppuration or
mortification, but often continues in the surrounding parts with
unabated intensity; and not unfrequently several of the terminations
occur combined with each other.
Adhesion has also been mentioned as a termination of inflammation,
but perhaps improperly; for, although in certain parts of the body,
as in the serous cavities, adhesion is produced in consequence of
inflammatory action, and during its progress, still the process of
adhesion is altogether independent of this action in other textures,
such as the cellular. In the uniting of a flesh wound, a certain
degree of incited action of the blood vessels is necessary for the
accomplishment of the adhesive process; but should that incited action
reach the inflammatory pitch, the union by the first intention is
interrupted, and the wound must heal by granulation with suppuration.
The process of adhesion will be more properly attended to when treating
of wounds.
The various terminations of inflammation are salutary or destructive,
according to circumstances; but resolution is, in general, the one most
to be desired; complete resolution, however, perhaps seldom occurs;
after the inflammatory action has attained a certain point, this cannot
be expected to happen.
Resolution takes place in consequence of the reëstablishment of the
circulation in the capillaries, in which the blood had stagnated;
hence the diminution of the increased action in the larger vessels—the
effused fibrin, at the same time, if there was much swelling, is26
partly absorbed. The circulation in the part becomes again natural, and
the circulating fluid also resuming its healthy properties, the redness
and sensation of throbbing cease. In consequence of the bloodvessels
regaining their contractility, the nervous system is no longer
preternaturally stimulated, and thus the increased sensibility is
done away with. In short, when inflammation terminates in resolution,
the part is left in the same state in which it was previous to the
supervention of the attack. It is not an instantaneous process, but
gradual in its completion.
Again, it not unfrequently happens, when inflammation has occurred in
the surface, and continued for a short period, that it spontaneously
disappears, and does not again return; the action is said to terminate
in Delitescence, and of course this is always a favourable
occurrence. But if the inflammation, after having suddenly disappeared,
attacks another part at a distance from that first affected, the change
is termed Metastasis. If the inflammation leaves an internal viscus,
and appears on the surface of the body, the circumstance is favourable;
but if it leaves the latter to attack the former, the result is highly
dangerous.
Treatment.—In the treatment of inflammation, with a view of procuring
resolution, our attention must be first directed to the exciting cause:
it is, if possible, to be discovered, and removed. Thus, foreign bodies
are to be extracted—fractures reduced—strictures divided—unnatural
accumulations of fluid withdrawn, &c. In many cases, if the exciting
cause is removed, nothing more is required; the inflammation speedily
subsides. If the cause cannot be removed, or if, after its removal, the
inflammation proceeds unabated, the arterial action must be reduced
by general and local abstraction of blood. By general depletion, the
action of the whole sanguiferous system is diminished, as well as of
those vessels more immediately engaged in the morbid action; but the
affected capillaries are still dilated, and less capable than the
larger trunks of effective contraction to propel their contents; and
are therefore only sufficiently depleted by the local abstraction of
blood, by leeches,3 cupping, punctures, or inci27sions.4 Blood may
be drawn either from arteries or from veins. In Arteriotomy, the blood
is discharged more rapidly, and its flow is of longer continuance,
than from a vein, so that the system may thereby be almost completely
deprived of its circulating fluid; and perhaps a more speedy impression
may be made on the inflammatory action. One objection to venesection
is, that after frequent and copious venous hemorrhage, the internal
vessels become gorged with blood, and a disposition to apoplexy is
induced.
But bleeding is not to be had recourse to without due consideration of
the age, strength, constitution, and idiosyncrasy of the patient; if
employed, it must be modified according to these; and it has already
been mentioned, that depletion is not always to be persevered in on
account of the presence of the buffy coat.5
28
Bleeding is materially assisted in reducing the activity of the
circulation, by the employment of saline purgatives, along with
nauseating doses of antimony. Diaphoretics are of essential service
in promoting the action of the exhalants, and thereby relieving
the affected capillaries. The exhibition of opium is frequently
advantageous, more especially after depletion, in allaying the painful
sensations when severe, and averting reaction, and also in procuring
refreshing sleep, when the patient is anxious and restless. Digitalis
has been administered, with the view of reducing the arterial action;
but it has been fully established, that this medicine acts at first
as a direct stimulant, and that it is only after its use has been
continued for some time that its effects become sedative.
The local applications to an inflamed part are sometimes made hot,
sometimes cold. The latter will perhaps be at first the more grateful
to the sensations of the patient. They are, however, with greater
propriety employed before inflammatory action is fairly established,
and they act by constringing the superficial vessels with which
those more deeply seated sympathise to a certain extent; but warm
fomentations are more pleasant and useful when inflammation has really
taken place; they relieve the pain more effectually, and at the same
time promote the cutaneous transpiration; they relax the surface
moreover, effusion is thus encouraged, the deeper vessels are so far
relieved of their load, and the pressure upon, and stimulation of,
the nerves are thus diminished. After the violence of the symptoms
has abated somewhat, the vessels still, however, being loaded with
blood, the inflammation in fact having become chronic, stimulants
may with propriety be applied directly to the affected parts; these
are employed, perhaps, with greatest advantage immediately after the
bloodvessels are unloaded by leeching, scarification, or punctures;
this practice is borne out by the result of experiment and observation.
It is seen, that after the vessels have become dilated, and the
blood has stagnated in them through the infliction of injury, or the
application of some stimulating substance, that the employment of
another and different stimulus immediately causes the contraction of
the capillaries, and the renewal of active circulation.
29
During an inflammatory attack, the patient should be allowed very
little food, and what he does receive must contain little nutriment in
proportion to its bulk. But in many cases it is unnecessary to enjoin
such abstinence, as the patient has no appetite, and refuses food.
In inflammation of deeply-seated parts, such as the apparatus of some
articulations, it is a frequent mode of assisting the completion
of resolution to excite inflammatory action in an external, and
consequently less vital and important part. This is accomplished by the
application of stimuli, caustics, cautery, setons, &c.
It appears that the stimulating substance produces an incited action
of the bloodvessels, or a revulsion, according to the older authors,
in the part to which it is applied; and that, consequently, the
neighbouring arterial trunks, in order to sustain that incited action,
supply the part with a larger proportion of their contents than it
usually receives; and the necessary consequence of the stimulated part
receiving an additional supply of blood is, that the part originally
inflamed receives less. The effect, indeed, seems analogous to that
of topical bleeding, with this difference—that it is more permanent.
Besides, it determines suppuration on the surface, and so renders it
less necessary for the vessels to produce pus in a worse situation—the
deeper seated parts.
But it must be borne in mind, that this method is not to be resorted to
in the commencement, or during the active state, of the inflammatory
action, but only when that action has begun to decline, otherwise the
disease may be much aggravated, instead of being relieved.
If, notwithstanding all the means employed to procure resolution,
the inflammatory action continues unabated, the result next to be
desired and accelerated is Suppuration; and with this view, it becomes
necessary to change the treatment, both local and general.
Above all, disuse and a proper position of the affected part must not
be neglected. Unless absolute repose is strictly enjoined and attended
to, and the return of blood from the inflamed tissues is favoured,
very great difficulty will, in the majority of cases, be experienced
in removing any of the signs or symptoms of inflammatory action, even
by the most energetic means, general or local. This will be more fully
insisted upon in the progress of the work.
OF SUPPURATION AS A CONSEQUENCE OF INFLAMMATORY ACTION.
It has already been stated, that the blood is stagnated in the
capillaries occupying the centre of the inflamed part, as well as
extravasated in the contiguous cellular tissue. Pus has long been
considered as a secretion; but, from the time of Mr. Hunter downwards,
a great similarity between the globules of pus and those of blood
has been recognised: the former, however, are spherical, larger, and
rougher on the surface, and are not so regular in size as those of
blood; their diameter is between 1/2000 and 1/3000 of an inch, although
some of the globules may be occasionally seen a little larger or
smaller than these measurements. Smaller particles are also detected,
the molecules of30 the pus globules, each of which contains two or
three. These molecules are insoluble in acids, soluble in caustic
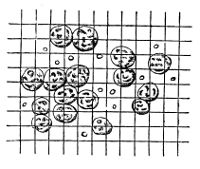 alkalis, and can be freed from the fibrous capsule in which they are
contained, and of which the pus globule is composed, when treated
with acetic acid. The appearance of the pus globules and molecules
is here shown upon a scale, the squares of which are 1/4000 of an
inch. These small particles were pointed out to me by my friend, Mr.
Gulliver, nearly two years ago, as constituting an important element
in suppuration. It results from his observations that the entire pus
globule is composed in its central part of these minute molecules,
the diameter of which is from 1/10666 to 1/8000 of an inch, cemented
together, as it were, by a superficial deposit of matter possessing
all the properties of coagulated lymph. And these minute nuclei
constitute a proximate animal principle, possessing such well marked
characters as to justify us in regarding them as peculiar in their
nature, and essential to the composition of the pus globule. Thus
they resist putrefaction with remarkable pertinacity, are very dense,
and spherical in form, and are insoluble in some acids which act with
facility on albumen, fibrin, or the blood-corpuscle. They are easily
seen by treating a little recent pus with sulphurous acid, which so
acts on the pus-globule as to render the nuclei distinctly visible
through its fibrinous capsule; by sulphuric acid the external part of
the pus-globule is quickly dissolved, and the nuclei, somewhat shrunk,
are seen in considerable numbers floating separately about the field
of vision. The instrument used by Mr. Gulliver in these observations
was a compound achromatic microscope, with a deep object glass, having
one-eighth of an inch focal length.
alkalis, and can be freed from the fibrous capsule in which they are
contained, and of which the pus globule is composed, when treated
with acetic acid. The appearance of the pus globules and molecules
is here shown upon a scale, the squares of which are 1/4000 of an
inch. These small particles were pointed out to me by my friend, Mr.
Gulliver, nearly two years ago, as constituting an important element
in suppuration. It results from his observations that the entire pus
globule is composed in its central part of these minute molecules,
the diameter of which is from 1/10666 to 1/8000 of an inch, cemented
together, as it were, by a superficial deposit of matter possessing
all the properties of coagulated lymph. And these minute nuclei
constitute a proximate animal principle, possessing such well marked
characters as to justify us in regarding them as peculiar in their
nature, and essential to the composition of the pus globule. Thus
they resist putrefaction with remarkable pertinacity, are very dense,
and spherical in form, and are insoluble in some acids which act with
facility on albumen, fibrin, or the blood-corpuscle. They are easily
seen by treating a little recent pus with sulphurous acid, which so
acts on the pus-globule as to render the nuclei distinctly visible
through its fibrinous capsule; by sulphuric acid the external part of
the pus-globule is quickly dissolved, and the nuclei, somewhat shrunk,
are seen in considerable numbers floating separately about the field
of vision. The instrument used by Mr. Gulliver in these observations
was a compound achromatic microscope, with a deep object glass, having
one-eighth of an inch focal length.
In many constitutions, the slightest incited action of the vessels
is followed by the formation of pus, and the appearance of a depôt
of purulent matter is often the first indication that such action
has existed; but in the majority of instances, the deposition of
pus is preceded by the usual characters of well-marked inflammatory
action. Suppuration occasionally occurs without previous solution of
continuity; for pus is frequently contained in the serous and mucous
cavities, when no breach of continuity can be discovered, at least
we find a fluid not distinguishable from purulent matter; it may be
a vitiated secretion, but still it presents the usual characters of
pus. But it occurs, generally, when there has been a previous læsion
of structure, and in this case its progress is most distinctly marked.
In exposed cellular texture, for example, particles of blood are
effused; the serum is afterwards absorbed, and the lymph remains;
this latter gives transmission to minute vessels which deposit the
purulent fluid, whilst others secrete particles of organised matter
to form granulations, in order to repair the loss of substance. This
process is often unattended with any great degree of constitutional
disturbance, because the fibrin effused sets a bound to the pus, and
is the provision31 against its being mixed in large quantities with the
blood. In healthy suppuration, the separation of fibrin and pus from
the blood in this way seems to have direct relation to each other;
and in unhealthy inflammation, when this does not take place, the
consequences are mixture of pus with the blood as formerly noticed. In
the latter form of suppuration the fibrin, instead of being assimilated
to the contiguous mass, is mixed with the pus; hence the proneness
to putrefaction of such discharge, and its disposition to coagulate
spontaneously when evacuated. This kind of suppuration, being matured
generally without thickening of parts, has been sometimes pointed out
as suppuration independently of previous inflammatory action.
After purulent matter has begun to accumulate under the surface, the
pressure thereby occasioned produces condensation of the neighbouring
cellular tissue, which, along with the previously effused lymph,
forms the parietes of the abscess; and in proportion as the matter
accumulates, the cavity enlarges by the successive processes of
ulceration of portions of its parietes, by continued effusion of lymph,
and by farther condensation of the surrounding parts. Thinning of the
parietes takes place by ulcerative absorption, particularly towards
the surface—or, if that be difficult, towards a mucous outlet—as is
exemplified by the bursting into the bowels or bronchiæ of abscess of
the liver.
But in some instances, when no lymph is previously effused, and no
cyst is formed, the matter is not confined, but pervades the cellular
substance extensively, and is generally followed by more or less
sloughing of that tissue, and by great constitutional disturbance. This
most frequently occurs in patients of a debilitated habit, in whom
the incited action has been so slight as not to cause the effusion of
lymph, by which nature usually sets bounds to the suppurating process.
M. Gendrin advanced the opinion that pus was nothing but transformed
blood; but his experiments on frogs are at least doubtful, since Mr.
Gulliver, on repeating them, could not by any means induce the process
of suppuration in these animals. It has been rendered probable by
this gentleman’s observations that suppuration is a sort of proximate
analysis of the blood, the fibrin being added to the contiguous
parts, as in causing them to swell, forming the cysts of abscesses;
the blood globules altered into pus being discharged as useless and
excrementitious matter.
Pure pus is heavier than water, of a yellowish-white colour,
somewhat of the consistence of cream. It is very little inclined to
putrefaction, less so, perhaps, than any animal fluid not oily. It
is composed of globules, and a clear transparent fluid, coagulable,
it has been said, by the muriate of ammonia. When a solution of this
salt produces any change, it is by rendering the pus more ropy; not
coagulation, but a sort of gelatinisation follows. It is said also to
be sweet and “mawkish to the taste.”
In unhealthy pus, such as already noticed, or in vitiated
muco-puriform secretion, the colour and consistence are different, and
flakes, resembling portions of lymph, are seen floating in it: they
consist of32 fibrin thrown off with the pus, instead of being used for
reparation and bounding the extent of the abscess; and by this latter
circumstance such fluid is distinguished from the pure or laudable pus.
In purulent matter also, especially that of an unhealthy character,
the existence of a quantity of sulphureted hydrogen is indicated by
the blackening of silver probes, and of various substances applied to
the sore. It is necessary to bear in mind, that a matter resembling
pus in many particulars, but in reality differing essentially from it,
has generally been regarded as true purulent fluid; for it results,
from some observations of Mr. Gulliver, that the pulpy matter, so
frequently found in the substance of fibrinous clots of the heart and
veins, is simply fibrin which has coagulated and passed into the state
of softening, which he regards as a very frequent elementary disease.
The subject is one of great interest, because it is connected with the
theory of suppuration, and tends to modify materially our views on the
pathology of the veins.
The symptoms attendant on suppuration vary much according to the
nature of the parts involved. In general, it is accompanied with the
subsidence of acute pain and fever; but, in unyielding textures, the
increase of swelling, by the formation of purulent matter, is often
attended with an aggravation of the symptoms, and with an increase
of danger to the structures affected. The pain which accompanies
suppuration is dull, and attended with a sensation of fulness and
throbbing, and an increase of the tumour; ultimately the parietes
of the abscess become absorbed, and the collection, being more
superficial, the most careless observer must be convinced of its
existence, by the less equivocal signs of fluctuation and pointing.
In general, especially when the abscess is deeply seated, a greater
or less degree of œdema surrounds it, producing a soft pitting
tumour; but not unfrequently, when the degree of excitement is more
intense, lymph, instead of serum, is effused, rendering the part more
hard and resisting: in such cases it may be difficult to discover
the existence of purulent matter, and the tactus eruditus, as it is
called, will be found of material service; for, though pus is neither
acrid nor corroding, still, if allowed to remain for any long period,
much mischief may be caused—the bones may become diseased—muscles
and tendons may slough—and the matter may discharge itself, by means
of ulceration, into certain cavities and canals, and produce very
serious consequences. Of the bad effects produced by the pressure and
irritation of extensive and undisturbed collections of purulent matter,
every practitioner must have seen numerous examples. Still, through
prejudice, erroneously conceived opinions, or servile imitation, the
greatest dread seems, with many, to exist of the practice of giving a
free exit to the contents of such depôts.
The symptoms and sensible signs of suppuration are usually preceded
by shivering, recurring at intervals, and commonly terminating in
profuse perspiration. But this is by no means an unequivocal sign of
the occurrence of suppuration; and this process very often takes place
without any feeling of rigor.
The older authors supposed that pus was derived from the solids—or that
it was formed by the melting of dead animal matter—or33 that it was the
result of putrefaction; in accordance with which latter opinion, the
term pus was given to the fluid; but such opinions have long since
been justly exploded. Pus is generally supposed to be separated from
the blood by the secreting power of the bloodvessels of an exposed
and inflamed part, in consequence of their having assumed a new
mode of action. The secretion from exposed surfaces is not at first
purulent, but is transparent, serous in fact, and is somewhat of a
gelatinous appearance; and it is only, it is said, after exposure to
the atmosphere for some time, and when drying, that it presents the
appearance of globules. Pus is often formed where the secreting surface
has not been exposed to the air; on opening an abscess, the parietes
of which had been previously entire and not much attenuated, purulent
matter of the usual properties is discharged. It has been asserted
that pus globules may be formed independently of any vital action; and
that, if the serous fluid be removed immediately after its secretion
by a granular surface, and kept in a temperature similar to that of
the inflamed part, and be at the same time freely exposed to the air,
globules will appear in as short a period as when the secretion is
allowed to remain in contact with the sore. Some have also supposed
that the mere admission of air into the cellular substance causes
suppuration; but this is far from being correct. In chronic purulent
depôts, however, the admission of air, by favouring putrefaction
probably, often produces most serious results; other causes are
generally in operation at the same time, as will be afterwards more
fully explained.
Pus was formerly regarded as irritating and corroding, and was
therefore carefully removed from every granulating sore; but purulent
matter, though it may prove a source of irritation to the neighbouring
parts, does not disturb the surface which secretes it, but, on the
contrary, protects the tender granulations, and acts as a temporary
cuticle. A crust is formed by the evaporation of the thinner part of
the fluid; and we frequently see small sores healing rapidly when thus
protected. In some instances, we adopt the hint given to us by nature,
and produce a scab by the application of powders, lunar caustic, &c.
The discharge does not always consist of laudable purulent matter.
Pus formed in the diseased part itself has particular characters,
according to the tissue involved; thin and greyish in bones, opaque and
caseiform in cellular tissue, flocculent in serous, and greenish and
thready in mucous membranes; it is said to be reddish in the liver, and
yellowish-grey in muscles. Its sensible properties are various, often
very offensive when proceeding from a cavity containing decayed bones,
and it degenerates in consequence of disturbance of the constitution,
or of the part affected. It is also frequently suppressed, in
consequence of over-action in the vessels of the part, or from debility,
partial or general.
Suppression of a purulent discharge is to be regarded as an untoward
symptom, fraught with considerable danger, being generally followed by
the most violent constitutional disturbance. Certain cases would seem
to warrant the belief that a species of metastasis occurs; that the
matter is absorbed, and again deposited in some34 other part, perhaps
of the utmost importance in the animal economy. The danger arising,
when the pus is not separated from the blood, has already been adverted
to. No wonder, if from any cause it does not escape by its accustomed
channel, that an effort should be made to deposit it somewhere else,
for the temporary relief of the system. The most vascular parts are
commonly chosen, as the lungs, spleen, and liver. In the cavities
of joints, also, matter is often found in great quantities. This is
sometimes indicated by the occurrence of tenderness and swelling for
only a short period previously; but, in other cases, its presence
has never been suspected. In purulent collections, after wounds from
accident or operation, on the suspension of the discharge, the patient
becomes affected with severe constitutional irritation, and gradually
sinks; the existence of purulent depôts in the viscera of the chest or
abdomen, being perhaps not indicated by any, unless very equivocal,
symptoms, and these appearing only a short time before dissolution. A
late writer has endeavoured to connect this with inflammation of the
veins; but such an opinion is not borne out by observation, although
the two circumstances may occasionally coexist. In many cases the veins
of a limb are found filled with pus, yet their coats present no marks
of inflammatory action having existed in them. Their mouths are open in
the wound, from failure of that healthy action by which they would have
been closed by coagulated lymph, and the matter appears to be taken up
by them as secreted.
From the discharge varying according to the state of the system, the
latter can in general be accurately ascertained by examination of the
sores which afflict the patient.
In collections of matter not far removed from the surface, the most
superficial, and generally the most dependent, portion of the parietes
appears inflamed; its inner surface is gradually absorbed; and, when
it has thus become attenuated, a portion of the integument sloughs or
ulcerates. A communication is established with the diseased parts,
through the external surface, thus providing an aperture for the
evacuation of the matter—of extraneous substances—or of parts of the
body which have either mortified, or otherwise become useless to the
system. In such collections, more especially if deeply seated, the
matter generally seeks the surface, or extends in the course of the
bloodvessels.
Cold abscesses, as they are called, often contain as much flaky
fibrinous matter as true pus: hence one of the signs of inflammation,
swelling, is absent; the fibrin being discharged instead of having been
added to the neighbouring parts.
As formerly remarked, suppuration occurs much more readily in some
constitutions than in others; and patients peculiarly liable to the
formation of abscesses, without any great degree of previous excited
action of the bloodvessels, are said to labour under Struma or
Scrofula. These terms are by some used to denote a distinct or
specific disease, while others consider them merely as a peculiar state
of the constitution.
The strumous diathesis is said to be marked by hair and irides of a
very light colour, and by the skin being of a peculiar white hue;35 but,
in some instances, the complexion is unusually dark and sallow. The
upper lip generally presents a swollen appearance, as also the columna
and alæ of the nose. The organization throughout is delicate, and the
patient is frequently of a handsome, though infirm, structure.
Constitutions, in every respects strong and originally vigorous, may,
from various causes, become weak, and present many of the symptoms
usually termed scrofulous. I recollect a young patient, born of healthy
parents, who had enjoyed excellent health, becoming covered with ulcers
and chronic abscesses, in consequence of exposure to cold during
menstruation.
To the continued irregular and imprudent exhibition of mercurial
alteratives, as they are called, may be attributed the cachectic and
scrofulous constitutions of many thousands of patients of all ages.
The strumous diathesis is said to depend upon a want of balance, or
proportion, between the solids and circulating fluids. Want of action
and power in the organs forming and circulating the blood, disordered
digestion, and various other circumstances which it is unnecessary
to detail, have also been considered as causes of this state of the
constitution.
Many suppose that the diathesis, or a disposition to the diathesis,
is always congenital; and this opinion is supported by the majority
of cases. However, certain circumstances produce a scrofulous habit
of body in patients who previously appeared to be vigorous and
healthy, and untainted with any peculiar disposition to disease. Of
these predisposing causes may be mentioned, a poor diet, an impure
atmosphere, exposure to damp and cold, inattention to cleanliness, the
latter circumstance acting sometimes by producing local irritation:
in fact, whatever deranges the general health, seems, in many cases,
to induce the strumous diathesis. Some constitutions are incapable
of resisting any unusual incitement of the vascular system, or of
repairing the consequences of the action, or of any injury, in
whatever way inflicted. In such individuals, all the parts of the body
are deficient in power—some, however, are more so than others, and,
consequently, more readily give way; thus, the lymphatic system, the
mucous membranes, the skin, the bones and their coverings, generally
suffer in the first instance.
Glandular swellings of all kinds, and in all situations, often
followed by suppuration, are apt to occur from irritation of various
descriptions, but more so in constitutions originally weak, or which
have become debilitated by disease or any other cause. The larger
glandular tumours are formed by congregation and agglutination of
the smaller ones, and by the deposition of adventitious matter in
the connecting cellular substance; separation of the smaller tumours
composing these, naturally, or under the use of deobstruents exhibited
internally, or applied to the surface, is a highly favourable sign, and
equally encouraging to the surgeon and the patient.
Dentition, the presence of carious teeth, of stumps of teeth;
excoriations behind the ears, eruptions on the scalp, affections of
the lining membranes of the eyelids, mouth, or nose, of the skin of
the face, are36 daily found giving rise to glandular swellings in the
neck; whilst irritations in the urethra, excoriation or slight disease
about the anus, corns or sores about the feet or toes, produce similar
affections of the glands in the groin. Such sources of irritation are,
of course, to be looked for in the first instance, and will often
materially influence the diagnosis, though too much is occasionally
attributed to their influence. Such glandular tumours, however,
sometimes occur spontaneously, or, at least, without any evident
cause. They have been mistaken for other diseases, according to their
situation—for aneurism, hernia, or venereal bubo; the latter mistake is
often committed unintentionally by the ignorant, or designedly by the
unprincipled.
Tumours formed by the enlargement of glands are frequently productive
of dangerous consequences. If situated in the neck, they may render
breathing and deglutition extremely difficult, and in the event of
their suppurating, the purulent matter may be discharged into the
trachea or gullet; fatal results have followed the giving way of an
abscess into the former canal. The breathing is also seriously impeded
by enlargement of the bronchial glands, by the pressure of which
the lungs may be much condensed, and unfitted for their functions.
The immediate effect of enlargement of the mesenteric glands, is
interruption to the passage of the chyle, and a consequent decline of
the powers of life. Such tumours in the abdomen have been mistaken for
enlargement of the liver, spleen, ovarium, &c., and the most noxious
treatment employed.
Inflammatory glandular enlargements terminate either in resolution, in
delitescence, or in suppuration; sometimes in death of the part. When
the tumour, after having attained a certain size, gradually disappears,
it is said to be resolved; when, however, it is rapidly discussed, it
terminates in delitescence; the difference between the terms being
the same as when used to express the corresponding terminations of
inflammatory swelling in general.
Suppuration is by far the most usual termination, and the matter is
frequently evacuated through numerous small apertures, exposing the
gland denuded and prominent in the middle of the chasm; in such cases,
the gland proves the source of much irritation, and must be destroyed,
otherwise the cure is extremely tedious.
Though inflamed and swelled lymphatic glands very generally disappear
by suppuration, it is to be remarked that the conglomerate glands,
though often violently inflamed, seldom, if ever, have pus formed in
them; in mumps, for instance, the action often runs very high, yet
abscess of the parotid is rare. The submaxillary salivary glands are
often supposed and said to be inflamed and enlarged; the conglobate
glands superficial to them are in such cases only affected.
Collections of pus in the lymphatic glands or cellular substance, in
patients of a weak constitution, (whether naturally or in consequence
of disease,) are attended with little or no pain, or inflammatory
action; and although it is probable that inflammation does precede the
formation of such purulent depôts, still it is generally so slight
as not to attract the attention of the patient or his attendant. The
sensation is dull and uneasy, rather than painful; and, even after the
accumu37lation of a considerable quantity of purulent matter, redness of
the surface and pointing do not occur till a late period. The contained
matter is thin, flaky, and of a brownish colour. The collections often
attain a very great size, and, if improperly treated, terminate in the
formation of numerous and extensive sinuses.
The skin, particularly that of the face, becomes, in very many cases,
affected either primarily or secondarily with scrofulous ulceration,
which commonly extends to the neighbouring textures. The disease has
sometimes been mistaken for cancer, and other affections of a malignant
nature, and has received various names accordingly. The integuments
in the neighbourhood of the ulcer are of a purple hue, and become
undermined, from the extension of the disease in the subjacent cellular
tissue. The discharge is thin and gleety—the sore is of an unhealthy
and debilitated character, and makes but little attempt at reparation;
its surface is covered by a viscid fluid, and sloughing occasionally
occurs in consequence of the extreme debility of the parts. Numerous
sinuses frequently extend in a superficial direction, and render the
cure more tedious and complicated.
Those of a scrofulous constitution are most liable to be affected with
caries, softening, and other diseases of the bones and their coverings;
these, however, will afterwards be treated of, along with ulceration
of cartilages, diseases of ligaments and synovial membranes, lumbar
abscess, &c.; all of which affections, in the plurality of instances,
are connected with the strumous diathesis.
In the treatment of abscesses, the principal indications are, to remove
any degree of inflammatory action with which the surrounding parts may
be affected—to keep the part moist, clean, and at rest—to remove all
source of local irritation—to promote and accelerate the progress of
the matter to the surface—and, lastly, to give it free vent; for though
it sometimes happens that collections of purulent matter disappear,
still the occurrence is so rare, that to treat abscess generally when
in an advanced stage with the expectation of resolution would be highly
injudicious. By blistering and pressure, however, tumours containing a
small quantity of purulent fluid can occasionally be discussed. Warm
fomentations afford great relief, especially at the commencement, when
there still remains a considerable degree of surrounding inflammation.
These may be either what are termed anodyne, or not; in general,
fomentation with chamomile flowers or hops, contained in a woollen
bag, and wrung out of warm water, will be found the most convenient
and efficient, and is well entitled to the term anodyne, which is
usually applied to others of a complicated, and not more efficacious,
character. Poultices are of material service, particularly when the
collection is advancing to maturation; and their composition is of
little importance, provided they are moist, warm, and soft. Stale
bread soaked with hot water, or an equal quantity of grated bread and
linseed meal, (if not adulterated with mustard, as is sometimes the
case,) mixed with sufficient quantity of boiling water, form excellent
and soothing cataplasms. Their use, however, may be persevered in too
long; for, after an abscess has given way, the suppuration may be
kept up in conse38quence of continuing the poultice. The opening will
enlarge, the skin become undermined, loose, and flabby, the abscess
will extend, while the process of granulation may be in a great measure
suspended. In many cases, the poulticing cannot be continued until an
opening has formed naturally, and the cure is often much accelerated by
the artificial evacuation of the matter. When the abscess is situated
deeply, or beneath a fascia, a free and early opening must be made.
For example, when suppuration has occurred in the cellular tissue
beneath the fascia lata of the thigh, it at first naturally tends
towards the surface, but its progress is impeded by the tendinous
aponeurosis; a painful feeling of tension is thereby occasioned, and
the matter extends where there is least resistance, making its way in
all directions into the surrounding cellular tissue—separating the
muscles—isolating the arterial trunks—burrowing beneath the fascia
over the whole limb, and producing most serious, and often irreparable
mischief, with violent constitutional disturbance. The bad effects of
delay are again daily witnessed in neglected cases of paronychia; most
excruciating pain is produced—the system is seriously affected—the
tendons slough, and the member is rendered useless.
By the continued presence of purulent matter, absorption, ulceration,
caries, and even death, of bone, is frequently produced, all which
might have been prevented by its evacuation. If pus collect in the
neighbourhood of cavities or canals, it is of the utmost importance
that it be early discharged; and the evil effects of negligent and
dilatory treatment are well exemplified in the following cases:—A
patient had been allowed to suffer, for a long time, under an extensive
abscess at the lower part of the neck, beneath the origins of the
sterno-mastoid muscles. The abscess at length gave way externally; but
the patient was at the same time seized with profuse expectoration
of pus, and during expiration the air escaped through the external
openings in the neck. It was evident that the abscess communicated with
the trachea, and it also appeared to have extended deeply into the
mediastinum. The patient soon perished, but there was no opportunity
of examining the parts. In another case of extensive abscess at the
root of the neck, an opening was proposed, but delayed. At length, the
abscess gave way spontaneously; and from the circumstance of portions
of solid as well as fluid ingesta escaping by the external opening,
it was evident that the œsophagus had ulcerated. The cure was very
tedious, but ultimately complete, and apparently much accelerated by
free counter openings.
In suppuration of the cellular substance in the neighbourhood of the
anus, the matter may present itself externally, whilst it is making
extensive progress internally; and if a free opening is not made,
fistula ani is the result. The propriety of an early evacuation of
purulent matter in important, or very sensible, organs, such as the eye
and testicle, is very evident.
The larger arterial and venous trunks appear not to suffer from
suppuration, for in purulent depôts we find them entire, and much
thickened by copious effusion of lymph into their outer cellular coat
and sheath; the nerves, however, are not so much protected, or do39 not
appear to resist the pressure and insinuation of pus, and suffer along
with the other tissues.
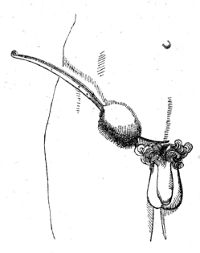 The most convenient and effectual mode of opening an abscess is with
a sharp-pointed bistoury, and the incision should vary in extent
according to the circumstances of the case. The straight instrument,
used as described and represented in the “Practical Surgery,” p.
56, will be found to answer best in deep-seated collections; in
the more superficial it may be slightly curved. It is used as here
shown, only that the edge of the knife should be turned more downwards
before the integument is divided by withdrawing it. The aperture must
always be made at the most dependent part, which is also, generally,
the thinnest; thereby a free exit is allowed to the matter. If the
incision be not made in a dependent part, a considerable quantity
of the matter will be retained within the abscess, and can only be
evacuated at the time by squeezing the parts—at all times a very cruel
and improper practice—applying compresses, &c., which produce much
irritation and unnecessary inconvenience to the patient. The cavity
of the abscess inflames, the discharge becomes bloody and putrid, and
great constitutional disturbance is apt to follow. When, again, the
opening is sufficiently large, properly placed, and the matter flows
out through the elasticity of the coverings, no air enters, the cyst
gradually contracts, and the cure is soon completed.
The most convenient and effectual mode of opening an abscess is with
a sharp-pointed bistoury, and the incision should vary in extent
according to the circumstances of the case. The straight instrument,
used as described and represented in the “Practical Surgery,” p.
56, will be found to answer best in deep-seated collections; in
the more superficial it may be slightly curved. It is used as here
shown, only that the edge of the knife should be turned more downwards
before the integument is divided by withdrawing it. The aperture must
always be made at the most dependent part, which is also, generally,
the thinnest; thereby a free exit is allowed to the matter. If the
incision be not made in a dependent part, a considerable quantity
of the matter will be retained within the abscess, and can only be
evacuated at the time by squeezing the parts—at all times a very cruel
and improper practice—applying compresses, &c., which produce much
irritation and unnecessary inconvenience to the patient. The cavity
of the abscess inflames, the discharge becomes bloody and putrid, and
great constitutional disturbance is apt to follow. When, again, the
opening is sufficiently large, properly placed, and the matter flows
out through the elasticity of the coverings, no air enters, the cyst
gradually contracts, and the cure is soon completed.
When the abscess has been deeply seated, and the incision made through
a considerable thickness of healthy parts, it is sometimes, though very
rarely, necessary to introduce a small piece of lint between the edges
of the wound, otherwise they may speedily adhere, and the discharge
of the matter be in this way prevented. In consequence of smart
hemorrhage, also, it may be proper to stuff the wound with lint, and
retain it for an hour or two; but in general the practice of stuffing
abscesses, or the openings into them, is hurtful. After the incision,
as already remarked, it is unnecessary and injurious to discharge the
pus by forcibly squeezing the sides of the abscess; the application
of a poultice will promote the evacuation of the matter, and allay
the irritation. In chronic abscesses of large size, it is sometimes
necessary to make a counter opening—that is, an opening in a part of
the tumour opposite to the original opening, in order that the matter
may be more completely discharged. Setons introduced into the cavity
of phlegmonous abscesses some time after their evacuation, are highly
injurious, as causing much irritation in parts which are already in a
morbid state of excitement; but in chronic 40collections, which show
no disposition to heal, their use may sometimes be followed by good
effects, on the same principle that they were hurtful in the preceding
case; if they should not cause a sufficient degree of excitement,
they may be smeared with some stimulating ointment. In extensive
collections, in which the matter is not sufficiently evacuated by the
external aperture, injections are by some recommended, and, perhaps,
occasionally employed: in those abscesses which are comparatively
recent, and in which the surrounding parts are still in a state of
over-excitement, they are quite inadmissible. The employment of setons
and injections in any case of abscess is not much to be commended or
trusted to. Caustic, the potassa fusa, may be frequently employed with
advantage for opening chronic abscesses, especially when they are the
consequence of glandular enlargement, and undermine the integuments,
which show no tendency to adhere to the subjacent parts. The potass
is best used in the solid form and well pointed; not in paste, as
is sometimes practised. By its application the unhealthy surface is
destroyed, and the surrounding parts are stimulated so as to assume
a sufficient degree of action to throw off the portions which have
become useless, and to form new and healthy granulations, whilst the
surrounding effusion of lymph or serum is for the most part speedily
absorbed. But it can never be employed in acute abscesses without
aggravating the disease; and in collections which are deeply seated,
it cannot be of much service, for in these a considerable thickness of
healthy parts must be destroyed, and if the potass be applied, it will
afterwards be necessary to cut through the slough, as was practised by
the older surgeons, in order to evacuate the matter and give relief to
the patient; or else to continue the application of the caustic for an
inordinate space of time, which is a practice altogether unnecessary,
extremely cruel, and productive of much irritation, constitutional as
well as local.
A too common result of abscess, when inertly treated, is the formation
of a Sinus; that is, a canal, the circumference of which is condensed
by deposited lymph, and which furnishes a discharge of unhealthy
purulent matter, frequently thin and gleety. Several sinuses frequently
unite, and evacuate their contents by one opening. Previously to
treating a sinus, its extent must be carefully examined by the probe;
this requires considerable caution, for the full extent of the canal
may not be discovered, in consequence of its tortuous course, or
from its diverging into collateral branches; or the probe, by being
used too forcibly, may pass into parts altogether unconnected with
the morbid cavity. Thus, in exploring a sinus at the lower part of
the leg, or in the foot, the probe may be pushed to a considerable
extent beneath the tendinous sheaths of the muscles, and induce the
surgeon to adopt treatment unnecessarily severe. In the treatment,
we may at first employ setons, injections, and graduated pressure,
as formerly explained; and if these fail, the canal must be freely
laid open by the knife—a mode of practice much more effectual; then
there is formed a cavity similar to that of a recent abscess, and to
be treated accordingly. Incision is most frequently necessary when
the sinus exists in adipose substance, in tendinous structure, in
parts possessed of little vitality, and in patients of a sluggish and41
enfeebled constitution. In sinus, as well as in chronic abscess, the
potass is of essential service; a stick of it may be introduced into
the canal, and if the sinus is superficial, the integuments may be
divided by this caustic as effectually as by the knife. The indolent
and callous surface of the sore is thereby destroyed, and the effects
are similar to those which have been already mentioned, when speaking
of the use of potass in abscess; in fact, by its application the sinus
is transformed into an acute and open abscess. Foreign bodies, such as
diseased and dead portions of bones, must be early removed; for it is
to be remembered that these are much more frequently the cause than the
consequence of suppuration.
The healing of an abscess which has been opened closely resembles the
process of union by the second intention in a flesh wound; granulations
arise, attended by the secretion of pus, the cavity gradually
contracts; the surrounding effusion is absorbed along with a portion of
the adipose matter; and on the granulations reaching the surface, new
skin is formed, and the parts coalesce.
After abscesses have been opened, the fomentations, poultices, or
warm-water dressing, as recommended in the treatment of ulcers, are
to be continued, but only for a limited time. The power of the system
must be carefully supported by exposure to a pure atmosphere; by
nourishing food; by the exhibition of wine, tonics, and such medicines
as promote digestion. In cases where the system is unusually inert, it
may be proper to administer stimulants. The most powerful stimulants
are frequently necessary, and by steady perseverance in the use of
them, patients have often been saved in very hopeless circumstances.
Great attention must be paid to the bowels, and the secretions poured
into them, for on the condition and quality of these the state of
the constitution materially depends. The internal Use of cantharides
is often advantageous in chronic suppurations and abscesses, but
it is inadmissible in cases where enlarged glands occupy dangerous
situations, either externally or internally; unless the tumours are in
progress towards resolution, suppuration is certainly induced, and may
be productive of the worst consequences. The glands not unfrequently
become enlarged during the exhibition of this medicine; and such an
occurrence must be watched attentively. In illustration of the good
effects of stimuli in certain cases, it may be mentioned that the
cavities of abscesses are often speedily effaced by granulations, and
that obstinate sores frequently contract and cicatrise, after the
occurrence of a febrile attack, though they had previously shown no
disposition to heal.
In glandular swellings, Deobstruents, as they have been called, are
used; and with this view, mercury is often had recourse to; this
medicine, however, instead of producing a salutary effect, very
generally tends still farther to impair the constitution. Preparations
of iodine, exhibited both externally and internally, appear to be
sometimes of use when the swellings have become stationary, or are
inclined to subside. Iodine may be given in combination or not with
iron. It is a medicine exhibited very generally and indiscriminately,
and is very much more trusted to than it deserves to be. When the
tumours are irritable, fomentations may be employed, and advantage42
taken of sea-bathing, warm or cold. The common adhesive or soap
plaster, spread on soft leather, or the ammoniacal plaster, are often
applied with advantage to indolent glandular swellings. Blistering is
sometimes resorted to with good effect, and in some situations pressure
may be usefully employed.
In the treatment of large indolent collections, it was proposed by
Mr. Abernethy to make a small and indirect aperture, and to evacuate
the contents of the abscess as often as the matter accumulated; but a
degree of constitutional irritation frequently supervenes upon this
proceeding, and the discharge becomes bloody, putrid, and mixed with a
considerable quantity of gaseous fluid. The discharge of blood probably
arises from the usual support being taken away from the vessels
ramifying on the surface of the cavity, in the same way that blood is
effused into the cavity of the abdomen, in consequence of the too rapid
evacuation of the serum in ascites.
Suppuration, more especially when extensive and long continued,
is attended with a peculiar species of fever, termed Hectic. This
fever is the remote consequence of local injury, or disease, whereas
symptomatic inflammatory fever is the immediate one. The incessant and
long-continued addition of pus to the blood may be the cause of hectic
fever. In cases of pulmonary consumption, pus globules are almost
uniformly detected in the blood. This fact has been noticed by Dr. Davy
and Mr. Gulliver. The pus is probably carried along the capillaries,
where it is always forming in chronic abscesses: in short, all the pus
formed is not separated from the blood. Hectic probably arises from
the never-ceasing addition of a little pus to the blood, inflammatory
fever from the sudden addition of a large quantity. In long-continued
disease, particularly internal, the hectic occasionally occurs before
the existence of suppuration is indicated; and it does not always
supervene upon suppuration, even though extensive. Hectic has been
supposed to arise from the absorption of pus; but pus cannot well be
absorbed without disintegration of its particles (and then it would
be no longer pus), for their diameter exceeds that of the more minute
bloodvessels and absorbents. Abscesses occasionally disappear, without
this event being followed by any unpleasant symptom.
Hectic fever is most apt to arise in constitutions originally weak; and
usually either from some incurable disease of a vital organ, or from
extensive affection of a part not essential to life; but it may also be
induced without any local assignable cause.
The general symptoms are those of a low and gradual fever, attended
with great debility; the pulse is frequent, unequal, small, and sharp;
the general surface is pale; there is flushing of the face, hands, and
feet; the skin, at one period, is cold and clammy, sometimes dry and
rough—at another, it is bathed in profuse perspiration, especially
towards evening; chills alternate with flushing; the appetite is much
impaired; diarrhœa supervenes; pale-coloured urine is voided in great
quantity, often with a lateritious sediment; there is want of sleep,
and great anxiety; the eyes are sunk, and of a glassy hue; the features
become changed; there is great emaciation; the patient, gradually more
and more weakened, falls into a state of coma, and expires.
A condition, somewhat resembling sympathetic fever, occasionally43
supervenes in a constitution that has been suffering from hectic,
when any additional irritation occurs, and this fever has been called
Irritative. The sanguiferous system becomes more excited—the
secretions are suspended—the sensorium is disturbed; but still the
symptoms are accompanied with the peculiar debility characterising the
state of hectic. It frequently follows the opening of large chronic
abscesses by a minute aperture, in the manner formerly described and is
relieved only by free evacuation of the confined matter.
In the treatment of hectic, the local disease giving rise to the
symptoms, if it cannot be cured by other means, must be removed by
operation. Thus, if hectic is consequent on long-continued, but not
extensive, disease of bone, the affected portion is to be taken away;
if from extensive chronic disease of an arm or leg, the limb must be
amputated.
In general, the removal of the hectic cause is followed by immediate
melioration of the symptoms, even though the patient has been reduced
to an almost moribund condition: the feeble hectic pulse of 120 or 130
sinks in a few hours to 90, and becomes more full and strong; anxiety
and restlessness cease, and a patient sleeps soundly the first night
after the operation, who for weeks had scarcely closed his eyes; the
cold sweats and colliquative diarrhœa immediately subside, and the
urine loses its sediment; in effect, all the hectic symptoms disappear,
and are succeeded by such as indicate a marked improvement in the power
and energy of the constitution; and the rapidity with which these
changes take place is in many cases truly astonishing. Nourishing food,
wine, tonics, &c., must be given, in the first instance sparingly, and
afterwards gradually increased in quantity, according as the stomach
can bear them; for it is not to be overlooked, that incautious and too
liberal use of them may be productive of irretrievable evils, as the
action of the system may be increased beyond its resources, in the same
way as the imprudent application of stimulants to a part debilitated
by an excessive degree of cold causes its sphacelation, in consequence
of the arterial action induced being greater than what the power of
the part can support. The mineral acids may be useful in checking
the inordinate perspiration; opium, astringents, and absorbents, in
arresting the diarrhœa; but all are of little avail unless the exciting
cause is removed, and to this latter circumstance the attention of
the practitioner ought therefore to be chiefly directed. It is not
always quite safe, however, to free the patient at once of a great
suppurating drain. Upon the healing up of extensive and long-continued
ulcers, it is often necessary, in order to prevent oppression of and
congestion in the viscera of the chest, abdomen, or head, to insert an
issue or seton, and gradually withdraw it. In amputations also, more
especially in patients above the middle period of life, to rid them of
disease which has caused hectic and wasting, in consequence of profuse
discharge, it is often advisable to keep part of the wound open, so
that it may suppurate, heal, and dry up slowly.
Mortification, or the death of a part, is also one of the results
of inflammatory action, and the term has been subdivided into
44Gangrene and Sphacelus. Gangrene is that state in which the
larger arterial and nervous trunks still continue to perform their
functions; a portion of the natural temperature remains, and the part
may be supposed still capable of recovery. Sphacelus, again, expresses
complete death, when, putrefaction being no longer resisted, the part
becomes black, cold, insensible, and fetid; but, in general, the
distinction between the terms is not strictly attended to. A division
of more importance is into humid and dry, or traumatic and chronic,
gangrene; humid or traumatic being applied to mortification produced by
external injury; dry or chronic to that resulting from a constitutional
cause.
Mortification is not always a result of inflammation; it is sometimes
preceded by incited action of the vessels, sometimes not. It follows
as a matter of course that if inflammatory action is so violent as to
cause stagnation of blood in most or all the vessels of a part, and
this is continued, there must be a consequent failure of nutrition,
which will terminate in mortification.
Humid or traumatic gangrene frequently occurs without previous
inflammation, the injury being so severe as at once to deprive the
part of its vitality. Dry or chronic mortification is often unpreceded
by inflammatory action, or at least it is slight and of very short
duration. It is preceded by stagnation, or is at all events coincident
with this stagnation, not in the smaller vessels only, but in the
trunks leading to the affected part. In humid gangrene, swelling with
erethismus generally precedes the death of the parts; whereas in
the dry, whether the surface change colour immediately or not, they
shrink immediately. In the former they quickly lose their vitality,
and consequently retain a considerable portion of their fluids; in the
latter the process is much slower, and they become dry and shrivelled.
The most common remote cause of spontaneous mortification is a rigid
state of the arteries, most frequently met with in the inferior
extremities of elderly persons, in consequence of the deposition of
calcareous matter between the internal and middle coat; this calcareous
degeneration may be confined to a part of the limb, or may pervade
the whole of it, and even extend throughout the arterial system.
There are many cases in which disease of the arteries has existed,
though no gangrene occurred; but this by no means invalidates the
assertion, since, when arteries are thus affected, the part cannot
withstand sphacelus when exposed to any of its immediate causes. An
attempt has been made to connect mortification with an inflamed state
of the arterial coats. This opinion is not confirmed by experience.
Obstruction from coagulation of their contents, and inflammation of
the venous trunks, sometimes precedes death of the extreme parts in
old people, and seems to act as a direct cause. After wet seasons,
spontaneous gangrene has prevailed as an endemial disease on the
Continent, where rye is a principal article of food. The rye is subject
to a disease called Ergot; the grains become large, black, and have a
horny consistence; and the use of it, when thus diseased, is assigned
as the cause of gangrene. The patients who have suffered from the use
of this ergot or cockspur rye have experienced pain and heat, with
swelling, generally in the lower limbs,45 though occasionally in the
upper. These symptoms abating, the parts became cold, insensible, and
discoloured, and were gradually separated from the body. The disease
attacked patients of both sexes and every age, did not appear to be
infectious, and was frequently fatal. It has occurred in this country
from the use of unsound wheat. A tendency to mortification sometimes
arises from a peculiar state of the atmosphere, want of cleanliness,
poor and irregular diet, &c. Cancrum oris, for example, and sloughing
of the pudendum in children, occur in those of the poorer classes who
live in low, damp, and dirty situations; and little or no incited
action precedes the sloughing. The same may be said of the phagedænic
affections of the genital organs. Mortification and ulceration seem to
differ merely in this,—in the latter, a part which, from any cause, is
unfitted to remain a portion of the living body, is only prevented from
dying by absorption just as it is about to lose its vitality; whilst in
mortification the part perishes too soon, or in too great quantity, to
admit of absorption. Sloughing phagedæna is a sort of connecting link.
Mortification, to a greater or less extent, may be produced in any
constitution, and at any age, by the application of heated substances,
caustics, acids, &c.; by the effusion of acrid matter into the cellular
substances, as urine or putrid sanies; by the interruption of the
circulation and nervous energy, as from ligatures or improperly applied
bandages—or by natural strictures, as those in hernia and paraphymosis;
by continued pressure, more especially in such patients as have, from
long suffering and confinement, had the powers of the circulating
system weakened; and by violent contusions, as in fractures, compound
luxations, and gunshot injuries. A frequent source of mortification,
in inclement seasons and climates, is exposure to extreme cold. In
this case, the cold is not the direct, but the indirect cause; the
power of the parts is very much weakened by exposure to the low
temperature, and is thereby rendered incapable of resisting the incited
action which follows the stimulus of sudden transition from cold to
heat, even though the degree of increase in temperature should not
exceed that of the natural standard. That cold is not the direct cause
of mortification, has been undeniably proved by facts derived from
military practice. No symptoms of inflammation or gangrene occur when
the soldier is on duty, and continuously exposed to severe cold; but
they speedily present themselves after a rapid thaw has commenced, or
after the soldier has imprudently approached a fire. Soon after the
half-frozen person has begun to feel a little more comfortable from
sudden warmth, he becomes aware of pain, attended with a sensation of
itching in the extremities, generally the lower, which are considerably
swollen, and of a dull red colour; these, and other symptoms of
inflammation, are of no long duration, the action speedily runs its
course, and the part soon plainly indicates that gangrene has commenced.
When gangrene follows the tight application of a ligature, the death
of the part seems to depend more on obstruction to the circulation of
the blood, than on any diminution of the nervous energy, for we do
not observe that paralytic limbs are peculiarly liable to gangrene.
The surgeon frequently takes advantage of the fact that a part soon
dies when its supply of blood is cut off, or its return in the46 veins
interrupted; and has recourse to ligature for removal of parts, When he
considers it inexpedient to employ cutting instruments.
Mortification may be produced by the above-mentioned causes, either
immediately or consecutively; and it will occur in some constitutions,
or states of constitution, at some periods of life, in some structures,
and in some parts of the body, more readily than in others.
Inflammatory action is seldom so intense as to terminate in death of
the part, unless the power of that part has been diminished by previous
local or constitutional disease, or by injury; and the inflammation
preceding gangrene is all along attended by symptoms of so well-marked
debility, both local and general, that it is frequently designated the
Inflammatio Debilis. Of inflammatory affections, the erysipelatous
most frequently terminates in gangrene; in other words, the power of
resisting incited action is not so great in the cellular tissue and
skin as in other parts of the body.
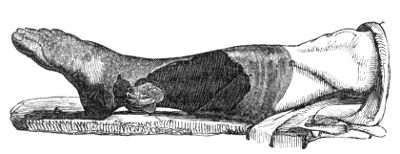
The period at which the symptoms of gangrene appear after an accident
varies, in general, according to the severity of the injury. As
was already observed, the part may be immediately deprived of its
vitality—if not, symptoms of gangrene sometimes appear within a few
hours after reaction has taken place; while in other cases, tension,
pain, and heat occur, and may continue for a longer or shorter time,
according to the degree of power remaining in the part. Tension often
exists to a great extent after severe injuries, from extravasation of
blood or serum; the functions of the vessels are thereby interrupted,
and gangrene is inevitable. As the action proceeds, the pain and heat
often subside—the parts become flaccid—dark-coloured serum is effused
beneath the cuticle, forming what are termed Phlyctenæ—the skin becomes
dull and livid—dark streaks extend along the limb, perhaps from the
colouring matter of the blood transuding, as in commencing putrefaction
in the dead body—air is effused into the subcutaneous cellular tissue,
causing a sense of crepitation when pressed by the finger—sloughs form,
either black or of an ash colour—and the gangrene involves a greater
or less extent of the limb. The mortification is here represented as
attacking a limb that had suffered from compound fracture. The dark
part around and above the protruded bone was in a state of sphacelus.
The dorsum of the foot and the integument towards the knee were only
gangrenous. The patient was advanced in life, and the state of the
constitution such as to induce a belief that there was a predisposition
to mortification. The removal of the limb was, under the circumstances,
reckoned inexpedient. In some instances, the mortifica47tion is most
towards the surface; in others, it is chiefly amongst the deeply seated
parts. Sudden cessation of pain is generally regarded as an unequivocal
sign of the occurrence of gangrene, especially in the internal viscera;
but it not unfrequently happens that the painful sensations suddenly
cease, whilst no gangrene supervenes, and that a part mortifies, whilst
the pain continues but little abated.
In compound fractures, dislocations, or severe bruises of the soft
parts, dark-coloured, prominent points occasionally appear, in
consequence of the effusion of bloody serum beneath the cuticle; in
these, however, the fluid is speedily absorbed, and the surface resumes
its natural aspect, the cuticle exfoliating and being reproduced;
and it is of consequence to know their real nature, for, if mistaken
for the gangrenous phlyctenæ, the inexperienced practitioner may be
alarmed, and, consequently, have recourse to very injudicious practice.
When the process of gangrene is checked, the skin immediately beyond
the mortified part becomes of a brighter hue, and is affected by a
more healthy species of inflammation, which ultimately terminates
in ulceration, with purulent discharge, and thereby forms what is
called the line of demarcation between the dead and the living parts;
the process, commencing in the integuments, gradually extends to the
deeply seated parts, so that the mortified portion is ultimately
attached to the living merely through the medium of bone or ligament.
Arteries appear more than any other texture to resist sloughing; and
those leading to a mortified part are found contracted and filled with
coagulated blood, so that the spontaneous separation of the sloughs,
and even incisions for their removal, made in sound parts, are followed
by little or no bleeding. This salutary change in the arteries may
be accounted for by supposing, that the inflammatory action which
leads to the separation of the dead substance from the living affects
the arteries at that point as well as the other structures, causing
adhesion of their internal surface, and obliteration of their cavities;
and the natural result is, that the calibre of the artery above
the obliterated point gradually diminishes in size, and the blood
coagulates up to the nearest collateral branch: but in consequence
of extension of the inflammatory action, the collateral branches may
also be obliterated to a considerable extent upwards, and thus the
contraction and coagulation in the larger trunk will also extend in
proportion. Besides, before the line of separation has commenced,
arteries cannot transmit their contents into the sphacelated part, any
more than into an extraneous body; so that the circulation of the blood
in them is as effectually obstructed as if a ligature were tightly
applied; in this way, also, the contraction and coagulation may be
accounted for.
Mortification is accompanied with great anxiety; coldness and
clamminess of the face and extremities; weak, irregular, and hurried
circulation; quick, short breathing; a cadaverous expression of
countenance; hiccup (which, however, often occurs in very slight
sloughing, or when no sloughing has taken place, in external or
internal inflammations, extravasations, &c.); by diarrhœa, vomiting,
and in hopeless cases, more especially of traumatic gangrene, by
delirium and coma; in fact, almost all the symptoms of severe
con48stitutional irritation are more or less fully developed. In some
cases, the patients are restless and unmanageable; in others, low
and dejected. The disease often proceeds with fearful rapidity to a
fatal termination, the patient becoming comatose from effusion within
the cranium; but in other instances, in which the vigour of the
constitution is greater, and the extent of mischief less, the system
bears up under the affection, and a separation is effected between
the dead and living parts. The danger is in general to be estimated
by a consideration of the size and importance of the part, and of
the age and constitution. The destructive consequences of sphacelus
arise both from a local and general cause; for the mere application of
putrid animal substance to a part still alive—the infiltration, for
instance, of dark serosity into the cellular tissue in the course of a
limb—causes a sort of inflammation attended with symptoms of diminished
power, and followed by constitutional disturbance; whilst the ultimate
extinction of life may be imputed to the effect produced on the system
by the part previously to its becoming sphacelated, and to the sympathy
between the system and the parts which are left in a weak and moribund
condition, and which seem endowed with a disposition to extend the
disease.
In the treatment of mortification, no one would think of using
any means, local or general, so long as the cause remained; and it
therefore must in the first place be removed, otherwise the mischief
may speedily become irreparable; thus, a stricture must be divided,
irritating fluids evacuated, foreign bodies extracted, &c.
In chronic gangrene the cause is constitutional, and the means
employed must be directed accordingly. In general, the power of the
constitution requires support, though, in cases where much fever is
present, it may often be necessary to keep the patient on low diet:
exhibit salines and mild purgatives in the first instance. The effects
of food should be attentively watched, and its quantity increased
or diminished accordingly. On the subsidence of the fever, and when
sphacelus has occurred, wine and animal food must be given abundantly.
Stimulants, strictly so called, are not admissible until the line of
separation be formed, and their exhibition must then be regulated by
the circumstances of the case. Opium and other anodynes are found
necessary during the progress of the disease, to allay irritation and
produce sleep; opium has been recommended on very high authority, that
of Mr. Pott, in mortification of the lower limbs. The bowels must be
attended to. Peruvian bark was at one time supposed to be a specific
in this disease, but experience has not born out the opinion; it
seldom agrees in substance, and the decoction, with or without the
compound tincture or sulphate of quina, will be found much more useful
in supporting the power and tone of the digestive organs. After the
line of separation has been formed, and not till then, the surgeon may
interfere, and assist nature in her work, dividing the exposed bones
or ligaments by which the dead parts still adhere to the living; or
he may perform amputation immediately below the line of demarcation.
Amputation in the sound parts cannot be recommended: for vitality is
impaired throughout the system, and more particularly near and above
the line of demarcation,49 where, though the structure seems entire, yet
the incisions are made in parts really diseased, and which would almost
certainly and speedily mortify. In fact, amputation above the line of
separation, in whatever way performed, is seldom if ever productive of
advantage in spontaneous gangrene.
In order to prevent the occurrence of gangrene after exposure to
intense cold, the frigid part must be cautiously and slowly restored
to its natural temperature; first by being either placed in very cold
water, or rubbed with snow; afterwards, by the degree of warmth in the
applications, and surrounding atmosphere, being gradually increased.
In acute gangrene, and in robust constitutions, when the affection
arises from over-action, abstraction of blood is had recourse to with
marked advantage. In some cases it may be employed, but with due
caution, even after sphacelus to a slight extent has occurred. In
gangrene, purging and bleeding must not be had recourse to but with the
greatest circumspection; for it ought always to be remembered, that
however strongly they may be indicated, the time is not far distant
when they will be totally inadmissible, and when the weakening effects
of depletion will prove highly prejudicial, particularly in cases where
the mischief is proceeding rapidly.
The loss of blood is frequently beneficial in sloughing phagedena, as
is exemplified on the occurrence of spontaneous hemorrhage in such
cases.
When a portion of a limb, throughout the greater part of its substance,
is so injured that it evidently cannot recover, it ought to be removed
instantly, and before the constitution has suffered.
When gangrene follows inflammatory action, this is first to be
moderated, and then the strength by all possible means supported.
When only a portion of the soft parts of a limb is destroyed by
mortification, and it is likely that the member may be saved and prove
useful to the patient, measures should be adopted to hasten separation
of the dead parts, and reparation of the breach in the living.
After the separation of sloughs has commenced, the attention of the
surgeon is chiefly to be directed towards the constitution; it must be
supported and strengthened by nourishing food, wine, and tonics, or by
stimulants, if necessary. Bark in substance, acids, and other supposed
antiseptics, are of but little use.
The local applications which have been employed are numerous; poultices
of all kinds, charcoal, carrot, and effervescing; various lotions to
the surrounding parts, spirituous applications, such as several of
the tinctures, liniment of turpentine, balsams, &c., with the view of
correcting the fetor. But it is evident that such applications to a
dead part can be productive of no effect; the only beneficial result
that can be expected from such means is removal of the fetid smell,
which can be effected, if need be, by sprinkling a solution of the
chloride of soda on the body-linens and bed-clothes. Scarifications are
sometimes used; when these are made merely into the sphacelated part,
they can be productive of good only by allowing the escape of matter;
when they extend more deeply, they are injurious.50 This practice,
however, as will be hereafter noticed, is adopted with the best effects
when mortification is threatened.7
When the sloughs become loose, they must be removed bit by bit with
scissors; and when the sphacelated part has separated entirely,
the healing of the breach is to be promoted by judicious dressing,
bandaging, and by proper position.
In mortification of an extremity, in consequence of injury, removal
of the part by incision in the sound substance was formerly as much
dreaded as in chronic cases before the separation had commenced; but
such fears have now subsided, and the practice of delay has been in a
great measure relinquished,—amputation being performed in the sound
part, at a considerable distance from the mortified or even gangrenous
tissues, and during the progress of the disease, occasionally with a
favourable result. If the surgeon defer the operation until a line of
separation have begun to form, he will soon discover the danger of
his delay; the constitution will, in the majority of cases, rapidly
sink under the malady before the progress of the disease is in any
measure checked, or any attempt is made to throw off the mortified
parts. Two cases which lately occurred in my hospital practice, are
here introduced from the “Lancet,” to show how different the progress
is, and how opposite the practice ought to be. Both the patients made
excellent and rapid recoveries.
“Sarah Arnold, æt. 75, was admitted on the 26th of January. She has
been a person of great mental and bodily activity, and has enjoyed
excellent health from her infancy, until her present illness, although
necessarily exposed, from the nature of her occupation, a gatherer and
hawker of watercresses, to all varieties of weather. 51About six weeks
ago, without being more than usually exposed to cold, she was seized
with severe rigors. Two days afterwards she began to complain of slight
pain, with clinching of the fingers, which at the same time became
discoloured at the tips, and were partially deprived of sensation.
This at first did not give rise to much uneasiness, and no treatment
was employed; and it was not until a week after the commencement of
the disease, when the discoloration had passed the wrist, and the hand
had become dry and shrivelled, and motion and sensation in it were
completely lost, that a medical man was called in. Both internal and
local remedies were then employed, but without in the least retarding
the progress of the disease, which in about a fortnight from her
seizure had extended a little way above the middle of the humerus,
beyond which it did not pass. At present there is a well-marked line of
separation between the living and the gangrenous parts, but there are
two livid spots beyond it, on the outer side of the arm; on the inner
side, where the disease has extended a little higher up than the outer,
suppuration has already commenced. The integuments in the immediate
neighbourhood of the diseased parts are slightly reddened and tumefied,
and it is there only that she complains of some slight pain. The hand
and wrist are dry and shrivelled, but above this the parts are soft
and flaccid. Below the line of demarcation, the extremity is of a dark
colour, resembling the skin of a negro, and completely deprived of the
power of motion and sensation; but she complains of a disagreeable
tingling, referred to the fingers. The discoloured parts are quite
cold, and the pulse cannot be felt, even in the axilla. Though she
complains much of debility, the system seems to be but little affected.
The appetite is very good; the skin is moderately warm; the pulse is
98, and of good strength; the tongue is moist and clean. She sleeps
little. ℞. Haust. c. Sol. M. Morph. gtt. xxv. M. Vini Rub.
℥iv. Water-dressing to the arm at the line of separation.

“27. She continues much the same as yesterday; slept little, bowels
moved twice; tongue clean and moist; appetite very good; pulse as
before; heat of skin natural; intellect clear; no expression of anxiety
in the countenance. ℞. Haust. Con. Vin. Full diet.
“28. The suppuration on the inner side of the arm is more copious, and
the discharge is more fetid. The livid spots on the outer side of the
arm have not extended, and there is some slight redness around them.
Pulse 104, of good strength; tongue clean and moist; heat of skin still
natural; appetite good; bowels moved once since the last52 report.
Continue. A little Sol. Chlor. Calcis to be added to the dressing.
“29. The dry and shrivelled state of the extremity has extended as high
as the middle of the forearm. The discharge is much the same as before
in quantity, but is more fetid. The separation between the gangrenous
and the sound parts, which had begun on the outer side of the arm when
she was admitted, is extending a little, both towards the inner and the
outer side. Pulse 90, of moderate strength; skin natural; tongue clean
and moist; bowels open; appetite excellent.
“30. Much the same as yesterday; sleeps a little better.
“31. The suppuration is more copious; the discharge extremely fetid.
The dead parts on the inner side of the humerus are gradually becoming
more detached. No change in the appearance of the livid spots beyond
the line of separation; pulse 102, of pretty good strength; bowels
continue regular, and the appetite is good. Cont. vinum et haust.
“Feb. 2. The separation of the gangrenous parts on the inner side
of the arm has advanced a little more since last referred to. The
livid spots have disappeared, with the exception of the largest,
where a small superficial slough has formed. The diseased parts were
removed to-day, the line of separation being fairly established, and
suppuration having taken place in a great part of its extent. The soft
parts were divided by means of a pair of scissors, cutting as near
to the living parts as could be done with safety; the bone was then
denuded as high up as possible, by passing a bistoury round it, and it
was then divided by the saw. There was no bleeding from the soft parts,
and only slight oozing from the bone, which was found to be alive where
it was divided. Cont. vinum et haust.
“3. Continues in much the same state as yesterday; pulse 104, of good
strength; tongue clean and moist; bowels moved once; skin natural;
appetite good; suppuration very free. Cont.
“5. Suppuration copious; a portion of the dead parts left have
separated, and left a healthy florid granulating surface. Continues
much the same.
“6. Discharge copious, and much less fetid; bowels regular; pulse 100,
of good strength; tongue clean; appetite good; wishes for more food. To
have an additional chop. Cont. alia.
“8. The greater part of the sloughs have separated, and have left a
healthy florid granulating surface; no change in the general symptoms.
Continue.
“9. The stump looks well, and the posterior part of the cut end of the
bone is covered by healthy granulations.
“In some notes of this case, kindly furnished me by the late Professor
Fergus of King’s College, who had an opportunity of watching the
appearances for some time before the admission of the patient here,
it is mentioned that the flow of blood in the veins was exceedingly
slow, and that hard knotty tumours could be felt in the parts before
they became sphacelated. These swellings all along preceded the
mortification. It is mentioned, besides, that the patient had a sort of
fit, but that it could not exactly be ascertained whether or not53 she
lost consciousness. Her left arm is said to have been motionless from
and after that time. There is considerable discrepancy in the accounts
of the mode of invasion, and of the duration of the disease, before the
line of separation became apparent. A period of six weeks is stated in
our case-book to have elapsed from the attack to the admission of the
patient into this hospital. It would appear, however, from the other
history, that not more than three weeks had passed over. The old lady
is not very distinct in her account; at one time she makes a statement
with great minuteness, and very soon after contradicts herself on
almost every point. When pressed on the subject, she states that she
got disgusted with her condition, became despondent and careless about
everything, and that her recollection is not now very good.”
“S.W., aged 16, was admitted March 12, under the care of Mr. LISTON.
She is a servant girl, of sanguine temperament and good constitution.
On Friday, March 9, she was cleaning the outside of a parlour window,
and stood on the sill. The window-sash, upon which she was depending
for support, being suddenly drawn down by a person inside, she was
precipitated into an area, a distance of fifteen feet. She was
immediately picked up, and conveyed to the hospital. The house-surgeon
detected a compound fracture of the ulna, and a fracture of the radius,
both fractures being a little above the wrist-joint of the right
arm. The fracture was adjusted, and the wound, which was inferiorly
to, and behind, the wrist, dressed in the usual manner. A dose of
house-medicine was administered; suitable directions were given in
case of the occurrence of pain or swelling; she was sent home, and
desired to remain quiet. The following morning (Saturday) she was
visited by the house-surgeon, who found her comfortable, but she had
passed a sleepless night. On Sunday morning the affected part became so
intolerably painful that she tore off the splints and bandages, which
one of the dressers of the hospital had a short time before readjusted;
in the evening she was in great pain, and the arm was much swollen.
“12. To-day (Monday) she was admitted into the hospital; water-dressing
was applied to the wound. The bandages were reapplied, and an anodyne
administered in the evening, with the effect of producing some rest.
“13. The pain and swelling were so great during the night that the
house-surgeon was called up to see her, and ordered the application of
fomentations; this morning she is much more comfortable.
“14. On removing the whole of the apparatus this morning early,
mortification was found to have taken place in the limb; at the time
of Mr. Liston’s visit in the middle of the day, the limb was very
swollen, the fingers were of a black colour, the forearm livid, there
were vesications near the elbow with fetid discharge. There was a good
deal of fever with slight delirium; pulse irregular, quick. Mr. Liston
considered the only chance the patient had was the immediate amputation
of the limb at the shoulder. The patient’s consent having been readily
obtained, Mr. Liston proceeded at once to the
“Operation.—He first introduced a long double-pointed knife under
the acromion, and brought the point out at the lower and pos54terior
border of the axilla, by this means the joint was laid open; the flap
thus formed of a portion of the deltoid was raised, and the head of the
bone separated from its attachments. The other flap was formed from the
integuments and muscles in front. The axillary, and one other vessel,
required ligature. The edges of the wound were drawn together by three
points of suture, and cold water-dressing applied. One grain of muriate
of morphia was given. In the evening, several strips of isinglass
plaster were applied, and the edges approximated. The delirium ceased
after a short but refreshing sleep.
“15. Passed a good night; has had little pain; feels very comfortable
this morning; she is cheerful, and has little fever; pulse 86, regular.
The wound looks healthy.
“April 2. Since the above date, the patient has been gradually
improving in her health and strength, and she is now able to walk about
the ward.”
In gangrene occurring after exposure to cold, amputation should not be
had recourse to till after the line of separation has formed; and in
this case the constitutional symptoms are much less urgent, and the
object of the operation might be frustrated by its being performed in
parts, which would speedily become sphacelated. The amputation may be
performed either at the line of separation by cutting the ligaments
or bones, as was done in the case from which the accompanying sketch
was taken, and when the line of separation is well declared; or,
if by these means a good covering is not likely to be had for the
exposed surface, the incisions may, in these cases, be with safety and
propriety made in the living tissues, at the most convenient point.
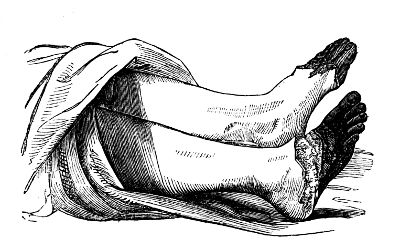
In gangrene arising from obstruction or injury of blood vessels, in
healthy constitutions, amputation must be performed early—for thus the
chance of ultimate success is increased, while the danger of delay is
the same as in cases of gangrene caused by severe injury.
55
OF ERYSIPELAS.
Erysipelas is an inflammation of the external surface, accompanied
with peculiar symptoms and appearances, the morbid action being
modified by the texture in which it occurs. According to the various
circumstances attending the disease, it has been divided into several
species: phlegmonous, bilious, œdematous, gangrenous, acute, malignant,
&c. The term Erythema is applied to cases of rash or efflorescence,
unaccompanied with fever, swelling, or vesication.
Inflammation of the skin only, is marked by bright redness, not
circumscribed, and disappearing when pressed. By pressure, the
bloodvessels are emptied for a time, the part sinks and becomes pale;
but, on removing the pressure, it soon regains its former colour and
relative situation; when these circumstances concur, the part is said
to pit. There is no tension,—the pain is not throbbing, but of a
burning or itching kind, and there is often a degree of œdematous
swelling. Swelling does not occur to any great extent, however, during
the existence of the inflammation in the skin and rete mucosum;
but the parts sometimes become much swollen after subsidence of
the inflammatory action, the vessels having relieved themselves by
effusion of serum; and afterwards the œdematous surface often assumes
a yellowish hue. In some cases, the serous effusion is from the
first, more extensive than in others, and hence the term œdematous
erysipelas, or inflammatory œdema. Upon the decline of inflammation, a
serous fluid is often effused also in great quantity under the cuticle,
giving rise to vesications, resembling the blisters produced by the
application of boiling water to the skin; and from this circumstance,
erysipelas has been classed amongst cutaneous affections in the order
bullæ. The erysipelatous redness does not terminate abruptly, and is
not defined by a distinct boundary, as some have asserted, but becomes
gradually lost in the surrounding parts. It frequently involves the
contiguous parts one after another, and extends with great rapidity.
It often leaves one part suddenly, and attacks another, either in the
neighbourhood, or situated at a considerable distance; in other words,
metastasis takes place. The disease takes on this erratic character
without our being able to assign any good reason for it; and this form
of the disease is frequently attended by symptoms of typhoid fever.
When it disappears suddenly, or is repelled by cold applications,
affections of the internal organs sometimes supervene, as of the
bowels, lungs, or brain; the diseased action leaving the external
surface, and attacking the deeply-seated organs; thus, in a case of
erysipelas of the ankle and foot, the external symptoms disappeared
suddenly, and an affection of the lungs supervened, under which the
patient sunk; and in erysipelas of the face and scalp, the sudden
disappearance of the redness is frequently followed by delirium and
coma. Again, in acute disease of an internal part, the symptoms are
much meliorated, and often entirely removed, by inflammation of the
skin being induced artificially, or occurring spontaneously.
56
The integuments of the face and head are frequently attacked by
erysipelas, in consequence of wounds and bruises of the face or scalp,
even though very slight, and it often takes place here spontaneously,
as in other parts of the body.
Erysipelas commonly arises from constitutional derangement, as is
shown by the symptoms which precede it, and also by the efficacy
of internal remedies in checking its progress; in such instances,
external applications, unaccompanied with constitutional treatment,
produce little or no effect. It is often produced around a wound by
the employment of improper dressing, rancid ointments, or irritating
plasters, by a too free use of the part, or by the friction and
irritation of the patient’s clothes. It occurs most readily in those
who live freely, indulging in the imprudent use of spirituous liquors,
and whose constitutional powers are thereby considerably weakened. It
is also said to be sometimes caused by violent passions, as anger or
grief; and by exposure to cold, or to heat,—the former acting only
as a remote, the latter as an immediate cause. As an example of its
occurring in consequence of heat, it is a common remark, that cooks,
who are necessarily much exposed to the fire, are frequently the
subjects of erysipelas of the face; but in the majority of such cases,
there may be other causes in operation,—the abuse of ardent spirits,
and habitual overcharging of the system with stimulating food. It is
more commonly met with in summer than in winter. And in certain states
of the atmosphere, even in healthy situations, a degree of erysipelas
is apt to occur after wounds by operation or accident.
It is often periodical, especially in females who have ceased to
menstruate, always recurring at regular intervals; it attacks parts of
the body, most generally the face, and in some cases monthly, in some
once in the year, and in others once every two years. It sometimes
appears to occur as a natural means of relief from impending affections
of more serious nature, as of the system or of internal organs. Those
who have once been afflicted with the disease become more liable to its
attacks.
Erysipelas is generally preceded and accompanied with more or less
disturbance of the digestive organs. In Bilious Erysipelas, the
portion of skin affected is said to present a more yellow colour than
in the phlegmonous, the derangement of the digestive organs is greater,
and hence the origin of the distinctive term; fits of shivering occur,
the patient complains of a bitter taste in his mouth, and the tongue is
furred and of a brown colour.
In the Phlegmonous, in which other textures than the skin are often
affected, viz., the subcutaneous and intermuscular cellular tissue and
the fasciæ, the pain is more intense, and of a throbbing kind; the
swelling is hard, more deeply seated, and more extensive; there is
considerable tension; and the redness is of a darker hue. Nausea and a
bitter taste in the mouth do not precede the erysipelatous appearance,
but the skin and tongue are dry, and there is great thirst. When the
disease begins to subside, then the foul tongue supervenes, with the
bitter taste and nausea.
Erysipelas, of a contagious and violent character, frequently occurs,
and is apt to spread extensively, in badly aired situations, where
a57 number of patients with sores are crowded together, without due
attention being paid to cleanliness and proper dressing.
Hospital Erysipelas, as this species is termed, is nearly allied to
that dreadful disease, Hospital Gangrene, and the two affections are
often blended. It comes on after operations, or in patients who have
sustained an external injury by accident. In unhealthy hospitals it
not unfrequently appears in previously sound parts, and without any
assignable cause; and, from its following the slightest wound, recourse
cannot be had with safety even to venesection, cupping or leeching.
It is a dreadful scourge in many hospitals, more especially during
particular seasons of the year—during hot, damp weather, and in spring
and autumn, attacking the patients indiscriminately.
Of late years Erysipelas appeared in the Royal Infirmary of Edinburgh,
during the wet and changeable summers which prevailed; some of the
cases were very severe, and a few terminated fatally. It was very
satisfactory, however, to observe that it did not spread as it used
to do formerly, that patients occupying the beds immediately around
those affected, though afflicted with sores and in indifferent health,
remained exempt from the disease; and that many of the most severe
cases did not originate in the house, but were brought from the crowded
and unhealthy parts of the city. The same may be said of the disease as
it has shown itself in the North London Hospital since it was opened
for the reception of patients up to the present time.
Hospital Erysipelas is for the most part preceded by violent
constitutional symptoms, derangement of the chylopoietic viscera,
shivering, brown tongue, and a bitter taste in the mouth; if there
is a sore on the body, it assumes a sloughy aspect; the surrounding
skin becomes of a dark red colour, and there is a feeling of tension,
accompanied with a burning pain. The erysipelas extends rapidly, and
generally terminates in suppuration and sloughing of the cellular
substance, or, if inertly treated, in immediate gangrene of the parts.
The concomitant fever is generally low, and though, in the first
instance, the circulation may be vigorous, symptoms of debility will
speedily appear. It will be more fully dwelt upon, along with Hospital
Gangrene.
In all cases of erysipelas there is more or less concomitant
fever, modified by the extent of the local affection—by the age
of the patient—by the previous habits and state of health—by the
constitution—and by other circumstances. The pulse is accelerated, and
is either of a sthenic or asthenic character, according to the state
of the system and type of the prevailing fever. There is headache,
languor, thirst, restlessness, and even delirium, especially when the
face or scalp is the seat of the disease.
Erysipelas may terminate in resolution. If this takes place in the
first stage of the disease, the redness gradually declines, along with
the swelling, the cuticle exfoliates, and the part regains its usual
appearance, the skin remaining loose and shrivelled. If it occurs after
vesications have formed, the effused fluid is absorbed, a scab forms,
and desquamates along with portions of the cuticle.
It may terminate in suppuration, when the inflammation has ex58tended
to the cellular substance. This termination is most frequent when
the disease is situated in an extremity, seldom when in the face,
though small purulent collections occasionally form in the eyelids.
Circumscribed collections of pus often present themselves after the
disappearance of the erysipelatous inflammation; but the purulent
matter is generally diffused through the filamentous tissue, and is of
a thin, unhealthy appearance, and mixed with sloughs of the cellular
substance. By the infiltration of matter, the integuments, fasciæ, and
muscles are extensively separated from each other, in consequence of
which the parts frequently die, their nutritive supply being cut off.
Acrid sanious matter is often infiltrated extensively into the
subcutaneous cellular tissue round a wound or sore. The superimposed
integuments are of a dark brown colour, and the part is boggy.
Sloughing of the cellular membrane here takes place in consequence
of the infiltration, and not from inflammatory action having
been established. The affection has been termed Diffuse Cellular
Inflammation, but a more proper appellation is Diffuse Cellular
Infiltration; the cellular tissue, even where treatment is adopted at
an early period, can scarcely be prevented from perishing.
Erysipelas, if properly treated from its commencement, will seldom
terminate in gangrene of the skin. This termination is occasionally
observed, however, in patients whose constitutions have been extremely
debilitated.
In mild cases of erysipelas, attention to the state of the bowels, and
regulation of diet, will often be sufficient to remove the disease.
When there is much disorder of the digestive organs, and particularly
of the biliary secretions, emetics may be given at the commencement;
these are productive of but little good in the more advanced stage, and
their place is advantageously supplied by nauseating doses of antimony,
combined or not with purgatives. One-eighth of a grain of tartarised
antimony may be given in solution every hour, with or without a
due quantity of the tart. potassæ and sodæ, or Rochelle salt. The
hydrargyrum cum creta is often given with great benefit when the tongue
is dry and covered with a brown crust: it may be combined sometimes
advantageously with the compound powder of ipecacuanha. With the same
view calomel with antimonial powder may be exhibited. The exhibition
of saline purges is attended with great good in some severe cases.
Such medicines tend to subdue any arterial excitement that may exist,
evacuate the bowels, promote perspiration, remove the superabundant
bilious matter, and serve to restore the healthy functions of the
liver. In severe cases, more especially of phlegmonous erysipelas,
in which there is acceleration of the pulse, and a degree of febrile
excitement, general bleeding may be had recourse to; but it must be
employed with caution, for the symptoms of increased vascular action
may arise from constitutional irritation, and not be meliorated by the
depletion. The practice is superseded by the timeous and free local
bleeding from incisions, as will be noticed by and by. The exhibition
of the extract of aconite in this and other inflammatory affections, is
often followed by great abatement of vascular excitement, so that the
necessity for abstrac59tion of blood is done away with. The medicine may
be given in doses of half a grain in substance, or dissolved in pure
water, and repeated every third or fourth hour. The sensible effect is
relaxation of the surface, and frequently profuse perspiration; the
arterial pulsations are diminished in frequency and force. The extract
of belladonna, in doses of one-sixteenth of a grain, may then be
substituted with great advantage, and often with the most extraordinary
effect upon the disease. In very many cases, the strength is from the
first to be supported by all possible means, by nourishing diet, by the
exhibition of wine, quinine, and other tonics; more particularly in old
people—in constitutions debilitated by disease—in unhealthy situations,
and when the fever is of a typhoid kind. Bleeding by leeches is not
admissible, for the leech-bites prove a source of irritation, and are
liable to suppurate; erysipelas has often been produced by leeching.
In erythema, the mere outer surface of the skin only being slightly
affected, and not to any very great extent, advantage sometimes
results from the application of nitrate of silver. A strong solution
may be pencilled upon the part, or, after being wetted, the affected
surface may be gently rubbed over with the solid caustic. The pain and
uneasy sensations in the part being thereby diminished or removed, and
extension of the disease seeming to be arrested. Discoloration caused
by such practice is of little consequence, as desquamation must follow.
It is questionable how far it may be safe to apply lunar caustic to any
extensively inflamed surface, more especially of the head and face,
lest metastasis should occur. The inflammatory action in the skin is
subdued by the application, whilst it may advance, in the cellular
tissue, to suppuration and sloughing, if other means are not adopted;
and from the hard and blackened state of the cuticle, the condition
of the subjacent parts is not readily perceived. The remedy is only
applicable to erythema, and most advantageously as a means of bounding
it. The line should be drawn at some distance from the affected
tissues; and if so, it is seldom that the disease oversteps it.
Local abstraction of blood, by puncture or incision, proves exceedingly
beneficial in cases of erysipelas, whatever its degree. It must be
borne in mind by the practitioner, when called to treat the disease,
that the state of parts is very various, and this may depend upon
the original nature of the disease, upon its site or duration. The
surface of the skin only may be affected—that and the subjacent
cellular tissue may be involved, gorged with serous, lymphatic, or
purulent infiltration—there may exist great tension of the parts, with
a sloughy state of the cellular tissue, established in addition to
suppuration—and again, there may be infiltration of the subfascial and
intermuscular tissues, leading ultimately to exposure and exfoliation
of bones or disease of articulations.
From inattention to these circumstances, the treatment being often
directed to the name of the disease, great discrepancy of opinion, as
to the most proper local management, has arisen; there has accordingly
been a controversy as to whether the blood should be drawn from mere
punctures from limited incisions, or from long gashes extending from
one joint to another.
In cases not very severe or extensive, when the skin only is af60fected,
the constitutional treatment already mentioned is first to be employed,
and then the affected part must be freely punctured with a fine lancet,
at numerous points, as recommended by Sir R. Dobson. These punctures
should reach the vascular layer, but not go deeper: the serous
effusion, if there be any, is thereby evacuated—the over-distended
vessels are relieved of a considerable portion of their contents—and
the œdematous swelling, with the formation of phlyctenæ, is prevented.
The part is afterwards to be fomented for half an hour, or an hour,
with bags containing chamomile flowers or hops; the fomentation,
repeated at intervals, proves highly grateful to the feelings of the
patient, allays any irritation which the making of the punctures may
have produced, and keeps the skin perspirable. Under this treatment,
every vestige of erysipelas will generally disappear in the course of
a few days. In more severe cases, especially in the extremities, the
parts must be freely incised. The incisions ought to extend through
the integuments and cellular substance, and their length and number
must be proportioned to the extent and severity of the affection. One
or two pretty free incisions, if made in the proper place, where the
greatest degree of boggishness, marking the disorganised state of the
tissues, is discovered, will generally suffice—the vast good and the
relief afforded depends partly upon the abatement of the tension,
in consequence of the evacuation of the effused fluids—upon the
unloading of the over-distended bloodvessels of the part, and upon the
acceleration of the suppurative process, which is often critical. The
constitution is, probably, relieved by the suppuration of the wounds,
and the consequent drain of the offending particles.
Some surgeons have disapproved of long incisions, alleging that they
are tedious in healing, and prefer making numerous small ones; but
it is difficult to understand how the cure should be more tedious in
the one case than in the other, when the actual extent of divided
surface is the same. According to my experience, several free incisions
are made with less pain than a number of trifling scratches, and
heal as soon, whilst by the former the purpose of the practitioner
is much better fulfilled: the same good effects result from them as
from punctures in the more slight cases, if they are made at the
commencement of the disease; and if the affection is in its advanced
stage, the effused fluid, and the sloughs, are discharged, and the
infiltration of pus, and destruction of parts in consequence of the
matter being confined, are prevented by its being allowed a free exit
as soon as it is formed. Incisions then are made both in the early
stage of the disease, and after effusion has occurred: in the former
case, they are justifiable, because they arrest its progress; in
the latter, they are absolutely necessary, to prevent its injurious
effects. The parts are to be fomented, and afterwards covered with
a common poultice, containing no oil or grease, or with soft lint
saturated with tepid water, and covered with oiled silk, to prevent
evaporation.
When the erysipelas has gone off, the incisions are treated as common
wounds, by dressing and bandage. After punctures, or incisions, more
or less blood is allowed to flow, according to circumstances. It often
escapes from the vessels of the part in great profusion; this, in many
cases, may be prejudicial or excessively dan61gerous. In the extremities
the flow can readily be arrested by elevation of the part, or by
pressure, for a short period. In erysipelas of the face, punctures
are preferable to incisions, as by the employment of the former the
countenance is no way disfigured; if, however, in erysipelas of the
scalp, the integuments become swollen, and present a puffy feeling,
whilst at the same time cerebral symptoms supervene, free incision or
incisions, through the whole thickness of the covering, and in the
direction of the fibres, must be made. If erysipelas be thus actively
treated, it may be safely affirmed that the disease will not often,
unless accompanied with symptoms of putrid fever, terminate fatally;
if these means are employed early, the constitutional disturbance will
be modified or prevented, and no derangement of the cerebral functions
will ensue.
Powders, such as flour, chalk, and camphor, &c., have been applied
to the erysipelatous surface, but are of little use, and, by their
irritation, frequently prove injurious on the bursting of the vesicles.
They are applied, according to some, with the view of cooling the
surface, and after all the part may be seen enveloped in folds of
flannel. Cold application, such as the spirituous and evaporating
lotions, containing vinegar and spirits, liquor acet. ammoniæ,
Goulard’s extract, &c., may, in many cases, afford temporary relief,
but their use is fraught with the utmost danger; for their direct
tendency is to produce metastasis, and if that be to an internal
organ of importance, the result is too generally fatal. Or if the
erysipelas, on leaving the part originally affected, attack another
also superficial, the local treatment has to be commenced anew. If
these lotions are to be employed at all in this disease, they must be
made tepid.
In case of the translation of erysipelas to any important part,
blisters may be applied to the surface which it has left, or to any
other in the neighbourhood, with the view of recalling the disease to
its original and less dangerous situation:8 the actual cautery has
even 62been recommended. In the great majority of cases, however, such
means are unavailing.
In Hospital Erysipelas, purging cannot be carried to any great extent
with safety, and general bleeding is seldom if ever admissible unless
the patients previously robust and in good health, in whom the disease
has occurred in consequence of their being conveyed to a distance and
during hot weather, after an accident or wound, and in whom the fever
is of a violent inflammatory nature. In civil hospitals, the patients
are generally in a weak state before the accession of this disease; and
in their case, after the stomach and bowels are regulated, stimulants
are more requisite. Great attention must be paid to cleanliness, the
sores must be frequently dressed, and the same sponges must not be
used for different individuals: in order to prevent contamination by
the promiscuous use of sponges, it is better to clean the parts around
sores with lint or tow, and to destroy immediately such dressings as
have been used. The apartments must be well ventilated, and those who
are affected with the disease should be separated from the rest of the
patients. The local applications will vary according to the particular
circumstances of each case. Strong escharotics may be required to clean
the surface of the sores, and put a stop to the sloughing. The nitric
acid will answer the purpose well, and is less objectionable than some
remedies that have been used; such as the arsenical solution, or the
red hot iron.
OF FURUNCULUS AND ANTHRAX.
Furunculi, or Boils, most generally occur in unhealthy constitutions,
particularly in those individuals who are habitually addicted to the
use of ardent liquors: they seem to arise from, at least they follow,
disorder of the digestive organs. Their seat is in the skin and
subjacent cellular tissue.
They generally occur in those parts which are possessed of little
vitality, as in the back, buttocks, shoulders, the posterior part of
the neck, &c. They are seldom single, are often numerous, and vary in
size from a pea to a pigeon’s egg.
A boil is of a conical form, elevated above the surface of the body;
its base is hard and firm, whilst its apex is acute, soft, of a white
colour, and exceedingly painful; the pain experienced in the tumour
63is severe and burning. From the comparatively trifling nature of the
affection, the assistance of the surgeon is seldom required, and hence
the apex of the tumour generally gives way either spontaneously, or
in consequence of being scratched by the patient, or rubbed by the
clothes; the purulent matter, which is generally small in quantity, and
mixed with blood, is thus discharged. This, however, is attended with
but little relief in bad forms of the affection; for at the lower part
of the cone is situated a considerable quantity of mortified cellular
tissue, which must be evacuated before the cavity can heal.
In this unhealthy species of inflammation, resolution cannot be
expected; on the contrary, suppuration is the natural termination of
the disease, and must be hastened by poultices and fomentations. A
simple or crucial opening, according to circumstances, must afterwards
be made in the apex of the tumour, so that the sloughs of the cellular
tissue may be permitted to escape readily. In the advanced stage, the
sloughs are the irritating cause by which the inflammatory action is
prolonged, and on their removal the cavity contracts speedily.
If there is much derangement of the digestive organ, it may frequently
be found necessary to administer an emetic. If the bowels are slow
and the liver torpid, calomel and antimony are highly useful, or
other mercurial preparations may be given, in combination with
active purgatives; if the state of the secretions is more natural,
these medicines may be administered in alterative doses. The mineral
acids are often usefully administered, with the view of removing the
disposition to the formation of boils. Twenty minims of the aromatic
sulphuric acid may be given twice or thrice a day in any convenient
vehicle. Anodynes are occasionally required.
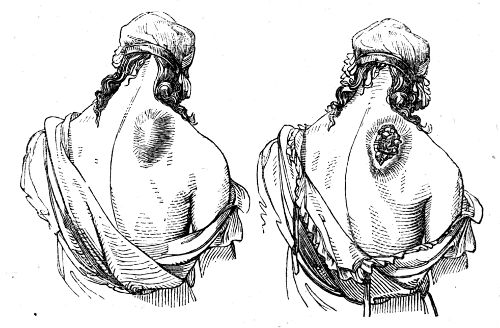
Anthrax or Carbuncle maybe considered as a severe form of boils.
It occurs in the plague, and is a characteristic symptom. It appears
in the same parts, and apparently from the same causes, as the boil.
The tumour is of a more flattened form, slightly elevated above the64
surface, and frequently of great extent; the base is deeply-seated,
hard, and unyielding. The integuments are at first of a bright colour,
but afterwards assume a dark-red or reddish-brown hue. The pain is
violent and burning. The process of suppuration is very tedious, and
the matter that is formed is small in quantity. If the tumour is not
interfered with, ulceration occurs in its surface, producing various
apertures, through which the matter is evacuated, the discharge is thin
and unhealthy, excoriating the neighbouring surface; and the mortified
cellular tissue, remaining at the base of the swelling, keeps up the
irritation. The extent of a carbuncle is frequently great, both as to
width and depth; on the back, or buttocks, it not unfrequently attains
an immense size. In one instance, the whole posterior part of the neck
was involved; the cellular tissue, muscles, and tendons, sloughed;
and the vertebræ were ultimately exposed. In another case, the whole
occiput, the posterior and lateral parts of the neck, and the space
betwixt the shoulders, exhibited one continuous mass of carbuncle. By
making free incisions, procuring early separation of the sloughing
parts, and supporting the strength of their constitutions, both
patients recovered, though considerably advanced in life.
It seldom occurs in the face or head, and when it does, it generally
proves fatal. In a male patient in the Edinburgh Royal Infirmary,
aged forty-eight, a carbuncle of the size of a very large orange
was situated in the centre of the forehead; by active local and
constitutional treatment, he soon got well.
The affection is sometimes attended with typhoid symptoms, rigors,
profuse perspiration, nausea, vomiting, disordered bowels, loss of
appetite, anxiety, restlessness, difficult respiration, palpitations,
faintings, pale-white tongue, low pulse, pale or turbid urine,
headache, giddiness, drowsiness, and, in severe cases, with delirium.
In old or exhausted patients, the prognosis is unfavourable.
An early and free incision must be made into the tumour; if the
swelling is large or extensive, the preferable form of incision is
the crucial; the ill-formed matter is thus evacuated, the slough
exposed, and more readily allowed to escape. If the mortification
of the cellular tissue be extensive, and the sloughs prove firmly
adherent, the free employment of the caustic potass will be found of
much service, the half-dead cellular substance being thereby completely
destroyed, and the surrounding parts stimulated to a new and superior
degree of action, necessary for the removal of the mortified parts, and
reparation of the breach of surface. Poultices and fomentations may
afterwards be employed, followed by the warm-water dressing, medicated
or not. The stomach and bowels must be put into proper order by the
exhibition of suitable medicines; and the vis vitæ may be still farther
supported by the administration of tonics and stimulants. If, after the
separation of the sloughs, the exposed surface shall assume an indolent
or debilitated action, stimulating dressings, such as turpentine
liniment, or elemi ointment may be employed.
Such practice will be found sufficient to procure a speedy and
favourable termination of the disease, in this country, where we have
not to combat any of those malignant diseases with which carbuncle is
accompanied in other climates.
65
OF INFLAMMATION OF THE MUCOUS MEMBRANES.
Mucous Membranes and the skin are analogous in structure, somewhat
similar in function, and sympathise closely with each other in
health and in disease. Both are endowed with that peculiar degree of
sensibility which enables them to bear with impunity the impressions
of foreign bodies; and both are protected from the influence of these
bodies by an inorganic covering; the cutis and rete mucosum by the
epidermis; the corium of mucous membranes by a laminated epithelium.
They are the seat of all excretions, and by them all substances are
introduced from without into the system. The capillary portion of
the vascular system appears to have somewhat the same arrangement
in both; the distribution of blood to the mucous membranes being,
however, more copious. At the commencement and extremity of the
alimentary canal, they insensibly pass into each other by means of
an intermediate structure, of which the prolabium may serve as an
example. In particular circumstances, they change into each other,
both in appearance and in function. Thus, in prolapsus of the gut or
of the vagina, the discharge from the protruded mucous surface after
a time subsides, the rugæ disappears, the membrane becomes thickened
and indurated, and gradually assumes an appearance exactly resembling
that of the skin. In natural paraphymosis, the delicate membrane
which, in the healthy state of parts, lines the internal surface of
the prepuce, becomes converted into a cuticular covering. In neglected
and long-continued excoriation of the nates, the raw surface, which
was at first tender and irritable, and discharged a serous fluid,
becomes villous, less sensible, and discharges a fluid similar to a
mucous secretion. In sinuses also of long duration, the secreting
surface becomes changed, so as to resemble a mucous membrane, and the
discharge, from being purulent or gleety, becomes mucous, or at least
resembles a mucous fluid,
A mucous surface, when inflamed, has for a short time, perhaps,
at first, its functions suspended; it then furnishes a secretion,
increased in quantity, and but little changed in appearance from the
healthy fluid; afterwards the discharge resembles purulent matter, and
is termed muco-purulent. When, however, the inflammation is violent,
the discharge becomes bloody, or is altogether suppressed, and the
membrane is thickened. Inflammation of a mucous membrane is very
apt to spread with great rapidity, in this respect resembling the
corresponding affection of the skin. It is attended with a sense
of itching, and a burning pain. This pain is much increased by the
muscles surrounding the parts being thrown into action, as in expelling
their contents, more especially if these be of an acrid quality.
The membrane is thickened, and of a spongy appearance; its surface
is red, and sometimes covered with flakes of lymph; occasionally it
is much softened, and coated with a viscid adherent mucus; and it
would appear, in many instances, that, in acute inflammation, the
membrane is generally softened, whilst it becomes indurated from
chronic inflammatory action. When the inflammation is violent, and66
consequently rapid, considerable quantities of lymph are effused either
on the surface of the membrane, or into the submucous tissue: and the
lymph subsequently becoming organised, the membrane is much thickened,
and a contraction is the consequence. The functions of a part lined
with mucous membrane are more or less deranged, in consequence of the
vitiation of the secreted fluid.
In inflammation of this tissue, metastasis is also apt to occur, from
one part of the membrane to another, and from the membrane to the
external surface. Cynanche, for instance, often follows upon erysipelas
of the face and scalp, and vice versâ.
The passages, the internal surfaces of which are invested by a mucous
membrane, are those subservient to respiration, nutrition, generation,
and the urinary secretions; in other words, the mucous surfaces are the
Pneumogastric and the Genito-urinary. Their particular diseases will be
treated of hereafter.
OF INFLAMMATION OF THE SEROUS MEMBRANES.
On such an extensive subject it is unnecessary to enter fully; not that
the inquiry is uninteresting, or that a knowledge of the diseases of
the internal cavities, and the mode of treating them, is not required
of the surgical practitioner before he can enter into practice, with
safety to his patients and comfort and satisfaction to himself, but
we have a very important class of diseases to bring under review in
a limited space, and it is properly the province of others to treat
of internal disorders, and to describe the best mode of alleviating
or curing them. It is, however, the duty of the surgeon to treat
the inflammatory affections of some of the serous membranes, and
the consequences of inflammatory action in most of them; and it is
therefore highly necessary that he understand the symptoms, progress,
and consequences of such actions. The affections of the serous
membranes are principally under the management of the physician; but
they not unfrequently follow wounds and surgical operations, and the
diseases of several of them are purely surgical. Inflammation of a
serous membrane is attended with heat and pain, aggravated by motion
of the parts and by pressure; the natural secretion is increased
in quantity, the process of exhalation being incited, and that of
absorption weakened; the serous fluid accumulates. The secretion
becomes altered in quality, and assumes a milky appearance; lymph
is effused, generally mixed with purulent matter, and floats in the
fluid, or adheres to the surface of the membrane, which is rough and
flocculent. The adherent lymph becomes organised, being penetrated
by numerous bloodvessels; and thus the original membrane is, in many
instances, much thickened, chiefly from the addition of new matter,
though also from enlargement of its bloodvessels and opening out
of the primitive tissues, principally the subserous cellular. When
inflamed serous surfaces, which have been altered, both in texture and
function, in consequence of inflammatory action, remain for a short
time in contact with each other, lymph is effused and penetrated by
bloodvessels from each surface; thus the new deposit is organised, and
forms a medium of connection. By this process the parts are inti67mately
united to each other, and consolidated into one mass; or are merely
approximated, and joined, at one or more points, by portions of lymph,
in some cases thin and narrow, in others extensive and of considerable
thickness; the adhering bands either extend in a straight direction,
from one surface to another, or interlace, forming a sort of network.
After adhesions of various kinds have been formed, they are often
lengthened and attenuated in consequence of the motion of the parts,
as is particularly the case with adhesions between the pleura costalis
and pulmonalis. When they have been of considerable duration, they
often resemble the original membrane from which they were deposited,
becoming thin and transparent, smooth on their external surface, and
furnishing a serous secretion. Not unfrequently, inflammatory action
in this tissue terminates in suppuration; and the pus, secreted by
the membrane, accumulates in the most dependent part of the cavity.
By collections of matter, whether serous, sero-purulent, or purulent,
within a serous cavity, the functions of the contained viscera are
deranged, much impeded, and in many instances morbid actions are
excited in them. The inflammation, whether it terminates in resolution,
or proceeds to serous effusion, adhesion, or purulent secretion,
is attended with constitutional disturbance, and the symptoms are
proportioned to the original intensity of the action, and the extent
and kind of its termination. The effusion of lymph, and consequent
adhesion, is, however, in many circumstances, a highly salutary
process, as in wounds and injuries of the hollow viscera: effusion of
their contents being thereby prevented, and the patient being saved
from the danger attending violent inflammation of those cavities and
their coverings, caused by the escape of a greater or less quantity
of irritating extraneous matter. Purulent collections also, in the
solid internal viscera, are thus allowed to discharge themselves
externally. The nature, symptoms, and consequences of inflammation of
serous membrane, will be more fully considered under the diseases of
particular parts.
OF INFLAMMATION OF TISSUES COMPOSING THE ARTICULATIONS.
Inflammation of the synovial surface occurs in consequence of wounds,
bruises, or sprains, and often from exposure to cold; from the latter
cause, the knee and elbow joints most frequently suffer, as they are
generally more exposed to its influence, and not so well covered with
muscular substance as the others. Constitutional diseases, such as
certain fevers, are followed sometimes by effusion of serous fluid into
joints. Purulent matter is also deposited in joints during certain
forms of suppurative fever; and this is attended by rapid change of
structure.
There is heat, throbbing, pain, and swelling of the part, sometimes
redness of the surface, and great constitutional disturbance; the
symptoms and appearances, however, vary much, according to the extent
of the joint which is involved. When part of the capsule is affected,
the inflammation spreads rapidly over all the surface; the68 synovial
membranes resembling the serous in this respect, as well as in healthy
structure and function. Like the serous, too, they are shut sacs, are
smooth on their surface, and furnish a secretion, the synovial, for
facilitating the motion between opposing surfaces; it is, however,
somewhat more glairy than the serous. Neither, in their healthy
state, are possessed of much sensibility, nor are ligaments, tendons,
tendinous sheaths, and bursæ, which two latter textures resemble in
every respect the synovial; when inflamed, they become most exquisitely
sensible. The incited action of the bloodvessels is followed by
increased discharge, which is less glairy and albuminous, partaking
more of the serous character. When the incited action soon terminates,
and the activity of the absorbents is diminished, the fluid accumulates
within the joint, producing Hydrops Articuli. This accumulation of
fluid in joints may take place without being preceded by any apparent
inflammation, and may remain a long time without any visible change
of structure in the membrane. The knee is more frequently the seat of
dropsy than any other joint.
When the action is more violent, and is not actively opposed, lymph
is effused on the inner surface of the membrane, or is deposited
amongst the ligamentous and cellular tissues external to the joint,
in consequence of which, the membrane and external ligaments become
thickened, and of an almost cartilaginous consistence. Serum is
effused into the more superficial cellular tissue, filling up the
hollows around the joint, concealing the protuberances of the bones,
and producing a globular swelling. The articulating surfaces become
ulcerated, and matter forms within the capsular ligament; or the
pus is deposited exteriorly to the joint, and gradually approaches
the surface. But although ulceration is so prone to occur in the
cartilages, the synovial membranes do not readily take on this action,
unless from the progress of matter, formed within the joint, towards
the surface. The synovial lining of the bursæ and sheaths of the
tendons are extremely indisposed to ulcerate; and it may be remarked,
that, while suppuration without ulceration is common in the synovial
membranes, the cartilages, on the other hand, afford frequent instances
of ulceration without suppuration, of which more particular mention
will be made in the sequel. The cartilage is occasionally swelled and
softened where the disease has long existed.
Along with ulceration of the cartilage, a portion of it may become
dead, or either state may occur separately; and in many cases, the
substance of the bone also becomes affected, of which two classes of
cases may occur, viz., great inflammation on the articular surface of
the bone, with separation of the cartilage by the ulcerative process
in this situation; and inflammation of the medullary web, leading to
atrophy of the cancelli, collections of pus therein, or even death of a
portion of the spongy texture of the bone, as will be more particularly
treated of in the chapter on diseases of the osseous tissue. These
changes often compose the primary disease, and to them the affections
of the synovial membrane and other parts succeed.
Such occurrences are attended with alarming disturbance of the
constitution, with fever, and even with the most threatening and
dangerous symptoms, such as delirium and coma. If the patient69 survive,
and the matter be evacuated from the joints by openings into its
cavity, hectic fever is almost certain to supervene.
An opinion has been broached lately by Mr. Key, that the ulceration
of cartilage was consequent upon the increased vascularity and
thickening of the synovial membrane, that the cartilage, in fact,
was removed by the action of the vessels ramifying in the membrane,
and the prolongations or fringes from it in its diseased condition.
Occasionally these fringes correspond, in a remarkable manner, to the
breach of surface in the cartilage; but again, ulceration is frequently
met with far removed from the membrane. It is also seen, in cases
where an opportunity is afforded of making the examination in the
earlier stage of disease, that ulceration exists to some extent whilst
the synovial membrane is unaffected. And certain cases, in which the
cartilage is affected with hypertrophy, and the common form of atrophy
of this part in old people, are altogether adverse to Mr. Key’s views.
When ulceration takes place at a point removed from the attachments
of the synovial membrane, it appears to proceed more frequently from
the attached than from the free surface of the cartilage; then the
adventitious membrane occupying the rugged spaces, and which under the
microscope appears highly vascular, is connected apparently with the
medullary web.
In acute inflammation of the synovial membrane, and in cases where the
cartilage is ulcerated, the pain is very intense, and the spasms of
the limb most distressing. This happens when the surface is ulcerated,
and perhaps to no great extent. We know that in the horse an ulcerated
hollow in the cartilaginous covering of the navicular bone, not so
large as to contain a grain of barley, will cause such lameness and
suffering as to render the animal so affected perfectly useless. If he
is not destroyed at this stage, as many valuable animals have been,
the mischief extends, and terminates in extensive disease of that
and the neighbouring bones and articulations. It is different if the
disease commence, as it sometimes does, in the human subject, in the
cancelli of the bone, and on the attached surface of the cartilage,
the free surface remaining some time entire and smooth. When the
synovial membrane is primarily affected by chronic disease, the pain
is in general trifling, often not complained of, and swelling of the
part, from effusion, into the joint or neighbouring bursæ, first
attracts attention, after it has existed, perhaps, in a slight degree,
for a considerable time. The joint is stiff, and pain is experienced
from extensive motion; on this account the patient is disinclined to
use it, and it is soon tired by the slightest exertion. The swelling
becomes more solid, though still remaining elastic, and the feeling of
fluctuation diminishes. Effusion of lymph follows that of serum, the
latter having been absorbed; the motion of the joint is still further
impeded, and the articulation is distorted; the patient keeps the limb
in the most easy position, generally that of partial flexion, in which
it becomes almost immovably fixed. The cause of the flexed position,
which is almost pathognomonic of knee disease, being preserved, seems
to be that the limb is insensibly brought into it in order to take the
pressure off the interarticular apparatus, the ligamenta mucosa and
alaria,—these swell—the70 muscles of the hamstrings get contracted from
habit, and a difficulty, even after the disease is completely subdued,
is often enough experienced in procuring complete extension. The
muscles, from disuse, shrink, the adipose substance is absorbed, the
shafts of the bones also are diminished in size, get into an atrophied
state, as the phrase is, and thus the whole limb is rendered slender
and wasted, so as to make the swelling of the diseased articulation
still more conspicuous. The bones are softened, and the muscles are
of a white colour, as in the limbs of the paralytic or bedridden,
and resemble more cellular than muscular tissue. The wasting of the
muscles and loss of power often precede the appearance of disease; this
is frequently observed in the shoulder-joint, the deltoid shrinking,
and almost disappearing, before any disease in the articulation
is suspected by the patient. Not unfrequently, also, this wasting
occurs without obvious cause, or any affection of the joint. When the
disease is advancing, the patient may feel no acute pain, but merely
a reluctance to use the limb; and from this, if long continued, the
muscles, and afterwards the bones, become wasted. Wasting of the limbs
in children, often of one of the lower, frequently arises from disorder
of the bowels, and the irritation and debility attendant on teething.
This must be distinguished from the wasting accompanying diseased
joint. The history of the case, the period at which the weakness of the
limb was observed, and its appearance, will lead to a correct diagnosis.
The swelling is often irregular, being more protuberant at one part
than another, from the fluid or the addition of solid matter being
accumulated where the least resistance is afforded; but the slighter
inequalities are generally filled up by œdema of the cellular
texture. As the disease proceeds, matter forms in the joint, and
is often attended with great pain and fever; or the pus is effused
into the bursæ, into the surrounding cellular tissue, or into the
filamentous tissue amongst the tendinous sheaths of the muscles in the
neighbourhood; being allowed to remain without an outlet, it at length
communicates with the cavity of the joint. Portions of the cartilages
are absorbed, though this, as already noticed, may occur at the very
commencement of the disease; the subjacent bone becomes affected by
ulceration, or perhaps its vitality is partially destroyed. When
matter has accumulated, a portion of the capsular ligament generally
ulcerates, the pus escapes, and is ultimately discharged externally.
When the disease begins with swelling, which is of a chronic character,
and produces but little inconvenience, and when the more urgent
symptoms supervene after the swelling has continued for a considerable
time, there is every reason to suppose that the disease has originated
in the synovial membrane, or perhaps in the osseous cancelli, and
this is generally met with in poorly fed and strumous subjects. But
when the first symptoms have been pain and stiffness of the joint,
without change of its appearance, and when the swelling has occurred
after these symptoms have been of some duration, then it is probable
that the cartilages are the primary seat of mischief. For the most
part, however, the symptoms have a general resemblance in most chronic
affections of the joints, and all the apparatus is sooner or later
involved. When the cartilage has been extensively71 absorbed, a grating
sensation is felt in moving the articular surfaces of the bones upon
each other. In consequence, also, of the softening and disorganisation
of the lateral and other ligaments, the affected articulation at length
becomes unnaturally loose, which is owing in some measure, also, to the
muscles being wasted and paralysed from pain and disuse. At an earlier
stage of the disease, the joint may be rigid from deposition of lymph
into the contiguous cellular tissue, and contraction of the muscles.
Purulent matter not unfrequently collects in the substance of the
bones, which in all cases ultimately become softened in a remarkable
manner. In many subjects, without actual disease of the osseous
tissue, the heads of the bones are so altered in consistence, are so
deficient of earthy matter, as to be easily cut with a knife. It has
been a matter of dispute, whether, in this affection, the articulating
extremities of the bones are enlarged or not; and the supposition that
they are always more or less increased in size, or hypertrophied, has
arisen from the extensive effusion and indurated state of the soft
parts being mistaken for this enlargement. In the first stages of the
disease, they are seldom, if ever, enlarged; but when ulceration of the
bone has occurred, new osseous matter is deposited to a greater or less
degree in the neighbourhood of the ulcer,—an attempt by nature towards
a cure, but too often an ineffectual one. The bones, in strumous
subjects, are often much enlarged, from collection of purulent matter
in their substance giving rise to a sort of spina ventosa. I removed
the upper extremity of a boy lately on account of extensive disease
about the elbow. The ulna to near the wrist was swollen enormously by
purulent collections in its medullary canal. In cases when the whole
of the articulating extremity of the bone is not enlarged, still that
portion which is more immediately concerned in the articulation is
often considerably expanded.
Frequently when the knee is the seat of the disease, the lymphatic
glands in the groin are enlarged; and when the elbow or wrist joints
are affected, there is often a similar enlargement of the glands in
the axilla: such glandular tumours have not rarely been confounded
with those accompanying malignant disease, and measures which were
absolutely necessary for the salvation of the patient, have thus been
delayed or neglected.
When the disease is extensive, and has endured for a considerable
period, hectic fever supervenes, and is aggravated after the abscesses
give way. The patient becomes much weakened and emaciated, and loses
his appetite; the pulse is rapid, with night sweats, diarrhœa, &c.;
and from a continuation of the hectic cause, the life is endangered.
In some cases, however, the health is restored, and the disease abates
spontaneously; in others, the disease is arrested, and a complete
cure accomplished, by the careful employment of such means as will be
afterwards mentioned.
The appearances produced by inflammation and consequent disease of
the synovial membrane, are the following. In the first stage, the
internal surface of the capsular ligament, and the rest of the synovial
membrane, is found of a red hue, its formerly colourless vessels being
now made apparent, from enlargement and consequent injection with a
greater quantity of red blood; and the serum within the cavity of72 the
joint is more abundant than in the natural state. When the disease
has been of longer continuance, the membrane is found considerably
thickened, its usual smooth glossy surface is destroyed, it is
irregularly flocculent, and frequently of a light yellow colour.
The interarticular adipose tissue also seems to be increased in volume,
from being infiltrated with a serous fluid, by the discharge of which
the diseased bloodvessels may have attempted to relieve themselves.
When the inflammation has been intense, or of long duration, lymph
is secreted, and deposited on the external surface of the membrane,
forming an intimate union between it and the ligaments, and producing
thickening of the external apparatus. Or the lymph is also effused on
the inner surface of the membrane, to which it adheres and becomes
organised; this is generally accompanied by the formation of purulent
matter; the organised effusion is often so extensive as to conceal
almost the whole of the synovial membrane, excepting portions of its
delicate reflexions which invest the articulating cartilages. By the
lymphatic deposit, to a less degree, the folds also of the synovial
membrane adhere to each other, whereby the motion is still farther
impeded, and the pain, when attempted, increased. Occasionally the
synovial membrane is found enormously thickened, much softened in
texture, and of a brown hue, when the disease has been of a very
chronic character. Along with these appearances, serum is generally
found effused, in a greater or less quantity, into the cellular tissue
exterior to the ligamentous covering. In cases in which the matter
has formed and remained long within the cavity of the articulation,
the synovial membrane and the ligaments become blended into one soft
mass, the internal surface of which is lined with a thick coating of
lymph, as in the case of common abscess. If purulent matter is effused
externally, and communicate with the joint, the capsular ligament will
be found to have ulcerated and given way at certain points, forming
apertures, usually of small size, and with ragged margins.
All these appearances may exist without disease of the cartilages
 or extremities of the bones; but generally they are also affected
at the same time. At first the surface of the cartilage is slightly
irregular and rough, and the change is not observed, unless on minute
inspection. Afterwards the surface is marked with small depressions,
which may be numerous, and are surrounded with irregular and somewhat
serrated margins. They gradually increase in depth and extent, and
the subjacent bone is ultimately exposed at one or more points, as
here shown. Often the greater part of the cartilage is removed by
absorption; the bone is exposed, opened out in its texture, softened,
of an irregular surface, and in some places excavated, containing a
thin ichorous fluid; the process of ulceration has also extended to the
osseous tissue. Sometimes scales of cartilage of considerable size are
either completely detached, having become dead, and been73 thrown off
by the natural process, and are found lying loose in the cavity of the
articulation; or they are all but separated, adhering by one or more
very slender attachments.
or extremities of the bones; but generally they are also affected
at the same time. At first the surface of the cartilage is slightly
irregular and rough, and the change is not observed, unless on minute
inspection. Afterwards the surface is marked with small depressions,
which may be numerous, and are surrounded with irregular and somewhat
serrated margins. They gradually increase in depth and extent, and
the subjacent bone is ultimately exposed at one or more points, as
here shown. Often the greater part of the cartilage is removed by
absorption; the bone is exposed, opened out in its texture, softened,
of an irregular surface, and in some places excavated, containing a
thin ichorous fluid; the process of ulceration has also extended to the
osseous tissue. Sometimes scales of cartilage of considerable size are
either completely detached, having become dead, and been73 thrown off
by the natural process, and are found lying loose in the cavity of the
articulation; or they are all but separated, adhering by one or more
very slender attachments.
The incipient stage of such disease may exist without the synovial
membrane being much, if at all, affected; but when the ulceration has
made farther progress, all the articulating apparatus is more or less
diseased. It may be here remarked, that the synovial membrane may be
affected for a long period, thickened portions may extend over the
cartilages, and these may have lymph upon them and yet remain intact.
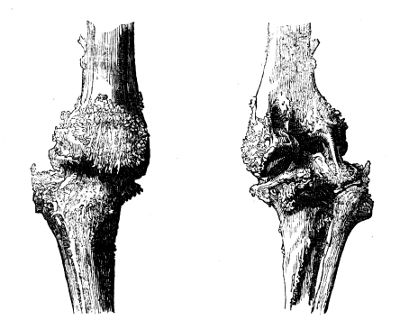
The cure, resorted to by nature, and in which she may be much assisted
by the surgeon, is Anchylosis, ligamentous or osseous. New bone
is deposited in the neighbourhood of the disease, and the ulcers
become, as it were, cicatrised; the articulating extremities of the
bones are joined to each other by a firm osseous matter, either
universally disposed or consisting of processes extended between the
bones at various points: or again, in consequence of the effusion of
lymph into the cellular tissue, and the consequent thickening and
induration of that and of the fibrous tissue exterior to the joint,
this connecting medium is so strengthened and concentrated as to retain
the articulating surfaces in exact apposition; from one, and usually
from both, of these changes, the joint is securely fixed and rendered
immovable, or nearly so. In complete anchylosis, the cancellous texture
of the two bones, after some time, becomes perfectly continuous, so
that they in fact constitute but one bone, as seen in cut, p. 84. A
very perfect specimen of anchylosed knee joint is also delineated in
the cut above. But even after this happens, the disease is still apt
to recur from slight causes, the bony or ligamentous union being74
disturbed or destroyed, and the original disease attacking the parts
with fresh activity; abscesses form,—may be extensive both in size
and number,—and thereby the health is again undermined. So that the
patient, after undergoing much suffering and risk, preserves, perhaps
only for a few years, a limb which is almost useless to him, and which
must be removed at last. In other cases, the union is permanent, the
disease does not return; by care and time the limb is brought into the
most convenient position, and proves of considerable service.
The joints are often affected by rheumatic and gouty inflammation;
and there are three species of disease, tolerably distinct in their
pathological characters, generally attributed to these causes. In
one there is a deposit of chalky-looking matter, composed chiefly
of super-lithate of soda, on the articular surfaces of the synovial
membrane and cartilage, but most abundantly in the cellular tissue
outside the joint, an affection in which the cartilage is seldom
known to ulcerate. In the second, the cartilages are atrophied, as if
 worn away by attrition, the articular surfaces of the bone being much
modified in shape, more or less denuded of cartilage, and remarkably
polished and hard, so as to have been compared to porcelain, as will be
described in another section. In the third, the fibrous tissue in the
neighbourhood of a joint is primarily affected, the synovial membrane
and cartilages not becoming involved till the disease is much advanced.
It is not uncommon in the elbow of middle-aged persons who have been
much exposed to the atmospherical vicissitudes, and is sometimes
attributed to the effect of mercury or syphilis. The periosteum
around the articular ends of the bones becomes swelled and painful;
the affection is very slow in its progress; abundant deposition of
adventitious bone takes place, often in short spiculæ, gradually
encroaching around the joint, which ultimately becomes involved. A good
specimen is here given. The disease was of twelve months’ duration, and
was attributable to rheumatic inflammation supervening upon sprain. The
affection involves extensively all the bones composing the articulation.
worn away by attrition, the articular surfaces of the bone being much
modified in shape, more or less denuded of cartilage, and remarkably
polished and hard, so as to have been compared to porcelain, as will be
described in another section. In the third, the fibrous tissue in the
neighbourhood of a joint is primarily affected, the synovial membrane
and cartilages not becoming involved till the disease is much advanced.
It is not uncommon in the elbow of middle-aged persons who have been
much exposed to the atmospherical vicissitudes, and is sometimes
attributed to the effect of mercury or syphilis. The periosteum
around the articular ends of the bones becomes swelled and painful;
the affection is very slow in its progress; abundant deposition of
adventitious bone takes place, often in short spiculæ, gradually
encroaching around the joint, which ultimately becomes involved. A good
specimen is here given. The disease was of twelve months’ duration, and
was attributable to rheumatic inflammation supervening upon sprain. The
affection involves extensively all the bones composing the articulation.
Although wounds penetrating the larger joints are attended with
danger, the synovial membranes are possessed of considerable powers of
reparation, and often heal readily after severe injuries. An occasional
result of inflammation is adhesion between the layers of the membrane,
but this is by no means so frequent as in the serous tissues. The
reparative power of cartilage is so low that the best termination that
can be expected from the ordinary forms of ulceration, is union between
the abraded surfaces. In experiments which have been made on the lower
animals, portions of cartilage which had75 been removed from their
joints were never reproduced, but the functions of the part were soon
restored by the cut surface becoming smooth. In like manner there is
occasionally to be seen in museums a circumscribed indentation in human
articular cartilage, as if it had been destroyed by a small ulcer in
this situation, which had cicatrized without any reproduction of the
destroyed tissue.
ON HYPERTROPHY AND ATROPHY OF THE ARTICULAR CARTILAGES, WITH EBURNATION
OF THE SURFACES OF THE BONES.
It has been already observed (at page 68), that the cartilages are
occasionally swelled and softened in cases of chronic inflammation; and
it now remains to notice instances in which they become hypertrophied
or atrophied, apparently without inflammatory action. Although these
affections are not likely to come often under the treatment of the
surgeon in civil life, yet they are of much importance to the naval or
military practitioner, since an accurate knowledge of them will lead
him to institute a careful inquiry when a man complains of inability to
sustain the fatigue of marching with the burden of a heavy knapsack;
and they are of considerable interest in a physiological point of view,
because they tend to show the inherent vitality of cartilage, and that
it is liable to serious organic changes quite independently of diseased
action in the surrounding tissues.
Some examples of hypertrophy of cartilage, principally affecting that
of the patella, have been described by Mr. Gulliver, and figured in the
third fasciculus of drawings from the Army Anatomical Museum. In these
the cartilage is swelled so as to form a ridge across the articular
surface of the bone, the hypertrophied part being perfectly smooth,
except where its continuity is interrupted by irregular fissures, as
if the perpendicular cartilaginous fibres were split into bundles of
variable size and shape. These cases occurred in young and middle-aged
men who died of pulmonary consumption; and it is probable that the
disease would be more frequently found, if it were more frequently
looked for, since it does not seem to have been accompanied by any
change in the surrounding parts, and would perhaps only be indicated by
weakness of a joint rendering it unfit for severe work.
The atrophy, or absorption of cartilage, is so frequently seen in
the joints of old subjects, that some authors have been disposed to
regard it rather as a physiological than a pathological condition.
It is, however, unquestionably a disease; and in the drawings above
mentioned, are some specimens of it from a soldier under the middle
age. The cartilage seems in the first instance to be opened out in its
texture, and numerous little villous processes appear on its surface,
often as if its fibres were enlarged after absorption of the substance
which connected them. The thinning sometimes takes place in patches,
occasionally in grooves, corresponding to the motions of the articular
surfaces; the subjacent bone becomes at length completely denuded,
and soon presents a polished porcelain-like surface, which is so
re76markable that it is commonly known under the name of porcellaneous
deposit. It is obvious that, when the disease has proceeded thus
far, the joint must become more or less deformed, and its motions
considerably impeded. Accordingly, old men are often seen at work
with much rigidity of the joints, particularly of the knee, which is
frequently projected inwards, from absorption of the cartilage from the
outer condyle of the femur and corresponding part of the tibia, with
a thinning and degeneration of the inner-articular cartilage into a
tissue resembling the cellular.
The hard, polished, and ivory-like appearance of the articular surface,
would lead us to suppose that it contained an unusual quantity of
earthy matter, yet an analysis by Dr. Davy, here given, shows the
contrary.
| Composition of the Shaft. | Composition of the polished Articular
Surface. |
| Phosphate of lime, &c. | 58·8 | Phosphate of lime | 54·2 |
| Animal matter | 41·2 | Animal matter | 45·8 |
| | —— | | —— |
| | 100·0 | | 100·0 |
In many instances where the disease is of long standing, a deposit of
adventitious bone takes place around the articular surfaces, and this
may occur to such an extent as to produce anchylosis of the joint, the
articular extremities of the bone often presenting several irregular
depressions, and becoming variously altered in shapes, as shown in the
cuts, p. 86.
It is curious that the atrophy of cartilage is generally seen in
its early stage to attack the joints in pairs, and to occur also in
corresponding parts of the articular surfaces; a fact which coincides
with the disposition of caries to appear simultaneously or successively
in corresponding molar teeth.
Of the causes of the disease but little is known, although it is
generally attributed, like some other obscure affections, to the
effect of rheumatism. It often follows in old people upon long disuse
and confinement of a limb to one position, as during the cure of
fractures. A very valuable specimen was presented to me lately by my
friend Mr. Busk, of the Dreadnought hospital ship. The elbow had been
apparently subjected to great injury. The radius and ulna had been
fractured: the former had united, whilst a false joint had been formed
betwixt the portions of the ulna. There is profuse deposit of bone
around the elbow-joint, which must have been quite stiff, or nearly
so, as regarded flexion and extension; but the end of the radius and
corresponding articulation of the humerus are beautifully polished.
This polish is not unfrequently seen also upon disunited fractures, as
in the neck of the femur. Atrophy of the cartilages has been seen where
no rheumatism was ever known to have troubled the patients; and they
are more generally disposed to ascribe it to the effect of incessant
hard work. At all events it is comparatively rare among women, and in
the upper ranks of society; and the wasting often presents very much
the appearance which would result from the77 effects of attrition, as
if the wear of the cartilage had not been supplied by a corresponding
reproduction. It is probable, therefore, that the affection is
attributable to defective nutrition, somewhat allied to certain changes
in the cornea, which are known to proceed from this cause, and which
are also unattended by inflammation or the formation of pus.
The symptoms of the disease are generally obvious enough in the more
advanced stages by the crackling which may be heard when the joint
is moved; and in the early stage a grating may be felt by a careful
manipulation.
SCROFULOUS DISEASE OF JOINTS.
Affections of the membranes, ligaments, and bones, often occur in
persons of weak constitutions, and proceed very gradually. They have
been all classed under the general term of white swelling. They most
frequently present themselves without any assignable cause, or are
attributed to the slightest injuries. The disease generally commences
in the cancellated texture of the bones: these are soft and light, and
contain in their cells a quantity of caseous or tubercular matter. The
softness is attributable to an interstitial atrophy of the bony tissue,
as well as to an alteration in the proportion of its constituents; the
animal matter being in excess, with a corresponding deficiency of the
phosphate of lime. There is an increased vascularity of the medullary
membrane, and the cancellated texture contains thin brownish-looking
fluid instead of marrow. In cases of disease which has commenced
in the cancellated texture, there is hardly any pain at first, and
the progress of the disease is remarkably insidious. When the lower
extremity is affected, the child is observed to limp; the limb wastes;
it appears to be longer, partly from atrophy of the muscles, partly
from relaxation of the ligaments and effusion into the joint.
The term white-swelling, which ought to be discarded from surgery,
was at one time made to include all the different affections to which
joints are liable in weak constitutions—thickening of the parts,
with an external colourless swelling—collections of matter about
articulations, with or without an external aperture—effusion of fluids
into the cavities of joints, or into the bursæ—destruction of cartilage
by ulceration, or in consequence of portions becoming dead—absorption,
ulceration, caries, or intractable ulceration of the bone adjoining the
articulation.
Those under twenty years of age are most liable to chronic affections
of the joints, and they occur very frequently in children. Great
anxiety is often shown by friends of patients to account for chronic
disease of a joint, so as to save their whole generation from the
imputation of being tainted with scrofula. It is attributed, sometimes
correctly enough, to some injury perhaps trifling; to a sprain, or
twist, or squeeze from a tight shoe, or to a bruise from falling; and
it is no doubt true, that young or old people of the most healthy
con78stitutions, if thrown out of health from one cause, will present
all the appearances of scrofula, and become affected with chronic
diseases of the mucous membranes, glands, joints, or bones, from very
slight existing causes.
Such affections advance slowly; all the articulations are liable to
them; but those which are most subject to the disease are the hip,
knee, ankle, and elbow. Of these, the knee-joint is most frequently
affected, probably from the greater extent of cancellated and
articulating surface. In young persons of unhealthy constitutions,
the joints not unfrequently become affected one after another, and
superficial abscesses form, terminating in open sores. I was obliged to
amputate the upper extremity of a young lady a few days ago, in which a
metacarpal bone and its articulation, the entire chain of carpal bones,
the wrist and elbow joints, were all thoroughly involved in disease.
NEURALGIC AFFECTIONS OF JOINTS.
The joints, like other parts of the body, are very often the seat of
painful affections, without organic disease existing. These neuralgic
affections are often connected with, or followed by, hysterical
symptoms. They frequently also depend upon derangement of the digestive
organs,—upon the lodgement of irritating matters, sordes, or worms in
the intestinal tube; and when we reflect upon the extent of the lining
membrane, the expansion of nervous filaments, and upon the sympathy
which they hold with the whole system, we cannot be astonished at the
circumstance. Many cases of supposed hip-disease in children, with
the symptoms and some of the signs of it, have come under my notice,
which have yielded at once to the expulsion of offending matters or
worms. Some affections of joints seem to depend upon gouty diathesis;
others are intermittent: at one time the joint complained of is hot,
and somewhat swollen; at another cold, and bluish on the surface. In
these affections of joints the pain, indeed, is seldom constant: the
patient’s rest is not broken; there are none of the violent spasms
during sleep, which attend upon certain alterations of structure. The
pain is equally complained of when the part is touched with the utmost
gentleness, or when a thorough and searching examination is made, when
the joint is freely moved, and the articulating surfaces of the bones
are forcibly squeezed against each other. The pinching of the skin
causes pain. There is seldom throbbing, or heat, or swelling; though,
after long continuance of the diseased state, these may supervene to a
slight extent. The pain complained of is seldom referred to one point,
but to a large extent of the limb; and if the attention is diverted,
the examination may be carried to any extent, without complaint being
made.
Sir B. Brodie, who has done a great service to the profession by
directing attention to these nervous affections in his excellent work,
and in his lectures, notices that the knee, when the seat of pain, is
generally kept in the extended position, and this is very different
from79 what has been stated to be the position of one affected by
organic disease. The tumefaction following upon local treatment, and
especially when leeching and counter-irritants have been employed, is
sometimes, as he remarks, very perplexing.
This class of diseases generally affects females of delicate
organisation about the age of puberty, and in whom the menstruation
is irregular. Males in delicate health are also subject to similar
affections.
ON GROWTHS FROM THE SYNOVIAL MEMBRANE, AND LOOSE SUBSTANCES IN THE
JOINTS.
The synovial membrane is sometimes studded on its inner aspect with
loose fleshy or semicartilaginous substances projecting into the cavity
of the joint. The entire surface of the membrane is occasionally
covered with these bodies, which are of a white or yellowish colour,
and very variable in size and shape; the smallest presenting the form
of villi not much larger than those of the jejunum, the largest having
somewhat the magnitude and appearance of the appendices epiploicæ of
the large intestine, while many of an intermediate size approach in
appearance to a lemon-seed. In some instances the membrane is only
partially pervaded by them, and they are not unfrequently arranged like
a fringe around the edge of the articular surfaces. They are generally
very smooth on the surface, which appears to be perfectly continuous,
if not identical, with the synovial membrane. Their attachment is
frequently broad, and occasionally very narrow and pedunculated, often
merely filamentous, so that a little further thinning of the part, or
slight force acting on the body, would remove it from the capsule, and
throw it loose into the cavity of the articulation. The disease has
been most frequently seen in the knee, and sometimes in the elbow.
The affection is obscure in its nature; it is slow in its progress;
the joint is the seat of pain after and during exercise, probably from
the morbid processes interfering with the motions of the articular
surfaces. As the disease advances, the joint becomes swelled and
elastic, unattended generally by ulceration of the tissues within or
around it. In examining the part, when the articular surfaces are moved
on each other, it will be found that their motion is more or less
interfered with; and considerable irregularity in their action may be
felt by the hand placed firmly on the joint during the procedure.
Loose bodies may be found in the articulations, particularly in the
knee and elbow, under the circumstances just described; but we often
find others of a different structure loose within the capsule, which
may be throughout smooth and apparently healthy. These bodies are
extremely variable in size, generally rounded or oval, with a polished
surface; many of the smallest present the character of fibro-cartilage
or cartilage; the larger are often more or less modulated, very firm
and gristly, and sometimes contain a considerable nucleus of bony
matter. The articular ends of the bones are occasionally80 more or less
misshapen by the formation around them of knobs of adventitious osseous
substance.
The disease is common in the knee; and patients frequently go about
for years, who will tell you that they have something rolling within
the joint, which will often be found on examination to be actually
the case. It is obvious that loose bodies in the joint must prove
an obstacle to easy progression; and the smaller ones seem to be
particularly so, probably from becoming easily entangled by different
parts of the articular apparatus.
However difficult it may be to account for the cause of these
formations, the means by which they may get within the articulation
seems obvious enough. If a small knob of coagulated lymph should
form on the inner aspect of the membrane, the point of attachment,
as has already been noticed, might gradually become narrower, from
the motions of the joint or other causes, till the connection were
severed. But there is reason to believe that many of the substances
found loose in the joints are formed altogether in the cellular tissue
without the capsule; for it is difficult to conceive that they can
increase in size, or take on the ossific action in their centre, by an
act of independent vitality, after they have been separated from the
surrounding parts. Accordingly, dissection has occasionally disclosed
loose bodies within the knee-joint, and others of just the same
structure outside the synovial membrane, which was however protruded by
their pressure, and appeared to connect some of them by a pedicle only,
ready to break and allow the foreign body, with its covering of the
membrane, to fall into the cavity of the articulation.
AFFECTIONS OF SYNOVIAL POUCHES OR BURSÆ.
Bursæ are lined by a membrane, greatly resembling the synovial in
appearance, function, and disease. They are frequently the seat of
inflammation of an acute character; but in most instances the action
is of short duration, and generally terminates in an increase and
accumulation of the secreted fluid. The attendant pain is very severe,
and much increased by any motion of the neighbouring parts.
Occasionally a portion of the cellular substance, which is exposed
to pressure of motion, as over a prominent portion of bone, assumes
the appearance of a bursa, secretes a similar fluid, and is similarly
affected in consequence of inflammation. These adventitious bursæ are
met with in various situations. Bunion is a good example of such a
bursa thickened from long-continued pressure. They are seen on the
outer ankles of tailors, on the shins of boot-closers, on the forehead,
point of the elbow, &c.
Disease of the bursæ may occur from external injury, and they often
become affected subsequently to disease of the neighbouring joint.
If the action is violent, lymph is effused on the inner surface, or
external to its cavity, causing considerable thickening. The sac is
thus sometimes all but obliterated. Tumours, originally house81maid’s
knee, aggravated by continued pressure, are met with over the ligament
of the patella in almost a solid state. Occasionally the action
terminates in suppuration, pus being effused to a greater or less
extent into the cavity; and if allowed to remain or accumulate, the
abscess extends, and frequently communicates with the neighbouring
joint, which may not have been previously diseased. In chronic cases
of enlarged bursæ, especially of the bursal thecæ of the tendons of
the wrist or ankle, we not unfrequently meet with loose cartilaginous
bodies of various sizes, and of a flattened oval form, floating in
the accumulated fluid. These have been also supposed to be formed by
portions of lymph which have been deposited on the surface, condensed
in structure, and afterwards become detached.
When inflammatory action has commenced in a bursa, it must be subdued
by copious topical bleeding, along with the exhibition of purgatives;
in most cases general bloodletting will not be required. After the
inflammation has subsided, the parts remain swollen, from the effusion
either of serum or lymph; stimulating applications may then be employed
with advantage. In general, the ammoniacal plaster, or the brushing
over the surface with tincture of iodine will answer. Blisters are
sometimes employed with the same view. In obstinate cases, when the
tumour is of no large size, a seton may be passed, retained till
suppuration has taken place, and gradually withdrawn. Great risk
attends interference with bursæ of large size near joints or cysts
containing serous or glairy fluid in any situation. Even trifling
punctures into such have been sometimes followed by inflammation of
the inner secreting surface and violent constitutional disturbance.
When suppuration has occurred, it will in many instances be prudent
to evacuate the matter by one or more incisions, in order to prevent
farther mischief, especially if the bursa, a superficial one, is in
the neighbourhood of a joint. After the matter has been evacuated, the
cavity gradually contracts, and ultimately the bursa is completely
obliterated. Diseased bursæ, near the surface, and unconnected with
important parts, have been dissected out. The operation is not often
necessary, and in some situations attended with considerable risk.
Tumours, solid or nearly so, arising from diseased bursa of long
standing, may sometimes require to be so treated.
OF COXALGIA, MORBUS COXARIUS, OR HIP-JOINT DISEASE.
This disease has been supposed to commence in the cartilages; it
appears, however, to originate indiscriminately in the cartilage and
the bone, as well as in the membrane lining the capsule and investing
the cartilage and the ligaments; but whether it begins in one or other
of these tissues, it soon, if neglected, involves them all. It affects
patients of all ages, though children under twelve are most generally
its victims; and in these it often makes considerable progress without
its existence being suspected. The patient is observed to be a little
lame, and to be awkward in the use of the affected limb, but he
experiences little or no pain in the first instance; and if he82 does,
it is of a dull kind, and generally referred to other parts. Thus, pain
in the knee is generally the prominent symptom of this affection, and
occasionally pain is also referred to the ankle, or to the sole of the
foot: careful study and considerable experience are here required, to
guard the young practitioner from error in diagnosis. Parts remote from
the seat of morbid action have often been made the subject of treatment
in this and other affections; the knee, in morbus coxarius, has been
leeched, poulticed, blistered, and burnt, and that, too, when this
joint was not at all altered in appearance, and showed no symptom of
disease.
Again, and particularly in adults, the limb is easy only in certain
positions, and cannot be moved without great suffering; pain is also
complained of in the groin, and often immediately behind the trochanter
major. If an examination is made when the patient is thus halting, and
even though he complains of no pain, the limb is found shrunk, wasted,
and lengthened. The elongation of the limb occurs mainly in consequence
of the inclination of the pelvis towards that side. When the disease
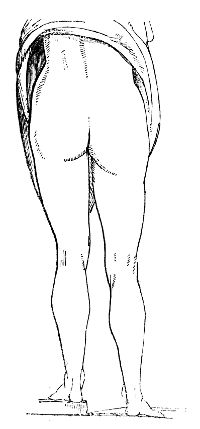 has made progress, it has been supposed that swelling of the apparatus
of the joint, and effusion into its cavity, might separate the head
of the bone from the acetabulum, when pressure from the trunk was not
applied. The lengthening is often great, and its extent and cause are
ascertained by accurate comparison of the two limbs, laid in contact
when the patient is in the recumbent posture.
has made progress, it has been supposed that swelling of the apparatus
of the joint, and effusion into its cavity, might separate the head
of the bone from the acetabulum, when pressure from the trunk was not
applied. The lengthening is often great, and its extent and cause are
ascertained by accurate comparison of the two limbs, laid in contact
when the patient is in the recumbent posture.
The degree of lengthening is here carefully represented from a recent
case. But occasionally, even in the first stage, before destructive
ulceration has set in, in consequence of the pain and spasms, the limb
becomes remarkably shortened and retracted. This also will be found, on
careful examination, to depend upon the relative positions of the two
ossa innominata.
When the patient stands, the affected limb is considerably advanced
before the other, on which the weight of the trunk is chiefly, or
entirely, supported; the knee is generally bent, and the toes only
rest on the ground. In the advanced stages of the disease, and when
there is reason to suppose that ulceration of the cartilages has set
in, the patient, during progression, moves the affected limb with the
hands grasped round the thigh, and in bed it is moved by the aid of the
sound one. The spine is frequently affected, becoming bent in different
directions, to preserve the equilibrium of the body; and a deformity of
the trunk to a certain degree occurs, which, however, may be in general
easily remedied. The83 nates are much altered; they become flattened,
and those parts which are naturally most prominent are reduced to the
level of the others; the usual niche between the buttock and thigh,
in the erect position, is effaced, and the upper part of the thigh
is often considerably swollen. The alteration is at once manifest on
contrasting the healthy with the diseased side. Even from the first,
locomotion is difficult: in the morning, the movements of the joint
are constrained and stiff; afterwards, however, the patient walks with
more ease, though still by very slight exertion the limb is speedily
tired, and he is unwilling to use it. Pain is produced by pressing on
the groin, or by tapping on the trochanter, and by pushing the head
of the femur forcibly against the acetabulum. The inguinal glands
occasionally become enlarged. As the disease advances, the lameness is
more apparent; pain is produced and increased by motion, and by any
attempt to stretch, and more especially to abduct the limb whilst in
the recumbent posture. The emaciation of the member becomes more and
more visible. The muscles, as it were, are paralysed from inaction and
pain, abscesses form, and the constitution then sympathises remarkably;
hectic fever supervenes, with its usual train of symptoms.
The circumstances attending the first stage of the disease in
childhood, in which the limb is lengthened, and there is no decrease,
but rather an enlargement of the parts composing the joint, have been
already described and illustrated. When, however, absorption occurs,
and the articulation begins to be destroyed, the second stage of the
disease commences, and the limb becomes then sensibly shortened; the
toes are turned inwards or outwards; in many cases there is every
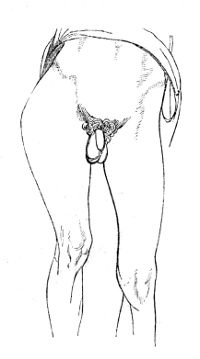 appearance of dislocation of the thigh upward and backward; and in
others the limb is much bent, the toes only reaching the ground.
The ultimate position of the limb and degree of shortening will
depend much upon the extent to which the head and neck of the femur
is destroyed, upon the inclination of the pelvis, and also upon the
portion of the acetabulum which is most diseased. The joint becomes
tender, the slightest motion causing much pain, and the parts around
appear swollen. The patient retains the limb in the most comfortable
position, and it is generally bent upon the pelvis and inverted. This
may arise from relief being afforded when the psoas is relaxed, and
the pressure thus removed from the fore part of the joint. In many
cases matter forms behind, or rather below, the trochanter major, and
the collection often attains a large size. When the presence of matter
has been ascertained in this situation, it has been84 recommended that
an early opening should be made, on the supposition that the disease
arises from an acrimonious discharge into and round the joint, and
that, by the matter being allowed to escape, the cause of the disease
may be removed. The synovia has been compared by one old author to
bland oil, the vitiated secretion to oil of vitriol. Though the
principle is incorrect, still the rule of practice is important; for in
consequence of the long-continued presence of matter, accumulating in a
cavity which is not dilatable in proportion to the increase of purulent
secretion, the original affection will be much aggravated, and disease
induced in the neighbouring parts. But the existence of matter in the
joint could only be ascertained to exist in a very emaciated person.
appearance of dislocation of the thigh upward and backward; and in
others the limb is much bent, the toes only reaching the ground.
The ultimate position of the limb and degree of shortening will
depend much upon the extent to which the head and neck of the femur
is destroyed, upon the inclination of the pelvis, and also upon the
portion of the acetabulum which is most diseased. The joint becomes
tender, the slightest motion causing much pain, and the parts around
appear swollen. The patient retains the limb in the most comfortable
position, and it is generally bent upon the pelvis and inverted. This
may arise from relief being afforded when the psoas is relaxed, and
the pressure thus removed from the fore part of the joint. In many
cases matter forms behind, or rather below, the trochanter major, and
the collection often attains a large size. When the presence of matter
has been ascertained in this situation, it has been84 recommended that
an early opening should be made, on the supposition that the disease
arises from an acrimonious discharge into and round the joint, and
that, by the matter being allowed to escape, the cause of the disease
may be removed. The synovia has been compared by one old author to
bland oil, the vitiated secretion to oil of vitriol. Though the
principle is incorrect, still the rule of practice is important; for in
consequence of the long-continued presence of matter, accumulating in a
cavity which is not dilatable in proportion to the increase of purulent
secretion, the original affection will be much aggravated, and disease
induced in the neighbouring parts. But the existence of matter in the
joint could only be ascertained to exist in a very emaciated person.
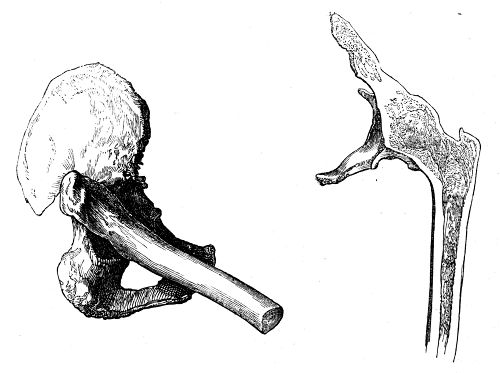
The formation of matter is preceded by great pain, and frequent
startings of the limb during sleep, accompanied with fever, and other
symptoms of severe constitutional disturbance. On the escape of matter
by the natural process from the capsule the painful feelings usually
subside. The abscess may appear, as already stated, near the trochanter
major, or in the back part of the thigh. Matter sometimes makes its way
into the pelvis, through a perforation in the acetabulum, thence it may
fall through the sacro-ischiatic notch into the thigh, and find its
way under the fascia, nearly to the knee; or again, it may present to
the side of the rectum, or even, as I have seen, burst into the bowel
and continue to be discharged thus for a long period. If the treatment
is neglected, abscess succeeds abscess; and in consequence of the
profuse discharge, which may be evacuated from one or many openings
round the joint, the patient is at length exhausted, and sinks. In
some instances the spontaneous cure by anchylosis occurs, as in the
instances from which these sketches are taken. In the one, the head and
neck of the bone had85 been almost entirely destroyed by ulceration,
before anchylosis had begun; in the other, the change is very slight,
but the head of the femur and os innominatum are inseparably united
by bone, and their cancellated texture runs into each other. Or when
the femur has been dislocated, which is a very rare occurrence, the
disease sometimes gradually abates, and a sort of new joint is formed;
the limb, after some time, may thus again become so far useful to the
patient.
In many cases, the appearance which the various parts of the diseased
joint present, are similar to those which have been already described
when treating of affections of the joints generally. Frequently,
however, the osseous tissue in this situation is much more extensively
affected. Often the whole cartilage on the head of the femur is
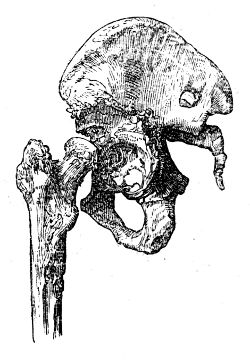 completely removed, exposing the bone in an ulcerated condition; and
when the system has long borne up under the disease, the greater
portion of the head, neck, and even of the trochanter, is destroyed,
the extremity of the bone being completely altered in form, and
composed of a loose and spongy structure. A similar disorganisation
occurs in the acetabulum; the mucous gland is destroyed, the cartilage
is often wholly removed, and the margins of the acetabulum absorbed,
a large and flat ulcerated depression merely being left for the
reception of the diseased femur; in other instances the margins
remain unaffected, whilst the ulceration proceeds in the centre, and
the cavity is thereby much deepened. Not unfrequently the ulceration
proceeds farther, and an aperture is formed in the acetabulum, so that
matter accumulates within the pelvis. The opening is sometimes so large
that the femur is protruded through it. When matter has formed in the
soft parts round the joint, portions of the bones of the pelvis, in
contact with the pus, are ulcerated to a greater or less extent, and
sometimes these ulcers are surrounded by deposits of new bony matter.
completely removed, exposing the bone in an ulcerated condition; and
when the system has long borne up under the disease, the greater
portion of the head, neck, and even of the trochanter, is destroyed,
the extremity of the bone being completely altered in form, and
composed of a loose and spongy structure. A similar disorganisation
occurs in the acetabulum; the mucous gland is destroyed, the cartilage
is often wholly removed, and the margins of the acetabulum absorbed,
a large and flat ulcerated depression merely being left for the
reception of the diseased femur; in other instances the margins
remain unaffected, whilst the ulceration proceeds in the centre, and
the cavity is thereby much deepened. Not unfrequently the ulceration
proceeds farther, and an aperture is formed in the acetabulum, so that
matter accumulates within the pelvis. The opening is sometimes so large
that the femur is protruded through it. When matter has formed in the
soft parts round the joint, portions of the bones of the pelvis, in
contact with the pus, are ulcerated to a greater or less extent, and
sometimes these ulcers are surrounded by deposits of new bony matter.
From such changes in the osseous parts of the articulation the limb
is shortened, sometimes to a great degree, though no dislocation has
occurred. Indeed, dislocation is by no means so frequent a cause of the
shortening as is generally believed.
If the head of the femur has been dislocated, and if the disease in
the joint has afterwards subsided, the acetabulum is found to be much
contracted, with its margins smooth and little elevated, and, if
the patient survive for a number of years, it will be almost wholly
obliterated. But a portion of the dorsum of the ilium, upward and
backward, which is the most frequent dislocation in this disease, is
gradually86 absorbed, so as to form a sort of glenoid cavity for the
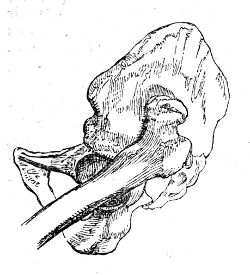 reception of the femur, the extremity of which becomes more solid in
texture, and more smooth on its articular surface. The remaining neck
of the bone is in the sketch here given turned forwards, and must
have given rise to great eversion of the toes. I have seen one other
specimen of this form of luxation. The limb is generally, however,
inverted; and what remains of the head of the bone consequently points
backwards. The consecutive luxation occasionally, also, though rarely,
takes place upon the pubis. Whilst a depression is thus formed, new
bone is sometimes deposited round its margins, whereby the cavity is
increased in depth, so as to resemble somewhat the original acetabulum,
the new deposit having become smooth and of a regular form.
reception of the femur, the extremity of which becomes more solid in
texture, and more smooth on its articular surface. The remaining neck
of the bone is in the sketch here given turned forwards, and must
have given rise to great eversion of the toes. I have seen one other
specimen of this form of luxation. The limb is generally, however,
inverted; and what remains of the head of the bone consequently points
backwards. The consecutive luxation occasionally, also, though rarely,
takes place upon the pubis. Whilst a depression is thus formed, new
bone is sometimes deposited round its margins, whereby the cavity is
increased in depth, so as to resemble somewhat the original acetabulum,
the new deposit having become smooth and of a regular form.
ON CERTAIN ALTERATIONS OF FORM IN THE HEAD AND NECK OF THE THIGH BONE.
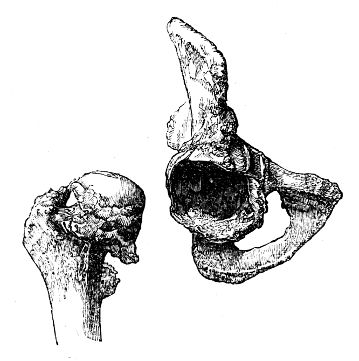
When treating of atrophy of the articular cartilages, it was observed
that, in the latter stages of the disease, the subjacent bone was
liable to become denuded, and its articular extremity more or less
deformed. Now one of the most interesting of these changes occurs in
the head of the thigh bone, which becomes polished on its surface,
flattened87 and expanded, with a corresponding alteration in the
acetabulum. In other cases the head of the thigh bone is somewhat
elongated, and the acetabulum becomes deepened in proportion, by a
deposition of new bone around its margin, as shown in the preceding
 page, frequently to such an extent as to render the removal of the
head of the bone, even after the removal of all the soft parts by
maceration, almost impossible without fracture of the edge of the
socket. The head of the bone may also become still further misshapen,
and anchylosis result; while in some instances the new bony matter
presents in the form of nodosities, sometimes projecting towards the
cavity of the articulation. This cut represents a section of the
upper end of the femur of a labouring man, aged 49, who had fallen on
the trochanter ten years before death, and became gradually lame in
consequence, with shortening of the limb and anchylosis of the joint,
although he had never been confined more than a day or two on account
of the injury.
page, frequently to such an extent as to render the removal of the
head of the bone, even after the removal of all the soft parts by
maceration, almost impossible without fracture of the edge of the
socket. The head of the bone may also become still further misshapen,
and anchylosis result; while in some instances the new bony matter
presents in the form of nodosities, sometimes projecting towards the
cavity of the articulation. This cut represents a section of the
upper end of the femur of a labouring man, aged 49, who had fallen on
the trochanter ten years before death, and became gradually lame in
consequence, with shortening of the limb and anchylosis of the joint,
although he had never been confined more than a day or two on account
of the injury.
But there is another affection in which the femur may be shortened in a
comparatively brief space of time from absorption of the intra-capsular
portion of its neck, generally succeeding to a fall on the trochanter,
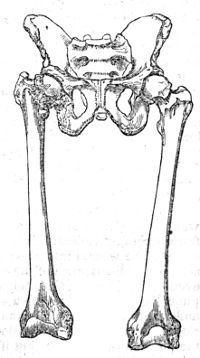 and sometimes occurring in young and middle-aged subjects. In treating
of fractures of the cervix femoris, it will be observed that retraction
of the limb is occasionally delayed for a while: hence the importance
of an accurate knowledge of those cases in which shortening of the
neck of the thigh bone may succeed to an injury short of fracture. The
deficiency of accurate anatomical details concerning such cases led to
a doubt as to their existence; but this question has been completely
put at rest since the history and dissection of two unequivocal
examples by Mr. Gulliver; and the annexed cut represents the changes
of form in the head of the bone, the shortening of the neck and
comparative length of the femora, in a young man from whom these bones
were obtained, and who walked about as many others have done, during
the progress of the disease.
and sometimes occurring in young and middle-aged subjects. In treating
of fractures of the cervix femoris, it will be observed that retraction
of the limb is occasionally delayed for a while: hence the importance
of an accurate knowledge of those cases in which shortening of the
neck of the thigh bone may succeed to an injury short of fracture. The
deficiency of accurate anatomical details concerning such cases led to
a doubt as to their existence; but this question has been completely
put at rest since the history and dissection of two unequivocal
examples by Mr. Gulliver; and the annexed cut represents the changes
of form in the head of the bone, the shortening of the neck and
comparative length of the femora, in a young man from whom these bones
were obtained, and who walked about as many others have done, during
the progress of the disease.
In the above, and in many other cases, the shortening of the neck88 of
the bone is unaccompanied by any absorption of the articular cartilage
of its head. A section of another well marked specimen may be here
added. This bone also exhibits approximation of the head to the shaft,
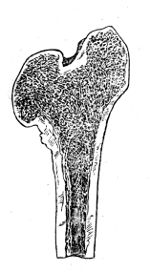 from absorption of the neck. The head is somewhat flattened and
expanded, but the articular cartilage is entire, and of its natural
thickness. The acetabalum was diminished in depth, but enlarged
laterally, so as to correspond with the alteration of shape in the head
of the thigh-bone. The preparation was obtained from a man at 32, who
died at the General Hospital at Chatham of pulmonary consumption, after
a confinement of two years in hospital. Previously to his admission,
he had regularly performed his duty as a light infantry soldier, from
which it is plain that his limbs were then of equal length, although,
when the body was examined, the affected femur was upwards of one inch
and a half shorter than the other. From a careful inquiry after his
death, it appeared that he had, five years previously, fallen on the
trochanter, in consequence of which he often complained of pain in
the hip, but continued to do his duty long after, never having been
confined on account of the accident. It therefore results, that morbid
change had taken place during his long confinement in hospital, a
circumstance not very favourable to the recommendation by some surgeons
of the horizontal posture, as a remedy in such cases, and equally
adverse to the opinion of certain continental pathologists, who inform
us, that shortening of the neck of the femur is to be attributed to the
gradual operation of the superincumbent weight of the body.
from absorption of the neck. The head is somewhat flattened and
expanded, but the articular cartilage is entire, and of its natural
thickness. The acetabalum was diminished in depth, but enlarged
laterally, so as to correspond with the alteration of shape in the head
of the thigh-bone. The preparation was obtained from a man at 32, who
died at the General Hospital at Chatham of pulmonary consumption, after
a confinement of two years in hospital. Previously to his admission,
he had regularly performed his duty as a light infantry soldier, from
which it is plain that his limbs were then of equal length, although,
when the body was examined, the affected femur was upwards of one inch
and a half shorter than the other. From a careful inquiry after his
death, it appeared that he had, five years previously, fallen on the
trochanter, in consequence of which he often complained of pain in
the hip, but continued to do his duty long after, never having been
confined on account of the accident. It therefore results, that morbid
change had taken place during his long confinement in hospital, a
circumstance not very favourable to the recommendation by some surgeons
of the horizontal posture, as a remedy in such cases, and equally
adverse to the opinion of certain continental pathologists, who inform
us, that shortening of the neck of the femur is to be attributed to the
gradual operation of the superincumbent weight of the body.
In old subjects, particularly in fat women, the neck of the femur is
often shortened, and becomes more transverse and brittle than natural,
from a true interstitial absorption or atrophy of the osseous tissue.
This has sometimes been described as a natural effect of age, but it
is undoubtedly disease, for in the greater number of old people the
neck of the thigh-bone presents its usual length and obliquity. The
affection is obviously a very serious one, as predisposing to fracture
of the part, under circumstances which render its reunion almost
hopeless.
Treatment of Affections of the Joints.—After the infliction of
a wound, accidental or not, in order to prevent inflammation of a
joint from becoming violent, it is of the utmost importance to bring
the edges of the wound into close apposition. Sometimes neither
local action, nor disturbance of the constitution, supervene on an
opening, even of considerable size, being made into a joint, while the
slightest puncture often gives rise to the most dreadful symptoms,
both local and general. An incised wound, of no great extent, will be
sufficiently closed by the careful application of adhesive plaster,
and attention to the position of the limb; but if it is extensive
stitches become indispensable. The parts must be kept in a state of
complete relaxation and rest; cold cloths or iced water, allowed to
drop or run over the89 surface by capillary attraction, should be
assiduously applied. The patient’s bowels must be freely opened, and
he is to be kept on low diet. If inflammatory action occur, bleeding,
locally and generally, must be had recourse to energetically,
accompanied with warm fomentations to the parts; and, at the same
time, preparations of antimony, and other saline medicines, are to be
administered internally. If there be reason, from the symptoms, to
suspect the formation of matter, the parts ought to be attentively
examined, in order to detect its presence; and, when discovered to
exist, it must be evacuated without delay. In chronic cases, even local
bleeding to any great extent is inadmissible. In some a few leeches
may be applied, followed by counter-irritation, with advantage. The
employment of counter-irritation is, perhaps, chiefly to be trusted
to in the treatment of those more chronic affections of the joints in
which, from the painful feelings, there is reason to dread disease
of cartilage or bone. Of these, blisters are most in use; though,
from my own experience, I cannot much recommend them. Their constant
repetition is exceedingly annoying, and the slow progress which is
made towards a cure under their use is far from encouraging. Tartrate
of antimony, applied in the form either of ointment or of plaster,
is generally productive of much advantage, in the first instance, by
causing a great degree of superficial irritation, and relieving the
internal parts. After the pustules have been fully developed, its
use is to be discontinued till the surface be nearly whole, when it
is again to be resumed, if the recurrence of painful feelings should
demand it. Caustic issues have been much praised, and are occasionally
beneficial. An eschar is made by the caustic potass applied to the
skin, or by rubbing the bichloride of mercury, or any other caustic,
into scarifications made by the lancet: the slough separates, and pus
is discharged. Instead of promoting a continuation of the discharge, by
applying savine ointment, and inserting foreign bodies, or employing
other irritating dressings, it is better, when the sore begins to heal,
to repeat the application of the caustic to another part; or, when the
issue begins to dry up, to apply for a few hours a pledget of strong
antimonial ointment.
The employment of the bichloride of mercury, though a most efficient
escharotic, appears not to be unattended with danger, as in many
instances violent purging, with tenesmus and bloody stools, follow its
application. When swelling exists without pain, considerable advantage
may be derived from frictions and liniments of various kinds, with
careful bandaging. No applications can be of the least avail unless the
joint be kept completely at rest.
When there is no pain in the joint, when swelling exists, with or
without fluctuation, and there is every reason to believe that the
extremities of the bones are not much diseased, a cure may be, in
general, obtained by the employment of rest, support, and slight
superficial excitement. A practice which has been extensively and
rather indiscriminately pursued in diseases of joints and of other
parts, in affections of synovial membrane, ulceration of cartilage,
disease of bone, and even in cases of necrosis, is here detailed. It
is useful in proper cases, very hurtful in others. The joint is well
washed with90 soap and water, and afterwards rubbed with camphorated
spirits of wine: it is then covered with an ointment spread on lint,
and composed of equal parts of the unguentum hydrargyri cum camphora
and the ceratum saponis—in the majority of cases the mercurial ointment
would be better omitted—strips of lead, soap, or adhesive plaster are
then applied with a moderate degree of tightness round, from two or
three inches below the joint to the same distance above it: these are
covered with soap-plaster spread on thick leather, and the whole is
surrounded with a bandage, which extends from the extremity of the
limb. The bandage should be put on as far as the joint, before the
plasters are applied. The irritation produced on the surface tends
to check the deep-seated action, whilst the compression excites the
action of the absorbents to remove the effused fluids, and thus to
reduce the swelling: by the joint being kept completely motionless,
not the least salutary indication of the treatment, the cartilage and
bones, if ulcerated, are placed in a condition tending much to expedite
their restoration to a natural state. If they are diseased to such an
extent that the process of cicatrisation cannot be expected, a cure by
anchylosis is, by these means, much more likely to occur. The dressings
may be left undisturbed for the space of a week or two; at which
period, and, in many cases, sooner, they will be found much slackened,
in consequence of the swelling being greatly reduced. By repetition
of the application at intervals, the disease will, in a great many
instances, rapidly cease, and the joint resume almost its natural
appearance; but the period at which this takes place will be found
to vary much according to circumstances. If, however, the plasters
produce such irritation as to cause a return of inflammatory action,
their use must be discontinued till such action has been subdued by
the usual means. If the thickening of the external parts has occurred
to such an extent as to cause immobility of the joint, or if partial
anchylosis has ensued, the limb may be brought to the most convenient
position, the knee nearly, but not quite, straight, the elbow half
bent, and so on, by the cautious use of a jointed splint, fitted with
an extending screw. The practitioner is not to be deterred from having
recourse to the above practice, even when matter has collected and
burst externally, for sometimes under its employment the cavities of
abscesses contract rapidly. After the swelling and other symptoms of
disease have subsided, the joint is to be slightly moved, but with
great care; and, by a gradual increase of the movement, the natural
motion of the part may be ultimately restored. The great object in
treating chronic affections of joints must be to give them support, and
prevent motion as much as possible. This is effected pretty well in the
articulations, removed from the trunk, by the process above described,
modified according to circumstances. The filth and smell arising from
the plasters often becomes annoying, and, above all, the eruptions and
excoriations produced by them prove so troublesome that the application
requires to be discontinued. The principal and most essential
indication, that of securing repose to the affected parts, is fully
as well obtained by the application of well-adjusted splints. These
may be formed of lint soaked in a mucilage of gum acacia, as described
in the Practical Surgery, p. 150,91 or coarse linen may be smeared
over thickly with a coating of mucilage mixed with common whiting,
and another layer of linen spread over that. This is laid out smooth
and allowed to dry; portions of this sheet are cut to the form of the
affected joint, and, after being moistened, are applied and retained
by a roller. A firm case is thus formed, which may be afterwards lined
with lint or cotton wadding, and so reapplied. The most suitable
splints of all are made of leather, prepared without oil, softened
in warm water, and put on as above described. They are, when they
have become dry, pared and well fitted, then lined with wash-leather,
and padded as may be required. The employment of these splints gives
great relief in cases where further excited action has been lighted
up in the joint in consequence of the surface of the articulating
cartilage having become ulcerated from its free or attached surfaces,
or in consequence of matter finding its way into the synovial cavity
from the cancelli in the head of the bone. In cases, also, where the
painful sensations have existed from the first, and even before any
great alteration in the external form of the joint has taken place,
indicating primary ulceration of cartilage, this practice affords
immediate relief. These splints are easily applicable to the shoulder
or hip-joints; and, in the majority of instances, nothing further
requires to be done. It appears that Dr. Physick of Philadelphia had
been for many years in the habit of confining the motions of the
hip-joint by means of hollowed wooden splints, and his practice was
marked by very favourable results.9
92
It is seldom that local abstraction of blood is at all required, and
its employment in cases of morbus coxarius in weak constitutions,
which it generally seizes upon, is very questionable. Neither is
counter-irritation called for; and it is only in extreme cases, when
the suffering is intense, that small blisters over the fore part of the
joint, or a slight drain in that situation, or behind the trochanter,
is admissible. The nitrate of silver rubbed on the surface causes
vesication and discharge; and its early repetition is often followed
by good effects. The tincture of iodine, or a liniment containing
sulphuric acid, may sometimes be applied with the same view. There
is no doubt whatever, that much of the benefit that attends upon
counter-irritation, both in the human body and in the lower animals,
is to be attributed to the rest that is at the same time enjoined,
and often indispensable. It is thus that the firing and blistering
of horses does good in the majority of the diseases of tendons,
bursæ, bones, and joints. In some instances, it may be necessary to
have recourse to soothing applications, as fomentations to affected
joints, and to employ general antiphlogistic means suited to the age,
strength, and constitution of the patient. In the greater number of
cases in young subjects, after the stomach and bowels are unloaded, the
system must be supported by tonics and nutritious food; none are more
beneficial than the preparations of iron.
When the occurrence of anchylosis affords the only hope, this process
ought to be encouraged by rest, and the limb at the same time kept in
that position which will be most useful in after life; this will be
effected here also by the employment of splints.
In cases of disease of the knee, ankle, elbow, or wrist joints,
notwithstanding everything that can be done, the disease often runs its
course, abscesses form and give way, the patient’s health declines,
and he becomes emaciated and hectic. In such cases amputation, when
not contraindicated by internal disease, must be had recourse to, as
the only remedy. In some few instances, the excision of the diseased
extremities of the bones may supersede this operation; but 93this will
be discussed in a future part of the work. Every circumstance must be
well weighed before mutilation be resorted to; and there can be little
doubt that thousands of limbs have been saved by the employment of
the means above mentioned, which would have been otherwise doomed to
amputation.
Hydrops articuli will in general be got rid of by the use of friction,
either dry or with liniments; by stimulating plasters or by blisters;
and by the proper application of bandages. Mercurial ointments are used
in this affection, and often with very great benefit. Electricity has
been recommended.10
In neuralgic affections of joints, it is clear that the symptoms are
to be combated by general and not by local means, at least of a severe
nature. The patient must be amused and occupied, exercise in the open
air must be enjoined, and attention paid to diet. The state of the
digestive organs and secretions should be looked to, and corrected if
need be. Medicines directed to the regulation of the functions of the
uterus are essential in the majority of cases. When there is reason to
suspect the lodgement of sordes or worms in the intestinal canal of
children so affected, the balsam of copaiba, in doses of Ʒss., or
more, on an empty stomach, followed, if need be, by brisk purgatives,
will be found to answer admirably. Tonics, such as preparations of
iron, of quina, &c., are then given with advantage: many apparently bad
cases yield at once to such treatment.
As local applications, anodynes, fomentations, or cold lotions are
employed, according to circumstances. Frictions with gently stimulating
liniments, belladonna, veratria, &c., may be used as occasion
demands. The patient must be encouraged to use the affected limb as
much as possible; and the use of all severe and heroic remedies, as
bleeding, blistering, counter-irritation, setons, issues, or moxas,
discountenanced.
94
OF INFLAMMATION OF BONE, AND DISEASES THENCE ARISING.
Bones grow and are nourished by the same means, and are subject to
the same laws, with other parts of the system. Like all the tissues
of a white colour, particularly when their growth is completed, they
are less freely supplied with bloodvessels and nerves than other
parts. When incited action of the bloodvessels occurs in the harder
textures, sensibility is roused to an exquisite degree, and the healthy
and perverted processes often advance with great vigour and amazing
rapidity.
Inflammation of bone often arises from external injury, and in some
constitutions from very slight causes. Its occurrence is supposed to
be favoured by a syphilitic taint, but the inflammatory disposition
is much more frequently produced in a system vitiated by the abuse of
mercury. From the unyielding nature of the tissue, the pain attendant
on inflammatory action is dreadfully excruciating; it is also most
violent during the night, even in chronic cases, a circumstance which
does not admit of satisfactory explanation. The integuments over the
inflamed bone are swollen, and the tumour is œdematous; whilst a hard
and solid tumefaction exists in the more deeply-seated parts, caused
partly by enlargement of the osseous tissue and partly by effusion of
lymph into the cellular substance. The bone is imbedded in a gelatinous
or lymphatic effusion, situated mostly beneath the periosteum. This
membrane is more vascular than in its natural condition, thickened,
 and at the same time opened out in texture. The bloodvessels of the
affected bone are much increased, both in activity and in size; and,
in consequence of enlargement of the vessels, and thickening of the
naturally delicate membrane on which the vessels ramify, the bone is
swollen and increased in size; its texture, as shown in the annexed
cut, is loose, somewhat resembling the cancellated structure, and
its surface is occupied by numerous foramina, which are enlarged in
proportion to the size of the vessels which they contain. The limb is
often enormously swollen and indurated. The gelatinous effusion beneath
the periosteum speedily becomes organised, nodules of osseous matter
project into it, and adhere to the surface of the bone frequently by
a narrow neck; these increase in number, gradually assume a solid
appearance: the bone is thus thickened, often to a very great extent.
and at the same time opened out in texture. The bloodvessels of the
affected bone are much increased, both in activity and in size; and,
in consequence of enlargement of the vessels, and thickening of the
naturally delicate membrane on which the vessels ramify, the bone is
swollen and increased in size; its texture, as shown in the annexed
cut, is loose, somewhat resembling the cancellated structure, and
its surface is occupied by numerous foramina, which are enlarged in
proportion to the size of the vessels which they contain. The limb is
often enormously swollen and indurated. The gelatinous effusion beneath
the periosteum speedily becomes organised, nodules of osseous matter
project into it, and adhere to the surface of the bone frequently by
a narrow neck; these increase in number, gradually assume a solid
appearance: the bone is thus thickened, often to a very great extent.
It has been supposed that the new osseous matter is deposited by the
vessels of the soft parts and of the periosteum; but there can be
little doubt but that it is secreted principally by the vessels which
ramify within the substance of the bone, and by the vessels of the
periosteum after they have entered the osseous tissue. Thus, in the95
case of fracture, the new osseous particles lie between the periosteum
and bone at a distance from the broken ends, where the vessels are
enlarged and increased in activity, or adhere to fragments which have
been detached in part and retain their vitality, but not to the under
surface of the periosteum. There is no doubt that thin laminæ of bone
are now and then found attached to the periosteum, or impacted within
its substance; but this is to be attributed to that morbid action of
the tissue, to which this as well as several other membranes is subject.
When bone is extensively affected with inflammation, motion is
impaired; the muscles being displaced and retarded in their action by
the swelling and irregularity of the bone, by effusion of lymph into
their tissue and intermuscular spaces, and, perhaps, also, by their
partaking, in some measure, of the inflammatory action. Any attempt
to move the parts very much aggravates the patient’s suffering.
Occasionally inflammation attacks almost all the bones in the body,
and causes great constitutional disturbance, by exhausting the powers
of life: it sometimes terminates fatally. Bones become inflamed from
various causes. However it originates, the action ends, as in the other
tissues, in resolution, suppuration, or mortification. The effusion
by which the diseased vessels naturally relieve themselves in softer
textures cannot here take place so readily, or to such an extent as
to prove beneficial: the intensity of the action is with difficulty
subdued, and, consequently, resolution is comparatively rare. When it
does occur, the parts do not soon regain their natural condition, but
often remain considerably swollen and indurated, as is seen in nodes,
which continue during the life of the patient, without causing pain or
much inconvenience.
Suppuration on the surface, or in the centre, and partial or total
death of a portion of bone are the most frequent consequences of
external injury and incited vascular action; but suppuration in the
cancellated texture frequently follows very slight incited action
in those of a scrofulous habit. Tubercular matter exists, in all
probability, previously, and it leads very often to long continued
disease, curable only by operation. The matter may find its way to the
surface after long suffering and great constitutional disturbance.
Again, it may be confined for months, or even years, the patient
suffering from time to time the most excruciating agony. The bone
becomes thickened towards the surface by new deposit, as the cavity
is increased by ulcerative absorption, and relief is only afforded, a
correct diagnosis having been formed, by artificial evacuation of the
matter. In many cases small sequestra lie in the cavity; and though
the matter escapes naturally, or is evacuated, the patient’s strength
becomes worn out, and he perishes, unless the limb is removed. So
long as dead portions of bone remain, the discharge cannot cease
permanently. Fresh collections are apt to form in the soft parts if
the original openings close. It is no easy matter to discover or
remove sequestra from deeply seated bones. A section of the femur is
represented on the next page, showing a cloaca leading to the cavity
of an abscess in the medullary canal. The bone is very dense in
consistence, and irregular on its surface.
96
SUPPURATION IN BONE
Suppuration in bones is necessarily connected with loss of substance,
and condensation of the surrounding parts; and purulent collections
exteriorly, if allowed to press long, or if bound down by unyielding
sheaths, will sooner or later produce a breach of continuity, by
 causing absorption of the outer lamella and the subjacent cancellated
texture. A similar effect is produced by aneurismal and some other
tumours. Such loss of substance is, in some instances, speedily
repaired, after removal of the cause, by effusion of new matter
from the surrounding bloodvessels of the bone; thus, in disease in
consequence of pressure from large aneurism, there is reason to suppose
that the healing process commences as soon as the aneurismal sac begins
to diminish, as after operation. But, as has been already observed,
the healthy actions are more vigorous in the softer tissues than in
bone; and when ulceration has occurred in the latter, it is generally
attended with weak action, and presents the same general characters
as an ulcer in the soft parts, connected with a feeble action of the
bloodvessels; the discharge is thin and fetid, absorption gradually
proceeds, and there is little or no effort towards reparation.
Cavities in bones are necessarily slower in healing than those in
the soft parts; the vitality and power of reparation are lower; and
there being no elasticity in the parts, the walls cannot come rapidly
together, contract and coalesce. It may tend to prevent confusion of
the two different morbid states, if we confine the term ulceration to
suppuration in, and absorption of, bone, whilst the vessels retain
a considerable power of action, throw out new matter, and procure a
reparation of the breach; and this condition of the osseous tissue
exists when the disease is situated in the surface of the bone, and
when it has been produced by an external cause. On the contrary, the
term caries will denote that peculiar kind of ulceration in which
reparation is hardly attempted by nature, and is with difficulty
obtained by the most active interference; and this disease will most
generally be found to affect the cancellated structure. The comparative
frequency of one or other of the terminations of inflammation depends
much on the kind of bone implicated.
causing absorption of the outer lamella and the subjacent cancellated
texture. A similar effect is produced by aneurismal and some other
tumours. Such loss of substance is, in some instances, speedily
repaired, after removal of the cause, by effusion of new matter
from the surrounding bloodvessels of the bone; thus, in disease in
consequence of pressure from large aneurism, there is reason to suppose
that the healing process commences as soon as the aneurismal sac begins
to diminish, as after operation. But, as has been already observed,
the healthy actions are more vigorous in the softer tissues than in
bone; and when ulceration has occurred in the latter, it is generally
attended with weak action, and presents the same general characters
as an ulcer in the soft parts, connected with a feeble action of the
bloodvessels; the discharge is thin and fetid, absorption gradually
proceeds, and there is little or no effort towards reparation.
Cavities in bones are necessarily slower in healing than those in
the soft parts; the vitality and power of reparation are lower; and
there being no elasticity in the parts, the walls cannot come rapidly
together, contract and coalesce. It may tend to prevent confusion of
the two different morbid states, if we confine the term ulceration to
suppuration in, and absorption of, bone, whilst the vessels retain
a considerable power of action, throw out new matter, and procure a
reparation of the breach; and this condition of the osseous tissue
exists when the disease is situated in the surface of the bone, and
when it has been produced by an external cause. On the contrary, the
term caries will denote that peculiar kind of ulceration in which
reparation is hardly attempted by nature, and is with difficulty
obtained by the most active interference; and this disease will most
generally be found to affect the cancellated structure. The comparative
frequency of one or other of the terminations of inflammation depends
much on the kind of bone implicated.
CARIES
Caries most frequently occurs in the heads of long and in the
cancellated structure of the short bones, as unhealthy suppuration most
frequently takes place in the loose, fatty, and cellular tissues of
the soft parts. The formation of abscess in the cancelli is generally
preceded by deposit of tubercular matter, isolated or collected in
masses, and by the softening of this cheesy substance. When pus has
formed in the substance of a bone, the outer lamella, in the end,
becomes absorbed, and the effusion undermines the periosteum, which,
from the distension, also ulcerates: the matter then spreads into the
neighbouring cellular tissue, or makes its way to the surface, and is
evacuated, or, what is still worse, it escapes into an97 articulation.
The discharge is often continued, as already stated, in consequence
of a dead portion of the cancellated structure being imbedded either
in the carious cavity, or in the soft parts, where they sometimes are
lodged for a long period.
It was formerly remarked that bones become highly sensible from incited
action; hence, during the progress of this disease, which is attended
with more or less inflammation, the patient generally suffers most
excruciating agony—so great, in general, as to prevent him, perhaps
for weeks, from enjoying the least repose. The affected part is
considerably swollen, but the enlargement is seldom so general, or so
great as in the diseased state of the ligaments and other apparatus
of a joint. White swelling, however, may be the precursor of caries;
or, in other words, a disease commencing in the bursæ, ligaments,
synovial membrane, or cartilage, may extend to the bone; and breach
of continuity, attended with weak action, be the consequence. In
caries the affected portion appears neither to possess vitality enough
to enable it to repair the breach, nor to be sufficiently deprived
of vitality to be thrown off by the surrounding parts. Considerable
portions of dead bone are occasionally found in carious cavities, in
the heads of bones, and even in the vertebral column. Small portions
are also detached piecemeal in the progress of ulceration, and
discharged; but it is seldom that the whole surface is thrown off, so
as to give place to a healthy and reparative action. When the parietes
of the cavity have remained a considerable time in this inactive state,
the surrounding vessels become more active, and the surface of the
bone in the vicinity is studded with nodules of new osseous matter.
The disease here delineated affected only a small portion of the
cancellated texture of the condyle. An ashy looking substance fills the
cavity, and this again was concealed in the recent state by lardaceous
 matter. The elbow joint is unaffected, excepting only that, from the
deposit of new bone in spiculæ and nodules, and the condensation of
the soft parts, almost complete anchylosis had taken place. This
deposit is not always limited to the affected bone, if one only be the
seat of the disease, but frequently extends to those articulated with
it. The soft parts are commonly more or less thickened, and rendered
exceedingly dense by effusion of lymph into the cellular texture; and
so great is this thickening sometimes, that the knife is resisted as
if by cartilage. The discharge which proceeds from the carious part is
generally highly fetid, very profuse, is often poured through several
openings, and the surrounding skin is excoriated and generally of a
livid colour. The ichorous discharge occasionally dries up for a short
period and again breaks out more violently. The surface of the ulcer
is, in some cases, occupied by soft unhealthy granulations; in others
the earthy part of the bone is most prominent. When the parts have been
macerated and dried, the disease is often found to have proceeded more
in width98 than in depth, and the absorption has not reduced all points
of the diseased surface to the same level, thin portions remaining
somewhat elevated, and giving the part a cancellated appearance; and
there often project numerous minute osseous fibrillæ of considerable
length, which intermix with one another, and form a most delicate
network. In other instances, the ulceration has extended more deeply
and uniformly, and a considerable cavity is formed, with irregular
margins and surface; not unfrequently it contains dead portions of the
cancellated structure, in some of a dark, in others of a light colour;
or it is occupied, in the recent state, by a substance resembling
lard. The surrounding bone is much softened, and, after maceration,
becomes exceedingly light. The disease is generally confined to one or
two bones, but occasionally involves a whole chain. It may be limited
to a part of one bone in a joint, or may embrace the whole of it. Its
extent will depend on the severity of the primary action, or on the
degree and duration of the pressure of fluid which has been allowed to
exist, whether from the nature of the superincumbent texture or the
carelessness of the surgeon.
matter. The elbow joint is unaffected, excepting only that, from the
deposit of new bone in spiculæ and nodules, and the condensation of
the soft parts, almost complete anchylosis had taken place. This
deposit is not always limited to the affected bone, if one only be the
seat of the disease, but frequently extends to those articulated with
it. The soft parts are commonly more or less thickened, and rendered
exceedingly dense by effusion of lymph into the cellular texture; and
so great is this thickening sometimes, that the knife is resisted as
if by cartilage. The discharge which proceeds from the carious part is
generally highly fetid, very profuse, is often poured through several
openings, and the surrounding skin is excoriated and generally of a
livid colour. The ichorous discharge occasionally dries up for a short
period and again breaks out more violently. The surface of the ulcer
is, in some cases, occupied by soft unhealthy granulations; in others
the earthy part of the bone is most prominent. When the parts have been
macerated and dried, the disease is often found to have proceeded more
in width98 than in depth, and the absorption has not reduced all points
of the diseased surface to the same level, thin portions remaining
somewhat elevated, and giving the part a cancellated appearance; and
there often project numerous minute osseous fibrillæ of considerable
length, which intermix with one another, and form a most delicate
network. In other instances, the ulceration has extended more deeply
and uniformly, and a considerable cavity is formed, with irregular
margins and surface; not unfrequently it contains dead portions of the
cancellated structure, in some of a dark, in others of a light colour;
or it is occupied, in the recent state, by a substance resembling
lard. The surrounding bone is much softened, and, after maceration,
becomes exceedingly light. The disease is generally confined to one or
two bones, but occasionally involves a whole chain. It may be limited
to a part of one bone in a joint, or may embrace the whole of it. Its
extent will depend on the severity of the primary action, or on the
degree and duration of the pressure of fluid which has been allowed to
exist, whether from the nature of the superincumbent texture or the
carelessness of the surgeon.
Interstitial absorption of those bones which are in the neighbourhood
of the carious ulceration often occurs in the tarsus and carpus. The
superincumbent integuments are livid and cold, and pain is felt in
the situation of the bones; yet they are not affected with continuous
ulceration, but portions of their substance are gradually removed
by absorption, so that they are much loosened in texture, and may
be altogether destroyed, or come to consist merely of a thin and
reticulated osseous shell, whilst at the same time their cartilaginous
surfaces often remain in their healthy condition.
The constitutional disorder attendant on caries is at first very great;
the sympathetic fever is followed by hectic, under which, and the
discharge, many patients sink. The general affection in some degree
keeps pace with the local in violence and duration. The irritation is
in some cases so great as to destroy the patient in a very few months
or weeks; but not unfrequently a constitution, by no means strong, will
be enabled to bear up for a long period under very extensive disease of
a bone. The paroxysms of pain and inflammation occasion fresh attacks
of constitutional derangement: this occurs till the patient’s health
and strength are exhausted, and he sinks under the disease, or is
relieved by the spontaneous or artificial removal of the cause.
A natural cure of caries may occur in consequence of the diseased
parts so far recovering their natural degree of vascular action as to
form granulations and repair the breach; but most frequently it is
necessary, for the accomplishment of this purpose, that incited action
occur to a very considerable degree; and the diseased parts, already
extremely weak, have not sufficient power to withstand the action, but
perish; whilst the action of the surrounding parts, not being increased
to such a degree as to overcome their powers, throws off the dead,
secretes a more bland discharge, and deposits healthy granulations,
which gradually fill up the cavity.
Treatment.—In inflammation of bone, resolution must be brought
about, if possible; the other terminations are to be prevented by all99
possible means, since they frequently endanger the limb, and even the
life, of the patient, and, at best, never admit of a speedy cure. To
promote resolution, blood must be drawn copiously from the part; and
general bleeding may also be required, though in some constitutions it
cannot be safely carried to any great extent. After local bleeding,
fomentations assiduously applied will tend much to relieve the
sufferings of the patient. Purgatives, nauseating doses of antimony,
and all safe measures likely to subdue the vascular action, must at the
same time be adopted. Free incisions through the periosteum sometimes
relieve the pain, and cut short the disease, the distended vessels
being thereby emptied; but such practice is only a last resource, when
the action has resisted all other means, and threatens an unfavourable
termination. If, notwithstanding the resolutive means employed, the
inflammation proceeds unabated, and suppuration occurs, the effused
pus ought never to be allowed to remain on the surface of the bone,
but must be evacuated by early incision. Otherwise the pressure of
the extraneous fluid will cause absorption of the bone, or detachment
of periosteum and superficial necrosis; the absorbed surface will,
in its turn, secrete pus, and thus an ulcer will be produced; and,
from the vascular action becoming debilitated in consequence of the
previous incitation, that ulcer will in all probability degenerate into
caries. Much mischief is produced by squeezing and bandaging tightly
the inflamed parts, as can readily be understood; yet such practice is
frequently adopted after suppuration. By it the inflammatory action
is excited anew, the formation of matter is very much increased, and
however useful such manipulation may be in stiffness of a joint, or
mere swelling of bursæ, and sheaths of tendons, still, in inflammation
and abscess of bones or joints it is extremely prejudicial, and from
its indiscriminate employment by those ignorant of the profession,
many limbs have been destroyed. General chronic periostitis, which
is produced by exposure to cold, or occurs after or during mercurial
courses, and is often supposed to be a symptom of syphilis, is relieved
by the internal exhibition of the bichloride of mercury, or other
mercurial preparations, combined with sarsaparilla and diaphoretics.
In many instances such an affection will yield to no other treatment;
and thus the practitioner is occasionally obliged to have recourse to
a somewhat paradoxical practice, that of giving mercury for a disease
which seems to have been produced by that mineral.
In inflammation of the short bones or heads of the long bones, if
the action does not yield to topical bleeding and becomes chronic,
counter-irritants must be employed. Blisters repeated are often useful
in subduing the remaining action, and in obstinate cases small caustic
issues are sometimes of service. During the adhesion of the eschar, the
best application is a common poultice or water dressing, which, on the
separation of the dead part, may be exchanged for any simple ointment,
it not being at all desirable in general to check the discharge and
heal up the breach of surface. Moxa is sometimes employed to make an
issue in these and other cases, but it is not superior in any respect
to the potential cautery, whilst its employment is generally very
alarming to the patient. The sores following the use of100 the moxa are
in some instances tedious in healing; and this may be ascribed to
the vitality of the surrounding parts having been diminished by the
application.
In cases of atrophy of bone, and where there is reason to suspect
the scrofulous or tubercular deposit to be going on, the affected
part should not be much used, and means taken to give tone to the
system. Preparations of iron are often exhibited with advantage. The
combination of iodine with iron may sometimes answer. Abscesses should
be opened early, so as to prevent extension of the mischief. In abscess
in the shafts of the long bones, it is occasionally necessary to make
an opening through the outer lamella by the trephine, so as to evacuate
its contents. Some instructive cases have been given by Sir B. Brodie,
illustrative of the good effects of this practice. I subjoin one out of
many from my own hospital practice.
“W. A., aged 22, was admitted Oct. 26, 1837, under the care of Mr.
Liston. He is a policeman of weak conformation. He states that when
about six or seven years of age he was first attacked with an aching
pain in the right leg, near its middle, and since that period has
been subject to three or four attacks every year. These usually were
experienced in the spring, during rough, windy, and cold weather, and
continued from one to three weeks. The pain was always aggravated at
night, and so trifling in the day that he was always able to go about.
These attacks ceased to occur when he was between 15 and 16 years of
age, and since that time, until last May, he has been free from them.
He states that up to about his 16th year the bone of the leg gradually
enlarged in its middle portion, but then became stationary, and at
the period of entering the police the difference between the bones of
both legs was not great; this was about two years ago. Since then he
has been accustomed to walk for a considerable length of time daily.
During some months he was obliged to do the night work, and then he
was much exposed to cold and wet. Last May, while thus engaged, he
experienced again an aching pain in the middle of the right tibia; this
was aggravated at night; and after a fortnight’s duration, during which
it became gradually worse, he was obliged to give up his duties in
the police, being unable to continue them any longer. At this time he
consulted the surgeon of the subdivision with which he was connected;
his treatment was fomentations to the leg and aperient medicine
occasionally. Not being much relieved by this, he afterwards ordered
the application of leeches on three several occasions, and mercury to
salivation. At the end of three weeks he returned to his duty. In the
latter part of September he was again attacked with pain during night
duty; this pain increased rapidly in severity, and after three nights
he was again obliged to leave duty. He was now treated again with the
frequent and copious application of leeches at different intervals,
and likewise took some pills, which did not affect his mouth. This
treatment, with frequent fomentations, was persevered in for a month,
but without permanent benefit, and then he was brought to this
hospital. Has never had any syphilitic complaint.
“Present state.—Has an enlargement of the tibia about its middle
third, of a diffused character, and which seems to extend a good
deal101 inwards and backwards; in this part he experiences a throbbing
and lancinating pain at night; during the day he is in general easy;
at night there is considerable heat and swelling in the leg; tongue
whitish; appetite good. The following pills were ordered:—℞.
Bichloride of mercury, two grains; powder of gum guiacum, two scruples;
oil of sassafras, ten minims; extract of sarsaparilla, four scruples.
To be divided into twenty-four pills, of which let two be taken three
times a day. Apply eighteen leeches to the affected part.
“Nov. 4. The leeches were repeated; much the same.
“8. Symptoms as before. As he complains of pain over the eyebrow, with
nausea, let the mercury be left off. A variety of constitutional and
local treatment has been pursued during Mr. Liston’s absence from the
hospital, but without affording any relief; the patient’s nights were
passed in great agony, and his general health began to suffer. On the
27th, after consultation with Mr. Fisher, the surgeon to the Police
Force, Mr. Liston had the patient carried into the operating theatre.
He made an incision along the spine of the tibia of about three inches
in extent; another shorter one was made to fall on this at right
angles from the inner side. The surface of the bone thus exposed was
perforated to the depth of fully half an inch by a small trephine. A
very dense circle was removed from the perforation; still the fluid,
which was suspected to exist, did not appear. Mr. Liston, encouraged by
the intense pain complained of as the process of perforation proceeded,
again applied the crown of the instrument, and after a few more turns,
brought out a further circle of considerable thickness, and this was
forthwith followed by a flow of well-digested purulent matter.
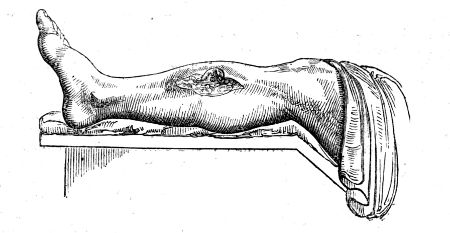
“28. Complains of no pain comparatively; slept well last night after
an anodyne draught; has felt much relieved since the operation; a
good deal of matter was discharged from the sore during the night;
water-dressing to be applied to the wound.
“30. Slept well without any anodyne the last two nights. The relief
afforded by the operation is felt more now than it was at first.102 The
wound discharges a good deal. A tonic mixture, containing infusion of
gentian, sulphate of magnesia, and sulphuric acid, was ordered.
“Dec. 2. The wound looks florid and clean; granulations are springing
up; general health very much improved.
“4. The edges of the wound are thickened by the granulations; the
discharge from the wound still considerable; feels quite well in health.
“12. The wound continues much the same; the rollers have been
discontinued.
“14. Feels himself gaining strength daily; can walk without pain; wound
is contracting and hard; granulations seem to lessen the depth of the
opening in the bone; there appears to be no sequestrum.”
When caries is fairly established, and the integuments have given
way, the best and most successful proceeding is that pointed out by
nature—destruction of the diseased portion; and the means must vary
according to the particular circumstances. In many cases, nature seems
to wait but for the separation of the sickly parts, either by accident,
or by the interference of art. The means are to remove, partially or
wholly, the diseased part, or to effect such a change of action as will
throw it off. The first indication will be accomplished by trephines,
scoops, saws, and forceps; the second by active escharotics; frequently
both are required.
If there be extensive disease in the medullary canal of a bone, several
perforations may require to be made, and these may be connected by the
use of a small saw, or the cutting forceps. The diseased cancelli, thus
exposed, can be readily removed by the scoop or graver, as recommended
by Mr. Hey, primus, in his excellent work. If, with the probe, it
is ascertained that a portion of the cancellated texture has become
dead and loose, it is to be removed after dilatation of the external
opening. It may frequently be difficult to distinguish in the effused
blood, between what is diseased and what is not; it will often be
necessary afterwards to cauterise freely the exposed surface, and
for this purpose the oxidum hydrargyri rubrum ought generally to be
preferred. The slough will soon be thrown off, and healthy granulations
fill up the breach. The application of the actual cautery may be by
some considered necessary: at one time I employed this remedy very
extensively in caries, and occasionally with very good success; I have
since, however, been led to change my opinion, and am now inclined to
prefer the potential cautery already mentioned. By the application of
the red-hot iron, the diseased portion is destroyed effectually, but
at the same time the vitality of the surrounding parts is often very
much weakened and their power of reparation diminished, so that they
are incapable of assuming a sufficient degree of action for throwing
off the dead part; their action being increased whilst their power is
diminished, they may become affected with caries, and thus, instead
of being arrested, the original disease will either be increased,
or extensive necrosis may take place. The red oxide of mercury is
not calculated to produce such bad effects; it does not spread or
insinuate itself into the bony tissue,103 as liquid caustics are apt to
do; and it is sufficiently powerful for complete destruction of the
diseased parts. It will be necessary to keep the wound open, by proper
dressings, till all the dead portions of bone be discharged, and every
part of the parietes of the cavity produce healthy granulations: if
the discharge be offensive, its fetor may be corrected by the use
of spirituous applications, such as the tinctures of myrrh, opium,
or aloes, separately or combined. After healthy granulations have
appeared, and the cavity has begun to contract, light dressing is all
that is necessary.
In operating on the carpal and tarsal bones for removal of caries, the
surgeon must be well acquainted with the connexions and relations of
the parts. If one bone is diseased, its removal will be sufficient; if
several, the operation becomes more painful and difficult. When one
only of the tarsal or carpal bones is almost completely destroyed,
and the surfaces of those articulated with it are also more or less
affected, it is not sufficient or safe merely to remove the loosely
attached portions of the one primarily attacked; the diseased parts
of those surrounding it must also be taken away, and it will often be
necessary to apply the caustic afterwards. In caries of the distal
range of bones, the bases of those supported by them are in general
involved, and must also be removed. If one only is diseased, with the
base of the metacarpal or metatarsal bone attached to it, the removal
of these will be enough, and can be accomplished without difficulty.
Some have recommended the total extirpation of a metacarpal or
metatarsal bone, leaving the finger or toe appended; but the member,
when thus left unsupported, can never become of any service to the
patient, and may be productive of much inconvenience; whilst removal
of them, along with the diseased bone, renders the operation much more
easy of execution. If the whole disease can be extirpated, leaving the
surfaces of the surrounding bones covered with healthy cartilage, the
use of the caustic is not required, and would be productive of harm;
but wherever it is impossible to avoid encroaching on the cancellated
texture, such as of the os calcis, which it would be unsafe or
imprudent to take away entirely, its use is then indispensable. After
the removal of carious bones, the symptoms soon disappear, and the
patient obtains a rapid, and often permanent cure. The instruments for
these operations, and the method of performing them, will be afterwards
mentioned. In conclusion, it may be remarked that the temporary
cicatrix of a sore leading to a diseased bone has a very different
appearance from the sound scar which is formed after its removal. The
former is bluish, soft, on a level with the surrounding parts, and
moveable; the latter is depressed, white, and firmly adherent to the
bone.
NECROSIS
Death of bone, or Necrosis, is an effect of violent inflammation,
particularly of the medullary web, or external injury; a termination of
inflammatory action in bone corresponding to sphacelation in the softer
tissues. It has been observed, that the bones are not extensively
supplied with bloodvessels, and that their natural powers are inferior
to those of the softer parts; and from this circumstance the frequency
of necrosis can be readily accounted for. The short bones104 and the
heads of the long bones, are more vascular than the flattened bones
and the shafts of the long ones. Hence necrosis most frequently occurs
in the latter. Necrosis, fortunately, seldom occurs in the heads of
the long bones, or penetrates the separation betwixt the cancelli of
the shaft and the epiphysis. Bits of dead bone in the articular ends,
however, very often lead to disease in the joint. There are in my
private collection a few specimens of necrosis, in which matter found
its way into the neighbouring joint, leading to disease of the tissues
composing it, and rendering amputation necessary for the preservation
of the patient’s existence. External injury may produce this disease
by causing a violent increase of action, or it may be so severe as at
once to deprive part of the bone of its vitality. Destruction of the
periosteum, and of the vessels which enter the surface of the bone,
frequently gives rise to superficial necrosis or exfoliation. Such a
result, however, does not always follow; for we not unfrequently find,
when the periosteum has been forcibly torn off, to a considerable
extent, by external injury, that the part still retains its vitality.
When, however, the bone has been at the same time contused, it is
extremely probable that external necrosis may occur. Again, when the
periosteum has been removed in the most careful manner possible,
exfoliation occasionally takes place. If the exposed bone remain of a
brownish hue, it will generally retain its vigour; if, on the other
hand, the colour is white, it will most probably be cast off. Necrosis
may come on at various periods of life, but is most commonly met with
in young subjects, in whom the inflammatory action is allowed to
make progress before it is noticed or attended to. It may affect the
external or the internal part of a bone, or nearly its whole thickness.
The whole of a bone seldom or ever dies in consequence of increased
action, and it is not often that the entire thickness of any part of
it is found to be necrosed. If the entire thickness dies to a great
extent, there is no reproduction; the epiphyses approximate, and the
limb, if there is only a single bone, must be lost. A large portion
of a bone, or numerous small irregular portions, may die; but still a
part of the original shaft remains, and by its vessels reproduction is
accomplished. The articulating extremity is very rarely destroyed by
this disease. Many writers have talked of death of a bone throughout
its whole extent, and, in fact, the term necrosis was originally
adopted on this supposition.

The progress of necrosis is, as has been said, similar to that of
sphacelation. The affected bone gradually changes its colour, and
loses its sensibility; a line of demarcation is formed, and ultimately
the dead portion is completely detached from the living. Previous
to its separation, the surrounding parts, the portions of bone
which are not doomed to perish, have commenced forming new osseous
matter, which is secreted in nodules, and from continued deposition
soon becomes consolidated. The commencement of the process is well
seen in the following sketches from specimens in my collection. The
disease, as represented in the two first cuts, was of the most acute
kind, and a great part of the shaft of the tibia had perished. This
is seen at various points through the sort of cortical deposit of
new bone. The new bone, in its turn, secretes a texture similar to
itself,105 whereby the deposit becomes more and more extended, and not
unfrequently affords an almost complete encasement to the dead portion,
or sequestrum, as represented in the cut on the right-hand side of the
page. In general bone dies irregularly, so that the sequestrum presents
an uneven surface, and its margins are rough and serrated by numerous
 sharp projections, as seen in the one taken from the tibia, and
represented here. From the appearance of the dead bone, it was imagined
that after its separation, portions of it were removed by absorption;
and this opinion was strengthened by the thin exfoliations of the
external lamina being found perforated at several points by minute
apertures,—worm-eaten, as it was called. These cases of death of inner
or medullary shell are irregularly separated, like any other slough;
the remaining living outer shell is enlarged by inflammatory action
and deposit. But a dead portion of bone, detached from the surrounding
parts, is in every respect an extraneous body, and is not, and cannot
be, acted on by the absorbents, any more than a piece of metal, wood,
or stone. Some have gone so far as to affirm that portions of foreign
bodies, ligatures, &c., are absorbed; but this opinion is altogether
too absurd to require any contradiction; the knots of ligatures, like
portions of glass, or other foreign substance, become surrounded with
a dense cyst, and often remain in the body for a long time; so do
portions of dead bone separated by the process here described. A series
of experiments were made by Mr. Gulliver, in order to put this question
at106 rest, many of which I witnessed and assisted at, and several I also
repeated. Setons of bone were inserted and worn for a long time; thin
plates of bone were confined on suppurating surfaces; pieces of bone
were inserted in the medullary canal of various animals, and kept there
for months, and in one instance for more than a year. These foreign
bodies were weighed with the greatest care and accuracy before and
after they were so exposed to the absorbents, and were found unaltered
in any respect. A paper, detailing these experiments, is published in
the Medico-Chir. Transactions.
sharp projections, as seen in the one taken from the tibia, and
represented here. From the appearance of the dead bone, it was imagined
that after its separation, portions of it were removed by absorption;
and this opinion was strengthened by the thin exfoliations of the
external lamina being found perforated at several points by minute
apertures,—worm-eaten, as it was called. These cases of death of inner
or medullary shell are irregularly separated, like any other slough;
the remaining living outer shell is enlarged by inflammatory action
and deposit. But a dead portion of bone, detached from the surrounding
parts, is in every respect an extraneous body, and is not, and cannot
be, acted on by the absorbents, any more than a piece of metal, wood,
or stone. Some have gone so far as to affirm that portions of foreign
bodies, ligatures, &c., are absorbed; but this opinion is altogether
too absurd to require any contradiction; the knots of ligatures, like
portions of glass, or other foreign substance, become surrounded with
a dense cyst, and often remain in the body for a long time; so do
portions of dead bone separated by the process here described. A series
of experiments were made by Mr. Gulliver, in order to put this question
at106 rest, many of which I witnessed and assisted at, and several I also
repeated. Setons of bone were inserted and worn for a long time; thin
plates of bone were confined on suppurating surfaces; pieces of bone
were inserted in the medullary canal of various animals, and kept there
for months, and in one instance for more than a year. These foreign
bodies were weighed with the greatest care and accuracy before and
after they were so exposed to the absorbents, and were found unaltered
in any respect. A paper, detailing these experiments, is published in
the Medico-Chir. Transactions.
The separation of the dead part from the living is accomplished with
greater or less ease, according to the bone which is affected, the
state of the constitution, and the general health; in the bones of the
superior extremity, this, as well as every other action, proceeds more
rapidly than in those of the inferior. It occurs in consequence of
absorption of the living part of the bone, which is in close proximity
to the dead. The sequestrum, if large, is not pushed off, as some
have supposed, by granulations, deposited on the living margin of the
bone. A small portion of the inner shell, when completely detached,
may sometimes be observed to be extruded from a cloaca by granulations
from the living bone. During its progress, matter forms, makes its way
to the surface, and is discharged through minute, and often numerous
apertures, which afterwards become fistulous. The soft parts are
thickened and indurated, and the integuments are red, and sometimes of
a livid colour.
Formation of matter upon the bone is occasionally the cause of
necrosis, the periosteum being destroyed or separated from its
connections by the pressure or insinuation of the pus. I have seen
several instances in which it followed neglected erysipelas of the
lower extremity.
The matter is in general thick and laudable; at first it is secreted
profusely, but afterwards in smaller quantity. The external openings,
or papillæ, through which it is discharged, are found to lead to
cloacæ, or apertures in the new and living bone, which encase the dead,
and through these the dead portions can be discovered by the probe;
and it will thus be ascertained whether the sequestrum is fixed or
detached: when loose, it can sometimes be moved upward and downward in
the cavity. When the shaft of a bone is much affected, the whole limb
is enlarged, by the inflammation having extended to a considerable
distance above and below the portion about to become necrosed. The
unshapely appearance of the limb continues until the sequestra are
discharged; for by their presence incited action is still continued,
and subsides only after their removal. Some time before any portion of
bone has become dead, or begun to be separated, great effusion of new
bone has, in general, occurred; thus a preparation has been made for
the strengthening of the limb, which, after a considerable portion of
the bone has been detached, would otherwise be incapable of supporting
the weight of the body. The unnatural bulk of the limb is afterwards
much diminished, for the new bone gradually becomes consolidated, and
smooth on the surface by the action of the absorbents. Nature seems to
construct her107 substitute after the model of the original, and in some
instances but very little change can afterwards be observed in the limb.
In external necrosis, or death of the outer lamella, reparation is
chiefly made by the subjacent parts; and this species of necrosis
occurs most frequently in the flat bones. In necrosis involving a
greater thickness of the bone, the new matter is also furnished by
the subjacent parts, which, however, are materially assisted in the
process by the living bone, which forms the margins of the void caused
by the absorbent process for the detachment of the dead portion. The
bony matter is deposited with great activity, and frequently columns of
the new deposit cross over the sequestrum, binding it firmly down, and
rendering it almost immovable, although it may be completely detached
from the living parts.
It has already been stated, that those vessels which ramify within the
substance of the periosteum have no share in the reproduction of bone,
but plastic matter is effused by the ramifications extending from the
membrane to the bone: this effusion becomes organised, and greatly
assists in forming the substitute.
It has been formerly remarked, that a limited, and, on after
examination, an apparently trifling necrosis of the cancellated
structure, may produce the most violent local symptoms; the painful
feelings, the discharge, and the thickening of the bone, continue, as
long as the cancellated sequestrum remains; severe symptomatic fever
is induced, endangering the life of the patient, and often rendering
removal of the limb absolutely necessary.
Occasionally abscesses form at a considerable distance from the
necrosed part, and terminate in sinuses, which communicate with
the diseased bone, and are consequently long and tortuous, so that
examination by the probe is rendered difficult. When necrosis is
extensive, there is a risk of fracture occurring, if motion of the limb
be permitted before a sufficient quantity of matter has been effused,
before nature has had sufficient time for the consolidation of her
substitute, and consequently before the new bone has come to resemble
the old in thickness and cohesion.
Violent inflammatory fever attends the incited action of the vessels
of the bone and periosteum which precedes necrosis. But after the
abscesses have given way the painful symptoms subside, and the health
seldom suffers to any great extent, the system becoming gradually
accustomed, as it were, to the new condition of the parts. Hectic
supervenes only when the disease is very extensive, and joints become
involved. Frequently fresh collections of matter form as each piece of
bone approaches the surface. When the effusion of new bone has extended
to the neighbourhood of a joint, its motion may be very much impeded,
and, from the limb being kept in a state of rest for the cure of the
necrosis, anchylosis may even occur.
Treatment.—The means of preventing inflammatory action from
running high and ending in death of bone have been already alluded
to—abstraction of blood, rest, purgatives, and antimonials. When
necrosis has occurred, no interference with the bone is allowable,
unless the sequestrum is quite loose, or unless the patient’s health
is108 suffering severely under the discharge and irritation. When the
sequestrum can be readily moved about, or when, projecting through the
external opening, it can be laid hold of by the fingers or forceps,
attempts must be made to remove it. The surgeon ought not, however,
to allow it to approach the surface, and project externally, for the
natural discharge of the sequestrum is a much more tedious process
than the removal of it by art, and by the irritation produced during
its spontaneous ejection the inflammatory action is continued, and may
prove alarming. Long before it has appeared externally, it must have
been completely separated from the living parts, so as to admit of
ready extraction by the proper means. When it has been ascertained that
the sequestrum is separated, it ought to be laid hold of by forceps,
and moved freely upward and downward, so that any slight attachments
by which it is connected to the neighbouring parts may be destroyed,
whether these be minute filaments which still in some degree retain
their vitality, or small portions of newly deposited bone, which are
so situated as to prevent the free movement of the sequestrum. In
general, no impediment of this nature exists, and the dead bone is
easily removed. Before extraction can be accomplished, it is generally
necessary to enlarge freely the external opening, in all cases where
the dead portion of bone is of considerable size. If, on thus exposing
the parts, the sequestrum be found detached, but still firmly bound
down by the substitute bone, deposited over it either in one continuous
sheet, or in irregular columns, this must be divided by a trephine, a
small saw, or cutting pliers, before the sequestrum can be extracted.
When a dead portion of bone, of considerable length, is exposed at its
centre, whilst its extremities are entangled by the old or substitute
bone, the division of the exposed part of sequestrum, by means of the
cutting pliers, will often be sufficient for its removal, the cut ends
being seized by the forceps, and one half removed after the other;
thus the perforation or removal of any portion of the substitute will
be rendered unnecessary. The instruments, and especially those for
extraction, ought to be very powerful, and suited to the purpose; for
in the employment of inefficient means there is much folly and cruelty.
Incisions into a necrosed limb are attended with profuse hemorrhage
from the enlarged and excited vessels; and in some cases it is with
difficulty arrested, in consequence of retraction of the cut ends of
the vessels not taking place within the condensed and indurated parts.
Pressure, and an elevated position of the part, will generally be
found to answer. When necrosis has been extensive, the limb must be
carefully supported by the application of splints and bandage, till
the process of reparation be completed, in order to prevent fracture
of the recently formed substitute. This proceeding is seldom, however,
necessary.
The treatment may be summed up in a very few words. Prevent the
necrosis, if possible; open abscesses whenever they appear; encourage
the patient to move the neighbouring joints; support the strength;
remove sequestra when loose, but do not interfere till they are
ascertained to be so; give the limb proper support and rest, when109 a
large sequestrum is formed. When fracture has taken place, when the
 health has been undermined, or when neighbouring joints have become
diseased, amputate, in order to save the life, if it be impossible to
save the limb.
health has been undermined, or when neighbouring joints have become
diseased, amputate, in order to save the life, if it be impossible to
save the limb.
It is almost superfluous to remark, that leeching and blistering are
worse than useless after necrosis has occurred, however useful they may
be in preventing it; and that the adoption of measures to promote the
dissolution and absorption of the sequestra are glaringly absurd.
Necrosis, after amputation, was formerly frequent; but in the present
improved state of this operation it is so rare as scarcely to demand
separate consideration.
Such specimens as here depicted are common enough in the collections
of those who have practised the old round-about operation; in fact,
it is only by this painful and tedious interference of nature that a
tolerable stump is formed in many of these cases. Death of a small
portion will sometimes, though very rarely, follow even a very well
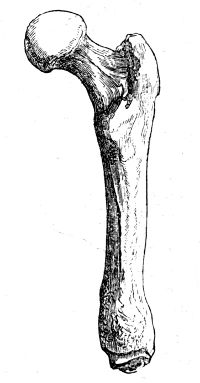 performed amputation, if through any mischance the recovery is
slow, and wasting discharge takes place with emaciation. It happens
sometimes, as when secondary hemorrhage (that is to say, bleeding after
the fourth day) has taken place, that the flaps are separated by the
coagula, and it may be impossible to bring the parts together and give
them due support; then the muscles, wasted and shrunk, may leave the
bone a little, but the exfoliation is but very trifling.
performed amputation, if through any mischance the recovery is
slow, and wasting discharge takes place with emaciation. It happens
sometimes, as when secondary hemorrhage (that is to say, bleeding after
the fourth day) has taken place, that the flaps are separated by the
coagula, and it may be impossible to bring the parts together and give
them due support; then the muscles, wasted and shrunk, may leave the
bone a little, but the exfoliation is but very trifling.
The inner shell of bone, as may be seen in the above sketch, perishes
more extensively than the outer; and this arises probably from
inflammation of the medullary membrane, in consequence of exposure, or,
perhaps, from its being sometimes injured by the operator or assistants
seizing the bone rudely to steady the stump, in order to facilitate the
ligature of the vessels. In experiments on animals, the disturbance
and injury of the medullary membrane is followed by internal necrosis,
thickening of the outer living shell, and effusion betwixt the
periosteum and bone. New bone is also furnished from the medullary
canal, as is also shown in the sketch.
110
FRAGILITAS OSSIUM
Occurs chiefly in old people, whose bones contain an undue proportion
of earthy matter, are endowed with little vascularity, and filled with
an oleaginous fluid. They contain an undue quantity of phosphate of
lime compared to the gelatin; and the liability to fracture is further
increased by the interstitial absorption of the outer shell. They are
in an atrophied state, and this is often in part attributable to disuse
of the limbs. This state of the osseous system very often follows upon
an attack of rheumatic fever, and is met with in patients who have
laboured under cancerous affections.
The bones, when in this condition, often break from the slightest force
applied; as from the action of the muscles when the patient turns
himself in bed, whilst walking across the room, or when endeavouring
to attain the erect posture when seated on a chair. After fracture
the process of reunion is extremely slow, and it does not take place
at all in patients very old and of worn-out constitution. With a view
to prevent the occurrence of fracture when the bones are in this
condition, for it is impossible by any treatment to prevent the change
in the texture of the bones, the only rational indications seem to be
to keep the patient on a generous diet, and to prohibit him from making
any great muscular exertion—to avoid, in fact, all circumstances likely
to produce a sudden action of any particular set of muscles.
OF MOLLITIES OSSIUM, RACHITIS, ETC.
These affections differ only in this, that in the latter the earthy
matter is not deposited originally, whilst in the former it is absorbed
after having been deposited; in both the result is the same. The latter
is peculiar to the very young, the former to those of an advanced
age.11
Rickets and mollities ossium seem to differ also in this. In the latter
there is seldom, if ever, any reparative action. The diseased process
of deposit continues in the bone, the softening increases, and 111the
patient ultimately perishes. Whereas, in rickets, the softened and
yielding state of the bones is only temporary: after a time earthy
matter is deposited in due quantity, and the bones become compact,
firm, and solid, capable of supporting the weight of the body, though
necessarily permanently bent and deformed, if proper means have not
been employed during the softened condition. The thickness of the
rickety bone, as Mr. Stanley has shown, takes place on the concavity,
which is the situation where the greatest strength may be added with
the least expense of new matter. In the same way the reparation
of fractures not accurately adjusted goes on most actively in the
concavity formed by their displacement.
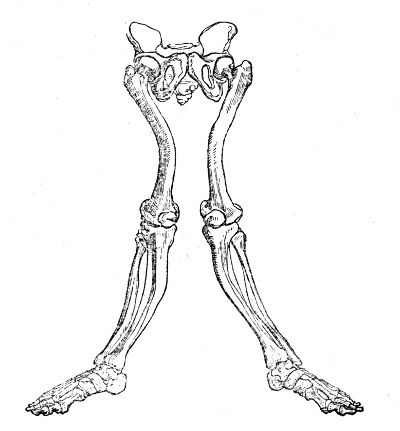
Softening of the bones is met with at all ages, and in different
degrees. It seems sometimes to be congenital, and combined with
hydrocephalus. It often follows dentition, measles, hooping-cough, or
other infantile diseases inducing debility. In females it seems to be
produced, or at least often accompanied, by the debilitating effects
of leucorrhœa, miscarriages, and floodings. Loss of blood, in any way,
predisposes to it. Mercury, given in immoderate quantities, produces
a softening of the bones; and, in some most remarkable instances on
record, the free use of common salt was the only cause assigned. When
the disease affects children, all the bones generally suffer, those of
the extremities as well as those of the trunk; the limbs become bent
in an extraordinary manner, and the heads of the bones are swollen,
and appear to be much more so in consequence of the wasted and flabby
state of the muscles. The child walks with diffi112culty, and in many
cases the legs are utterly incapable of supporting the weight of the
body, so that he cannot remain in the erect position. The chest and
pelvis become deformed, breathing is oppressed, the digestive organs
are deranged, and the belly is tumid. The bones of the limbs become
flattened as well as bent, and in their concavities, as remarked in the
preceding cut, new bone is effused, in order that the column of support
may be thereby strengthened. The new deposit is of extremely dense
consistence, and is effused in greater or less quantity, according to
the degree of curvature.
The bones of rickety subjects are soft, cellular, and of a brown
colour, contain a dark fluid, and are very deficient in earthy matter.
As a simple proof of the latter circumstance, it may be mentioned
that distortions of the pelvis can be, and often are, accurately
imitated by soaking the bones for some time in acid, whereby the earthy
matter is extracted. In many instances this component of the bones is
almost entirely removed, and soft matter deposited instead; they then
consist merely of an extremely thin external osseous shell, covered by
thickened periosteum, and containing a pulpy substance resembling fatty
matter. During the progress of the disease, the urine deposits, often
in great quantity, a white sediment, which, on analysis, is found to
be the phosphate of lime. In rickets the head is generally enlarged to
a greater or less degree, and the bones of the cranium are thickened
and spongy; not unfrequently the intellectual faculties remain acute.
In adolescents and adults the limbs seldom become affected; the
bones composing the spinal column are the seat of the disease, and,
along with the distortion of the spine, the position of the ribs is
necessarily altered. Certain rare cases have occurred, in which all
the bones of the adult were softened to a very great degree. In one
remarkable instance, the patient complained of an annoying sense of
tightness in the limb most affected, and, on examination, the softened
bone was found greatly depressed at that point, as if a strong ligature
had been drawn tightly round it. Mr. Howship, who attended the patient,
was so kind as to present me some years ago with a portion of the
altered femur, which consists of a fatty-looking substance, and appears
to contain little or no earthy matter.13
113
Though incurvation of the spine occurs in boys, and even in adults,
still it is most frequently met with in young females; and in them it
is often induced by their having assumed a bad habit by sitting long in
one constrained and awkward posture, as in writing or drawing, without,
perhaps, the bones being unnaturally soft in the first instance.
It often follows affections of the lower limbs, as of the knee or
hip-joint; and is also caused by shortening of a limb, which has been
negligently or ineffectually treated after fracture during child114hood,
or by the patient being allowed to continue a custom of standing
awkwardly on one leg. In a very remarkable specimen in my possession,
the curvature seems to have resulted from the tremendous enlargement
and consequent weight of the head. The whole skeleton (head, thorax,
pelvis, and extremities) is deformed, flattened, and twisted. This may
have arisen more readily in consequence of the atrophy of the bones,
and retardation of their growth, produced by the long confinement
to bed. The number of ossa triquetra in the lambdoidal suture was
unusually great. The patient attained the age of twenty-five. The
affection commenced from birth.
At first, during slight curvature from such causes, the spine can be
brought into its original straight position by the voluntary action of
its muscles. After some time, however, the curve cannot be remedied
by any effort; interstitial absorption of the bodies of the vertebræ
towards the concavity of the curve occurs; they become changed in
form, and accommodated to their altered position, as shown in the
accompanying sketch; the muscles also accommodate themselves to the
new position, as do also the various ligaments connected with the
spinal column. When the curvature is seated in the dorsal vertebræ it
is generally to the right side; this shoulder is raised, and the chest
is protruded, whilst the opposite side is depressed and flattened. The
clothes hang loose, or fall off on the left side—the patient rests
the weight of his body chiefly on the left leg—on stooping the right115
scapula projects, and, on examination, is found to be nearer to the
spinous processes of the vertebræ than the left. The left cavity of
the chest is diminished, and the ribs press upon the heart and lungs,
causing difficulty of breathing. To preserve the balance of the body,
a curvature occurs below the former, and in the opposite direction;
and not unfrequently there is a third incurvation situated above the
primary one.
The bones of the pelvis become distorted, and are twisted to one side;
or, when the softening is great, and the patient confined to the
recumbent position, the introitus of the cavity becomes diminished
in the antero-posterior diameter; and, if the patient walk about,
the ossa pubis are squeezed together, in consequence of the pressure
of the ossa femora against the acetabula. The crests of the ilia are
often bent inwards, in consequence of the pressure of steel apparatus
injudiciously applied with a view of removing deformity. When the bones
become consolidated after such distortion, they present most serious
obstacles to parturition; and, most unfortunately, crooked and deformed
women possess, it is said, “great aptitude for conception.” When, in
such females, the untoward circumstance of pregnancy has occurred,
it has been necessary, in some, to have recourse to the Cæsarean
operation, and others have been delivered with the greatest difficulty
and danger; notwithstanding which, many of these latter have, after
recovering from a long and tedious illness, again become pregnant.
In some cases the softened ribs not only compress the organs of the
chest, but are also pressed down upon the abdominal viscera, or even
into the pelvis. The symptoms arising from such displacement are at
first urgent, as can readily be imagined, and are often treated as
inflammatory, to the detriment of the patient.
After some time, as the state of the patient’s health improves, the
bones in some degree regain their original firmness, and the curvatures
are rendered permanent. New bone is deposited in the concavity of the
curve, at first in irregular masses, but afterwards becoming condensed,
and assuming a more regular form, the column is thereby supported and
strengthened.
Bending of the spine backward, with depression of the spinous
processes, is extremely rare. But curvature forward, with projection of
these processes, is by no means uncommon, and is generally supposed to
be caused by caries of the bodies of the vertebræ; in many instances,
however, it arises from interstitial absorption only.
Curvature from caries of the vertebræ, though not so frequent as the
curvature from other causes, is met with pretty often. In adults, the
curvature from ulcerative absorption is more common than that from
softening of the bones. It is attended with the formation of purulent
matter, which presents in the loins, at the top of the thigh, or near
the anus; the bones may become affected secondarily, though much
less frequently, in consequence of the formation and accumulation of
purulent matter in their neighbourhood. There is pain in the loins; the
patient walks in a stooping posture, and often complains of pain in
the knee or thigh. The lower limbs sometimes become paralytic, as also
the sphincters and extremities of the hollow viscera;116 this, however,
may arise, without curvature, from softening of, or effusion on, the
chord, or diseased thickening of its membranes. In some cases the
palsy supervenes slowly; at first the patient has an awkward gait; he
lifts his feet high to avoid stumbling, and afterwards puts them down
clumsily and suddenly; the foot, in some cases, is extended, so that
the patient is unable to plant the sole on the ground. Retention of
urine occurs, and is followed by incontinence, with copious deposits.
In the treatment of Rachitis, the chief indication to be fulfilled
is to support and increase the powers of the system; and this may
be accomplished by affording the patient a generous diet, keeping
the bowels in good order, enjoining gentle exercise and exposure to
pure air, by the assiduous use of frictions, and by supporting the
softened bones by properly applied and light machinery. Much mischief
may be done by clumsy and heavy apparatus which confine the movements
of the patient; the muscles are wasted, consequently the spinal
column is weakened, the general health is impaired, and the disease
is aggravated. Some have recommended the internal administration of
the phosphate and muriate of lime, but their efficacy is extremely
doubtful. Preparations of iron seem to answer much better in the
greater number of cases. In cases of curved spine, apparently arising
from bad habit, the patient should be in no degree confined at writing,
or drawing, or music; her posture while at work or play ought to be
attended to, as well as her mode of walking or standing; and, if
awkward, prohibited. Gymnastic exercises of the more gentle kinds ought
to be enjoined, such as those with poles and light wooden clubs, the
turning of a wheel, the exercise with balls, &c. Carrying weights on
the head can only be applicable in certain cases. The shoulders, in
some instances, ought to be kept back by means of a light back-board;
and in aggravated cases the weight of the shoulders, and sometimes also
of the head, must be taken off the spine by a light and well-contrived
apparatus. Sea-bathing, good air, out-of-door exercise, and attention
to diet, are of material importance. Frequently advantage will result
from the patient’s sleeping on a hard mattress; and, in bad cases, from
lying down, when tired, on an inclined plane.
In great softening, it will be necessary to confine the patient
entirely to the recumbent position, and to support the head and
shoulders by a light and firm machine. The causes, symptoms,
appearances, and treatment of caries of the spine, in its different
regions, with or without curvature, will be afterwards considered.
OF INFLAMMATORY AND OTHER AFFECTIONS OF THE ARTERIAL SYSTEM.
During inflammation of arteries, the actions of the vessels are
accelerated and attended with pain; the internal coat is found to be
of a red colour, from increase of its vascularity, and not from its
being merely tinged with the colouring part of the blood; or it is of a
yellowish hue and rough, from the deposition of lymph on its surface,117
whilst the external coat is thickened by the infiltration of serum and
lymph. When bloodvessels are inflamed from mechanical irritation, lymph
is secreted on their internal coat, becomes organised, and obliterates
their calibre; if deficient in nervous influence and circulating fluid
at a particular point, there ulceration of their coats occurs; if
violently injured or completely isolated, their coats mortify; and
these circumstances must all be calculated on in the surgical treatment
of arteries. A universal inflammatory state of the arterial coats is
said to have existed, and its symptoms have been minutely detailed; but
its occurrence seems to be extremely rare, and the treatment is medical.
Inflammation is supposed to precede degeneration of the arterial
coats. As a person advances in life the arteries lose elasticity, and
the heart its balance with them; either the one or the other becomes
dilated, their parietes are thickened, and the valves are altered
in structure; the enlargement of the vessels is generally greatest
towards their origin. The dilatation of arteries, more especially of
the internal ones, is often very great; ultimately the internal coat
gives way, and the external, with the surrounding tissues, yields
in proportion as the blood diffuses itself. The internal tunic is
occasionally burst in consequence of violent and sudden muscular
exertion; and, even when the vessels are pretty limber and sound,
effusion of lymph, and obliteration of the vessel ensue, or, more
frequently, aneurism.
Previously to the rupture of the internal tunic, however, there is,
in most cases, a morbid alteration in the texture of the vessel. The
internal coat becomes dry; its textures is more dense and less elastic,
and consequently more brittle. Morbid matter is deposited between the
middle and internal coats, and this, by stretching the latter still
further, diminishes the elasticity and cohesion of their texture.
The deposit is at first to a slight extent and of soft consistence,
somewhat resembling condensed fatty matter. Afterwards it increases
in quantity and consistence, becoming, instead of soft and yielding,
dense, hard, and incompressible; in short, calcareous.
Though the morbid deposit is at first confined, as above related, its
limits are afterwards extended; calcareous matter is insinuated, either
in minute particles or in broad laminæ, amongst the fibres of the
middle coat, is also found external to it, and occasionally situated in
 the cellular coat. In fine, the various component parts of the parietes
of the vessel degenerate, according to the degree of advancement which
the disease has attained; and such a condition is the predisposing
cause to ulceration of the internal coat, and subsequent effusion of
blood. The steatomatous, ulcerated, earthy degeneration of the proper
coats of an artery, as Scarpa, the celebrated professor of Pavia, has
it, are well exhibited in the accompanying sketch.
the cellular coat. In fine, the various component parts of the parietes
of the vessel degenerate, according to the degree of advancement which
the disease has attained; and such a condition is the predisposing
cause to ulceration of the internal coat, and subsequent effusion of
blood. The steatomatous, ulcerated, earthy degeneration of the proper
coats of an artery, as Scarpa, the celebrated professor of Pavia, has
it, are well exhibited in the accompanying sketch.
ANEURISM
During violent and sudden exertions118 the more brittle parts may burst,
either at a certain point, or throughout the whole circumference of the
artery; and on this such results will supervene as on ulceration of the
internal tunic. Ecchymosis then takes place under the cellular coat,
which becomes thickened, and incorporated with, and strengthened by,
the surrounding tissues; this is the incipient state of an aneurismal
tumour. The effusion of blood, gradually increasing, distends the
cellular coat, forming the cavity into which it is poured, and produces
a tumour of a size proportional to the distensibility of the tunic and
the force of the effusion. Sometimes the external coat is separated
from the others to a considerable extent by the insinuation of blood.
An aneurism, however, may exist from simple dilatation of a portion of
the vessel, gradually increasing, and forming a cavity in which the
blood accumulates. At one time it was supposed that all spontaneous
aneurisms were caused by simple dilatation of the canal; but such an
opinion has been long shown to be incorrect, and the term of true
aneurism is now confined by many to that tumour and accumulation of
blood consequent on the giving way of the internal coat, and situated
externally to the canal of the artery. It is true that dilatation may
occur previously to the giving way of the coats, and thus the two
causes are combined. The dilatation occurs from the calibre of the
artery being considerably diminished, in the first instance, at the
point where its coats have undergone the calcareous degeneration, and
only acts as a predisposing cause to the failure of the coats when
thus diseased. When there is mere dilatation, the tumour is generally
of an oval form; but when the internal coat gives way, a lateral
prominence is formed, and gradually increases in size. The shape of
the true aneurism is various: sometimes the tumour is globular, with a
narrow neck; and, from this being of considerable length, it becomes
difficult, in some situations, as above the clavicle, to ascertain the
particular artery which is the seat of disease, the globular extremity
of the tumour presenting itself at some distance from the vessel with
which its pedicle is connected. This is rare, however. At other times
its form is very irregular, being most prominent at the part where the
accumulation of the blood is least resisted. Pulsation in the tumour
is distinct from the first, and is painful to the patient; and in the
external aneurisms it is so strong as to be perceived by a bystander
at a considerable distance. The tumour is at first compressible, and
completely disappears on firm pressure being applied, either directly
to the sac, or to the artery above, the sac being thereby emptied of
its contents, or prevented from being filled. It may sometimes be
difficult to form an accurate diagnosis, from the circumstance that
tumours, not aneurismal, receive a pulsatory movement from an artery
or from arteries immediately beneath them; such difficulty is obviated
by attention to this simple test—that in an aneurism the pulsation is
felt equally in all directions. Besides, if the tumour is moveable,
it can be partially displaced, so as not to lie immediately over a
large artery, and, if it be not aneurismal, it will then be found to
possess no pulsation; if it be an aneurism, its pulsation will not be
diminished by any change of position.
The blood contained within the aneurismal sac, being comparatively
motionless, coagulates, and the coagulum is attached to the119 inner
surface; at first it contains red globules, but it afterwards loses
them, and becomes of a pale hue, consisting solely of fibrin. This
coating gradually increases, and attains no small thickness, fresh
portions of fibrin being superadded in concentric laminæ. These layers
are chiefly deposited from the blood within the cavity, but they also
appear to receive addition from lymph being effused by the vessels
proper to the original parietes of the tumour. By such thickening, it
can be easily conceived that the pulsation will be somewhat lessened.
In large aneurisms the accumulation and deposit of fibrin may be much
greater at some points than at others, and hence pulsation may be
rendered “not equal in all directions.” It is not, however, diminished
to any great extent; for absorption of one or more points occurs, and
the coating is again attenuated.
In some rare cases the deposition of fibrin has gone on gradually
accumulating, filled completely the aneurismal cavity, and thus
effected a spontaneous cure, the remaining solid tumour imperceptibly
diminishing by the action of the absorbents. After obliteration of
the aneurismal cavity, the fibrin is generally deposited in so great
quantity as to occupy the calibre of the vessel above and below the
tumour, obstructing the progress of the blood, causing it to flow by
the smaller and collateral branches, and effecting a spontaneous cure,
somewhat similar to that produced by the artificial application of a
ligature. Coagula are seldom formed in the dilated vessel, to whatever
size it may be enlarged, unless there is fissure of the internal
coat; for in no other way can a portion of the blood readily become
stagnant, while the calibre of the vessel remains pervious. There
is in my collection a preparation of dilated aorta, to the coats of
which adheres a large firm coagulum. Occasionally, though rarely, a
dilatation of the internal coats is met with accompanied by thinning of
the external ones. Of this sort of diverticulum, there is also a good
specimen in the collection here alluded to.
A spontaneous cure may also be accomplished from the original aneurism
being compressed by one of a more recent origin, causing ultimate
obliteration of the canal. Of this I recollect one remarkable instance;
the patient was afflicted with an aneurism of the axillary artery,
which had attained a large size, and the cure for the disease in
this situation being then unknown or unattempted, the patient was
considered as lost; but some time after the tumour began to diminish,
and disappeared. The patient died; and the cause of death was found to
be the giving way of an aneurismal tumour of the arteria anonyma, which
was situated so closely to the aneurism of the subclavian as to have
acted as a mechanical compress, causing obliteration of the vessel at
that point.
When a cure has been effected, the vessel is found to be converted into
a dense and impervious cord at the site of the tumour. The canal above
is dilated; the coats are thickened, especially the middle; and from
the thickening and increased action of the fibres, the internal coat
becomes somewhat rugous, the rugæ being in a transverse direction.
The aneurismal tumour in general increases, and approaches the surface,
involving and destroying all the intervening textures. If resisted in
its enlargement by bone, even this is not sufficient to impede its
progress; the bone is absorbed, and perhaps ulcerated, at120 the point
where it is compressed by the tumour. The osseous is more liable to
destruction from this cause than the cartilaginous tissue, contrary to
what occurs from compression by abscess. Ultimately the sac gives way,
and its contents are discharged either externally, or into an internal
cavity or canal, in consequence of its parietes sloughing from the
compression made by the tumour; and such termination is instantly fatal.
 An aneurism of the descending aorta, in a great measure one from
dilatation, is here represented: the patient also laboured under
popliteal aneurism of one limb, and inguinal of the other. He died
suddenly, in consequence of the giving way of the internal tumour.
The escape of blood into the cellular tissue may even take place to
such an extent as to prove fatal in a few hours. The disease may also
prove fatal by mere compression, as of the trachea, impeding breathing,
and inducing disease of the respiratory organs; or by pressure on the
gullet preventing the passage of food: in the latter case, however, the
dissolution is generally more sudden, in consequence of the compressing
part of the tumour giving way, and the contents being evacuated into
the stomach or mouth. If the aneurism compress a plexus of nerves, or
the spinal chord itself, the anterior part of the vertebræ having been
previously absorbed, paralysis is produced.
An aneurism of the descending aorta, in a great measure one from
dilatation, is here represented: the patient also laboured under
popliteal aneurism of one limb, and inguinal of the other. He died
suddenly, in consequence of the giving way of the internal tumour.
The escape of blood into the cellular tissue may even take place to
such an extent as to prove fatal in a few hours. The disease may also
prove fatal by mere compression, as of the trachea, impeding breathing,
and inducing disease of the respiratory organs; or by pressure on the
gullet preventing the passage of food: in the latter case, however, the
dissolution is generally more sudden, in consequence of the compressing
part of the tumour giving way, and the contents being evacuated into
the stomach or mouth. If the aneurism compress a plexus of nerves, or
the spinal chord itself, the anterior part of the vertebræ having been
previously absorbed, paralysis is produced.
In consequence of aneurism, the circulation of blood in the vessel
is obstructed; hence the collateral branches above the tumour become
enlarged, and through them the circulation is continued; by their
anastomosis with collateral branches which arise below the seat of the
tumour, a portion of the fluid is brought back into the canal of the
original artery. The circumstance of collateral enlargement used to be
distinctly enough demonstrated in amputation, one of the old cures for
the disease.
The tumour may be suddenly increased by a portion of the parietes
giving way, and the blood being propelled into the cellular tissue,
which becomes thereby condensed, and supplies the deficiency in the
original sac; diffuse is thus superadded to the true or encysted
aneurism.
The disease is generally accompanied with great pain, the neighbouring
nerves being much stretched by the enlargement of the tumour, as in the
axilla or ham; in these situations also the limb below the aneurism
is much swollen from the compression of the absorbents and veins and
consequent infiltration into the cellular tissue. Diffused aneurism
from wounds, and the other species of the disease, will be afterwards
treated of.
The peculiar degeneration of the coats of the vessels has been already
stated to be the predisposing cause of aneurism; and the disease
may be directly caused by over-excitement of the circulation, or
by an over-exertion of the muscles. It is more frequent in males121
than females.14 In men somewhat advanced in life the arteries get
hard and rigid, whilst at the same time the muscles are strong, the
general health good, and the whole frame stout and active; so that the
patient is capable of violent muscular action, such as the arteries
are ill able to bear, and consequently the internal coat of a vessel
yields, and lays the foundation for an aneurism.15 The lower limbs
being chiefly subject to such exertions, aneurism in them is most
frequent;16 and for the same reason it is said to be common in those
who 122ride much on horseback. Degeneration of the coats of the vessels
in the superior extremity is extremely rare. This is another reason why
spontaneous aneurism seldom assails them.
Treatment.—In internal aneurism the only indication which can be
followed, with any chance of success, is to favour the occurrence of
a spontaneous cure, by abstracting all stimuli, mental and corporeal,
by enjoining complete rest, by keeping the patient on low diet, and by
repeated bleeding. Thus the force of the circulation is diminished,
and coagulation, it is said, promoted; by this practice aneurisms,
the progress of which defies external means, are occasionally, though
very rarely, cured. Ice and other cold applications to external
aneurisms, or those which have made their way to the surface, have been
recommended to induce coagulation, but their use is not unattended with
danger; for they may, in some stages, so far diminish the vitality of
the coverings as to cause sloughing, and fatal hemorrhage.
In the treatment of aneurisms exterior to the great cavities, important
improvements have been made in modern times. No success can be expected
to follow palliative and temporizing measures, and a cure can result
only from operation. Formerly it was the practice to lay open the
aneurismal tumour, to search for the extremities of the artery opening
into the cavity, and to secure them by a ligature, or close them by
pressure, styptics, or both. In some few instances this method had
permanent success; but in the majority the operation proved wholly
abortive, and not unfrequently fatal. It was necessarily tedious in its
performance, and attended with much danger, the blood being discharged
in great profusion immediately after the opening of the sac, and the
extremities of the vessels being with great difficulty detected and
secured. Besides, the vessels in the immediate neighbourhood of the
tumour having generally undergone the degeneration already mentioned,
were incapable of taking on any healthy action; the application
of ligature on a vessel thus circumstanced could consequently be
productive of no advantage. From this method having almost invariably
proved unsuccessful, practitioners in those days generally preferred
amputation, when the tumour was so situated as to allow it; and when
the disease occupied a situation in the limb so high as to prevent
amputation, the case was deemed incurable, and the patient abandoned
to his fate. But amputation was accompanied with circumstances almost
equally alarming with those attendant on division of the sac: the
hemorrhage was very great; for as a consequence of obstruction to the
free passage of the blood in the aneurismal vessel, the circulation
was chiefly carried on by the collateral anastomosing branches, which
were there123by so much enlarged, as, on their division, to pour out
blood with a profusion resembling that of arteries of the second or
third magnitude. Continued pressure was employed as a less hazardous
method of cure, but was equally inefficacious; and was also attended
with danger, from the risk of sloughing. If the practice ever proved
successful, it was only after a tedious perseverance in its use, and
long confinement of the patient.
The operation of applying a ligature on the vessel at a distance from
the tumour, and thus intercepting or weakening the flow of blood into
the cavity, so as to allow complete coagulation to take place, is of
comparatively modern invention, and is the one now practised with
almost invariable success. To John Hunter without doubt belongs the
merit of proposing and putting it in practice; it has been claimed also
for the celebrated Desault. This operation has been variously modified.
Some have advocated the temporary application of a ligature, conceiving
that the effects produced will be as complete and permanent when it
has been allowed to remain only for a certain time, as when it is left
undisturbed and ultimately separated by nature. Such a theory, however,
has proved to be incorrect in most of the instances in which it has
been reduced to practice on the human subject; and the operation is
at best very uncertain, and not to be relied on. Others have employed
a double ligature, and some of the Continental surgeons have applied
a great many; some were tightened, others left loose, and looked upon
as ligatures of reserve to be tightened, should hemorrhage take place,
an occurrence likely enough to follow their clumsy and unsurgical
proceedings. A thick broad ligature like tape has also been used, from
an ill-grounded apprehension that all the coats of the artery would
be cut completely through by the tight application of a thin and firm
one. With the same view, a roll of linen or plaster has been interposed
betwixt the noose and the vessel, and this practice has been advocated
even by good surgeons—as Scarpa. Such complications can do no good,
and may do much mischief. The artery must be greatly detached from its
surrounding connections before the numerous and flat ligatures can be
applied, in consequence of which its coats will be apt to slough or
ulcerate, and hemorrhage occur. When, from any cause, the vessel has
been detached to a greater extent than is sufficient for the passing of
one ligature, two ought undoubtedly to be used, and one applied close
to each extremity where it is attached to the surrounding parts.
Again, it has been proposed, after the application of a double
ligature, that the vessel should be cut through betwixt the two
deligated points; it being supposed that in this way the closure of
each extremity will be more rapid, the cut ends retracting, and being,
in fact, in the same circumstances as the extremities of arteries
which have been tied on the face of a stump. Mechanical contrivances
have also been invented for the compression of the artery,—such as the
serrenœud and presse artere; these, however, are clumsy, insufficient,
and often injurious.
The single ligature, when properly applied, is the most safe, and
preferable to any other, for arresting permanently the flow of blood124
in a vessel. In its application, the artery must not be separated from
its connexions farther than is barely sufficient for the passage of the
armed needle beneath it; but the external incision ought to be free,
in order that this may be readily effected, and that the operation
may be easily and speedily performed. By the firm application of a
single ligature, the vessel is rendered impervious; the internal and
middle coats are divided, so that the ligature only encircles the outer
or cellular one, which resists the influence of any moderate degree
of force by which it may be tightened. The blood coagulates above
the deligated point,—the coagulum is of greater or less extent, in
proportion to the vicinity of a collateral branch, and is of a conical
form, the apex of the cone pointing to the free portion of vessel.
Incited action in the vessel takes place at the deligated point; the
divided margins of the internal and middle coats secrete lymph, by
which they adhere, and so obliterate the canal of the artery. Lymph is
also effused on the external surface, and in this deposit the ligature
becomes imbedded. The direct influx of blood into the aneurismal sac
is thus intercepted, and time is allowed for coagulation of the blood
which it contains; the artery for a considerable distance below the
ligature becomes ultimately converted into a firm and impervious
chord. The coats of the vessel above the ligature are much thickened,
and the internal membrane is occupied with the transverse rugæ
occasioned by projecting fasciculi of the fibres, which are always
apparent after obstruction of an artery. If this operation be properly
conducted, success must almost uniformly follow. Before determining
on its performance, however, the state of the arterial system ought
to be examined as carefully as possible; for not unfrequently the
degeneration of the coats is almost universal, and therefore an artery,
or even arteries, may be diseased at more points than one; and if this
aneurismal diathesis exist, the patient may be found to labour under
an internal aneurism of the aorta. In such a case, an operation could
not with propriety be undertaken for the cure of the external aneurism;
there might be no inconsiderable danger of the patient’s death being
suddenly accelerated by the operation, the sac of the internal aneurism
giving way perhaps during its performance: such a circumstance has
actually occurred.
Ligatures composed of animal substance, such as catgut, have been
proposed as preferable to all others, on the supposition that they
would be absorbed, and occasion less irritation; the fallacy of any
such theory has already been adverted to. After the ligature has been
applied for some time, it induces ulceration of the external coat which
it envelopes, by which means it becomes detached from the vessel;
acting as a foreign body, and causing a slight degree of suppuration,
it makes its way by nature to the surface and is discharged. The
period at which it separates may be said to be from the tenth to the
twentieth day; sometimes sooner, seldom later. If, however, much of
the surrounding parts have been extensively included along with the
vessel, a longer period will probably elapse before the separation of
the ligature. One end only of the ligature should be cut away close
to the artery, the other being left hanging from the external wound;
perhaps it is even safer to leave both, unless a third125 knot is made
upon it; thus the extraneous body, when detached, can be gently pulled
at so as to hasten the separation: this must be done with very great
caution. When both ends are cut short, and the knot closed in, there is
a risk of secondary hemorrhage, from the ligature causing formation of
matter round it, perhaps detaching the vessel from its connections, and
causing ulceration of its coats.
The operation ought to be performed at as early a period of the disease
as possible. Some recommend that it should be delayed in recent cases,
with the view of allowing sufficient time for the anastomosing vessels
to enlarge, in order that the circulation may be more vigorous in the
smaller branches after obstruction of the principal vessel. Such delay
prolongs the patient’s sufferings, which are in many cases extremely
acute, and the precaution is altogether unnecessary, as has been amply
proved by experience. On the same principle, the previous application
of pressure to the vessel has been recommended; but few surgeons,
if any, are now afraid of trusting to the resources of Nature when
the principal vessel of a limb is obliterated, and that suddenly,
without previous dilatation of the anastomoses. Cases are on record,
in which the abdominal aorta has been completely obstructed by a
natural process, without much impeding the inferior circulation; and
in one remarkable instance of this description, the inconvenience was
so slight that the disease was not suspected during the life of the
patient, the lower limbs retaining their usual size and activity. In
plethoric habits it may sometimes be prudent to abstract blood, even
more than once, previously to the operation.
When the ligature is placed immediately below a collateral branch
of considerable size, a bloody coagulum is not formed, though
adhesion may occur; but if the excited action should extend to the
collateral branch, and its canal become thereby obliterated, a
coagulum is speedily deposited. In consequence of the enlargement of
the anastomosing branches, and the increasing circulation in them,
pulsation generally returns in the tumour, to a slight degree, some
days after the operation. This, however, is by no means a sign that
the operation has been ineffectual; for the renewed pulsation almost
always disappears in the course of a very short time. In one instance
only have I found it assume a more permanent and troublesome aspect; in
that case, it recurred about ten months after the performance of the
operation, but speedily disappeared under the careful use of a compress
and bandage.
On account of the aneurismal diathesis, it occasionally happens,
that after the cure of one aneurism, another appears in a different
situation; in two instances, I operated on both thighs, at a
considerable interval, successively and successfully, for popliteal
aneurism, in the same patients.17
126
When the tumour is so situated as not to admit of the application of a
ligature between it and the heart, it has been proposed to place the
ligature on the distal side of the aneurism, upon the supposition that
coagulation will occur within the sac in this case as after the common
operation.18 The practice has been made trial of, but its expediency
appears very doubtful; neither has the success attendant upon it been
such as is generally supposed: the post mortem examinations have been
 very unsatisfactory in some of the cases. The application, indeed, of a
ligature in that situation can seldom be of any advantage, the artery
being already obliterated, in aneurisms of some standing, a long way
beneath the tumour; and it is, perhaps, from this circumstance that, in
such operations, great difficulty has been experienced in securing the
vessel, and that it has been thought necessary even to pass a needle
under a thick mass, somewhat in the situation of the artery. It would
appear, in some instances, that the artery when pervious had even
remained untouched, not being even exposed by the burrowing process
employed by some of the operators; and that if any vessel was tied, it
was not the trunk in which the disease existed. It would appear that a
very correct diagnosis had not been formed in some of the cases.
very unsatisfactory in some of the cases. The application, indeed, of a
ligature in that situation can seldom be of any advantage, the artery
being already obliterated, in aneurisms of some standing, a long way
beneath the tumour; and it is, perhaps, from this circumstance that, in
such operations, great difficulty has been experienced in securing the
vessel, and that it has been thought necessary even to pass a needle
under a thick mass, somewhat in the situation of the artery. It would
appear, in some instances, that the artery when pervious had even
remained untouched, not being even exposed by the burrowing process
employed by some of the operators; and that if any vessel was tied, it
was not the trunk in which the disease existed. It would appear that a
very correct diagnosis had not been formed in some of the cases.
The appearance of the vessel after the application of a ligature
above the tumour has been already shown. The obliteration of the sac
proceeds, in some cases, very rapidly; it assumes a harder feel,
decreases, and disappears; being connected with the vessel by means
of a dense impervious chord, to which condition that portion of the
artery has been reduced. The anastomosing vessels enlarge more and
more, carry blood freely from above to below the ligature, and thence
to below the tumour; some even passing to the latter situation directly
from above the ligature. Along with the muscular and other 127branches,
the neurilemmal vessels also become enlarged, and compress the nervous
filaments; and to this are to be attributed the annoying pains which
sometimes occur in a limb after the operation for aneurism. The
enlargement of the arteries of the neurilemma can be distinctly shown
by dissection.
Immediately after the operation, the circulation in the limb cannot
be so vigorous as before; its temperature is consequently diminished,
and it possesses less power of resisting the influence of stimuli. The
limb ought to be kept only moderately warm; for if too much heat be
applied, there is a risk of gangrene. The temperature afterwards rises,
and soon gets above the natural standard; the blood, from obstruction
in the internal parts, being chiefly determined to the surface. After
the collateral circulation has been completely established, the limb
regains its natural temperature.
Secondary hemorrhage is occasionally a consequence of this operation;
nor is it to be wondered at, should one ligature only be used, seeing
that this is often clumsily applied; the cellular tissue being
lacerated, and the vessel detached from its connections by the use of
blunt instruments, directors, and silver knives. When many ligatures
are employed and foreign substances placed in the wound, the patient
can scarcely be expected to escape profuse bleeding. If, however, the
operation by single ligature be properly performed, and the coats of
the artery be sound at the deligated point, the occurrence of secondary
hemorrhage must be rare. It generally supervenes when the ligature
is about to separate: at first there is a thin bloody discharge,
afterwards the quantity of blood is more copious; it is evacuated at
first in a gentle and continued stream, but afterwards per saltum,
and in profusion. The discharge not unfrequently stops for a short
time, but, on the circulation being excited, it again returns; and
the patient soon dies, unless active measures be practicable, and
immediately resorted to. Compression can be of no use; nor can
astringents, nor venesection, which I have actually seen practised in
such cases. The application of a ligature betwixt the heart and the
open point of the vessel affords the only chance of saving the patient;
the surgeon must interfere, and do what is in his power—he cannot look
on and see the patient bleed to death.
Occasionally the aneurismal sac deviates from its usual structure and
appearance. Sometimes osseous or calcareous matter is found deposited,
to a greater or less extent, in the substance of the parietes of the
sac, or between the laminæ of fibrin which it contains. The tumour
may also occupy unexpected situations, occurring after fracture of
the bones and laceration of an artery, and perhaps from more slight
external injuries. A disease of bone, somewhat resembling aneurism in
that tissue, will be afterwards noticed.
OF ANEURISM BY ANASTOMOSIS.
This disease is generally seated in the external cellular tissue. It
has been supposed to attack occasionally the internal organs; and
a case is related in which it was situated in the cellular tissue,
between128 the vagina and rectum. Frequently the congenital marks of
children, termed Nævi, degenerate into this disease: occasionally,
though very rarely, it occurs in sound skin and in adults. A good
case of this kind will be found in the Practical Surgery, p. 336.
When the cutaneous tissue is involved, the colour of the tumour is
a dark red, or inclining to purple; it is irregular on its surface,
and has a soft, spongy feel. Often it is raised distinctly above the
surrounding parts; at other times it is flat, scarcely prominent, and
seems to enlarge chiefly in a lateral direction. The skin is then
frequently unaffected; pulsation, in some instances, is perceived;
often, however, the tumour is of an inactive character, affords
no pulsation, and, on being handled, feels like a doughy, elastic
intumescence, appearing to be composed of a congeries of distended
vessels, in which the blood circulates slowly, and resembling varix.
The tumour is formed by enlargement, tortuosity, and increased activity
of the capillary and other vessels; in some cases the arteries are
chiefly affected, in others the veins. That such is its structure, can
be distinctly proved by dissection; the vessels are found enlarged to
many times their natural size, and their coats are much attenuated;
it is certainly not cellular, as some have supposed. The tissue is
similar to that of the cavernous and spongy bodies of the penis, and
has hence been named erectile. A natural structure of the same kind
is met with in the lower animals in different situations. The tumour
is much increased on the general circulation being hurried, as by
crying in children, by fits of passion, by the excitement of ardent
liquors or venery, and during or before the menstrual discharge. On
such occasions the surface frequently gives way, hemorrhage ensues,
and is often profuse; in females it sometimes takes the place of the
regular discharges. The tumour, in general, increases rapidly in
size, and bleeds from time to time; now and then, however, it becomes
stationary, even in circumstances where it could hardly be expected,
and remains so during the remainder of the patient’s life. Again, in
children, the surface of the tumour is not unfrequently ulcerated,
even to a great extent, without hemorrhage occurring; when such is
the case, the ulceration for the most part extends, with surrounding
induration and condensation of the parts. The whole or part of the
adventitious tissue may thus be destroyed; the parts cicatrise, and a
spontaneous cure is sometimes accomplished. In other cases, though the
disease is not extensive, frequent and most violent hemorrhage occurs.
A hemorrhagic tendency also occasionally occurs in affections of a
different nature,—a trifling sore pouring out blood on the slightest
touch. In some constitutions, leech-bites, trifling punctures, or the
extraction of a tooth, have been followed by dangerous hemorrhage. The
disposition very often exists in many members of the same family, and
is sometimes hereditary. Great trouble has been experienced in staying
the bleeding; large vessels have been tied without effect, and some
patients have even perished notwithstanding every exertion on the part
of the attendants. It becomes a difficult matter to treat surgical
diseases in such constitutions: openings cannot be made with the knife
for the evacuation of matter or any other purpose. A good case will be129
found in the Lancet, 1838-39.19 The same patient again presented
himself with a very large and deep abscess of the hip, which was opened
by caustic, though nearly one inch and a half from the surface. It is
not easy to account for this disposition to bleed so profusely, or
from slight causes. The blood is in a diseased state, probably as in
the patient here referred to, in whom it contained pus globules, and
coagulated slowly; there is probably also a want of tone in the vessels
themselves. Many such cases are on record. The cause, or causes, of
aneurism by anastomosis are also unknown.
In very slight cases of erectile tumour, or in nævus threatening to
assume an aneurismal action, cold and pressure are sometimes, though
very rarely indeed, sufficient for the prevention or removal of the
disease. The most effectual remedy is excision, though this can very
rarely indeed be had recourse to with safety; for when the disease is
extensive, the vessels in its neighbourhood are much enlarged, and
their action increased; so that any attempt to remove the tumour by
the knife is followed by profuse, and often an uncontrollable, flow of
blood. When excision is practicable, it ought to be accomplished by
cutting very clear of the disease; the tumour, like every other, must
be cut out, not cut into. If the incisions encroach on the substance of
the tumour, or are made in the immediate neighbourhood of the diseased
part, the tremendous bleeding which invariably ensues will convince
the practitioner of the impropriety of his conduct, and rashness of
the proceeding. Attempts have been made to arrest the progress of
the diseased action, by tying the principal arterial trunks entering
the tumour; but these have proved ineffectual, as might be expected,
considering the unusually free and numerous inosculations which then
exist. In a few instances, ligature of the carotid artery, on the same
side with a tumour on the face or head, has put a stop to the disease;
in the others, it has been unavailing.
130
When the tumour is so situated, or of such a size, as to render
the expediency of excision doubtful, it may often be safely and
expeditiously removed by ligature. In some cases the tumour is
prominent, so that it readily allows of the application of a ligature
around its base; in others, it is flat and broad; in which case, a
long needle, or needles, armed with a double ligature, can be passed
beneath it, and the ligatures can then be separated, and so disposed as
to cause sufficient constriction of the entire mass.—Vide Practical
Surgery, p. 331, 336. In many cases, incisions may be made with great
advantage, either before or after introducing the ligatures; the
diseased mass is thus more effectually included and strangled, and much
pain and deformity are avoided. The disease, however, occasionally
occupies such situations as are totally beyond reach. The application
of potass has been recommended; and this caustic is certainly
sufficiently powerful to destroy the diseased parts; but its use is
attended with danger from profuse hemorrhage. Superficial nævi may
occasionally be got rid of by the application of nitric acid, but it
requires to be applied over and over again; and, after all, some more
effectual means must probably be resorted to. Stimulating injections
into the substance of the growth have been sometimes employed. Cures,
it is said, have followed the use of setons, or the repeated puncturing
and breaking up of the tissue with a needle. None of these means are
to be depended upon. The cases are innumerable in which I have been
obliged to employ the ligature in an effectual manner, combined or not
with incision, where caustics, injections, puncturings, setons, and
even imperfectly applied ligatures, had been previously resorted to in
vain. Besides, in children there is as much resistance and crying, and
as much anxiety in parents, produced by a slight operation, as by a
more effectual one.20
OF INFLAMMATION OF VEINS.
Veins are very susceptible of inflammation, and the action is very
apt to extend along the coats rapidly; in some cases it reaches the
131right side of the heart, producing most violent symptoms, and speedy
dissolution.
Inflammation in the venous, as in the other tissues, may terminate in
resolution. Otherwise, lymph is secreted, whereby the coats of the
vessel become thickened, and its internal surface agglutinated, causing
obliteration of the canal to a greater or less extent. Suppuration
also occurs, and the pus may be deposited in a cyst formed amongst
the coats of the vessels; or, as is most frequently the case, it is
secreted from the internal coat, and occupies the canal of the vein.
It then generally accumulates, its passage into the circulation being
prevented by a deposition of lymph sufficient to occupy the calibre of
the vessel betwixt the heart and the seat of the purulent matter. The
termination in purulent secretion is accompanied with a high degree of
constitutional irritation, and typhoid symptoms, more especially if any
pus finds its way into the circulation.
The integuments in the course of the inflamed vessel or vessels are of
a dark red colour, and great pain is caused by pressure. Often there is
a considerable œdematous swelling of the limb, occasionally followed
by the formation of unhealthy pus, diffused in the cellular membrane,
causing sloughing of that tissue, or of the soft parts more deeply
seated.
This disease generally follows an accidental wound or operation, as
venesection or amputation; it is also of frequent occurrence after the
application of a ligature to the extremity of a vein. Many patients
have died of this disease, induced by the application of a ligature
to the vena saphena major, for the cure of varix. Wounding of large
veins ought to be studiously avoided; and if wounded, the bleeding
from them should, if possible, be arrested by pressure. When from any
cause the extremity of a large vein in a wound is not closed, when it
is not plugged up by plastic matter, pus seems to enter it readily, and
by mixing with the circulating fluid causes dreadful mischief; great
constitutional disturbance accompanies the purulent deposits which
follow in the solid viscera and in the joints.
Inflammation of veins is a very unmanageable disease; the exhibition of
purgatives and antimonials will be prudent, in order to evacuate the
bowels, produce diaphoresis, and diminish the force of the circulation;
the pain will also be much relieved by the application of warm
fomentations to the affected part. General depletion is not admissible
unless at the very commencement of the disease, and local bleeding
must be had recourse to with very great caution; for by copious
abstraction of blood, gangrene may be induced, or at least hastened.
The limb must be altogether disused and elevated, the patient being
kept in a state of complete rest, and not exposed to any excitement or
anxiety. Blisters have been employed, but with no good effect. If the
vein is much distended, and it is evident that it contains a confined
accumulation of pus, it ought to be treated as a common abscess, the
matter evacuated by an incision, and various dressings employed,
according to circumstances. Such practice I have found successful, and
not followed by any untoward symptoms. The abscess is often limited at
each extremity by the deposition of lymph in the canal of the vessel;
and after the evacuation of its contents, the cavity contracts, and the
portion of the vessel which has been the seat of suppuration becomes
completely impervious.
132
Inflammation of a vein is also occasionally followed by the sudden
appearance of a purulent depôt in some part of the body, external or
internal, at a distance from the inflamed part. Thus, in inflammation
of a vein in the forearm, it is not unusual to find an abscess formed
suddenly in the axilla on the opposite side; after amputation, or other
capital operation, the patient is often suddenly affected with violent
symptoms of disease in the chest, and, on examination, abscesses will
probably be discovered in the substance of the lungs, the existence of
which had only been suspected a short time previous to death. Possibly
some pus globules, the seeds of disease, may be arrested in their
course through the capillaries of these organs, and thus a foundation
be laid for mischief. A very satisfactory explanation of these
phenomena cannot readily be given.
It has already been noticed, that the softening of coagulated fibrin
must not be confounded with suppuration. The fibrinous pulp has
commonly been called pus, though erroneously; and when occurring
in the veins, as it frequently does, has been generally described
as inflammation and suppuration of the vessel. The distinction is
important; first, because many of the so-called cases of phlebitis are
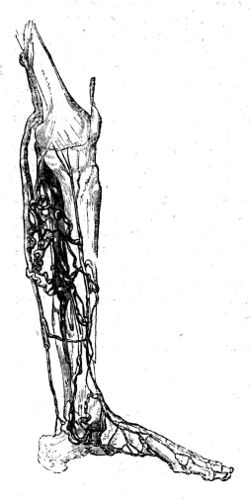 shown to be of a different nature, and secondly, as to the theory of
suppuration, on which subject many writers in this country have been
engaged in making commentaries on, and compilations of, the French
doctrines, which are not deserving of much regard.
shown to be of a different nature, and secondly, as to the theory of
suppuration, on which subject many writers in this country have been
engaged in making commentaries on, and compilations of, the French
doctrines, which are not deserving of much regard.
There exists without doubt a capillary phlebitis, and the vast
importance of inflammation, and its consequence in these vessels, will
be estimated when their great extent and functions are recollected. It
is probably in this class of cases especially that the blood becomes
contaminated with pus.
Veins frequently become dilated or varicose; they assume a tortuous
course, appear much enlarged, and present an elastic, soft feel,
except in the situation of the valves, where they are more hard and
incompressible: occasionally the tortuous windings form a bluish tumour
of considerable size. The dilatation of the superficial branches is
increased by heat, the skin being thus relaxed, so as to give less
support. The limb is swollen and œdematous. The dilatation is generally
supposed to be confined to the vessels near the surface, but it appears
that the deep-seated ramifications133 are not exempt from the affection.
When a dilated vein becomes inflamed, great pain is felt in the part;
the vessel feels like a firm chord, its coats are much thickened, and
its cavity proportionally contracted; lymph is effused, and by it the
canal may be obliterated to a greater or less extent; a spontaneous
cure is thus accomplished. In the lower limbs, the disease is often
complicated with ulcers; and as long as the veins remain varicose, the
ulcers are almost incurable, or if they are brought to cicatrise, the
skin soon ulcerates again, and the disease is reëstablished. The coats
of the vessel not unfrequently ulcerate, and blood is discharged in
appalling profusion: such an occurrence may even prove rapidly fatal.
Sometimes, though rarely, skin thinned by pressure from within gives
way without previous ulceration, and profuse bleeding ensues.
The cause of this affection is obstruction to a free return of the
blood; as by tumours, either natural or adventitious, from pregnancy,
constipation, &c.; or by the tight application of a ligature round the
limb, as of a garter. It often occurs in those who have been in the
habit of great muscular exertion, the blood being thereby forced from
the deep-seated veins into the superficial. This even occurs, though
very rarely, in the upper extremity, and I have witnessed more than
one instance of it. Here it is more readily got rid of. Dilatation of
venous branches is met with in the scrotum, labium pudendi, lower part
of the abdomen, in the neighbourhood of the anus, and at the lower part
of the neck. The lower limb is, however, the most common seat of the
disease: when the veins in this situation are dilated, the valves are
insufficient to obstruct the calibre of the vessels, and consequently
the lower and smaller ramifications have to sustain the column of
blood in the superficial veins of the whole limb, its weight not being
diminished by the support which, in the natural state of parts, is
afforded by the valves; the disease is thus more and more aggravated.
The left limb is generally the one affected; and this circumstance may
probably be explained by the pressure of the sigmoid flexure of the
colon on the left iliac vein.
In the majority of cases, the palliative treatment can only be adopted.
The limb must be used as little as possible, and, if practicable, be
kept in a state of complete rest; the veins must also be supported by
the application of a bandage, or the wearing of a laced stocking. The
Indian rubber bandage worn over the stocking or drawers answers fully
as well as any other method. In some instances, the application of cold
has been of advantage, by promoting the contraction of the dilated
vessels. When pregnancy is the cause, it is needless to commence any
method of cure, until the cause be removed; and the same remark is
applicable when the affection arises from habitual constipation. The
varices occasionally become inflamed, painful, and much swollen, with
considerable œdema of the whole limb. Their contents become coagulated,
and their coats thickened; in the end, the swelling abates and the
vessels are closed. In certain cases, this spontaneous cure, a radical
one, may be imitated by the surgeon; an escharotic being applied over
the trunk of the vein at a healthy point, whereby inflammation is
produced in the coats of the vessel, and obliteration of its cavity
accomplished: the134 caustic which will be found most convenient and
effectual, is the potassa fusa. The caustic may be made into a paste
with soap; or a solid piece, of the size of a split pea, is placed over
the vein, and there retained for a few hours by plaster or bandage. The
vessel being obliterated, the lower venous branches necessarily pour
their contents into those deeply seated; as they freely communicate
with these, they readily empty themselves of their accumulated
contents, and soon regain their calibre under the employment of
bandaging. When the varicose veins are numerous, as is generally the
case, the potass is to be applied to the healthy point of the larger
trunk in which they terminate. But the practice is not unattended with
danger, for the coats of the vessel may ulcerate in consequence of the
application, and violent hemorrhage ensue; the degree of inflammation
excited may be greater than that intended, and extend so as to give
rise to suppuration in the vessel and the most alarming constitutional
disturbance. These unfavourable results, however, must be of rare
occurrence. Success has, however, followed the practice in innumerable
instances.
A much preferable method, as being less painful and unattended with
risk, is that of passing needles under the vessel, and twisting a piece
of thick and strong silk round them. Two needles should be applied
together, at an interval of about half an inch, at whatever points it
is thought right to close the vein. Coagulation takes place in the
included part, and also frequently for some distance below it; the
coats of the vessel are thickened, and its canal closed. The needles
are withdrawn before they begin to cut their way out by ulceration,—say
at the end of from three to five days,—according as the parts become
condensed. The needles suited to the purpose are soft, but tempered
at the point, which is spear-shaped; the ends are cut off with pliers
after the thread is fixed. Other operations have been performed on the
veins, to procure a radical cure of varix; one or more ligatures have
been passed round the vessel, as in the operation for aneurism; and the
vessel has been divided, or a portion of it dissected out, and its cut
extremities afterwards either compressed or secured. Such proceedings
are now almost entirely abandoned.
OF TUMOURS.
A tumour is a swelling or new production, and not a part of the
original composition of the body. Blood may have been effused, and the
coagulated part, becoming organised, is increased in size by deposits
from the vessels which enter it; or perhaps the blood, the coloured
part of it at all events, is taken up and lymph is deposited, which,
if not also removed, “undergoes further changes of a secondary nature,
and remains a parasite or new structure.” Its structure and growth
are modified according to the action which its own vessels assume,
independently of the surrounding vascular system. The bloodvessels may
enter this new growth by a narrow135 pedicle; or it may be of such a
form as to present an extensive surface, by which it communicates with
the surrounding parts, receiving vascular ramifications from them. As
the growth of the tumour proceeds, the surrounding parts yield, are
condensed, and form an envelope for the new formation; the neighbouring
bloodvessels are excited to a greater degree of action, and more
blood is poured into the vessels of the tumour; the action of these
in turn is very vigorous, and the increase of the new growth is more
and more rapid. They become, it would appear, dilated and tortuous.
Morbid enlargement, or rather new productions, often attain an enormous
size; some have weighed, when recent, upwards of 60 or 70 lbs. Tumours
differ much in structure; and though their general appearance may not
be dissimilar, one will scarcely be found exactly resembling another.
In many cases, the external appearance proves no certain index of the
nature of the tumour; sometimes, however, its feel and general external
character lead the experienced surgeon to form a correct estimate of
its internal structure. It is impossible, by any process of reasoning,
to account for the different actions which these growths possess; and
even minute anatomical investigation, either of healthy or morbid
structures, has not as yet thrown much light upon the subject.
Tumours are divided into Solid and Encysted. The solid are
generally enveloped by a dense cellular sheath of the surrounding
cellular substance, yielding and becoming condensed in proportion
as the tumour increases in size; this covering appears as a barrier
between the healthy and diseased parts, shutting out the latter, as
much as possible, from connection with the rest of the body, and
preventing the former from participating in the injurious tendencies
of the latter. Some tumours have no such limit, but extend in the
direction where there is the least resistance, hold a free intercourse
with the surrounding parts, and impart to them their morbid disposition
and action; others are limited in their situation and communications,
but prove dangerous or annoying from their bulk. Some grow rapidly,
and prove troublesome in a few weeks or months; others remain without
much increase for years, and produce little or no inconvenience.
Occasionally tumours partly resemble the texture in which they grow;
those of a fatty nature are frequently found to have their nidus in
the adipose tissue; cartilaginous tumours project from the surfaces
of bones or of a joint, are subsequently detached, and lie loose in
its cavity; growths of a cellular structure internally, and invested
by an apparently mucous lining, protrude from the surface of mucous
membranes. Others differ, not only from the texture in which they are
situated, and from which they derive their nutritive vessels, but
also from every other part of the healthy structure. In one instance,
a congenital tumour was found to be composed of an aggregation of
numerous materials, many of them resembling the healthy textures of the
body. But again, tumours are constantly met with, composed of matter
which in no respect resembles any of the natural tissues of the body:
those are what have been called heterologous formations.
The simple tumour is mere enlargement of a part, from the infiltration
of solid matter deposited by its bloodvessels. There can136 be little
doubt that the action which lays the foundation of such enlargement is
inflammatory: in consequence of inflammation of the tissue, lymph is
effused into the cellular substance during the progress of the incited
action; and after it has subsided, the dilated and debilitated vessels
probably do not regain their condition, as to size and vigour, but
remain somewhat dilated, and continue to free themselves from portions
of their contents; thus the cellular tissue is opened out in proportion
as the infiltration advances, and the process may be occasionally
accelerated by fresh attacks of subacute inflammatory action. The
patient at first feels pain, heat, &c., as in an inflammatory tumour;
these afterwards abate, and ultimately go off entirely; and during the
increase of the swelling, little or no pain is experienced, unless
when these subacute inflammatory attacks supervene, and then it is
but slight; or unless the enlargement be resisted by an unyielding
structure, and then it is acute and troublesome. The size and rapidity
of increase in such tumours will vary according to circumstances; the
vessels of the part soon regain their size and action, either by the
efforts of nature or of art, so that the tumour will have attained
no great size, and be stationary in its progress, being denied the
materials necessary for its increase. If the morbid action be thus
stopped, the absorbents will remove the newly-formed matter, and
restore the parts to their healthy condition. But when the deposition
proceeds in a superior ratio to absorption, the new matter becomes
organised, and by means of its own vessels, secretes a substance
similar to itself, whereby the increase of the tumour becomes more
rapid, and the new structure may attain an enormous bulk. Thus the
tumour is formed, not merely by dilatation of capillary vessels, and
extension of its original tissue, but by the formation of new matter,
which, becoming organised, assumes a secreting power. At first the
former circumstance is the chief cause of the enlargement; but after
the latter process has existed for some time, the tumour loses much of
its resemblance to the primary tissue, assumes a more dense structure
and a different action, and therefore cannot be designated a simple
enlargement.
This species of tumour, or rather this enlargement which precedes
the formation of a tumour, is chiefly met with in the cellular and
glandular structures. Sometimes it is described under the term of
œdema solidum. In the scrotum, where the cellular tissue is remarkably
loose and extensile, such tumours attain a very large size. They are
found in this country, though more frequently in warm climates. I
removed one from this situation successfully, which weighed upwards
of 44-1/2 lbs.; it had been of twelve years’ duration, and caused
much inconvenience to the patient. It is sketched in the Practical
Surgery, p. 341. It occurs in the mamma, apparently in consequence of
suppression of the menstrual discharge; the gland becomes enlarged,
there is no pain in the tumour, and it feels soft and doughy. When the
subcutaneous cellular tissue is the seat of the disease, the tumour is
often of considerable extent, but rarely forms a great protuberance.
It sometimes is situated in the coverings of the nose, which, as they
become enlarged, lose their natural colour, and assume a purple hue;
the mucous follicles also are often much enlarged, and occasionally
emit a profuse discharge of their secre137tions. It can be readily
understood that in this situation the tumour is a source of much
annoyance, from its partially obstructing respiration, and even vision,
interfering with the functions of the parts and the comfort of the
patient.
It has been already observed, that when simple enlargement exists for
some time the structure changes. It becomes more dense, and assumes a
peculiar action, independent of that of the surrounding parts. It has
a harder and more firm feel, and all traces of the texture in which it
was formed are destroyed. It may be considered as the next in order to
the one already mentioned, both as to the simplicity of its structure
and action; but in consequence of its action being independent of
those of the neighbouring parts, and liable to change from even slight
causes, it is very apt to degenerate into those tumours which are more
complex and injurious.
ADIPOSE TUMOURS.
Another species of tumour seems to be composed almost entirely of fatty
matter insinuated amongst extended and delicate cellular substance, and
has been therefore termed adipose. It is surrounded by a cyst of dense
cellular tissue, and to this it loosely adheres; its bloodvessels are
few, and it is of an inactive and innocuous character. It is generally
lobulated, and often attains a large size. It is not only irregularly
prominent on its outer surface, but in its whole circumference, and
its lobuli often insinuate themselves to a great depth amongst nerves,
bloodvessels, and other important parts; owing to this circumstance
they frequently prove a source of the greatest inconvenience from
their bulk, for of themselves they are neither hurtful, nor possess
any disposition to involve those parts with which they are in contact.
This tumour is found only in the cellular and adipose tissues. From
its loose connection with its envelope, it admits of ready removal by
operation. A tumour of this kind is here represented, which, but for
this circumstance, owing to its awkward situation under the tongue,
could not by any possibility have been extirpated. It is fully larger
 than an orange, and had caused very great suffering. It is not so much
lobulated as fatty tumours generally are. The adhesions of adipose
tumours are, however, rendered firm and more numerous by pressure or
external stimulants—in fact, by whatever induces inflammatory action
in its substance or in its surrounding connections; and from this
cause the extraction is often rendered exceedingly difficult. The skin
becomes thickened and of a red hue, and the tumour itself is much more
vascular. From this cause it is apt to assume a138 new mode of action,
and to change in structure and in character, invariably for the worse.
I have removed a few tumours, originally of this benign species, but
which had apparently degenerated and assumed a malignant action. In
one, distinct indurated bands radiating from a central mass of the same
kind, are discernible. In two others, as a consequence of pressure,
condensation and ultimate softening had occurred. The largest alluded
to was removed from betwixt the shoulders of a soldier, and had borne
the pressure of his knapsack for eight or ten years. It was attached by
a thickish neck, presented the common lobulated appearance of adipose
sarcoma; but its external surface, its feel, and section, were very
different.
than an orange, and had caused very great suffering. It is not so much
lobulated as fatty tumours generally are. The adhesions of adipose
tumours are, however, rendered firm and more numerous by pressure or
external stimulants—in fact, by whatever induces inflammatory action
in its substance or in its surrounding connections; and from this
cause the extraction is often rendered exceedingly difficult. The skin
becomes thickened and of a red hue, and the tumour itself is much more
vascular. From this cause it is apt to assume a138 new mode of action,
and to change in structure and in character, invariably for the worse.
I have removed a few tumours, originally of this benign species, but
which had apparently degenerated and assumed a malignant action. In
one, distinct indurated bands radiating from a central mass of the same
kind, are discernible. In two others, as a consequence of pressure,
condensation and ultimate softening had occurred. The largest alluded
to was removed from betwixt the shoulders of a soldier, and had borne
the pressure of his knapsack for eight or ten years. It was attached by
a thickish neck, presented the common lobulated appearance of adipose
sarcoma; but its external surface, its feel, and section, were very
different.
The patient does not complain of any pain or uneasiness in the
tumour, unless inflammation be excited in it; then the pain and other
symptoms are such as attend incited action, and the sensations which
are afterwards experienced vary according to the character which the
tumour assumes. Certain changes may occur in its texture, though
not in its general character or disposition; thus osseous or earthy
matter is occasionally deposited in some part of the tumour, while
the surrounding adipose substance retains its appearance and density.
Suppuration, it is said, has followed inflammatory action, excited in
an adipose sarcoma.
OF FIBROUS TUMOURS.
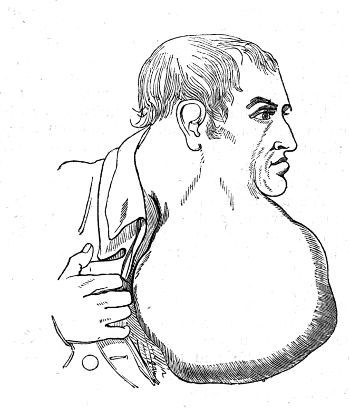
Fibrous tumours are not uncommon, and are formed in various textures.
In general they are composed of a substance of a dirty139 grey colour and
considerable density, through which minute, firm, ligamentous fibres
ramify; in some cases irregularly, in others radiating from the centre
of the tumour. The new formation is surrounded by condensed cellular
tissue, to which it intimately adheres, and does not mingle irregularly
with the surrounding parts; in this respect differing from malignant
tumours, which occasionally contain fibrous matter. It cannot be
considered of an equally innocuous nature with those already described,
but is still, in its original state, not of a malignant disposition.
After some time, the consistence and structure of such tumours vary:
some are of a loose texture, and contain cells; others are hard, and
intermixed with cartilaginous matter, or even with bone. In general,
the tumour is slow in its progress, though it may attain a very large
size, as seen in the cut on the preceding page, if allowed to remain;
occasionally its growth is rapid.
Besides those tumours which have been described, there is a number of
others not of a malignant disposition, which are so various in their
structure as to baffle all attempts to reduce them to a scientific
classification. Some are composed of a homogeneous substance of
almost cartilaginous consistence and a whitish colour; some consist
of cartilaginous matter, mixed with substance of less density and
of a different appearance; in some, fibrous matter is mixed with a
homogeneous glandular-looking substance, partially softened. Some are
almost entirely composed of osseous matter; others contain it in small
proportion. It would be endless to enter into a minute detail of the
structure of such tumours, for it may be said that their appearances
vary with their number. In almost all tumours cysts are found, and the
internal structure of some tumours consists almost entirely of cysts,
or hydatids, as they have been called; in others, these only occupy
certain parts, and compose but a minor feature in the structure. The
sacs are generally lined with a delicate and smooth membrane, which is
often vascular at various points; some contain a transparent and glairy
fluid, albuminous or gelatinous; some bloody serum; some purulent, some
curdy matter, or this mixed with a serous or purulent fluid; some pure
blood; some a fluid like printer’s ink; and not a few are occupied by a
dense elastic substance, which, on a section being made of the tumour,
rises irregular and ragged above the cut surface. Some tumours are
smooth; others lobulated or tuberculated.
OF ENCEPHALOID TUMOURS.
The tumour which comes next to be described is decidedly malignant.
It is the Encephaloid, or Medullary Sarcoma. Although these tumours
have been called encephaloid and medullary, it must not be understood
that their intimate structure has any relation to that of the brain or
marrow; for this reason the old term fungoid is perhaps a preferable
one, since it leads to no false notion as to their nature, while
it expresses a condition which at one time or other is remarka140bly
characteristic of them. This tumour consists of a homogeneous matter,
resembling the substance of the brain in colour and consistence It
rarely has a distinct cyst; occasionally it is subdivided by membranous
bands. It is always soft, though often more so in some parts than in
others; portions of it being frequently so much softened and broken
down as to resemble thick cream in consistence, and these are generally
of a darker colour, from being mixed with a greater or less quantity
of effused blood. Partial or universal softening only occurs after
the tumour has existed for some time, for in its original state its
structure and density are uniform throughout; and, on making a section
of it, some few drops of blood may escape from vessels, the coats of
which are of a very delicate nature. Some of these vessels seem to give
way, in consequence of the process of softening, for we frequently
meet with fluid blood, or masses of fibrin, in the midst of the pulpy
matter; and, when the softening has been extensive, the blood is
diffused throughout the whole substance of the tumour, so that it will
appear to be chiefly, or entirely, composed of effused and degenerated
blood, as here represented.
 The mamma and testicle, and the contents of the orbit in children, are
the most frequent seats of this disease; it not unfrequently occurs
in the lymphatic glands, and few textures can be considered as exempt
from it. The part at first enlarges slowly: but afterwards the disease
advances with great rapidity, involving the adjacent parts. In general,
the affection is not attended with much pain; the part has a spongy and
elastic feel, and frequently presents an obscure sense of fluctuation,
indicating that softening is more or less begun. The skin is tense,
generally brownish, and is pervaded by large venous branches. This
venous enlargement is always observable in the advanced stage of the
disease, before or after ulceration has taken place; it is peculiarly
evident in the eyelids, when the contents of the orbit are involved,
and is to be attributed to obstruction of the circulation in the deeper
vessels. The tumour is increased by the surrounding parts assuming
a similar action, and being converted into a similar mass; and the
disease also seems to be propagated by means of the absorbent system,
and by the irritation conveyed along the vessels which emanate from
the tumour, or from its immediate vicinity. Thus, when the testicle
or mamma is affected, the lymphatic glands, both above and below the
tumour, and the course of the absorbent vessels, are converted into
an encephaloid mass, all traces of their glandular structure being
completely destroyed. The same brain-like or cancerous matter is also
found in the bloodvessels, large and small. When the disease has been
of long duration, the superincumbent integuments appear tense, assume
a purple colour, and ultimately ulcerate; a portion of the pulpy
mass then protrudes, of a fungous141 appearance, the resistance being
at that point removed, and the compressed matter relieving itself by
the extension of a portion of its substance; the protruded portion
afterwards becomes discoloured, and sloughs, to be speedily reproduced
either by further dilatation, or by actual increase of the tumour;
unhealthy pus is discharged, often mixed with blood, and occasionally
slight hemorrhage occurs; the integuments become further ulcerated,
assume a dull brown colour widely around, and are undermined,
presenting a boggy feel.
The mamma and testicle, and the contents of the orbit in children, are
the most frequent seats of this disease; it not unfrequently occurs
in the lymphatic glands, and few textures can be considered as exempt
from it. The part at first enlarges slowly: but afterwards the disease
advances with great rapidity, involving the adjacent parts. In general,
the affection is not attended with much pain; the part has a spongy and
elastic feel, and frequently presents an obscure sense of fluctuation,
indicating that softening is more or less begun. The skin is tense,
generally brownish, and is pervaded by large venous branches. This
venous enlargement is always observable in the advanced stage of the
disease, before or after ulceration has taken place; it is peculiarly
evident in the eyelids, when the contents of the orbit are involved,
and is to be attributed to obstruction of the circulation in the deeper
vessels. The tumour is increased by the surrounding parts assuming
a similar action, and being converted into a similar mass; and the
disease also seems to be propagated by means of the absorbent system,
and by the irritation conveyed along the vessels which emanate from
the tumour, or from its immediate vicinity. Thus, when the testicle
or mamma is affected, the lymphatic glands, both above and below the
tumour, and the course of the absorbent vessels, are converted into
an encephaloid mass, all traces of their glandular structure being
completely destroyed. The same brain-like or cancerous matter is also
found in the bloodvessels, large and small. When the disease has been
of long duration, the superincumbent integuments appear tense, assume
a purple colour, and ultimately ulcerate; a portion of the pulpy
mass then protrudes, of a fungous141 appearance, the resistance being
at that point removed, and the compressed matter relieving itself by
the extension of a portion of its substance; the protruded portion
afterwards becomes discoloured, and sloughs, to be speedily reproduced
either by further dilatation, or by actual increase of the tumour;
unhealthy pus is discharged, often mixed with blood, and occasionally
slight hemorrhage occurs; the integuments become further ulcerated,
assume a dull brown colour widely around, and are undermined,
presenting a boggy feel.
Along with these local symptoms, there is a complete subversion of the
system,—there being at first symptoms of constitutional irritation,
afterwards those of hectic and extreme exhaustion. When the lympathic
glands are diseased, the limb beneath is much swollen from œdematous
effusion, the return of the blood and lymph being prevented; violent
and excruciating pains are experienced in the course of the nerves
of a limb; it also frequently loses its sensation, from those organs
being either involved in the disease, or pressed on by the tumour.
The vessels in the neighbourhood of the affected parts are materially
altered, though they are seldom converted into encephaloid matter; the
arteries are often completely obstructed by coagulating lymph for a
considerable extent, and the coagulum not only occupies the principal
trunk, but extends into the minute ramifications; and this explains
why hemorrhage seldom occurs, even after ulceration of the tumour is
far advanced; the veins also are frequently obstructed in a similar
way; but in many cases they contain a soft and pulpy matter, exactly
resembling the substance of the tumour. The fungus which protrudes
after ulceration of the integuments sometimes bleeds, when it would
appear that the hemorrhage proceeds from those bloody collections
in the substance of the tumour already mentioned. According to my
experience, when bloody points, or cysts containing bloody fluid,
exist in a medullary or other tumour which has been removed, and if
the diseased matter be reproduced, a bleeding fungus will almost
certainly follow. This species of tumour occurs in all ages and in all
situations, and during its progress evinces strong proofs of inveterate
malignancy: if removed early, the disease may be arrested; but if the
operation be long delayed, a tumour of a similar nature, and more
extensive, will almost invariably be produced. In several instances
I have removed encephaloid tumours, from the situation both of the
mamma and testicle, and the disease did not return; but in the other
cases the result has been as above stated. Encephaloid disease of the
internal organs frequently supervenes on that of the external parts,
and accelerates the patient’s dissolution; when in such situations they
are beyond the reach of surgical art, and their existence is only, if
at all, ascertained, in order to enhance the unfavourable nature of the
surgeon’s prognosis.
142
OF MELANOID TUMORS.
The Melanoid tumour is rather of rare occurrence in the human subject;
it originates in the cellular tissue, and most frequently attacks the
internal viscera; sometimes it occurs in the eyeball, where it has been
seen with the encephaloid disease, and occasionally melanotic matter is
diffused amongst the cellular tissue throughout the whole body, even
in that of the bones. The external surface of the tumour is generally
of a shining and mottled appearance; internally it consists of a
homogeneous black matter infiltrated into the cellular tissue, which is
condensed, and in some cases distinctly increased in vascularity. The
tumour, seldom of a large size, extends chiefly in a lateral direction.
Occasionally it is pretty firm; in other instances it is soft, broken
down, and semifluid. The melanotic matter is not always so deposited
as to form a distinct tumour, but frequently seems to be sparsely
infiltrated into the cellular tissue; and occasionally it is diffused
in so minute a quantity as merely to tinge the part, or form dark
streaks. Sometimes it is infiltrated in the substance of an organ, and
sometimes it is effused on its surface; occasionally it is surrounded
by a distinct delicate sheath; usually it is confined by no envelope,
excepting the partial condensation of surrounding parts. In the skin
it sometimes presents in a tubercular form. The tumour is said to be
chiefly composed of albumen, mixed with a peculiar colouring matter.
The disease mostly occurs in the trunk, seldom in the extremities;
it is not uncommon in the orbit, and in the internal organs the
melanotic deposits are generally both numerous and extensive. There is
seldom pain, and the patient seems to suffer chiefly from lassitude
and extreme debility, which gradually increase; anasarca frequently
supervenes; the functions of the organs affected are much impeded, or
even altogether destroyed, and thereby the sinking of the powers of
life is accelerated according to the viscera affected and the extent of
the disease. Melanosis occurs most frequently in advanced life, though
it is not confined to it; whereas encephaloid attacks indiscriminately
all ages.
OF CARCINOMATOUS TUMOURS.
The most malignant and intractable of tumours is the Carcinomatous.
This term is applied to the disease in its occult state, whilst Cancer,
a term pretty indiscriminately employed, may denote its condition
after ulceration. The word scirrhus is often used synonymously with
carcinoma; but the former has been, and still is, improperly employed
to denote indurations and enlargements of structures in all situations,
and has been altogether so much abused as to warrant its being erased
from the nomenclature of diseases. Carcinoma seldom occurs before the
age of thirty, and generally not till a later period of life; there are
instances, however, of its appearance at143 a much earlier period. Very
frequently it is not primary, but supervenes on adventitious formations
originally of an innocuous character, and which might have long
remained so. All tumours, though at first not of a hurtful tendency,
are liable to assume malignant action, either from a constitutional
cause, from external injury, or from latent disposition. When it
occurs in newly-formed parts, the surrounding cellular substance is
frequently condensed and thickened, so as to form a cyst round the
tumour; and when it supervenes on chronic tumours, the cysts which
enveloped these remain, for some time, as entire and distinct as
formerly, though the character of their contents is remarkably changed.
Afterwards the cyst may be contaminated with the same disposition as
its contents, assume the same action, and be converted into a similar
substance. When the disease is seated in the lymphatic glands, the
cyst is at first distinct, and gradually disappears; whilst in this
affection of the conglomerate glands a cyst is at no time perceptible,
and the cancerous matter insinuates itself, and is lost, in the
surrounding substance. The carcinomatous tumour is of great density,
and communicates a peculiarly grating sensation and noise when cut. In
its section there appears a central point, or nucleus, from which dense
ligamentous bands of a white colour proceed towards the circumference,
diverging in regular succession, as rays of light from a luminous
body; or the larger bands subdivide into smaller ones, which follow
a similar course with their parent trunk, or ramify regularly; or,
from the first, follow an irregular and intricate course, uniting with
and crossing one another, so as to present a retiform appearance. In
general, the interposed substance is of a greyish colour, extremely
dense, and generally homogeneous, though sometimes granular. Often
the ligamentous bands are so numerous, and so intimately interwoven,
as to leave little or no room for any intervening substance.
Sometimes, and most frequently in the advanced state of the tumour,
the greyish matter appears to have been broken down and removed,
its situation being occupied by a glairy or turbid fluid, by a soft
pulpy substance, or by blood; the parietes of such cysts are formed
by the whitish bands, which sometimes appear to be much thickened,
and coated with a membranous lining. The term gelatiniform cancer has
been applied to that kind in which the reticulated texture is filled
with glairy-looking fluid. Frequently, as has been already observed,
the external cyst or covering becomes assimilated to the substance
of the tumour, and the ligamentous bands then shoot forward into
the surrounding tissues, more especially the cellular and adipose,
establish a new footing for the disease, and thereby gradually enlarge
the boundaries of the original tumour. All parts in its immediate
neighbourhood become affected, and none withstand its morbid and
destructive influence; bone, muscle, ligament, skin, and membrane, are
successively or simultaneously involved; and even the bloodvessels and
nerves. From what has been already said, it is almost superfluous to
add that the tumour is most malignant, incessantly encroaching on the
neighbouring parts, and imparting to them its own disposition; and this
too frequently continues to exist after the removal of the primary
source of the evil. The disease, in its commencement, occupies a144
minute and limited space, composed, it has been said, of enlarged and
varicose capillaries, interspersed with the peculiar matter of cancer.
It would even seem that these dilated aneurismal or varicose vessels,
in morbid growths, are from the first gorged with what has been called
heterologous matter. Judging from the imperfect account which has
yet been given of them, it would appear, from the observations of
Mr. Kiernan, that cancerous growths are entirely vascular in their
early stages,—composed, in fact, of capillaries filled with cancerous
matter, which shoot from the free surfaces of membranes in a flocculent
or villous form, having no albuminous matrix, as has been commonly
imagined in regard to adventitious growths generally; the progress
of the cancerous tumour appearing to depend on the multiplication of
the capillaries, their becoming remarkably varicose, tortuous, and
dilated, the dilatation being accompanied by thinning, by more or less
absorption of their coats, so as to allow of the escape partially of
the accumulated matter from their cavities. Thus may be formed a tumour
of unlimited extent. As the secerning vessels are excited to undue
action in all cases where they have to form and supply preternatural
growths, it is to be expected that they will in such cases become
enlarged. Accordingly, the enlargement both of the smaller arteries
and veins in tumours, generally, is a fact with which surgeons who
have been in the habit of operating on such parts must be familiar.
Farther, the enlargement of the capillaries in inflammation has been
shown by the experiments of Hastings, and Thompson; and Mr. Gulliver,
who informs me that he has seen pus in the capillaries of a suppurating
surface, remarks, in regard to the observation of Professor Müller, as
to the capillaries having only the diameter of a blood corpuscle, that
these vessels become during suppuration sufficiently dilated to admit
of rows of pus globules. Thus, during the formation of an ordinary
product of inflammation, the capillary vessels are enlarged; and if
excited to still further activity, and for a more protracted period, in
the nutrition and formation of tumours, the minute vessels will become
still more dilated, and filled with other materials than purulent
matter. In a melanotic eye, which I lately examined with Mr. Dalrymple,
there was a part in which the black matter seemed to be contained
within the capillary vessels.
The cancerous tumour afterwards presents a stony hardness, is generally
of a globular form, and irregular and unequal in its surface. At a
still later period it gradually enlarges, in the way already mentioned,
remains moveable for some time, but ultimately becomes fixed by the
increased extent of its connections. By these circumstances it may,
in general, be distinguished from the tumours which, from the first,
occupy a wide space, and are firmly fixed by intimate connections
with the surrounding parts. When the tumour has once been developed,
its progress is slow and steady, being arrested, or made to recede,
neither by the efforts of nature nor by the interference of art. Pain
is generally complained of in the region of the tumour, and is of a
lancinating kind, compared by the patient to the passing of sharp
instruments through the part; occasionally, however, there is no pain
in the new formation, and little inconvenience is145 caused by it. When
the disease is left to itself ulceration occurs, frequently at an
early period; but sometimes only after the tumour has been of long
duration. The superimposed integuments appear stretched, change their
natural colour, assume a dusky or livid hue, become attenuated, and
ultimately give way; the breach of surface not being caused by tension
and pressure, but by the parts having assumed an action similar to that
of the tumour. The ulcerated point slowly enlarges, a thin ichorous
fluid is discharged, the surrounding integuments are of a dusky red,
and the margins of the ulcer are thickened, callous, everted. Whilst
the destructive action proceeds in a lateral direction, it at the
same time advances towards the more deeply-seated parts, the cavity
becomes excavated, irregular, and ragged; and the parts seem to be
destroyed partly by ulceration and partly by sloughing. The exposed
surface seldom aims at reparation; and when it does, the granulations
are greyish, hard, warty, and endowed with but little vitality; never
investing the whole surface, but protruding from certain points,
and presenting somewhat of a fungous character. The thin unhealthy
discharge becomes profuse, and exhales a peculiarly fetid odour, highly
offensive to the patient and attendants. By these means the ulcerated
cavity may attain an enormous size, presenting a most disgusting
and lamentable spectacle. If the patient bear up under the profuse
discharge, the greater part of the original tumour may be destroyed by
the ulceration, and some attempts may be made at cicatrisation; that is
to say, the cavity may contract, and granulations be formed: but these
are always unhealthy, and, in fact, carcinomatous, and often bleed
profusely. New skin is seldom formed, the remaining parts resume their
virulency, and the process of destruction again advances, surpassing
the former both in extent and rapidity.
Along with these local symptoms and appearances, it can be readily
understood that the constitution is, from the first, materially
affected. The alimentary organs are deranged in function, the patient
has a wan and sallow countenance, and is in general weak and much
 emaciated. After ulceration, the system is still more reduced by the
discharge, the patient becomes hectic, and is often afflicted with
diarrhœa; along with the other symptoms of extreme debility, the
patient may become anasarcous, is affected with cough and dyspnœa, or
by other symptoms indicating disease of some internal organ, and is
ultimately carried off in a state of exhaustion.
emaciated. After ulceration, the system is still more reduced by the
discharge, the patient becomes hectic, and is often afflicted with
diarrhœa; along with the other symptoms of extreme debility, the
patient may become anasarcous, is affected with cough and dyspnœa, or
by other symptoms indicating disease of some internal organ, and is
ultimately carried off in a state of exhaustion.
The disease attacks various textures, but perhaps most frequently the
mammary gland. The mamma generally diminishes in size from absorption
of the fatty matter; the nipple is retracted, often to a great
degree, and the surrounding integuments are of a purplish hue, and
exude a sanious fluid; at length the nipple is completely destroyed
by ulceration. In other146 instances the tumour is large, and there is
a hard œdema of the integuments; the skin is thick, coarse, and of a
dark red colour. The tumour soon adheres immoveably to the subjacent
muscles and ribs, converting the contiguous portion of the former into
a substance similar to itself. There may be other varieties in the
appearances and symptoms of carcinoma; but the above are those which
are most frequently observed, and are sufficient to denote the general
character of this species of tumour, and to show its peculiar and
inveterate malignancy.
Ulcers or swellings, at first simple, may assume a malignant action,
either carcinomatous or of another kind; thus, in one instance,
a simple ulcer, produced by a burn, assumed a foul and unhealthy
aspect; and ultimately degenerated into a most malignant sore. Various
malignant actions commence in glands of the conglobate or conglomerate
kind, at first simply enlarged from irritation or injury. The female
breast often becomes indurated from a blow, or from milk abscess, and
remains for a series of years, half a lifetime perhaps, without any
perceptible change in the enlargement and induration; but the tumour
frequently is roused into activity at the critical time of life, and
malignant action ultimately commences. The menstrual period ought to be
particularly attended to in affections of the mamma more especially,
but also in all tumours and ulcers; for both during and before it
tumours become larger and more painful, the whole system appears to be
excited, then relaxed, and all morbid actions seem to possess increased
activity.
In this disease, as in soft cancer, as it has been called, (and
they occasionally pass into each other,) the bloody masses, or sacs
containing bloody fluid, are to be dreaded, and when they exist are
to be considered as very unfavourable; for if, on the removal of a
carcinomatous tumour, such appearances be found, the disease will
certainly return; a new tumour, of even a worse character than the
preceding, will be formed; a fungus will be protruded, and from this
hemorrhage will occur.
The lymphatic glands, both above and below the tumour, generally
enlarge early in the disease, become hard, and cut like cartilage,
and with a grating noise. Frequently they become converted into a
dense and fibrous substance, resembling carcinoma; sometimes they are
softened and broken down at several points, and contain a purulent or
bloody fluid. They enlarge, coalesce, and form irregular masses, which
rise more and more above the surface; the superimposed integuments
give way, and then occur those destructive ravages by ulceration and
sloughing already described. The lymphatic vessels entering these
tumours and emerging from them feel hard and wiry, as if thickened.
The integuments in the neighbourhood of the tumours, and in the course
of these absorbents, are of a blue colour, and the veins enlarged and
tortuous; the limb below the enlargement swells and is œdematous. The
absorbents often become affected months or even years after the removal
of the original and exciting tumour; the immediate cause being taken
away, yet the inherent disposition to malignant action is too often
left, not to be eradicated. In fact, the disease generally returns,
either in the original integuments,147 in the form of tubercles or buds,
in the cicatrix, or in the glands; very frequently all are affected. It
seems also to spring not unfrequently from fascia. Such enlargements
of the glands have been said to arise, in the first instance, from
irritation, and not from any participation in malignant action; and on
this supposition, though in general extremely incorrect, cruel, bloody,
and unnecessary operations have been performed.
Cancer seizes either the mucous or the cutaneous surface, with hardness
and a warty excrescence; this ulcerates, and is surrounded by a
hardened base. The process of destruction advances, and the ulcerated
part presents the same appearances as those of a sore arising from a
similar action in a deeply-seated carcinomatous tumour. The glands also
enlarge, and assume the same aspect as if they had been the original
seat of the disease. Some pathologists seem disposed to deny this, but
apparently on no very sufficient grounds.
FUNGUS HÆMATODES
Has been much confounded with medullary sarcoma, but the two diseases
are materially different. Fungus hæmatodes almost always supervenes on
other morbid formations, when they have been ulcerated and exposed;
and the particular formation which most frequently precedes is the
medullo-sarcomatous; a bleeding fungus, however, occasionally protrudes
from tumours of a different character, which, though they may have been
at first simple, have degenerated, ulcerated, and assumed a malignant
action. The disease certainly does not occur so frequently as some have
asserted; for many, instead of limiting the application of the term
to those fungous protrusions which bleed, honour with the appellation
of fungus hæmatodes every growth which protrudes after the ulceration
of a tumour, and every tumour which is unusually prominent, of soft
consistence, and of a somewhat fungous appearance, although such have
never shown any disposition to bleed, either spontaneously, or from
irritation. But fungus hæmatodes, as the name implies, is truly a
fungus which resembles blood; and as bloody or blood-like tumours are
formed from the rupture of some vessel of rather a large size, and
as they almost invariably evince a tendency to profuse hemorrhage,
as a necessary consequence of the mode of their formation, the term
is correctly applied only to those fungous growths which either have
at one time emitted a discharge of blood, and exhibit symptoms of a
recurrence of the hemorrhage, or which frequently pour out a quantity
of blood, sometimes inconsiderable, but often profuse, and generally
altogether uncontrollable. In short, the circumstances necessary to
entitle a morbid formation to the appellation of fungus hæmatodes are
a fungous structure and appearance, and hemorrhage proceeding from it
to a greater or less degree, and with more or less frequency. Fungi are
frequently met with, but there are certainly few hæmatoid fungi.
The excrescence is generally of a dark colour, resembling a mass of
coagulated blood, but of more soft consistence, and its extremity148 has
often a sloughy appearance. It is evidently organised; for, on being
injured even in a very slight degree, hemorrhage ensues from the part
which has been broken or contused, and frequently the growth bleeds
spontaneously. At first the hemorrhage is in general slight, but is
often repeated, becomes very profuse, and in most instances cannot be
arrested. The vessels in the substance of the morbid mass are diseased
in their coats, and have altogether lost their power of contraction;
they give way either spontaneously or by laceration, and by their
non-contraction they appear to serve merely as passive tubes, through
which the blood is poured out by the active vessels which supply them;
the latter are not exposed to any of the causes which tend to produce
speedy obstruction of their canals, therefore continue to transmit
their contained fluid through their subservient branches, and from this
the uncontrollable nature of the hemorrhage can be accounted for; from
the number of vessels which supply the new structure, and which are
thus employed, it can be readily imagined that the hemorrhage will be
profuse. In many instances, the application of firm pressure on the
limb above the seat of the disease is even insufficient to arrest the
flow of blood; and though this may, in some degree, be explained by
supposing the continued stream to be venous, still it must be confessed
that the disease appears connected with a peculiar hemorrhagic
tendency. Frequently the fungus is found to communicate with, or rather
to arise from, numerous cysts of a glossy appearance, from which also
blood is copiously effused. The surrounding tissues are completely
disorganised in the immediate neighbourhood, and also much altered in
structure for a considerable extent around; the muscles, besides their
disorganisation, have acquired a peculiar brown hue. Sometimes the
hemorrhage does not seem to proceed so much from the fungus as from
the subjacent cysts; for when a superficial incision or puncture is
made into it, the bleeding is often inconsiderable, and only becomes
alarming after masses of coagulated blood have been removed, and the
cysts thereby exposed. Occasionally the fungus communicates with a
cavity of enormous size, filled with blood, partly coagulated and
partly fluid, and from the parietes of which the hemorrhage proceeds.
When the disease has supervened on a medullo-sarcomatous tumour,
the coagulated blood is mixed with a substance resembling the brain
in a state of putrescence. It may supervene on polypous tumours,
particularly of the antrum; and of this I have seen several instances.
Sometimes it is produced after the removal of a tumour apparently
not of malignant character, and in this case it frequently does not
appear till the wound has almost cicatrised. When once established, it
proceeds with all its virulency. The diseased parts may be removed as
frequently as they appear; but they will be reproduced, and the disease
will assume a still more frightful aspect, both in extent and malignity.
In consequence of the repeated and profuse loss of blood, the patient
is gradually worn out, becomes hectic, is affected with nausea,
vomiting, and indistinct articulation, with all the symptoms of extreme
debility, and he generally sinks exhausted, or may be suddenly carried
off by profuse hemorrhage.
149
The size of the bleeding fungus is extremely various, but it is rarely
large; in fact, we frequently find that the most violent hemorrhage
occurs from those of a small size; and in illustration of this, I
shall briefly relate the following case. A man, aged forty, had been
afflicted for some time with ulceration in the ham, and exfoliation
of the posterior part of the femur. The sore healed; but about two
years afterwards the cicatrix became ulcerated, and produced a very
small fungus, resembling, in fact, a minute cluster of exuberant
granulations: from this blood was effused in small quantity, and was
easily restrained by the application of a bandage; but the hemorrhage
returned at various intervals for upwards of a week, became extremely
profuse and altogether uncontrollable. By this the patient was
greatly exhausted, and amputation was rendered absolutely necessary.
On examining the limb, the lower portion of the femur was found
somewhat enlarged, its internal structure completely destroyed, and
the periosteum on the inner side much thickened. On the posterior and
inner part of the bone, about three inches above its articulation,
there was a small fungous tumour of an irregular surface, and of soft
consistence, resembling congealed tallow. From this excrescence the
blood had been effused into a cyst formed amongst the muscles, and
afterwards discharged externally. He recovered from the amputation, and
remained well.
THE PAINFUL TUBERCLE.
Though of small size, and not possessed of malignant action or
disposition, is a tumour of very great interest, on account of the
excruciating pain with which it is accompanied. It is mostly situated
in the subcutaneous cellular tissue, but not unfrequently in the
intermuscular cellular substance; one tumour of this species which I
have removed was so deep as to be in immediate contact with the sheath
of the posterior tibial nerve. The tumour, generally of the size of a
garden pea, rarely exceeds that of a cherry. It is invested by a dense
ligamentous cyst, to which it intimately adheres; but occasionally
the capsule is thin and cellular: in many instances its surface is
perfectly smooth, in others it is slightly nodulated. It is not
connected with any large nervous trunk; but minute nervous fibrillæ
can occasionally be traced expanding on its surface, and apparently
entering its substance. Internally it is composed of numerous whitish
fibres, of considerable density, ramifying irregularly throughout
its structure; and betwixt these is insinuated a firm substance,
generally of a grey colour, and frequently of an almost cartilaginous
consistence. Such is the structure most frequently observed; but in
this morbid formation, as in all others, the appearances may be said
to vary in almost every instance. Sometimes the fibres are indistinct,
and of a yellowish or dirty grey colour; and the interfibrous matter
is often found to vary in density and colour in different tumours,
being at one time dense and almost transparent, at another opaque and
cartilaginous, and sometimes rather soft, brownish, and occasionally
tinged with blood.150 From attentive examination, it appears extremely
probable that the enlargement is at first produced by infiltration of
lymph betwixt the fibrillæ of a nervous twig, which becomes separated
and inclosed by the deposit—that they afterwards increase in size—that
the interfibrous matter is deposited in greater quantity, and is
farther condensed—and that thereby the nervous filaments are still more
separated and extenuated. In short, it would appear that the fibrous
matter is nervous, though altered, and that the interposed substance
is organised and condensed lymph. The tumour, at first extremely
minute, enlarges slowly; when deep, it can only be obscurely felt,
and its existence is with difficulty discovered by manipulation; but
the attending symptoms are so peculiar, and so forcibly developed,
as to lead the surgeon at once to an accurate diagnosis. When it is
subcutaneous, the skin is rendered slightly prominent, and the size,
density, and loose connections of the growth, are readily ascertained.
The slightest pressure causes the most excruciating torments, and
totally unmans the patient, even though induced by the most trifling
movement of the adjoining muscles. From a fearful and well-grounded
knowledge of this circumstance, the patient is extremely anxious to
preserve the limb in a state of complete rest, and, in fact, he is
often wholly unable to use it; although the part is completely set
at rest, still he frequently suffers from paroxysms of severe pain,
commencing in the tumour and shooting through the limb. The painful
sensations are sometimes very much alleviated by gentle friction with
the hand. The disease is most frequent in the extremities, and in the
inferior more than in the superior.
The larger nervous trunks sometimes become diseased, being affected
with an enlargement resembling the structure and appearance of the
preceding tumour, and such enlargements are termed Neuromata.
Occasionally a portion of a nervous trunk is thus enlarged, from a
blow or wound; and sometimes there can be no cause assigned. Nerves
when divided, become bulbous on that extremity towards their centre.
In stumps this is well seen; whilst all the tissues entering into it,
after a time shrink, and become more or less atrophied (bone, muscles,
vessels, &c.), the extremities of the nerves swell out and present
a bulbous appearance. When these tumours are connected to, and only
covered by, integument, or when they are adherent to the ligamentous
substance covering the bone, and become exposed to pressure, as in
badly made stumps, the patient often suffers excruciating agony. The
nervous trunk above is, in general, slightly enlarged, sometimes has a
tortuous course; and in some instances the neurilemmal bloodvessels are
considerably increased in size. The same symptoms exist, though in a
less acute form, as in the painful tubercle.
OF POLYPUS.
A common species of tumour is that which is attached to a mucous
surface, and is called POLYPUS. Polypi vary in structure and
disposition; some are simple and benign, others are most malig151nant.
The simple mucous polypus has a shining appearance, being invested
by an extremely delicate membrane, in some degree resembling the
mucous, and moistened by a fluid similar to the mucous secretion; it
is of soft consistence and homogeneous structure. They are generally
light brown, sometimes greyish, and in some degree diaphanous. They
are connected to the mucous membrane by a narrow pedicle; generally
occur in clusters, and are of pyriform shape; one or more are often
suspended from one narrow base, and they seldom attain a large size.
They possess but little vascularity, though occasionally minute
vessels are seen ramifying pretty freely on their surface, and may be
considered as almost devoid of sensibility. The malignant polypus,
on the contrary, is always attached to the mucous membrane, and also
to the subjacent parts, by means of a broad base; and its form and
structure vary according to the particular action which it has assumed.
Most frequently it is encephaloid, of an irregular form, and often
presenting a cauliflower appearance, its surface being studded with
numerous excrescences of medullary consistence and colour. Such tumours
will be afterwards treated of, as occurring in different situations.
OF ENCYSTED TUMOURS.
Along with these have been classed the enlargements of bursæ, sheaths
of tendons, &c., but with equal propriety might we include hydrocele
and other collections in natural cavities. Encysted tumours are
almost always situated superficially. The skin is distended, seldom
inflamed, and often contains enlarged bloodvessels, which give it a
streaked appearance. They consist of an external cyst, which is in some
instances extremely thin and delicate, in others dense, of considerable
thickness, and composed of fibrous looking substance, occasionally
it is almost cartilaginous; the internal structure may be said to be
almost always more or less fluid, but varies much in consistence. The
tumour is surrounded with condensed cellular substance, which is of
greater or less thickness and strength according to the size of the
tumour. Some of these tumours are supposed, and on good grounds, to be
mere enlargements of the natural mucous follicles, in consequence of
obstruction in their ducts, by hardened and vitiated secretion; the
cyst, therefore, will be at first thin and delicate; its contents will
resemble the natural secretion of the follicle, and in many cases may
be readily squeezed out. There is a black point on the most prominent
part, marking the obstructed orifice of the follicle, and the sac is
found at this point to adhere firmly to the skin. Even after all other
marks of its original formation have disappeared, the situation of the
orifice is sometimes indicated by small dark spots, by depression, or
by a minute ulcer.
Encysted tumours, or wens, as they have been called, often appear
to be hereditary; seldom occur single, and are met with under the
surface of all parts of the body. They have been divided into different
classes, according to the nature of their contents: Atheroma152tous;
containing curdy matter; Meliceritous, containing a substance like
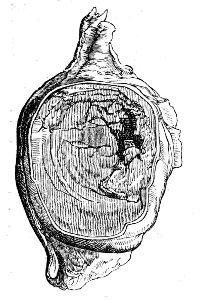 honey; and Steatomatous, containing fatty matter, generally in
a semifluid condition. But such terms are not adequate to express
the nature of all encysted tumours; they are extremely various in
their actions, and their contents vary according to the particular
secretory action which the lining membrane of the cyst assumes; for
the same reason, also, the contents of a tumour will differ in the
different stages of its progress. Some contain a thin, fetid, brown
fluid, mixed with solid particles, resembling half-dissolved fibrinous
matter; in some the contents are serous, or sero-purulent,—in others
they are gelatinous; whilst in those which have become inflamed from
external irritation, the contents are altogether purulent, or contain
a very considerable proportion of that fluid; not unfrequently the
cyst is covered internally by a layer of calcareous matter, to which
similar particles are loosely attached. Sometimes, in consequence of
irritation, organisable matter is poured out on the inner surface of
the cyst, adheres firmly to its inner surface, and is often disposed in
concentric laminæ.
honey; and Steatomatous, containing fatty matter, generally in
a semifluid condition. But such terms are not adequate to express
the nature of all encysted tumours; they are extremely various in
their actions, and their contents vary according to the particular
secretory action which the lining membrane of the cyst assumes; for
the same reason, also, the contents of a tumour will differ in the
different stages of its progress. Some contain a thin, fetid, brown
fluid, mixed with solid particles, resembling half-dissolved fibrinous
matter; in some the contents are serous, or sero-purulent,—in others
they are gelatinous; whilst in those which have become inflamed from
external irritation, the contents are altogether purulent, or contain
a very considerable proportion of that fluid; not unfrequently the
cyst is covered internally by a layer of calcareous matter, to which
similar particles are loosely attached. Sometimes, in consequence of
irritation, organisable matter is poured out on the inner surface of
the cyst, adheres firmly to its inner surface, and is often disposed in
concentric laminæ.
Sometimes, though rarely, the most prominent parts of the tumour
ulcerate, and on the exposed surface is deposited a substance of
semifluid consistence and gelatinous appearance, which afterwards
increases in density, and ultimately assumes all the characters of
horn. This hard excrescence in some instances increases only to a
slight degree, and afterwards remains stationary; in others it attains
a large size, and occasionally assumes a curved or tortuous form,
like that of the horns of inferior animals. Horns are generally met
with on the forehead, and the scalp may be said to be their seat. The
largest which I have seen, measured seven inches in length, and two in
circumference; but others have been removed still larger.
In many encysted tumours, hairs grow from the internal membrane of the
cyst, often numerous, and are generally found in those situated on the
eyelids; in some the hairs are destitute of bulbs, lie loose within
the tumour, and are often rolled into a globular form. The adhesions
of these tumours are in general very slight and easily broken up, but
when seated amongst tendons, or in unyielding parts, they are often
extremely firm. Violent inflammatory action may follow injuries of the
tumours, or the making of even minute openings into them; suppuration
occurs, the discharge is thin, fetid, and often bloody; there is much
pain, and frequently severe constitutional irritation. Occasionally
a fungus, bleeding or not, is protruded through the aperture; more
frequently, however, the opening heals, and the tumour remains as
before. External injuries sometimes appear to153 check the secreting
action, and to excite the absorbents to remove the morbid growths,
and this with or without rupture of the cyst. Thus, in the case of
an encysted tumour the size of a hen’s egg, on the external lateral
ligament of the knee joint, free and pretty rough manipulation was
necessary to ascertain its nature and exact situation; in consequence
of which, the tumour gradually disappeared, and no traces of it
remained twelve days afterwards. Others of less size, I have known to
disappear in a much shorter period.
OF TUMOURS OF BONES.
The vascular action of bones, in their healthy state, is feeble, but,
as in other feeble parts, it is easily excited, and disease of an
obstinate and unyielding nature is apt to follow.
The morbid growths vary much in texture. The most frequent are the
osseous, or those of the same structure with the original bone;
but even these differ much in the density and arrangement of their
particles: they have been termed exostoses. They may be of great
density, and are then called the hard, or ivory; these never attain a
large size, seldom exceed that of a bean, have a smooth and polished
surface, and are of a flattened and hemispheroidal form, their greatest
circumference being at the base; they occur in many of the bones, but
generally in those of the cranium and face.
Others, being of a more loose and spongy texture, have been called
cancellated. These are commonly formed by the bones of the extremities,
and often attain a very considerable size; they grow from the
periosteum, or from the outer surface of the bone, and are then
covered by an expansion of this membrane. Sometimes they adhere by a
narrow neck, and expand into a bulbous form, so that they can be very
readily removed by operation, and are very apt to be broken off by
external injury. Others have a broad and firmer attachment, and are of
an irregular shape, often projecting in the form of a large spicula,
and at other times assuming a somewhat stalactical appearance. Such
frequently prove the source of much inconvenience, by impeding the
motions of the muscles, or disturbing the functions of any adjoining
organ. They possess no malignant disposition, but are under the same
laws, though perhaps in a less degree, with their parent trunk.
On making sections of exostoses, and of the bones from which they
arise, some appear to be mere enlargements or processes of the
parent bone, the cancellated tissue extending itself so as to form
the interior of the exostoses, whilst the exterior resembles a
proportionate extension of the outer lamina. Others are evidently
formed by the deposition of osseous matter externally to the outer
lamina, many being dense and compact throughout, others containing an
internal cancellated structure, but which is not continuous with that
of the bone, as it is separated by the natural outer lamina. Their
formation appears similar to that of the fœtal bones: a glutinous
matter is effused, becomes dense, and is converted into cartilage;
bloodvessels shoot into it, ramify throughout its whole structure in a
radiated form, and154 deposit osseous matter. This deposit increases, and
extends from a central nucleus towards the circumference; the cartilage
is in part absorbed, and the new structure becomes osseous, and similar
to the original tissue by the vessels of which it was formed. These
tumours, even when they have attained a large size, contain a mixture
of bone and cartilage, covered by a dense fibrous investment. The bony
matter is arranged in spicula, adhering to the surface of the shaft or
head of the bone, and projecting into the morbid mass: the spaces are
filled up by a cartilaginous substance. The growth is sometimes rapid,
and the tumour soon becomes troublesome from its immense size.
Frequently a bone is much enlarged throughout its whole extent, or the
greater part of it, and presents a cancellated texture: sometimes,
also, it is much thickened, and, at the same time, of great solidity;
but such enlargements cannot be considered as tumours of bones, or
exostoses, any more than those nodules of new osseous matter, which
are effused in consequence of inflammation of the osseous tissue. The
most frequent cause of exostoses appears to be external injury; their
progress is slow, attended with slight dull pain, and often accompanied
with no inconvenience; their existence can be readily ascertained,
a hard and immoveable body being felt where no bone exists in the
natural state of parts; but when the tumour projects into an internal
cavity, the diagnosis is rendered obscure. Most frequently, they remain
stationary, after having attained a certain size, and are productive
of little inconvenience, the surrounding parts having accommodated
themselves to the new formation. Occasionally, suppuration occurs in
the soft parts, the matter comes to the surface, and a troublesome
abscess is formed.
To this class of tumours would I confine the term exostosis, not
including those consisting of softer materials, and possessed of a less
benign action.
OF OSTEOSARCOMA.
By this term is meant, an enlargement and alteration in the structure
of a bone, accompanied with the deposition of a morbid sarcomatous
substance internally. This morbid change appears to be the consequence
of inflammation, and its origin is frequently attributed to some
mechanical injury or local irritation. In the commencement of the
disease, the bone is slightly enlarged, perhaps somewhat thickened
in its outer laminæ; and on a section of it being made, is found to
contain a brown fleshy substance instead of its cancelli. This appears
to be formed in consequence of a morbid action, perhaps inflammatory,
of its internal structure. By the pressure of the new formation, the
parietes of the bone are pushed outwards, in some cases attenuated,
in others thickened by deposition of new osseous matter, inflammatory
action having been induced by the pressure. As the internal formation
increases, the parietes are extended, and are generally much
attenuated, becoming in some places thin as paper, and diaphanous; they
also would seem to lose a portion of their earthy matter, for they are
flexible, somewhat elastic, and not155 of their usual density. Frequently
they are in several places deficient, and their situation occupied
by a membranous expansion, sometimes thin and delicate, but mostly
thick and ligamentous; in some cases, the external lamina appears to
be converted into a substance resembling the internal growth, with
which it is continuous. The investing periosteum is much thickened,
and its bloodvessels are enlarged. Occasionally, the deficiency of
the bone is not supplied by any membranous expansion, and the morbid
growth protrudes, fungous. The internal structure varies much in
appearance; generally it is brown and soft, in some places broken down
and mixed with a dark-coloured fluid, or with gelatiniform matter;
sometimes it is much more dense, and resembles cartilage; in others,
the cavity contains an ichorous fluid, mixed with small portions of
more solid matter; in the advanced stage of the disease, the contents
are often of the encephaloid nature, either in its homogeneous and
solid form, or softened, broken down, and mixed with blood, or with
a lard-like substance. Sometimes the cancelli of the bone are not
destroyed, but extended, forming numerous cavities of considerable
size, in which the morbid matter is deposited; in other instances,
there is no appearance of cancellated structure, and the diseased mass
contains rough osseous spicula, some detached, some loosely connected
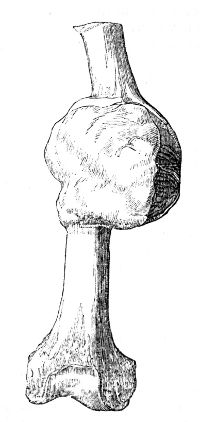 with each other, and others projecting from the inner surface of the
bony parietes of the tumour. At the commencement of the disease, the
patient feels acute pain in the part, the constitution is disturbed;
afterwards, the pain becomes more dull, and there is a considerable
swelling externally, which feels hard, and slightly elastic; in the
advanced stage, the pain again becomes severe, and is of a lancinating
kind, and the system is much deranged, the tumour is softer, often
presents a sense of distinct fluctuation, and on being freely handled,
is found to crepitate, in consequence of the loose spicula of bone
rubbing upon each other. Ultimately, the integuments become tense,
livid, or dark-red, ulcerate, and allow a portion of the softened
tumour to protrude, in the form of a frightful fungus; there is profuse
discharge, thin, and sometimes bloody; there is much constitutional
irritation, and the patient is greatly exhausted. Not unfrequently,
during the progress of the disease, especially in the long bones,
fracture occurs at the diseased part, either from external injury, or
sudden muscular exertion. This occurred in the case from which the
specimen here delineated was obtained some months before the patient
submitted156 to amputation. The morbid structure had not broken through
its periosteal investment. The muscles and their interfilamentous
tissue were sound. The patient remained free from any return of the
local disease. Bones so affected, when broken, do not unite, the
movement of the loose and rough ends is a cause of much irritation:
inflammatory action is kindled in the morbid structure, suppuration
occurs, the integuments give way, and ulcerate to a greater or less
extent, and the advancement of the disease is thus much hastened. The
tumour may be safely pronounced malignant; it is true, that for some
time it shows no tendency to involve the adjoining soft parts, further
than by the effects of inflammation induced by its pressure; but then
it is limited by the external lamina of the bones, which confines
it to the tissue in which it originated; but after this barrier has
given way, the tumour projects through the aperture, contaminating the
adjacent soft parts, imparting to them a morbid action, and extending
also in the cancellated tissue of the shaft of the bone. In some cases,
the integuments are tense and discoloured, with large vessels running
on their surface; the tumour feels soft and fluctuating, though the
skin may not ulcerate till long afterwards. Perhaps the most common
seat of this disease is the under-jaw, but it may occur in any of the
bones; when it has been of chronic duration, not one bone but several
are affected; and in one case which I saw, the disease commenced in the
under-jaw, which it deformed to a frightful degree; almost every bone
in the body was similarly, though less extensively diseased; this could
be readily observed during the life of the patient, and was confirmed
by dissection. From this, it appears, that the affection is not only
dependent on local causes, but connected with a morbid state of the
constitution, predisposing to it, and cooperating with its exciting
cause.
with each other, and others projecting from the inner surface of the
bony parietes of the tumour. At the commencement of the disease, the
patient feels acute pain in the part, the constitution is disturbed;
afterwards, the pain becomes more dull, and there is a considerable
swelling externally, which feels hard, and slightly elastic; in the
advanced stage, the pain again becomes severe, and is of a lancinating
kind, and the system is much deranged, the tumour is softer, often
presents a sense of distinct fluctuation, and on being freely handled,
is found to crepitate, in consequence of the loose spicula of bone
rubbing upon each other. Ultimately, the integuments become tense,
livid, or dark-red, ulcerate, and allow a portion of the softened
tumour to protrude, in the form of a frightful fungus; there is profuse
discharge, thin, and sometimes bloody; there is much constitutional
irritation, and the patient is greatly exhausted. Not unfrequently,
during the progress of the disease, especially in the long bones,
fracture occurs at the diseased part, either from external injury, or
sudden muscular exertion. This occurred in the case from which the
specimen here delineated was obtained some months before the patient
submitted156 to amputation. The morbid structure had not broken through
its periosteal investment. The muscles and their interfilamentous
tissue were sound. The patient remained free from any return of the
local disease. Bones so affected, when broken, do not unite, the
movement of the loose and rough ends is a cause of much irritation:
inflammatory action is kindled in the morbid structure, suppuration
occurs, the integuments give way, and ulcerate to a greater or less
extent, and the advancement of the disease is thus much hastened. The
tumour may be safely pronounced malignant; it is true, that for some
time it shows no tendency to involve the adjoining soft parts, further
than by the effects of inflammation induced by its pressure; but then
it is limited by the external lamina of the bones, which confines
it to the tissue in which it originated; but after this barrier has
given way, the tumour projects through the aperture, contaminating the
adjacent soft parts, imparting to them a morbid action, and extending
also in the cancellated tissue of the shaft of the bone. In some cases,
the integuments are tense and discoloured, with large vessels running
on their surface; the tumour feels soft and fluctuating, though the
skin may not ulcerate till long afterwards. Perhaps the most common
seat of this disease is the under-jaw, but it may occur in any of the
bones; when it has been of chronic duration, not one bone but several
are affected; and in one case which I saw, the disease commenced in the
under-jaw, which it deformed to a frightful degree; almost every bone
in the body was similarly, though less extensively diseased; this could
be readily observed during the life of the patient, and was confirmed
by dissection. From this, it appears, that the affection is not only
dependent on local causes, but connected with a morbid state of the
constitution, predisposing to it, and cooperating with its exciting
cause.
There are other tumours of bones in some degree resembling, which
do not strictly come under the term Osteosarcoma. Some are wholly
cartilaginous, the disease commencing in their centre, and involving
their entire substance, emitting a gelatinous fluid when cut, but
containing no cells; others are not uncommon, partly osseous, and
partly cartilaginous, containing cells filled with a glairy fluid;
others are composed of cartilage, intersected with dense fibrous
matter, in a greater or less proportion. In fact, the individual
tumours of bones vary as much from one another as those of the
softer tissues; scarcely two are alike in their progress, action,
or anatomical characters. Irregular spicula of bone are found in
many parts of their structure; in the same way that portions of bone
often exist in tumours having no connection with the bones; in many
places they are softened and broken down, the partitions between
the cells are destroyed, and these contain a pulpy mass of a dark
sanious appearance. On making a section, they are observed to be
continuous with the interior of the bone, which is converted into a
substance similar to themselves, or is of a more soft and medullary
character. The external surface becomes tuberculated, the integuments
are painful, and changed in appearance; they ulcerate, the tubercles
burst, the discharge is thin and bloody, the ulceration157 extends; not
unfrequently a fungus protrudes, and occasionally bleeds; this may
slough, the tumour becomes farther exposed, portions of it die, and
are discharged, unhealthy fungous granulations project from amongst
the cancelli of the tumour, and emit a sanious putrid discharge, often
bloody; severe constitutional irritation accompanies this state, the
patient becomes hectic, is much exhausted, and sinks, unless the morbid
parts be removed. There are also tumours of bones, composed partly of
cartilaginous or fleshy, or partly of osseous matter, arising from the
periosteum and outer shell of the bone, and these often acquire a great
magnitude before the diseased mass reaches the interior or medullary
part of the bone.
SPINA VENTOSA.
By this term is understood a mere expansion of a bone from a collection
of matter in its substance. The disease may be produced by external
injury, exciting inflammation, and consequent suppuration, in the
cancellated tissue; or in a weakened and unhealthy constitution, the
action may be of a chronic nature. The fluid accumulates, the cancelli
are broken down, and the much-attenuated parietes of the bone are
pressed outwards. Occasionally inflammatory action is excited on
the external surface, from the pressure of the contained fluid, and
minute nodules of bony matter are effused, as if nature endeavoured
to strengthen those walls which are daily becoming thinner, and
more incapable of supporting the weight of those parts which they
encircle. The disease differs from Osteosarcoma in the contents being
uniformly fluid, generally purulent, though often mixed with more
liquid and dark-coloured matter, or with a curdy substance—in the
gradual extension of the bone—in no fungus protruding after a portion
of the attenuated bone has given way, matter being discharged as
from a common abscess; and in the tumour not possessing a malignant
disposition. At first there is considerable pain in the part whilst
the matter is forming, but afterwards it becomes much less acute, and
in many instances there is no inconvenience, except from the bulk of
the tumour. Often after having reached no very large size, it becomes
stationary, neither recedes or enlarges, and all painful sensations
cease; in other cases it enlarges gradually, attains an enormous
size, and produces much disturbance of the constitution; but in such
instances the patient is generally weak and cachectic. The largest
tumour of this species which I have seen, occurred in the lower part of
the femur. It measured, in breadth, seven inches, in length, seven and
one-fourth. The parietes were composed of an extremely thin lamina of
bone, and in this there were numerous deficiencies supplied by delicate
ligamentous matter; its cavity was divided into several compartments by
thin septa, partly osseous and partly membranous. A representation of
the femur so affected is given in the Practical Surgery, p. 350. The
patient was a boy of twelve years of age; amputation of the limb was
earnestly advised, the friends objected, he died hectic.
158
ANEURISMAL TUMOURS.
Besides these tumours a species of an anomalous character is sometimes
met with, appearing to arise from an aneurismal or varicose state
of the venous radicles or capillaries, and partaking somewhat also
of the nature of fungus hæmatodes.21 I shall detail shortly the
159more important circumstances of one case. The patient, a lad aged
sixteen, was admitted into a public hospital on the 7th of November,
1819, on account of a tumour over the left scapula. It was there
deemed imprudent and inadvisable to attempt operation; and, after the
application of leeches, he was dismissed, at the end of eight days.
He then applied to me. The tumour was very large, hard, inelastic,
firmly attached to the left scapula, and extending from its spine over
all its lower surface. It also stretched into the axilla to within
half an inch of the nervous and vascular plexus, and a large arterial
trunk could be felt along its under surface. The arm hung useless,
and, from the wasting of its muscles, was hardly half the size of the
other. According to his own account, the uneasiness produced by the
tumour was trifling when compared to the lancinating and excruciating
pains in the limb. On attempting to move the tumour independently of
the scapula, crepitation was distinctly perceived, as if from fracture
of osseous spicula. A tumour was first perceived about three months
previous, situated immediately below the spine of the scapula, about
the size of a filbert, of a flat form, and attended with distinct
pulsation; it had subsequently increased with great rapidity. About ten
days before his admission into the hospital, it had been punctured;
nothing but blood escaped. It was evident, from the rapid growth of
the tumour, and the severity of the symptoms, that the patient would
soon be destroyed if no operation were attempted. There were no signs
of evil in the thoracic viscera, the ribs and intercostal muscles were
unaffected; though the tumour was firmly fixed to the scapula, yet that
bone was moveable as the one on the opposite side, and the vessels and
nerves in the axilla were quite unconnected with the swelling. The
operation was commenced by making an incision from the axilla to the
lower and posterior part of the tumour. The latissimus dorsi was then
cut across at about two inches from its insertion, so as to expose the
inner edge of the tumour, with a view to tie the subscapular artery
in the first instance; in this, however, I was foiled, owing to its
depth. The dissection was proceeded with to where the branches from
the supra-scapular were expected to enter. In detaching the tumour from
the spine of the scapula, the knife and fingers suddenly dipped into
its substance. This was attended with a profuse gush of florid blood,
with coagula; by a sponge thrust into the cavity, the hemorrhage was in
a great degree arrested; at the same time an attempt made to compress
the subclavian failed, on account of the arm being much raised to
facilitate the dissection in the axilla. The patient, exhausted, made
some 160efforts to vomit, and dropped his head from the pillow, pale,
cold, and almost lifeless. Then only the nature of the case became
apparent. The sponge being withdrawn, one rapid incision completely
separated the upper edge of the tumour, so as to expose its cavity;
and, directed by the warm gush of blood, a large vessel in the upper
corner, which with open mouth was pouring its contents into the sac,
was immediately secured. The coagula being removed, by dissecting
under the finger, the subscapular artery was then separated, so that
an aneurism needle could be passed under it at its origin from the
axillary, and about an inch from the sac. After securing this and two
other large vessels which supplied the cavity, the tumour was dissected
from the ribs without further hemorrhage, cutting the diseased scapula
and the under part of the sac. It was then found necessary to saw
off the ragged and spongy part of the scapula, leaving only about a
fourth part of that bone, containing the glenoid cavity, processes,
and half of its spine. The edges of the wound were brought together,
and the patient lifted cautiously to bed. At this time he was pale,
almost insensible, and without any pulsation perceptible through the
integuments in the greater arteries, though the ends of the vessels
in the wound beat very forcibly. Stimuli were employed externally and
internally; in the evening his pulse at the wrist was ninety, and soft.
The sac of the tumour was composed of bony matter, containing little
earth, and arranged in strata of short fibres pointing to the cavity.
Its outer surface was smooth, and covered by a dense membrane; whereas
the inner, to which so equable a resistance was not afforded, was
studded with projecting spicula. The lower part of the scapula,
partially absorbed, lay in the middle of the sac, covered by the
remains of its muscles and coagula. Very large vessels were perceived
ramifying on the surface of the tumour.
The patient made a rapid recovery, and the wound all but healed.
A fungus, however, began to appear in about six weeks, which grew
rapidly. This was removed, and the bone cauterized with little good
effect. The tumour was soon reproduced. It was proposed to remove
the remainder of the scapula with the extremity, as the only chance,
though perhaps a slight one. This was objected to, and he died about
five months after the operation, worn out by hemorrhage and profuse
discharge.
The diseased parts presented the following appearances. Portions of
the acromion process, superior costa, and spine of the scapula, were
of their natural appearance. But the coracoid process, the glenoid
cavity, and the cervix, were entirely destroyed, and their situation
occupied by an irregular broken-down tumour, consisting of osseous
spiculæ, and cancelli, irregularly disposed, and forming cavities which
were filled with blood, partly fluid and partly coagulated. The head
of the humerus was extensively absorbed. The articulating cartilage
was almost entirely destroyed, particularly on the inner side, where a
large portion of the bony matter had also been removed. The ulcerated
surfaces were of a dark, bloody colour.
161
HYDATIC TUMORS.
Another disease of the bones which ought to be introduced here is the
development of hydatids, which I described twelve years ago under the
name of osteo-hydatidic tumours. The seat of this affection is not
confined to any particular class of bones; though the long are perhaps
most prone to it. Its precise nature and origin have not yet been
determined; nor are its symptoms such as to enable us, in the present
state of our knowledge, to distinguish it from exostosis, osteosarcoma,
and other maladies. Its progress is commonly slow, the surface of the
tumour is smooth and regular, the skin exhibits no unusual appearance,
and the adjacent textures rarely participate in the morbid action.
The hydatids, usually of a globular figure, vary greatly in size and
number, and are generally filled with a thin, limpid fluid. They appear
to be of the nature of acephalocysts. The prognosis unfavourable, owing
to the difficulty of destroying these parasites, and their constant
tendency, when interfered with, to reappear.
As soon as the true nature of this tumour is ascertained it should be
laid freely open, its contents turned out, and the sac destroyed. For
this purpose the sides of the cavity should be seared with the actual
cautery, or touched with some of the more powerful escharotics, as the
nitrate of silver, or the caustic potash. If these measures fail, and
the disease involve the whole circumference of the bone, nothing short
of amputation will suffice. This was successfully resorted to in one of
the cases which came under the observation of Mr. Lucas of London.]
TREATMENT OF TUMOURS.
It may be observed generally, that no benefit can be derived from
external applications to tumours, such as friction with liniments or
ointments containing iodine, mercury, &c.; and that, therefore, it is
injudicious to employ such temporising measures; for though a tumour
at its commencement appear to be of a very harmless nature, yet it
may soon assume a most malignant character. If an apparently simple
tumour increase, and exhibit symptoms of inflammation, it will perhaps
be advantageous to apply leeches, to arrest that incited action which
affords the accession of new materials; this, however, cannot check
the morbid activity inherent in the new formation, though it may
hold the growth in check a little. If a tumour is to be removed by
external applications, it is evident that these must be such as shall
prevent the deposit of new matter, and allow the absorbents to remove
that which already exists; for absorption is always going on in a
tumour, though it leaves no evidence of its progress, on account of
the deposition of new matter exceeding the removal of the old. I must
say that I am unacquainted with any remedies capable162 of performing
the above indication. The removal of a swelled gland may occasionally
be accelerated by such means when stationary, or on the decline,
and before cheesy tubercular unorganized matter is infiltrated into
its texture; but to trifle so with a new and independent growth is
altogether absurd. The knife only is to be depended on.
Many of the tumours first described have no malignant disposition
originally, and only require surgical interference when they produce
deformity or inconvenience from their bulk. Yet even these ought not
to be allowed to attain any great size, however indolent they may
appear at first, and however little pain they may produce; for there
is always a danger of their assuming a malignant tendency, or forming
connections with important parts, so as to render their removal either
altogether impracticable, or at least attended with much difficulty.
Tumours of every kind, when seated near important organs, must be early
removed. Glandular tumours, however, even when of great size and long
continuance, are not to be rashly interfered with, when they arise from
irritation in the neighbourhood.
Those in which it is feared that malignant action has commenced cannot
be trifled with; and the only means which afford a chance of the
patient’s being effectually delivered from them is an operation. With
a view to their complete extirpation, the external incisions ought
always to be free, so as to admit of the after-dissection being easily
and rapidly performed: they ought also to be made in the direction of
the muscular fibres, whether these lie above or beneath the tumour. In
this way the margins of the wound are easily brought into apposition,
and there retained; whereas, if the fibres be divided transversely,
the wound will gape, and union by the first intention be rendered
absolutely impossible. If there is no reason to suppose that the tumour
is malignant, little or no integument ought to be removed, unless the
growth is of a large size; but, when malignity is dreaded, all the
discoloured, tense, and adherent integument, all that is permeated
by dilated and tortuous vessels, ought to be taken away, and the
incisions made at a distance from the disease. In all cases they ought
to commence at the point where the principal vessels enter; these are
thus divided at the outset, can be readily secured by ligature, or
by the fingers of an assistant, and the dissection is proceeded in
without risk or interruption from farther hemorrhage. If the opposite
course be pursued, the vessels will be divided two or more times during
the operation, and thus the performance of it will either be delayed
by the application of numerous ligatures, or will be attended with
a considerable loss of blood. After the tumour has been exposed it
ought to be principally detached in one direction, as in this way its
removal will be sooner accomplished, and not first cut on one side and
then on another. If malignant, great care should be taken that all the
diseased mass be removed, for a minute portion remaining will form a
nucleus in which similar diseased actions are certain to arise; in most
instances, it will be prudent not only to remove the parts actually
diseased, but those also which are in immediate connection with the
tumour, though at the time they appear healthy. All important parts
must be carefully avoided. After removal of the mass, and the complete
cessation of bleeding, the edges of the wound163 must be approximated, so
as to favour union by the first intention; if this fail, granulation
must be promoted, and the wound dressed according to the particular
circumstances of the case. All operations on malignant tumours, in
their advanced stages, are unwarrantable; they are necessarily painful
and severe, and cruel because unavailing; they often, indeed, expedite
the dissolution of the patient. If the integuments over the tumour have
ulcerated, and if the lymphatics in the neighbourhood are diseased, the
disease if removed will certainly be reproduced, and the succeeding
tumour will be still more malignant. The operation ought, if at all, to
be performed when the disease is in its incipient state, for then only
can success be expected.
Exostoses need not to be interfered with, unless they are the source
of much inconvenience, either from their size and form, or from their
having been detached, and lodged amongst the adjacent soft parts. If
loose, they can be removed in the same way as any other extraneous
body; if firm, their attachment must be divided by a saw, or by cutting
pliers, close to the bone from which they spring. Sometimes, as in the
scapula or other flat bone, a portion of the original bony tissue can
be cut out along with the new growth, and this renders the chance of
any return of disease much less likely.
Osteo-sarcomatous tumours are to be taken away, along with the part
of the bone in which they are imbedded, and, if possible, before the
integuments have ulcerated. The incisions must be made, and the bone
sawn, at a healthy part. The removal of the entire bone in which the
disease has commenced, when practicable, will afford a still better
chance of immunity from farther disease.
In spina ventosa more is seldom required than to lay open the
cavity, give vent to the matter, and then treat the case on the same
principles as in abscess of the soft parts. The cellular tumours,
partly cartilaginous, partly osseous, ought not to be permitted to
remain; the operation can generally be done without much difficulty;
and thus the danger of their degenerating avoided. Frequently, however,
a considerable part of the bone must be removed along with the tumour,
since the neighbouring tissue is generally softened, and intimately
adherent to the diseased part, which it somewhat resembles in structure.
In general, regular dissection is unnecessary in the removal of
encysted tumours. An incision is made, or an elliptical portion cut
out; the contents escape, and the cysts, being then laid hold of by
dissecting forceps, is readily separated. In some situations, as on
the eyelids, under the tongue, or amongst tendons, the sac, which is
thin, is not so easy of extraction; it is then inseparable, either
naturally, or from previous inflammation. Caustic is used with safety
to destroy those parts which cannot be detached, and for this purpose
the potass is to be preferred. When, however, the tumour is large, a
part of the integuments covering it must be removed, otherwise a large
cavity will be left, in which pus might accumulate. In this case, the
base of the tumour is to be surrounded by two elliptical incisions,
and the cyst dissected out entire, leaving only integument sufficient
to cover the exposed surface. In the smaller tumours, it is vain to
attempt regular dissection; a portion of the cyst will be left, and the
disease164 reproduced: whereas, by using the potass, the operation is
much more speedy, and always successful. The making a minute aperture,
and squeezing out the contents, is at best but a palliative measure,
and is often followed by severe constitutional disturbance.
OF WOUNDS.
These vary in extent and nature. The instrument by which they are
inflicted, the violence attending the injury, and the nature and
importance of the parts divided, or in the neighbourhood of the
wound, must all be attended to, for, from an accurate knowledge of
these circumstances, the treatment of the case comes to be conducted
accordingly. Wounds are divided into incised, punctured, bruised,
and lacerated; that is, into such as are inflicted by a sharp-edged,
sharp-pointed, or an obtuse body. In the first kind, there is greater
or less effusion of blood, according to the size and number of the
vessels divided. Some extend but a little way beyond the subcutaneous
cellular tissue, and are consequently attended with but slight
bleeding; others penetrate to a greater depth, and occasion hemorrhage
from a large vessel, or other alarming symptoms, by having reached
some important organ; others, though not of so great a depth as the
former, may still, on account of their mere extent, be accompanied with
very considerable loss of blood from a number of small branches. It
is seldom that fatal effects immediately follow external wounds; but
they may and do occur when bloodvessels of the first class only are
cut. They are most likely to prove suddenly fatal when the arteries
are only partially divided, and when the large veins accompanying them
are also involved. When the artery is cut through, its extremities
retract, effusion takes place into the sheath and compresses the
orifice; the formation of a coagulum within the vessel is thus
promoted, and the hemorrhage arrested. But, when a portion only of
the circumference is divided, the blood continues to flow through the
aperture and onwards, as if into a smaller ramification of itself, no
retraction or contraction of the vessel can occur, coagulation is slow,
and the bleeding profuse. I have seen a wound of so small a vessel
as the internal mammary prove almost instantaneously fatal. Wounds
of the large internal vessels for the most part prove immediately
fatal; as wounds of the heart, or the large vessels passing to and
from its cavities, at the root of the lungs, or at the upper part of
the liver. When the heart, or the vessels within the pericardium,
have been divided, it can be readily understood how life should be
immediately destroyed, since the blood effused into the cavity of the
pericardium by its pressure completely arrests the action of the heart.
But occasionally punctured wounds, in such situations, have not been
followed by instant death. In such cases, alarming symptoms occur at
the time, but subside, and the patient may for some time suffer no
uneasiness, but afterwards expires suddenly during muscular exertion,
or perhaps in a fit of violent passion. Blood must have been effused
into the pericardium at the first, causing165 symptoms of, or actual,
syncope; but then the aperture in the vessel had become obstructed
by coagulum before blood had been poured out in such quantity as to
effectually prevent the actions of the heart; at a future period the
coagulum gives way, and the subsequent effusion is limited only by
the pericardial cavity being completely filled. In wounds, hemorrhage
is the symptom which most alarms the bystanders, and which demands
immediate attention; but, to operate successfully, the surgeon must
divest himself of all fear, and learn to look boldly on the open and
bleeding mouths of arteries. Effusion of blood ceases spontaneously,
even from considerable vessels, on faintness supervening, and thus many
lives are saved; but as soon as reaction commences it generally recurs,
and may prove fatal, unless proper measures be resorted to.
When an artery is divided, its extremity retracts within the sheath, it
also contracts, and coagulation occurs; thus the orifice is obstructed,
and a temporary barrier formed to further hemorrhage. The tube,
however, is permanently closed by effusion of lymph from its orifice,
and consolidation of the surrounding parts.
The circumstances which follow division of an artery are these:—The
immediate effect is retraction of its ends within the investing sheath,
and a simultaneous contraction of the coats, so as to diminish the
calibre. From the superior orifice there is necessarily a profuse flow
of blood, which is discharged through the sheath that formerly enclosed
that part of the vessel which has retracted. After considerable
effusion of blood, the flow becomes slower and less profuse; particles
of blood adhere to those filaments which previously connected the
artery to the sheath, but which were lacerated by the sudden retraction
of the divided extremity; these particles coagulate, and lessen the
canal through which the blood is discharged, whilst they present an
irregular surface, on which the blood continues to be deposited and to
coagulate; and thus the aperture in the sheath is ultimately closed.
This external coagulum is found to commence at the extremity of the
artery, where it is of a cylindrical form, and shuts up the mouth of
the vessel; it then extends along the canal in the sheath, frequently
assuming a conical form; and, if a free discharge has been allowed for
the blood, it will terminate at the cut margin of the sheath, otherwise
it will be found continuous with the coagulum blocking up the external
wound. Also, when hemorrhage has been resisted by the shutting of the
external wound, blood is infiltrated into the cellular tissue around
the bleeding point, and there coagulates; but this circumstance can
be productive of little or no pressure on the parietes of the vessel,
so as to assist those other natural means which obstruct it. The flow
of blood through the divided vessel being prevented, the circulating
fluid necessarily passes through the nearest collateral branches,
leaving the blood in the extremity of the larger trunk in a state of
comparative rest; consequently, coagulation occurs in this situation.
The internal coagulum, however, is small, and not sufficient to occupy
completely the cavity of the vessel; it is of a conical form, its apex
being towards the heart, and opposite to the first collateral branch,
and its base resting on the external coagulum, and there adhering to
the internal surface of the166 artery. But, whilst this latter process
is advancing, the capillary vessels supplying the cut margins of
the artery have begun to act; they throw out coagulating lymph, and
continue to do so until their secretion has completely filled the
vessel immediately opposite to its divided margins; thus a third and
more effectual coagulum is formed,—one of plastic matter, situated
between the external and internal coagula of blood, and in general
closely adherent to them. Lymph is also effused externally to the
artery and its sheath, forming a dense stratum, which separates the
extremity of the vessel from the external wound; it becomes organised,
forms granulations, and thus the parts are consolidated, and the wound
cicatrised. When the artery is permanently obstructed by the adhesion
of its cut margins, the external coagulum can be dispensed with, and
is gradually absorbed. Afterwards all the newly formed parts are
condensed, and diminish in size; the artery contracts, its internal
surface finally embraces the coagulated blood which lay loose in its
canal; its coats appear to be thickened, and it is firm and hard.
Ultimately, in consequence of the continuance of absorption, it becomes
much more attenuated, so as scarcely to differ from the surrounding
cellular tissue. Similar changes occur in the lower extremity of the
divided artery; in general it retracts farther, its orifice is more
contracted, and, the flow of blood being much less profuse than in
the superior, the natural means for its temporary closure are sooner
accomplished. When an artery has been divided close to the origin of
a collateral branch, no bloody coagulum can form internally, for the
blood in that situation is necessarily in a state of constant motion.
If the hemorrhage is suppressed artificially, either by ligature, or by
otherwise well-applied pressure, no external coagulum is formed; there
appears only the internal bloody coagulum, the lymphatic effusion,
and consolidation of the compressed part. The natural contraction and
retraction cannot occur in vessels partially divided; hemorrhage,
therefore, is more violent and dangerous from a partial than from a
complete section. Again, transverse wounds are more dangerous than
longitudinal; in the latter, the edges of the wound are spontaneously
approximated on account of the structure of the vessels, whilst, from
the same cause, the margins of the latter continue separate, and, in
fact, the aperture is a complete circle; the lips of an oblique wound
will be more or less apart, in proportion as it approaches to the
transverse direction. When an artery has been punctured, the wound in
the sheath perhaps does not correspond with that in the vessel; blood,
therefore, accumulates between the vessel and its sheath, and there
coagulates. The wound is thus compressed, its edges kept in contact,
and the farther escape of blood prevented; the lips of the incision are
then agglutinated by effused lymph, and cicatrisation occurs. This,
however, cannot be expected to take place unless methodical pressure
has been applied from the first. Even from small punctures blood is
effused under the sheath and into the neighbouring cellular tissue,
rapidly, and in such quantity as to prevent adhesion. The effusion
continues, and a false aneurism is formed. If a considerable part of
the circumference has been divided, the lymph may be, and generally
is, superabundant,167 and often to such an extent as to close up the
canal of the artery at that point; but, if the aperture is minute and
in a longitudinal direction, lymph will seldom be effused in greater
quantity than is sufficient for the cicatrisation; and, though it
should be superabundant, it is afterwards removed by the absorbents.
In all cases, the cellular tissue round the wounded point is much
thickened and condensed by the deposition of lymph, but this gradually
disappears after cicatrisation has been completed. Sometimes, and
generally when the wound has been transverse and large, the process of
adhesion is disturbed, and suppuration occurs; in this case the wound
in the vessel communicates with the fistulous track in the externally
effused lymph, and may be the source of troublesome hemorrhage.
In other instances of extensive transverse wounds, the undivided
slip ulcerates, and the artery becomes obliterated, by means of the
same natural processes that occur in complete division. In cases of
laceration of an artery, when its coats have been forcibly torn rather
than divided, little or no bleeding takes place. The vessel retracts;
the lacerated margins of its inner coat become puckered up, so as to
contract greatly the orifice of the vessel; the lacerated sheath is
pulled out to a point, and closed at a little distance from the divided
inner coats. If a large artery is torn asunder in the dead body, this
stretching out and contraction of the sheath will prevent injection
passing; in short, the immediate effects of the injury are such as to
favour the instant formation of coagula, by which the hemorrhage is
arrested until the orifices of the vessel be permanently closed by the
adhesive process. Thus, in instances where the whole of an extremity
has been torn off, the patients have generally lost but a very small
quantity of blood.
From wounds of veins the blood flows, not in a sub-saltatory but in a
uniform stream: its colour is dark, and the flow is easily suppressed.
The common opinion is, that to place a ligature on a vein is dangerous,
and to be scrupulously avoided. The process of reparation, besides,
in a wounded vein, is different from that in an artery. Veins are
less disposed to the secreting action by which adhesion is perfected;
and, when inflamed, the inflammation is extremely apt to extend along
the coats of the vessel; which latter circumstance has been ascribed
to the great proportion of cellular tissue in their coats. When
punctured longitudinally, the lips of the wound remain in contact,
and cicatrisation, by means of effused lymph, is soon effected; in
fact, the wound heals by the first intention. But if opened obliquely
or transversely, not to a great extent, the immediate result is
discharge of blood, and, when this has ceased, a coagulum forms in
the wound, the margins of which remain separate; and this coagulum
generally communicates with blood effused into the sheath of the
vessel. After some time, the lips of the wound, encircling the coagulum
which occupies the aperture, and which has temporarily averted the
hemorrhage, become somewhat turgid, and increased in vascularity;
they then appear to assume a secreting action, by which a membranous
substance, of extreme delicacy, is produced; and the extent of this
membrane is increased until it form an expansion, investing the outer
surface of the clot; it then becomes thickened, by168 addition of matter,
similar to itself, from the recent vessels which ramify in it. At the
same time it forms adhesions to the surrounding cellular tissue, and
resembles the original tunics of the vein. After being consolidated,
so as to prevent the flow of blood through that part, the coagulum,
formed to arrest the hemorrhage until a more complete barrier should
be furnished, is gradually absorbed. But the membrane long remains
smooth, thin, and diaphanous, and can be thereby readily distinguished
from the original coats. This reparative process is much longer in
being finished than the corresponding one in arteries; and, from what
has been stated, it is evident that the two actions differ in other
respects than the time requisite to complete them. When a vein has been
completely divided, the extremities are closed by means similar to
those which have been already detailed in regard to arteries.
In many, nay in most, instances of hemorrhage from a wounded artery,
the surgeon cannot wait for the natural processes by which the flow
of blood is arrested, but must have recourse to immediate and certain
means. In division of the smaller arteries, or in minute wounds of the
larger, pressure, well applied, will often be sufficient. In both cases
it immediately stops the flow: in the former, it prevents the blood
from penetrating into that portion of the sheath which has been vacated
by the retracted artery; and it being thereby confined, and kept in
a state of rest, coagulation soon takes place. At the same time,
the compression brings the divided margins of the vessel into close
apposition, and thereby permanent closure, by adhesion, is quickly
accomplished. In the latter, the mere circumstance of the escape of
blood being prevented, naturally hastens the closure of the minute
aperture by the natural process; and, if the compression be accurate
and very firm, the opposite surfaces of the vessel, being brought in
contact, may adhere, and the canal be obliterated at the wounded point.
It is obvious that, in this latter class, pressure can only be of
advantage immediately after the infliction of the wound, and not when
blood is extravasated to a great extent.
Pressure may be used along with styptics, or along with escharotics,
actual or potential. They may be often employed when pressure ought
not; styptics promote the contraction and retraction of the divided
extremities, and thereby expedite the formation of a coagulum.
Escharotics form a slough, which, adhering to the extremity of the
vessel, stops the flow of blood, and the cut margins of the vessel,
being stimulated by the application, soon cohere. Active stimulating
applications merely cause effusion quickly of coagulated lymph, and
thus often arrest hemorrhage from very vascular surfaces better than
the so-called styptics. Not unfrequently, after the separation of the
slough, it is found that union has not taken place, and hemorrhage
is renewed; from this circumstance, the remedy cannot be trusted to,
except when the divided vessels or vessel are of small size. It may
be stated, generally, that these means are of little avail without
methodical pressure. In oozing from small vessels, pressure may be
applied by means of agaric, sponge, or lint. In bleeding from small
vessels, where there is general oozing from the surface, and pressure
cannot readily be made, applications tending to produce169 effusion of
lymph—stimulants, such as turpentine or creosote, are often remarkably
efficacious, and very speedily so; but in wounds of the larger vessels,
the most efficient mean is a graduated compress of lint placed
immediately on the external wound, and supported by a firmly-applied
bandage. The bandage ought to encircle not only the wounded part, but
every part of the limb with a uniform tightness, not so great as to
arrest the general circulation; the parts are thereby supported, and
engorgement prevented. This method, when employed previously to the
effusion of much blood into the cellular tissue, has proved effectual
in wounds even of the brachial, femoral, and carotid arteries. When
blood has been extensively injected into the limb, when the aperture in
the vessel has remained pervious, and when a large diffused aneurism
exists, bandaging is worse than useless. By its application in such a
case the limb becomes discoloured and swells extensively; there is a
risk of mortification from impeded circulation. If a small quantity
only of blood has escaped, its diffusion and increase may be prevented
by the bandage: but a cyst will nevertheless be formed in the cellular
tissue; its parietes will communicate with the margins of the aperture
in the artery, its cavity with the canal of the vessel; an aneurism
of the false kind will be established, and will run the course of one
arising spontaneously.
A ligature, well applied, is the only means that can be relied on. The
immediate effect of a tightly-drawn ligature is to avert the flow of
blood, to divide the internal and middle coats at the deligated point,
the cellular coat remaining entire, and to narrow the canal for some
extent above the point at which it is applied. Coagulation then occurs
within the vessel above the ligature, provided there is no collateral
branch in the immediate vicinity. The ruptured margins of the internal
coat effuse lymph and cohere; lymph is effused also in the cellular
tissue, exterior to the artery and to the ligature; by the compression
of the ligature, ulceration occurs in those parts which it envelopes,
and the foreign body is discharged; but before this occurs the canal
of the vessel has been obliterated by an internal coagulum, and by the
effused lymph. Afterwards, the same absorption and consolidation occur
as in a divided artery, the orifice of which has closed permanently and
spontaneously.
When from a punctured wound profuse hemorrhage ensues, there is reason
to suspect that an important vessel has been hurt, and the bleeding
point must be sought for. After the artery giving out the blood has
been discovered, the external wound must be enlarged, so as to expose
the vessel, and admit of the convenient application of a ligature. It
will not be sufficient to include the vessel above the wounded point,
for the lower part will, after some time, be supplied with blood
by the collateral branches almost as freely as by the large trunk,
and, consequently, bleeding will be renewed. Two ligatures are to be
employed, one above, the other below, the wound. The wounded vessel
must be exposed, as already stated, but not detached more than is
sufficient for the application of the ligature; and at the same time
the ligatures ought to enclose nothing but the vessel. Neither ought
the ligatures to be placed at any considerable distance,170 but as close
to the wounded point as possible; otherwise circulation in the included
part may be restored. The ligature, round, narrow, and firm, ought to
be tightly applied. Cases of hemorrhage have occurred in which the
tying of the vessel immediately above the wound has been successful;
but these are few, and by no means afford any authority for the general
adoption of such a measure. If the vessel is merely punctured, it is
necessary to apply the ligature by means of a blunt pointed needle, and
the parts are to be disturbed as little as possible. If, however, the
artery is completely divided, its cut extremities are to be drawn out
of their sheath by a hook or forceps, and the ligatures applied close
to the connections of the vessel; the vasa vasorum, in the immediate
vicinity of the deligated point, being left to carry on those processes
by which obliteration is accomplished. In punctured or partial wounds
of arteries, it deserves consideration whether the hemorrhage may not
be restrained by the application of slight pressure, so regulated as
to prevent the flow of blood laterally through the wound, but not so
forcibly applied as to stop the onward current of the blood along the
vessel, from the part of the tube above to that below the puncture.
Some experiments made by Dr. Davy seem favourable to this view; as
bleeding from the carotid arteries, partially divided transversely, in
dogs was easily arrested by the means above-mentioned, the wound of the
vessel readily healing, so as to preserve its tube entire; whereas,
when the pressure was increased, the hemorrhage became violent.
The subject is mentioned as one worthy of a further experimental
investigation. The instrument which will generally be found most useful
for laying hold of the vessel is the common dissecting forceps, but a
tenaculum will, in certain circumstances, be more convenient. By far
the most convenient machine is that here represented.

When no assistant is at hand, and in cases of emergency, the surgeon
provided with this little instrument can tie vessels without the least
difficulty; and in operation, when many vessels spring, several of
these forceps can be applied; there is besides this great advantage
in their employment, that a clumsy assistant can scarcely include the
point of the instrument with the vessel. Hemorrhage from the smaller
vessels soon ceases; and, before reaction occurs, their orifices have
generally become so obstructed as to resist the effusion of blood.
The effects of ligature on a vein are somewhat different from those
on an artery. The inner coat of the former is more dense and elastic,
and remains entire, whilst the external and middle are divided. It
is puckered by the ligature, and its opposite surfaces are placed in
immediate contact; but there is no breach of surface, and adhesion171
does not occur till the tunic has been divided by ulceration; then
the opposite margins cohere, the vessel is obliterated, and undergoes
changes resembling those in an artery similarly circumstanced. The
coagulum between the ligature and extremity is of considerable extent,
dense, and completely filling the canal of the vein, and consequently,
of a cylindrical form.
The edges of the wound, in the soft parts, ought not to be approximated
till the bleeding has entirely ceased, and the surface become glazed,
for the interposition of the slightest quantity of blood prevents union
by the first intention. When bleeding has ceased, the divided edges
are to be brought together as accurately as possible, and adhesion
promoted. The minute vessels assume an action greater than in the
healthy state, though not equal to inflammatory action; they effuse
coagulating lymph, by which the opposed surfaces are agglutinated,
though the union is at first feeble and easily broken up. Soon the
lymph is firmly attached, by newly-formed vessels, to the surface from
which it was secreted; in effect, it becomes organised, and rendered
capable of undergoing, through its inherent powers, the changes
necessary for its perfection and stability. Similar processes go on
in it as in any sound part of the body; new matter is deposited, and
the superfluous is absorbed. The process of nutrition, however, is
not the same in all parts of its substance, that is, the new matter
deposited is not exactly similar at all points; but, according as the
new secreting vessels proceed from the different tissues of which the
margins of the recent wound are composed, so, in various parts of the
new formation, these vessels assume peculiar modes of action, one set
forming muscular, another cellular tissue, and a third a substitute for
skin, formations corresponding to the primary tissues from which the
secreting vessels proceed.
Thus the vasa vasorum, ramifying on the divided ends of the minute
vessels, secrete a substance which is transformed into a set of minute
capillaries, and these also, assuming a secretive action, produce an
arterial or venous tube, similar to that nourished by the original
vasa vasorum. By this process the lymph becomes well supplied with
bloodvessels, those from the opposite surfaces meeting, and freely
inosculating with each other. These bloodvessels, as already stated,
have been produced from arteries possessing different powers, and hence
the newly-formed assume actions similar to those of the primary, and
thereby interstitial matter is deposited of its proper kind and in
its proper place, a cuticular membrane superficially, then cellular
tissue, afterwards muscular, and so on according to the primary tissues
which had been divided; these parts do not at first resemble exactly
the corresponding natural tissues, but, by the continued action of
the new vessels and capillaries, they are moulded and prepared for
the due performance of their respective functions. If the degree of
action necessary for the accomplishment of these processes increase to
inflammation, adhesion is interrupted till the action be lowered to its
previous standard.
From this view it is evident, that, besides a certain excitement of
the bloodvessels, it is necessary that the raw margins be in close
apposition, and carefully retained so, for, by ever so slight movement172
of the parts, the recent and delicate bond of union will be ruptured;
and, if this motion be allowed to continue, adhesion may be at divers
times begun, but can never be perfected. Whereas, if the necessary
precautions are adopted, union is often completed in thirty or forty
hours, sometimes sooner, seldom later. From a knowledge of the
astonishing powers of nature in repairing injuries, many and important
improvements have of late years been made in the practice of surgery.
In the majority of instances it is also requisite that the parts be
brought in contact soon after division, otherwise granulation will have
commenced in the different parts of the wound, and the surfaces then
approximated will not so readily adhere: pus is formed, and, having
lodged between the surfaces, acts as an extraneous substance, keeping
them apart, and separating them still farther by its accumulation.
All foreign bodies in the wound must be removed before adhesion can
occur; and, on the same principle, care ought to be taken that no
effused blood be interposed. In many cases the margins of the wound
can be accurately adjusted by careful attention to the position of
the part, or by the application of a few strips of adhesive plaster;
but the latter, from indiscriminate use, often prove the source of
much irritation, and totally frustrate the end for which they are
designed. When employed, they ought to be narrow and few. If such means
be considered insufficient, recourse must be had to a few points of
interrupted suture, and these are not productive of bad consequences
which have been by some attributed to them. When neatly applied, they
can produce but little irritation, more especially if removed as soon
as their presence is unnecessary, that is, as soon as adhesion has
fairly commenced, and the natural bond of union is of such strength
as to need no artificial assistance. By these the edges of the wound
are more neatly and suitably placed than by any other means; they meet
easily, without the puckering or overlapping of each other; and, from
the circumstance of sutures obtaining a more just coaptation, they can
be sooner discontinued. In most wounds no other dressing is required;
but in some a combination of sutures, adhesive plaster, and compress,
is necessary.
Of late, I have greatly dispensed with stitches and the common adhesive
plaster, using, instead of the latter, slips of glazed riband smeared
with a saturated solution of isinglass in brandy, which is much less
irritating and more tenacious than the common adhesive compost. The
parts are fixed temporarily with a single stitch, or two at most, and
cloths dipped in cold water are placed over the wound; the ribands are
not applied till the adhesive substance has partly congealed, and the
oozing of blood ceased. The divided margins being approximated by the
fingers of an assistant, the ribands are laid gently over, and held for
a few seconds. Soon after a sufficient number have been applied the
stitches are withdrawn, being no longer necessary. No other dressing
is required unless suppuration occur; the ribands will adhere firmly
till the completion of the cure, and thus the pain and irritation
caused by frequent dressing is avoided. Even the largest wounds, as
after amputation, are treated in this manner with the most satisfactory
results. Of late years a plaster, made by coating oiled silk with a
solution of isinglass, has173 been used instead; the glazed surface of
the slips is moistened, and applied as here directed.
If at any part adhesion fail, suppuration and granulation must follow.
The adhesion may be prevented by any of the circumstances already
mentioned, or by an unfavourable state of the constitution, the nature
of the wound, exposure to bad air, the occurrence of fever, or of a
flux natural or not. The wound may contain foreign matter; blood or the
contents of canals may be effused into it, and many other obstacles
may exist to retard, or prevent adhesion. Notwithstanding, in all
cases, though the chance of union be but small, the parts should be
approximated. A great point is gained if certain parts only are brought
to adhere, for by their natural attachments the opposite surfaces are
preserved in more direct contact than they could otherwise be, and
thereby but little space remains to be filled up with granulations.
If, on the contrary, the surfaces are not approximated, the flap is
diminished in size, and when afterwards placed in contact with the
surface from which it was detached, it is found not to correspond,
leaving considerable deficiency to be repaired by the comparatively
slow process of granulation. Whereas, if it had been early replaced,
partial attachments would probably have been formed by adhesion, the
flap thereby retained in situ, and prevented from shrinking, so that
but little new matter would be required.
Sometimes union does occur, and that speedily, after the flap has
remained separate for a considerable time; and in such cases it may be
doubted, whether union is accomplished by adhesion, strictly so called.
Most probably it is by this process that the rapid union occurs in such
circumstances: the divided parts have assumed an excited action, and
effused lymph; during their state of separation, the lymph will become
organised when it is connected with the original parts, just as well
as if the surfaces had been in contact; and when they are at length
so placed, they will be agglutinated to each other by the outer part
of the effused lymph, which still continues soft and unorganised. If
motion be then prevented, organisation, which has already commenced
in the connecting medium, will proceed undisturbed, converting the
agglutination of soft unorganised lymph into firm and permanent union
by means of organised tissue. In these circumstances, it is not to
be wondered at if adhesion should be completed in a shorter time
than when the surfaces are brought together immediately after their
division; in each instance the process is the same, only in the one
it has to proceed from its very commencement, whilst in the other it
is previously all but perfected, and after the parts have been put
together, the last stage only requires completion. It is only in a
particular stage of a granulating surface, that adhesion will take
place speedily, when the discharge is diminished, but healthy, and the
granulations florid and firm.
When a wound is to heal by granulation, the exposed surface at first
is dry, painful, and slightly swelled, and afterwards a thin discharge
of bloody serum is poured out, with relief to the painful sensations;
the surface is at this time covered by a thin layer of coagulated
lymph, and the parts, if approximated, are in the most174 favourable
state for adhesion. Soon, however, the vessels assume a different mode
of action, and secrete a fluid which becomes purulent; the effused
lymph has been organised, forms a living part of the surface from which
it was deposited, and is covered and protected, in its yet delicate
condition, by the purulent fluid. This new matter is disposed in
numerous small conical projections of a florid colour; and these, by
their own power, form others similar to themselves, at the same time
discharging purulent matter; so that, in a healthy constitution, the
cavity is soon filled by the granulations, which come to the same level
as the surrounding integument. Sometimes they are exuberant, soft, and
spongy, and in this state possessed of little sensibility, and but ill
supplied with bloodvessels. At others, they are slow in approaching the
surface, and then often morbidly sensible. In all cases, the new matter
is very apt to be absorbed, either from the state of the patient’s
health, or from the nature of the applications; and foreign substances,
in a state of solution or minute division, are more readily taken into
the system from the raw surface than from the sound skin. When, then,
the granulations approach the skin, the sore contracts, the newly
formed parts being modelled into a more firm and dense condition by the
action of the absorbents. Sometimes, in superficial sores, the skin is
seen spreading from several parts near the centre; but at these points
portions of the original skin must have remained uninjured, though
the others were destroyed, and have formed cutaneous matter as soon
as they were on the same level with the surrounding granulations; for
these insulated portions of skin are not a product of granulations, as
some suppose, but of a substance similar to themselves. Skin is formed
from skin. Thus, where a part of the integuments has been completely
removed by operation, or destroyed by accident, no islands of skin are
observed during the cure, but the sore is uniformly covered by skin
proceeding from its margins. The margins of a healing sore are of a
white colour, and adherent to the subjacent parts; but in an unhealthy
one the margins are often unsupported, the subjacent granulations are
absorbed, and their place is occupied by thin purulent matter; the
new skin is unable to maintain its independent existence, continues
of a dark colour, perhaps for a long period, then wastes away or
sloughs. The recent cutaneous matter covering a sore contracts, and the
neighbouring old skin is extended; the new surface is thus diminished;
it assumes a slightly puckered appearance, and is termed cicatrix. This
is at first pretty vascular, the vessels running straight; after a time
they contract and become invisible, and scarcely admit fine injections.
Frequently the scar is so far absorbed after some time, as to leave
only a firm line, whiter and more dense than the surrounding integument.
If union by the first intention does not take place, then all the
application to procure it must be abandoned, all sutures, plasters,
compresses, &c., must be dismissed, for they now can do no good, and
may be productive of harm; the attention, on the contrary, must be
directed to effecting union by granulation; with this view, other means
are to be chosen, so that to continue those which were formerly used
to promote adhesion would be absurd, when adhesion175 can no longer be
expected. The stitches must then be taken out, when inflammation has
gone off, and œdema remains, the parts are to be supported; and by
attention to position, and gentle bandaging, the size of the wound
will be diminished. Inflammation must be subdued by the usual means,
and suppuration encouraged by fomentation and poulticing, or warm
water dressing. After inflammation has subsided, tension disappeared,
purulent discharge occurred, and granulations formed, the edges of the
wound are to be gently brought together, so as to render the quantity
of new matter requisite for filling up the cavity as small as possible.
Nature will then accomplish the union in her own way, and we can only
assist and minister to her; for who thinks now of healing wounds by
pure force of surgery? The dressings ought to be light, the ointment,
if any is used, scanty; in some cases the application may be dry; but
in many cases various lotions will be found of much advantage. These
latter are used of different qualities, according to the nature of the
sore; and these can be of little avail unless evaporation be prevented,
by a piece of oil-silk laid on the outer surface of the dressing. In
most granulating wounds, they require to be of a mildly stimulating
nature, and the one which I have most frequently employed is a weak
solution of the sulphate of zinc. The integuments round the wound may
be occasionally washed, to prevent excoriation, but no good can accrue
from washing the sore; its natural discharge is its best protection,
and if superabundant, it can be removed by means of dry lint or tow
from the surrounding parts.
From bruised and lacerated wounds there is little or no hemorrhage, but
in proportion to the severity of the bruise, is the bleeding slight,
and the danger great. The bloodvessels are so torn and twisted as to
permit the spontaneous and temporary suppression of hemorrhage to
occur almost immediately; and the larger arteries may escape entirely,
owing to their elasticity. Sometimes after bruised wounds, such as
those inflicted by gunshot, the large vessels bleed instantly and
violently; often, however, hemorrhage occurs only after the sloughs
separate, many days after the infliction of the injury, and then it is
generally very profuse; in some instances, limbs are torn, bruised,
or shot away, without hemorrhage occurring to any great degree, or at
any period. Frequently the vitality of the parts surrounding the wound
is much diminished; and the whole limb is apt to become gangrenous,
either immediately, on account of the extreme violence of the injury,
or consecutively, from greatly excited action going on in parts whose
power of resistance has been much impaired: it often arises also from
constitutional peculiarity. The gangrene extends often rapidly, in
consequence of the infiltration of putrid serosity into the cellular
tissue. In the treatment of bruised wounds, the position of the parts
must be carefully attended to; they must be placed in a state of
relaxation. In general, it is unnecessary to retain the margins of the
wound in contact, for adhesion cannot occur—suppuration must ensue,
and is to be desired—and the dead and dying parts must be loosened and
discharged before union can take place. Sometimes, as when a large
flap has been detached, and the parts not much injured otherwise,
approximation176 ought to be accomplished, for the reasons already
mentioned. In almost all cases, and most certainly in those in which
the mechanical injury has been severe, and its effects extensive,
violent inflammatory action is to be dreaded, and measures must be
taken to ward it off: notwithstanding the prophylactic treatment,
violent inflammation often comes on, and then recourse must be had to
the means proper for the subduing of it. Blood is to be taken from
the part, if necessary, and soothing applications used, in the form
of fomentation and poultice. The main indications are to prevent
extravasation into the substance of the limb, and strongly excited
action. When the sloughs begin to separate, emollient poultices promote
the suppuration and discharge of dead matter, and afterwards the
sore must be dressed, according to the nature of the case, with the
applications most fit for granulating sores in their different degrees
of action and advancement. During the after treatment, the sides of the
sore ought to be well supported, so as to prevent, as much as possible,
suppuration from extending along the neighbouring cellular tissue; but,
at the same time, the dressing must not be so tightly applied as to
cause irritation. When abscesses have formed in the neighbourhood, the
cavities should be freely exposed by incision; thus a free discharge
will be given to the matter, and the cavity brought to granulate from
the bottom. During the suppurating stage, the patient’s strength must
be maintained by generous diet.
Punctured wounds are dangerous, from the deep and internal effusion of
blood and serum which usually attends them. The effusion, which in open
wounds is poured out externally, and moderates and prevents the excited
action from exceeding what is salutary, is, in punctured wounds, poured
into the substance of the limb to its detriment. It is followed by
severe inflammatory action and profuse suppuration. In order to prevent
these untoward results, it was formerly the practice immediately to
dilate the wound; but this is hurtful, for if the wound be deep, as it
generally is, dilatation of its whole extent is a proceeding severe in
itself, and in its consequences; whilst, if the external part only of
the wound is dilated, the operation will entirely fail to effect what
is intended. The knife will be used in great good time where a foreign
body is found to be lodged in the wound, when tension has occurred, or
matter has formed. Sometimes the wound heals throughout its whole track
by adhesion, without any bad symptoms being so much as threatened.
Setons, recommended in this class of wounds, are of no service. It is
not the narrowness of the external opening, as is sometimes supposed,
that is the cause of all the mischief, but the injury and consequent
inflammation of deep-seated parts.
Poisoned wounds are rare in this country. Wounds by the stings of
certain trifling insects produce considerable swelling in some
constitutions, and when the injury has been inflicted on a loose
texture. In some parts of this country, the bite of a small adder
causes pain, swelling, and unhealthy suppuration of the part, with
some constitutional disturbance, but the results are seldom serious,
and never fatal. In warmer climates, the bites of some snakes are
followed by the most violent symptoms; in some cases proving fatal
in a few hours,177 in others after a day or two. Great swelling occurs
almost immediately, attended with excruciating pain, and extends upward
along the limb; vision becomes impaired, the patient lies in a state
of stupor, and ultimately succumbs under convulsions and delirium; the
symptoms vary in particular instances according to idiosyncrasies and
the state of the constitution when the injury is inflicted.22 In this
country, the bites of rabid animals are more dangerous than those of
animals naturally poisonous. Rabies most frequently occurs in dogs,
and others of that species, such as wolves, foxes, &c. They become
dull, sluggish, and irritable; have unnatural appetites and cravings,
devouring their excrement and urine; the stomach is generally found
full of chopped straw, pieces of wood, &c. Derangement of the cerebral
functions is not complete,—they know and obey their master. They are
often not afraid of water, but lap it and go into it readily. From them
the disease is communicated to the human subject, and to the lower
animals, such as cats, sheep, cattle, and even fowls; the virus is not
communicable, except by the deposition of the saliva on an abraded
surface, or into a wound. It is not produced by eating the flesh of a
rabid animal. During the first days of the attack, pustules are, it is
said, observed under the tongue, but there is no apparent change in the
glands. The symptoms of hydrophobia in man seldom appear before the
twentieth day after the infliction of the wound, 178and in some instances
they have not presented themselves till after the lapse of months. The
most prominent are great restlessness, much irritability and anxiety,
and convulsions of the muscles concerned in deglutition, produced
either by attempts to swallow, or by fluid being presented to the
patient. Ultimately, the spasms become general, are induced by the most
trifling exertions or noises, and prove fatal in a few days. Frequently
the patient retains his senses throughout, and is fully aware of his
lamentable situation; in other instances, he soon becomes delirious,
raves, and threatens his attendants. For this horrible disease we
are unacquainted with any cure. In general, profuse bleedings are
employed, and large quantities of opium given internally; every
powerful antispasmodic, as well as every violent medicine, has been
made trial of, but in vain: some certainly mitigate the symptoms, but
none cure the patient. It has been even proposed to suspend or destroy
the function of the nervous system for a time, by the employment
of the Wourali poison, keeping up at the same time respiration by
artificial means, under the expectation that thus the impression
on the system might be got over. The morbid appearances usually
observed after death are marks of inflammation of the pharynx and
air-passages, and of the mucous surface of the stomach and intestines.
It is evident that the disease ought to be prevented if possible, and
for its prevention the most efficient measure is timely excision of
the affected parts; and they should be cut out a long period before
the constitutional affection comes on: when excision is dangerous,
or wholly impracticable, and when the patient does not apply soon
after the accident, the injured parts may be destroyed by some active
caustic, as the potassa fusa. The nitrate of silver has been strongly
recommended and extensively employed by Mr. Youatt, whose experience in
this disease is very great. This application should scarcely be trusted
to alone. The removal of parts wounded by snakes, even after violent
symptoms have appeared, has proved successful, ammonia having been
at the same time administered internally. In some instances, arsenic
has been found efficacious when given in large doses, and frequently
repeated.23
179
Wounds received during dissection occasionally have unpleasant
consequences from the absorption of animal matter. The absorbents
leading from the wounded part become swelled and painful, and in
slight cases there are shivering and general indisposition for some
days. The more violent symptoms arise from examining bodies which are
rather recent, and in which putrefaction is just commencing, and very
frequently from inspecting the bodies of females who have died of
puerperal diseases. The absorption may take place from punctures made
by scissors, the point of a knife, or spiculæ of bone, or from old
scratches, or chops by the side of the nail or on the hand. There is
little or no danger from an open and bleeding wound, as by the flow
of blood the part is completely cleaned; it is generally from slight
punctures that untoward symptoms need be apprehended. Effects similar
to those resulting from wounds in dissection often occur in nurses
and others who have pricked themselves with pins while washing foul
clothes, or from handling poultices or dressings removed from bad,
putrid, or sloughing surfaces. The symptoms already mentioned are soon
followed by others more severe: shivering continues, and the patient
is seized with vomiting; the part affected, and often the greater
part of the arm, becomes red and much swollen; the cellular tissue
is infiltrated with serum often dark and putrescent, abscesses form
at various points along the limb to the axilla, and purulent matter
is diffused throughout the unhealthy cellular tissue, which in many
instances sloughs, and gives rise to extensive sores. Typhoid symptoms
soon appear, and in the more aggravated cases speedily prove fatal.
When such local and constitutional symptoms arise, it will generally be
found that the patient was of a broken-up constitution previously to
the infliction of the wound; did they solely depend on the inoculation
of virus, they would be of very common occurrence, considering that
wounds are so frequently received during dissection; but it is seldom
comparatively that any unpleasant symptoms follow such an accident. In
all cases, however, it is prudent to adopt measures in order to prevent
absorption of the virus. With this view, the wound is made to bleed
by means of pressure or suction, and by the latter method the exposed
surface is most effectually purified; afterwards nitrate of silver
maybe applied to deaden the surface, and protect it by an eschar. If
such means be unavailing, the after symptoms must be encountered as
they appear, local inflammation subdued, tension re180lieved, abscesses
opened, sloughs removed, &c. General bleeding is seldom admissible, but
purgatives and antimonials will prove beneficial at the commencement;
afterwards the strength is to be supported, and, if the patient be much
reduced, stimulants are to be liberally administered.
We shall next treat briefly of gunshot wounds; under this head are
included the contused and the lacerated, caused by splinters, &c.
The vitality of the injured surface is generally destroyed at once,
whence bleeding seldom occurs, even after whole limbs have been shot
away; in some cases, however, hemorrhage is profuse, as when a large
artery has been wounded by small shot. The effects on the system are
extremely various; some persons are affected with tremors, anxiety,
and depression from slight wounds; while the most severe injuries
are often unaccompanied by any disturbance of the nerves. The shock
is generally of short duration, disappearing soon, on the patient’s
being reassured and encouraged, or after his taking a little wine or
opium. In gunshot wounds, those inflicted from a distance or close
at hand can in general be readily distinguished. In the latter, the
wound is large and lacerated, portions of the wadding are impacted,
and the skin around is marked with grains of gunpowder. In the former,
the wound is small and clean. When a ball passes through a fleshy
part, the opening at its entrance is small and depressed; whilst that
by which it escaped is open, with everted edges. When it follows a
superficial course, its track is marked by a wheal, or elevation of the
skin with discoloration. At one time, it was believed that the most
serious consequences resulted from a ball passing close past the body
without even touching it—that in this way violent concussion of the
brain, proving instantly fatal, was produced; but this notion has been
disproved by experience; part of the head accoutrements, of the hair,
of the nose, and of the ears, have been shot away by cannon-balls, and
yet no disturbance of the brain has followed either immediately or
consecutively. The opinion originated from the circumstance of soldiers
having been found dead without any evidence of injury; but bones are
often broken and comminuted by an indirect blow, or by a spent ball,
without any breach of surface or external sign remaining; internal
injuries indeed—rupture of viscera—more than sufficient to cause
instant death, are thus inflicted without any apparent external læsion.
The course of a ball in the body is often very strange, depending
on the force with which it is projected, or the resistance which is
opposed to it, and on the position of the struck part. Balls often pass
under the integument almost completely round the head or chest, having
first struck the bone at a very oblique angle. Frequently they remain,
lodged along with part of the clothing which they thrust before them.
In such cases, they may be immediately removed, their exact situation
being previously ascertained by external examination, or by means of a
probe. They can generally be extracted through the aperture by which
they entered; but if situated superficially, and at a distance from the
opening, this will be more readily accomplished through an incision
made upon them; if allowed to remain, suppuration will occur in the
neighbourhood, the surrounding cellular tissue181 will be condensed, an
abscess will be formed containing the foreign body, and by the process
of absorption proceeding in the parts external to the abscess, the
ball will at last reach the surface, and be discharged. The track is
often so extremely tortuous, as to render it impossible to ascertain
the situation, or even the existence of the foreign body, which greatly
impedes the operation; and, in other instances, it may be necessary to
allow the ball to remain undisturbed, on account of its being placed
near important parts, which might be injured by any attempt at removal.
Foreign bodies often remain lodged in fleshy or membranous parts for
years, having become enveloped in a dense cyst, and having ceased to
produce any great irritation. In consequence of the force with which
they have been projected, and the resistance which has been opposed
to their progress in the body, musket-balls, when extracted, either
immediately after the infliction of the injury, or after a considerable
time has elapsed, are seldom found to retain their globular form, but
are flattened and ragged, and not unfrequently completely divided by
the bones on which they have impinged. A bullet may be divided into
numerous fragments on a bone, and part may enter into the osseous
substance, whilst other portions penetrate in all directions into the
soft parts, and, though sharp and irregular, may remain long in the
dense cellular cyst which forms over them, without producing pain or
inconvenience. There will necessarily be suppuration, and generally
discharge of dead matter, from gunshot wounds, in consequence of the
bruising of the parts by the ball, which may be expected to injure
the superficial layer of parts in its tract so severely, that it must
slough more or less.
Besides, the bones are often splintered by the force with which they
are struck, and loose portions of them lodge amongst the muscles; then
they are the cause of much mischief, for, on account of their long,
sharp, and irregular form, they occasion great irritation, suppuration
ensues in various parts, sinuses form, and the cure is rendered very
tedious. In other cases, the bone is split in a longitudinal direction,
and, in the cylindrical bones, these fissures are often of great extent.
Considering the nature of the body which inflicts the injury in a
gunshot wound, and the velocity with which it is impelled, it is
evident that the cure must be in all cases tedious, in consequence of
the sloughing and suppuration which is induced, particularly at the
aperture through which the ball passed. The foreign body ought always
to be removed as early as possible, provided it can be accomplished
without much violence, or injury to the parts. Dilatation of gunshot
wounds is now had recourse to only to facilitate the removal of balls,
splinters, &c., and even with this view, it ought to be employed but
to a very slight extent, if at all; for foreign substances, when
deeply seated, can be much more easily taken out when the sloughs are
separating, and the parts relaxed by suppuration; then, too, they can
be more readily reached through a counter-opening, when their situation
renders this expedient. In short, the surgeon is not justified in
cutting for balls, unless they are easily felt, and not deeply lodged.
In order to discover the foreign body, probes will sometimes be
required; the finger often answers the purpose best, unless when the182
wound is of considerable depth. If, on examination, the ball cannot be
discovered, and if there is reason to think that it has followed an
indirect course, the surgeon will, sometimes, be assisted in his search
by placing the patient in that position in which he received the wound,
and then judging of the circumstances most likely to affect the foreign
body in its passage. In many cases, extraction can be accomplished
by means of the finger alone; in others, forceps and scoops, various
in length and size, are indispensable. Afterwards, light dressings
are to be employed; and in the first instance, cold applications
may prove advantageous in keeping down the inflammatory action; but
when inflammation has commenced, and to encourage suppuration, warm
fomentations and poultices are to be preferred; they will in many
cases be both more grateful to the patient and more beneficial in
their results, when used even from the commencement. Afterwards,
it will be necessary to afford sufficient support to the parts by
bandaging, and to change the applications according to the particular
circumstances:—soothing, if the wound be irritable, stimulating, if
inert, and gently escharotic, if the granulations be exuberant.
In severe injuries of the limbs, the surgeon must be guided by the
state of the part, and of the constitution, by the circumstances in
which he is placed, as to accommodation, and mode of transportation,
&c., in deciding on the removal of the part by amputation,—or on
making an attempt to save it, by trusting to, and assisting, the
processes of nature. The question whether to amputate immediately,
and on the spot, merely allowing the shock, if any exist, to pass
away, or to delay till suppuration occur, is now scarcely a matter of
dispute. When it is evident, from the extent, violence, and nature
of the injury, that there is danger of speedy mortification, or of
extensive and severe inflammation and suppuration, amputation is to
be instantly performed,—delay is inadmissible. In comminution of the
hard, with contusion and laceration of the soft parts—where limbs have
been shattered and completely detached, or nearly so—in lacerations of
parts, including the principal bloodvessels and nerves—fractures of
the heads of bones, with openings into the joints—and in bad compound
fractures, more especially of the thigh (for all compound fractures
of the upper part of the thigh are dangerous), amputate at once.
When the limb has been retained, and gangrene arises in consequence
of the external injury, and when there is no reason to suppose that
any internal cause is also in existence; or when the violence of
inflammatory action has subsided, and the patient is become hectic,
with profuse purulent discharge, and with disunited bones, then
amputate. But, in this latter case, the chance of recovery is not
so great, and the proportion of recoveries small; whereas, in the
immediate or primary operations, the very reverse holds true. Such is
the experience of the greater number of military surgeons. In civil
practice, the results are somewhat different; a greater proportion of
primary amputations are unsuccessful, and the secondary turn out more
favourably than the statements of military surgeons would lead one to
believe. In all cases, the judgment of the surgeon must guide him in
his determination. The circumstances of the case, and the probable
contingencies, must be all duly considered, and he must not proceed183
with his knife where there exists even a slight chance of preserving
the limb.
Paralysis occasionally follows wounds of the arm, forearm, face, &c.,
inflicted by accident or operation, and this arises from an important
nerve, or set of nerves, being divided. In cases of simple division,
without much separation of the parts, reunion of the nerves may take
place, and their functions be restored. If the limb remains paralysed,
after cicatrisation of the wound, tepid effusions, friction, dry
or with liniment, stimulating applications, &c., may sometimes be
advantageously employed.
TETANUS
Is a disease which occasionally follows a wound, but rarely in this
country. It is a spasmodic contraction, with rigidity, of the voluntary
muscles, in some cases involving the whole body, in others the upper
part of it only, and in some it is confined to a certain class of
muscles. When the extensors are affected, the disease is termed
opisthotonos; when the flexors, emprosthotonos. Complete tetanus is
said to exist when the flexor and extensor muscles exactly balance
each other, and the body is thereby kept straight and rigid. But when
the affection is confined to the muscles of deglutition, and chiefly
to those moving the lower jaw, it is called trismus. The disease has
besides been divided into acute and chronic, and into traumatic and
idiopathic; the one following wounds, the other arising from internal
causes, or circumstances not connected with the læsion of the surface.
The disease supervenes at various periods; sometimes, though rarely,
not long after the infliction of the injury, in other instances after
the lapse of eight or ten days, and often when the wound is healing,
or nearly cicatrized. In warm climates, where it is of very frequent
occurrence, it occasionally seems to be caused by exposure to damp
and changeable weather; in children, it supervenes on the slightest
irritation. It is often induced by the presence of splinters, or
rather bodies of an irritating nature, and by the partial division of
nerves. Not unfrequently it occurs after clean wounds, as amputation
or venesection; in the former it may perhaps arise from a nerve being
included in the same ligature with an artery, in the latter, from a
nervous twig being partially divided. The more prominent symptoms are,
stiffness of the back of the neck, and contraction of the features;
difficult deglutition supervenes, and the efforts to accomplish it
are attended with violent spasms of the muscles of the pharynx and
œsophagus. Spasms of the injured limb often precede those of the
muscular system generally; the muscles of the lower jaw become rigid
and spasmodically contracted, and by a continuance and increase of
the spasmodic action, the mouth is at last completely and immovably
shut. The muscles of the trunk and limbs become affected, and there
are violent spasms of particular sets of them, most generally of those
situated posteriorly; thus the body is bent violently backward, so
that its whole weight is supported on two points only, the heels and
the oc184ciput. These symptoms are not constant; relaxation occurs,
and the patient enjoys a cessation of the malady: but this is only
temporary; the painful feelings and the spasms soon return. A symptom
of the most distressing nature is pain and spasmodic twitching of
the diaphragm, impeding respiration, and imparting a shock to the
whole system. Occasionally, emprosthotonos occurs, but, so far as my
experience goes, the body is much more frequently bent backward; the
muscles are sometimes ruptured by the violence of their own action.
The circulating system and sensorial functions are often not much
disturbed; but during the whole course of the disease, the bowels
are much constipated. In most cases of traumatic tetanus, after four
or five days, all the symptoms become aggravated; the countenance is
horribly distorted, the spasms of the diaphragm are more frequent and
violent, and the patient dies convulsed. Sometimes, though rarely, the
fatal termination does not take place till the eighteenth or twentieth
day. On dissection, the pharynx is found contracted, and bearing marks
of acute inflammation. In one case, which fell under my observation,
there was ultimately great difficulty in breathing and expectorating;
and on examination, the trachea, as well as the pharynx, bore evident
marks of inflammation, and were filled with a viscid mucus. In some
instances, there are evident marks of inflammation of the spinal
chord; the vessels, more especially at the lower part, are found
enlarged, tortuous, and engorged with blood; portions of lymph are seen
deposited on the arachnoid covering, and a serous fluid is effused,
not unfrequently mixed with blood. Such appearances, however, are not
observed in every case of fatal tetanus, and therefore it cannot be
asserted as a fact, that the disease is dependent on a morbid condition
of the spinal chord, though in certain cases the two affections
coexist. By some it has been supposed, that in consequence of the
distended and engorged state of the spinal arteries, the origins of
the nerves are stimulated, and that a morbid affection of them ensues,
giving rise to the tetanic symptoms; but want of uniformity in the
morbid appearances prevents such a cause from being generally set down
as the origin of tetanus.
This disease is one of the most intractable with which the surgeon
has to contend. In the acute form, time is scarcely allowed for
remedies; and in the advanced stage, it is with much difficulty that
medicine can be received internally. Of course all irritations must be
removed, both local and general, as far as that can be accomplished.
If the patient be robust, and if the tetanic symptoms be ushered in
with arterial incitement, general depletion ought certainly to be
practised; and if the symptoms be such as to render the propriety of
general bleeding dubious, blood may be abstracted locally, from the
back of the head, or along the spine; and this may be followed by such
counter-irritants as act rapidly. At the same time, powerful purgatives
must be given, so as to bring the bowels into a better state; for, as
already observed, obstinate constipation is a constant attendant on
this disease. But the most important indication is to alleviate and
prevent, if possible, the spasms; and for this purpose, opium is to be
administered in large doses, either by itself, or combined with camphor
or other antispasmodics. By such means, the185 disease has in some cases
been arrested, but in the majority it has proceeded unabated. Some
practitioners recommend and employ cold affusion and immersion, whilst
others prefer the warm bath; and the latter appears to be the safer
application, though neither can be considered as efficacious. Great
relief and benefit seem to have accrued from the frequently repeated
use of a warm bath, with some drachms of the tart. antimonii dissolved
in it. I have had only two opportunities of trying this practice; one a
chronic ease, where, after the division of the nerves proceeding from
the wound, this remedy, with others, seemed to allay the spasms in a
very remarkable manner: the patient recovered. In the other, a very
acute case, after the extraction of a splinter from betwixt the thumb
and forefinger, the bath was tried; the patient felt much comforted by
it; but suddenly expired in a violent convulsion, whilst being replaced
in bed. Great relaxation follows this remedy, profuse perspiration,
and subsidence of the rigidity and convulsive action of the muscles.
The practice was recommended to my notice by my excellent friend Dr.
Stevens, Professor of Surgery at New York. In some cases, it would be
worth trial to produce instant vesication by the acetic solution of
cantharides or ammonia, and then try the effect of the application
to the blistered surface of some of the alkaloids, such as morphia,
aconitine, &c., or belladonna might be applied.
Some practitioners have used mercurial frictions along the spine, or
on other parts of the surface; while others administer stimulants,
and enemata with tobacco and turpentine. When there is reason to
apprehend that the symptoms arise in consequence of laceration or
partial division of a nervous trunk, it has been recommended to
complete the division of it; and the practice is worthy of adoption,
as in some cases it appears to have been successful. Little good can
result from scarification of the wound. Amputation of the wounded
member has also been proposed, particularly in chronic cases, and
in one or two it has succeeded. I have made trial of it in but one
instance, and in that it failed. Acute tetanus had followed a lacerated
wound betwixt the thumb and forefinger; amputation of the forearm
was performed, and immediately after the operation the spasms abated;
but they soon returned, notwithstanding the free use of opium, and
other remedies, and the patient died. In this case, the branch of the
median nerve was found partially divided, and its cut extremities were
thickened and inflamed. During the operation, I wished to abstract
a considerable quantity of blood, but the arteries seemed to be so
spasmodically contracted, as to permit the flow of a small quantity
only. On examination after death, the median nerve was of its natural
appearance, excepting at the bend of the arm, where it was of a
bright-red colour. No change could be perceived in the brain or spinal
chord, though the examination was conducted with the utmost care.
186
OF ULCERS.
By ulcer is generally understood a breach of continuity in the soft
parts of the body, with secretion of purulent or other fluid. But as
suppuration may be independent of ulceration, so may we occasionally
see a loss of substance like an ulcer on the surface of parts,
without the production of pus, or any other morbid secretion, of
which some instances are noted in the remarks on Atrophy of Articular
Cartilage. Mr. Burns, in his excellent volume on the Principles of
Surgery, has extended the term to the reparative process, as well
as the destructive; this, if adopted, would lead to confusion and
misapprehension.
Ulcers vary much in disposition and appearance, follow wounds,
abscesses, sloughing, eruptions, &c., and often occur without any
previous læsion of the surface. Those most generally met with are
comprehended in the following classes:—1. The simple purulent ulcer,
or healthy or healing sore. 2. The weak or sluggish ulcer,—a sore
with undermined integuments and an unhealthy state of the cellular
tissue. 3. The indolent ulcer,—a sore with hard elevated edges, and
presenting little or no appearance of reparation. 4. The irritable
ulcer,—a sore with over-action, and generally affecting only the mere
surface of the true skin. Besides these, there are sores connected with
diseases of the bones, and others arising from specific action; some
are complicated with a varicose state of the veins: the former have
been already treated of; the latter are reserved for consideration.
Ulcers change their characters, as from simple to irritable, and from
indolent to inflamed; the change depends on situation, on the state of
the constitution, and on the treatment which they receive.
I. The appearances of the first class were described when the healing
of wounds by granulations was considered, p. 173. They heal more
readily on the upper extremities, on the face, neck, and trunk, than
on the lower limbs; for in the former parts the circulation is more
vigorous, the natural processes of cure proceed more easily, and are
less liable to interruption. The sore only requires rest, a clean
condition of the surrounding parts, mild and light dressings, and
moderate support; dry lint or lotions are preferable to ointments,
since the latter are apt to irritate by their rancidity. When the sore
is of considerable size, and there is a tendency in the granulations to
rise above the level of the surrounding skin or cicatrix, the edges may
be protected by very narrow slips of fine old linen or cambric, spread
with fresh spermaceti ointment or cold cream; a pledget of dry lint is
then laid on, and retained by a roller. The dressings thus arranged
do not adhere, and the tender cicatrix is not ruffled and disturbed;
or a piece of pierced linen spread thinly with unirritating ointment
may be placed over the sore, and above that dry lint. When the sore
has contracted to a small size, and some powder, as starch or calamine
stone, or a piece of dry lint, may be applied, so as to allow a scab
to form for the protection of the subjacent surface; but this will,
in most cases, be better accomplished by touching the surface lightly
with lunar caustic or blue stone; the fluids on the187 part are thereby
immediately coagulated, a crust is quickly formed, and by covering it
with charpie, it is retained in its situation, whilst the process of
cicatrisation proceeds beneath it: if a small quantity of matter should
be secreted, it readily escapes by the sides of the crust, without
disturbing either it or its covering; the limb should be raised above
the level of the trunk. Sores on the lower limbs are always difficult
to manage. The reparative process is tedious, on account of their
situation; the parts are at a distance from the centre of circulation,
their action is weak, the return of blood is tardy, and the same
facility is not afforded of restraining the motions of the part as in
the upper extremities. In persons of a good constitution, however,
the simple purulent sore often heals speedily, even in the lower
limbs. Before cicatrisation can take place, it is essential that the
granulating surface should be on a level with the sound surface around;
this soon takes place when a favourable position is observed, and the
part is kept at rest; but by neglect, the new matter is often absorbed.
Again, the healing process cannot advance where the granulations are
exuberant, large, and flabby, and have risen above the proper level:
they must be kept in check by due compression, and by astringent
lotions, containing salts of zinc, copper, &c. The constant meddling
with sores, the touching them with this, that, or the other caustic, is
much to be reprobated. Should it be necessary to destroy granulations,
and bring them down to the surrounding surface, one good rubbing with
the blue stone will generally suffice. If the ulcer is large, the
granulations close to the cicatrix should only be destroyed, leaving
the centre to be dealt with as the cure advances.
During the cure, the patient must be a good deal confined to the
recumbent posture; when erect, a bandage or laced stocking must be
applied to the limb; thus the return of blood is assisted, swelling
is prevented, and the affected parts placed in a state of comparative
rest. Much pressure ought to be avoided, as it is apt to produce
bad effects upon the sore, causing absorption of the granulations,
thin bloody discharge, and great tenderness of the surface. After
cicatrisation, the scars may be absorbed, and sores reproduced, by
external injuries, or an unhealthy state of the body; and so much does
the state of a sore depend upon that of the general health, that the
one is a good index of the other.
II. In the second class of sores, or those with weak action, the
granulations are flabby, of a pale colour, and possessed of little
sensibility or vascularity; the discharge is gleety, and the surface is
liable to be destroyed by ulceration or sloughing, upon the slightest
excitement of the circulation in the part. The surrounding integuments
are generally of a bluish colour, in consequence of their separation
from the subjacent parts; and in several places of the neighbourhood,
small, unhealthy, detached abscesses may exist; at some points of the
sore, glairy fluid is seen to ooze out on pressure, and a probe can
be passed pretty deeply into the cavity of an abscess in the soft
parts beneath. These sores may arise from an unhealthy condition of
the cellular tissue, taking place spontaneously, or following slight
injury; they are attributable to the state of the constitution, and
may result from an ulcer, originally of a healthy188 character, which
has remained long open, in consequence of its great size, or other
impediments to its contraction.
It is the business of the surgeon, in cases of this description, first
to obtain a sound foundation, by destroying the unhealthy skin and
cellular tissue; the free application of caustic potass will answer
this end most readily and effectually. Its application is attended with
considerable pain, but the practice is more successful and less severe
than the removal of the unsound parts by the knife or other means. The
small abscesses may be all freely laid open; the diseased cellular
tissue may be cut into, or cut away; in short, incisions may be made in
all directions, and in every portion of the affected part; but still
it will be found that the granulations, as they appear, become pale
and flabby, that they spring from a loose and powerless base; matter
will again collect; the surrounding skin will again be undermined; no
progress will be made towards soundness. But by attention to the state
of the constitution, and the application of potass, the neighbouring
sound parts have their actions roused, and the healing is carried
on rapidly. After its application, a poultice may be applied for a
few days, and followed by water dressing, and then stimulants, both
internally and externally employed according to circumstances, the
parts being all along well supported. The long continued use of warm
fomentations, or poultices, is prejudicial, as tending to diminish
still farther the action of the parts; ointments can be of little
service, and will generally do harm.
III. Indolent ulcers, which have long existed, are frequently met
with on the lower limbs. Their margins are thick and insensible—their
surfaces smooth, hollow, and of a pale colour—the discharge is
scanty, and adheres to the surface. A sore, having been long open and
neglected, degenerates into this state. Poultices are to be applied for
a day or two, to clean the surface, promote the discharge, and soften
the callous margins. This is the more necessary, if, as is often the
case, the sore, or the surrounding integuments, are inflamed when the
patient applies for relief. Afterwards, the applications must be of
such a nature as to moderate the discharge and keep the granulations
firm and healthy. In such cases only is adhesive plaster applicable,
and in them it produces the most beneficial results. Supposing the
ulcer to be situated on the fore and middle part of the leg, a bandage
should first be firmly applied from the toes to a little below the
sore; the ulcerated part of the limb is then encircled by narrow
strips of adhesive plaster, tightly drawn, and with the extremities
of each strip crossing immediately over the ulcer. A pledget of tow
is placed on the plasters to absorb the discharge, and the bandage is
brought over dressings, and continued for some way upward. By this
application, the margins of the sore, it is supposed, are brought
nearer to each other, and the ulcerated surface diminished; the
sluggish granulations and the subjacent parts are stimulated, and a
more vigorous action being excited, the process of reparation proceeds
speedily and effectually; the surrounding parts, previously turgid
and œdematous, are by the pressure brought to the same level with the
newly-secreted matter, and new skin is quickly formed. In the previous
state of matters, the old skin was much189 elevated, and an action was in
progress, causing a continuance of that elevation; by the compression,
the whole limb is properly supported, serous effusion prevented,
absorption excited, and œdema removed; the livid swelling of the lower
part of the limb, which might arise from the tightness of the adhesive
plaster, is obviated by the bandage being first applied. A feeling of
uneasiness in the limb sometimes follows such dressing, but is of short
duration; should it increase, so as to amount to pain, the elevation of
the limb and the pouring of cold water occasionally over the dressings
will soon restore the parts to comfort. Or the adhesive plaster may
be slit up behind, immediately after its application; indentation of
the limb being thereby avoided, and sufficient pressure at the same
time kept up on the sore. If possible, the dressings ought not to be
removed before the second day, as much irritation will be produced
by their frequent renewal. The benefits arising from this mode of
treatment are truly surprising; the slow and indolent ulcer is speedily
converted into the simple purulent sore; the white and recent cutaneous
substance encircles small pointed and florid granulations, which bleed
from the slightest rudeness of touch; and the space formerly occupied
by an unsightly sore is soon diminished to a small and firm cicatrix.
It is only necessary to continue this mode of dressing so long as the
granulating surface is below the level of the surrounding surface.
Then the object being attained, the deranged state of the cellular
tissue being got rid of, and the ulcer put in a state favourable for
cicatrisation, the sulphate of zinc lotion not over strong may be
resorted to; positive rest and support of the affected part being still
enjoined and observed. In the old and debilitated, however, in whom the
indolent sore most frequently occurs, the integuments remain purple
and shining, and from very slight causes the cicatrix is absorbed, and
breach of surface is reproduced.
These sores are often connected with a varicose state of the veins.
In all such cases, a degree of compression on the affected limb must
be maintained, both during the continuance of the sore, and after it
has healed. The usual situation of such sores is on the leg, and the
varicose state of the veins does not, in general, extend above the
knee; in such cases, a radical cure may be attained (provided the
patient wishes to encounter the attendant risks, rather than submit
to a continuance of the disease) by effecting an obliteration of the
saphena major vein. The manner of doing this, and its effects, were
mentioned while treating of diseased veins. In some cases, the saphena
minor is also varicose to some extent, the varices on which must also
be obliterated. Sometimes as many as eight or ten needles must be
applied, in pairs, before the circulation of a limb can be brought into
a right state.
IV. In this fourth class of sores, or the irritable from over-action,
the sore and its edges are of a jagged, irregular appearance, the
discharge is thin and bloody, and considerable pain is experienced.
This ulcer is very superficial, involving only the surface of the
corium and the more sensible part of the integument, the papillæ,
and extremities of the nervous filaments. They often succeed to
scaly eruptions, and present a remarkable character and appearance,
cica190trising in the centre, whilst they extend towards the
circumference. The sore is often covered by an ash-coloured slough;
on the removal of which, granulations arise, but these either again
slough, or are removed rapidly by the ulcerative process. In the
treatment of such sores, complete rest and soothing applications
are the means on which most reliance is to be placed. Warm and
soft poultices, such as those of arrow-root, fomentations, tepid
water dressing, solutions of opium, or of extract of poppy, and the
occasional use of a local vapour bath to the part, may be enumerated
amongst the means best fitted to allay the irritable condition of the
ulcer. When the surrounding integuments are swollen, red, painful,
in short, evince marks of inflammatory action going on in them, the
feelings of the patient will be rendered grateful, and the cure
advanced, by abstraction of blood from the parts by punctures. When the
nature of the sore is changed, and when cicatrisation has commenced,
the treatment is similar to that of a simple granulating surface—light
dressings, due support of the parts, and repression of exuberant
granulations by the sulphate of copper. The nitrate of silver, applied
in substance round and about the ragged edges, is of great service at
an earlier period. This practice must be sparingly and seldom resorted
to, but it does wonders when judiciously employed.
Ulcers are occasionally prevented from healing by the presence of dead
portions of tendon, fascia, or cellular tissue, and are accompanied in
general with a bad state of constitution; in such it is necessary to
clean the surface by a powerful escharotic, and the best is potass.
Otherwise, granulations will be produced quickly, it is true, and in
abundance, to supply the original substance; but then they are flabby
and exuberant, new skin is formed slowly, if at all, and the sore does
not contract; but by removing the dead or half-dead surface, a healthy
and firm foundation is prepared, on which is securely and gradually
raised the new matter for cicatrisation. But caustics are applied
injudiciously to firm and healthy granulations which have not yet
reached the level of the surrounding parts; they are only useful in
repressing exuberant granulations, or in destroying half-dead parts,
which interrupt or deteriorate the cure: and when employed, it should
be effectually, and once for all.
Along with the topical treatment of ulcers, internal means are, in
most cases, indispensable. Thus, in indolent ulcers, the state of
the constitution is often sluggish, and ought to be changed by the
exhibition of alteratives or stimulants; with this view, much benefit
is derived from a prudent and restrained use of mercury, from the lytta
vesicatoria, from minute and occasional doses of arsenic, from the free
exhibition of sarsaparilla, and from generous diet, porter, and wine.
It is however, altogether impossible to lay down fixed rules for the
management of sores; every one has some peculiarity in its nature and
appearance, every one requires some peculiarity in the applications
and mode of dressing, and what may suit well one day will often prove
inert or injurious on the succeeding. Again, when any one application
or internal remedy is found to agree with the sore, it ought not
to be changed for fashion’s sake, from caprice or routine. In this
department of surgery, one practitioner excels another, not by his
supe191rior knowledge of the various applications, but by his acuteness
in selecting the remedy adapted to the particular state of the sore,
and in accommodating the various ointments, lotions, or powders, to the
different characters which the ulcer assumes during its progress. The
healing of sores is very easy in some constitutions, and very difficult
in others. Hence, it has been supposed that the long existence of a
sore is a salutary process of nature, tending to relieve or prevent
some more serious affection, and on this account some are little
solicitous to procure its cicatrisation, or at least are careful that
the cure shall not be a speedy one. If, indeed, an extensive sore,
or a series of sores, be suddenly dried up, the circumstance must be
considered as very unfortunate, and the consequences may even be fatal;
but such an occurrence is unusual, and the patient may in general be
saved by the timely insertion of an issue in the neighbourhood of
the sore, or by an active employment of what is best calculated to
insure a renewed discharge. Some sores have a disposition to extend
by sloughing, and such frequently attack the lips and pudenda of
weakly children; they are also met with, amongst the lowest class of
prostitutes, in the cleft of the nates, in the groin, &c., and in such
cases the sore closely resembles hospital gangrene.
OF HOSPITAL OR CONTAGIOUS GANGRENE, AND SLOUGHING PHAGÆDENA.
This disease has been long known, and has proved very fatal in crowded
and badly-aired hospitals. It may break out at any season, but hot,
sultry, and damp weather is most favourable to it. No breach of
surface, however small, is secure from its attack. The wound becomes
painful and swollen, and loses its healthy, florid appearance; the
granulations are flabby, and appear as if distended with air; vesicles
form, containing serum or a bloody fluid; the pain is stinging; the
secretions are suspended; and the wound is either altogether dry,
or covered with slimy, tenacious, and peculiarly offensive matter.
An ichorous discharge follows, the pain increases. The sore assumes
a circular form, and its edges are everted; erysipelas attacks the
surrounding integuments, often extending over the whole limb, and
forming a principal feature of the disease. In fact, violent erysipelas
and hospital gangrene are affections very closely allied to each other,
often arising at the same time, and from the same causes. Both are
accompanied with great constitutional disturbance; but in erysipelas,
this generally precedes, whilst in hospital gangrene, it follows, the
appearance of the malady. The lymphatic glands, in the neighbourhood of
the gangrenous part, inflame and suppurate, the skin gives way, and the
gangrene soon seizes the newly-formed sore. Fever supervenes, the pulse
is often full and strong, and the surface hot; there is great nausea
and thirst; the tongue is brown, and the bowels much disordered. The
inflammation and ichorous discharge increase. A thick slough covers the
sore, and its fetor is peculiar and intolerable. The burning pain is
excruciating. Blood oozes out, and, in the192 last stage, the hemorrhage
is often copious from large vessels exposed by the ravages of the
disease.
Now, extensive mortification occurs, the strength fails, the pulse
becomes tremulous and indistinct, the features collapse, the surface
is bedewed with a cold sweat, diarrhœa and hiccough come on, and death
puts an end to the patient’s suffering. Such is the progress of the
disease in those who were previously in perfect health. Often, however,
it is attended with typhoid symptoms almost from the beginning, in
people whose constitutions are wasted, who have long laboured under
disease, or who have been long confined in hospital. The important
distinction between these cases must influence the treatment; what
succeeds in the one will destroy in the other. It is not the name of
the disease which is to be combated, but each symptom as soon as it
presents itself.
Those who have been once afflicted with hospital gangrene are extremely
liable to its recurrence, and that too on the same sore; though the
secondary disease is much less acute. This form has been termed
Sloughing Phagædena, and may seize a sore not previously affected with
gangrene. The wound, recovering from the first attack, and appearing to
heal rapidly, with good discharge and healthy surface, presents, near
its edge, a small dark spot or ulceration, of the size of a small bead
or shot, of a circular form, with a ragged edge, excavated surface, and
fetid discharge. Several such points may appear; they spread rapidly,
unite, and the surface is soon destroyed. It is not uncommon to find
one part of the sore of a healthy appearance, and even cicatrising,
whilst in another part the surface is rapidly disappearing. The
patient complains of a burning sensation in the part; suppuration
occurs round the edges and beneath the slough, and the dead parts
separate; but the same process again takes place, and another slough
forms. The malady proceeds often with a rapid and alarming pace; the
sloughs are soft, pulpy, and reddish, and separate one after another,
exposing muscles, nerves, bloodvessels, and bones. Joints are opened
into, and the vessels, having been exposed, perhaps for a day or
two, give way, and fatal hemorrhage ensues, their cavities not being
obstructed with coagula as in sphacelus. The patient is sick, has no
appetite, and labours under other symptoms of deranged stomach; there
is restlessness, with a small quick pulse, and all the symptoms of a
weakened and sinking system. The ulceration becomes more rapid, the
discharge is bloody and peculiarly offensive; all the symptoms increase
in violence, and may proceed for fifteen or twenty days, or terminate
in four or five, either in convalescence or death.
Hospital gangrene is supposed to arise from a variety of causes:
from the state of the atmosphere, moist and hot—from inattention
to cleanliness, the parts around the sore being seldom wiped, the
matter collecting amongst the dressings, and becoming acrid by
putrescence—from irritating applications, as rancid ointments—from
a too stimulating diet, and from the abuse of wine and spirits—from
mechanical irritation, in moving the wounded over rough roads and in
bad conveyances, as after great engagements—from specific contagion
without immediate contact. After being once generated, it is193
propagated by direct communication, by the application of morbific
matter from sponges, dressings, or instruments. It is not easy to say
how the disease originates.
In the treatment of this scourge, great attention must be paid to
cleanliness in all circumstances. Free ventilation must be constantly
preserved in the apartments of the sick, and fumigations assiduously
employed. The infected ought to be separated from the others, and but
few patients placed in the same ward. Stagnant drains and accumulations
of filth out of doors are to be removed; otherwise, during hot weather,
the atmosphere becomes much vitiated. Care must be taken, also, to
destroy all the dressings which have been used; not to employ sponges,
but to wipe the surface in the neighbourhood of the sore occasionally
with tow, which is to be burnt immediately, being an article of little
value, and easily procured. Too much attention cannot be paid to
the cleaning of those instruments with which gangrenous sores have
been treated, before they be applied to healthy wounds. As to the
constitutional treatment, the alimentary canal must first be purged
of its solid contents, and the secretions afterwards kept in as good
a condition as possible. When the wound or sore is surrounded with
intense inflammation, and when the skin is dry and the pulse strong
and full, with all the other symptoms of an inflammatory diathesis,
immediate recourse must be had to free abstraction of blood from the
system, as thus only can the progress of the disease be efficiently
arrested; and if inflammatory symptoms exist, when there is reason to
expect the occurrence of the disease, though no symptom of it has yet
appeared, then, too, venesection combined with purgatives is demanded,
as being the most powerful preventives. Emetics are also recommended.
When the affection is from its commencement accompanied with typhoid
symptoms, depleting measures must do irreparable mischief: in such
cases, the local pain and irritation will be relieved by the exhibition
of opium or camphor, and it may also be of service to preserve a
perspirable state of the surface by means of Dover’s powder, or other
diaphoretics. Preparations of Peruvian bark, the decoction with or
without the tincture and acid, or the sulphate of quina, are often
given with great advantage—opium is also usefully exhibited. Vinegar,
weak acids, the nitric and muriatic acids diluted, have been used as
external applications, and nitrate of silver, the red oxide of mercury,
and the actual cautery, have been applied with the view of removing the
diseased parts, and procuring a healthy surface. Arsenic in solution,
used so as to produce a slough, followed by hot dressings, has been
supposed to be serviceable. A much safer and more powerful application
is the strong nitric acid, which sometimes requires to be applied over
the diseased surface very freely, and repeated if need be.
THE MALIGNANT PUSTULE
Is a gangrenous inflammation of the skin, rarely extending to the
subcutaneous cellular tissue, and in this respect differs from
carbuncle,194 which commences and is seated in the cellular texture. It
arises from the application of the fluids of animals which have died
of putrid diseases common in some marshy and low situations. It is
communicated not only by matter from the diseased part, but also by
the blood of the animal; thus it is frequently observed in those who
handle the recent skin or flesh; and the excrements also appear to be
possessed of the poisonous principle. It spreads from one person to
another by contact. There is much reason to doubt, whether carrion
introduced into the stomach produces this disease, though by some it
is maintained that even the respiration of effluvia from putrescent
substances produces malignant fever, with fetid evacuations and
gangrenous patches on the skin. In the West of Scotland, an instance
occurred some years ago, in which several persons lost their lives
from eating the flesh of dead animals which had been washed ashore.
The occurrence of malignant pustule is rare in this country. Some time
since, I met with a well-marked case in a shoemaker, who had been
employed in killing some sickly pigs. Whilst turning over and removing
the abdominal viscera of one of them, he had scratched his finger
slightly with a pin stuck in his jacket, and he then perceived that
the contact of some putrid matter from the intestines caused great
pain. On the third or fourth day afterwards, he presented himself with
a malignant pustule formed on the hand between the fore and middle
fingers. The pain was very intense, and the disease seemed to be fast
extending. Active treatment was employed, and the patient had a speedy
recovery.
The disease generally attacks the hands, neck, face, or shoulders of
butchers and others, who carry, or in some way deal in carrion. It has
also taken place in consequence of the hand being introduced into the
rectum—a veterinary method of removing scybala—of an animal labouring
under putrescent disease. A pustule appears on the part affected,
containing a serous or a dark-coloured fluid; and the base ulcerates,
extending through the skin to the subjacent parts; at first it is
accompanied with a pricking sensation, afterwards the pustule enlarges
and becomes brown, and the pain is burning and itching. The vesicle
when opened, or when it has burst spontaneously, furnishes a few drops
of red serum, and the pain is thereby relieved for a few hours. A hard,
moveable, and circumscribed tubercle forms, without alteration of the
surrounding skin. The bottom of the sore is yellow, greenish, or livid,
and the sensation is that of acute heat and erosion. Phlyctenæ spread
around. The tubercle becomes black in the centre, and an eschar forms;
the patient becomes irritable and languid. The gangrenous point begins
to extend, and that alarmingly; great swelling takes place, elastic,
red, and shining, more emphysematous than inflammatory or œdematous.
The burning pain is aggravated; the patient has a feeling of weight
and stupor; great constitutional disturbance follows, there is slow
fever, with a small pulse, a dry and brown tongue, and unquenchable
thirst; a low muttering delirium ensues, and under these symptoms the
patient soon sinks. After death, the fetid body swells rapidly. The
disease sometimes terminates fatally in twenty-four hours or less;
but generally the patient’s sufferings are more195 protracted. In the
treatment, superficial scarifications are of little avail. The only
topical application which can be relied on is a powerful escharotic,
applied freely to the part, and at an early stage, before swelling
and constitutional affection have been added. By it the parts replete
with virus, being immediately deprived of vitality, are soon thrown
off. Thus the virulence of the poison is annihilated, it is rendered
inert, and is concentrated in the slough, and the surrounding parts are
stimulated, and receive vigour of action, which enables them to resist
any further inroad, and to detach quickly the mortified substance.
For this purpose, the most effectual and convenient escharotic is the
caustic potass, but the liquid muriate of ammonia may also be employed.
The vesicle is opened, and the caustic applied to the exposed surface;
and if necessary, the eschar may be afterwards divided, and the remedy
reapplied. In the absence of other escharotics, the actual cautery will
prove a valuable substitute. After the separation of the slough, the
sore is to be dressed with slightly stimulating applications. Bark,
camphor, and mineral acids, are given internally, and the patient is
enjoined a light diet, with a moderate allowance of wine.
OF ULCERS OF THE GENITAL ORGANS, AND THEIR CONSEQUENCES.
It were unprofitable to enter here upon the History of Venereal
Affections, as it is a subject of no practical utility, still involved
in uncertainty, and mystified by disputation. It will suffice to
describe the different forms of the disease, and state the treatment
applicable to each.
During the last century, and in the beginning of this, much greater
ravages were produced by the disease than at the present time; and
though this may be, perhaps, partly owing to a change in the poison
itself, it is mainly attributable to the mildness of the measures by
which it has been, and is, opposed. Every form of the affection, as
soon as it appeared, was at one time opposed by a counter poison,
mercury; and the practitioner, relying implicitly on this mineral as
a specific, and not being fully aware of its dangerous properties,
continued to gorge the system with the supposed remedy, subverting the
constitution of his patient, making, in many cases, no impression on
the disease, but still persevering in the use of a poison equal, if
not more potent, than the one which it was intended to destroy. The
change of treatment has been propitious to our science and to mankind.
But let it not be inferred that mercury now is, or ought to be,
entirely dismissed from the treatment of this disease, or from practice
generally: often no other means are effectual; but it should always be
prescribed most cautiously and sparingly.
The effects of the venereal virus are divided into primary or local,
and secondary or constitutional; and these present a great variety
in their appearances, characters, and tendencies. They are sometimes
modified by the constitution, or by the remedies ordered in the
first stage; but there can be no doubt that different poisons exist,
pro196ducing distinct kinds of ulcers, which again are succeeded by
different constitutional affections.
The most common kind of sore is the simple ulcer, at first excavated,
in consequence of the process of ulceration continuing; afterwards
the ulceration stops, and granulations, somewhat fungous, supply its
place, so that the surface is raised above the level of the surrounding
parts, and has a smooth, soft appearance; there is no hardness of the
edges, and there is no tendency to slough or extend by ulceration.
Sometimes it commences in the form of a pustule, which soon gives way,
discharging its contents, and leaving an exposed surface, in which
the process of ulceration quickly proceeds; but often it arises from
simple abrasion of the surface. Different forms of sores may exist on
the glans and prepuce at the same time; and it is maintained, that
one sore may produce another of a different kind, and the same is
asserted with regard to eruptions. The simple ulcer, as well as other
sores, is produced by the contact of secretions, generally morbid,
but often apparently healthy, with a susceptible surface. Sores, with
eruption and sore throat, sometimes appear in one or both individuals
immediately after marriage, and probably arise from the acrimony of
the female secretions causing tenderness and ulceration of the parts.
The application of gonorrhœal matter readily produces the simple
ulcer on the glans or prepuce, particularly if an abrasion or rawness
existed; and if the matter be allowed to remain on an unbroken surface,
a pustule will form, and ulceration follow. From this latter cause
numerous sores are produced, separated from each other by sound parts,
and not extending into one continuous ulcer; and this condition may
have been preceded, on the glans, by a rawness of the surface and a
profuse discharge, or by a herpetic eruption on the mucous lining of
the prepuce. One man may be affected with gonorrhœa, and another with
ulcer, from connection with the same female, the same day or hour; and
it is doubtful whether the effect is not similar, in both cases, viz.,
ulceration; for it is supposed, that in gonorrhœa, the discharge, in
some rare cases, proceeds from patchy ulceration of the mucous lining
of the urethra, similar to the ulceration usually met with on the
glans. In examining women who have communicated infection, very often
no sores are found, and but little unhealthy discharge. In short, the
simple elevated sore may arise from the application of secretions from
an unbroken surface, from inoculation of matter from a similar sore,
or spontaneously, from inattention to cleanliness. Sores with elevated
surface, more extensive than those of the glans and prepuce, occur
on the skin of the penis and scrotum, or in the folds of the thigh;
and in women they are often met with in the perineum, or the cleft of
the nates. Sores of different kinds arises at various periods after
the application of their cause, from a day or two to some weeks, or
longer, but the usual time may be said to be from four to eight days.
The duration of the simple elevated sore may be modified by various
circumstances—by the constitution of the patient, his mode of living,
and the attention paid to the affected part. It seldom remains open
above a few weeks, but occasionally it may be seen unhealed at the end
of several months in those who lead careless and irregular lives.197
Such ulcers produce, as readily as any other sores, enlargement of the
inguinal glands; they are a source of irritation, the effects of which
may be extended along the lymphatic vessels, to the cluster of glands
through which the absorbents pass, so as to cause inflammatory action,
ending in indurated enlargement; or venereal virus from the sore may
be taken up by the lymphatics, deposited in the glandular structure,
and produce a similar affection. Buboes thus caused are situated in the
upper cluster of inguinal glands; if the lower cluster is affected, it
is to be presumed that the cause is not in the organs of generation,
but in some part of the inferior extremity. From the existence of bubo,
nothing can be deduced as to the nature of the poison, or the probable
effects to be produced on the constitution; for enlargement of glands
in the course of their lymphatics will occur from irritation, whether
connected with a mild or malignant virus, or with one totally devoid of
any poisonous quality.
From the simple ulcer there arises a constitutional affection, in all
respects resembling that which follows gonorrhœa (a disease which will
be treated of under affections of particular mucous surfaces); but
before attending to this, it will be proper to advert to another form
of ulcer, which differs but slightly from the preceding in primary and
secondary symptoms. It is a sore with a brown surface, either on a
level with, or above the surrounding parts, with defined and elevated
edges, with no cartilaginous hardness of base or margins, and with
no tendency to spread either by sloughing or by ulceration. Such may
occur in the same situation as the simple sores, but they often form
on the outer surface of the prepuce, or on the scrotum; and are not
unfrequently met with round the orifice of the prepuce, which is a most
troublesome situation, as, in healing, they generally produce phymosis.
Sores and fissures in this situation are very often kept up by the
tense and irritable state of the aperture. The bubo which follows
this differs from that caused by the simple sore, in having, after
ulceration of the integument, a greater disposition to burrow; and this
tendency is more marked where mercury has been employed. From either
of these forms of ulcer, it sometimes happens that constitutional
affections arise, either during the existence of the sore, or some
weeks after it has cicatrised.
The usual secondary symptoms are those attendant on a papular eruption.
There is fever, with pains referred to the head, to the joints, chiefly
the larger ones, and to the chest, which latter symptom is sometimes
attended with dyspnœa. This indisposition is followed by the appearance
of a papular eruption, termed lichen, on the face and trunk, the
extremities being less thickly studded. The fever subsides in a great
measure after the eruption appears and comes fully out; but fresh crops
of papulæ may appear, and, in this case, the fever continues little
abated until the eruption begins to fade. The eruption consists, in the
first instance, of simple elevations or pimples of a red colour, and
these do not appear at once, but gradually: so that some have assumed
the form of cones, with minute collections of matter in their apices,
whilst others are mere elevations of the cuticle. When they fade the
spots are of a copper tint, and become covered with thin scales, in
consequence of the cuticle de198squamating; but this latter appearance
can never be confounded with the scaly eruptions following another
description of primary sore. In all cutaneous eruptions, attended with
any febrile action, there is a tendency to sore throat, with tenderness
of the eyes; and this eruption is not exempt from a similar affection:
the fauces feel raw and tender, and are pained in deglutition; on
looking into the throat, the mucous surface is found red and swollen,
and the tonsils are generally enlarged; but there is seldom any breach
of surface; and, when this does occur, it is rather entitled to the
appellation of excoriation than of ulceration. Occasionally the
surface is covered with a thin coating of lymph, and sometimes this is
confined to the situation of the mucous crypts, so as to give a false
appearance of small sores. As in similar affections, unconnected with
any discoverable cause, the lymphatic glands, at the angle of the jaw,
are not unfrequently swollen and painful.
Such is the usually mild character of this affection; but if its
progress has been interrupted by any means, more particularly by
mercury, it assumes a more complicated form, and a less tractable
nature. If that mineral is administered in the usual style, and at the
commencement, when the fever and other symptoms are high, the patient’s
sufferings are all much aggravated. After the fever has subsided, the
eruption will often be found to disappear under the use of mercury;
but it is extremely apt to recur, as soon as the system has shaken
itself free from the effects of that medicine. The mercury produces an
irritation, which supersedes the eruption, but by frequent repetition
its effects on the system diminish: it at last fails to create an
irritation more powerful than the disease to which it is opposed,
and, consequently, the eruption does not yield, but during its use
is frequently reinforced by fresh crops of papulæ. If the eruptive
fever, and advanced stage of the disease, are imprudently and suddenly
arrested by the use of mercury, by exposure to cold, or by other means,
inflammation of the iris or joints often follows, of a very violent
form, and not to be easily moderated. No one thinks of repelling
measles or other eruptive diseases, and with good reason, for such
practice would almost certainly induce serious affections of internal
organs. For the same reason, every precaution must be used to allow
this form of eruption to take its own course, while we merely regulate
the constitutional symptoms as they obtrude.
Another form of eruption, which occasionally, though much less
frequently, results from either of the above mentioned sores, is
the pustular. It is preceded by fever, and consists of rather large
pustules, separated from one another, and not very numerous. After
their apices give way, and the contained pus is discharged, a thin
scab is formed, and on its separation a small ulcer is left, which in
general soon heals from its margins, leaving a dark-coloured spot to
mark its situation. The papular and pustular eruptions are sometimes
blended; a few pustules appearing amongst numerous papulæ, or vice
versâ. The pustular disease is not of frequent occurrence; and in
proportion as it approaches the papular, with desquamation, it becomes
milder and more easily removed. In it, as in the papular, mercury
proves injurious.
199
The phagedenic form of ulcer is the most dreadful and unmanageable
of all; most uncertain in progress, and direful in event, and often
rendered still more destructive by the mode of treatment adopted.
Fortunately, it is now seldom seen, though not long ago it was well
known, as a perpetrator of dreadful havoc, under the name of black pox.
It is a corroding ulcer, without hardness of the surrounding parts,
presenting no appearance of regeneration of the tissues which have
been destroyed. It may follow either upon a pustule or an abrasion.
Sometimes it destroys the prepuce and glans in a few days, or again,
when chronic, it spreads deceitfully, healing at one part and
destroying at another. The ulceration is often deep, penetrating the
corpora cavernosa, or the corpus spongiosum urethræ: in such cases
it is followed with violent hemorrhage, which often produces a great
and sudden improvement in the sore. After slow cicatrisation it not
unfrequently happens that the scar gives way, and the ulceration
returns.
Sometimes another character is given to the sore, by the rapid
sloughing of the parts. In this modification, a small black spot is
first observable, unattended with pain: it enlarges rapidly, and, after
no long time, the mortified part separates, exposing an unhealthy
surface, which is immediately attacked and progressively destroyed
by phagedena. The part may again slough, and, by an alternation of
mortification and phagedenic ulceration, the external organs of
generation, male or female, may be wholly destroyed. In the present
day, however, its ravages are much less extensive and more easily
combated than formerly, and it seldom, if ever, proves fatal. One very
troublesome case is in my recollection, where the patient suffered
two attacks at the interval of two years. During the progress of
the disease he was seized with delirium tremens; a bubo formed and
ulcerated; a violent hemorrhage occurred from the sore; sloughing and
phagedena alternated; and both prepuce and glans were entirely lost.
An eruption followed, accompanied with ulceration of the throat and
nostrils. He recovered much mutilated. Ulcers originally of a simple
character may become affected with phagedena, or sloughing, from the
state of the constitution, from mismanagement, or from exposure to an
unhealthful atmosphere. But in such cases, after the separation of the
slough, the exposed surface is found to be of a healthy granulating
character, contrary to what is observed in the originally phagedenic
disease. Buboes, when they occur, have the same malignant action as the
primary sore: the breach of surface is extended either by sloughing
or by phagedenic ulceration, and the edges of the sore are ragged and
undermined.
The secondary eruption which follows the phagedenic form is pustular,
though differing from that which has been already noticed. The pustules
soon give way, and ulcers remain, covered with thick scales or crusts,
which sometimes increase, layer by layer, so as to become prominent,
dense, and of a conical form,—the rupia prominens. After the separation
of the crusts the ulcers are found, superficial, rather unhealthy, and
showing a disposition to extend, chiefly200 towards the circumference.
When healing, the process of cicatrisation frequently proceeds from
the centre of the sore, which is still enlarging at its circumference.
The reason for this unusual mode seems to be that ulceration does not
commence in the secondary sores till the crusts which cover them have
been removed: they then are very superficial, not extending through
the thickness of the true skin; and the ulceration does not go on in
the centre of the original sore, but towards its margins, so that a
portion of true skin remains in the centre of the sore, whilst it is
gradually destroyed towards the margins. Then, whilst the surrounding
skin, which usually forms the new cutaneous texture necessary for
reparation, is gradually and progressively destroyed, the remaining
old skin in the sore assumes an excited action, as in ordinary cases,
and from it the requisite new texture is formed, and gradually extends
over the surface, until it meet with a similar substance, which has
been produced by the surrounding skin after the ulceration in that
quarter has ceased. Thus the general principle that skin is formed
by skin is, even in such instances, found to be correct; the healing
from the centre not following, as some have supposed, the complete
destruction of the cutaneous tissues, but from its having remained
unaffected, or nearly so. The appearance of the eruption is preceded by
general indisposition, and occasionally by smart fever. It is sometimes
extensive, but is in general confined to the upper parts of the body.
Ulcers of the throat occur, of a very alarming kind, quickly destroying
the parts attacked, spreading chiefly towards the posterior part of the
fauces, rapidly extending to the pharynx and to the nostrils, and in
some instances also involving the larynx. The pendulous velum of the
palate and the tonsils are often wholly destroyed, the bones of the
nose, more especially the turbinated, are deprived of their coverings,
and exfoliate, the osseous and cartilaginous portions of the septum
are discharged, and the nose becomes sunk, or is supported merely by
the columna. The patient’s breath is fetid, respiration is in some
degree obstructed, a foul ichorous discharge flows from the nares,
and the surrounding parts are inflamed, swollen, and excoriated. The
countenance is greatly disfigured. On looking into the throat, nothing
is seen but an extensive ulcerated surface covered with white adherent
matter, and exhaling an offensive fetor, particularly when the bones
are affected. Respiration is nasal, and the speech indistinct. When
the larynx becomes affected, the patient may be almost considered as
lost: phthisis laryngea is established, the symptoms and treatment of
which will be afterwards mentioned. The mutilating affection of the
nose does not seem to be produced by any other form of the venereal
disease, if not in any way aggravated. Along with the eruption and
its after effects, severe pains in the articulations, particularly in
the knee-joint, often occur, and are always much increased during the
night. Nodes seem to be produced only in those cases in which mercury
is exhibited; their most usual situation is on the fore part of the
tibia; severe pain is felt in the part, which becomes slightly swollen,
and of a bright red colour; the swelling feels dense and firm, being
a simple enlargement of the bone. They often occur when the patient
is201 taking mercury, and when, in fact, the constitution is completely
saturated with it. This medicine may interrupt the progress of the
disease, may remove the eruption and the ulcers of the throat, but it
at the same time transfers the disease to deep unyielding parts, to the
bones and their coverings, and the fasciæ.
The last distinct form of the venereal disease is the scaly—syphilis,
or true pox. The primary sore, termed a chancre, “is somewhat of a
circular form, excavated, without granulations, with matter adhering
to the surface, and with a thickened edge and base. The hardness or
thickening is very circumscribed, not diffusing itself gradually and
imperceptibly into the surrounding parts, but terminating rather
abruptly.” Such is the appearance generally presented by the sore
when situated on the glans and prepuce. It generally commences in the
form of a pimple, without much surrounding inflammation. Sometimes
the ulcerated surface is very inconsiderable, but there is always the
abrupt and remarkably dense thickness which serves as a distinguishing
mark. The non-syphilitic ulcers may have surrounding hardness from
the first, or in consequence of the application of stimulants and
escharotics; but this is diffused into the neighbourhood, and is not,
it is said, of that remarkable solidity peculiar to chancre. It is
seldom that more than one chancre occurs: the usual situation is on
the glans and lining of the prepuce; but they occasionally form on
the outer surface of the prepuce, and on the dorsum penis. In the
latter situation the sore assumes a somewhat different appearance: it
is, in general, larger, the hardness of the base is not so great, the
excavation is less, and the surface is of a livid hue. When allowed to
proceed uninterrupted, the livid surface is alternated with that of a
light brown or tawny colour. Chancre is an indolent ulcer when compared
with the phagedenic or sloughing sore, the ulceration proceeds very
slowly, and, in proportion as it advances, the surrounding hardness
increases. It is also contumacious and obstinate in taking on any
reparative action. Phymosis occasionally takes place, in consequence of
chancre situated at the orifice of the prepuce, but not so frequently
as when that situation is occupied by superficial sores of a more
active nature. Bubo sometimes appears in both groins, or in one;
sometimes on the same side with the sore, often on the opposite, and
not unfrequently when the sore is healing, or after it has healed. It
may suppurate and give way, or may subside without having advanced to
suppuration. It differs in no respect from the swelling of the glands
from other causes, either in its swelled or open state. Neither does
the occurrence of a bubo render it more probable that constitutional
symptoms will follow. Enlargement of the glands is often caused, or
at least hastened, by the patient continuing to walk about and exert
himself during the existence of a sore, and whilst the absorbents
are in an irritable state; but a bubo may be caused by irritation
or excoriation in any way produced; and it not unfrequently occurs
without any apparent cause. In some cases of chancre or other ulcer,
the absorbents along the dorsum penis become swollen, and occasionally
suppurate. In former times, it was not uncommon for the surgeon to
insist that all swellings in the groin were venereal, though no primary
sore had ever202 existed: the virus was said to be absorbed from an
unbroken surface; the patient’s system was saturated with mercury; and
the use of that medicine was persevered in, with the view of opposing
those symptoms of a ruined system which itself had produced. Such
delusions have now happily passed away.
The eruption which follows the chancrous form of primary sore is scaly
from the commencement, and by this character is readily distinguished
from every other venereal affection. It is generally preceded by
an efflorescence or discoloration, rendering the skin of a mottled
appearance. The scaly eruption is a form either of lepra or of
psoriasis. The patches usually do not exceed a sixpence in size, are
distinct and separate from each other; their base is of a dark red
or coppery hue, the affected skin is not hard or rough, but soft and
pliable, and seldom covered with crusts; as they extend, the edges
are slightly elevated at the centre, which alone is covered with thin
white scales, appears flattened and somewhat depressed; when they
begin to fade, the margins shrink and become paler, and desquamation
proceeds slowly; a circular, purplish-red discoloration, with a central
depression, remains for some time after the blotches have declined: the
depression is permanent, but the discoloration disappears. The smaller
patches, which assume a variety of forms, continue for some time of a
dark colour, extend towards the circumference, become pustular, and
at length ulcerate superficially, enclosing an area of sound skin.
When depressions of the skin, as the folds of the nates, are affected,
a scaly eruption does not take place, but soft and moist elevations
arise, discharging a whitish matter, varying in form and size, and
accordingly receiving various appellations, as condylomata, fici,
or marisci. From them a secondary form of disease is occasionally
communicated. If no decided treatment is resorted to, and if the
eruption is consequently permitted to follow its own course, thick
crusts form, ulceration proceeds beneath them, the matter is confined,
and the patch becomes prominent. Another secondary symptom of chancre
is ulceration of the throat, sometimes extensive, but generally
situated in the tonsils, or their immediate neighbourhood. The ulcer is
not preceded by much pain or swelling: “it is a fair loss of substance,
(part being dug out, as it were, from the body of the tonsil,) with
a determined edge, and is commonly foul, with thick matter adhering
to it, like a slough, which cannot be washed away.” Such ulceration
may be simulated by excavated sores attending the phagedenic form of
disease; and it ought to be more especially distinguished from an
affection to which the tonsil is extremely liable, irregularity of its
surface, enlargement, and effusion of lymph, in consequence of chronic
inflammation.
A more serious part of the secondary disease is affection of the
deep-seated parts, ligaments, periosteum, and bones. The bones nearest
the surface are principally affected: a swelling gradually forms on the
tibia or ulna, without discoloration of the integuments, and without
pain occurring till after a long time. The pain is most severe during
the night. The inflammation of the periosteum is often very violent,
the subjacent bone, as in the head or extremities, becomes dead, and
exfoliates; but it remains to be seen whether this203 will take place
when mercury is more sparingly, if at all, administered. Ulcers betwixt
the toes, occurring along with the above symptoms, are supposed to be
venereal: they are unseemly, and peculiarly fetid.24
Such are the affections, local and constitutional, arising from a
venereal cause; but the latter may be simulated. Many affections of the
skin, mucous membranes, and bones, resembling the venereal disease,
may be produced by disorder of the constitution, by a decay of the
digestive organs, by unwholesome food, and exposure to inclement
weather, by inattention to cleanliness, and many other circumstances.
Morbid poisons, not venereal, but of various kinds, may exist, and
cause much mischief.
A disease resembling syphilis was produced by the cruel practice of
transplanting teeth from sound people into the jaws of persons in the
higher ranks of life, whose corresponding teeth were decayed. The
latter were the affected party, and that justly.
A very infectious disease was at one time common in the poorer parts
of Scotland, and known under the name of sibbens, or sivvens, chiefly
occurring amongst the poor, ill-fed, badly-clothed, and worse-housed
people in the Highlands. It was communicable by very slight contact
by kissing the lips of an infected person, smoking the same pipe,
drinking out of the same cup, or using the same spoon. Cases of it
are still occasionally seen. There are ulcers of the lips, mouth,
throat, and nose; ulcerated patches and warty excrescences in the
cleft of the thighs, in the axilla, and round the anus and pudenda.
A pustular eruption appears, and terminates in hardened crusts. The
same disease is known in Ireland, under the name of button-scurvy;
and a similar one, called raddesyge, has been described as occurring
on the sea-coasts of Norway and Sweden. In Canada, also, something
of a like nature was at one time prevalent. The yaws, at one time
common and destructive in the West India Islands, appear to be much of
the same nature. Some of these diseases, more particularly sivvens,
are very common amongst children. Even in these days children are
not unfrequently born with copper-coloured blotches of the skin and
desquamation of the cuticle; or they may come into the world with these
appearances, along with affections of the mucous membrane, hoarse
voice, redness round the anus, &c. These are forthwith attributed to
a syphilitic taint existing in either of the parents; and one or both
are put under mercury; but child after child comes into the world in
the same plight. Again, the disease is communicated by children to the
nurses, and vice versâ. All these 204affections are rendered much more
obstinate by full courses of mercury: the bones and ligaments become
affected in consequence; but small doses of that medicine may prove
useful towards the decline of the disease.
Some have believed mercury a certain test of syphilis; maintaining that
the disease, still checked by the specific, is never overcome by the
constitution; that it is unchangeable, and regularly and progressively
grows worse, where no mercury is employed; that, opposed by that
medicine, it is stationary, and is permanently cured by adequate
mercurial influence on the constitution. Whatever were the appearances,
if they went off under mercury, the advocates for this practice set
them down as those of syphilis, lues, or pox. If they did not yield
to that mineral, they were termed syphiloid, pseudo-syphilitic, or
mercurial; for they did admit, now and then, that their favourite
remedy produced unpleasant effects. Such theory and practice are now
very happily exploded.
As to the treatment of local venereal affections, it may be, in
the first place, remarked, that prevention is better than cure. The
means employed for accomplishing this end are very various: oily
applications, alkaline and spirituous washes, &c., with the view
either of preventing the matter from coming into contact with the
genitals, or of completely removing it, when it has been but a short
time applied. There is one certain method of avoiding disease, which
it is unnecessary to mention. In all affections of the penis, it
is of the utmost importance to keep its extremity bound up to the
abdomen, in order to prevent congestion or inflammatory swelling.
Celsus knew this well; “Sursumque coles ad ventrem deligandus est,
quod in omni curatione ejus necessarium est;” rest and quiet must
be strictly observed; the patient must be confined to the recumbent
position, particularly when the sore is irritable, when swelling or
bubo has occurred or is threatened; and when the system is excited,
and the eruption has commenced, the bowels must be kept gently open,
the patient’s diet must be low, and the parts surrounding the sore are
to be kept carefully clean. Whatever the nature of the ulcer may be,
it is safe and prudent, in the first instance, to change its action
by the use of the nitrate of silver, or to destroy the surface by the
free application of escharotics, as nitric acid, or solution of nitrate
of mercury: the morbid poison is thus got rid of, and the surrounding
parts stimulated to a proper degree of action. This is absolutely
necessary in the phagedenic form of ulcer, whether of an acute or
chronic nature. But, in most cases, the patient does not apply for
medical assistance till the sore has been of so long duration as to
preclude all hope of counteracting the virus by any local application.
The simple superficial sores, and those with elevated margins, must be
treated on the same principles as if they were totally unconnected with
any specific cause; and the applications must be varied according to
the peculiarities of the part affected, and the different appearances
which the surface assumes during the progress of cure. Lotion is the
form of application found preferable in most cases, and may consist
of calomel and lime-water, with mucilage, called the black wash; of
muriate of mercury, with lime-water, called the yellow wash; of a
solution of sulphate205 of zinc, with spirit of a solution of nitrate of
silver, or of sulphate of copper. The linimentum æruginis or Barbadoes
naphtha, are often useful in foul sores. Ointments, if at all, ought to
be used sparingly. The application of dry lint, or the sprinkling of
a little fine powder, is often all that is requisite. Of course these
applications must be varied, according to the particular circumstances
of each case.
Buboes are to be treated in the same way as any other inflammatory
swellings; local means being taken at the commencement to subdue the
inflammatory action, and resolve the swelling. Rest is indispensable.
When they are stationary, the application of a blister will either
cause resolution or suppuration, and so the enlargement will be got rid
of, either in the one way or the other. The painting of a rubefacient
solution of iodine occasionally on the swelling is also useful, and
preferable to frictions with iodine ointment. When they have passed
into a decidedly chronic state, absorption may be promoted by pressure,
or, again, means must be taken to hasten suppuration, and the matter
which forms is to be early evacuated. If suppuration occur in the
cellular tissue, and not in the substance of the enlarged gland,
neither cicatrisation, nor a permanent cure, can be expected until
the prominent and indurated parts have been destroyed by the caustic
potass. In phagedena, bread and water poultices or tepid-water dressing
are, in the first place, to be applied, and the pain and irritation
may be soothed by solutions of opium, or extract of poppy. If bands of
skin intersect the ulcerated parts, they are to be divided, as being
a source of irritation which prevents healing. If the frænum præputii
be surrounded by ulceration and undermined, it must be incised for a
similar reason. It is often advisable, also, to divide the prepuce.
After the process of destruction has ceased, gently stimulating washes
will promote contraction of the sore.
It is an important fact, that the majority of primary ulcers can be
made to heal without mercury. Cavillers object to the mercurial washes,
supposing that they may act by affecting the constitution. The sores
with hardened edges, chancres, heal as well as others, when mercury
is not employed, but much more slowly. In some mercury is injurious:
in chancres it promotes the cure. In any case, I would never think of
ordering it, unless the progress were very tedious, the ulcer being
indolent and contumacious; then mercury may be advantageously used,
and moderately continued, until the callosity disappear. It is no
easy matter to say, judging from the appearance of the ulcer, whether
secondary syphilitic symptoms are likely to arise in consequence of it
or not, or what their nature may be should they occur: they follow upon
sores of all characters, and, again, do not appear, after what might
be set down as the genuine Hunterian chancre. Whatever the nature and
appearance of the ulcer may have been in the first instance, should it
become stationary, and show no disposition to heal under local means,
mercury may then be given cautiously, and with advantage. Considering
that very obstinate sores are now seldom met with, it would seem that
very little mercury is required in the treatment of primary venereal
ulcers. During the progress of acute inflammatory action, this medicine
should206 not be given for the primary affection, whatever the nature of
the ulcer. Mercury cannot prevent constitutional affections.
Constitutional symptoms do not often occur, taking place scarcely in
one case out of a hundred of all the forms of sores which present
themselves. In the papular form mercury is hurtful, as already
remarked; it interferes with the natural and mild progress of the
affection, frequently gives rise to iritis, and produces pains of the
joints and bones. The powers of the constitution, aided by simple
remedies, are sufficient: the cure may be tedious, but cannot be
destructive. Whereas, if mercury be considered as the only specific,
its use will be long continued; it will frequently be resumed after it
has been dispensed with on the supposition that the virus is destroyed;
and by the effects of excessive mercurial irritation, combined with
those of the disease, tampered with and aggravated, the patient may
ultimately perish. The fever, which precedes and attends the eruption,
must be moderated by depletion, antimonial medicines, and purgatives;
but depletion ought not to be carried far, lest the eruption be thus
checked and disappear; and the patient ought to be carefully removed
from external circumstances which might produce a similar effect. After
the eruption has come fully out, and the febrile symptoms subsided,
it will be sufficient to attend to the general health, and employ the
decoction of sarsaparilla, a medicine which excites the secretions, and
more especially promotes diaphoresis. In short, the treatment may be
said to consist in allowing the disease, in a great measure, to follow
its own course, taking measures to prevent it from being interrupted,
and merely moderating such violent symptoms as may precede or accompany
it.
In the pustular form of eruption the general treatment is the same
as in the papular. Mercury is hurtful, and increases the tendency to
burrow. When the surface is nearly covered with pustules and ulcers in
all stages, desquamation may be hastened by fumigations of sulphur, the
general sulphur baths, lotions of sulphuret of potass, nitro-muriatic
baths, vapour baths, or by smearing the affected surface with equal
parts of tar and sulphur ointment.
In phagedena the patient ought to be, if possible, placed in an airy
and healthful situation. In most cases free bloodletting may be
necessary at the commencement, and will be advantageously followed
by purgatives and antimonials. The patient ought to be strictly
confined to his room, and ordered low diet with diluents. Afterwards,
the internal use of nitric acid, the decoction of sarsaparilla, and
an occasional dose of Dover’s powder at night, will be beneficial,
particularly if sleep be disturbed with pain of the bones and joints.
Mercury, even in small quantities, protracts the disease, and in
large doses it hastens the ulceration and sloughing. When all febrile
symptoms have subsided, when the ulcers are nearly healed, when no
fresh pustules appear, and when desquamation is begun, alterative
doses of mercury, as a blue pill or grey powder every second night,
may sometimes be ventured upon, will tend to hasten the cure, and will
not, possibly, be followed by any unpleasant symptoms. The safe course
is to promote the secretions by some safe substitute—preparations of
sarsaparilla, ipecacuan, taraxacum, &c.
207
In fact, in all scaly eruptions, whether scaly from their commencement,
or having become so in their latter stages and previously to their
disappearance, mercury, prudently administered, will be useful by
expediting the cure, and not injurious by deranging the system. The
tar or citrine ointments may be applied to the eruptions and cutaneous
ulcers.
For the ulcers of the throat, unless in a sloughing state, the lunar
stone appears to be almost a specific, removing the irritability of
the sores, and protecting them from further irritation by coagulating
the discharge, which then more effectually covers and protects them.
The application requires to be repeated every second or third day, as,
by the frequent and necessary motions of the parts, the crust loosens
and separates, leaving the surface exposed and irritable. At the same
time the sore will contract very considerably under each successive
crust. The lunar stone may also be applied in solution; or a solution
of the bichloride of mercury in spirits or laudanum may be used, in
the proportion of from four to six grains to the ounce, or stronger.
The solution of the nitrate of mercury is sometimes employed with
advantage. Fumigation of the throat with the red sulphuret of mercury
has been extolled as a powerful means of checking the alternating
sloughing and ulceration which often accompany the ulcers of these
parts, but the propriety of its employment is doubtful; the system
is thereby rapidly put under the influence of the mineral, which, as
already remarked, generally aggravates the violent disturbance under
which the constitution labours. More permanent good may be expected
from means taken to remedy the constitutional evils than from such
violent remedies as are directed against the affected part, but which
also produce a baneful effect on the system. In ulcers of the nostrils,
with fetid discharge, snivelling, exfoliation of the inferior spongy
bones, affections of the palate, &c., the nitrate of silver is also
very efficacious; or the affected parts may be occasionally touched
with a hair pencil, dipped in a liniment composed of lime-water, olive
oil, and the golden ointment. They ought to be frequently washed
with tepid water, and all sources of irritation must be removed. If
the patient be in the habit of taking snuff, the practice must be
abandoned, and the powder already impacted in the nostrils removed.
If there be carious teeth or stumps in the upper jaw, the sores can
scarcely be expected to heal till these be extracted, as constant
irritation is kept up by them. When the affection proves obstinate, a
recourse to mercury is recommended by some writers; but this will make
bad worse. Sarsaparilla in these cases, with attention to diet and
air, will always prove a better alterative than any form of mercury.
It may be combined, according to circumstances, with the nitric or
nitro-muriatic acids, or with the hydriodate of potass, in which many
practical men have great faith. This medicine is employed in cachexia,
following or not the use of mercury, and is directed against eruptions,
sore throat, and pains in the limbs.
The constitutional symptoms of the scaly disease, or true pox, when
they occur, which is now but seldom, are decidedly benefited by a
prudent employment of mercury. It may be administered externally or
internally, though the latter method is the one generally208 adopted. It
may be introduced into the system under various forms, according to the
particular circumstances of the case, or the ideas of the practitioner.
The most common form, and the simplest, is the pil. hydrargyri; but
for this may be substituted hydrargyrum cum creta, Plummer’s pill, or
calomel with antimony. In painful affections of the bones, with or
without swelling, the muriate of mercury (bichloride) is the form which
I have found most efficacious; one-eighth of a grain of the muriate
being given thrice a day in a pill; or the medicine may be given in
solution. The iodide of mercury is also a very useful medicine in some
cases. It is impossible, and would be absurd, to lay down any precise
rules as to the quantity of mercury which is necessary for the cure
of pox: in some patients the system is with difficulty put under its
influence, whilst in others a single grain will produce salivation,
constitutional disturbance, and eczema. When the mouth becomes affected
the mercury ought to be discontinued: much harm and no good resulting
from the medicine being pushed to profuse salivation; the tongue swells
hideously, the teeth loosen, and portions of the jaw die and exfoliate.
It is sufficient that the system be under the influence of mercury;
and that circumstance is marked by the tenderness of the gums. If,
after the medicine has been disused, the disease does not appear to
recede, it may be resumed in the same moderate way as before; but there
certainly can be no use in continuing mercury after the symptoms of
venereal affection have ceased. Nodes may still exist, portions of bone
may be dying, abscesses forming, and various other changes of structure
going on, but these are no reasons for a continuance of the mercury.
If they have originated from the venereal affection, that cause has
been removed, and the diseased actions will now proceed altogether
independently of their original cause. Mercury proved beneficial in
removing a disease of which they are not a part but a consequence; and,
if that medicine be now blindly persevered in, the only effect will be
to ruin the constitution, and thereby greatly retard the cure of those
affections which, if the natural powers of the system had been merely
supported, or in a great measure left to themselves, would have soon
ceased to annoy the patient or alarm the antisyphilitic mercurialist.
Slight swellings and pains of the bones often yield to local
abstraction of blood, friction, and the internal use of the compound
decoction of sarsaparilla. Nodes, however, sometimes continue to
enlarge, and occasion much pain, notwithstanding these means; and in
such circumstances much relief will be afforded by a free incision over
the affected part, from whatever cause the swelling may proceed. When
the pain has subsided, and the swelling remains stationary, a decrease
of it may be sometimes effected by a blister.25
209
Of the bad effects of mercury on the constitution much might be said.
Treatises have been written on mercurial pox, a species reported to
be much the most violent; and others have detailed an accumulation
of evils, under the title of mercurial disease. There is no doubt
that extensive, deep, and sloughy ulcers of the throat are produced
by mercury; and of this I witnessed the following unexceptionable
instance:—The fauces presented one extensive mass of ulceration,
sloughing at its margins, and the uvula was almost detached. The
patient was an old and emaciated woman, who neither 210had, nor could
be supposed to have, any venereal complaints. She employed herself in
coating mirrors with quicksilver, and to that she ascribed her malady.
In fact, her system had been long under the influence of mercury, in
consequence of her occupation. When I visited her, her daughter and
husband, the latter of whom was paralytic, and almost bedridden, were
affected, from the same cause, with a pustular eruption of the face,
with disease of the nostrils, and snivelling. Another old woman had
numerous and deep ulcers of the fauces, tongue, and lips, having been
kept unmercifully under mercury for nine continuous months. She had,
besides, taken it from time to time, for upwards of four years, though
her sole complaint was slight sore throat. Pains of the joints, too, I
believe, are attributable to the use of mercury. That medicine has no
power to prevent the occurrence of nodes, for these often form during
its action. Affections of the periosteum are very frequent in horses
and other lower animals, and also easily excited in some human subjects
who have neither had pox nor been put under mercury; but in no instance
of venereal disease have I observed serious affections of the bones
where mercury had not been given. Even the advocates for mercurialising
speak of mercurial nodes. It has been asserted that nodes do not occur
when mercury has been given for liver or other complaints; but they do
form under such circumstances, though not so frequently as when the
medicine has been exhibited during venereal symptoms. A cachectic state
is often induced by a continued use of mercurial preparations, or at
least by mercury and disease together, in constitutions not originally
strong. It is marked by pale lips; bloodless conjunctiva; a rough
anserine skin; a relaxed state of the mucous membranes; hemorrhages
from these, particularly from the gums, which may prove fatal, as
I have myself witnessed; exfoliations of the alveolar processes;
slimy stools; pale urine; pains of the limbs; sores, showing great
indolence, or even assuming malignant action; dropsical symptoms, and
other evils, of which a lengthened catalogue might be made out. Such
symptoms were often met with when mercury was exhibited for every
trifling or suspected sign of disease arising from carnal conjunction.
On this subject, Mr. Samuel Cooper has well remarked: “Experience has
fully convinced me, that in no forms of chancre, nor in any other
stages of the venereal disease, is it proper to exhibit mercury in
the unmerciful quantity, and for the prodigious length of time, which
custom, ignorance, and prejudice, used to sanction in former days.
Violent salivations ought, at all events, to be for ever exploded. When
I was an apprentice at St. Bartholomew’s Hospital, most of the venereal
patients in that establishment were seen with their ulcerated tongues
hanging out of their mouths, their faces prodigiously swelled, and
their saliva flowing out in streams. The wards were not sufficiently
ventilated, and the stench was so great, that the places well deserved
the appellation of foul. Yet, notwithstanding mercury was thus
pushed (as the favourite expression was), it was then common to see
many patients suffer the most dreadful mutilations, in consequence
of sloughing ulcers of the penis; other patients, whose noses and
palates were gone; others who were covered with nodes and dreadful
phagedenic sores.” This woful picture is not211 exaggerated, and cannot
be too strongly impressed on the minds of young practitioners. A small
quantity of mercury will affect violently some constitutions; as of
those who have been in warm climates, or who have taken much of the
drug, even in this country.
Eczema Rubrum, a disease resulting from external causes, but which
may also be produced by mercury, often arises from but a very small
quantity of that medicine even applied externally. It most frequently
affects the scrotum and upper and inner parts of the thighs. It is
preceded by heat and itching in the part; a diffused redness appears,
and the affected surface is rendered rough by the eruption of numerous
minute vesicles. In a short time, these vesicles, if not ruptured,
attain the size of a pin’s head, and the included serum becomes opaque
and milky. The affection soon extends over the rest of the body in
successive large patches, and is accompanied with considerable swelling
of the integuments, tenderness of the skin, and itching. The vesicles
burst, and discharge a thin acrid fluid, which renders the surrounding
surface painful, inflamed, and excoriated. The discharge becomes
thicker, adhesive, and fetid, and by its drying, partial yellowish
incrustations are formed. The disease terminates in desquamation, and
in some cases, the hair and nails are also lost. It is preceded and
accompanied with smart fever, and general disorder of the system.
Erethismus is another occasional consequence of mercury,
characterised by remarkable depression of strength; small, quick, and
often unequal pulse; anxiety, sighing, and trembling; a pale contracted
countenance, and occasional vomiting. While in this state, sudden
exertions are apt to prove fatal.
OF SCALDS AND BURNS.
Different degrees of injury are inflicted on the surface from the
application of heated solids or fluids. The term scald is generally
confined to the effects of heated fluids, whilst burn denotes the
consequences of the application of a heated solid, or of ignited
combustible matter; the latter class of accidents is, in general, the
more serious, yet the former, though not injuring the skin deeply,
gives rise to the most alarming symptoms when a large extent of surface
is affected. A slight degree of heat is productive only of redness of
the surface, with a sharp hot pain, and these symptoms may subside with
or without vesication. However, effusion of serum under the cuticle
often takes place almost immediately after the contact of the heated
body—the cuticle may be destroyed by the intensity of the injury—or the
true skin may die, either partially or throughout its whole thickness,
and the subjacent parts be at the same time injured to a greater or
less depth. But parts, not severely injured at first, may afterwards
perish, violent inflammatory action being excited, which terminates in
sloughing. The neighbouring parts have their vitality much diminished,
by the direct influence of the injury; and hence, when these parts
come to be the seat of increased action,212 sloughing almost inevitably
ensues, from the want of corresponding power. From the same cause,
subsequent sores are tedious in healing, being so far debilitated as
to be unable to assume full vigour; even slight ulcerations following
vesication contract very slowly; the granulations are flabby, and the
discharge profuse and thin. The inflammation is often at first very
violent, and kept within bounds with difficulty. Burns of the trunk,
particularly of the genital organs, are to be considered as attended
with much danger. And extensive burns and scalds, wherever situated,
are always to be dreaded. Violent constitutional irritation takes
place, dyspnœa is apt to occur, with effusion into the chest of serum,
or a sero-purulent fluid; and the nervous system ultimately becomes
oppressed. Great sinking of the vital powers is generally the immediate
consequence of extensive and severe burns; there is shivering, weakness
of the pulse, cold extremities, anxiety, and vomiting, requiring the
exhibition of warm drinks, and even sometimes of cordials, opium, or
strong stimulants. These must, however, be given with a sparing hand,
or the depression following the excitement is with difficulty got over.
Nor can it be matter of surprise that such serious effects occur, when
we reflect on the extreme sensibility, and highly organised state of
the affected part, and the important functions which it is intended
to perform, as well as those sympathies which it holds with internal
parts, on which life principally depends.
In trifling burns cold applications are generally used—as immersing the
part in cold or iced water. A great variety of remedies are employed,
spiritous, watery, acid, alkaline, cold or hot; some apply a coat of
cotton or flour, some of tar or pitch, and they state that when these
artificial crusts separate, the skin is found healed beneath; in fact,
every practitioner, and almost every individual, possesses a favourite
application for this very common accident. Some have recommended
holding the part to the fire, or plunging it into hot liquid; but this
practice, and all similar, are too severe ever to become general,
when milder means prove equally effectual. Perhaps the most common
applications are, a mixture of lime-water and olive oil, or the ceratum
acetatis plumbi. The vesicles, when left to themselves, burst, expose
an irritable surface, and the acrid discharge from them excoriates
the surrounding skin. Their contents ought to be evacuated by a small
puncture, and the cuticle being left carefully undisturbed, a scab
soon forms, by which the part is protected while healing. In extensive
injuries of the skin, where the cuticle has been altogether destroyed,
finely carded cotton is sometimes applied; it is of use in somewhat
the same way as the cuticle in the former instance, and being a sort
of cushion over the part, prevents it from being irritated by bed or
body clothes, or by the patient’s resting on it. It soon becomes soaked
with the discharge, and must either be frequently changed, or become a
receptacle for pus to putrefy in, and maggots to breed; on account of
these circumstances it is objectionable. Dusting the part with common
flour, starch, or hair powder, is equally advantageous, and much more
convenient; relief is afforded by its immediate application; the parts
are cooled; the flour, absorbing the discharge, is soon formed into
crusts, which213 effectually protect the surface; and the after-secretion
readily escapes from beneath this, no more moisture being imbibed than
is merely sufficient for the encrustation. The artificial covering
ought not to be removed until completely detached, by purulent matter
accumulating beneath it; then its presence can be of no service, and
its removal is accomplished by fomentation or poultice, and without
pain to the patient; whereas, by pulling off the crusts shortly after
their formation, as some do, whilst they are adherent to the surface,
and protecting it from injury, much pain is given to the patient, the
raw surface is irritated, and made liable to over-action; a useful
application is taken away to make room for another, and, perhaps, not
so congenial. After the spontaneous separation, fresh flour may be
again sprinkled over the suppurating surface, and, if the affected part
is small, it may heal under this application. But when, in burns of
considerable extent, suppuration is fully established, and granulations
have begun to arise, tepid-water dressing, and lotions, are to be
applied as to any other granulating sore; for the reasons already
assigned, the applications require to be of a gently stimulating nature.
In severe cases, there is first extreme depression of the powers
of life, under which patients sometimes sink; but most frequently
this state is obviated by the employment of cordials or stimulants.
But these ought to be administered with caution, for reaction soon
commences, and often increases to well-marked inflammation, requiring
for counteraction low diet, and even bleeding. In such cases gentle
laxatives are preferable to purgatives, as by the latter the patient
is obliged to make frequent movements, and those are always painful.
Stimulants have been strongly recommended, at first powerful, and
afterwards gradually weaker, so as, it was said, to restore the balance
between the affected parts and the system; and the latter is again
to be excited, in order to meet the increased action which the parts
assume. The practice is founded on fancy, and cannot become general,
being in its first part cruel, and in its second absurd. Whilst
debility exists, stimulate cautiously; when over-action ensues, adopt
those measures which are best calculated to subdue excitement; this is
common sense, and the common practice.
During the process of healing, position of the parts ought to be
carefully attended to; contraction of the cicatrices, and cohesion of
opposed surfaces often causing unseemly deformities. Surfaces opposed
to each other, and naturally separate, may be prevented from uniting
by dressing interposed; and contraction of joints is to be guarded
against by keeping the limb extended by splints and bandages. Where
deformity has occurred, the hardened cicatrix which is in fault may
be either divided or excised, and by paying attention to position in
the after-treatment, the evil may be greatly lessened. In the case of
contracted joints, it is not necessary to excise the whole or greater
part of the callous web; simple division is sufficient, if carried deep
enough, through the altered and condensed cutaneous tissue. A horrid
case of deformity is sketched on the next page, and from a very horrid
and atrocious scoundrel, the companion and assistant of Messrs. Burke,
Hare, and Co., the Thugs of the Modern214 Athens. In such a deformity
the art of surgery could not avail. In others, however, the cicatrix
is not so extensive; it is separated into bands, by the division of
which the position of the head and lip is improved, and the comfort
of the patient much enhanced. In one case, in which I operated with
success very lately, the scar, though extensive, was remarkably soft
and pliable, as much so as the finest kid leather.

215
PART SECOND.
OF PARTICULAR SURGICAL SUBJECTS.
INJURIES OF THE HEAD.
Wounds of the Scalp are attended and followed by more dangerous
symptoms than wounds of the integuments on any other part of the
body. This is in a great measure attributable to the nature and
connections of the parts. The subcutaneous fatty matter is condensed,
and closely attached to a firm and unyielding tendinous expansion; and
betwixt these tissues and the pericranium, a loose cellular tissue
is interposed, so as to allow of free motion of the parts. They are
highly vascular, with the exception of the occipito-frontalis fascia,
and between them and the internal parts, as is well known, a free
communication exists. Injuries of these coverings, though at first
apparently trifling, and consequently looked upon as of no importance,
and unattended with danger, often assume a very alarming character.
No injury of the head, in fact, is too slight to be despised, or too
severe to be despaired of.
Punctured and lacerated wounds, more especially those penetrating
all the layers of covering, are frequently followed by violent and
extensive inflammation of all the tissues, with severe constitutional
disturbance, and with delirium and other symptoms denoting functional
derangement of the brain. The swelling is often extensive, involving
the whole scalp, together with the integuments of the face, and
completely shutting the eyelids. In some cases resolution may
be accomplished, but the most frequent termination is extensive
infiltration of purulent matter into the cellular, or even into the
more deep structures, with sloughing of the tendinous expansion.
Collections of matter frequently form in the loose cellular tissue of
the eyelids, when the parts are affected with inflammation, whether
superficial or deeply seated.
As to treatment, after the infliction of an injury, the scalp ought to
be shaved, and the wound cleansed of coagula and foreign substances.
If a large flap of integument is detached, it should be replaced,
and retained as nearly as possible in its natural situation; and
if, for this latter purpose, slips of uninitiating adhesive plaster
and methodical compression prove insufficient, it will be necessary
to em216ploy a very few points of interrupted suture: these, however,
must be removed at an early period, that is, when either adhesion or
suppuration has commenced, and ought, if possible, to be altogether
dispensed with, being apt in this situation to produce injurious
effects by their irritation. Light dressing is afterwards applied.
On the accession of swelling, heat, and pain, the parts are to be
well fomented with a hot decoction of chamomile flowers, or hops, and
afterwards covered with a warm and soft poultice; and should these
symptoms continue, the fomentation ought to be frequently repeated.
Fomentation and poultice are also the best applications when a
day or two has elapsed between the receipt of the injury and the
patient’s application for cure. The constitutional symptoms are to be
moderated, and may in many instances be averted, by the exhibition of
antimonials and purgatives; and by general bloodletting, when demanded
and authorised by the symptoms, and the state of the constitution.
Punctures or incisions are to be employed according to circumstances,
in order to lessen the vascular congestion of the part, and prevent
the formation of matter, to evacuate it if already secreted, or to
relieve inflammatory tension and promote the formation of pus at the
incised parts, where erysipelatous inflammation is threatened, healthy
suppuration in such circumstances often appearing to be critical. In
many unpromising cases of lacerated scalp, when a great part of the
cranium has been exposed, and partially deprived of its periosteum, a
rapid cure has taken place without the formation of much matter. The
detached scalp, though much torn and bruised, ought not at first to be
removed, it being more prudent to leave nature to determine how much
must be destroyed. After the sloughs, if any, have separated, and
granulation has commenced, the loss of substance is rapidly repaired
in this region, more especially when the patient is young and healthy.
General or partial support, by bandaging, is required in many cases, as
by a handkerchief, split cloths, or a roller applied in various forms.
Wounds of the Temporal Artery are either the result of accident, or
made intentionally for the purpose of abstracting blood; and it may be
here proper to make a few remarks regarding this latter circumstance.
When it is wished to take away blood from the head, no one thinks
of opening the trunk of the temporal artery; its anterior branch is
generally chosen. By some the vessel is first exposed by means of a
scalpel, and then opened with a lancet. But preliminary incisions
are altogether unnecessary. The vessel ought not to be cut entirely
through, and the incision should extend obliquely across its course;
and care is to be taken that the external aperture shall be larger than
that in the cellular tissue involving the artery, as thus the blood
escapes freely, and no risk is incurred of its becoming infiltrated
into the surrounding parts. When the branch is of the ordinary size,
a sufficient quantity of blood is readily obtained from it; but if,
from its small size, or a faulty form of incision, blood does not flow
freely and quickly, a cupping-glass may be applied, and its lower
edge slightly raised. This latter precaution is absolutely necessary,
for if neglected, little or no blood can escape, the artery being
firmly compressed against the cranium by the edge217 of the exhausted
glass. No other mode of cupping ought to be practised on the temples,
for the cupping by scarification is here both unwarrantable and
unnecessary—unwarrantable, because the cicatrised scarifications
leave an unseemly and permanent mark on a prominent part of the
countenance,—and unnecessary, since there can be no occasion for six
or eight incisions when one is fully sufficient. The bleeding may be
readily stopped, after the requisite quantity has flowed, by a small
graduated compress placed over the wound, and retained by bandages,
which surround the head, and are afterwards twisted and brought
under the chin in order to increase the security. If by these means
the bleeding is not readily restrained, the vessel may be divided
throughout its whole circumference, by entering the lancet at the
original wound, and moving its point laterally. Then compression is to
be again employed, by the assistance of which the natural processes for
closing the divided extremities are speedily accomplished.
When this artery has been injured by external violence, the wound of
the integuments is generally large, and the bleeding profuse. In such
cases, both ends of the vessel must be pulled out by means of forceps,
and tied separately; afterwards the integuments are to be approximated
and supported.
Unpleasant consequences sometimes result from the simple operation of
opening the temporal artery, and occasionally also from accidental
wounds of that vessel. The integuments unite, and may soon heal; but,
from the compression not being sufficient, a small quantity of blood
is insinuated into the cellular tissue, which becomes condensed for a
considerable extent around the wound, and ultimately a sac is formed,
which communicates with the ununited opening in the artery, and is
consequently filled with sanguineous clots; in short, an aneurismal
tumour is formed. For the cure of this untoward occurrence, the artery
may be tied between the heart and tumour, as in the case of spontaneous
aneurism; but in consequence of the free inosculation which exists
between the numerous ramifications of the artery, this measure may
not prove successful, and it will be found necessary, either then
or afterwards, to secure the vessel beyond the tumour. But there is
another mode of procedure. From the tumour being generally small and
circumscribed, excision of the whole of it can be effected easily,
and so as to leave but a slight scar: this operation is not liable to
failure, and is not more severe than the first mentioned. After the
removal of the diseased part by elliptical incisions, the two ends of
the artery are to be included in separate ligatures, and the edges of
the wound kept together.
A more troublesome accident sometimes takes place,—ulceration of, and
over, the vessel, with effusion of serous and purulent fluids into the
surrounding cellular tissue, often to a great extent. A profuse flow of
blood bursts from the ulcerated surface, perhaps twelve, fifteen, or
twenty days after the vessel had been opened, and, if active means are
not speedily adopted, the hemorrhage by its recurrence may prove very
dangerous. In such cases compression is of no avail; the bleeding may
be staid for a time by this means, but upon the circulation becoming
again active, fresh hemorrhage must and218 does take place; the parts
around are separated and engorged more and more, the blood escapes in
alarming quantities, and the patient is saved only by the occurrence of
syncope. To search for, and make a clean dissection of the wounded part
of the vessel in such cases, is impossible. A long and deep incision
must be made through the swollen and diseased parts in the course of
the arterial branch, and a ligature passed under it, on each side of
the ulcerated point, by means of the common curved suture-needle, or
of one in a fixed handle. The ligatures should be at a considerable
distance from each other, in order that they may surround healthy parts
of the vessel; after they have been firmly tied, all risk of further
hemorrhage is gone. Of course the ligatures should enclose as little
as possible of the parts surrounding the artery. A poultice is perhaps
the best application for a few days, and under its soothing influence
the effects of the continued compression, which had been previously
employed, soon subside. The after applications must be varied according
to the appearances which the part presents.
Laceration of a large or small bloodvessel is a frequent consequence
of bruise of the scalp.—Blood is effused, and the surrounding parts
are thereby separated to a greater or less extent; and thus a tumour
is formed, either rapidly or slowly, according to the size of the
injured vessel. The swelling is in general large, soft in the centre,
and hard towards its circumference; the blood in the latter situation
being coagulated, and firmly impacted in the condensed cellular
tissue; whilst in the centre it is fluid, or at least partially so,
and occupies a free cavity. These characters of the tumour are apt
to mislead a careless or inexperienced examiner, the feel being in
some degree similar to that attending fracture with depression, but
still easily distinguishable from it by attentive and experienced
manipulation. By pressing the finger or thumb firmly on the centre
of the tumour, the blood is displaced, and the bone felt distinctly.
In slight cases of this affection, no treatment is required, as the
tumour is of no importance, and soon disappears, by the effused blood
being absorbed. When, however, the swelling is accompanied with
unpleasant symptoms, cold applications are to be made to the part,
and low diet, with occasional purgatives, enjoined. If inflammatory
symptoms occur, local abstraction of blood may be necessary, followed
by hot fomentations to the part. When the pain has ceased, and the
swelling is not speedily removed, absorption is promoted by stimulating
applications, such as fomentation with a solution of the muriate of
ammonia in a decoction of the anthemis nobilis, in the proportions
of ℥ss. to ℔ii.; a spirit lotion containing the tincture of
arnica montana, in the proportion of one part to fifteen or twenty of
water, will be found a good application in many such cases.
Such tumours may ultimately require to be laid open, in consequence
of the blood putrefying and becoming mixed with purulent secretion.
Under no other circumstances is incision warrantable, as unhealthy,
troublesome, and tedious suppurations are sure to follow.
Of Concussion.—Concussion, in a greater or less degree, attends
most injuries of the head. The functions of the brain are either
disturbed or suspended; there is loss of sensibility, of volition,
and219 frequently of the power of motion. The confusion of intellect
or stunning may disappear in a short time, or may continue, though
diminished in intensity, for many days, and even for weeks; it is
seldom, however, that the functional disorder exceeds in duration two
or three days, and in general it disappears before that length of time
has elapsed. The stupor is seldom complete; the patient can perhaps
be roused, though with difficulty, so as to answer questions by a
hurried monosyllable, or make signs in regard to the seat of pain, or
for such things as he may suppose himself to be in need of. At first
the circulation is weak; the pulse is fluttering, often intermitting,
and scarcely to be felt in the extremities; the countenance is pale,
and the surface cold; there is occasional vomiting, a symptom which
seldom occurs when compression of the brain exists, and the breathing
is difficult, though scarcely ever stertorous. The pupils are generally
contracted, but not uniformly so; one pupil may be contracted and the
other dilated; at first, they are insensible to light, neither dilating
when in darkness, nor contracting further when the light is suddenly
increased; not unfrequently a considerable degree of squinting exists.
The muscles are neither much relaxed, nor spasmodically contracted.
After a time, the circulation is restored, and the heat of the surface
returns, with more or less of regained sensibility. The pulse either
becomes altogether natural, or else more slow or more rapid than in
health. The circulation is then easily excited; by even raising the
patient in bed, the pulsations of the carotids are increased, in some
cases, by fifteen or twenty beats. Sensibility returns, always very
gradually, and in some cases more slowly than in others; frequently the
patient becomes quite collected after the lapse of some hours or a few
days, but in other instances a degree of mental confusion remains for
many weeks; occasionally the intellect continues weak for a lengthened
period, and sometimes even for the remainder of life.
When the insensibility has begun to diminish, the patient can be roused
with less difficulty; if pinched, he complains of it by uttering some
inarticulate sounds, or by attempting to move himself further from the
quarter whence he supposes the injury to come; he answers, though with
unwillingness, loud questions regarding the pain which he suffers, and
points to the part where it is chiefly felt. As the stupor goes off,
symptoms of inflammatory action, or a threatening of it in a greater
or less degree, manifest themselves. The pulse becomes more rapid and
sharp, the skin is hot and dry, the face is flushed, the conjunctiva
is redder than usual, and the pupils are often much contracted: the
patient is restless, and tosses about in bed; mutters confusedly to
himself; often attempts to enact a part in some fanciful scene which he
supposes to be passing around him, or talks rapidly and incoherently
concerning circumstances which have formerly occurred. His flitting
ideas are often of an alarming nature; he endeavours to get out of bed,
and struggles violently if opposed. He frequently puts his hand towards
his head, and gives other indications of suffering acute pain in that
region, much increased by any movement of the part.
Such symptoms are often followed by vomiting and rigors, and too220
frequently by convulsions, more furious delirium, and coma. On
examination after death, an increased vascularity of the cerebral
membranes is observed; there is an effusion of gelatinous-looking
matter on the surface of the membranes, and in the cellular tissue
beneath the arachnoid. In more advanced cases, thin patches of lymph,
or more extensive strata of it, cover the arachnoid and the inner
surface of the dura mater; a puriform fluid is found effused between
these membranes, and sometimes blood and matter are deposited in
some part of the cerebral substance; bloody serum is effused into
the cavities, and at the base of the brain. The above symptoms and
appearances sometimes follow injuries not at first thought severe, but
are most frequently the result of such as are attended with læsion of
the bone, or of the internal parts.
It is not at all improbable that concussion is produced after a manner
somewhat resembling the following. The brain has a natural tendency to
remain at rest, but is liable to be brought into a state of commotion
by impulses on the cranium being communicated to it. When a slight
blow is inflicted on the skull, only a slight commotion of the brain
is induced, the cranial contents are, as it were, slightly jumbled,
and a temporary and trifling confusion of its functions follows. When,
however, the stroke is more severe, the brain is separated from its
cranial attachments, both at the point struck and at the part directly
opposite,—it is thrown upon itself towards its centre; its substance
is thereby condensed, its diameter in the direction of the impulse is
diminished, and a separation between the brain and cranium is formed at
each extremity of that diameter. By post mortem examinations, it has
been ascertained that condensation of the substance of the brain does
exist in cases of severe concussion. Such commotion may be sufficient
to cause instant extinction of life, or the brain may gradually resume
its former condition, or with only such slight incited action as may
be required to reunite the dura mater with the inner table of the
skull. Extravasation of blood or serum is extremely liable to occur
in such cases, the vessels being either compressed, stretched, or
otherwise thrown out of their natural relations along with the other
cranial contents, reparation can only take place by absorption of the
extravasated fluid, and gradual deposition of plastic matter. When
extravasation takes place to a greater extent, compression is the
consequence, as will be more fully explained further on. Perhaps the
brain does not recover itself gradually, but suddenly; the impulse,
which was at first directed from the circumference towards the centre,
now acting from the centre towards the circumference; and then the
propulsions and recoilings may be repeated, though gradually lessening
in their intensity, until the effect of the original impulse is lost,
and all vibration consequently ceases. But concussion may be caused by
an impulse received not immediately on the cranium, but on some other
part of the body, as when a person falls from a considerable height and
alights on the feet or buttocks; and in such a case also its effects
may be indirectly communicated to it through the brain, and may produce
equally violent effects, without there ever being any appreciable
lesion of the cerebral matter.
221
The circulation may be merely disturbed, or laceration of the brain may
occur with extravasation of blood into its substance. It may present
the appearance of having been bruised, or the tear of its substance may
be extensive. A multitude of minute vessels may be torn without the
substance of the brain being much broken, in which case bloody specks
will be observed over a large surface of the interior of the organ.
In many fatal cases no change in the state, either of the vessels or
of the cerebral substance, is perceptible on minute examinations. The
organ in these cases has been merely disturbed and shaken, without
visible rupture or hurt having occurred. Again, many patients are
supposed to labour under concussion only, in whom fracture of the base
of the cranium, or extravasation of blood on the surface, or into
the substance of the brain, are discovered after death. It is always
difficult to distinguish between the effects of mere concussion and
those of compression of the brain by extravasated fluid; for, in the
greater number of cases, the symptoms of both affections are blended
together. In both there is insensibility from the first; but if an
interval of sensibility occur, diagnosis is rendered more easy and
certain, it being a fact well verified by experience, that the state
of stupor which precedes the return of correct intellectual function
is the effect of concussion, and that there is every reason to believe
that the insensibility into which the patient subsequently sinks, is
caused by compression of the brain; if compression existed from the
first, the stupor might not be of longer duration than if it were
the effect of concussion, but its stillness would not be interrupted
by any restoration of mental exercise, however short. Remarkable
effects sometimes result from commotion of the brain; the patient may
suffer loss of vision or of hearing, either partial or complete; or
partial paralysis may occur; of the muscles, for instance, supplied
by the portio dura. In many cases such affections may be supposed
to arise from compression of nerves, or other læsion subsequent to
and caused by the effects of concussion, and probably connected with
fracture of the base of the cranium. Again, it occasionally happens
that the senses are rendered more acute than previously, and of this
I shall mention an example which came under my own observation. An
old nurse sustained fracture of the vertex, with slight depression of
the broken part, in consequence of some rubbish having fallen on her
from a considerable height. Stupor, along with the other symptoms of
concussion, was the immediate effect of the injury, but disappeared in
two or three days. Her hearing, which previously to the accident had
been long so obtuse as to render it necessary for her to discontinue
her employment, became so intensely acute, that the most trifling
noise became a source of pain. She gave immediate orders for the clock
to be stopped, the ticking of which annoyed her greatly. Her hearing
gradually became of the natural intensity, and continued perfect. In
this case there can be little doubt that restoration of a sense which
had long remained dormant arose entirely from cerebral commotion, for
no discharge of blood or other fluid occurred from the ears, by which
cerumen accumulated in these organs might have been displaced.222 People
sometimes forget languages from hurts of the brain, whilst they retain
memory in other respects; or, rather, the memory on certain things
becomes injured, but remains quite perfect on others.
Treatment.—Whilst the circulation remains depressed after injuries
of the head, or of other parts of the body, it is a common practice to
abstract blood; but it is one which cannot be too much reprobated, for
it is attended with great risk, and can be productive of no benefit;
the feeble remains of vital power, whilst struggling as it were against
the depressing cause, may by depletion be quickly annihilated, when
the vigour which they still retained might have been sufficient, if
encouraged and supported, to overcome those effects of external injury
which had so far reduced them.
When a patient is seen insensible, it is highly proper and necessary
to examine carefully the trunk, head, and limbs, in order to ascertain
whether either fractures or displacements have occurred; for it is by
no means creditable to the care or science of a surgeon to be made
aware of such accidents when the patient regains his senses, after the
lapse perhaps of weeks, and when they can be remedied, if at all, with
much difficulty.
In the first stage of concussion, as was already observed, the
circulation is much weakened, and it is therefore necessary to adopt
means for sustaining and strengthening it; and with this view, warmth
is to be applied to the surface, more especially to the extremities and
epigastrium.
When the powers of life appear to be failing, stimulants must be
administered internally. Perhaps the most convenient stimulus is ardent
spirit, the only objection to its use being, that when imprudently
given in large quantities, its effects, though at first stimulant,
become sedative; it ought to be given in small quantities, and at short
intervals. Other stimuli, as preparations of ammonia, may be given
by the mouth; and much advantage will often be found to follow the
employment of a turpentine enema, free motion of the bowels, as well as
excitement of the system, being thereby procured.
Stimuli, however, should always be used with much caution and prudence,
and never unless fully warranted by the train of symptoms under which
the patient is labouring at the time; when the circulation is restored
in the limbs, and is becoming throughout steady and more natural, all
sources of excitement must be abandoned and carefully avoided, as there
is considerable risk of reaction proceeding to too great a height.
The patient is to be kept quiet in a darkened room, cold applications
made to the head, previously shaved, and free motion of the bowels
procured by neutral salts with antimony, or by other purgatives not of
an irritating nature, and not given in such doses as to prove violently
cathartic. Enemata are in some cases preferable, and are always a
valuable adjunct, to the employment of purgatives by the mouth; they
procure evacuation from the larger intestines, in which feculent matter
chiefly accumulates; they ought to contain asafœtida and turpentine;
with these additions more salutary effects are produced than from mere
evacuants. The latter ingredient would seem, by its local stimulus, to
impart energy to the bowels sufficient for the correct performances of
their func223tions, while the former tends to allay spasm and irritation,
both locally and generally.
If the circulation becomes unduly excited, abstraction of blood
from the system, in sufficient quantities and at proper intervals,
is absolutely necessary; and the depletion must be regulated by the
symptoms and circumstances of each case. The action will in general
be more speedily and effectually moderated by one copious bleeding
at the commencement, than by repeated bleedings to a less extent. An
easy and open state of the bowels is of much importance in the excited
stage. Mercurial preparations are sometimes useful, as they are known
to possess the power of causing the absorption of coagulated lymph and
serum, and probably of preventing their effusion.
In cases where insensibility continues after the arterial excitement
has been subdued, counter-irritation on the head or the back of the
neck is often useful, as the application of blisters, or the rubbing in
of antimonial ointment. These are supposed to act by causing an unusual
influx of blood to the surface, producing a change in that fluid by the
copious purulent, serous, and lymphatic secretions from the irritated
part, and thereby diminishing the distended and engorged state of the
internal vessels, which might produce considerable compression of the
brain.
If, at a late period in the case, the powers of life begin to flag,
stimulants must be again had recourse to, and may now be pushed pretty
freely, there being less risk of inordinate action ensuing, and much
reason to fear that life can be prolonged only by the continued use of
powerful means for the excitement of the system. Nor ought the surgeon
to cease stimulating though the vital powers continue to diminish in
spite of the treatment, and though the circumstances of the case may
be so hopeless as to lead him to suppose that death cannot be further
delayed; for many patients, who would otherwise have necessarily
perished, have, by the continued use of stimuli, recovered under my
care their sensibility, and been ultimately restored to health.
Separation of the dura mater from the cranium, with more or less
extravasation of blood between, sometimes takes place as a consequence
of blows on the head, even though not severe. The blood may be
absorbed, or an unhealthy abscess may form between the bone and
membrane, attended with violent, dangerous, and, if neglected, fatal
results. The internal mischief is not without external marks of its
occurrence. If the scalp is undivided, a puffy tumour forms; and, when
it has been injured, the wound degenerates, its surface is pale, and
the discharge gleety; the exposed bone appears white and dry. It is
also preceded by general disorder of the system, by restlessness and
fever; there is sickness, occasional vomiting, shivering, pain of the
forehead and back of the neck; in some cases, delirium and convulsions,
and perhaps partial paralysis, and ultimately coma. All these symptoms,
however, may exist without indicating precisely either the existence or
the site of abscess, as I experienced in the following cases.
A middle-aged man was brought intoxicated into the Royal Infirmary with
a lacerated wound of the scalp, over the upper part of224 the occipital
bone, on the right side of the mesial line. For thirteen days after
the accident he did well, walking about the wards in good health, with
the wound healing kindly; but on the fourteenth he became affected with
hot skin, restlessness, slight incoherency, severe pain in the head,
and intolerance of light, with a full but not quick pulse. A vein was
opened, but after three ounces of blood had flowed, he was seized with
rigors, vomiting, and violent convulsions; and these symptoms again
occurred after the application of leeches to the head. Rigors returned
at various intervals; stupor supervened and gradually increased. He
became delirious on the eighteenth. A considerable part of the bone
was exposed and dead, and there was a puffy swelling of the scalp
around the wound. On the nineteenth he lay insensible. A portion of the
dead bone was removed by the trephine, and the dura mater was found
covered with lymph, but no appearance of effused blood or pus could
be perceived. He seemed to suffer nothing from the operation, but
continued insensible, passing his urine and feces in bed, with dilated
pupils, quick breathing, and subsultus tendinum; his pulse, which had
previously never been above 80, now rose to 100. He died on the morning
after the operation. On dissection, the right hemisphere of the brain
was found of the healthy appearance; but four ounces of pus lay over
the left hemisphere, between the dura mater and arachnoid, which
latter membrane was of a granular appearance; there was also a small
sloughy spot of the dura mater over the left anterior lobe.—A woman,
aged 40, fell down and sustained a wound of the scalp on the upper part
of the occipital bone on the left side; she suffered but little from
the accident, and continued to live freely and irregularly. Seven days
after the injury she was seized with shivering: and on the ninth day
she lay comatose, voiding her feces and urine involuntarily. The wound
was pale and gleety, and the surrounding scalp puffy; the bone was bare
and white; pupils dilated; pulse slow. The trephine was applied, and
fluctuation felt beneath the exposed dura mater, which was otherwise
unchanged in appearance; the membrane was divided by a trifling crucial
incision, but only a small quantity of bloody serum escaped. Shortly
after the operation she became quite sensible, but again sunk into a
state of stupor, with slightly stertorous breathing and contracted
pupils. However, all traces of coma disappeared next day, and she
recovered soon and perfectly, apparently without having received either
benefit or injury from the operation of trephine.
Purulent collections under the cranium, between the bone and dura
mater, are not of very frequent occurrence, when symptoms are well
watched and treatment properly conducted. But these collections
certainly may and do occur, and usually at a considerable period after
the accident: many such cases are related by the older authors. Their
attendant symptoms are materially different from those of extravasated
blood; in the latter case, all the symptoms of compression ensue
immediately after the effusion has occurred, and that is generally
very shortly after the injury. But matter is not formed till after a
considerable period has elapsed; it is not attended with symptoms of
compression suddenly supervening, but is preceded by225 restlessness
or febrile excitement; and in the later stages only of the affection
do the symptoms of cerebral compression manifest themselves. By the
external injury, those bloodvessels by which the dura mater is attached
to the skull, and by which it communicates with the pericranium and
more external parts, are lacerated, or otherwise materially injured,
inflammatory action is excited in the connecting medium, unhealthy
suppuration ensues, and by the accumulation of matter, the membrane
is completely separated from the cranium, and generally participates
in the morbid action. It may ultimately slough and give way, and the
matter will then be effused internally. A similar process goes on in
regard to the bone and its pericranium, a tumour forms externally, and
the bone, being deprived of its supply of blood, necessarily dies,
either in part, or throughout its whole thickness. When an external
wound exists, the altered appearance of the bone, with the sloughy
state of the detached pericranium, gives evident warning of the
mischief which is proceeding internally.
The general symptoms of suppuration are the same, whether the
collection forms in the substance of the brain, or on its surface.
Perhaps the symptoms are not so severe, nor the collection so speedily
fatal, when in the substance of the brain, as when situated immediately
under the bone, or at the base of the cranium. The external marks
already mentioned, are generally indicative of the site of such
internal collection, but not uniformly.
Formation of matter in the diploe of the skull, in consequence of
external injury, is of rare occurrence; and when it does occur,
somewhat similar symptoms and appearances ultimately ensue as when the
suppuration commences between the bone and dura mater.
Sometimes the abscess under the bone is of a chronic nature, as in
the following case:—The patient, a boy, æt. 11, received a blow on
the vertex, after which a puffy tumour formed in the injured scalp,
and was freely incised. He afterwards became subject to epileptic
fits, which were relieved by copious evacuation of matter from the
wound. Exfoliation of the cranium occurred; one small sequestrum
was separated, which involved the whole thickness of the bone, and
a collection of matter between the dura mater and skull-cap was
thereby exposed. The contained matter was evacuated, and the wound was
carefully dressed, with the view of procuring adhesion between the
membrane and bone, but without effect. The dura mater was ascertained
to be extensively detached around the opening; it was found necessary
to remove a large portion of bone by means of the trephine and cutting
pliers, and then the dura mater soon became united with the integuments
of the head. Many months afterwards, the patient complained of severe
pain in the back of the neck; an abscess formed in that situation, and,
pointing under the right scapula, was opened. Weakness of the right
arm and of the inferior extremity suddenly supervened, and the patient
gradually sunk. On examination after death, the cervical portion of the
spinal chord was found much softened, with infiltration of purulent
matter into its substance. The deficiency in the cranium was supplied
by a ligamentous expansion, to which the dura mater and scalp adhered
intimately.
226
Of Compression of the Brain.—Compression is produced by extravasation
within the cranium of blood or other fluid, by the lodgement of a
foreign body on the surface of the brain, or in its substance, or
by displacement inwards of portions of the cranial bones; and these
causes are usually the effects of external injury. It may either
follow the injury instantaneously, or supervene some time thereafter.
Many examples have occurred of a patient, at first insensible, with
symptoms of concussion, having had the functions of the brain restored
almost entirely, and again having relapsed very quickly into a
comatose state, in consequence of extravasation of blood. The whole
circulation is at first lowered by the shock of the commotion, and the
blood scarcely flows in the cerebral vessels; but on its restoration,
blood is poured out from the lacerated vessels, or from those which
have been so injured in their coats as to be unable to withstand the
increasing impulse of their contents. As was already observed, the
symptoms of compression are often mixed up with those of commotion,
but, when an interval of sensibility has occurred, mistake in diagnosis
can scarcely occur. Compression is attended with slow, stertorous
breathing; a distinct slow pulse; a relaxed state of the limbs,
features, and sphincters; and dilated pupil. Total insensibility to
external impressions attends compression of the brain, whatever the
cause of it may be. These symptoms may, and do sometimes, gradually
disappear after a time. But they may continue unabated, and the patient
may gradually sink under them. Or, again, his dissolution may be
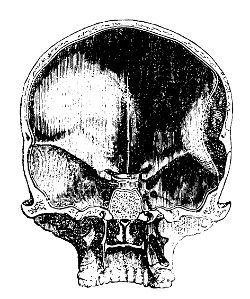 preceded by excited circulation and furious delirium, the vital powers
recovering from their first depression, only to become roused into
violent and destructive action, again to sink to a still lower ebb,
and be ultimately annihilated. Extravasation is most commonly met with
on the lateral parts of the brain in the situation here indicated; the
coagulum is perhaps extensive, reaching to the base of the skull, in
consequence of rupture of the middle meningeal artery, with or without
fracture of the parietal bone.
preceded by excited circulation and furious delirium, the vital powers
recovering from their first depression, only to become roused into
violent and destructive action, again to sink to a still lower ebb,
and be ultimately annihilated. Extravasation is most commonly met with
on the lateral parts of the brain in the situation here indicated; the
coagulum is perhaps extensive, reaching to the base of the skull, in
consequence of rupture of the middle meningeal artery, with or without
fracture of the parietal bone.
Little or nothing can be done in cases of compressed brain from
extravasation. We possess no means of preventing the effusion, and
though we did, the mischief has generally taken place before the
patient can receive assistance. Again, the site of the extravasation
can seldom be ascertained; and, should that objection to the propriety
of surgical interference not exist, still the coagulated blood cannot
be evacuated even after extensive removal of the bone. If the coagulum
is small, it may be gradually and wholly absorbed, or the brain may
become accustomed to the pressure of what remains. It is the surgeon’s
duty to take227 means for averting inflammatory action, and to subdue
or moderate it when it has been excited. The symptoms arising from
displaced bone may be relieved by surgical operation; but we must
premise some observations on fracture, before speaking of the treatment
necessary in such cases.
FRACTURES OF THE CRANIAL BONES.
At an early period of life the bones are soft and elastic; they yield
readily under external violence, and it requires a great and direct
force to produce fracture of them. Late in life, when the diploe
disappears, the external and internal tables come in contact; the bone
is brittle, and solution of continuity in it is easily effected. And
it is wisely so arranged, for thus in the recklessness of childhood
and youth, severe blows on the cranium, which are then of so frequent
occurrence, are seldom attended or followed with danger; whilst the
aged are taught by experience to avoid the unfortunate consequences so
apt to result from even a slight blow on the then brittle cranium, by
cautiously preserving themselves from exposure to violence.
Solutions of continuity in the cranium, caused by external force,
are either attended with depression or not. Fissures, mere capillary
rents in the bone, may take place at the part of the cranium which is
struck, or on the side opposite to that to which the force is applied.
They will be found either short and limited by sutures, or extending
in different directions through several sutures, as from the vertex to
the base of the skull, and terminating perhaps in the foramen magnum.
Fissures in the upper part of the cranium are of themselves attended
with comparatively little danger; they produce of themselves no claim
to attention, and really require none. But the force which gave rise
to the injury of the bone may have disturbed the internal parts; and
though the patient may have recovered from the first shock and the
immediate effects of the violence, severe and dangerous consequences
often result, and at a late period from the infliction of the injury.
Fractures of the base of the skull are the result of great force
applied to the lateral parts of the head, to the vertex, or to the base
itself through the spinal column. A blow inflicted by an obtuse body
on the top of the head, whilst it is at rest and fixed—by producing
expansion of the lateral parietes, and forcing the base down upon the
upper part of the spinal column—may have the effect of breaking up the
connections of the bones at the base, which is the weakest part of the
cranium, and splintering them to a greater or less extent. Again, if
a person falls from a height, he perhaps alights on some part of his
trunk, as the buttocks, and this coming to a state of rest, whilst
the head is still in projectile motion, the spinal column is driven
towards the cavity of the cranium, and the same effects are thereby
produced as in the preceding instance. Or the patient alights on his
head, and the base of the cranium is then impinged upon by228 the weight
of the whole trunk, as well as by the force of the projecting power,
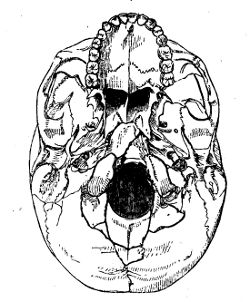 and in this case also the base is frequently broken up. In the sketch
here given, showing extensive fracture of the occipital and sphenoid
bones into the foramen magnum, the patient, a brick-layer, fell from
a ladder on the vertex. He lay comatose for some days before death:
there was found extensive extravasation over the middle lobes and
cerebellum. Concussion has resulted from falls when the person has
alighted on his nates or feet; but the symptoms attendant on fracture
of the base are more generally those of compression of the brain. In
this accident the bones are seldom displaced to any great extent; the
dura mater is generally lacerated, its bloodvessels, and frequently its
sinuses, are wounded, and blood is consequently effused at the base
of the brain, where injury is most fatal. The upper part of the brain
may bear pressure to a considerable degree without bad consequences
ensuing, but compression at the origins of the nerves is always highly
dangerous and generally fatal. Bleeding from the nose, mouth, and ears,
when attended with other circumstances and symptoms evincing a violent
injury and consequent cerebral disturbance, has been considered as
decisive of fracture at the base having occurred. But we find that such
bleeding happens in slight injuries unattended with any circumstances
or consequences to induce a belief that so serious an injury has taken
place: and again, in cases where dissection has shown most extensive
fracture in the temporal, sphenoid, and æthmoid bones, no blood had
issued from their external openings. Fracture of the base of the skull
generally proves fatal, but many cases are met with in which there is
reason to believe that it had taken place, and yet the patients have
recovered with perhaps partial paralysis. Of this I lately met with
a good example in the case of a girl seven years of age, whose head
had been squeezed between a wall and the back of a cart, and thereby
considerably flattened. She lay insensible for several days, with all
the symptoms of compression, and with blood flowing in small quantity
from the nose, mouth, and right ear. An extensive abscess formed
over the right temporal bone. She ultimately recovered, but remained
affected with paralysis of the right side of the face and amaurosis of
the left eye; sensation in the paralysed parts being quite perfect.
and in this case also the base is frequently broken up. In the sketch
here given, showing extensive fracture of the occipital and sphenoid
bones into the foramen magnum, the patient, a brick-layer, fell from
a ladder on the vertex. He lay comatose for some days before death:
there was found extensive extravasation over the middle lobes and
cerebellum. Concussion has resulted from falls when the person has
alighted on his nates or feet; but the symptoms attendant on fracture
of the base are more generally those of compression of the brain. In
this accident the bones are seldom displaced to any great extent; the
dura mater is generally lacerated, its bloodvessels, and frequently its
sinuses, are wounded, and blood is consequently effused at the base
of the brain, where injury is most fatal. The upper part of the brain
may bear pressure to a considerable degree without bad consequences
ensuing, but compression at the origins of the nerves is always highly
dangerous and generally fatal. Bleeding from the nose, mouth, and ears,
when attended with other circumstances and symptoms evincing a violent
injury and consequent cerebral disturbance, has been considered as
decisive of fracture at the base having occurred. But we find that such
bleeding happens in slight injuries unattended with any circumstances
or consequences to induce a belief that so serious an injury has taken
place: and again, in cases where dissection has shown most extensive
fracture in the temporal, sphenoid, and æthmoid bones, no blood had
issued from their external openings. Fracture of the base of the skull
generally proves fatal, but many cases are met with in which there is
reason to believe that it had taken place, and yet the patients have
recovered with perhaps partial paralysis. Of this I lately met with
a good example in the case of a girl seven years of age, whose head
had been squeezed between a wall and the back of a cart, and thereby
considerably flattened. She lay insensible for several days, with all
the symptoms of compression, and with blood flowing in small quantity
from the nose, mouth, and right ear. An extensive abscess formed
over the right temporal bone. She ultimately recovered, but remained
affected with paralysis of the right side of the face and amaurosis of
the left eye; sensation in the paralysed parts being quite perfect.
Fractures of the upper part of the cranium are generally attended229
with displacement to a greater or less extent, and with wound of the
cranial coverings. The size of the depressed portion, the depth to
which it is displaced, and the extent of wound, will depend upon the
nature and intensity of the force applied. When both tables are broken,
the fracture of the inner is almost always more extensive than that of
the outer one, as fissures will extend furthest in the most brittle
part. A broken fragment, comprehending the entire thickness of the
skull, presents generally a much larger portion of the inner than of
the outer table, so much so that the piece would sometimes not admit of
removal, though perfectly detached, without enlarging the opening in
the outer table. Fractures, with depression of a considerable portion
of one of the flat bones, are sometimes unattended with any alarming
symptoms. The effects of the injury soon disappear, and even in cases
where the depression has been very considerable, and where, from the
escape of brain, it was evident that both this organ and its membranes
had been seriously injured, no bad symptoms have occurred to retard
the patient’s recovery. Symptoms of compressed brain, however, may
generally be expected to attend depression of any considerable portion
of bone below its natural level. Still the brain may become accustomed
to the pressure, and the symptoms may gradually subside without
surgical interference. And if the indications of compression are not
very alarming, the coma not very profound, a little delay is allowable,
means being taken to avert inflammatory action: for danger is not
imminent, the cure may not be expedited by operative aid, and there is
chance of injury resulting from rash interference.
But it is in general necessary to remove the cause of the symptoms, to
elevate the depressed bone, and take away those portions which may be
detached.
It has been said that we must be regulated in our proceedings very much
by the existence or not of external wound; that we must be cautious in
cutting down upon fractures of the cranium where there is no wound, and
so converting a simple into a compound fracture. In fact, so much is
the danger increased, it is alleged, by the existence of wound, that
the symptoms must be very urgent indeed which would demand division
of the integuments in order to admit of examination of the fracture,
the application of the trephine, or the elevation of the bone; whilst,
on the contrary, if the fracture is exposed by the accident, very
slight symptoms will fully warrant performance of the operation of
trephine. In other words, it is said that simple fractures should be
left to nature, unless under very urgent and alarming circumstances,
and that compound ones ought almost always to be interfered with. But
the facts are otherwise. The greatest danger of compound fractures of
the cranium does not arise from the admission of air. It is not the
wound of the scalp, but the mechanical irritation of the brain and its
membranes that proves dangerous. Injuries of the cranium inflicted by
sharp bodies, such as divide the scalp and cause compound fractures,
are generally attended with splintering of the internal table, and
require the trephine. The existence of this sort of fracture of itself,
without a single bad symptom, without any present disturbance of the
sensorial functions, is a suffi230cient warrant for the application of
the trephine, so as to permit the removal of the detached portions of
the inner table: and this should be done before inflammatory symptoms
have shown themselves. The brittleness of the internal layer of the
skull is well known. In fractures inflicted with sharp and pointed
instruments, as a bayonet or pike, the corner of a sharp stone, or
the heel of a horse’s shoe, the external opening is often very small,
it is a mere puncture; in the bone there is a central depression,
from which fissures proceed around in a radiated form, and hence the
injury has been termed punctured, or starlike fracture. But though
the external wound is apparently insignificant, the vitreous table is
extensively separated, and, perhaps, broken into innumerable minute
and sharp spicula. These sharp portions are driven down upon the
dura mater, and by them the membrane is often severely lacerated. If
these be not removed soon after the accident, inflammatory action
is almost invariably lighted up on the surface of the brain; and we
cannot expect to allay or avert such action by general antiphlogistic
means, however energetically applied, so long as their exciting
cause remains. It is in such cases, I repeat, that the operation of
trephining is imperiously called for. Sometimes, however, patients
are found to recover from punctured fracture of the cranium, without
the operation having been performed, as in the following case, the
only one so terminating with which I have met:—On the 4th September,
I was consulted by a gentleman, aged 35, who had received a punctured
fracture of the cranium, on the 29th of August; a heavy dung fork had
fallen from the top of a haystack, and struck him on the upper part of
the head. Immediately after the accident he became confused, but not
insensible; he lost the power of motion in the right lower extremity,
but almost instantly regained it. Next day the right arm became weak,
and when I saw him, he was almost wholly unable to move it: he could
not bend his fingers, nor raise the arm, and he retained the power of
exercising but very slight motion in the elbow-joint. There was a small
wound of the scalp, nearly healed, over the posterior part of the left
parietal bone, close to the sagittal suture, and nearly midway between
its two extremities. A probe passed down to, and through, the bone;
and there was slight swelling of the scalp around the wound. He had
felt pain in the right ear, and in the forehead, whilst stooping, for
some days after the accident. No blood had ever escaped from the ear. A
fit of shivering occurred on the night following the injury, but never
returned. He soon recovered completely.
I subjoin a case of an opposite description. A coachman was knocked
down, late on a Saturday night, and fell with his head on the corner
of a stone on which masons had been recently working. After being
carried to his lodgings, he recovered from the stupor produced by the
combined causes of liquor and blows; and next morning he went to have
his head dressed by an apothecary, who with difficulty extracted a
fragment of the stone from the wound of the head. The patient then
drove a party to church, and probably drank some more whiskey during
the day. He afterwards felt indisposed, and was seized with sickness
and shivering in the afternoon. On Monday231 he was in a violent fever,
and I saw him in the evening. He had been delirious, but was now lying
in a state of stupor. There was a hole in the right parietal bone,
capable of admitting the point of the little finger, and many loose
fragments of bone were felt lying on the dura mater; a trephine was
applied, and numerous spicula were removed. Afterwards, the circulation
became much excited, he was bled copiously, and antimony was exhibited
in nauseating doses; but he died early on Wednesday morning. On
dissection, there were found marks of violent inflammatory action on
the surface of the hemispheres. The vessels were unusually numerous
and highly engorged, and lymph and pus were effused in considerable
quantity, the arachnoid was opaque, and the cerebral substance was
somewhat softened. Had the operation been performed at an earlier
period, there is every probability that the inflammation, which proved
fatal, would have been averted, as in the following instance:—A
quarryman received a blow from a sharp stone of considerable size,
which rolled down a precipitous bank, and struck him on the vertex.
He lay insensible for half an hour, but recovered, and followed his
occupation during the rest of the day. In the evening he came for
advice. There was a small wound in the scalp, and the subjacent bone
was fractured exactly in the same manner as in the former instance, but
he felt no uneasy symptoms whatever. The consequences likely to result
from such an injury, and the necessity for trephining, were represented
to him; he agreed, and the operation was performed on the spot. Many
sharp fragments of the inner table were extracted; he proceeded home,
never had a bad symptom afterwards, and consequently required no
treatment save dressing of the wound.
The operation, if undertaken early, will, in all probability succeed in
averting future evil, more especially if the dura mater be not wounded.
As a proof of the unfavourable nature of this latter circumstance,
I give the following case:—A young man, aged 18, received a kick
on the forehead from a horse, September 9th. He remained perfectly
sensible, and did not fall to the ground. Shortly after, he was seized
with vomiting, which recurred at intervals; his pulse was regular,
but feeble; pupils dilated. On the centre of the forehead, there was
an irregular wound, which extended to the root of the nose; and on
introducing the finger, the os frontis was found fractured, and a small
portion of it comminuted and depressed. The trephine was applied, and
several detached portions were removed, with some difficulty, from
beneath the undepressed portion of the bone. A spiculum had lacerated
the dura mater, and penetrated the substance of the brain, to the
depth of half an inch; on removing it, a small portion of cerebral
matter escaped. The fracture extended apparently in the direction
of the right orbit. In the afternoon, the pulse was sixty-four, of
good strength, and the pain in the wound had slightly increased. He
was bled to fourteen ounces, and ordered an antimonial solution.
Afterwards, the pain of the head increased, the pulse rose, the scalp
around the wound became the seat of puffy swelling, and several small
abscesses formed: the antiphlogistic regimen was rigorously followed,
and the abscesses were freely opened as soon as they began to form.
On the 21st, a portion of the232 brain had sloughed, and there was some
appearance of fungus cerebri; an incision was made into a swelling over
the right temporal muscle, and ℥viii. of blood allowed to flow.
On the 22d, several portions of brain were discharged, the pulse was
100, and intermitting. Next day, he was delirious, and a hernia cerebri
protruded, of sloughy appearance, and considerable size; pulse 142.
Soon afterwards he became comatose; and died early in the morning of
the 23d. On dissection, the integuments and pericranium surrounding
the aperture, in the frontal bone, were found much thickened, and
infiltrated with pus and serum. The dura mater at the wound had a
sloughy appearance. There was great effusion of purulent matter, under
the dura mater, investing the right hemisphere of the brain; the
corresponding tunica arachnoidea was thickened and opaque; and between
it and the pia mater there was considerable deposition of lymph and
pus. The fungus was collapsed, of a dark colour, soft consistence, and
connected with the anterior lobes; the surrounding cerebral matter was
much softened, and mixed with pus. The fracture extended through the
orbitar plate of the right os frontis, over which lay two small spicula
of bone; and a similar fragment was situated over the right optic nerve.
Many cases illustrating the danger of punctured fracture might be
related, but are unnecessary, inasmuch as they would lead to the mere
repetition of such facts as have been already stated.
Fracture of the external table alone must be rare, but we occasionally
see in museums specimens exhibiting a small portion of the outer table
driven into the subjacent cancelli, without any fracture of the inner
table. This kind of injury belongs entirely to that period of life in
which the diploe is of considerable thickness. The treatment would of
course be simply that adapted to contusion or concussion.
It is also possible for a blow on the head to produce fracture of the
brittle inner table, the outer table remaining entire. However uncommon
such a form of injury may be, as its effects may possibly be very
serious, it is right to bear it in mind. A splinter of the inner table
thus driven into the dura mater might cause violent symptoms and even
death.
Wounds of the Brain.—Laceration of this organ to a slight extent,
with more or less extravasation of blood, often takes place, without
external wound, and when the patient has symptoms of concussion only.
In such cases, the blood may be absorbed, and the læsion repaired,
without permanent impairment of the sensorial functions. Wounds of
it, along with fracture of the skull, are often very extensive; and
portions of its substance may be either severely injured, or entirely
separated. Loss of substance, even to a considerable extent, in the
upper part of the hemispheres, may occur, without bad symptoms or
consequences ensuing. The exposed surface of the brain granulates,
and is healed as other parts of soft structure. Generally, however,
untoward symptoms result sooner or later in such cases. Hemorrhage
occurs from the injured part, and a clot protrudes from the external
wound. Or the cerebral substance in the neighbourhood of the wound
softens, and becomes converted into a semifluid mass, often mixed
with pus; and a fungous growth,233 connected with the disorganised
matter, gradually protrudes through the aperture in the cranium, and
is repressed with difficulty. If removed by knife or ligature, it is
rapidly reproduced. Pressure is the only means left by which to attempt
its retardation; and this, too, is generally ineffectual; for if not
very moderate, the effects of compression extend from the fungus to
the whole of the brain, and an impairment of the sensorial functions
in a greater or less degree necessarily results. The formation of such
a growth is generally attended with shivering, sickness, and fever, by
a weak, rapid, and irregular pulse; the strength declines, convulsions
and delirium supervene, and coma terminates the symptoms.26
234
Perforation of the Cranium is not often resorted to since the
treatment of injuries of the head has become better understood. In
former times, the operation of trepan was performed frequently,
235and many seemed to rate the dexterity and science of a surgeon by
the number of holes which he was able to bore in the skull of an
unfortunate patient. It ought never to be performed, unless the
necessity for, and the propriety of, the proceeding be clearly
indicated. It used to be practised in a most unlimited manner for
fissure: cracks were sought for with the greatest care, rules were
propounded to enable the surgeon to distinguish fissures from the
cranial sutures, and from furrow made in the bone by periosteal
vessels; and the trepan was frequently applied over each part of the
fissure, however extensive it might be, the only apparent end of the
operation being to widen very materially the solution of continuity in
the cranium. It was also resorted to in cases of compression without
fracture, with the view of discovering the effused fluid, and removing
it; but, as was already stated, it is unwarrantable in such cases; and
much more so in concussion, for which latter accident, however, it
has been occasionally performed. I met with a case some years since,
in which the patient was certainly not much benefited by such active
practice. The operation is of itself attended with danger, and likely,
236under many circumstances, to aggravate the patient’s symptoms, and
diminish his chance of recovery.
The cranium must be perforated, however, when the existence and site
of abscess under the bone is distinctly marked: and in such cases
the practitioner is much to blame if he does not give his patient a
chance of recovery by the operation: many are lost by its not being
performed, and the following case is a striking example of such
negligent practice. A young female fell from a great height amongst
some rubbish, and sustained a severe blow on the left side of the os
frontis, a considerable portion of which was thereby denuded. She
seemed to be doing well for some time; but about the eighth day after
the accident, pain in the head, with vertigo, rigors, and sickness,
febrile excitement, and a white and dry state of the bare portion of
the bone, supervened. She was depleted copiously, but notwithstanding
all the symptoms indicating formation of matter under the exposed
bone were present, the operation of trephine was deemed inadvisable.
Severe rigors continued; she became affected with spasmodic twitchings
of the muscles of the face, and stiffness of the jaw, neck, back,
and breast, and was, in short, allowed to die. On the dissection,
the dura mater below the diseased bone was found separated to a very
considerable extent, and the cavity was filled with thin purulent
matter; the abscess extended along the superior longitudinal sinus, and
communicated with this vessel through an ulcerated aperture; the canal
was filled with pus, as far as its junction with the transverse sinus,
near which point its cavity was obstructed, and the abscess limited by
a firm plug of lymph. A small abscess had formed between the bone and
pericranium, above the extensive collection within; the internal table
of the diseased bone was fractured and slightly depressed, and its
fractured edge was rough, sharp, and projecting.
But the operation may sometimes fail to prove beneficial; the brain may
have become diseased, as well as its membranes, or the patient may not
recover from the irritation caused by the abscess, and the depressing
tendency of the antiphlogistic treatment which may have been put in
force, previously to the formation of matter. But still there is a
probable chance, after the collected matter has been evacuated by the
operation, of the dura mater granulating, the cavity filling up, the
membrane becoming adherent to the cranium around the aperture, and the
patient regaining his former health and vigour.
If, after removing a portion of bone on account of symptoms of
suppuration in that situation, the dura mater be found adherent, and of
a healthy appearance, the surgeon is scarcely justified in going deeper
in search of effused fluid: the evils liable to result from wounds
of the dura mater have been already mentioned, and illustrated by an
example.
The operation of trephine must also be resorted to in cases of
punctured fracture. One perforation will generally be sufficient to
enable the surgeon to remove the detached fragments of the inner table.
In fractures with depression, when the brain is oppressed and its237
functions suspended, means must be taken to elevate the displaced
portion or portions to their natural level, and so remove the pressure.
For the accomplishment of this purpose, it may or may not be necessary
to divide the integuments. If they are entire, which is rarely the
case, a crucial incision must be made, or one in the form of the
letter T, and the flaps raised so as to show the extent of depression.
No portion of the integuments ought to be cut away; the preparatory
process of scalping, formerly in use, has been abandoned as cruel
and unnecessary. If a wound already exists, but is not sufficiently
large, it may be dilated in such a direction as appears most likely to
facilitate the after part of the proceedings. The elevation can often
be then effected by the judicious application of the lever, its point
being carefully placed under the depressed portion, and the sound
part of the bone being made the fixed point on which the instrument
acts. Those depressed portions which are completely detached, must be
removed; but those which adhere, either to the dura mater or to the
scalp, ought to be left after having been raised to their former sites,
as they will furnish a large contribution towards the filling up of the
deficient parietes. Reparation of the skull, when a small portion is
removed, or when a single narrow fracture exists, is effected by bone;
but when the opening is large, the deficiency is always repaired by
a dense ligament, to which the dura mater and integuments adhere. By
employing a small saw—represented in both ancient and modern surgical
works—so as to widen the fracture, or remove a projecting corner of
bone, sufficient room may be obtained for the introduction of the lever
and the removal of splinters. In old subjects, the bones are brittle,
and a small corner may be readily removed by pliers, or cutting
forceps, so as to allow the depression to be raised.
But it may be necessary, in order to elevate portions that are wedged
under the sound part of the cranium, to take away a considerable
portion of the latter. One or more circular pieces must be removed by
the trephine, and it may, perhaps, be necessary to cut out the parts
between these apertures by means of the straight-edged saw. The size
of the crown of the trephine must be varied according to the object
which is in view. The trepan is now disused, and the trephines best
suited to the purpose are those fluted on the side of the crown, with
the perforator made to slide and fix by means of a proper screw. The
centre pin, or perforator, is fixed on a sound and firm part of the
bone, and the edge of the crown made to project slightly over the
fractured margin. A few turns will suffice to fix the instrument. The
saw is then made to turn steadily and lightly, pressure being made when
the instrument is moving from left to right, until a pretty deep sulcus
is made. The centre pin is then withdrawn, the saw being sufficiently
retained by its own groove. The centre pin can scarcely be used at all
in children, the cranium being at that age soft and thin. I once had
occasion to operate with an old-fashioned trepan, at a distance from
town, on a child with abscess under the bone, occasioned by a punctured
wound from the point of a spinning top. The centre pin was long, very
sharp, and screwed in; and, if it had been used, would have perforated
skull, dura mater,238 and nearly half an inch of the brain, before the
saw could come in contact with the bone. I was obliged to use the crown
of the trepan, without a centre pin.
In patients at the middle period of life, a different feeling and
sound is communicated to the operator after having cut through the
outer table of the skull. Whether this change is experienced or not
after getting to some depth, he ought to proceed cautiously, moving
the saw lightly, quickly, and sharply, in the direction of the teeth,
and using no pressure. The operator should not be hurried, for he is
apt to do harm if he is; there is no inducement to make great haste,
for the patient does not suffer much, if any pain. After every two or
three turns of the saw, it is prudent to examine the track with the
flat end of a probe, or with a toothpick. If the perforation is found
to be completed at any point, then the instrument is to be inclined to
those which are undivided; and the fluted crown allows of this being
done with great facility. After the circle of bone is separated on all
sides, it is to be removed by forceps, or by means of the lever; and
the sharp points ought to be taken from the edge of the perforation by
means of the latter instrument, otherwise the dura mater may be fretted
and torn when following the natural motions of the brain. The lever
must be strong, and simple in its construction. And after a sufficient
space of bone has been removed, its point is to be introduced
cautiously under the part that requires elevation; the edge of the
sound bone at various points affords a fulcrum, and by persevering
and steady efforts, the object of the operation will be accomplished.
The dressing of the wound should be simple; the integuments are made
to cover the aperture, or as much of it as possible, and due support
is given by compress and bandage. The after-treatment must be varied,
and conducted according to circumstances. It may become necessary
to repress the granulations, or else to soothe the wound and abate
inflammatory action in the surrounding parts. Perhaps incisions may
be required, to prevent the formation of matter, and destruction of
the cellular tissue, and of the tendinous expansion, or to evacuate
fluid already secreted. The patient’s strength may require support. He
may stand in need of stimulants; or, on the contrary, the most active
means may be required to subdue vascular action, and to prevent the
evil consequences which would result to the important parts within the
cranium from such over-action.
Inflammation of the Scalp occurs either spontaneously, or in
consequence of external injury, though slight; and is generally met
with in those who have lived freely and irregularly, and are of a bad
habit of body. It is more dangerous than inflammation of any other
part of the surface, on account of the sympathy and connection which
exists between the parts affected and those situated internally:
frequently, at an early stage of the affection, delirium occurs, with
violent fever. In slight cases, in which the external surface merely
is affected, there is little swelling, and but little pain or fever.
But when all the pericranial coverings are involved, the symptoms are
uniformly severe. The swelling is elevated and puffy, and extends to
the eyelids, to the face, and, in some cases, even to the neck: the239
constitutional symptoms run high, and there is considerable risk of the
patient dying comatose. If he recover, and if the disease is little
interfered with, but allowed to take its own course, much sero-purulent
fluid is infiltrated into the cellular tissue, which generally
perishes, along with a greater or less portion of the tendinous
expansion lost by sloughing. Often, in neglected cases, a large abscess
forms, separating perhaps one-half of the scalp, and bulging over the
ear.
The constitutional treatment must vary according to the nature of
the symptoms which present themselves; in some cases they show great
vascular excitement, and in others they bear unequivocal evidence
of general debility from the first. In slight cases of the local
affection, it is sufficient to relieve the tension, and abstract blood
and effused serum by means of a few punctures, and afterwards to use
warm fomentation. More violent cases require free incision in the
direction of the fibres of the occipito-frontalis muscle, and thus only
can destruction of the parts be averted; the incision must necessarily
be deep, for the scalp is often swollen to the thickness of one or more
inches. When a depôt of matter has formed, it must be evacuated early,
otherwise there is a risk of the bone becoming extensively denuded and
exfoliation ensuing.
Chronic thickening of the Scalp is a consequence, by no means
unfrequent, of slight injuries in those of strumous habit, but may also
occur without any assignable cause. In delicate subjects it is often
attended with chronic periostitis of other bones besides those of the
cranium. The patient perhaps complains of pains about the shoulders,
in the tibiæ, femora, the tuberosities of the ischia, the sternum,
the cervical vertebræ, or in the clavicles and ribs. He cannot bear
pressure on some points without suffering the most excruciating agony.
The pain is also much increased by motion of the parts, as by coughing
when the ribs are affected. Such painful affections of parts external
to cavities are often mistaken for diseases of the internal organs, and
are treated as such by violent bleedings, purgings, and starvation,
to the still farther impairment of the patient’s constitution. The
symptoms are frequently and correctly attributed to exposure to cold
and moisture, sleeping in a damp bed, sitting with wet clothes or on
the cold ground; but such affections are very apt to occur in those
whose constitution has degenerated into that peculiar cachectic state
formerly mentioned, after mercurial courses, whether short or severe;
or in those who for some real or fancied derangement of the digestive
organs have persevered in swallowing, for months or even years, the
universal panacea of some practitioners, Plummer’s or blue pill. The
bones and their coverings, of even the best constituted, can scarcely
resist a perseverance in such a course.
The swelling of the scalp is often general, and is slightly œdematous;
some points are more elevated than others, feel soft, and are the seat
of extreme pain when pressed upon. But such affections frequently
flit from one part to another; what was most unsound, at one time,
recovering itself, and painful swellings attacking that240 which was
comparatively free of disease. The same holds true in regard to the
other bones at the commencement of the affection; but when much change
of structure takes place, then the pain and swelling become fixed. The
pains are most severe during the night, being then so violent as to
deprive the patient of rest, and even prevent him from placing his head
on the pillow: they abate towards morning, and remain tolerable during
the day. They are always aggravated by change in the atmosphere from
dryness to moisture, and the prevalence of easterly winds is peculiarly
distressing to patients afflicted with such diseases. The swelling
is composed of thickened and vascular periosteum with œdematous
integuments. The bone too is often increased in size, and condensed,
from continuance of increased vascular action; and its surface is
roughened in consequence of its texture being opened out, and new bone
having been deposited. Death of portions of the bone often follows,
either spontaneously, or after slight bruises received during the
continuance of the disease. A few accidental blows on the head, and a
perseverance in the use of mercurial alteratives for a series of years,
gave rise to the state of matters represented in the accompanying
illustrations. The large dead portion represented was removed some
months before death. Here the deficiency in the cranial bones is partly
owing to ulceration, partly to death of portions of them. The patient’s

 health becomes undermined by want of sleep and continual suffering; and
he may at the same time have relaxation of the mucous surfaces, with
increased discharge from them, produced by the same cause as occasioned
the affection of the coverings of the bones. He may be subject to a
relaxed or ulcerated state of the throat, increased or caused by the
slightest exposure; and may have hemorrhage from the nostrils, copious
expectoration, mucous stools, &c. The periosteal affection alone is a
troublesome and serious complaint.
health becomes undermined by want of sleep and continual suffering; and
he may at the same time have relaxation of the mucous surfaces, with
increased discharge from them, produced by the same cause as occasioned
the affection of the coverings of the bones. He may be subject to a
relaxed or ulcerated state of the throat, increased or caused by the
slightest exposure; and may have hemorrhage from the nostrils, copious
expectoration, mucous stools, &c. The periosteal affection alone is a
troublesome and serious complaint.
When the pains are fixed and violent, we are sometimes obliged to
give small doses of the bichloridum hydrargyri at first, even though
there is reason to think that mercurial medicines, perhaps imprudently
or carelessly administered, have brought the constitution into241 its
present morbid condition. The good effects of this medicine are well
marked and speedy. The patient is freed from the nocturnal pain, gains
flesh, and the swellings subside. It ought not to be resorted to,
however, unless in severe cases, when the disease cannot otherwise be
successfully combated; and when used, it should not be continued longer
than is necessary for the removal of the more urgent symptoms: when the
pains begin to yield, it is time to discontinue the medicine. Great
care is necessary on the part of the patient; he must industriously
avoid exposure to moist atmosphere, and ought to be well and warmly
clothed, wearing flannel, chamois leather, or both, on the trunk and
extremities. A patient treated with the corrosive sublimate of mercury
is perhaps more subject to recurrence of the affection, after imprudent
exposure, for a considerable time afterwards, than if simple and less
powerful means had been employed. A cure can often be effected by the
exhibition of the compound decoction of the woods, with or without
antimony. Moderate diet and strict abstinence from wine and other
internal stimulants should be enjoined; the patient, soon experiencing
the good effects of temperance, is exceedingly willing to restrict
himself to a somewhat antiphlogistic regimen.
In cases of violent fixed pains, with swelling and threatening of
matter forming, incision may be sometimes practised with relief to the
patient, but is not to be had recourse to unless there is a risk of the
bone suffering. Local abstraction of blood is advantageous, and may,
if necessary, be followed by counter-irritation, as the application of
blisters or sinapisms. Friction with stimulating substances, or with
opiate liniments, is often useful when the disease begins to yield,
the pain and puffiness of the parts being thereby dispelled. The hair
should be kept short during the cure, and ought not to be allowed to
grow till the scalp is firm and sound.
The disease is often so far advanced that, in spite of the most active
treatment, abscess forms in one or more points; and, on the matter
being evacuated, the bone is found denuded. Exfoliation is then very
likely to take place.
Exfoliation generally follows denudation of the bone by accident, but
not uniformly. When the periosteum is stripped off by violent injury,
the bone in some cases does not lose its natural colour; granulations
arise from the exposed part, and it again becomes covered without any
part of its substance having been destroyed. Again, careful removal
of the periosteal covering, as in excising a tumour or ulcer by the
knife, may be followed by death of the outer table of the skull; small
portions only separating in some cases, whilst in others a large part
of the bone, and of considerable thickness, perishes. The cranial
bones may in part become dead throughout their entire thickness,
and separate, either after a severe bruise, or in consequence of
inflammatory action following injury or arising from disease. The
process of separation is either speedy or tedious, according to the
vigour of the constitution. The deficiency is repaired, in a great
measure, from the subjacent bone, when its whole thickness is not
thrown off. But when the breach is complete, the surrounding parts
assume the reparative action; the granulations from the dura242 mater and
integuments coalesce, and a dense membrane fills up the space.
The denuded bone should be kept covered and moist, and for this
purpose lint frequently wetted with tepid water is the best dressing:
spirituous or greasy applications can do no good. A free discharge
for the matter should be afforded, and the wound kept clean. If the
exfoliation goes on slowly, perforation in the dead bone may be made at
different points down to the living parts, with the view of expediting
the process. Exfoliations are sometimes retained by surrounding
granulations overlapping their edges and confining them in their
situation; or are fixed by atmospheric pressure, after separation has
taken place from the parts underneath by the action of the absorbents,
in the same way as a boy’s leathern sucker becomes firmly fastened
to the stone to which it is applied. In such circumstances a small
screw may be fixed into a perforation carefully made in the bone,
and thus the dead part may be lifted out without pain or difficulty,
when otherwise it might have lain for many weeks, keeping up the
discharge. In this way the large sequestrum, represented at p. 240, was
extracted from its bed. The powdered red precipitate of mercury may
be occasionally sprinkled on the parts surrounding the dead portion,
in order that the granulations embracing it may be destroyed, and the
part more completely detached. The general health must be all along
carefully attended to. Sarsaparilla with guaiac, sassafras, mezereon,
&c., is often useful, more especially if pains in other parts continue
to annoy the patient. Under such medicines he in general improves very
rapidly in appetite, flesh, and strength.
The scalp is sometimes, though rarely, the seat of malignant ulcer.
In the early stage the ulceration is not of great extent, and affects
only the soft parts; perhaps it is confined at first to the common
integument, but is extremely apt to extend to the deeper layers which
invest the cranium, and even to the bone itself. It is by no means
uncommon to find the cranium very extensively diseased, though the
affection originated in the superimposed soft parts. Such ulceration of
the bone is of a peculiarly destructive nature; it is a disease of the
osseous tissue, corresponding to the most malignant ulceration of the
soft parts. The bone around the ulcerated cavity is spongy and soft,
its margin is irregular, and bristles with numerous spiculæ; the centre
is composed of soft morbid deposit, entangling small portions of bone
which have become detached, and flabby, almost lifeless granulations
shoot from the distempered mass. Such disease, when the patient does
not soon succumb to its virulence, advances to a frightful extent,
affecting a large surface, destroying the whole thickness of the bone,
and even exposing the internal parts. In a case of this description,
which occurred in the Royal Infirmary under my care, the anterior half
of the cranium was totally destroyed, the left orbit contained a putrid
mass, consisting of the disorganised eye mixed with pus and bloody
fluid; the dura mater was exposed, and sloughed at several points,
and the unhealthy discharge from the parts lodged on the surface of
the brain. In malignant diseases of scalp, as of other parts, the
lymphatics become secondarily affected: the absorbents feel hard and
thickened, the glands in the neighbourhood en243large and ulcerate,
and the sore thereby formed soon assumes the characters of decided
malignancy,—hard everted edges, an angry surface, and fetid thin
discharge.
Before the disease has become very extensive in the scalp, and when
it is still limited to the superficial parts, it may be removed by
the knife; the incisions being made at a considerable distance from
the margins of the ulcer, so that those parts which may be supposed
to have assumed a disposition to malignant action, may be taken away
along with the ulcer. In more advanced cases, it may be necessary
that the incisions should extend in depth to the bone; and it may
be prudent to insist on a portion of the bone exfoliating, the
periosteum being removed, and some potential cautery applied to the
exposed surface,—as the alumen ustum, oxydum hydrargyri rubrum, &c.
The actual cautery cannot be applied with safety to the cranium. Even
where the integuments only are removed, and that to a small extent,
and in a proper form, it is vain to think of approximating the parts
and procuring union by adhesion; the wound must granulate. There is
no difficulty in suppressing hemorrhage; either ligature or temporary
pressure may be employed according to circumstances. Mild dressings
are to be applied, and proper support afforded. The parts should be
kept clean, and for that purpose the surrounding scalp must be shaved
repeatedly.
Tumours of the Scalp.—Tumours of a sarcomatous nature are seldom
met with in this situation, but the adipose are not so unfrequent.
The latter are easily removed, being seldom of large size, and their
attachments being loose, unless when they have been irritated by
accident or maltreatment. When sarcomatous growths do occur, they are
to be excised, with those precautions which were formerly mentioned
when treating of tumours generally.
Vascular growths not unfrequently form in the scalp, and attain
considerable size; in general they are either congenital, or the
degenerations of nævi materni. They may be so extensive as to forbid
surgical interference; or they may be so indolent, may partake so much
of the nature of simple varix, as not to warrant it. If small, they
can be readily removed by the knife, the incisions being made rapidly,
and wide of the diseased structure. If the tumour be prominent,
extensive, and at all active, the employment of ligature is a more
safe and equally effectual practice. One or two ligatures may suffice
to encircle the swelling, or, as in other parts of the body, it
maybe necessary to pass a great many double ones beneath the part,
to separate their extremities, and to tie them to each other around
the base of the tumour, the last being drawn so as to tighten all the
others. Little benefit can be expected from tying, either at once or
at different periods, the larger arterial trunks whose ramifications
supply the diseased structure, the inosculation amongst the vessels
around the tumour being so extremely free. But, in cases where the
disease cannot be otherwise combated with any hope of success, ligature
of the common carotid, on the affected side, may be tried as a last
resource. The practice has proved successful in some cases of this
disease, involving parts of the head and face to such an extent, or in
such a situation, as to forbid any attempt at removal of the growth.
244
Encysted tumours frequently form in the scalp, and, if undisturbed,
become large; they seldom occur singly. The disease appears in many
cases to be hereditary, and it frequently happens that several members
of one family are at the same time afflicted with it. The contents of
the tumours vary as to consistence, but are generally atheromatous.
The cyst is thick, and loosely connected with the surrounding cellular
tissue; but as the tumour increases, the adhesions often become firm
and intimate, more especially towards the skin. When the tumour is
of small size, it is unnecessary to adopt any preparatory measures
for its removal, not even to shave the scalp: the surface may be
cleared a little with scissors. The swelling is transfixed, in the
direction of the fibres of the occipito frontalis, by means of a curved
sharp-pointed bistoury, and its internal structure is exposed by the
knife being carried outwards. The soft contents are evacuated, and
the sac is easily extracted by means of common dissecting forceps.
The integuments are then laid down and retained in apposition, no
sutures being necessary, and in many cases the wound heals by adhesion;
sometimes a small coagulum forms between the edges of the wound, and
is detached some days afterwards; then slight suppuration ensues.
In larger tumours, however, a straight and narrow knife is perhaps
the most convenient instrument for accomplishing removal. The part
is transfixed, and in most cases it is necessary to take away an
elliptical portion of the integuments, a part of the cyst corresponding
to which is of course simultaneously removed; the remainder of the sac
is pulled out by the forceps. If the adhesions at certain points are
firm, they may be touched with the extremity of the knife, so as to
expedite the extraction; and if after the operation there is reason
to believe that the whole of the secreting surface has not been taken
away, a pointed piece of caustic potass may be applied to the suspected
parts. If the tumour is very large, the cyst can often be removed
without difficulty unopened, sufficient integument being left to cover
the exposed surface. In consequence of such operations on the scalp,
erysipelas often supervenes, and precautions ought therefore to be
adopted to prevent its occurrence, by a little preparation beforehand,
by keeping the patient’s bowels freely open, confining him to moderate
and mild diet, and avoiding exposure to moist atmosphere and easterly
winds.
Osseous tumours of the cranium seldom attain any great size, and are in
general neither troublesome nor dangerous. Small ivory exostoses are
the tumours most frequently met with in this situation, and require no
treatment whatever.
Tumours of malignant character occur, though rarely; commencing either
in the diploe of the skull or on the surface of the dura mater, soon
enlarging, and involving the parts around. Two or more sometimes form
in one patient; they are attended with excruciating pain, and rapid
destruction of the bone, and are followed by extinction of life either
at an early or remote period. They are entirely beyond the reach of
surgery; as are also those tumours, occasionally met with in children,
which project through the cranial sutures and contain fluid; such are
analogous to the disease named spina bifida, hereafter to be spoken of.
245
I may here remark, that puncture of the brain, with the view of
abstracting fluid in chronic hydrocephalus, is an operation not often
likely to be followed by success, and it may even accelerate the
fatal issue. Some cases are recorded in which benefit is said to have
arisen from the practice. Pressure was applied and kept up after the
evacuation of the fluid.
DISEASES OF THE EYE AND ITS APPENDAGES.
Of Inflammation and Abscess of the Lachrymal Passages.—In former
times, all affections of the lachrymal passages, and of the parts in
the neighbourhood, were denominated fistula lachrymalis, and were all
treated nearly in the same manner, by opening the sac, and inserting
probes, knives, terebræ, scalpra, caustics, and red-hot irons; the
anatomy of the various parts being then ill understood, and the
opinions as to the origin and nature of the diseases being founded on
erroneous theories regarding the defluxion of acrid humours, formation
of imposthumes, fungous growths, &c. The term, however, which was
indiscriminately applied to all diseases in the inner corner of the
eye, accompanied with derangement of the lachrymal secretion, is now
confined to a distinct form of disease, as will afterwards be mentioned.
Inflammation sometimes occurs in the loose cellular tissue covering the
lachrymal sac,—whilst that cavity remains free of all disease,—and is
attended with some obstructions to the passage of the tears in their
natural course, on account of the eyelids becoming swollen, from an
extension of the inflammation. The morbid action resembles erysipelas
in its nature, and usually terminates in unhealthy suppurations; thin
purulent matter lodges in the opened out cellular membrane, a soft
boggy tumour is formed, and the superimposed integuments become of a
bluish colour, as in the case of other scrofulous collections.
Though the affection is at first unconnected with the lachrymal sac,
this organ may ultimately be involved. It may become the seat of a like
unhealthy inflammation, and matter may consequently form within its
cavity; or, on account of the pressure of interstitial deposit around,
the parietes of the sac may ulcerate before the abscess of the cellular
tissue in front has discharged externally. Thus, the cavities of the
lachrymal sac, and of the external abscess, will communicate with each
other. If, after an external aperture has been made either by nature or
by art, any doubt exist as to whether the sac is involved or not, such
doubt will soon be removed by dexterous use of the probe.
In the treatment of this affection, it will be necessary, at the
commencement, as in all other local inflammatory diseases, to attempt
the accomplishment of resolution, by attention to the general health,
local abstraction of blood, and warm fomentations. When matter246 has
formed, it ought to be evacuated as soon as possible by a small
incision, as there will then be less risk of the deeper parts becoming
secondarily affected; or if the integuments have sloughed, and the
matter has been discharged spontaneously, the natural opening may be
enlarged either with the knife, or with the caustic potass. If it be
discovered that the lachrymal sac is opened into, the same treatment is
necessary as if it remained entire; the matter is to be allowed free
exit, and granulation encouraged; in most cases, the aperture in the
sac is soon repaired, and the parts heal as quickly and soundly as if
the disease had been confined to the external cellular tissue. Light
dressing during the cure, preferable in all cases, is more especially
necessary in this situation.
Of Inflammation of the Lachrymal Sac.—When the lachrymal sac becomes
inflamed, it enlarges considerably; the swelling is small, hard,
circumscribed, deeply seated, and extremely painful, more especially on
pressure. At first the integuments are of their natural appearance, the
increased action being confined to the sac, but they are soon involved,
and often to a considerable extent; they become red and swollen, and
as the surrounding parts are affected, the swelling increases. In some
cases, the eyelids, the caruncle, and the conjunctival covering of
the eye, participate in the inflammatory action. The inflammation is
in most instances caused, or at least preceded, by some obstruction
in the nasal duct, in consequence of which, the tears are interrupted
in their natural course downwards, and either accumulate in, and
distend the sac, or flow over on the cheek, the puncta lachrymalia
remaining open. After increased vascular action has been produced,
the lachrymal secretion is increased to a greater or less degree, and
much inconvenience is caused to the patient by the profuse discharge
following an unnatural course. When inflammation is intense, lymph is
effused into the passages, producing obstruction sometimes complete.
The mucous lining of the nasal duct becomes swollen, from the vascular
excitement, either throughout its whole extent, or at one point only;
and in either case the flow of the tears must be interrupted, either
partially or wholly, according to the degree of swelling. The vitiated
secretion of the part may also contribute towards narrowing the canal,
by lodging and concreting there. But a more complete and permanent
obstruction is formed by effusion of lymph, under or on the mucous
lining, as happens in other canals of similar construction: and in this
case also, the stricture may be partial or complete, according to the
quantity of effused matter, and the extent of surface affected.
As the inflammation abates, mucous fluid is copiously effused from
the surface of the sac, and the swelling increases, though the pain
is less. The collected fluid may be partially evacuated through
the puncta, either spontaneously, or in consequence of the patient
instinctively pressing with his finger on the swollen part; or the
puncta may be obstructed by the same causes as the nasal duct, and
then the discharge of the fluid is prevented in both directions; it
consequently accumulates still more, and causes greater bulging.
Fluctuation is perceptible, and the collection protrudes outwards and
forwards, being least resisted in these directions. It is seldom that
the247 puncta are obstructed, and consequently the swelling does not
attain any great size, the sac being relieved by some of its contents
always flowing upwards, after a certain degree of distension. As the
inflammation farther subsides, the mucous secretion diminishes, and
the accumulation and swelling are less: in fact, the patient may at
this period prevent a tumour from forming in the corner of his eye, by
from time to time pressing gently on the sac, and forcing the lachrymal
secretion upwards, as it begins to accumulate. This state of matters
may continue for a long period, without causing much inconvenience,
and getting neither better nor worse; the patient is merely obliged to
apply his finger and handkerchief more frequently to his eye than would
otherwise be required. In almost all cases, the obstruction of the
nasal duct is complete, or nearly so, and consequently the fluid cannot
pass downwards into the nose, though it may occasionally appear to do
so, on account of the discharge from the Schneiderian membrane being
increased at the same time with that of the lachrymal sac. The ductus
ad narem, though wide in the skeleton, is of very limited dimensions
in the living body, and is in consequence readily made impermeable to
mucous fluid, by even slight thickening of its lining membrane.
It has been already observed that the above-mentioned condition of
the parts may continue for a considerable period; but in other cases
purulent matter soon forms within the distended sac; or, at least, the
contents of that organ are so altered in colour and consistence as to
resemble intimately purulent fluid. The secretion may or may not be
pus, probably it is not in some cases; but as the decision of this
point is practically unimportant, the description of it as purulent
can scarcely be objected to. In most cases, when the puncta either are
or become clear, no suppuration, or deterioration of mucus into fluid
like pus, occurs; merely chronic distension of the sac continues, the
patient being able to avert incited action, by occasionally squeezing
out the contents, and thereby removing tension. There is merely an
Epiphora; or, as it is otherwise called, Blenorrhœa, or Stillicidium
lachrymarum. The last term is by some applied to increased lachrymal
secretion, without affection of the sac, the tears being secreted more
quickly than the puncta can carry them away, and consequently running
over on the cheeks, excoriating the surface, and producing an irritable
condition of the eye. The simple epiphora may be of long duration,
yet the parts are extremely liable to assume inordinate action, in
consequence of slight injury, or exposure to cold; thus suppuration
will ensue.
When purulent matter forms, fluctuation becomes more distinct, the pain
increases, and there is slight headache and fever. The integuments
inflame more and more, and, if the case is neglected, ultimately
give way by sloughing. A small ragged opening, often indirect, is
formed, and the contents of the sac are not thereby all discharged;
the thinner fluid only escaping, whilst the more viscid remains and
clogs the aperture. The swelling is not much diminished; the margins
of the aperture thicken, become indurated, and contract, the purulent
contents of the sac are gradually discharged, and the tears afterwards
flow through the opening. The parts are248 now in that condition to
which the term Fistula lachrymalis is with propriety applied. The
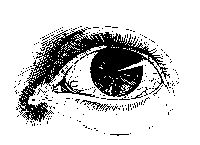 swelling of the canal may gradually subside, the tears resume their
wonted course, and the opening may then contract, and the parts
cicatrise; but frequently the fistula remains open for a long period,
gradually diminishing in diameter, and only a small passage, almost
imperceptible, ultimately remaining, through which a few drops of
lachrymal fluid are occasionally discharged. Sometimes the fistula
closes entirely without the obstruction of the nasal duct having been
removed, and the lachrymal sac remains in consequence distended; then
the tears or mucus, either clear or turbid, can generally be squeezed
through the puncta.
swelling of the canal may gradually subside, the tears resume their
wonted course, and the opening may then contract, and the parts
cicatrise; but frequently the fistula remains open for a long period,
gradually diminishing in diameter, and only a small passage, almost
imperceptible, ultimately remaining, through which a few drops of
lachrymal fluid are occasionally discharged. Sometimes the fistula
closes entirely without the obstruction of the nasal duct having been
removed, and the lachrymal sac remains in consequence distended; then
the tears or mucus, either clear or turbid, can generally be squeezed
through the puncta.
It frequently happens that the meibomian glands are the seat of morbid
action, along with the lachrymal passages; their secretion is changed,
becoming in some cases thick and caseous, in others puriform. By some,
affection of the meibomian glands has been considered as the cause of
inflammation and abscess of the lachrymal sac. This opinion, however,
cannot be agreed to, for the diseases are not always coexistent; and
besides, the affection of the surface of the lachrymal sac and ductus
ad narem is as likely to be the consequence of morbid action, extending
upwards from the nostrils, as of morbid secretion from the eyelids
blocking up and irritating the puncta and the lachrymal passages.
Disease of the meibomian glands in the under eyelid often exists along
with disease of the lachrymal passages, but the latter is generally the
primary affection; the conjunctival covering of the eyelid is at the
same time inflamed, swollen, and often granulated.
In some cases of abscess in the lachrymal sac, before the integuments
give way, the subjacent bone becomes diseased in consequence of the
pressure of the confined matter; portions are affected by necrosis,
and after their separation considerable deformity is produced. The
exfoliation is often very tedious, and is attended with discharge
of fetid thin fluid from the nostril, and from the ill-conditioned
lachrymal fistula.
Fistula lachrymalis is often merely one of the symptoms of disease
in the bones of the nose, with obstruction of the nasal duct,—as in
patients who have suffered from mercury.
Treatment.—In the treatment of epiphora or blenorrhœa—that is,
chronic collection of a mucous fluid in the lachrymal sac, with weeping
of the eye—a primary object of attention is the state of the general
health. The habit of the patient will commonly be found weak, and, if
not decidedly strumous, at least inclining towards that diathesis. In
such cases the digestive organs must, if possible, be brought into a
vigorous state by tonics and nourishing regimen. The local treatment
chiefly consists in applying stimulants to the internal surfaces of the
palpebræ and lachrymal sac. For this purpose, solutions of stimulating
and astringent substances, termed collyria,249 and various ointments, are
employed. At first they ought to be used of rather a mild nature, and
their stimulating power must be afterwards increased gradually. The
applications are placed between the eyelids, and, becoming mixed with
the natural secretion, pervade the diseased surfaces; and, being taken
up by the puncta lachrymalia, are afterwards conveyed into the sac. It
was formerly the custom to inject the fluids into the sac; but this
is unnecessary so long as the puncta and canaliculi remain pervious,
and the permeability of these can be readily ascertained by means of a
small probe. Permanent pressure on the sac can be productive of no good
effect, and is extremely liable to do harm. The repeated application of
very small blisters over the sac has been found useful.
Introducing minute gold probes through the puncta has been much
recommended, but in the generality of cases can be of little service.
The probes are too limber for removing mechanical obstruction, or for
affecting in any way the contracted or strictured duct. But passing
of the probe may tend to remove the irritability of the passage,
as happens in the urethra, and thence some relief may follow. Much
dexterity is required in using either the probe or syringe. The puncta
are often very small, and it is in general necessary to dilate them by
means of the point of a common pin, before any instrument can be passed
through them into the sac. The point of the probe being introduced
into the punctum, either superior or inferior, must first be carried
towards the nose for about 2-10ths of an inch, the instrument being
lightly held betwixt the fore and middle fingers of the right hand. It
is then directed downwards and backwards. Care must be taken to prevent
entanglement in folds of the membrane. Should obstruction be felt, the
instrument is withdrawn a little, and then carefully and gently carried
in the right direction. The small syringe is managed with one hand,
whilst, with the forefinger of the other, the punctum not occupied by
the pipe is compressed.
Neither can much or any benefit be expected to follow attempts to force
obstruction in the lachrymal passages, by the weight of a column of
mercury. A plan of dilating and rectifying the nasal duct by styles
introduced through the puncta has been proposed, but scarcely deserves
to be mentioned as a means of cure.
When suppuration is threatened, with increase of the swelling,
inability of the patient to empty the sac by pressure, redness of the
integuments, &c., an early opening should be made into the tumour, in
order to prevent further and more serious mischief. A small opening
into the sac cannot be productive of so much injury as forcible
dilatation of the canaliculi, followed by and causing ulceration. The
point of a straight narrow bistoury is to be entered into the sac,
and carried on into the nasal duct, the knife being pushed downwards,
backwards, and a little inwards, in the direction of that passage. The
point to be punctured can always be readily ascertained by feeling for
the firm ligament which attaches the orbicularis palpebrarum to the
nasal process of the superior maxillary bone, as the upper orifice
of the ductus ad narem is situated immediately below this tendon; by
introducing the knife below the ligament, and250 within the sharp edge
of the orbit, and then carrying it forward in the direction already
mentioned, the surgeon cannot fail to enter the nasal duct. The knife
should be followed by a probe, and ought not to be entirely withdrawn
till the probe is fairly lodged in the duct, otherwise the surgeon will
experience much difficulty in the after proceedings. If the knife be
not pushed into the duct, a blunt instrument can scarcely be introduced
afterwards. Some force is required, but is not hurtful, provided it be
made in the proper direction, so as to remove the obstruction in the
duct without injuring the bones and other parts in the neighbourhood.
After the operation, some drops of blood should escape from the
corresponding nostril, showing that it has fairly entered this passage;
or the patient being made to expire forcibly, the nostrils being at the
same time compressed with the fingers, air, blood, and mucus are forced
upwards through the opening made.
Many and various modes have been pursued with a view of securing a
pervious state of the nasal duct. Instruments of different kinds have
been introduced through the puncta, through the opening in the sac,
and through the termination of the duct under the spongy bone, and
have been retained for a longer or shorter period, according to the
fancy, or theory, or plan of the surgeon. The first of the methods
of introduction is abandoned, as already stated. By the ancients the
passages in fault were got rid of altogether, being either cauterised
or destroyed by escharotics.
The passing of probes into the duct from its lower aperture is useful
in removing trifling obstructions caused by concretion of deteriorated
mucus, or slight thickening of the lining membrane, and in chronic
dilatation of the sac with probable contraction of the duct. But, at
the same time, it is an operation requiring much dexterity, and which
ought not to be attempted till after much practice on the dead body.
The first introduction of the instrument is always the most difficult,
from obstruction by a valvular projection of the membrane at the lower
orifice, the use of which in the healthy state of the parts must be
apparent. Destruction of it renders after-introduction of instruments
much more easy.
But the preferable practice is making an opening into the sac, and
then introducing instruments from the upper orifice of the duct; more
especially in cases where the swelling and pain are considerable.
The instruments employed for dilatation of the passage are tubes and
styles. The tubes are made either of silver or gold, of equal calibre
throughout, and of the same length as the passage. For some time
after their introduction they cause much irritation; this gradually
diminishes, and the wound heals over them. But, according to my
experience, the effects are not satisfactory. The irritation which
they at first occasion generally subsides, but abscess again occurs,
with much swelling, and it becomes necessary to remove the foreign
body. Again, the tube sometimes becomes obstructed by thickening and
concretion of the discharge, and then, when it is necessary to remove
it, the process is found to be by no means an easy one; a free incision
is required; a screw must be fastened into the tube, or, when that
cannot be accomplished, the foreign body must be laid firmly251 hold of
with strong forceps; altogether the extraction is very painful, and
often extremely tedious. In short, the practice of introducing tubes
does not appear to be founded on sound surgical principles.
After extensive and impartial trial of both the tubes and style, I
decidedly prefer the use of the latter. On the point of the bistoury
being fairly lodged in the lachrymal duct, a probe is passed along it;
the knife is then withdrawn, and the passage is gently dilated by the
probe. The probe again is followed by the style, which should be made
of silver, of the same thickness throughout, of the same length as the
duct, and with a flattened head placed obliquely to the body of the
style. The size of the style should be at first small, and gradually
increased. The irritation caused by the first introduction is in many
cases very severe, but the parts soon accommodate themselves to the
presence of the foreign body; the pain and swelling diminish, as also
the discharge. If a large style be pushed forcibly in at first, violent
inflammatory action will ensue, and much mischief may be produced.
After irritation has gone off, the tears pass readily down in the
nose by the sides of the style, according to the laws of capillary
attraction, little or no fluid escapes from the external opening, the
wound contracts around the instrument, and, its head being covered with
black wax, no deformity is produced. The instrument should be removed
from time to time, cleaned, and replaced. When, by the continued use of
styles gradually increased in size, the duct has been dilated to its
full extent, and appears restored to a sound condition, the instrument
may be withdrawn, and afterwards introduced only occasionally. The
external aperture, which has become fistulous from the long presence
of the foreign body, then begins to contract, and, on its completely
closing, the tears continue to follow their usual course, and the
disease is overcome. But sometimes a small fistulous aperture remains,
and there appears to be a disposition towards the renewal of the
affection; in such a case, a small style, not exceeding a thin gold
probe in diameter, should be introduced every evening, and retained for
some hours: this causes little or no inconvenience to the patient, and
insures the permeability of the canal.
Such is the method by which a permanent cure may often be obtained, and
which, in my opinion, is preferable to the use of tubes. If these are
to be employed, they should, as already mentioned, be nearly of equal
calibre throughout; the external opening must not be allowed to close
for a considerable time after the introduction of the instrument; and
the tube must be kept pervious for some time by a style introduced
through it. But by these means, which are essential for the success of
the practice, the main advantage arising from the use of a tube, viz.,
little irritation being produced at first, and the parts being allowed
to close soon over it, are completely done away with.
The practice of perforating the os unguis never can be required; it is
cruel, unnecessary, and unsurgical.
Sometimes the lachrymal passages are entirely destroyed. In such cases,
it has been found that no great inconvenience arises from their252
obliteration, as the lachrymal gland ceases, in a great measure, to
secrete fluid, and the conjunctival secretion, after having performed
its office, evaporates from the surface. In truth, the lachrymal gland
always enjoys long periods of repose, and is only called into active
exercise of its functions occasionally, as the eye in its ordinary
condition is sufficiently lubricated by secretion from its conjunctival
covering.
The treatment of fistula lachrymalis, as has been well remarked
by an eminent author, must be varied and regulated according to
circumstances;—by the degree of obstruction in the duct, by the state
of the coverings of the sac, of the sac itself, and of the subjacent
bone, and by the general state and habit of the patient.
Encanthis is a tumour situated in the corner of the eye. The
caruncula lachrymalis appears to be the original seat of the disease,
at least it is involved at an early period. The growth is at first
 small, and appears to be simple enlargement of the caruncle: it is of a
reddish colour, and its surface is studded with numerous granulations.
It often attains a very considerable size; and, on account of its
propinquity to the lachrymal passages, is accompanied with watering of
the eye, the puncta being either involved in the growth, or compressed
or displaced by it. Sometimes the whole inner corner of the eye,
from the margin of the cornea to the inner junction of the eyelids,
is occupied by the granulated swelling; and in such cases it is not
uncommon for the tumour to extend itself outwards, in the form of
a lunated appendage, on the under surface of each lid; thereby the
motions and functions of the ball are much impeded, and a prominent
deformity is occasioned. In most instances the growth seems to be
a simple enlargement of structure, and is of a benign nature; but
sometimes it is firm, hard, of rather a livid hue, with a smooth slimy
surface, and is decidedly malignant,—enlarging, and gradually involving
the surrounding parts.
small, and appears to be simple enlargement of the caruncle: it is of a
reddish colour, and its surface is studded with numerous granulations.
It often attains a very considerable size; and, on account of its
propinquity to the lachrymal passages, is accompanied with watering of
the eye, the puncta being either involved in the growth, or compressed
or displaced by it. Sometimes the whole inner corner of the eye,
from the margin of the cornea to the inner junction of the eyelids,
is occupied by the granulated swelling; and in such cases it is not
uncommon for the tumour to extend itself outwards, in the form of
a lunated appendage, on the under surface of each lid; thereby the
motions and functions of the ball are much impeded, and a prominent
deformity is occasioned. In most instances the growth seems to be
a simple enlargement of structure, and is of a benign nature; but
sometimes it is firm, hard, of rather a livid hue, with a smooth slimy
surface, and is decidedly malignant,—enlarging, and gradually involving
the surrounding parts.
Cancerous ulceration, attacking and destroying the eyelids, and the
parts around the ball of the eye, often commences in the situation
of the caruncle, or in a wart on the edge of the lid. Cancer, though
a rare and uncommon disease of the eyeball, frequently seizes on the
appendages of the eye, extending rapidly in all directions, and often
completely detaching the ball by ulceration. Warty tumours also occur
on the conjunctiva of the lids, or of the ball, and are inconvenient as
a source of much irritation to the neighbouring parts, even though of a
benign nature in themselves.
Extirpation, by means of a small pointed knife, or curved scissors, is
the only means to be relied on for the cure of such warty tumours, and
of encanthis. The growth must be fixed and pulled outwards with a small
hook, and carefully dissected away; the eyelids, and, if necessary,
the ball of the eye, being kept fixed with the fingers, or by means of
a speculum: the fingers are generally sufficient, and more convenient
than any instrument. If from the appearance of the parts,253 and from
induration surrounding the tumour, malignant action has evidently
taken place or is dreaded, then the incisions must be made wide of the
base of the swelling. For malignant, open, and extensive ulcerations,
nothing can be done farther than to allay the pain, and soothe the
constitutional disturbance. On the whole, encanthis is a rare disease;
however, I have seen, and operated on, several instances of it.
Encysted Tumours of the Eyelids.—These occur beneath the conjunctival
lining of either the upper or under lid, but most frequently in the
former. They form rapidly, but seldom attain any very considerable
size; and may be found to contain, along with glairy fluid, a mixture
of pus, or curdy matter. The contents, however, are generally glairy,
rarely atheromatous. The cysts are very thin and adherent, and the
tumour projects externally, forming a dusky red elevation of the
integuments. They cause considerable deformity, watering of the
eye, and stiffness and difficulty in moving the lids. On everting
 the eyelid, the contents of the tumour are seen shining through the
distended conjunctiva, and present a bluish appearance. They are seldom
single, and are not remediable but by operation. It is improper to
attempt their extirpation from without, as there is a certainty of
cutting completely through the eyelid, the inner covering of the cyst
being merely attenuated conjunctiva. The lid is to be everted, and
an incision made into the prominent and thin cyst with the point of
a cataract knife; the contents can then be readily scooped out with
the end of a probe. It is impossible to dissect out the tender cyst
entire, and, when this is attempted, the cure can seldom be permanent.
If, after incision and discharge of the contents, nothing farther is
done, the disease will almost certainly return, in consequence of the
remaining cyst reassuming a secreting action. The only effectual and
radical cure is the application of a finely-pointed piece of caustic
potass to the interior of the cyst, after discharge of the contents and
cessation of bleeding. The cyst is thereby completely destroyed. A slip
of soft lint, dipped in oil, is interposed betwixt the lid and eyeball,
for an hour or two, in order to protect that delicate organ from the
caustic. The wound suppurates and heals kindly, and no mark is visible,
the incision having been made from within. I have had no instance of
return of the disease since adopting this practice; and I have operated
on many which had been previously treated by other and ineffectual
means. The laceration of the cyst with a pointed probe is sometimes
followed by a permanent cure, but it cannot be depended upon.
the eyelid, the contents of the tumour are seen shining through the
distended conjunctiva, and present a bluish appearance. They are seldom
single, and are not remediable but by operation. It is improper to
attempt their extirpation from without, as there is a certainty of
cutting completely through the eyelid, the inner covering of the cyst
being merely attenuated conjunctiva. The lid is to be everted, and
an incision made into the prominent and thin cyst with the point of
a cataract knife; the contents can then be readily scooped out with
the end of a probe. It is impossible to dissect out the tender cyst
entire, and, when this is attempted, the cure can seldom be permanent.
If, after incision and discharge of the contents, nothing farther is
done, the disease will almost certainly return, in consequence of the
remaining cyst reassuming a secreting action. The only effectual and
radical cure is the application of a finely-pointed piece of caustic
potass to the interior of the cyst, after discharge of the contents and
cessation of bleeding. The cyst is thereby completely destroyed. A slip
of soft lint, dipped in oil, is interposed betwixt the lid and eyeball,
for an hour or two, in order to protect that delicate organ from the
caustic. The wound suppurates and heals kindly, and no mark is visible,
the incision having been made from within. I have had no instance of
return of the disease since adopting this practice; and I have operated
on many which had been previously treated by other and ineffectual
means. The laceration of the cyst with a pointed probe is sometimes
followed by a permanent cure, but it cannot be depended upon.
Closure of the Eyelids may be either congenital, or a consequence
of injuries, as burns of the parts. The closure may be complete or
partial. In general it is partial, though perhaps extensive; and the
adhesions can be readily separated by the point of a knife, or small254
probe having been previously introduced beneath; or a small and narrow
probe-pointed bistoury may be conveniently used for the purpose. In the
after-treatment means must, of course, be taken to prevent the lids
from again adhering.
Ectropion, or eversion of the eyelids, may be produced, merely by
swelling of the conjunctival lining protruding the lid: or the lid may
be relaxed, and the conjunctiva may swell in consequence of repeated
inflammation of the parts, caused by frequent and careless exposure;
or the disease may be the result of contraction, by cicatrisation of
the integuments of the face, as after burns, extensive superficial
wounds in the neighbourhood of the eye, or the effect of periosteal
disease of the orbit. The affection may exist to a greater or less
degree, being in some instances scarcely visible, and not troublesome,
whilst in others, the eyelashes lie on the upper part of the cheek,
 and the swollen granulated conjunctiva is exposed. The lower lid is
generally the one which is affected. The disease may exist in both
eyes, or only in one. In strumous habits both are frequently affected
in a slight degree; and the upper lid, too, is sometimes turned a
little outwards. When eversion is of long continuance, and complete or
almost so, the conjunctival covering of the ball of the eye, and of the
cornea, becomes dry and wrinkled; in short, the membrane completely
changes its character, and becomes cuticular. In a lad who laboured
and the swollen granulated conjunctiva is exposed. The lower lid is
generally the one which is affected. The disease may exist in both
eyes, or only in one. In strumous habits both are frequently affected
in a slight degree; and the upper lid, too, is sometimes turned a
little outwards. When eversion is of long continuance, and complete or
almost so, the conjunctival covering of the ball of the eye, and of the
cornea, becomes dry and wrinkled; in short, the membrane completely
changes its character, and becomes cuticular. In a lad who laboured
 eleven years under eversion of the upper and lower lids—arising from
abscess and exfoliation of the external angular process of the os
frontis, following a blow received when a boy—the conjunctiva was hard,
wrinkled, scaly, and exactly similar to cuticle: this change of the
membrane also extended over the whole cornea. The surface of the eye
had lost its lustre, and vision was much impaired, the patient being
able to distinguish only very bright objects. By such cases, continuity
of the conjunctiva with the outer layer of the cornea is beautifully
demonstrated.
eleven years under eversion of the upper and lower lids—arising from
abscess and exfoliation of the external angular process of the os
frontis, following a blow received when a boy—the conjunctiva was hard,
wrinkled, scaly, and exactly similar to cuticle: this change of the
membrane also extended over the whole cornea. The surface of the eye
had lost its lustre, and vision was much impaired, the patient being
able to distinguish only very bright objects. By such cases, continuity
of the conjunctiva with the outer layer of the cornea is beautifully
demonstrated.
Some of the most intractable of all cases of eversion are the result
of burns. The constantly increasing contraction of the cicatrix draws
either the upper or the lower lid far from its natural situation,
and produces frightful deformity. The tarsal cartilages are greatly
extended, and in any operation for the relief of the patient it is
necessary to remove a portion before the lid can be properly adapted.
Great inconvenience is caused by the state of eversion: the surface
of the eyeball is subject to inflammation, in consequence of being
in255sufficiently protected; the change of its investing membrane is
a serious evil; and in some cases the cornea becomes extensively
ulcerated, unusually vascular, and opaque.
When the conjunctiva only is in fault, the deformity is slight, and
the state of matters is readily ameliorated by excision of the relaxed
portion. This is done by sharp curved scissors. As the wound gradually
contracts, the eyelid is drawn inwards, and, on cicatrisation taking
place, the parts have become restored to their healthy condition. Care,
however, should be taken that too much of the swollen conjunctiva is
not removed, otherwise the subsequent contraction may cause inversion
of the lid. Combined with the above practice, relaxation of the lid
itself will in many cases be remedied by removal of a portion of it
in the form of the letter V, by means of a sharp-pointed bistoury:
the edges of the incisions are afterwards put together by a point
of interrupted suture. When eversion arises from a cicatrix of the
integuments, the part in fault may be divided; but a temporary benefit
only can be procured. For, during the healing of the wound, the parts
again contract; and, though a portion of the conjunctiva is at the
same time removed, the contraction internally will hardly counteract
that which is going on externally. In order fully to obviate the evil
of this contraction of the cicatrix in inveterate cases of ectropion,
a form of plastic operation may be successfully resorted to. The
cicatrix being dissected out, and the tarsal cartilage brought neatly
into position, a piece of integument from the temple or cheek may be
adapted, and a portion of a new eyelid formed. The parts may sometimes
be brought into a good position without the necessity of borrowing
any portion of integument. A V-shaped incision can be made, the apex
pointing downwards, so as to loosen the under lid; and after it has
been drawn upwards and put straight, the edges of the lower part of the
exposed space are united by suture.
Entropion, or inversion, consists in the turning in of the tarsal
margins of the lids, and generally takes place during inflammation
and swelling of the conjunctival lining of the lid. During violent
inflammation of the lid the conjunctiva and integuments are much
swollen, and bulge out externally; by the projection the margin is
forced mechanically towards the ball, and entropion takes place. But
 in this state of matters, should the lid be by any chance everted,
and not replaced, then the bulging is from the conjunctival surface,
and prevents the margin from regaining its former site, and permanent
eversion or ectropion occurs. In fact, inversion and eversion, like
phymosis and paraphymosis, exist from the same parts being put in
different relation to each other. More permanent entropion is caused by
the contraction which follows removal of tumours from the under surface
of the lids, or destruction of large portions of the conjunctiva. The
disease is most frequently met with in the upper lid.
in this state of matters, should the lid be by any chance everted,
and not replaced, then the bulging is from the conjunctival surface,
and prevents the margin from regaining its former site, and permanent
eversion or ectropion occurs. In fact, inversion and eversion, like
phymosis and paraphymosis, exist from the same parts being put in
different relation to each other. More permanent entropion is caused by
the contraction which follows removal of tumours from the under surface
of the lids, or destruction of large portions of the conjunctiva. The
disease is most frequently met with in the upper lid.
Trichiasis consists in a vicious bend of the eyelashes, or in a
su256pernumerary growth in the rows or numbers of individual cilia,
whereby they are inverted, and sweep the surface of the conjunctiva
covering the cornea; thus great distress is caused by the friction of
the hairs and edge of the lid on the sensible surface of the eyeball,
and inflammation is frequently kindled and kept up by the continued
irritation; it is accompanied by its usual distressing symptoms when
seated in that organ, and too often followed by a greater or less
number of untoward consequences. Sometimes only one or two hairs are at
fault; in other instances, the half of the eyelash grows inwards; and
sometimes there is a double row of cilia; one set being in the usual
position, while the other projects against the eyeball. If proper means
are not taken to remedy the evil, and moderate the irritation which it
produces, the cornea becomes thickened and changed in structure; and
vision, at first impaired and indistinct, may be entirely lost.
The symptoms may be for a time palliated by plucking out the faulty
hairs, abstracting blood from the loaded vessels, and subsequently
using ointments or collyria,—the best of which, perhaps, is the
solution of nitrate of silver. In some cases it may be necessary to
employ counter-irritation, as blistering the nape of the neck; and in
all the general health must be strictly attended to. Other means may be
required, and will be mentioned when treating of chronic ophthalmia.
The permanent cure of the disease is effected either by removal or by
destruction of the roots of the cilia. The whole edge of the eyelid,
or the offending part of it, is removed with a sharp narrow bistoury,
the operator steadying the parts by laying hold of the cilia with the
fingers of his left hand. It is necessary to remove the mere edge only,
the cilia and their roots, and not the whole of the tarsal cartilage,
as has been proposed.
Inversion of the lid, from contraction of a cicatrix in the
conjunctiva, may be counteracted, by destroying with caustic, or
removing with cutting instruments, a portion of the outer integuments,
corresponding to the internal cicatrix. Forceps with broad points
are used for taking up a fold of the skin, and an oval portion is
then excised with a knife or scissors, cutting instruments being
less painful and more precise than caustics. Of the latter, the
sulphuric acid has been particularly recommended for this purpose.
The contraction of the wound releases the cilia from the power of the
internal cicatrix, and the parts are restored to their healthy state.
The term Pterygium is employed to denote a thickened and vascular
 state of part of the conjunctiva. The diseased portion is generally of
a triangular form, commencing at the inner corner of the eye, extending
towards the cornea, gradually diminishing in breadth, and terminating
in a sharp apex, either at the margin of the cornea, or somewhere
between its margin and centre. The thickening is seldom great, but the
vessels which traverse the thickened part are numerous, enlarged, and
tortuous—are, in257 fact, varicose. The base of the pterygium is always
on the circumference of the eye, generally at the inner corner, and
its apex is seldom, if ever, situated beyond the centre of the cornea:
frequently the sclerotic conjunctiva alone is affected. The motions of
the eye are little disturbed by the disease, but vision is materially
impaired when a considerable part of the cornea is covered. Pterygium
is in general single, but sometimes, though very rarely, there are two
or more pterygia in one eye; and, in such cases, the patient’s vision
is seriously affected, in consequence of the apices of the different
pterygia uniting and coalescing on the cornea, and investing the
greater part of that organ with a thick and dark shade. When several
occur, they sometimes unite throughout their whole extent, and cover
the half or more of the eye. This disease is very common amongst
negroes and persons residing in equatorial climates.
state of part of the conjunctiva. The diseased portion is generally of
a triangular form, commencing at the inner corner of the eye, extending
towards the cornea, gradually diminishing in breadth, and terminating
in a sharp apex, either at the margin of the cornea, or somewhere
between its margin and centre. The thickening is seldom great, but the
vessels which traverse the thickened part are numerous, enlarged, and
tortuous—are, in257 fact, varicose. The base of the pterygium is always
on the circumference of the eye, generally at the inner corner, and
its apex is seldom, if ever, situated beyond the centre of the cornea:
frequently the sclerotic conjunctiva alone is affected. The motions of
the eye are little disturbed by the disease, but vision is materially
impaired when a considerable part of the cornea is covered. Pterygium
is in general single, but sometimes, though very rarely, there are two
or more pterygia in one eye; and, in such cases, the patient’s vision
is seriously affected, in consequence of the apices of the different
pterygia uniting and coalescing on the cornea, and investing the
greater part of that organ with a thick and dark shade. When several
occur, they sometimes unite throughout their whole extent, and cover
the half or more of the eye. This disease is very common amongst
negroes and persons residing in equatorial climates.
When the pterygium is of considerable size, extending over the cornea,
the only remedy is excision. The apex of the web is laid hold of and
pulled outwards by forceps or a hook, and the whole diseased part is
then carefully dissected off with scissors, the incisions commencing
at the apex, and being carried on to the base. The wound gradually
contracts; and though an opaque cicatrix must form on the corneal
surface, the speck is of much less dimensions than the space formerly
occupied by the pterygium. If the web be thin and not exceedingly
vascular, it may be sufficient to make a semicircular section of it
transversely, by means of a hook and scissors, between its base and
the margin of the cornea; its growth is thereby arrested, and there
is a probable chance of its beginning to diminish, and ultimately
disappearing. When it is small, and so situated as to cause no
impairment of vision, it is prudent and good practice not to interfere
with it at all.
DISEASES OF THE EYEBALL
Diseases of the eyeball are numerous, and various in their nature. Some
are acute, others chronic; and their attack is either sudden, or slow
and insidious. Most of them are attended with pain and other annoying
symptoms, and some cause loss of vision. Some are cured by internal
means; others require surgical operations; and the cure is either
complete and permanent, or palliative and temporary. Some destroy the
organ, and others, still more malignant, cause extinction of life. All
require much attention and care.
Of Ophthalmia, or Inflammation of the Eye.—The symptoms and
appearances of ophthalmia vary much according to the particular
texture or textures affected. They require to be minutely attended
to, that the treatment may be varied in such a way as to obviate any
bad consequences which may be threatened. The great importance of the
organ, and the danger to its structure and functions which is likely to
occur from any other termination of the affection than resolution, must
never be lost sight of.
We shall first treat of inflammation of the more external parts of
the ball, an affection generally less dangerous than inflammation of
the interior, but at the same time of more frequent occurrence, and
produced by slighter causes.
258
Inflammation of the conjunctiva occurs in many individuals during very
warm and sunny weather. At such a period, the eye is often excited
by reflection of intense light from the surface of the earth; and is
irritated by sudden exposure to a degree of light to which it has not
been previously accustomed. Different directions of the sun’s rays,
and different kinds of light, seem to exert different influences
on the organ. The rays are most hurtful when they do not fall in a
perpendicular direction on the eye, but slopingly or horizontally.
Strong light from the moon, and light reflected from scarlet, are also
particularly injurious. Undue exertion of the eye weakens it, and
renders it prone to become inflamed. The eyes of infants are often
violently inflamed, in consequence of imprudent exposure to light
before they have been gradually accustomed to its stimulus. Again,
inflammation is caused by imprudent exposure of the eye directly to
cold, or by exposure of other parts causing suppression of their
discharges, whether natural or not. Inflammation of the conjunctiva
often follows suppression, however occasioned, of the menstrual or
hemorrhoidal discharges, as also suppression of discharges from
the urethra, from the Schneiderian membrane, or from behind the
ears. Irritations in the neighbouring parts, as in the mouth during
dentition, may also excite the disease. Immediate irritations, however,
are the most frequent cause, as the lodgement of extraneous bodies on
the surface of the organ—particles of sand, dust, snuff, pepper, or
gunpowder, minute insects, loose or inverted eyelashes. By the presence
of such substances, the eye is often kept in a very irritated state for
a long period. The most violent conjunctival inflammation is sometimes
produced by contact of gonorrhœal matter through carelessness.
Occasionally metastasis of inflammation takes place from one eye to
another; so that a person may be seen one day with severe inflammation
of the right, and on the following day with a similar affection of
the left, and the right entirely free from disease. Another cause,
sometimes met with, of inflammatory action in the conjunctiva, is
the lodgement of large foreign bodies in the orbit, with or without
destruction of the eye; as splinters of wood, straws, rusty iron nails,
sharp portions of stone, &c., penetrating the globe of the eye, or
parts in the immediate neighbourhood. Upon removal of the cause, the
redness, discharge of tears, pain, &c., sometimes subside without
inflammation having been established, the vessels of the part regaining
their contractility; but if the cause is continued for any considerable
time the effects do not rapidly abate. Wounds and other injuries of the
organ are generally followed by inflammation. But a simple clean wound
or puncture made with a fine instrument, as in many operations, and in
a favourable constitution, frequently produces little or no excitement
of the part. The degree of excitement must of course depend upon the
nature of the wound, the structure of the parts involved, the lodgement
or not of the body by which the wound is inflicted, and many accidental
circumstances. The eye may be injured by acids or by lime, and the
textures acted upon chemically; again, the membrane may be wounded by
pieces of hot metal, and then the destructive action is both chemical
and mechanical: in both cases active inflammation of the injured
conjunctiva is kindled. The state of the pa259tient’s constitution
modifies very much inflammatory action of the eye, however induced;
and it has been observed, that dark eyes bear injury or incited action
better than those of a light hue. Not unfrequently conjunctivitis is
a secondary affection, accompanying eruptile diseases, as measles or
small-pox.
In considering the disease, it is necessary to keep in mind the loose
connection of the membrane with the subjacent parts, as well as its own
texture and functions.
In conjunctival inflammation, the patient first feels a degree of pain
and stiffness in moving the organ; and has always a feeling as if a
foreign body were present, whether such is the case or not. There is
also a degree of itching with a sensation of fulness in the part, and
this is followed by redness of the membrane, becoming more and more
intense. If the disease gain ground, the colour changes to a darkish
red or purple hue. To the redness succeeds heat, with profuse and
hot lachrymation. Then swelling supervenes, often to a great extent:
the vessels, both veins and arteries, are much gorged, and effusion
of serum or blood takes place into the loose cellular tissue which
connects the conjunctiva to the sclerotic.
In some cases, the effusion in this situation is very considerable;
lymph as well as blood is deposited, and a bulging forwards of the
conjunctiva is produced; the stretched membrane becomes thickened, of
a raw granulated appearance, and a bright scarlet hue, and the cornea
appears sunk in the midst of the swelling, and almost hid by it: this
state of matters is termed Inflammatory Chemosis, and only occurs
when the excitement is very intense.
Blood is frequently effused beneath the conjunctiva in small quantity,
in consequence of a bruise or other injury of the eye,—from violent
exertion, as during coughing,—or from a less degree of inflammatory
action than in the preceding case; but the swelling thereby occasioned
is comparatively trifling, and the effusion is, in general, speedily
absorbed. To this affection the term Ecchymosis is attached.
In inflammation of the external parts of the eye, the redness begins
from the margins of the organ, and gradually diffuses itself towards
the cornea. Such is not the case in inflammation more deeply seated.
There is intolerance of light in a slight degree, and the patient is
inclined to keep the eyelids shut. At first the discharge from the
conjunctiva and meibomian glands is increased and changed, and flows
occasionally over the cheek, producing a scalding sensation. When the
eyelids are at rest, as during the night, they become glued together by
the viscid fluid from the meibomian follicles; but, if the inflammation
increases in intensity, the discharge is arrested.
In external inflammation there is more or less constitutional
disturbance, proportioned to the violence of the action and the
irritability of the system. In most instances the patient complains of
headache.
The above symptoms subside along with the inflammation; but, if this
has been at all severe or protracted, distension of the vessels to a
considerable degree continues, and the ophthalmia becomes chronic. This
change from acute to chronic takes place at various periods of the
affection, according to the intensity of the action, the nature of the
cause, and the irritability of the constitution. And again, the second260
stage of ophthalmia may revert to the first, acute inflammation being
rekindled by fresh irritation of the organ.
Purulent Ophthalmia most frequently occurs in warm climates, and
is attended from the first with profuse puriform discharge from the
conjunctiva. In the natural state of the organ, the conjunctival
discharge is pellucid, and so small in quantity as to be indiscernible;
but in this disease it possesses all the external characters of pus,
and is secreted in large quantity. The affection commences generally
in the under eyelid, with a feeling as if sand or foreign bodies were
lodged in the eye. The parts swell very much, and the eyelids become
more or less inverted, in consequence of serous effusion into their
cellular texture. Frequently the patient experiences an exacerbation
of the complaint about three or four hours after each meal. Though the
disease usually commences in the conjunctival lining of the eyelids,
the external coverings of the ball are often secondarily affected. In
some cases the bulb becomes the seat of lancinating pains; its coats
give way; the humours are discharged; and the eye sinks, with immediate
relief to the patient from the more urgent symptoms, but at the same
time with irreparable loss of vision. In other instances the effects
are less injurious to the structure of the organ, but equally so to
the sense of vision: the cornea becomes dull, and ultimately opaque,
or ulcerates, or partially sloughs; the swollen conjunctival surface
of the lids is covered with granulations, and secretes a copious
puriform discharge, with or without eversion, according to the degree
of swelling. At first the lids are more or less inverted, on account of
œdematous swelling of the cellular tissue: in the latter stages they
are everted by thickening and turgescence of the conjunctiva. This
membrane is at first villous and of a dull red colour, relaxed, and
its vessels enlarged and loaded; afterwards it becomes hard, almost
warty, and continues to discharge puriform fluid. The latter state
of the lining of the lid produces disease of the cornea, opacity of
a greenish colour, or an ulcer with intolerance of light, and other
symptoms of disorganisation proceeding in that tissue. The disease is
supposed to be contagious, and was the scourge of the British army for
many years after the campaign in Egypt. In that country it seems to be
caused by exposure to cold and damp during the night, and the intense
rays of light during the day, more especially when these causes act
on eyes which have not been accustomed to such vicissitudes. After
its invasion, it is communicable to others by contact of the morbid
secretion; and in individuals who have been once affected the disease
is very apt to recur when they are crowded together in unhealthy
situations.
A disease of equal malignity, and resembling in all respects the
Egyptian ophthalmia, occurs from the application of gonorrhœal matter
to the conjunctiva, or on sudden suppression of the gonorrhœal
discharge,—metastasis of the action sometimes takes place from the
urethral membrane to the conjunctiva. The eye is seldom saved from
the destructive effects of the violent inflammation which follows the
contact of the morbid fluid. Of all forms of purulent ophthalmia, the
gonorrhœal is the most rapid in its course and destructive in its
effects.
261
Children are not unfrequently the victims of purulent ophthalmia—the
ophthalmia neonatorum. Immediately after birth the conjunctival
lining of the eyelids seems unusually red and turgid, and a great
degree of swelling soon takes place, so as to render separation of
the eyelids very difficult. Occasionally eversion of the lids occurs,
when the child cries, from sudden and forcible contraction of the
strong external fibres of the orbicular muscle. In general, the lids
soon relapse into their former situation; but sometimes the eversion
remains, if the internally projecting tumour of the conjunctiva is
allowed to become still more swelled from strangulation, caused by
the outer margin of the reflected lid. The inflammation spreads over
the ball; and, in general, the swelling of the conjunctiva, being
greatest at the circumference of the eye, bulges out the eyelids, and
turns in their margins. Puriform matter is secreted copiously, and is
confined, more especially when, from inattention, the margins of the
lids are allowed to become glued together. They often adhere so firmly
as to require a very considerable force for their separation, and when
opened the matter gushes out as if from the cavity of an abscess. From
confinement of the matter the inflammation is still more increased,
and the cornea involved. Whitish specks form on it, or it ulcerates,
and the ulcers make their way into the anterior chamber of the eye; or
portions of it slough, causing partial loss of the organ and openings
into the chamber, in consequence of which the aqueous humour is
discharged, and the cornea sinks and becomes flaccid. In many instances
the cornea becomes opaque, changed in texture, and increased in
thickness, so as to form a convex projection from betwixt the eyelids,
termed Staphyloma; the sclerotic coat also is occasionally affected
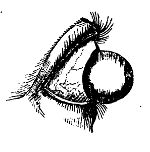 in a similar manner. A frequent cause of purulent ophthalmia in
children is imprudent exposure of the eyes to strong light, the parent
or nurse not remembering that the organ must be gradually accustomed to
the stimulus. Exposure to cold may also induce the inflammatory action.
The application of leucorrhœal or gonorrhœal matter to the eyes of the
child, whilst passing through the vagina of the mother, is perhaps
the most common cause of the disease. A very unhealthy state of the
constitution accompanies the affection: the scalp and other parts of
the surface are frequently covered with eruptions. A singular result
sometimes follows the purulent ophthalmia of infants. A small opaque
spot is observed on the capsule of the lens, which remains through life
a central spurious capsular cataract.
in a similar manner. A frequent cause of purulent ophthalmia in
children is imprudent exposure of the eyes to strong light, the parent
or nurse not remembering that the organ must be gradually accustomed to
the stimulus. Exposure to cold may also induce the inflammatory action.
The application of leucorrhœal or gonorrhœal matter to the eyes of the
child, whilst passing through the vagina of the mother, is perhaps
the most common cause of the disease. A very unhealthy state of the
constitution accompanies the affection: the scalp and other parts of
the surface are frequently covered with eruptions. A singular result
sometimes follows the purulent ophthalmia of infants. A small opaque
spot is observed on the capsule of the lens, which remains through life
a central spurious capsular cataract.
Inflammation of the Cornea supervenes on simple conjunctival
inflammation, and frequently on the purulent. The vessels of the part,
both veins and arteries, previously carrying single and therefore
invisible blood corpuscules, become much dilated, are filled with
numerous globules, and hence are rendered red and conspicuous to the
unassisted eye. Writers on ophthalmic surgery, in their rage for
refinement, speak of three kinds of this inflammation—inflammation
of the external or conjunctival covering, of the middle tunics or
cornea262 propria, and, lastly, of the third coat, the capsule of the
aqueous humour: such distinctions, however, are found to effect no good
practical end, and it is unnecessary to follow them. One particular
layer of the cornea may be first attacked, but the whole structure
soon becomes involved. The inflammation generally commences in the
conjunctival covering. Vision is necessarily much obscured from even
slight inflammatory affection of the cornea. Part only of the organ may
be affected, but frequently the whole is involved. Sometimes only one
or two vessels remain dilated; but still they, passing over the centre
of the cornea, render vision indistinct. Opacity of the cornea, to a
greater or less degree, always attends dilatation of its vessels.
In inflammation of the internal and middle tunics of the cornea,
most of the enlarged vessels which traverse it are seen to be
continuations of those that ramify in the conjunctival covering; while
the anastomotic vessels derived from the sclerotic coat are smaller
and less apparent than those of the conjunctiva. The cornea, and the
sclerotic immediately surrounding it, frequently appear to be almost
entirely covered with meshes of their dilated capillaries. At first
the whole cornea has a clouded appearance, but as the disease advances
portions become distinctly opaque, and at these points either lymph
or pus is effused. Sometimes matter collects between the laminæ,
distends them, and, causing ulceration, discharges itself either into
the anterior chamber or externally. Inflammation of the cornea arises
frequently from lodgement of a foreign body in it: and ulcers of it
are often produced by a similar cause. If the extraneous matter is not
removed soon after its insertion, nature commences her endeavours to
detach it, and the process employed is ulceration. Sometimes, however,
a sac is formed around the foreign body as in other parts, and no ulcer
is produced.
Ulceration of the cornea also takes place in order to afford an exit
to matter formed between its layers deeply or superficially. Deep
abscess of the cornea is by no means a rare consequence of violent
inflammatory action in the part. A minute opaque spot is at first
seen; this extends, assumes a yellow colour, and does not change its
situation on the head being moved. The internal lamellæ may ulcerate
in consequence of the pressure; but this seldom happens; the matter
is discharged externally. Suppuration in this situation is often
attended with much pain. Abscess of the surface of the cornea is of
more frequent occurrence than one more deeply seated: from its external
covering yielding readily to the pressure of the accumulating matter,
it generally assumes a pustular form. The fluid in such cases is
sometimes absorbed, and no vestige of disease remains in the part; but
more frequently the apex of the pustule gives way, and an ulcer is the
consequence. A similar result takes place if an artificial opening is
made for evacuation of the matter; and it may be considered as a good
rule in practice not to interfere with collections in the cornea, as
there is a probable chance of the matter being absorbed, and the cornea
regaining its transparency; while it is certain that breach of its
surface, in such cases, though made by the most delicate instrument,
will give rise to ulceration.
263
Pustular Opthalmia is at some seasons frequently met with: small
pustules, sometimes numerous, form on the conjunctiva, whilst that
membrane is turgid and its vessels dilated; the sclerotic conjunctiva
around the cornea is their most common situation, but sometimes almost
the whole conjunctival surface appears studded with them. When the
cornea is affected, the pustules frequently give way, and produce
ulceration; and when the pustules are numerous, and surrounded by much
vascularity, the part becomes opaque as well as ulcerated.
In weak constitutions Ulcers of the Cornea occur from slight
causes,—exposure to strong light, intemperance, inverted or irregular
ciliæ, a granulated state of the lining of the lids, or from momentary
irritation of the part by extraneous matter. The ulcer appears at first
circular, but during its progress it often becomes of an irregular
form; its surface is depressed and ragged, and can readily be seen by
directing the patient to fix the eye, and then looking at the part
from one side. The edges are elevated; and the surface, which is of
an ash colour, discharges an acrid colourless fluid, as in similar
affections of all surfaces that are covered with a delicate, tense,
and exquisitely sensible expansion. Sometimes the ulcer is very minute
and superficial, and enlarges very slowly, if at all; but in other
instances it extends rapidly in depth and size, with great pain and
irritability of the organ, and intolerance of light. Occasionally their
increase is expedited by partial sloughing. At first, when the ulcer
is minute, the part often retains its natural transparency. But as the
disease advances, when the sore spreads superficially either by the
sloughing or the ulcerative process, or by both, the cornea becomes
opaque, often to a considerable extent, around the ulcerated part;
and if the ulcer extends deeply, so as to perforate the tunics, the
aqueous humour escapes, the iris falls forward, and the pupil becomes
distorted: in either case vision is impaired or destroyed. In some
cases great relief follows discharge of the humour, and the consequent
flaccidity of the cornea, the ulcers seeming to have been prolonged
and irritated by the fulness of the chamber. Sometimes an ulcer will
penetrate the laminæ of the cornea, even to the aqueous membrane. This
latter tissue may resist the ulcerative process, and will then be
pushed forward into the opening by the pressure of the aqueous fluid.
This is the hernia of the aqueous membrane, so called, instances of
which have been known to acquire a considerable size before the bag has
given way.
Abrasion of the conjunctival covering of the cornea is produced by
accident, or follows incited action of the vessels. The abraded surface
either ulcerates, or contracts and heals kindly, with or without
opacity of the part. Breach of surface in the cornea,—whether an ulcer,
an abrasion, or a raw surface, caused by the giving way of a pustule,
or of a small abscess,—is constantly liable to irritation, on account
of not being protected by mucous membrane and mucous discharge: even
the contact of the tears irritates, and keeps up inflammatory action in
the membranes. When the ulcerative process ceases, lymph is effused,
and a grayish halo forms around the sore; the ash colour of the surface
of the sore disappears, and is succeeded by florid granulations,
extremely minute, which fill up the cavity;264 cicatrisation follows
in due time, with subsidence of all the symptoms and appearances of
inflammation. There remains, however, an opaque speck of a pearly
hue corresponding to the sore, but occupying rather less space. When
the cornea is perforated by ulceration, the sore sometimes shows no
disposition to heal, becoming a fistulous aperture through which the
aqueous humour is from time to time discharged. By this condition of
parts vision is much impaired, the cornea being always more or less
flaccid. Touching the fistulous opening with the nitrate of silver,
reduced by scraping to a very fine point, will often promote a healthy
action in the tissue, and effect adhesion of its sides.
The pearly speck which remains after cicatrisation of a corneal sore
is termed Leucoma, and is permanent. It is generally of an uniform
colour, but occasionally a black speck is perceptible in some part of
it. For, when an ulcer lays open the anterior chamber, part or the
whole of the aqueous humour is evacuated, and the iris falls forward;
a portion of the iris falling into the opening, provided this is
not in the centre of the cornea, closes it up, and becomes adherent
to that part. If the opening is large, the prolapsus of the iris is
considerable; and in some cases this membrane, being pressed on by the
humours, is forced through the opening in the form of a small bag.
This change of position is termed Hernia of the Iris; and the dark
sacculated portion of the iris which projects from the surface of
the cornea is called Myocephalon, from its resemblance to the head
 of a fly. The myocephalon may remain for a considerable time, or may
sphacelate and drop away. The pupil is thus rendered irregular, is
perhaps nearly obliterated, or is drawn down behind the opaque part,
and thereby rendered totally useless to the patient. The impairment
of vision caused by Leucoma depends on the size and situation of the
speck. The disease is irremediable, though the thin cloudy opacity,
which frequently surrounds the leucoma, may be dissipated. The
operation of artificial pupil is sometimes required, in order to afford
a degree of vision in this affection of the cornea,—as well as in the
speck of a similar appearance occasioned by effusion and organisation
of lymph betwixt the deep lamellæ of the cornea, and which is termed
Albugo.
of a fly. The myocephalon may remain for a considerable time, or may
sphacelate and drop away. The pupil is thus rendered irregular, is
perhaps nearly obliterated, or is drawn down behind the opaque part,
and thereby rendered totally useless to the patient. The impairment
of vision caused by Leucoma depends on the size and situation of the
speck. The disease is irremediable, though the thin cloudy opacity,
which frequently surrounds the leucoma, may be dissipated. The
operation of artificial pupil is sometimes required, in order to afford
a degree of vision in this affection of the cornea,—as well as in the
speck of a similar appearance occasioned by effusion and organisation
of lymph betwixt the deep lamellæ of the cornea, and which is termed
Albugo.
Albugo occurs during the intensity of inflammatory attacks. It also
is surrounded occasionally by thinner opacity, but not depressed and
unequal on the surface, as leucoma sometimes is. Large and tortuous
vessels are generally seen passing into albugines, but meshes of dilated
vessels are seldom present. When the affection is recent, it sometimes
disappears under proper treatment, especially in young subjects; but
the albugo is by no means so readily removed as the Nebula, or thin
cloudy opacity which is the frequent consequence of obstinate chronic
dilatation of the conjunctival vessels. Nebula is superficial, and
consists of mere thickening of the conjunctival covering, from lymph
having been effused. It impairs vision, but does not destroy it, for
the affected part remains semitransparent.
In strumous constitutions specks of the cornea are often accom265panied
with ulceration of the edges of the palpebræ, and destruction of the
ciliæ—the ophthalmia tarsi. The margins of the eyelids are red and
slightly tumid, and discharge an acrid fluid; the ciliæ are matted
together; pustules form at their roots; the bags which secrete them
are laid open and destroyed, and they consequently fall out. The
affection is often of long duration, and may be in part prolonged by
vitiated secretion from the meibomian glands. During its progress it
excites very considerable irritation in the whole eye, and, as has been
already stated, opacities of the cornea not unfrequently accompany it.
Veins become enlarged, and varicose on the conjunctiva, as also their
minute ramifications on the clear part of the ball; small reddish lines
appear on the cornea, and around them is “diffused a thin, milky, or
albuminous humour,” which destroys its transparency at that part.
Such spots may be solitary or numerous, and darken the cornea either
partially or entirely. They are always surrounded with a fasciculus of
enlarged veins.
In elderly people a dim opaque ring, of a greyish colour, sometimes
encircles the margins of the cornea, and is called Arcus Senilis; but
this can scarcely be looked upon as a disease.
Sometimes the cornea presents a spotted appearance; and this state of
the organ is generally attended by obstinate inflammatory action in the
part. The affection, however, is rare. I have seen several instances of
it: in one, both corneæ were spotted, and sight was almost destroyed,
without much irritability of the organ. The disease yielded to external
stimulants, and the internal use of the bichloride of mercury. It is
met with in a chronic and very intractable form.
The cornea may sometimes be rendered dim by over-distension, the
aqueous humour being unusually copious.
Occasionally sloughing takes place in the cornea from over-action. It
is dangerous to the structure and functions of the organ, according to
the extent to which it occurs.
Ossification of the cornea is said to take place; but few cases are
on record, and these were in very old people.
The cornea sometimes becomes conical to a great degree in persons
considerably advanced in life. The cone has its apex in the centre of
the organ, seems thick and crystalline when viewed laterally, and when
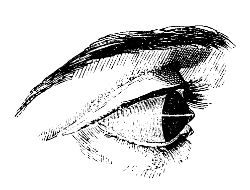 looked on from the front has a sparkling appearance. In some cases it
is opaque in the centre, and occasionally its surface is irregular.
Vision of objects at any distance is very indistinct; those placed
within an inch or two of the eye are most distinctly seen, especially
if looked on through a small aperture. The disease usually affects both
eyes, though not always in an equal degree. The patients cannot judge
accurately of distance, and see objects multiplied and disfigured.
looked on from the front has a sparkling appearance. In some cases it
is opaque in the centre, and occasionally its surface is irregular.
Vision of objects at any distance is very indistinct; those placed
within an inch or two of the eye are most distinctly seen, especially
if looked on through a small aperture. The disease usually affects both
eyes, though not always in an equal degree. The patients cannot judge
accurately of distance, and see objects multiplied and disfigured.
266
Staphyloma has been already alluded to as an occasional consequence
of purulent ophthalmia in children. The cornea is thickened, prominent,
and opaque; and in most cases vision is either much impaired or
entirely lost. The prominence varies in different cases, being
sometimes very little elevated beyond the natural state of the part,
while in other instances it protrudes from between the eyelids. After
having attained a certain size it often becomes stationary; but very
frequently it continues to enlarge gradually. When the prominence is
large, much inconvenience arises from the eyelids not being allowed to
close; and the eye, being thereby deprived of its natural covering, is
extremely liable to become inflamed from external irritation. When one
eye is affected with staphyloma, the other not unfrequently becomes
similarly diseased.
Dropsy of the anterior chamber, or Hydrophthalmia, occasionally takes
place in persons of weak constitutions. The aqueous humour is either
secreted in greater abundance than it usually is, or absorption is
diminished. The cornea gradually accommodates itself to the increase
of the fluid behind, and becomes wider and more prominent, but retains
its transparency; in looking at the eye, the anterior chamber is seen
evidently enlarged, and occasionally the aqueous humour is of a turbid
appearance. There is little or no pain in the eyeball, but the patient
complains of an annoying sense of fulness and tension in the part. In
consequence of the vitreous humour also accumulating, the whole organ
is ultimately enlarged considerably, and its motions are thereby much
impeded. At first, vision of near objects is impaired, whilst the
patient sees very distinctly those placed at a distance; ultimately
sight is entirely lost.
Exophthalmia, or protrusion of the eye, attends the preceding
disease, and is also a consequence of various other morbid actions
in the globe and its neighbourhood, especially from the pressure of
tumours in the orbit. The chronic enlargement of the bulb is noticed
more fully in the succeeding chapters.
Treatment of External Ophthalmia, and its Consequences.—The exciting
cause, if such exist and can be discovered, ought in the first place
to be removed. The surface of the organ and of the palpebræ should be
carefully examined, either with the naked eye or with a magnifying
glass, in order to detect any small extraneous body which may be
lodged in the part. In examining the inner surfaces of the palpebræ,
it is necessary, to produce complete eversion, to bring the parts
completely into view; and the most convenient method of accomplishing
this is to lay hold of the ciliæ between the finger and thumb, and
reflect the lid over a silver probe placed along its base. This can,
by a little practice, be accomplished readily without using a probe,
and even by the fingers of one hand only. This is the more necessary,
as small particles of foreign matter lodge more frequently on the
palpebral conjunctiva than on any other part. If a particle of glass,
metal, stone, &c., be discovered, it should be gently removed by the
flattened extremity of a silver probe, or by a scoop, a fine needle,
or a delicate brush. In some cases washing the surface by means of
a small syringe, filled with a bland fluid, is extremely useful; as
when an impalpable powder has been thrown267 into the eye, and can with
difficulty be removed, in consequence of spasmodic contraction of
the eyelids preventing exposure of the parts. The application of an
emollient poultice, with the addition of hyoscyamus, is beneficial when
it has been found impossible to remove the whole of a fine powder. When
particles of lunar caustic have, by accident, come in contact with
the eye, they are to be removed, as soon after insertion as possible,
by a fine hair pencil dipped in oil or fresh butter,—not in water.
Small loose bodies are generally carried, by the increased lachrymal
secretion, along the sulcus formed by the apposition of the eyelids,
to the inner canthus, and there discharged. And, in order to favour
this natural process for removing extraneous matter, the patient should
be directed to keep the eyelids shut, and as quiet as possible, to
cover them with his hands, and to blow his nose forcibly: thus the
greater number of the extraneous particles will be got rid of. Those
which remain lodged in the membranes must be speedily removed by those
artificial means which have been already enumerated. If entropion is
the cause of the inflammation, the eyelashes are either plucked out,
or completely destroyed by removal of their roots. The inflamed organ
should be carefully protected from the stimulus of strong light; the
patient is to be placed in a darkened room, and the eye protected by a
thin green shade. The shade, however, may be worn too long, so as to
induce an extremely weak and tender state of the organ.
If there be good grounds for believing that the incited action has
been caused by suppression of any discharge, that should be encouraged
to return, and the cause of the suppression must be avoided. If a
gonorrhœa have been suddenly arrested by the employment of stimulating
injections, these must be instantly discontinued; and some have even
gone so far, in such cases, as to introduce bougies impregnated with
gonorrhœal matter, in order to procure a renewal of the discharge.
In cases of suppression of purulent discharge from the ears, or the
surrounding parts, followed by external ophthalmia, a blister or
sinapism should be applied in the neighbourhood of the part from which
the discharge formerly issued. When the menstrual evacuation has been
arrested, leeches and fomentations should be applied to the pudenda, or
around the anus, and emenagogues administered internally; the patient
should be placed in a quiet and well ventilated apartment, and kept
free from any emotions of the mind; all noise and other sources of
irritation should be studiously avoided.
If the incited action in the eye do not subside, as it often will
not, on removal of the exciting cause, recourse must immediately be
had to very active means for its subjugation; for in no other organ
does inflammatory action proceed more rapidly to an unfavourable
termination. By timely use of antiphlogistic means, those consequences
of external ophthalmia, which we have already treated of, may be
avoided; and, with respect to most of them, it is much better to
prevent their occurrence, than combat them after they have been allowed
to take place. The eye is more valuable to a great proportion of people
than a limb; and the surgeon is very culpable if he be not master of
this part of his profession, and able to undertake the manage268ment
of every disease and accident to which the eye is liable. “In cases
of inflammation the general treatment is the same; but each variety
requires peculiar attention during the cure, depending on the structure
and function of the tissue affected.”
In the first stage of external ophthalmia, active antiphlogistic
measures must be put in force. In full habits, and cases of intense
action, general bleeding must be employed, even to fainting, from the
veins of the arm or of the neck, or from the temporal artery,—and
repeated, if necessary, according to circumstances. Blood is sometimes
abstracted by cupping from the temples or the nape of the neck; but
it is a painful and uncertain mode of emptying the vessels. Local
bloodletting, in many cases, suffices to moderate the action; in all
it is most beneficial and important, after the employment of general
depletion. The application of leeches to the inner canthus is the most
effectual method of abstracting blood locally, as at that point the
venous return is made from the eye. If placed on the temples, they can
produce very little benefit; if on the outer surface of the eyelids,
ecchymosis follows, on account of the extreme looseness of the cellular
tissue in that situation. Or the angular vein, at the inner canthus,
may be opened with a lancet, and a considerable quantity of blood
thereby abstracted from the seat of the disease. Leeches applied to the
conjunctiva of the lower lid are sometimes advantageous; but leeching
and scarification are more useful in the chronic stage: and the latter
is injurious in acute ophthalmia. Saline purgatives, and antimonial
medicines, a very material part of the antiphlogistic regimen, must not
be omitted. Enemata, with occasional pediluvia, are much recommended
by some Continental writers. In bilious habits emetics, followed by
mercurial purges, will be found very useful. With respect to topical
treatment, warm applications are found to afford decided relief in
the first stage, and are, in consequence, generally used. By some,
however, cold water, or water with vinegar, is applied from the first.
Poultices, whether warm or cold, prove annoying from their weight. Warm
fomentations, simple or anodyne, are preferable, and may be repeated
according to the feelings of the patient; or the eye may be exposed to
the steam of water.
When by these means the violence of the symptoms has abated, as
usually happens in the course of a very few days, the organ must be
gradually accustomed to its natural stimulus, light. The shade must be
discontinued, and the room no longer darkened; and now leeching becomes
of great service, while the evacuation is to be followed by gently
stimulating or astringent applications, so as to produce contraction of
the still dilated, though partially emptied, vessels. Various collyria
may be employed for this purpose. Solutions of the sulphate of zinc,
of muriate of mercury, of sulphate of alum, of acetate of lead, or of
the lapis divinus—wine of opium—the citrine ointment, or the unguentum
oxydi hydrargyri rubri, &c.—or stimulating vapours of various kinds.
Camphor is a good addition to many of the applications. The collyria
may be cold, or slightly warmed; and maybe dropped into the outer
canthus, flowing over the eye, and escaping by the inner canthus,
according to the natural course of the fluids269 of the eye; or they may
be inserted at the inner canthus, the head being immediately afterwards
inclined so as to allow the fluid to pass towards the external canthus;
or they may be applied by means of an eyeglass. Warm fomentations,
and other relaxing remedies, however useful during the first stage,
are worse than useless, are hurtful in the highest degree, when the
affection has passed into a chronic state; as also are antiphlogistic
means, and exclusion of light,—remedies so essentially necessary in the
first stage.
In ophthalmia, attended with profuse purulent discharge, the
structure of the eye is in great danger of being destroyed, from the
intensity of the action, and its liability to extend to the deep parts
of the organ; the most active practice is required from the first.
Copious general depletion, ad deliquium, must be quickly had recourse
to; and the patient must be freely purged, and kept in a state of
partial nausea for some time, by exhibition of antimonials. After
general bloodletting, the repeated application of leeches to the inner
canthus is necessary, in order to empty sufficiently the vessels of the
part. Where the chemosis is so extensive as to bury the cornea, as it
were, beneath the folds of the swollen conjunctiva, sloughing of the
transparent tunic is frequently threatened. In order to arrest this
fatal result, much good is often obtained by division of the chemosis.
A sharp-pointed bistoury is passed through the swollen membrane, and
radiating incisions practised, commencing at the corneal margins, and
directing them towards the circumference of the globe. Sometimes four
or even five of such divisions are called for, while care is taken not
to wound the sclerotic coat beneath. A considerable quantity of blood
is sometimes lost by this procedure, and, the chemosis subsiding,
the cornea is saved. Infusion of tobacco, solutions of acetate of
lead, and nitrate of silver, æther and laudanum, have been used as
applications to the eye from the very commencement of the affection;
but the propriety of the practice appears very questionable. Blistering
the nape of the neck proves highly beneficial, after the employment
of the antiphlogistic measures; and in many cases it is necessary
to keep up discharge from the blistered surface for some time. On
subsidence of the violent symptoms, the swelled conjunctiva is to
be attacked with escharotics and stimulants, as the nitras argenti,
sulphas cupri, or various collyria: then only can such applications be
advantageous; at an earlier period they must do harm. They repress the
exuberant granulations which may have formed, or may be forming, on the
conjunctiva of the eyelids, promote contraction of the dilated vessels,
diminish the relaxation of all the tissues, and stimulate the now
dormant action of the part into a healthy state of excitement. Gently
stimulating collyria may be injected betwixt the lids, by means of a
small syringe. In granulated conjunctiva, it is sometimes necessary to
remove a greater or less part of the diseased membrane by escharotics,
the knife, or scissors; and after this has been accomplished it is
well to encourage bleeding to a slight extent. In removing part of
the palpebral conjunctiva, care must be taken to avoid injuring the
cartilage of the tarsus; and, in the lower lid, not to take away too
large a portion, lest entropion should occur during cicatrisation. In
hospital practice, the infected should be separated270 from the healthy;
and promiscuous use of towels and sponges must not be allowed.
In Purulent Ophthalmia of Children, antiphlogistic means must
be pursued, if the patient is seen during the first stage of the
disease; but children do not bear depletion well. After the discharge
is established, the surface of the eye must be kept free of matter,
by frequent injection of a bland, tepid fluid; and stimulating or
astringent collyria should be applied three or four times a-day.
When Inflammation of the Cornea is established, it is exceedingly
difficult to procure contraction of the vessels. Active antiphlogistic
measures must be employed in the acute stage; and in the chronic,
stimulant applications are to be had recourse to. As, however,
corneitis is frequently kept up in its chronic form, from deficient
constitutional power in strumous habits, strict attention must be paid
to the diet and secretions of the patient. Mild mercurial alteratives,
diaphoretics, and tonics combined, will often effect a cure, where all
local treatment has been tried in vain. When a large plexus of vessels
remain dilated on the part, the most effectual method of removal is to
divide them, as they ramify on the sclerotic, by means of scissors, or
a fine knife, and afterwards to employ stimulating applications.
The irritability of ulcers on the cornea is diminished by the
application of nitrate of silver, in solution or substance. If in
solution, the application is used in the proportion of three to ten
grains of the salt to the ounce of distilled water; if in substance, a
portion, finely pointed, is gently applied to the sore, which may be
afterwards besmeared with a little oil or simple ointment, in order
to confine the action of the nitrate to the ulcerated part. It is not
necessary, but, on the contrary, hurtful, to rub the caustic freely
on the sore; a very slight application is sufficient to coagulate the
secretions on the part, and form a covering for protection of the
surface. In two or three days afterwards, when the temporary covering
has become detached, and when the irritability of the sore has in
consequence returned, it will be necessary to repeat the application,
but not till then. On each application, and few are in general
required, the sore is found reduced in size considerably. The collyrium
nitratis argenti is very useful in many obstinate cases of affections
of the eye and eyelids, the strength of the solution being varied,
according to circumstances.
In Albugo and Leucoma, proposals have been made for excising,
scraping, or perforating the opaque part; but the cure by such means
is worse than the disease, as a raw surface is left larger than the
previous opacity, and the cicatrix which must inevitably form also
occupies a larger space, and is equally opaque. Leucoma and Albugo
are incurable diseases, though the opacities may become somewhat
thinner, by natural processes, after the lapse of a long period.
Nebulæ, however, are often removable. During the treatment of them,
or, rather, before beginning to treat them, it is of the utmost
importance to attend to the state of the surface of the eye, and of
the lids and eyelashes. Stimulating substances may be applied in cases
where the opacities are thin: powders of calomel, aloes, sugar, &c.,
have been blown into the eye; stimulating lotions or ointments are
preferable; one containing the nitrate of silver, with the addition
of271 a proportion of the liq. sub-acet. plumbi, is sometimes used
with advantage. These, however, are often of no avail, unless the
dilated vessels, when such exist, are divided, or a portion dissected
out; afterwards stimulants will be efficacious, and must be used
assiduously. The vessels may require to be divided again and again.
In Ophthalmia tarsi, gently stimulating ointments or lotions are to
be used, and in obstinate cases much advantage will result from the
application of blisters behind the ears and to the nape of the neck,
or from the insertion of a seton in the latter situation. In children
it is necessary to correct the state of the bowels, scarify teeth, and
remove other irritating causes to which that tender age is liable.
Sloughing of the Cornea should, of course, be prevented, if possible,
by subduing the incited action before it has attained such intensity
as to overcome the power of the part. The slough is slow in separating
when the constitution has been much weakened; and sometimes tonics and
stimulants, both external and internal, are required to hasten the
process of separation. When the surface has at length become clean, the
same treatment is required as to an ulcer of the part.
Conical Cornea.—This deformity can scarcely be cured, nor can any
optical contrivance effectually remedy the disturbance of vision.
When the apex of the cone is opaque, the removal of the pupil to the
circumference by operation affords the best chance of assisting the
sight of the patient.
When staphyloma is small, neither impeding the motions of the
eye, nor preventing its being protected by the lids, no surgical
interference is called for, as the loss or impairment of vision cannot
be remedied, and as no other inconvenience than blindness is produced
by the change of form in the part. But when the diseased cornea
projects from between the eyelids the prominence must be diminished,
on account of the deformity which it occasions, and in consequence
of the eye being deprived of its natural protection of the lids, and
being thereby exposed to constant irritation. In such cases it is
necessary to take away a portion of the cornea, that the eye may be
so diminished in bulk as to retract within the eyelids; the size of
the part removed must be proportioned to the degree of protrusion. A
cornea-knife is passed into the prominence, and carried forwards so as
to transfix the part, in a direction from the external to the inner
canthus; and by the knife being carried on, with its cutting edge
looking downwards, a flap of the cornea is made. This flap is then laid
hold of by means of forceps, and removed either with the knife or with
scissors. The aqueous humour immediately escapes, and in most cases
the crystalline lens and vitreous humour are also discharged. The eye
consequently shrinks, and retracts within the palpebræ. The cut margins
of the cornea soon assume a reddish appearance—they form granulations,
the wound contracts gradually, and ultimately closes; but the eye is
necessarily much shrunk, and totally useless as an organ of vision.
Generally suppuration takes place, causing complete disorganisation of
the parts; and the preceding inflammatory action may be so intense,
and attended with so much constitutional disturbance, as to require
active measures for its moderation. Deformity may be in a great measure
removed by adapting an artificial272 eye to the shrivelled remains of
the natural one. When it is necessary to remove only a small part of
the cornea, the aqueous humour alone escapes, and during the cure of
the wound the patient not unfrequently enjoys a tolerable degree of
vision; but after the wound has completely closed, vision is again lost
completely.
Hydrophthalmia, also, is a disease in which little hope can be
entertained of materially benefiting the patient. In the slighter
cases, in which no very annoying symptoms accompany the affection,
vision may be improved by the use of optical instruments; mercurial
preparations may be employed in moderation, with the view of promoting
absorption of the superabundant fluid. When the disease has made
considerable progress, temporary relief may be obtained from puncturing
the cornea at its lower part, so as to discharge the accumulated
aqueous humour; but a cure can scarcely be expected from such a
practice, however often the paracentesis may be repeated. In the worst
cases the pain is so excruciating, and the system so much disturbed by
the local affection, as almost to warrant the destruction of the organ,
in order to relieve the patient; but, after all, even such severe
measures will most probably prove unavailing.
In Exophthalmos the treatment must vary according to the
circumstances which cause the protrusion of the eyeball.
Of Internal Ophthalmia.—Inflammation of the internal parts of the
eyeball sometimes supervenes on conjunctival inflammation, and then
the distinctive characters of the two affections are not perceptible.
When inflammatory action attacks the deep parts primarily, the external
ciliary vessels ramifying on the sclerotic coat are seen, enlarged,
shining through the conjunctiva; and, as they advance towards the
clearer part of the eye, they form a zone of a pink colour, whose
vessels run in a straight direction towards the margin of the cornea;
but between the zone and the cornea a distinct white line is often
interposed. Then large arborescent and reticulated vessels soon appear
on the white part of the eye; and from their being more superficial
than the first, and of a brighter hue, it is obvious that they belong
to the conjunctiva. They also approach the clear part of the eye,
and, if numerous, obscure the former vessels—as also the red zone and
white line—for they pass over them, and reach the corneal margins, and
often go beyond it, in continuous ramifications. The sclerotic, in
consequence, assumes a pink-red colour, and the cornea becomes dim.
The iris may be primarily and principally affected, and, if so, the
disease is termed Iritis; but in most cases all the other internal
parts suffer more or less. The iris changes its appearance, becomes
of a dusky hue, either in part or throughout, and red vessels are
sometimes distinctly seen in it; from grey or blue it changes to
a greenish colour, and when formerly black or brown it becomes
reddish. The size of the pupil diminishes, and the contraction is
often irregular, when the inflammatory action is intense. The iris
swells perceptibly, and the pupil loses its dark colour, or is almost
entirely closed, either from effusion of lymph, or from inflammation
and consequent opacity of the crystalline lens and its capsule. The
iris projects forwards,273 and diminishes the capacity of the anterior
chamber; the pupil is irregular, and often assumes an angular
appearance; and the irregularity becomes permanent from adhesion of
the pupillary margin of the iris to the capsule of the lens, lymph
being effused and organised, and forming a firm uniting medium between
the parts. Occasionally adhesions form at the middle of the iris, and
cause so great contraction as to give the pupil an appearance of being
double. Of course irregularities of the pupil are most distinct when
the part is dilated, either spontaneously or by the application of
belladonna. Tubercles sometimes form on the iris, and not unfrequently
it presents a granulated appearance. From the commencement of the
inflammatory attack the patient feels great pain in the organ and in
the forehead, and there is great intolerance of light. There is a
feeling of tension of the eyeball, followed by deep throbbing pain
increasing every instant. As the disease advances, the cornea is
rendered opaque by the fulness of the chambers, and the aqueous humour
becomes turbid and of a milky appearance; or lymph is effused into the
anterior chamber, and floats about in flaky portions. Occasionally the
vessels of the iris are so distended as to give way, causing effusion
of blood into the chamber, often in considerable quantity.
More frequently, however, puriform fluid is deposited, occasioning the
appearance termed Hypopium. The pus is either fluid or of a thick
curdy consistence: when fluid and thin, it mixes with the aqueous
humour, rendering it white and opaque; if of firmer consistence, it
lodges in the lower part of the chamber, but changes its position, and
mixes partially with the humour, on the head being moved; when dense
and curdy, it remains separate from the humour, and its position is not
altered by motions of the head.
During the progress of the inflammatory action, all the symptoms
increase; the pain shoots to the top of the head, and is much
aggravated by pressure on the eyeball. Of course vision is materially
impaired. Constitutional disturbance always accompanies the affection,
and exists in a greater or less degree according to the extent of the
disease. The iris may be primarily affected, but the other textures,
both external and more deeply seated, too often become involved; and
in aggravated cases the whole eyeball suffers. When the most internal
parts, as the choroid coat, the retina, and the vitreous humour, are
affected, sudden and bright flashes of light disturb the patient,
whilst vision is rapidly lost, and for ever. Occasionally the intense
over-action terminates in suppuration of all the affected textures, and
the eyeball soon becomes completely disorganised.
In Rheumatic Ophthalmia the appearances of the diseased eye are
similar to those in ophthalmia produced by any other cause. But the
affection is accompanied with, and seems to arise from rheumatic
diathesis. There is pain in many of the joints, and frequently in the
scalp and portions of the face, increased on hanging the head, and by
pressing the parts. The pains are remittent, supervene at night, and
subside in the morning. In general the ophthalmia is external; but
in severe cases the internal parts become affected, and the eye is
sometimes lost by giving way of the cornea.
274
Internal ophthalmia is often occasioned by wounds inflicted either
accidentally or by operation. Laceration of the iris in the extraction
of cataract, or an improper performance of the operation for cataract
with a needle, is by no means an unfrequent cause of the affection.
Iritis often occurs during the exhibition of mercury in undue
quantities, and is said also to be a symptom of syphilitic taint. It
is, in many cases, preceded by cutaneous eruption, and seems to be the
consequence of the eruption being repelled, or interfered with in its
progress.
Choroiditis.—The choroid membrane is sometimes primarily affected:
but more frequently the inflammation of this tunic is the consequence
of sclerotitis, or the disease last described. When the result of the
former cause, it generally takes on the rheumatic type. The early
symptoms are zonular redness of the sclerotic, accompanied by a general
impairment of vision, so that the patient expresses himself as if
looking through gauze or some dark network. Presently the sight becomes
more and more impaired, until a complete amaurosis results. The pupil
is generally in a semi-dilated state, and, instead of presenting the
intense black hue of the healthy eye, it reflects a greenish-grey
colour, dependent upon the effusion of a turbid fluid between the
choroid and retina. The nervous structures, becoming thus pressed
upon, lose their sensibility to light, and are paralysed. This form of
inflammation is generally chronic, and imperceptibly advances to the
iris anteriorly, and to the retina within; the ultimate termination
being complete glaucoma. Various dull and heavy pains accompany
this affection; and, in the latter stages, acute circum-orbitar
neuralgia is the most distressing concomitant. By long-continued
chronic inflammation the sclerotic coat appears to lose its powers
of resistance—the accumulating fluid pushes before it the weakened
tunic, and Staphyloma Scleroticæ is produced. This protrusion of
the external tunic sometimes takes place in various parts, and to a
considerable extent, so that the figure of the globe is entirely lost.
The thinning of the sclerotic at these points allows the dark hue of
the choroid to shine through, and this, together with the bunched-like
appearance of the protruded portions, has entailed upon it the name of
Staphyloma Racemosum.
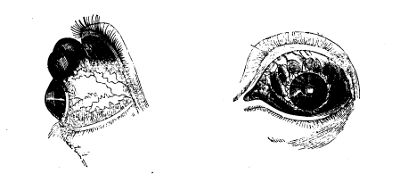
275
Treatment.—In the first stage of internal ophthalmia, active
treatment, properly conducted, should be successful in averting
the progress of the disease; in the latter stages, there is every
chance of vision being entirely lost. The treatment must be actively
antiphlogistic, consisting of general and local bleeding, the internal
use of purgatives and antimonial medicines, and strict abstinence. A
free use of mercury internally is said to check the disease, and, in
its advanced stages, to procure absorption of effused lymph. But the
inflammation can be subdued without the aid of that mineral, though its
effects are often powerful; and a recollection of the bad effects which
are so apt to follow its employment renders a prudent surgeon cautious
in having recourse to it. Mercurial ointment, with opium, rubbed on
the forehead, immediately above the affected eye, gives great relief.
The same relief follows friction with oil, in which the muriate or
other salts of morphia is dissolved. When the incited action declines,
the extracts of belladonna, hyoscyamus, or stramonium, rubbed on the
eyelids and brow, procure dilatation of the pupil, and thereby tend to
prevent its further contraction; but whilst acute inflammation exists,
the pupil is not dilatable; and it is consequently an encouraging
symptom when the pupil begins to yield to the influence of these
medicines. In hypopium it is sometimes necessary to evacuate the pus
when effused in large quantity, in order to prevent the injurious
effects that its pressure might occasion; but, if the quantity be
small, there is a good chance of its being removed by absorption.
In suppuration of the eyeball, whilst the other eye remains sound,
it may be prudent to open the cornea, and allow a free exit for the
matter, in order to prevent the healthy eye from becoming affected.
In the staphyloma of the sclerotic coat, when the eye, as it were, is
affected by a sort of chronic dropsy, (and this disease is met with
at various periods of life,) the tension and bulk of the organ may be
diminished by occasional puncture. The opening may be kept pervious by
the introduction of a conical probe from time to time. I have more than
once introduced a silk thread through the most dependent and prominent
part of the globe with good effect. The organ ultimately shrinks.
Amaurosis implies an impairment of vision more or less complete,
arising from disease in the brain, in the optic nerve, or in the
retina, whether consisting of change or destruction of structure, or
derangement of function. Vision may be diminished or lost by organic
disease in the coats or humours of the eye, or by morbid formations
in the orbit; but to such the term Amaurosis does not strictly apply.
But, after establishment of the disease, other textures of the eye may,
and often do, become affected. Usually one eye at first is amaurotic;
but the other soon participates, and ultimately vision is impaired or
entirely lost in both. The disease may occur idiopathically, or be
symptomatic of other affections.
The general symptoms of amaurosis are the following. Headache is felt
for some time, either constant, or, as is most commonly the case,
occasional, and most severe in the forehead: in many cases the pain
is at times most excruciating. The eyesight gradually becomes276 weak;
distant objects are unusually obscure, or not at all observed; and
those which are near cannot be accurately discerned. For a short
time vision may seem to be restored, but soon it diminishes more and
more, all objects seem to be enshrouded in a mist, at first thin and
shadowy, but gradually becoming opaque and impenetrable; or a feeling
is communicated of a dark network obstructing the view. Unnatural
impressions are made on the retina; flashes of strong light, or
luminous sparks, appear to dart across the eyes; darkened spots are
seen where none exist; gnats, flies, or other minute bodies, various
in colour and brilliancy, seem to flutter before the face; or a single
dark speck intercepts the vision. Usually the pupil is dilated and
the iris insensible to the stimulus of light; and the former has not
its natural translucent aspect, but is dull and cloudy. But the state
of the pupil cannot be accurately determined in amaurosis, for not
unfrequently it is much contracted, and in many cases the iris retains
both its natural appearance and the full exercise of its functions.
The disease either advances to complete blindness, or stops in its
destructive progress, leaving the patient with vision impaired to a
greater or less degree. When the disease is established, pain in the
head and eyes usually either ceases quickly and entirely, or gradually
abates.
Amaurosis is sometimes temporary, occurring at regular intervals; and,
during its accession, it often varies in intensity. With some patients
strong light is intolerable, and vision is best in the twilight;
others court sunshine, finding their eyesight thereby much improved;
accordingly the former are said to labour under nyctalopia, the latter
under hemeralopia. Some can discern the shape of objects, but either
have no perception of the colours, or mistake the individual colours;
others not only see all objects indistinctively, but conceive them
distorted, double, or extensively multiplied: in some one-half of the
object looked upon is obscured—and frequently there is strabismus, in
consequence of the paralysis being only partial.
Organic amaurosis (that depending on organic disease) may arise from
the change of structure consequent on inflammatory action in the
retina, whether chronic or acute—from atrophy of that membrane and of
the optic nerve—from extravasation into the substance of the nerve, or
compression of it by morbid formations—from softening or suppuration
of the nerve and its connexions—or from various diseases of the
encephalon. Functional amaurosis may proceed from temporary plethora
about the optic nerve and retina—from intense and long continued
use of the organ—from derangement of the digestive apparatus—from
general debility, however induced—from excessive influence on the
system of poisons or powerful medicines—from concussion of the nervous
and cerebral substance, or from long continued irritation in the
neighbourhood of the eye. Amaurosis may also follow injuries of various
kinds.
In the treatment of organic amaurosis but little can be done, and that
little is unsatisfactory. In the functional form, however, vision
may be improved, if not wholly restored, by removal of the exciting
cause, and the carefully avoiding of such circumstances as seem to
predispose to the affection. After due constitutional treatment,
con277siderable benefit is often derived from counter-irritation;
and I have in many cases witnessed the good effects of blistering
the temples and besprinkling the raw surface with the powder of
strychnine,—a practice very far from nugatory. On removing the blister,
the cuticle and lymphatic effusion beneath are carefully scraped
away, and from one-eighth to one-half of a grain of the powder dusted
over the exposed cutis. The sprinkling is repeated daily, and the
dose gradually increased. When the surface dries, a fresh blister
is applied, and the use of the powder resumed. It may be employed,
when gradually increased, to the extent of two grains on each temple;
but, if spasmodic twitchings and constitutional disturbance begin to
show themselves, it must be immediately abandoned, and not resumed
till after some days, and even then in diminished doses. In not a few
cases, both of complete amaurosis, and of vision impaired to such an
extent that the patient could merely distinguish light from darkness, I
have by this practice succeeded in restoring the sight completely; in
others, vision has been very much improved. Still, by far the greater
number of amaurotic patients are incurable; and even those who have
derived benefit from strychnine are, I am strongly inclined to suspect,
exceedingly liable to relapse.
In the treatment of functional amaurosis, it will be necessary to
investigate minutely the causes on which the defective vision may
depend. Thus we may find a congestive state of the retina or brain,
arising from suppressed natural discharges, as the menstrual flux,
or the sudden suppression of habitual but morbid discharges, as the
healing of an old ulcer, &c.
Again, amaurosis maybe the result of irritation in some portion of the
alimentary canal, as from the presence of worms. Patients who have long
laboured under imperfect amaurosis have occasionally been suddenly
relieved by the discharge of a tape-worm. Difficult and painful
dentition in children not unfrequently gives rise to this disease.
Hence the treatment of functional amaurosis will necessarily vary with
the cause; and no general rule can, with any propriety, be laid down as
to our selection of remedial measures.
Glaucoma, or green cataract, is a disease of the hyaloid membrane
and vitreous humour, probably depending on a varicose state of the
bloodvessels. The pupil is usually dilated, irregularly oblong, the
iris being narrowed towards the upper and inner side. There is a
dull shining appearance at the bottom of the eye, not fixed as in
cataract, but varying according to the position of the light. The lens
becomes opaque and greenish as the disease advances, vision gradually
diminishes, and the iris is immovable. After sight is lost, the patient
has a perception of a luminous appearance in the organ when pressed
upon. Both eyes are generally affected, one after the other; headache,
often violent, attends the disease; many remedies, both external and
internal, may be tried on recommendation, though without effect: the
disease seldom, if ever, admits of cure.
Of Cataract, or opacity of the crystalline lens and its capsule,
attended with partial loss of vision.—The disease is, in general,278
gradual in its progress: but sometimes it advances rapidly, as when
occasioned by a blow or wound. When slow, the opacity commences in the
centre of the lens, and extends gradually towards the circumference.
Before any change can be perceived in the organ, the patient sees
objects as if covered with a mist or veil; and, as the opacity becomes
distinct, vision is gradually impaired. During the day, vision is very
indistinct, as the pupil is contracted, and the rays of light reach
the retina only through the opaque centre of the cataract. But during
twilight vision improves, as then the pupil becomes dilated, and
admits of transmission of light through a portion of the transparent
vitreous humour, as well as through the semi-opaque margins of the
crystalline lens: for a similar reason, it is also more distinct after
the application of belladonna or hyoscyamus either to the eye or to
its neighbourhood. In the ordinary state of the parts, a clear black
ring is often visible around the opacity, either from the margins
of the lens being unaffected, or from the posterior surface of the
pupillary portion of the iris being pushed forwards by enlargement of
the lens. Patients, having become aware of the great improvement of
vision caused by dilatation of the pupil, are often contented to use
narcotic remedies externally, so long as they retain their dilating
influence—and, strange to say, they do not soon lose it—instead of
submitting to any operation. As cataract advances, even luminous bodies
cannot be accurately distinguished, though the situation from which the
light proceeds is perceived; thus the patient in a clear light may have
an indistinct perception of a candle or window, and in some cases even
of the bars of the window. The motions of the iris are not affected,
unless, in rare cases, when the cataract is large and compresses the
iris; or when the functions of the third pair of nerves have been
in any way impaired; or when the iris has been the seat of acute
inflammation.
Cataract may be confounded with other diseases of the eye, as with
amaurosis. But, in amaurosis, opacity, when it exists, is deep,
concave, greenish, or of a metallic appearance; whereas, in cataract,
it is of a more or less white colour, convex, and situated immediately
behind the pupil.
Cataract may be lenticular only, the lens being opaque whilst its
capsule remains transparent. In such a case the disease is slow in
its progress, and the opacity uniformly commences in the centre of
the lens, and gradually extends to the circumference. The degree of
opacity varies in different cases, from cloudy dimness to complete
whiteness. In general the predominant hue is white or greyish, but not
unfrequently the opacity is of several colours, and occasionally of a
mottled appearance. The consistence also of lenticular cataract varies,
being sometimes fluid, occasionally extremely dense and almost osseous,
but most frequently of caseous consistence. When fluid, the cataract is
of larger size than the healthy lens; when caseous, the part usually
retains its former dimensions; and when dense, the lens is often
considerably diminished in size. The motions of the pupil are seldom,
if ever, affected.
Cataract may be entirely capsular, the capsule being opaque, whilst
the lens either remains free of disease, or has been removed279 by
natural or artificial processes. The opacity in this case does not
always commence in the centre, but frequently begins at the margin, and
is of a spotted or mottled appearance, and in general not uniformly
opaque. No black ring around the opacity is observed, though the
pupil be dilated; and the motions of the iris are sometimes slow. The
opaque spots are said sometimes to move when the position of the head
is changed. The anterior portion of the capsule, the posterior, or
the whole, may be affected; but the anterior is the part which most
commonly becomes opaque in the first instance.
In many cases both lens and capsule are affected; and then the cataract
is termed capsulo-lenticular. Occasionally the diseased lens, in such
circumstances, is of fluid consistence; and in many cases is spotted.
Portions of lymph, organised or not, lodged in the posterior chamber,
have by some been termed spurious or adventitious cataract; since,
when the pupil is shut by such effusion, the appearances presented are
somewhat similar to those caused by opacity of the lens, or of its
capsule. Such deposits, however, can readily be distinguished from true
cataract, being in general of a yellowish colour, in close contact with
the posterior surface of the iris, and, when organised, often streaked
with red vessels. Generally, too, the pupil is irregular from adhesions
between the lymph and the pupillary margin of the iris.
Cataract would, in some cases, appear to be hereditary,27 and
frequently it is a congenital affection. In very young children it
may be caused by imprudent exposure to strong light. In adults it
often seems to be produced by the action of strong reflected light,
as by exposure to intense fires in forges, glasshouses, &c., or by a
dependent 280position of the head, accompanied with exposure to light.
People advanced in life are most subject to the disease.29 It is not
an unfrequent consequence of internal ophthalmia, and almost invariably
follows the slightest wound or most delicate puncture of the lens: it
often occurs after slight injury of the lens or its capsule, inflicted
during attempts to form an artificial pupil. Cataract may occur rapidly
from extensive dilatation of the lenticular vessels; or from such
an injury of the eye as causes laceration of the vessels supplying
the capsule and lens, detaches them from their other connexions, and
consequently leaves them without a nutritive source.
Cataract sometimes, though rarely, disappears spontaneously, being
absorbed; but most frequently an operation is required to remove the
opaque body from the axis of vision, though no hurry is necessary
in having recourse to it. The chance of success from operation must
depend very much on the state of the different parts of the eye, on
the kind of cataract, and on the state of the constitution. Many
remedies, external and internal, and mercury amongst the rest, have
281been employed with the view of dissipating cataracts; but all are
of no use. An operation, of one kind or another, only can be relied
on. And still, even in favourable cases, and in the best hands, the
contingencies attending operation are so great, that success cannot be
absolutely promised or expected. The mode of operating, and the kind
of operation, must be varied according to circumstances; and great
experience is required to determine the proper course of procedure
in each case. Steadiness is absolutely necessary both in the patient
and the operator, in order that the proceedings may be carried to a
happy conclusion. The operator must have a good eye; a steady, light,
and skilful hand; a fine touch; courage and caution—qualifications
necessary in all surgical operations, and in none more so than in those
on the eye.
When cataract is spontaneous, and vision not altogether lost, the
patient being able to distinguish bright objects, though unable to
direct his steps or follow his avocation—when the pupil is quite
sensible to the application or abstraction of light, or to the use
of belladonna, &c.,—when all the external parts are sound, the
cornea clear, the chambers of the proper size, and no reason to
suspect that the retina is affected—the prognosis in regard to the
effects of operation is good. When, on the contrary, the organ or the
constitution is not sound—when the patient is irritable in habit or
temper, or subject to gouty, rheumatic, or catarrhal complaints—when
headache has preceded the opacity, and vision is gone, or nearly so,
with flashes of light seeming to pass before the eyes—the prognosis
is very unfavourable. But even total blindness must not always be
considered as an indication of operation proving useless, for sometimes
the retina recovers its sensibility after removal of the cataract,
and thus sight has been restored in very hopeless cases. There is
no objection against operating, though one eye only is affected. By
some, operation is recommended as prudent, with a view of preventing
the opposite eye from suffering by sympathy; whilst others consider
it more safe to refrain from operating, lest violent inflammatory
action should follow, and, by extending to the other eye, cause
disease there. However, when the cataractous eye does not present
such appearances as forbid operation, I conceive it both prudent and
safe to remove the obstruction to vision, provided after-treatment is
carefully attended to, and all untoward symptoms actively combated
as soon as they appear. There is still a considerable difference of
opinion on the subject; but the patient, being anxious to get rid of
an inconvenience and deformity, often decides for the surgeon. When
both eyes are cataractous, a question arises as to operating on both
eyes at once. From my own experience I should say, that both eyes ought
not to be operated on at one time: if they are, there is great risk of
violent inflammation being established, and of the operation failing
to restore vision. Immediately after one eye has been operated on,
the other becomes very unsteady, and is altogether in an unfavourable
state for operation; and, if interfered with, the chance of a happy
result is but slight. But by operating on each eye at different times,
much less risk is incurred, and the chance of success282 is doubled.30
Cataract may be operated upon at all ages, excepting infancy and
the period of dentition. In congenital cataract, the eyes acquire
an uncontrollable rolling motion, and, if operation be delayed till
the patient has attained a considerable age, such motion cannot be
afterwards prevented. In such cases, therefore, the disease should be
attacked as soon as dentition is completed, for then an operation can
be undertaken with as little risk of injury to the organ as at a more
advanced age; and a child of twenty months or two years is unconscious
of what is intended, and can be more readily secured than at any after
period; besides the best period for education is lost if an operation
be not done early.31
Cataract is not remediable but by surgical operation. It may be removed
altogether by incision of the tunics of the eye, and extraction of the
opaque body; or by the introduction of a needle, it may be displaced
from the axis of vision, or so disturbed as to be acted on and removed
by the absorbents.
Operation with the needle is more generally applicable than that with
the knife, and is more easily performed. But much mischief may be done
with a needle, if the operator be not both cautious and dexterous; by
unskilful use of it many eyes have been lost.
In operations for cataract on the adult, the patient, having the eye
which is not the subject of operation covered, may be seated on a low
chair, opposite and near to a north window, in order that clear light
may be obtained. His head is supported on the breast of an intelligent
assistant standing behind. The upper eyelid is raised by the
assistant’s fore and middle fingers of the left or right hand, applied
so as to stretch the lid over the bulb; and the other hand is placed
under the patient’s chin, to steady the head. The eye may be very well
fixed by the fingers of the right or left hand of the operator himself.
He is, in that case, more conveniently placed behind or above the
patient’s head. The use of a speculum, for elevating the lid or fixing
the ball, is seldom admissible; and, if the eye be so unsteady or sunk
as to require it, the surgeon ought not to attempt extraction. No one
method can be exclusively followed; by a man of judgment, experience,
and skill, the operation will be varied according to circumstances.
The operation may be performed with the needle. The cataract 283is either
depressed or reclined, and is then said to be couched. Depression
is preferred by many good authorities in surgery. The needle is
introduced at a line—or a line and a half, so as to avoid the ciliary
processes—from the junction of the cornea with the sclerotic, towards
the external canthus, and below the transverse diameter of the eye;
and the opaque lens, if solid, is entangled with the point of the
instrument, and pushed into the lower part of the ball. Thus the opaque
body is removed from the axis of vision, so as not to obstruct the
passage of rays of light to the retina; and, in successful cases, it is
highly probable that the lens, after being detached and displaced, is
altogether removed by the absorbents. Violent inflammation occasionally
takes place after the operation, followed with destruction of the
eye from suppuration; or the iris becomes paralytic; or the pupil
closes, and sight is gradually lost; or the cornea becomes flaccid,
with congestion of the vessels and turbidity of the humours. The
needle should be of a conical form, thickest towards the handle, so
as to prevent the humours from escaping during its introduction. It
should also be straight, excepting a short curvature of its point,
rather slim than otherwise, and not longer than from an inch to an
inch and a quarter. The extracts of belladonna or stramonium should
be used in all cases, previously to determining upon operations, in
order to ascertain the state of the humours, the size of the cataract,
and whether adhesion of the iris to the capsule of the lens exist or
not. Dilatation so produced is allowed to disappear almost entirely
before the operation is proceeded in. It is sometimes necessary to
steady the eye by means of a speculum, and the wire one of Pellier
is the best. By pushing the needle, held like a writing pen, gently
forwards, and towards the inner canthus, in a direction almost parallel
with the iris, its point is seen in the posterior chamber, opposite
the pupil. The instrument is then fixed in the opaque lens, and the
cataract is depressed obliquely downwards; the needle is disentangled
by a gentle twisting motion, and then withdrawn in the same direction
as it was entered. Before depressing, it is necessary to lacerate the
capsule of the lens, and this is accomplished by giving the needle a
rotatory motion, and moving its point in different directions; the
anterior portion of the vitreous humour is at the same time disturbed.
Laceration of the capsule may be too great, and allow the lens to
escape entire into the anterior chamber; inflammatory action is in
consequence excited, and subsides only when an opening has been made
in the cornea, and the offending body extracted. If the cataract
rise to its original situation on withdrawing the needle, it should
be again depressed, and kept down by the instrument for a short
time; and when the needle is then removed, its point should be very
carefully disentangled. The lens is said frequently to regain its usual
situation, a considerable time after the operation; but in many such
cases, the opacity in the pupil is not occasioned by the lens, but
by the capsule having become opaque. It is said to have arisen, when
very solid, twenty or thirty years after depression; and that in many
cases no absorption of it occurs. When the vitreous humour has become
disorganised, the lens often floats about, rising and falling with the
motions of the head.
284
In reclination, the point of the needle is placed on the upper and
anterior surface of the lens; and by raising the handle, and pushing
the point slightly forward towards the inner part of the eye, the
lens is removed from the axis of vision, placed inferior to it, and
has the relative situation of its surfaces changed—its anterior
surface becoming the upper, and the posterior the under; the superior,
posterior; and the inferior, anterior.
Solid cataracts only can be depressed or reclined. When a cataract is
fluid, it is sufficient to puncture, or lacerate slightly, the anterior
part of the capsule; as then the opaque contents will be diffused
through the aqueous humour, and soon removed by the absorbents. Should
the capsule become opaque, after the removal of its contents, the
needle must be at a future period introduced; the capsule is to be
lacerated and reduced to minute shreds, so that it may escape into the
anterior chamber. In the soft or caseous cataract, displacement is not
easily effected; and the surgeon must rest satisfied with exposing a
part or the whole of it to the action of the aqueous humour.
The above operations may be had recourse to when—from diminution of
the anterior chamber, adhesions of the iris, a morbid state of the
pupil, and the temper of the patient—extraction cannot be attempted.
When the cataract is small, it is immaterial how it is displaced;
when large and solid, reclination is to be preferred. The operator is
obliged to decide as to the mode of finishing the operation, after he
has introduced the needle, and thereby ascertained the consistence of
the cataract. If it is so soft as to permit the needle to move in all
directions, it is impossible to displace it; it must be broken up, and
left in situ.
In the mode of operation termed keratonyxis, the needle is introduced
through the cornea, about two or three lines from its margin,32
and the cataract is either depressed or broken up for solution.
Depression through the cornea is, however, an operation not to be
recommended, as the surgeon has much less command over the motion of
his instrument, necessary in this form of procedure, than where it
is introduced through the sclerotic coat. The pupil is previously
dilated by belladonna, and the dilatation should be continued for some
time afterwards. The puncture may be made at any part of the corneal
circumference; it soon heals, and leaves no scar. The operation can be
performed without much disturbance of the organ, and it is applicable
when the cataract is soft or fluid, as in children, or its consistence
doubtful. Young subjects should be placed recumbent during the
operation, and rolled up in a sheet, so that they can have no command
over their limbs.
Extraction, in favourable circumstances, and in dexterous hands,
285is a beautiful operation, and most satisfactory; but ought not to be
undertaken unless the surgeon has perfect confidence in himself. It
can be resorted to only in adults, great steadiness on the part of the
patient being absolutely necessary. The case, too, must be judiciously
chosen. The conjunctiva must be sound, and indeed almost no operation
on the eye should be undertaken unless this membrane is in a healthy
condition; the cornea should be transparent in every part—the anterior
chamber of a proper size—the pupil regular—the iris steady, and not
protruded—and the cataract solid; there should be no rolling motion of
the eyeball, and no adhesions of the iris. I repeat, the iris should
be steady, for a tremulous motion of it indicates disorganisation
and fluidity of the vitreous humour; in such a case, the humour can
with difficulty be prevented from escaping; or the lens may fall
into the bottom of the eye, and all efforts to remove it will then
prove abortive. And though such descent of the lens should not occur,
still the organ is in a very unfavourable state for operation, being
apt to become affected with deep inflammation, followed by complete
amaurosis, or by closure of the pupil. The patient is prepared for
the operation by moderate living, and attention to the secretions and
digestive organs, for some time previously; and after the operation
leeching may be necessary either as a precautionary measure, or when
inflammation has occurred. Immediately before having recourse to any
of the operations for cataract, a small blister may be applied with
advantage behind one or both ears, and kept open for some few days,
as a precautionary measure against inflammatory action in the organ
operated upon.
The operator is usually seated immediately before the patient, and
so that his breast may be on the same level with the patient’s head;
if not ambidextrous, he may often be obliged to assume very awkward
attitudes. The recumbent position, however, is preferred by many
operators, and has the great advantage in the superior steadiness of
the head of the patient. The hand of the surgeon may also be rested on
the back of the couch, as, if ambidextrous, he will invariably take
his position behind the patient, in order that he may have the command
of the upper eyelid in his own hands. The incision is made either in
the lower or upper half of the cornea. The knife should have a very
keen edge, and become gradually broader and thicker, from its point
backwards: in using a narrow instrument there is danger of the aqueous
humour escaping. The best knife is Beer’s, well made. The light must
be good, the patient’s head completely steadied, the eye well fixed by
the fingers of the assistant, and the other one covered by a bandage.
No speculum should be employed, and the pupil should not be dilated by
belladonna. The surgeon, supporting his elbow on his knee, or resting
his fingers on the cheek of the patient, holds the knife like a writing
pen—in the right hand, if the left eye is to be operated on, in the
left, if the opposite (that is to say, if he sits before his patient:
if, however, he places himself behind, this must be reversed)—and
ascertains the steadiness of the organ by touching the cornea gently
with the side of the knife. The cornea is punctured about a line from
its margin, and near the outer extremity of its transverse diameter,
the point of the knife286 being directed towards the centre of the eye,
lest it should enter between the laminæ. The knife is then passed
through the anterior chamber, with its side parallel to the iris, and
its point is brought out at that part of the cornea exactly opposite
to where it entered: transfixion is thus completed, and by pushing
the knife steadily forward, without any sawing motion, a semicircular
section is effected. As soon as transfixion is accomplished, the
operator has complete command of the eye, and all pressure should be
taken off—the assistant should now merely keep the eyelid raised.
Should the edge of the knife not come easily through the cornea, its
passage maybe assisted by pressure with the finger-nail.
After the pupil has been allowed to dilate, by covering the eye for
a few seconds with the hand, the capsule must be opened sufficiently
for the escape of the lens. The eyelids are gently raised, a fine
curved needle, or curette, is introduced through the incision, and by
it a crucial wound is made in the capsule. The lens is then either
entangled in the point of the needle and withdrawn, or very gentle
pressure is made on the globe, so as to force out the lens; and, should
it not readily pass through the wound of the cornea, it can be removed
from the anterior chamber by a small scoop. After removal, the eye is
allowed to rest; then careful examination is made; and, if any opaque
substance remain, it is extracted by the needle or scoop. If the
capsule is opaque, it must be taken away along with the lens. Before
closing the eyelids the corneal flap should be carefully adjusted, and
any matter lodged between the divided surfaces removed: loose eyelashes
are to be taken away, inverted ones should be previously extracted, and
the margin of the lower lid should be so placed as not to disturb the
flap.
In transfixion, the point of the knife should not be brought out too
low, nor too much towards the centre of the cornea; and care should be
taken to avoid entanglement of the iris. When the iris falls forward so
as to come under the edge of the knife, and be in danger of division
should transfixion be proceeded in, pressure may be made on the cornea,
so that the remaining aqueous humour may repress the iris from its
untoward situation; or the knife may be withdrawn, and the operation
delayed till the eye has become quiet, and the inflammation, if any,
has subsided; or the incision may be completed with a blunt-pointed
narrow knife, or with probe-pointed scissors. Division of the capsule
by the point of the knife during transfixion has been practised; but
it is an unsafe, though dexterous, measure. In opening the capsule
care should be taken not to separate its attachments, otherwise it
will become opaque, and thereby passage of light to the bottom of the
eye will be again obstructed. Neither should much pressure be used for
extrusion of the lens; for, in the case of a large and firm cataract,
the iris may be lacerated, and the humours escape. When any of the
vitreous humour has escaped, in consequence of its cells having been
broken down, and its tenacity diminished, the eye soon fills again, but
good vision is hardly to be expected.
After the operation, applications to the eye should be very light; a
rag dipped in cold water, and renewed occasionally, is sufficient.287
All stimulants of the organ, as light, should be avoided, and
antiphlogistic treatment adopted. Should violent pain supervene,
bleeding, both local and general, and other means for subduing
inflammatory action, must be had recourse to. The eyelids should not
be raised or exposed for at least three days, unless in extraordinary
circumstances. Belladonna is of use when gradual contraction of the
pupil occurs. In very favourable cases, vision is completely restored
in the eye; in others, the functions of the two eyes do not correspond,
and vision is confused: the patient requires to wear a convex glass
before the one which has been operated on.
The operation of making an artificial pupil is far from being
uniformly successful, and ought not to be had recourse to unless vision
is entirely lost, or so much impaired as to be insufficient for the
guidance of the patient’s steps. It is necessary on account of central
opacity of the cornea—leucoma with entanglement of the iris—and entire
 closure of the pupil, or diminution of it, with concealment of the
remainder by corneal opacity. It may be required after badly performed
extraction of a cataract, the iris being entangled in the scar of
the incision, at a distance from the junction of the cornea with the
sclerotic; or on account of closed pupil from inflammation, when,
perhaps, the cornea is all clear. The operation is varied according
to the size of the anterior chamber, the presence or absence of the
crystalline lens, the extent of sound cornea, and the condition of the
iris. Interference is useless when disease of the retina is suspected,
from the extent of the previous disease—from violent inflammation, with
or without discharge of part of the contents of the eyeball. Three
distinct methods of operation are pursued.
closure of the pupil, or diminution of it, with concealment of the
remainder by corneal opacity. It may be required after badly performed
extraction of a cataract, the iris being entangled in the scar of
the incision, at a distance from the junction of the cornea with the
sclerotic; or on account of closed pupil from inflammation, when,
perhaps, the cornea is all clear. The operation is varied according
to the size of the anterior chamber, the presence or absence of the
crystalline lens, the extent of sound cornea, and the condition of the
iris. Interference is useless when disease of the retina is suspected,
from the extent of the previous disease—from violent inflammation, with
or without discharge of part of the contents of the eyeball. Three
distinct methods of operation are pursued.
I. Simple division of the iris, or corotomia, may be practised
when the iris is stretched, as after extraction. It is performed by
introducing a small knife, like a needle, through the anterior or
posterior chamber,—the surgeon being in this regulated by the size of
the anterior chamber and the presence or absence of the lens,—pushing
 its point through the iris, or cutting that membrane vertically,
horizontally, or both, to an extent sufficient for the transmission of
light. If the anterior chamber be of its natural size, a small opening
may be made in the cornea with a cataract knife, or a double-edged
broad and thin one; and through this opening small scissors may be
introduced for division of the iris.
its point through the iris, or cutting that membrane vertically,
horizontally, or both, to an extent sufficient for the transmission of
light. If the anterior chamber be of its natural size, a small opening
may be made in the cornea with a cataract knife, or a double-edged
broad and thin one; and through this opening small scissors may be
introduced for division of the iris.
II. Corectomia, or cutting out a portion of the iris, so as to make
the opening oval, square, or angular. This is performed by introducing,
through an aperture in the cornea, scissors and forceps, or hooks,
double or single—the latter to lay hold of the iris, the former to
divide it. After the escape of the aqueous humour, a portion of the
iris may be made to protrude; and, on288 the projecting portion being cut
off, the membrane, with a proper opening in it, regains its natural
situation, in consequence of discharge of the humour from behind.
This operation is applicable only in few cases; the whole, or the
greater part, of the cornea must be clear, and the anterior chamber not
diminished in size, so that sufficient room may be afforded for the
introduction of instruments between the iris and the concave surface of
the cornea.
In those cases where the natural pupil remains along with a still
transparent lens, while vision has been destroyed by a central opacity
of the cornea, the use of sharp and pointed instruments is forbidden.
Sharp hooks or scissors would endanger wound of the crystalline, and
the case becoming complicated with traumatic cataract. The blunt hook,
as proposed and used by Mr. Tyrrell, is here to be preferred. A small
opening is made through the cornea, as the most convenient part, and
the hook carefully introduced and entangled in the existing pupil: the
iris is then drawn to the corneal wound, and either left entangled in
the section, or removed by a pair of curved scissors. A pupil is thus
formed opposite to the remaining transparent portion of the cornea.
III. Corodialysis, or separation of the iris from its ciliary
attachments, is the method most easily performed, and most generally
applicable. The eye is fixed either with the fingers or with a
speculum; and a curved needle, perhaps more curved than that usually
employed for cataract, is introduced either behind or before the
iris, and at the upper, outer, inner, or lower part of the ball, as
circumstances may require. An artificial pupil at the lower part is by
much the most useful; but, if the lower part of the cornea is opaque,
it must be made opposite to the inner or outer clear part. The point
of the needle is entangled in the attached margin of the iris, and by
raising the hand quickly, and partially withdrawing the instrument, the
connexions are separated to a sufficient extent. Effusion of blood into
the chamber, and to a considerable extent, follows these proceedings;
and it is only after its absorption that it can be ascertained whether
benefit is likely to result or not. After all these operations,
inflammatory action requires to be kept down by antiphlogistic
measures, abstraction of blood, purgatives, antimonials, and, perhaps,
mercurial preparations. It is questionable whether belladonna can be
useful in preventing closure of an artificial pupil.
Wounds of the Eyeball and its Neighbourhood.—Wounds near the eye,
though unimportant in themselves, require considerable attention,
on account of the eye, or its appendages, being likely to suffer in
consequence. Thus, transverse wounds of the forehead or eyebrow,
if their edges be not approximated accurately and soon, may cause
prolapsus of the eyelids; or the eyelids may become swollen and turgid,
or erysipelatous, in consequence of inflammatory action attacking the
wound. When wounds of the forehead are in a perpendicular direction,
their margins are easily preserved in apposition, having little
tendency to retract, and there is no risk of the relative situation of
the eyelids being altered. If there be considerable loss of substance
in the lower part of the forehead, from the nature of the289 wound, when
inflicted, or from its having become the seat of unhealthy suppuration,
on cicatrisation of the part the eyelid will be drawn upwards, and
perhaps more or less everted. There is reason to believe that a
degree of blindness, and even complete amaurosis, has been caused by
wound of the eyebrow, the superciliary nerve having been contused,
wounded, or otherwise injured; or the functions of the eyeball may be
disturbed by concussion from injury. Paralysis, also, of the levator
palpebræ superioris, or of several of the muscles belonging to the
eyeball, may follow injury of the forehead and neighbouring parts,
from either laceration or concussion of the nerves. Wounds of the
eyelids, particularly when neglected, may cause much change of relative
situation in the parts, and thereby produce both inconvenience and
deformity. In some instances, the relative position of the puncta
lachrymalia is altered by the cicatrices of the eyelids or tarsal
cartilages, when the original wound has been imperfectly adapted: hence
results an incurable epiphora.
In wounds, such as those above mentioned, it is of great importance
to bring the raw edges into contact, and retain them so; and, in most
cases, one or more points of interrupted suture are necessary. Adhesive
plaster may be at the same time applied, but of itself is insufficient
to effect permanent coaptation.
Wounds of the eyeball, however slight, require much attention, being
inflicted on an important and highly sensible organ, and there being
always a risk of destructive inflammatory action. If the breach of
surface be clean, simple, and superficial, rest of the parts will in
general be sufficient to effect a cure. Lacerated wounds, and such
as penetrate into the interior of the eyeball, cannot be expected to
heal without morbid action having been excited: inflammation must be
anxiously looked for, and actively combated as soon as it appears.
When a foreign body lodges in the wound, it must be early removed.
But in certain cases it is imprudent to attempt extraction of foreign
matter; as when a small shot, or other minute substance, has lodged
in the interior of the eyeball. In such circumstances we can only
adopt such measures as prevent and subdue morbid excitement. The
organ may remain little disturbed for a short period, but violent
inflammatory action soon occurs, and, though subdued for a time,
again breaks forth, and, by its successive attacks, may ultimately
destroy the eyeball. Frequently all endeavours to avert untoward
results are unavailing, and the functions of the organ are more or
less impaired—the cornea may become opaque, the iris may protrude, the
pupil may become irregular, contracted, or obliterated—the crystalline
lens may lose its transparency, amaurosis may occur from injury of the
retina, the humours may be evacuated, and the eye sink in its socket.
The entrance of a large foreign body into the orbit may displace the
globe, and cause it to protrude between the eyelids: in such a case
the body should be removed and the ball gently replaced; vision may be
soon regained; but, if the protrusion has been such as to cause much
stretching of the optic nerve, blindness more or less complete remains.
Fatal effects may follow wound of the eye, on account of the foreign
body, as a sharp-pointed instru290ment, penetrating the thin parietes of
the orbit, splintering the bone, and injuring the brain.
Orbital Inflammation.—Inflammation seldom attacks the parts situated
between the orbit and the eyeball; but, when it does, the affection
is very serious. The action is very acute, and proceeds rapidly to
suppuration. The pain is excruciating, extends to the whole head,
accompanied with a sensation of extreme tension in the orbit, and is
much increased by the slightest motion of the eye: and from the matter
accumulating around the ball, and being confined to the unyielding
orbit, by the dense fibrous expansion which extends from the margin of
the orbit to the interior surface of the eyeball, the globe is pushed
forwards, and distends the lids. The palpebræ become erysipelatous,
and swollen by serous effusion. Violent inflammatory fever occurs;
and, as the disease advances, all the symptoms are aggravated, and
become almost intolerable. The globe is farther protruded, and the
retina is insensible to light. At length the accumulated matter makes
its way to the surface, and is discharged, giving great relief to the
patient, and permitting the protruded globe to regain its situation.
The inflammation seldom extends to the eyeball.
In the early stage of this affection, the most decidedly antiphlogistic
measures are imperiously called for. When fluctuation can be felt,
or when the symptoms indicate that suppuration has taken place,
whether fluctuation is perceptible or not, an early opening into the
affected part should be made through the dense orbital ligament. Thus
a free exit is allowed for the matter, the patient is instantaneously
relieved, and the extent of the local mischief is limited. It is unsafe
to wait for the spontaneous evacuation of the matter: such a process
is necessarily tedious, and, before it has been accomplished, the
orbital bones may have become diseased; they may have given way at
certain points, and the matter may have escaped within the cranium. The
artificial opening should always be free, and deep if necessary.
Tumours in the Orbit.—Sarcomatous tumours occasionally form in the
cellular tissue of the orbit. They occur at all periods of life, and
may, by slow and gradual increase, cause the eyeball to protrude and
disturb its functions; or their growth is rapid, and accompanied with
great suffering. In some cases, the eye is made to protrude to a great
degree, and by the extension of the optic nerve vision is impaired;
in others, the patient is totally blind at the commencement of the
disease. Yet the eye may be displaced to no small extent without
amaurosis following. The optic nerve appears to bear a good deal of
extension without disturbance of its functions. The majority of tumours
in this situation are of rapid growth, their structure is soft and
medullary, they sooner or later furnish a fungus, and, though removed
at an early period, are generally reproduced. The exophthalmos is often
the first indication of such a growth, and it is sometimes greater in
the early part of the disease than afterwards, when the fascia passing
down from the edge of the orbit has given way. The malignant tumours
are most frequently met with in childhood, though morbid growths of a
bad kind form in the eye291ball at different periods of life. They often
follow the infliction of a blow or wound. The patient’s sight speedily
declines, without any known cause; there is pain in the forehead,
temple, and eyeball; the ball protrudes, perhaps slightly, and at
first is not otherwise changed; but on careful examination a dimness
can be perceived deep in the eye. The opaque body approaches the pupil
and fills it, and may in this state be mistaken for disease of the
crystalline lens; but the tumour soon pushes forward the iris, and
fills the anterior chamber. It has an irregular surface covered with
flocculi. Blood-vessels are observed ramifying on it, and by this it
is distinguished from cataract, should the accompanying symptoms not
have previously convinced the surgeon of the nature of the disease.
If not interfered with, the cornea ulcerates, a fungus appears, often
grows with great rapidity, and may either furnish not a drop of blood,
or bleed profusely. The eyelids are œdematous and permeated by large
venous branches. Abscesses form around; the lymphatics of the neck are
involved; and the patient succumbs. The original tumour may possess the
usual structure of medullary sarcoma, may be of a melanotic nature,
or may contain a mixture of both; or it is of harder consistence,
containing cells filled with bloody, glairy, or other fluid. The
whole coats of the eye are seldom involved: part remains sound, but
compressed and disfigured by the morbid mass, and the humours are
either absorbed or discharged.
Circumscribed tumours, exterior to the ball, and surrounded by a
cellular cyst, may be removed by careful and cautious dissection,
without injury to the important parts. A free incision is made along
the edge of the orbit, in the course of the fibres of the sphincter
oculi. The tumour is exposed, laid hold of with a hook or small
vulsellum, and separated from its attachments by a knife, the edge of
which is directed towards the new growth. A man, aged 26, had laboured
under blindness with exophthalmos for eighteen months. A tumour could
be felt above the eyeball, which I dissected out, along with the
lachrymal gland, to which it adhered. It was of medullo-sarcomatous
structure, and of the size of a plum: at one point it contained a mass
of coagulated blood. After its removal, the eye resumed its place and
functions. The patient remains well; but such favourable cases are rare.
If the affection be more extensive, it may be necessary to remove
all the contents of the orbit: but, in disease involving the entire
structures, there is little chance of the patient remaining free from
it: it almost uniformly returns, as is also the case whenever the
disease has commenced in parts of the eyeball. The optic nerve is
often affected at an early period: its cut surface is unsound; and
from this, again, springs a fungus which grows rapidly. But under many
circumstances the surgeon is not only justified in removing the orbital
contents, but called upon to do so. The operation, though cruel and
painful, need not be tedious. The commissure of the eyelids is divided
with the point of a bistoury, and the forepart of the ball laid hold
of firmly and deeply with a vulsellum—that is, forceps provided with
a double hook at each extremity of the blades. A straight bistoury
is then entered at the margin of the orbit, pushed down to the base,
as near as possible to the entrance of the optic nerve, and292 carried
round the tumour rapidly, the blade towards the handle being made
to move more quickly than the point. The nerve is cut across, and,
after the removal of the morbid mass, the cavity is sponged out and
examined. The lachrymal gland, and other soft parts, particularly if
altered in texture, are raised with a hook, and removed by means of
curved scissors. In young subjects, and in adults, when the disease
is far advanced, the parietes of the orbit are thin, softened, and
attenuated by pressure: the knife should therefore be used cautiously,
and it is, perhaps, safer to finish excision with a narrow, curved,
and probe-pointed bistoury, after having penetrated to the bottom of
the orbit with a sharp-pointed knife: all other curious and crooked
knives are useless. Bleeding is restrained by charpie, pressed firmly
and quickly into the cavity, and supported by compresses and bandage;
but, before introducing the dossils, all coagula and fluid blood should
be carefully sponged out. Afterwards, excited vascular action, with
pain in the head and wound, may in some subjects require abstraction
of blood, the exhibition of purgatives and antimonials, and immediate
removal of the dressings, followed by fomentation and poultice. When
matters proceed favourably, the charpie is removed gradually as
suppuration advances, and the granulations are supported with light
dressing, either dry, or moistened with some slightly astringent
lotion. The discharge will gradually cease, and the granulated surface
cicatrise under the level of the eyelids. In such circumstances the
deformity may be remedied, after the parts have become quiet, by the
adaptation of an artificial eye of enamel, made so as to resemble
exactly the other eye. It is worn without inconvenience, removed at
night like artificial teeth or a wig, and cleaned and replaced in
the morning. Such a substitute is also useful when the humours have
been evacuated, or the organ destroyed, by injury or the effects of
inflammation. Too frequently the morbid growth is reproduced, and that
rapidly. It may be restrained by escharotics, the red oxide of mercury,
potass, acetate of lead, acids, or the actual cautery; but the patient
is thereby put to much pain without a chance of ultimate benefit.
It is too true, that the hopes of a cure, after the extirpation of the
eyeball for malignant disease, are defeated by the prior existence
of a similar affection within the cranium. In the majority of cases,
death has occurred from tumours of greater or less extent, along the
course of the optic nerve, or their tract: behind the commissure, and
extending to the optic lobes and even cerebellum.
[STRABISMUS.
Strabismus, or squint, as it is vulgarly designated, may be defined
to be an aberration from the natural direction of the optic axes, by
which the consent between the eyes is destroyed, and vision more or
less impaired. The resulting deformity varies in different cases,
from the slightest possible cast to the most disagreeable obliquity.
The affected organ may be turned inwards or outwards, upwards or
downwards, according to the muscle upon the derange293ment of which
the squint depends. When the eye is directed inwards, it constitutes
what is called convergent strabismus; if, on the other hand, it
inclines outwards it is said to be divergent. The upward and downward
obliquities have not received any particular names. As might be
supposed, these different forms of strabismus do not occur with equal
frequency. On the contrary, two of them are so rare that I have not
yet met with an instance, though I have examined the eyes of a very
considerable number of persons labouring under this infirmity. These
two forms are the upward and downward, both of which, but especially
the latter, are so seldom witnessed that their occurrence may well be
doubted, except as the result of external violence.
The most common variety of strabismus by far is the convergent, in
which the eye is directed inwards, or inwards and upwards. Of 536
cases collected from various sources by a writer in the Philadelphia
Medical Examiner, 506 were of this description, a proportion which
fully accords with my own but more limited observation. The degree of
obliquity may be very moderate, or so great that when the person looks
directly forwards with the sound eye the cornea of the other shall be
almost entirely concealed at the inner canthus. It is worthy of remark,
that in this form of the lesion, at least so far as my own experience
goes, the organ rarely, if ever, inclines downwards, but nearly
constantly somewhat in the opposite direction.
Next in point of frequency is the divergent form, which, however, is
comparatively rare. Of 866 cases reported in the work above alluded
to, it was noticed only forty-four times; and thus far I have myself
seen only three or four examples of it. The eye in this variety of
strabismus is seldom drawn out very far, nor is it so apt to be
attended with the same amount of upward obliquity as the convergent.
It seems to be the general sentiment of writers on strabismus, that, in
the great majority of cases, only one organ is affected. Thus, in the
article in the Philadelphia Examiner, before adverted to, it is stated
that the distortion occurred 459 times in one eye, and only 47 times
in both. Dr. Dix, of Boston, in a small treatise on strabismus, makes
a similar remark. Of 50 cases which fell under his notice, the lesion
is said to have been limited to one eye in 36. Now I am convinced from
a good deal of experience that nothing can be more unfounded than this
opinion, which is to be deprecated the more because it is calculated to
lead to very serious errors in practice. I unhesitatingly assert, that
in nearly all instances, at least of convergent squint, both organs are
implicated, though not in an equal degree. Usually—perhaps always—one
is more affected than the other, which the patient, therefore, regards
as his good eye, as it is the one which he constantly employs in
viewing objects. Nor is it surprising that this should be the case,
when we recollect the remarkable sympathy existing between these
structures, and the fact that when one eye is diseased the other is
very liable to take on morbid action also. Amaurosis of one eye is very
often followed by a similar malady of the other, and the same is true
of cataract and some other affections. In the natural state there is a
perfect agreement between294 the optic axes, produced by the harmonious
action of the straight muscles, but when this consent is destroyed,
as it is in strabismus, the eyes lose their parallelism, and the
distortion in question is the consequence.
As was previously intimated, one eye is commonly more affected than the
other, and this, if I mistake not, will be found to be the left, though
it is impossible, in the existing state of the science, to indicate
the proportion. Mr. Lucas thinks that the proportion in favour of the
left eye is as three to two; Dr. Phillips of Liège, on the other hand,
maintains that the right organ is more frequently involved than the
other. It rarely happens that both eyes become deranged simultaneously;
on the contrary, one generally squints first, and after a while the
lesion begins in the other, the interval being probably very short.
Whether strabismus occurs with equal frequency in both sexes, is still
an unsettled question. Of thirty-two cases on which I have operated,
only five were females, whereas in the fifty cases published by Dr.
Dix, of Boston, only nineteen were males, thus exhibiting a most
remarkable disparity in reference to this point. The difference, if
any, is perhaps not great either way, and, as it is of no practical
importance, it need not be pursued any farther here.
The exciting causes of this affection are numerous and diversified. One
of the most frequent is imitation. Nearly one-seventh of all the cases
that occur are probably induced in this manner. Hence our schoolrooms
may be regarded as a fruitful source of mischief, one cross-eyed child
being often the cause of strabismus in many others, merely from that
habit of imitation to which the young are so much addicted. Ophthalmia,
by whatever cause induced, is another, and that a very common source
of this distortion. I have seen repeated instances of this kind, and
many others are mentioned by authors. Convulsions, eruptive diseases,
such as measles and scarlet fever, hooping-cough, derangement of the
digestive organs, injury on the eye, and difficult dentition, may all
be enumerated as so many causes of the lesion in question. Frequently
it arises without any assignable reason, and when the individual is in
the most perfect health. Occasionally it is congenital, or, what is
more probable, makes its appearance within a few days after birth.
It is supposed that strabismus is occasionally hereditary. This is
doubtful; for if we sometimes meet with cross-eyed children whose
parents, one or both, are similarly affected, it by no means proves
that the distortion was transmitted to them in the manner of certain
maladies. It only shows a coincidence, which may be explained, in
most instances, on the assumption that the children have acquired
the obliquity by imitation, or by some other cause, not that it was
entailed upon them previously to birth. In the same manner we may
satisfactorily account for the existence of strabismus in several
members of the same family, of which a remarkable instance has recently
come under my own observation. Of three brothers, one has three
children affected with it, another two, and a third one. The parents
have all sound eyes, and so have the uncles and aunts, except one,
on whom I operated successfully several months ago.295 Last autumn I
operated for cataract on three children belonging to a gentleman from
Mississippi, who informed me he had six others at home, of whom three
were affected with strabismus. Both parents, as well as their immediate
relatives, are free from the affection.
Strabismus essentially consists in a contracted state of one or more
of the muscles of the eye. This, as was before intimated, is commonly
the internal rectus. The shortening, varying according to the extent
of the squint, is always attended with a corresponding elongation of
the opposite muscle, so that it gradually loses, either in whole or
in part, its antagonising influence. How this affection is brought
about, in the first instance, is still unknown, though it is probable
that it depends upon some lesion of the nerves which supply the
muscles of the eye, rather than upon any actual lesion of these fleshy
bundles themselves. Be this as it may, when the resultant distortion
is permanent, the affected muscle, from being constantly engaged in
holding the eye in its unnatural position, acquires a corresponding
degree of development, in accordance with a law of the animal economy
that, in proportion as an organ is exercised, will be its size and
strength. The more frequent occurrence of convergent strabismus is
owing, doubtless, to the fact that the internal straight muscle is not
only larger and stronger than the others, but that it is inserted much
nearer the cornea, deriving thus two important mechanical advantages.
One of the most disagreeable effects of strabismus is the deformity
to which it leads, rendering the individual an object of constant
observation and ridicule. Were this confined to infancy and childhood,
it would be of comparatively little consequence, but when we reflect
that it continues through life, and that it is a source of incessant
mortification, the influence which it exerts upon the temper and
disposition of the sufferer must often be of the most unhappy kind. A
still more serious effect, however, is the impairment of the vision
of the affected eye, which, never entirely absent, sometimes amounts
nearly to a total loss, from the insensibility of the retina, which is
sometimes as complete as in confirmed amaurosis. In another series of
cases the person is myopic, or sees objects only at a short distance.
In some instances, again, there is double vision, or objects appear
indistinct, and run as it were into each other, the image painted on
the retina being confused and imperfect.
The distortion in question can be remedied only by a surgical
operation, it having no tendency to a spontaneous cure. On the
contrary, it generally manifests a disposition to increase,
particularly in children of a nervous, excitable temperament. In fact,
the very worst forms of squint I have ever witnessed were in persons
of this description. The question then arises, at what age ought we
to operate? My opinion decidedly is the sooner the better. Provided
the child be in good health, and not under one year of age, I would
not hesitate a moment to resort to the knife for its relief. And why
should we? The operation itself is not particularly painful, and if it
be done at an early period it will commonly be necessary to perform
it only on one eye, whereas if it be postponed until the age of ten
or twelve, as some have suggested, we shall not be able to effect a
cure without296 dividing the corresponding muscle of the opposite side.
Moreover, the sight in the meantime will become considerably impaired,
the retina will lose its insensibility, and the individual be an object
of ridicule and insult; all of which may thus be obviated. But it may
be urged that a resort to the knife at this tender age will be both
difficult and dangerous; difficult, because of the struggles of the
little patient, and dangerous, because of the great susceptibility of
the nervous system. In regard to the first of these points, it may
be stated that the resistance, however great, may be easily enough
surmounted by proper management; and, as it respects the latter,
that it has been vastly overrated. Operations much more severe are
frequently performed even at a much earlier period. I have seen the
primitive carotid artery successfully tied in an infant of less than
six months; and I have myself repeatedly operated, with similar
results, for harelip, and that too in the very worst forms of that
malformation. I do not, therefore, in these objections, see sufficient
reason for deferring the division of the affected muscle.
The instruments which I employ for the operation, are two lid-holders,
a double sharp-pointed hook for fixing the eye, a pair of dissecting
forceps for pinching up the conjunctiva, and a scalpel or pair of
scissors. The surgeon should also be provided with two or three small
sponges and a basin of cold water.
The lid-holders (Fig. 1.) are each about six inches long, made of steel
with an ivory handle, quite slender, and curved at the extremity, which
is fashioned after the manner of a fenestrated speculum, and not more
than a third of an inch in width. These instruments may be conveniently
replaced by a common speculum and the fingers of an assistant: still,
they are very useful, and I prefer them to any other contrivance. The
hook for fixing the ball is double (Fig. 2.), resembling that contained
in some of the older eye-cases. It ought not to exceed five inches in
length, and should be provided with a movable slide, to allow of the
proper separation of the branches, each of which, two lines in width,
terminates in a short hook as delicate as the finest needle. The
forceps need not be quite the ordinary size; and, as to the scissors,
the common pocket-case pair will answer the purpose much better than a
curved or more delicate instrument. The knife I rarely use. A curved
director (Fig. 3.) is serviceable, as it enables the operator to judge
of the extent of his incisions.
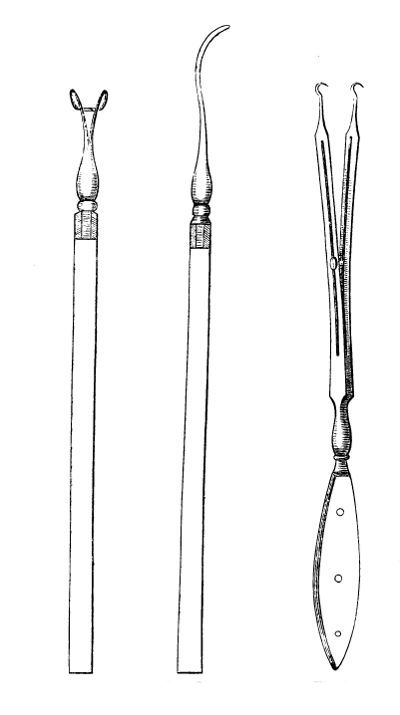
In performing the operation, the patient may be either in the
semi-erect or reclining posture, with his head supported by an
assistant, or properly elevated by pillows. I generally prefer the
latter, as the eye is more manageable, and the patient less apt to
faint than when sitting. The face should look towards the light, and
the sound eye be covered with a bandage, to enable the patient the
better to roll the other outwards. If the surgeon be ambidexter, it
does not matter where he stands: but if he uses one hand more adroitly
than the other, he should place himself on the right side when he
wishes to operate on the left eye; and, conversely, on the left if he
wants to operate on the right. Only two assistants are necessary; one
of whom, standing at the head of the patient, elevates the upper lid,297
and fixes the eye by inserting the sharp hook into the sclerotic coat,
about two lines behind the cornea: the branches of the instrument
being separated one-fourth of an inch, and the interval between them
accurately corresponding with the horizontal axis of the eye. This
precaution is important, and should never be neglected, otherwise it
will by no means be so easy to find the affected muscle. The points
of the hook should be fairly implanted into the substance of the298
sclerotic tunic, but no more. If it be passed simply through the
conjunctiva, it will be impossible to steady the eye, to say nothing
of the danger of lacerating that membrane, and thus inflicting
unnecessary pain upon the patient. On the other hand, if it be pushed
through the fibrous coat, violent inflammation might be set up. The
other assistant, placed on the side of the affected eye, depresses the
lower lid, and hands the sponges to the operator. It is sometimes more
convenient to let this assistant steady the eye.
Everything being thus arranged, the operator pinches up a small fold of
the conjunctiva, just behind the hook, or, in other words, about three
lines behind the cornea, and makes a vertical incision into it with the
knife or scissors, as he may prefer. Relinquishing the forceps, the
edges of the wound will at once retract, exposing thereby a surface
from four to six lines in length by two or three in breadth. At this
moment there is usually some degree of hemorrhage, amounting often to
more than half a teaspoonful, especially if the incision has been made
too far back near the semilunar valve, where the parts are always more
vascular than further forward. To arrest this a small sponge, pressed
out of cold water, should be repeatedly applied; or, if it prove
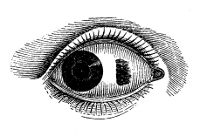 troublesome, the operation may be suspended until it ceases. The ocular
fascia33 is next divided, when the muscle, now fairly exposed, is to
be cut across with the scissors, one of the blades of which is passed
behind it. The moment this is accomplished, the eye, from the force
exerted upon it by the hook, springs towards the opposite side, and the
muscle retracts within its sheath, especially if it has been thoroughly
liberated from its connexions with the surrounding parts. To effect
this, which I regard as of paramount importance, the scissors should be
carried for some distance around the ball, nearly as far, indeed, as
the margins of the adjacent straight muscles.
troublesome, the operation may be suspended until it ceases. The ocular
fascia33 is next divided, when the muscle, now fairly exposed, is to
be cut across with the scissors, one of the blades of which is passed
behind it. The moment this is accomplished, the eye, from the force
exerted upon it by the hook, springs towards the opposite side, and the
muscle retracts within its sheath, especially if it has been thoroughly
liberated from its connexions with the surrounding parts. To effect
this, which I regard as of paramount importance, the scissors should be
carried for some distance around the ball, nearly as far, indeed, as
the margins of the adjacent straight muscles.
As soon as the affected muscle is divided, the eye usually at once
resumes its natural position in the orbit, moving, if the other be
sound, in perfect harmony with it. Occasionally, however, it retains
some degree of its original obliquity; in which case it becomes
necessary to reapply the instruments, to ascertain the cause of it.
This will generally be found to depend upon an imperfect division of
the muscle, or of the surrounding cellular tissue, by which the muscle
is prevented from retracting sufficiently within its sheath. In some
instances it remains without any assignable cause, but rarely beyond a
few minutes, or, at farthest, a few hours.
The operation being over, the eye is bathed in cold water, to rid it of
any blood that may remain in the wound, and the patient is con299fined in
a dark apartment. Low diet should be enjoined for a few days, and, if
inflammation arise, recourse must be had to antiphlogistic measures. In
no case have I yet been obliged to abstract blood; a dose of aperient
medicine being all that was required. Locally cold or tepid water may
be used, as may be most agreeable to the patient’s feelings. When there
is a good deal of pain in the eye, with more or less constitutional
disturbance, such as slight shivering, headache, and nausea, warm
drinks and an opiate will be required. The ecchymosis which attends
this operation, and which is sometimes considerable, demands no
particular treatment: no inconvenience arises from it, and it commonly
disappears in a few weeks. I have never known suppuration or abscess
to follow the division of the muscles of the eye; such an occurrence
implies unusual violence, and cannot be too much condemned. The same
remark is applicable to the wounding of the sclerotic coat, and the
escape of the humours of the organ; an accident which has happened
several times in the hands of ignorant bunglers.
A few hours after the operation is completed, the margins of the
incision become coated with coagulating lymph, which is sometimes
effused in such quantities as to give rise to considerable pain, and
a sensation like that produced by the presence of a foreign body.
The vessels in the parts around are somewhat enlarged, there is more
or less lachrymation, and the lids feel stiff and uncomfortable. The
sclerotic coat at the bottom of the wound remains visible for five or
six days, when it becomes covered with granulations, which, uniting
with those at the sides, gradually fill up the gap; the whole process,
from the commencement to the completion of the cicatrization, occupying
from three to four weeks.
Now and then the process of cicatrization is retarded by the
development of fungous granulations. When this is found to be the case,
they should be snipped off with the scissors; a procedure decidedly
preferable to the application of the nitrate of silver, which is not
only painful but rarely effective.
It has been recommended by some surgeons that, as soon as the soreness
occasioned by the operation has subsided, the patient should begin to
turn his eye in a direction opposite to that in which it was held by
the contracted muscle, and that these efforts should be continued daily
until it regains its natural position in the orbit. In my early cases,
before I had devoted much attention to the subject, I adopted and acted
upon this suggestion, but the result in every instance disappointed me.
Nor do I now perceive any good reason for following it, since it does
not seem to me to be founded upon correct principles. Where the eye
still retains some degree of obliquity after the operation, it may be
positively assumed that the section of the affected muscle, or of the
fasciæ by which it is invested, has been imperfect; and when this is
the case it would be in vain to expect Complete success. Again, the eye
operated on may be entirely straight, and yet not move in concert with
the other. This I have witnessed repeatedly, and hence my invariable
rule is to divide at once the corresponding muscle of the opposite
side, for the reason already mentioned—that the distortion generally
involves both organs.
300
The operation for strabismus is liable to occasional failure, the
principal causes of which may be thus enumerated:—1. Imperfect section
of the affected muscle, or of the ocular and submuscular fasciæ. To
this subject I have already several times alluded, and it is not
necessary, therefore, to offer any further remarks concerning it in
this place, than to say that the operator should never neglect to
divide these structures most thoroughly. In bad cases the scissors must
be carried up and down as far as the contiguous straight muscles, so
as to denude completely the sclerotic coat for more than one-third of
its circumference. The fasciæ must be effectually raked up, otherwise
it will be impossible for the muscle to retract fully within its
sheath. 2. Excision of a portion of the conjunctiva, eventuating in
contraction of this membrane during the process of cicatrization, may
be stated as another cause of failure. As there can be no necessity for
such a procedure, since it does in no wise facilitate the operation,
I need hardly say that it should be studiously avoided. 3. Strabismus
is sometimes complicated with other diseases, such as convulsions,
epilepsy, hydrocephalus, and analogous lesions. When this is the case,
the operation cannot be performed with any prospect of success, and
had better be declined altogether. The existence of amaurosis does
not necessarily lead to failure; if cataract be present, it should be
broken or depressed either at the time of the operation or before. 4.
But the most powerful cause of all, in my opinion, and one which has
not been sufficiently insisted upon by writers, is the coexistence of
strabismus in both eyes, and the fact that our operative procedures
are usually limited to one of these organs; a circumstance at variance
alike with good practice and common sense. In several instances in
which only partial success attended my efforts, the whole difficulty
was fairly ascribable to this cause; and so thoroughly am I persuaded
of its importance, that I have laid it down as a rule never to
operate on one eye only when it is certain both are affected. The
only exception to this is where the patient is very young, when the
section of a single muscle will sometimes, though even then not always,
be sufficient. 5. A fifth cause of failure is the readherence of the
posterior extremity of the muscle to an unfavourable point of the
sclerotica, by which it is again enabled to exert an undue influence
over the movements of the eye. The manner of obviating this occurrence
has been already indicated.
The effect upon vision is at first rather disagreeable, at least in
some instances. It is only by degrees that the affected organ recovers
its functions, and in many cases a considerable period must necessarily
elapse before this is brought about. Occasionally, in fact, the retina,
from long disease or other causes, is so effectually paralysed that the
sight is never restored, and it is in instances of this description
that a slight return of the distortion may be looked for, however
well the operation may have been executed. Another effect sometimes
witnessed is double vision. This is obviously dependent upon a want
of agreement between the optic axes, and rarely lasts more than a few
days, unless the obliquity has been only partially remedied.
The only other effect which it is necessary to notice here, as
attendant upon this operation, is a peculiar prominence of the eye.
This301 is generally well-marked, though not equally so in all cases, and
imparts to the organ a full, bold expression; it is accompanied with a
considerable separation of the lids, and is caused by the liberation of
the organ from its confined situation.
The preceding remarks have special reference to convergent strabismus;
with slight modifications they are applicable to the other forms of the
lesion. From the more exposed situation of the eye the outer straight
muscle is much more easily approached and divided than the internal;
as to the relative facility of operating on the upper and lower, I
can say very little from personal experience, but should suppose the
difference, if any, to be trifling. As to the oblique muscles, I have
not had occasion to divide them in a single instance, nor should I,
from the knowledge I have on the subject, deem such a step necessary,
it being very doubtful whether they have any agency in the production
of strabismus. In several instances in which these fasciculi were
divided by Lucas, Calder, and others, no impression whatever was made
upon the distortion, and nearly all surgeons agree in the opinion that
they should not be interfered with.
Attempts have been recently made to disparage the operation for
strabismus, on the ground of the alleged tendency of the eye to return
to its original malposition, or the occurrence of a new deviation. No
proof, however, of such a result, founded upon an adequate number of
statistical facts, has been given to the profession. In my own cases,
so far as my information extends, not a single relapse has taken place
where the operation was performed on both eyes, although nearly a year
has expired since some of them submitted to it. Confirmatory of this,
it may be stated that Dr. F. B. Dixon34 of Norwich, England, has
recently published a list of forty-one cases of convergent strabismus,
in thirty-one of which, twelve months after the division of the
internal rectus, both eyes were perfectly natural; in five, where one
organ alone was operated on, there was slight obliquity of the other;
in two, the squint was changed to a leer, and in three others, the eye
returned to its former malposition. These results, which are in the
highest degree gratifying, are sufficient to show that the operation
in question, first performed by Professor Dieffenbach of Berlin, in
October, 1839, deserves to be classed among the established resources
of surgery, which rarely exhibits such an amount of successful
terminations.]
Of Nasal Polypi.—These tumours vary in texture and disposition, as
formerly stated: but the soft mucous or benign polypus is, fortunately,
by much the most frequent. Generally a great many coexist in one
or both nostrils, growing from different parts of the Schneiderian
membrane. Sometimes there is but one tumour, of a large size; and
in some cases a large cyst, containing colourless fluid, fills the
nostril. When numerous, they are in different stages of growth, and
generally adhere to the membrane by a narrow neck, though sometimes
several are attached by the same pedicle. It is not un302common to remove
ten or twelve polypi, or even a greater number, before the nostril is
cleared. The parietes of the narrow passage betwixt the anterior and
posterior nares is their most common situation, though their bases may
proceed from the cells of the superior spongy bone.
The membranous covering of the inferior spongy bone, or of the anterior
cavity of the nostril, is often at the same time relaxed: indeed, this
of itself causes slight obstruction to the passage of air, and may be
mistaken for polypus by the patient and the unexperienced. Projection
of the cartilaginous septum to one side, with thickening of its
covering, may also give rise to the same mistake. This formation is not
uncommon, indeed it is rather frequent; and the projection is generally
to the left side, with corresponding depression of the right. The
circumstance may perhaps be accounted for by the pressure of the thumb
overbalancing that of the fingers in the habitual practice of clearing
the emunctory.

In polypus, the passage of air is obstructed, the patient feels as if
labouring under a common cold—his head is stuffed: in cold and dry
weather air passes through the cavity, though with difficulty; in a
damp day the obstruction is complete. The tumour evidently increases,
comes lower down, and even projects upon the lip. There is watering
of the eyes, the lachrymal secretions being prevented from flowing
into the nostrils; and, in cases of old standing, the patient is deaf,
from the pressure of the tumours on the extremities303 of the Eustachian
tubes. This latter symptom is not constant, but depends on the position
of the tumours. I recollect an old gentleman, an elder of the kirk,
afflicted with nasal polypus, who for thirty years had not heard his
clergyman, though for twenty of these years he had attended service
regularly, and from a sense of duty. On removal of the tumours hearing
was perfectly restored.
The nose changes its form, is expanded and flattened. If the disease
is extensive, and particularly if the tumour is malignant, the bones
are separated, the eyes are protruded, and pushed outwards; indeed,
the face is so distorted as to have been compared to that of a frog.
Even in the benign form, when of long duration, great deformity of the
features is produced, and the patient rendered very uncomfortable.
Besides the symptoms already detailed, he suffers from acute pain in
the forehead—he breathes loudly and with difficulty, particularly when
asleep—he has lost the sense of smell, and does not relish food or
drink—and there is often profuse discharge of a dirty mucous fluid,
both externally and into the pharynx.
Soft mucous polypus may exist for many years, without depressing the
palate, or projecting into the fauces. The anterior nasal cavity is
its most frequent seat, and it widens and fills up the fissure between
the anterior and posterior cavities: frequently it projects backwards,
but is not visible, though it may be felt with the finger behind the
soft palate. Its growth is slow. It may become malignant, as well as
other adventitious structures equally simple; but such an occurrence
is extremely rare. It may exist for many years; and, when at length
removed, will be found of simple structure; and, if the operation
be well conducted, no reproduction will take place. The tumours are
supposed to be easily regenerated; but the truth is, that they are
seldom eradicated completely. In general some are left, and these,
emerging from the narrow space or cells in which they were confined,
soon become fully developed—they expand, and speedily take the place of
those which were removed. They can never be got rid of at one sitting:
the operation requires repetition once and again; and of this the
patient should at the first be made aware.
Malignant Polypi are met with in different degrees of advancement.
Many are firm and fibrous, with an irregular surface and wide
attachment—do not grow with great rapidity—furnish a sanious and bloody
discharge, and give rise to painful feelings. If interfered with, their
increase is accelerated. If removed completely, reproduction may not
take place.
Tumours with broad bases, and of soft medullary consistence, attended
with extensive change in the structure of the membrane, and softening
of the bones and cartilages, grow very rapidly, fill the cavities and
expand them, giving rise to great deformity, as seen opposite. They
show themselves on the face, through the nostrils—protrude through
the floor of the orbit—get into the mouth behind the palate, through
the tuberous processes of the superior maxillary bone—or project
through the alveolar processes. The discharge from them is304 profuse
and fetid, and in some cases blood flows in no small quantity. Such
growths usually commence in one or other of the sinuses connected with
the cavity of the nose—sometimes, though rarely, in the frontal sinus.
When seated in the antrum maxillare, pain is experienced in the cheek
for a short time before swelling occurs. Soon the part enlarges, its
coverings are thickened, the bony cavity expands, and the patient’s
sufferings are excruciating. The teeth loosen, and sanious matter is
discharged from their roots. The tumour extends into the nostril, and
soon runs the course already mentioned. Malignant disease sometimes,
though rarely, commences in the anterior cavity of the nostril.
No satisfactory cause can be assigned for the appearance of either the
benign or malignant form of polypus.
The nostrils can be readily cleared of benign polypi, but seldom
completely, as already stated, by one operation: in several cases,
wherein only one or two tumours obstructed the cavities, I have had no
occasion to repeat my interference. If the attachments are broad and
extensive, a small curved blunt-pointed bistoury, or probe-scissors,
may be employed for their separation. Sometimes the tumours can be
pushed off by the finger, or by a probe with a blunt and forked
extremity: then they either are blown out by the patient, or fall
into the posterior cavity, thence into the pharynx, and are coughed
up or swallowed. In cases such as are usually met with, forceps and a
small vulsellum are the best instruments. The forceps should be about
half the size of those generally used or sold by cutlers as polypus
forceps. The patient is seated facing a good light and the body of the
prominent tumour is laid hold of by the vulsellum; the forceps are then
introduced, with the blades expanded, and carried backwards so as to
reach its neck, which is then to be firmly grasped by the instrument,
and gently twisted, so as to separate its connexions with the membrane.
No force, no jerking or pulling, is allowable. It may happen, even with
the gentlest and most careful management, that a small fragment of bone
comes away along with the tumour; but this generally can or should be
avoided: the cure is not rendered more certain by such an occurrence,
as has been supposed. One tumour being thus detached, the same process
is repeated with the others, till the cavity is cleared so far as
hemorrhage or the patient’s fortitude will admit. Both nostrils, if,
as is usually the case, both are stuffed, may be emptied at the first
sitting, so as to enable the patient to blow through them. When the
tumours filling the passage to the throat have been removed, so as to
allow the ready egress and ingress of air, and when the forceps can be
passed along the floor of the cavity, and are expanded and shut without
meeting any obstruction, examination is to be made with the finger. In
those who have long laboured under the disease, the fissure between
the cavities is so much expanded as to admit the little finger easily,
and by it the situation of the remaining tumours is ascertained, and
instruments guided to them.
After the operation the nostrils are stuffed gently with lint, to
prevent the access of cold air; and, if the hemorrhage be profuse,305
long pieces of lint pushed well back will generally be sufficient to
arrest it: if not, the posterior cavity must be plugged from behind.
It is prudent to prepare for the stuffing posteriorly in bad cases in
which violent hemorrhage may be expected. Instruments with springs,
&c., have been contrived for the purpose, but are useless, and cannot
always be had. A loop of thin flexible wire, or of thick catgut, is
passed along the floor of the nostril, and on reaching the throat
is caught by the finger, or by a hook or forceps, and brought into
the mouth. A piece of strong thread is then attached to the wire or
catgut, and the latter is withdrawn; one extremity of the thread
hanging from the nostril, the other from the mouth. To the middle
of the thread a piece of lint rolled up to the size of the point of
the thumb is affixed, and this is pulled back into the mouth, and
directed into the posterior nares with the fingers; by the pressure
of these, and by pulling at the thread, the dossil is firmly wedged
into the aperture. Lint is preferable to sponge, as being more easily
removed; sponge swells, and is apt to produce inconvenience. The plug
must be well proportioned to the opening: if too large, it cannot be
lodged in its situation; if too small, it does not fill it, and may be
pulled through altogether. It should be smaller, of course, for young
subjects and females than in adult males. It may be necessary to close
both nostrils in this manner, when both are bleeding profusely, or
when they communicate through an aperture in the septum. The anterior
cavity is then closed with lint, and the hemorrhage, however violent,
is completely commanded. The posterior plug is removed on the second
or third day by pulling the oral extremity of the thread, and, if need
be, by pressing through the nostril with a strong probe. Plugging may
be required in epistaxis from other causes, when other means, as cold
applied to the surface of the body, and astringent injections to the
part, have failed. The latter remedy is not much to be depended upon.
The operation for polypus may be repeated when the parts have
recovered, and the pain and discharge ceased. Ere then the patient
again finds himself unable to propel air easily through the nostril,
and, on examination, greyish, shining tumours are again visible. The
same process of extraction is repeated until all are eradicated.
Escharotics may be then applied with some advantage, but must be
used with caution, and not of too active a nature: nitrate of silver
and the red oxide of mercury are those commonly employed. But it is
questionable whether these applications have any effect in preventing
the future growth of the tumours.
The malignant form of the disease, even in a very early stage, is
unmanageable: the tumours, if removed, are speedily reproduced, and
the fatal termination may be accelerated by the interference. I have
removed tumours from the antrum maxillare, and from the frontal
sinus; but the parts became soon occupied by morbid growths of a more
formidable character than the preceding: the membrane and bone appear
to assume a disposition to generate such, and the fungous protrusions
cannot be kept down with escharotics, nor with the actual cautery: nor,
after free removal with cutting instruments,306 have escharotics, however
freely applied, any effect in counteracting the inherent disposition to
the disease, and preventing its recurrence.
The antrum, when filled with such tumours, is easily laid open. The
cheek is divided perpendicularly from over the inferior orbitary
foramen to the mouth, and the soft parts are dissected from off the
bone. The cavity may then be exposed by means of a small trephine:
but this instrument is scarcely ever required, the parietes being so
softened as to yield easily to the knife: pliers or cutting forceps may
be useful in enlarging the cavity. By the guidance of the finger, the
attachments of the morbid growth are separated with a blunt-pointed
bistoury; and a scoop is used to turn out the diseased mass. The
root of the tumour is then touched with a red-hot iron, and by this
implement, or by dossils of lint, the hemorrhage is easily arrested.
But such operations, considering the result of those which have been
practised, are scarcely justifiable.
It has been proposed for this disease to remove the tumour, along with
its investment—to separate and dissect out the superior maxillary
bone. It is a very severe operation, and one which puts the patient’s
life in imminent jeopardy, from profuse hemorrhage or constitutional
disturbance. In one case, the surgeon began the operation after having
tied the common carotid of the affected side; but, having made the
incisions of the cheek and palate, was obliged to desist, on account
of the violent bleeding: eight days after, the common trunk of the
temporal and internal maxillary was tied on the opposite side, and
the incisions repeated, but the result was the same; the growth
increased, and the patient perished. The disease is very insidious in
its progress, and has gained much ground before the patient becomes
alarmed and applies for surgical aid. The parietes of the antrum are
expanded and softened; the tumour has projected behind through the
tuberous process, upwards through the plate of the orbit, or inwards
to the nostril; and has contaminated by its presence and contact all
the neighbouring parts. Then removal of the maxillary bone, or of all
the bones in that side of the face, can be of no service. The disease
is seldom if ever seen by the surgeon early enough to admit of any
operation being practised with the least chance of ultimate success. At
a sufficiently early period, the removal of the bone—of the parietes
of the cavity containing, and from which the tumour has grown, must
without doubt afford a better chance, and is, in every point of view,
to be preferred to the old operation described above of what was called
trephining the antrum. In one case of soft and brain-like tumour
filling the antrum, and evidently commencing there, I succeeded in
removing the entire disease. The patient remained sound. I have more
than once seen the operation performed for this soft and malignant
growth of only some months standing; portions of the bone and tumour
crumbled under the fingers of the operator—the operation was harsh,
painful, and appalling—the cases hopeless. Execution of the manual
part is not attended with serious difficulty, and it can seldom be
necessary to tie arteries previously. To expose the bone, the cheek is
divided from the angle of the mouth, to the origin of the masseter,
and a second incision made from the inner canthus to the edge of the
upper307 lip near the mesial line, detaching the alæ of the nose from the
maxillary bone.
The flap of the cheek thus formed is dissected up, and the nasal
process of the maxillary bone and the body of the os malæ are divided
with a saw, or with strong cutting pliers. An incision having been
made through the covering of the hard palate, near the mesial line,
a small convex-edged saw is applied to the bone; and the alveolar
process is cut through by the pliers, after extraction of the middle
and lateral incisors. The bone is then pulled downwards and forwards,
and its remaining adhesions separated by means of the knife or
pliers. This last part must be accomplished rapidly, so as to reach
the vessels, and arrest the hemorrhage. During the progress of the
operation, cut branches of the facial and temporal are commanded by
ligature or pressure, and the violence of the hemorrhage is moderated
by compression of the carotids. After removal of the bone, the deep
vessels, branches of the internal maxillary, are secured either by
ligature, or by firm pressure with charpie or dossils of lint. The
facial flap is replaced, brought together over the charpie by which
the cavity is filled, and united by interrupted or convoluted suture.
Cures by such proceedings, in such cases, are reported; the patients do
not always die immediately after the operation; but there is reason to
complain of want of candour as regards the ultimate result.
The disease, it is said, has been arrested by ligature of the common
carotid; the allegation is not borne out by facts, nor is it easy to
discover on what principle the practice was adopted. Such a result
is not to be expected à priori, nor to be believed without farther
trial; and these trials are not likely to be made.
The superior maxilla is liable to become the seat of other tumours
beside the preceding. It may be occupied by fibrous tumour, commencing
in the bone, or in the alveoli. The tumour feels hard, and very often
not encroaching upon the antrum, is evidently circumscribed, and
presents a smooth and botryoidal surface. It has not that disposition
to involve neighbouring parts, hard as well as soft, but may remain
long without extending farther than the superior maxillary bone, and
occupying only a part of it. In such a case, excision of the maxillary
bone is warrantable, and ought certainly to be performed; for there
is no risk of the parts being extensively contaminated. I met with
one instance of it in the latter situation a good many years ago. The
patient was a female, about twenty-five years of age. The tumour was
of four years’ duration, and its origin was attributed to a severe
bruise of the cheek upon the corner of a table. The teeth had loosened
soon after the injury, and the disease commenced in the gums. When
she applied, there was a hard prominent swelling in the forepart
of the maxillary bone, and a firm tumour involved the gums on the
same side, and a part of the hard palate: the disease had made much
progress during the previous six months, but had evidently none of the
malignancy of the soft tumours which originate in, or early involve,
the cavity of the antrum: at first it had possibly been of the nature
of epulis. I removed the bone in the same way as already described,
and had the308 satisfaction to find the disease completely taken away.
The hemorrhage was restrained by compression behind the angle of the
jaw during the incisions, and not more than ℥iii. of blood were
lost. The tumour, when cut into, presented a homogeneous and fibrous
appearance; at one or two points, softening had begun, and a small
quantity of pus had been deposited. The external wound healed by the
first intention, and the internal cavity granulated kindly. The patient
remains perfectly free of disease, and bears little mark of so serious
a disease or of so severe an operation. Within the last four or five
years I have repeated the operation for this disease very often, and
with uniform success. The cases are recorded in the Medico-Chirurgical
Transactions, vol. xx., in the Lancet, and Practical Surgery, to
which the reader is referred for further information on the subject.
One of the tumours had attained an enormous size, and weighed nearly
four pounds.

Of Inflammation, Abscess and Ulceration of the Nose, and Cavities
connected with it.—Inflammation may be excited in the nose by external
injury, as a bruise, or fracture, or displacement of the bones. The
acute symptoms are swelling and discoloration of the integuments,
turgescence of the Schneiderian membrane, which covers the septum
narium and the turbinated bones, and consequent obstruction to the
passage of air. Unless active measures are pursued, abscess follows,
with great swelling and obstruction; and extensive loss of substance,
with deformity, may ensue. Unless the acute symptoms, the short
duration of them, and the rapid supervention of tumour be considered,
the swelling may be mistaken for polypus.
The septum suffers more than other parts of the nose, from the309
concussion produced by a blow, and is in general more seriously
affected by the morbid action which is induced. Matter is effused
beneath the membrane, in one or both sides, usually in both, and
tumours are thereby formed, which project into the cavities of the
nostrils; when attentively examined, fluctuation is felt, and, if the
affection has existed for a considerable time, the abscesses are found
to communicate with each other, the septum having been absorbed or
necrosed at one or more points. An individual received a severe blow
over the extremity of the ossa nasi, and a slight wound was produced.
The breathing soon became obstructed, by swelling in the nostrils, and
great pain in the part was complained of. A large tumour formed on the
septum, and completely filled the cavities; it was opened, and a great
quantity of matter evacuated. The septum was destroyed by ulceration to
a considerable extent, and a slight falling down of the middle of the
nose followed. Such cases are of common occurrence.
Independently of any vice in the constitution, ulceration of the
nostrils may be induced by injury, and proceed until great ravages
are effected, if the treatment be not properly conducted. A young
gentleman, playing at ball, was struck accidentally on the nose with
the flat part of his companion’s hand. Inflammation took place,
externally and internally, and the passage of air was obstructed,
abscess formed, and the matter was evacuated spontaneously; extensive
ulceration ensued; the cartilage and bone became affected, portions of
them separated, and a bloody fetid sanies flowed from the nostrils.
All the cartilaginous and part of the bony septum were destroyed; the
morbid action ceased after having continued for a long time; but the
organ was curtailed, sunk on the face, and altogether much deformed. In
this case I first proposed, and some time afterwards performed for the
first time, the operation for the formation of a new columna nasi from
the lip.
The alæ, as well as the septum, may suffer from external injury, indeed
the whole cartilaginous part of the nose may be destroyed.
Incited action must be subdued by abstraction of blood from the
external parts, or from the Schneiderian membrane, leeches being
applied in sufficient numbers, and repeated. Should suppuration not
be prevented, the abscess, particularly when internal, must be early
opened; the surgeon is, perhaps, somewhat to blame, if the patient,
having been under his care from the first, sustains any deformity. If
abscess has formed on both sides of the septum, each must be opened
freely; afterwards hot fomentations are to be used, and the cavity
should be frequently cleansed by the injection of a bland and tepid
fluid.
Intractable ulceration of the nostrils is often induced by trifling
irritations or injuries in constitution, either originally unsound, or
rendered so by imprudent conduct; slight blows on the prominent part
of the organ produce swelling with discoloration, and that is followed
by abscess and ulceration. Internal ulceration is frequently caused
by the continued use of snuff, or the presence of other irritating
matters,—by irritation communicated from diseased gums or alveoli, or
from decayed or crowded teeth, particularly the incisors310 of the upper
jaw—by stumps in any part of the mouth, or the pivoting of artificial
teeth on them—or by introducing the dentist’s perforator, with a view
of destroying the nerve of a tooth. I have seen ulceration, and loss of
substance in the skin, membranes, and bones of the face, arising from
each and all of these causes.
The ulceration occasionally commences, even in young subjects, in a
wart or fissure on the integuments of the nose or upper lip; it thence
extends to the alæ and floor of the nostrils; the cartilages, and
even the bones, are destroyed; the discharge is thin, acrid, bloody,
and fetid, and the action is with much difficulty controlled. The
disease is met with of various degrees of severity and malignancy; it
may cease spontaneously, may appear to be arrested by constitutional
and local treatment, or, resisting all means employed against it,
may go on consuming portions of the face, both hard and soft;
destroying the nose, lips, and eyelids, and ultimately the bones
in their neighbourhood. Horrid cases are occasionally met with, in
which scarcely the vestige of a feature is discernible—the patient is
nourished, and life is often protracted for a long period, by food
conveyed over the root of the tongue, through funnels or tubes. Noli
me tangere, and lupus, are names applied to the advanced stages of
the disease.
Ozœna, which denotes the internal ulceration of the nose, or rather
the discharge indicating such, is generally of long continuance.
The discharge is at one time profuse, at another scanty; sometimes
it ceases almost entirely, but the accompanying fetor, of a most
disgusting nature, is still perceptible on approaching the patient,
or coming within the influence of the air expired over the diseased
surface; the stench is particularly offensive when portions of bone
are separating. The bones may die either from inflammatory action in
them running high, or from being uncovered and deprived of support by
ulceration of the investing membrane. In many cases, the disease is not
arrested till the cartilaginous and bony septum, the turbinated bones,
the hard and soft palate, and frequently the alveoli, are completely
destroyed. The patient, if he live, is in a miserable plight;—his
countenance is deformed and ghastly; the situation of the nose is
occupied by a large dark and foul sore; the discharge is profuse and
weakening; the expired air is as a pestilence to himself and those
around; speech is almost unintelligible; breathing is difficult;
the strength is gradually exhausted; and the spirits sink under the
harrowing impression of misery. All these ills result more frequently
from the injudicious employment of mercurial preparations than from
any other cause. In almost every instance, the predisposition to such
frightful ulcerations has been induced by the use of mercury, and can
readily be traced to it. Exposure to atmospheric changes, during or
after the exhibition of mercury, may render the mucous surface and the
coverings of the bones more susceptible of the disease; that medicine
may be given with the utmost precaution, but for long after the
constitution cannot shake off its influence; and too frequently more of
the poison is administered for disease produced by it. Ulceration of
the tonsils, and other parts in the fauces, often coexist with disease
of the nostrils.
311
Ulceration of the nostrils is arrested with difficulty. It cannot
be expected to cease till dead parts have separated, become loose,
and fall out, or are removed by art. Portions of the bones, forming
the floor of the nostril, can often be removed, when dead, through
ulcerated apertures in the palate; whilst others are brought away
through the nostrils, there being generally sufficient space
allowed for their discharge—the nasal cavities being laid into one
by destruction of the columna, and more or less of the septum.
Occasionally the ossa nasi, or parts of them, escape through an opening
in the superimposed integuments; sometimes they cannot be discharged
otherwise, as in the following case:—Matter had come to the surface
over the nasal process of the frontal bone, an incision was made for
its evacuation, sequestra were found loose, and some extracted; one was
pushed down with the view of pulling it through the nostril, but this
was found closed from the effects of small-pox.
Various applications to the ulcerated cavities are employed. Injections
of spirituous and aromatic lotions are used to wash away the discharge
and correct the fetor, as diluted tincture of myrrh, or of aloes,
a lotion containing a proportion of kréosote the sulphate of zinc,
solutions of the chlorides of lime or soda, &c. Applications, soothing
or stimulant, are made to the exposed sores according to their
appearance and disposition. When the ulcer is of an angry and irritable
aspect, it is to be touched lightly with the nitrate of silver,
in substance or solution, and then covered with a bread and water
poultice. Fowler’s solution of arsenic is useful in some cases, when
the object is to clean or destroy the surface; this is also effected
by a slight application of the potass. A very manageable and efficient
escharotic is the chloride of zinc. It is mixed with an equal quantity
of dried plaster of Paris or flour, and made into a paste, with a few
drops of water for application. Black wash sometimes agrees well, as
also a liniment of olive oil and lime-water, with citrine ointment
(three parts of the former ingredients to one of the latter), or the
sulphate of zinc lotion. When the sore is very indolent, showing no
signs of granulation, it may be touched occasionally with spirit of
turpentine, either pure or combined with alcohol, and afterwards
covered with an ointment composed of ung. ceræ and spir. terebinthinæ;
under this application ulcers often heal, after having resisted all
others. But nitrate of silver applied gently, and repeated at the
interval of two or three days, will, in the majority of cases, be found
the most efficient remedy, combined with the simple dressing of tepid
water. Constitutional treatment must not be neglected. When the disease
cannot be traced to mercurial action, small doses of the bichloride
of mercury are allowable when excitement is required. The arsenical
solution given internally sometimes produces good effects. In foul
internal disease of the nostrils with cachexia, no medicine exerts so
beneficial an influence on the general health and local disease, as
sarsaparilla, exhibited either in decoction, in extract, or in powder.
Loss of substance, from ulceration or injury, is repaired by surgical
operation. A portion of integument is borrowed from some other312 part,
and by the adhesive process is made to cover and supply the deficiency.
Such operations were contrived and practised by Sicilian and Italian
surgeons some centuries ago, and were revived in our day in Germany.
The integument was borrowed from the upper part of the arm; it has
sometimes not been applied immediately, but detached gradually, and
allowed to thicken, to change its consistence, and to become more
vascular, previously to its adaptation to the mutilated organ. When
considered sufficiently prepared, it has been shaped so as to fit
accurately, though still remaining attached at one point to the arm;
the cicatrized edges of the deficient parts should then be made raw,
and the new substance affixed by suture; the original attachment is
preserved entire, and the patient kept in a constrained position—the
arm and head being approximated and bound together by apparatus—for
many days, till union occurred. Then the flap is separated entirely,
and the new nose moulded into its proper form, by subsequent paring and
compression.
The Rhinoplastic operation, introduced from India—where from time
immemorial it has been practised by one of the castes—has superseded
the preceding, and is variously modified. It is less difficult in
execution, not so liable to failure, and more easily undergone by the
patient. The same preparation of the flap is not required, though
it is said that the Indian operators are in the habit of previously
pummelling, with the heel of their slipper, the integument to be
used for the new nose, so as to excite the circulation, and produce
thickening; from the similarity of texture in the integument of the
face, its application to the new situation is not much observed.
The apex and alæ can be readily repaired by a flap of proper shape
and dimensions from the forehead. The cicatrized edges where the nose
formerly rested, must in the first place be dissected off pretty
deeply, so as to be prepared for the attachment of the new appendage.
The size of the lost organ, and the dimensions necessary for its
replacement, are then to be taken into consideration. It is recommended
to make a mould in wax of the part, and after flattening it out, to use
it as a guide for the incisions. But a piece of card or soft leather is
more convenient; this having been cut of the proper size and form, is
laid down on the forehead, the part representing the root of the nose
resting between the eyebrows. It is held firmly by an assistant, whilst
the surgeon traces its dimensions first with ink, or at once with a
knife carried deeply through the integuments. The pattern is then
removed, and the flap dissected down, being laid hold with the finger
and thumb, or with a hook. It is then twisted round, the lower part
being left undisturbed. This attachment at the root of the nose may be
narrow and long, so as to admit of its being twisted, but it is not to
be cut thin; it must embrace the fibres of the corrugator supercilii,
so that its vascular supply may be abundant. The incision on the side
opposite to which it is proposed to make the turn may be brought a
little lower than the other, so as to facilitate the twisting. After
bleeding has ceased, the flap is applied to its new situation, and
retained in apposition with the raw edges of the truncated organ by a
few points of interrupted or convoluted suture;313 a little oiled lint
is placed in the nostrils to support the flap, but no other dressing
should be applied. To cover the part with pledgets of lint smeared
with ointment, and adhesive strap, can answer no good purpose, and the
subsequent removal of such must endanger the adhesion. The attention
must now be directed to the wound of the forehead; the lower part is
easily brought together, and retained by a stitch; thereby the whole
surface is diminished, and what remains will soon be repaired by
granulation. It is at first dressed merely with a pledget saturated
with tepid water, afterwards some stimulating lotion may be gradually
added. The operation should not be performed in very cold weather,
and even in summer the patient should be enjoined not to leave his
chamber. The lint may be removed in three or four days, and then, too,
some of the stitches may perhaps be dispensed with. The flap will be
found adherent, but loose, and raised by every expiration; very soon
granulations rise from the inner surface, the part derives support from
below, and becoming firm, preserves its form well. It will be necessary
during the cure to keep the nostrils of their proper size and shape, by
means of dossils of lint, or well-fitted tubes.
Nothing has as yet been said of the columna. In the Indian operation it
is provided for by a slip purposely brought down from the forehead, and
attached to the point which the root of the original columna occupied.
Their flap is shaded as in the following figure. In the greater number
of foreheads, an encroachment must be made on the hairy scalp, in
order to obtain this part of the flap; and after bringing it down and
ingrafting it into the lip, there is a risk of its not adhering, as
 happened in a case on which I operated now many years ago. Besides,
during the healing of the internal surface, it will be difficult to
prevent it from shortening, and turning inwards upon itself, and thus
pulling down the apex of the nose. In the case to which I alluded,
a columna was made, after consolidation of the rest of the organ,
from the upper lip, as will be immediately explained; and in again
performing the operation for restoration of the whole nose, I should
proceed on the plan of taking only a flap sufficient for the apex and
alæ from the forehead, and should borrow the columna from the lip. In
this way the risk of failure will be diminished, and the form of the
lip materially improved. The columna might be provided at the same time
with the other parts; but it would be more advisable to delay this part
of the operation till a few weeks after adhesion of the other flap has
been perfected.
happened in a case on which I operated now many years ago. Besides,
during the healing of the internal surface, it will be difficult to
prevent it from shortening, and turning inwards upon itself, and thus
pulling down the apex of the nose. In the case to which I alluded,
a columna was made, after consolidation of the rest of the organ,
from the upper lip, as will be immediately explained; and in again
performing the operation for restoration of the whole nose, I should
proceed on the plan of taking only a flap sufficient for the apex and
alæ from the forehead, and should borrow the columna from the lip. In
this way the risk of failure will be diminished, and the form of the
lip materially improved. The columna might be provided at the same time
with the other parts; but it would be more advisable to delay this part
of the operation till a few weeks after adhesion of the other flap has
been perfected.
314
Since writing the preceding observation, I have in a very great many
 instances performed the operation according to the plan here proposed,
and with the most perfect success. The form of the nasal flap was
this. The little projection was made in order to be turned down, so
as to form the tip of the nose; as well as to constitute a convenient
attachment for the columna, which was subsequently to be made.
instances performed the operation according to the plan here proposed,
and with the most perfect success. The form of the nasal flap was
this. The little projection was made in order to be turned down, so
as to form the tip of the nose; as well as to constitute a convenient
attachment for the columna, which was subsequently to be made.
In separating the connexion with the forehead, a thin wedge-like
portion is removed, and the raw surfaces, after the cessation of
bleeding, are laid in apposition, and retained by gentle compression.
But this should not be done till the new nose is consolidated and
perfect.
Restoration of the columna is an operation which, in this, and other
civilized countries, must be even more frequently required than
the restoration of the whole nose. This latter operation came to
be practised in consequence of the frequency of mutilations as a
punishment; the punishment for some of our sins is left to nature, and
she generally relents before the whole of the organ disappears. The
columna is very frequently destroyed by ulceration, a consequence,
as before stated, of injury or of constitutional derangement. The
deformity produced by its loss is not far short of that caused by
destruction of the whole nose. Happily, after the ulceration has
been checked, the part can be renewed neatly, safely, and without
much suffering to the patient. The operation which I have for some
years practised successfully, and in a great many instances, is
thus performed:—The inner surface of the apex is first pared. A
sharp-pointed bistoury is then passed through the upper lip, previously
stretched and raised by an assistant, close to the ruins of the former
columna, and about an eighth of an inch on one side of the mesial
line. The incision is continued down, in a straight direction, to the
free margin of the lip; and a similar one, parallel to the former, is
made on the opposite side of the mesial line, so as to insulate a flap
composed of skin, mucous membrane, and interposed substance, about a
quarter of an inch in breadth. The frænulum is then divided, and the
prolabium of the flap removed. In order to fix the new columna firmly
and with accuracy in its proper place, a sewing-needle—its head being
covered with sealing-wax to facilitate its introduction—is passed
from without through the apex of the nose, and obliquely through the
extremity of the elevated flap; the small spear-pointed harelip
needle answers even better: a few turns of the thread suffice to
approximate and retain the surfaces. It is to be observed, that the
flap is not twisted round as in the operation already detailed, but
simply elevated, so as to do away with the risk of failure.315 Twisting
is here unnecessary, for the mucous lining of the lip, forming the
outer surface of the columna, readily assumes the colour and appearance
of integument, after exposure for some time, as is well known. The
fixing of the columna being accomplished, the edges of the lip must
be neatly brought together by the twisted suture. Two needles will be
found sufficient, one being passed close to the edge of the lip; and
they should be introduced deeply through its substance; two-thirds, at
least, of its thickness must be superficial to them. Should troublesome
bleeding take place from the coronary arteries, a needle is to be
passed so as to transfix their extremities. The whole cut surface is
thus approximated; the vessels being compressed, bleeding is prevented;
and firm union of the whole wound is secured. The ligature of silk,
which is twisted round the needles, should be pretty thick and waxed;
and care must be taken that it is applied smoothly. After some turns
are made round the lower needle, the ends should be secured by a double
knot; a second thread is then to be used for the other needle, and
also secured. With a view of compressing and coaptating the edges of
the interposed part of the wound, the thread may be carried from one
needle to the other, and twisted round them several times; but in doing
this, care must be taken not to pull them towards each other, else the
object of their application will be frustrated, and the wound rendered
puckered and unequal. Last of all, the points of the needles are to be
cut off with pliers. No farther dressing is required; as previously
remarked, no good end can be answered by any application, and the
separation of dressing may afterwards be troublesome; discharges from
the neighbouring passages are retained by it, fetor is produced, and
union interrupted. The needles may be removed on the second or third
day; their ends are cleared of coagulated blood, and, after being
turned gently round on their axes, they are to be cautiously withdrawn,
without disturbing the thread or the crust which has been formed about
them by the serous and bloody discharge. This often remains attached
for some days after removal of the needles, and forms a good protection
and bond of union to the tender parts. Some care is afterwards required
from the surgeon and patient in raising up the alæ, by filling them
with lint, and thus compressing the pillar, so as to diminish the
œdematous swelling which takes place to a greater or less degree in
it, and to repress the granulations. It is besides necessary to push
upwards the lower part of the columna, so that it may come into its
proper situation; and this is done by the application of a small round
roll of linen, supported by a narrow bandage passed over it and secured
behind the vertex.
Independently of the great improvement produced on the patient’s
appearance by the restoration of the lost part of so important a
feature, it may be observed, that, when the columna has been destroyed,
the lip falls down, is elongated, and becomes tumid, particularly at
its middle, so that borrowing a portion from it materially ameliorates
the condition of the part; the cicatrix being in the situation of the
natural fossa, is scarcely observable.
The alæ of the nose, deficiencies in the upper, anterior, or lateral
parts of the organ, in the forehead, &c., may be supplied from the316
neighbouring integument, on the same principle as the preceding
repairs. In many of these operations the flap can be so contrived
and cut out, as that it can be applied without its attachment being
twisted. The form of such flaps is here given.
It is merely necessary to bring the portion which has been dissected
from the subjacent parts of the forehead, cheek, or lip, to the part
prepared for its reception, by effacing the angle betwixt it and the
connecting slip. A flap to supply the greater part or even the whole of
the organ may thus be transplanted.
The integuments covering the apex and alæ of the nose are sometimes
opened out in texture by interstitial deposit, forming a lipomatous
tumour, lobulated, discoloured, and intersected by fissures. The
sebaceous follicles are enormously enlarged, so as sometimes to
admit the point of a small quill. On making a section of the parts,
accumulations of sebaceous or atheromatous matter are found inclosed
in cysts of considerable capacity. Turgid veins ramify superficially;
and the surface is of a reddish blue or a purple colour, varying its
hue from time to time, according to the state of the health, and
the changes in the circulation. The enlargement often attains great
magnitude, producing much deformity. Vision is obstructed, and the
introduction of food, both solid and liquid, interfered with: the lobes
tumble into the wineglass, spoon, and cup, and sometimes they are so
elongated as to require being pulled aside in order to uncover the
mouth. Breathing is also impeded more or less, by encroachment on the
nasal orifices. The disease may be often attributable to hard living;
but many, not intemperate, labour under it.
It is desirable to have the tumour removed, even before it has become
large; and it can readily be conceived that local applications must
fail in bringing the skin and cellular tissue into a healthy condition.
Incision is required. If both sides of the nose are affected, a
small scalpel is carried down in the mesial line through the altered
structure, and, whilst an assistant places his finger in the nostril,
the surgeon lays hold of the integument with a sharp hook, and
care317fully dissects away the diseased parts, first on one side, and
then on the other, so that they may correspond exactly, or present the
same uniform appearance. The vessels are then tied, and sometimes a
considerable number bleed smartly; oozing may continue, but is readily
suppressed by continued pressure, the nostrils being well stuffed.
Afterwards such dressings are to be employed as agree with the stages
of the sore. After cicatrization, the comfort and appearance of the
patient are much enhanced; and there is no risk of reproduction—the
disease is one of the skin, and all that is affected has been removed.
Sketches taken from one, of very many patients, on whom I have operated
for the removal of this shocking deformity, are given in the Practical
Surgery, p. 306-8.
Inflammation of the antrum maxillare is occasionally met with; but
the surgeon is more frequently called upon to treat the consequences
of this action in it. The symptoms of inflammation of the antrum
are violent throbbing pain, referred to the part affected, to the
temple, and to the teeth implanted in the alveolar processes that
form the lower part of the cavity; the side of the face is swelled
from infiltration of the soft parts, and the Schneiderian membrane
of the corresponding nostril is generally observed red and swollen.
The affection can frequently be traced to exposure to cold; it may
be the result of external violence; but is usually an extension of
disease in the sockets of decayed teeth. Unless active and early
measures are taken to subdue the inflammatory attack, the antrum
becomes distended by increased and vitiated discharge from its lining
membrane. The swelling of the cheek becomes more apparent, since, to
increased infiltration of the soft parts, enlargement of the cavity is
 superadded. The enlargement of the side of the face, and the bulging
into the orbit are seen in the accompanying cut. The membrane covering
the small aperture through which the antrum and nostril communicate
partakes of the general thickening, and thus no outlet is left for the
accumulating fluid. The escape of matter from the nostril, on the head
being turned to the opposite side, has been laid down as an indication
of accumulation or abscess in the antrum; the statement is incorrect,
and is a result of surgery being professed by those who have not
practised it, but judge of morbid states and their signs and symptoms
by the healthy condition of parts only. In the skeleton, fluid no doubt
will run over from the osseous shell, in some positions of the skull;
but it cannot escape from the cavity when covered with membrane, and
that membrane subject to vital actions. In short, the symptom is not
observable in318 the disease in question.35 Extensive ulceration of the
parietes of the antrum towards the nose may, perhaps, take place, as a
consequence of the accumulation, and the matter may then escape by the
nostril, if not allowed an exit otherwise; but such is not a common
occurrence.
superadded. The enlargement of the side of the face, and the bulging
into the orbit are seen in the accompanying cut. The membrane covering
the small aperture through which the antrum and nostril communicate
partakes of the general thickening, and thus no outlet is left for the
accumulating fluid. The escape of matter from the nostril, on the head
being turned to the opposite side, has been laid down as an indication
of accumulation or abscess in the antrum; the statement is incorrect,
and is a result of surgery being professed by those who have not
practised it, but judge of morbid states and their signs and symptoms
by the healthy condition of parts only. In the skeleton, fluid no doubt
will run over from the osseous shell, in some positions of the skull;
but it cannot escape from the cavity when covered with membrane, and
that membrane subject to vital actions. In short, the symptom is not
observable in318 the disease in question.35 Extensive ulceration of the
parietes of the antrum towards the nose may, perhaps, take place, as a
consequence of the accumulation, and the matter may then escape by the
nostril, if not allowed an exit otherwise; but such is not a common
occurrence.
In general, the cavity is considerably enlarged before the matter comes
to the surface. If not interfered with, it usually escapes through
the sockets of decayed teeth, or, the anterior thin parietes being
absorbed, it comes down by the side of the canine or small molar teeth,
and is discharged slowly, so as to annoy the patient by its flavour and
fetor, without the abscess being emptied, or a chance of cure afforded.
Accumulations of fluid sometimes takes place in this cavity, give
rise to great enlargement of the sinus, and continue for many months,
without pain or much inconvenience, and without any matter escaping.
The bony parietes are attenuated, yield to slight pressure, and
return to their original level with a crackling noise, such as is
produced by parchment. The contained fluid is thin, greyish, and
contains flocculent solid particles. In short, the antrum maxillare is
occasionally the seat of chronic, as well as of acute abscess.
Cancerous ulceration sometimes takes place in the cavity; the matter
is not long confined, the parietes soon soften, the teeth drop out,
the alveolar processes disappear, and a large opening is formed, which
furnishes a fetid, sanious discharge.
In inflammation of the antrum, carious teeth must be removed, blood
must be abstracted from the neighbourhood of the affected part—leeches
being applied to the gums, the Schneiderian membrane, and the
integuments—and fomentations to the cheek should be frequently and
assiduously employed. When the cavity has become distended with
fluid—mucous, muco-purulent, or purulent—such must be evacuated without
delay; and the opening must be of such size, and so situated, that the
fluid may escape as soon as secreted. In removing diseased or crowded
teeth opposite the part, an opening may be made from the extremities of
the fangs having projected into the cavity; it is in a good situation,
but cannot easily be made of sufficient size; an aperture of but small
extent may be sufficient for 319the draining of an abscess in soft
parts, but here the divided texture is unyielding, and the perforation
must be free. Bad teeth are taken away with the view of abstracting
a source of irritation which may give rise to, keep up, or induce a
return of collection in the antrum; but extraction of sound teeth, to
obtain an exit for the matter, is not warrantable. Even when they are
extracted for a different reason, and discharge of matter follows, the
surgeon must not be contented, but must make another and more efficient
opening. The membrane of the mouth is to be divided on the forepart
of the maxillary bone, immediately above the first small grinder, and
a large perforator then pushed into the antral cavity; little force
is required, for the parietes are soft and partially absorbed. The
perforation should be of a size sufficient to admit the little finger;
thereby a free and dependent exit is allowed for the concrete as well
as the fluid matter. Curdy and very offensive stuff is sometimes found
in great abundance in this cavity. If the discharge is very fetid, and
long of drying up, and if there is an appearance of disease in the
osseous parietes, injections into the cavity may be required, though
seldom. They are occasionally useful in dislodging the atheromatous
matter. In general the discharge gradually diminishes, the membrane
of the antrum resumes its healthy condition and functions, and the
aperture in its parietes is shut by a fine ligamentous substance.

Ulcers of Lips.—The prolabium is liable to ulceration from various
causes; from long-continued irritations, as sharp corners of teeth,
rugged tartar on the external surfaces of the teeth, the habitual use
of a short tobacco-pipe; from external violence; from the application
of acrid matter; or from an ulcerative disposition unconnected with
external circumstances. The constant and free motion of the parts is
prejudicial to healing, and consequently the sores often remain long
open. Though ulcers on the lips are generally of a bad cha320racter, it
does not follow that all are so. Many are simple; but these, after
remaining long, are apt to degenerate. Others from the first assume
malignant action, and unfortunately they are more frequently met with
than simple and well-disposed sores. The malignant sore often commences
in a warty excrescence which ulcerates at the base; the ulceration
extends, the warty appearance is succeeded by ragged and angry fleshy
points, the surrounding parts become indurated, and the stony hardness
spreads. The appearance which the sore presents is that of open
cancer, described at page 147, and represented on preceding page. The
ulceration may either be limited in depth and extent to a small part
of the lip, or may involve the greater part of the prolabium, and that
without much induration. It is generally situated on the right side
of the lower lip; sometimes in the angle of the mouth; the upper lip
is rarely affected. I have removed a few malignant ulcers from this
last situation. Sooner or later the lymphatic glands participate in
the disease; a chord of indurated lymphatic vessels is felt passing
over the jaw in the course of the facial artery, and the glands with
which these are more immediately connected, soon enlarge and become
hard. This disease, though by some pathologists said to be “improperly
called cancer,” differs apparently in no respect in its progress,
and is in all respects as malignant as the disease commencing in any
other structure and in any other way. Indurated swellings over the
jaw, lymphatic or not, usually depend on the labial disease; they in
some instances increase very slowly, in others acquire such volume
as to induce by their pressure on neighbouring parts alarming and
dangerous symptoms at an early period. Without much increase of size
they sometimes attach themselves firmly to the bone, and involve it
in the disease. The malignancy seems to acquire fresh virus, the skin
ulcerates with fetid discharge, all the neighbourhood is speedily
infected, and the patient sinks slowly under the evil.
Simple ulcers of the lips may be made to heal readily,—by abstracting
the exciting cause, preventing the motion of the lip by the restraint
of a bandage, disusing the part as much as possible, and by employing
such applications to the sore as are best suited to the character and
appearance which it may present; but it must be borne in mind that
all remedies can be of little service unless motion of the lip be
prevented. Sores of a bad kind must be attacked early, otherwise no
hope of success can be entertained. Escharotics are not to be trusted
to; the knife is the only effectual means of removing the disease.
When the sore does not involve much of the lip, the molar teeth
having been lost, and the alveolar processes absorbed, the cheeks
are thus rendered flabby and relaxed: in such circumstances, all the
diseased part is taken away with facility, and the features are not
thereby deformed, but rather improved. The part cut away resembles
the letter V, the angle being towards the chin: this form of incision
is preferable, on account of the diseased portion being chiefly in
the prolabium, and the parts afterwards coming together very neatly
and readily. The lip is stretched by the operator and his assistant
laying hold of the prolabium on each side of the portion destined to
be taken away; a narrow straight bistoury is321 passed through the lip,
at the angle of the form of incision; and the operator, standing in
front of the patient, makes the first incision towards himself, by
bringing the knife up to the prolabium. He then takes hold of the
part to be removed, and laying the edge of the knife on the prolabium
at the other side of the induration, cuts down to the point where
the instrument originally entered. The incisions must always be made
far from the indurated parts. The edges of the wound are retained
in apposition by means of convoluted suture, as formerly described.
When the wound is extensive, as when a considerable part of the cheek
is involved, approximation may be accomplished by a few points of
interrupted suture, and afterwards the parts may be more securely and
accurately fixed by convoluted sutures placed between the interrupted.
When a large portion of the cheek is removed, as for disease which had
commenced at the angle of the mouth and extended around, all the parts
cannot be brought into contact, and some of the deficiency remains
to be filled up by granulation. The neighbouring parts stretch, and
the deformity that may be the immediate result of the operation in a
great measure disappears after some time. In cases of superficial and
malignant ulceration of great extent, no attempt can be made to bring
the parts together after excision: great deformity, and almost total
closure of the mouth, would be the consequence. The diseased parts must
be freely removed (for this is the primary and essential part of the
operation, all other considerations yielding to it), and the deformity
will prove much slighter than might be supposed: granulations arise,
and considerable reparation of the lost parts thence ensues. Still
there is a risk of the sore, at first healthy and active, gradually
assuming the nature of that for which the incisions were made.
It may be necessary to remove the whole lip, or the greater part of
it. Hence arises much inconvenience to the patient; he is much reduced
by the profuse secretion and loss of saliva; the surrounding parts
are excoriated and irritable; his clothes are wetted; his speech is
very indistinct; his teeth become thickly coated with tartar; and he
is in short kept in a state of constant annoyance. The part may be
supplied from under the chin; but this reparative operation should
not be performed at the same time with the removal of the original
and carcinomatous lip. By making two operations, with a considerable
time intervening, the chance of success is greater, and indeed the
difficulty is much diminished. After removal of the disease, allow
the parts to fill up by granulation and contract as far as they will,
then form a new lip. I have done so in several instances; in one case,
the parts had perished by external violence; in another, they had
been destroyed by some powerful escharotic. A piece of soft leather,
of the size and shape of the under lip, is placed under the chin, and
a corresponding portion of the integuments is reflected upwards, an
attachment being left at the symphysis menti. The callous margins of
the space formerly occupied by the original lip are pared; and the
flap, having been twisted round, is adapted to the edges of the wound,
and retained by points of interrupted or convoluted suture. To insure
adhesion, the attachment at the chin322 should be left thick and fleshy;
the flap should not consist of mere integument, but contain no small
share of the subcutaneous cellular and adipose tissues, in order that
circulation may be vigorous in the part. The integuments below the chin
are naturally lose, and consequently the margins of the wound there are
readily approximated. The flap soon becomes œdematous, and remains so
for some weeks; it must be supported by a compress and bandage. After
adhesion of its upper part is completed, the mental attachment, which
prevented the lower portion from uniting, is to be removed; a bistoury
is introduced beneath the non-adhering point, and carried down so as
to divide the attachment, which is then removed by a second stroke
of the knife. The lower part of the flap is now laid flat and close
to the chin, and supported by a bandage. In the adult, union may be
retarded by the edges of the flap twisting inwards, and interposing the
hairs upon them between the opposed surfaces; when such is the case,
the offending margins must be pared away. The advantages of such an
operation, when successful, are too evident to require detail.
Removal of glands in the neck or beneath the jaw, that have become
diseased in consequence of malignant disease in the lip, is attended
with danger, and not followed by any benefit. But for this disease I
have known most bloody and cruel operations undertaken,—even portions
of the jaw to which the glandular tumours adhered have been cut out.
Such proceedings cannot be too strongly reprobated.
Congenital Deficiencies of Lips, Palate, &c.—Congenital deficiency
of the lip uniformly occurs in the upper one; it is either simple or
complicated. Frequently there is only a fissure on one side of the
mesial line. This may, though seldom, be combined with division of the
soft or of the hard palate; or there may be a fissure on each side of
the mesial line, with an intervening flap. The flap may be either of
the same length as the rest of the lip, or more or less shortened; and
it may be either free, or attached to part of the alveolar process.
In such cases as the latter, the central alveolar processes and
teeth often project considerably beyond the arch of the hard palate,
greatly increasing the deformity. The deficiency of the lip produces
a disgusting and horrible deformity of the countenance; and when
there is division of the palate, the voice is indistinct, or almost
unintelligible.
The simple fissure of the lip, without deficiency of the palate, is
easily remediable by operation. As already mentioned, the fissure is to
one side of the mesial line; and its edges, covered by a continuation
of the prolabium, are rounded off at their lower part. The operation is
not attended with much loss of blood, nor is it very painful. It can
be performed at any period of life, but in young children it is not
advisable to have recourse to more severe operations on these or other
parts. Children bear the loss of blood badly, and their nervous system
is apt to be shaken; convulsions are induced, and often terminate
fatally. The most proper age for removing deformity by operation is
from two and a half to four years; there is then no323 danger incurred,
and during the growth of the individual the parts recover more and more
their natural and healthy appearance.
The operation for single harelip consists in paring off freely the
edges of the fissure, and removing completely the rounded corners
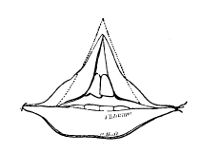 at the free margin, thus. This is most neatly, quickly, and easily
accomplished by passing a straight bistoury through, from without
inwards, so as to penetrate the membrane of the mouth, above the angle
of fissure. The parts are stretched by the fingers of the surgeon
or assistant, whilst the instrument is carried downwards, so as to
detach a flap composed of the edge and rounded corner. Unless the
rounded portions are taken clean away, an unseemly notch is left in
the prolabium, where in the natural structure is prominent. A similar
proceeding is followed on the opposite side. Hemorrhage is prevented
by the assistant making gentle pressure whilst he stretches the lip.
Two sewing needles, the heads covered with a small nodule of sealing
wax, are introduced as directed after the operation for removal of
diseased parts in the lower lip, and the twisted suture completed. For
some years I have used pins made purposely; they are spear-pointed
and tempered near their points. From their length they can be easily
inserted without being fixed in a handle, or provided with a head. One
needle should always be passed close to the free margin of the lip.
No further dressing is required, for reasons already assigned. The
forceps of different kinds for holding the edge during its removal are
worse than useless; and paring with scissors is to be reprobated, as
an effectual means of preventing immediate union. By the plan above
recommended, bruising is avoided, and union takes place rapidly.
at the free margin, thus. This is most neatly, quickly, and easily
accomplished by passing a straight bistoury through, from without
inwards, so as to penetrate the membrane of the mouth, above the angle
of fissure. The parts are stretched by the fingers of the surgeon
or assistant, whilst the instrument is carried downwards, so as to
detach a flap composed of the edge and rounded corner. Unless the
rounded portions are taken clean away, an unseemly notch is left in
the prolabium, where in the natural structure is prominent. A similar
proceeding is followed on the opposite side. Hemorrhage is prevented
by the assistant making gentle pressure whilst he stretches the lip.
Two sewing needles, the heads covered with a small nodule of sealing
wax, are introduced as directed after the operation for removal of
diseased parts in the lower lip, and the twisted suture completed. For
some years I have used pins made purposely; they are spear-pointed
and tempered near their points. From their length they can be easily
inserted without being fixed in a handle, or provided with a head. One
needle should always be passed close to the free margin of the lip.
No further dressing is required, for reasons already assigned. The
forceps of different kinds for holding the edge during its removal are
worse than useless; and paring with scissors is to be reprobated, as
an effectual means of preventing immediate union. By the plan above
recommended, bruising is avoided, and union takes place rapidly.
Fissures, more or less extensive, of the hard palate, generally
attend double harelip. The position and size of the intermediate
portion of the lip, and of the superior maxillary bone, are various;
and the operator, in forming his plan of procedure, must be guided
by the state of the parts. If the fissures are not very wide—if the
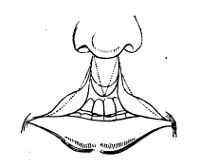 intermediate portion of bone, that adhering to the septum narium, is
not prominent—and if the soft parts covering this are free and long,
the operative procedure is simple. Two such operations as are described
for single harelip, the latter performed at an interval of some weeks,
are required. Thereby the intervening flap is united first to one side,
and then to the other.
intermediate portion of bone, that adhering to the septum narium, is
not prominent—and if the soft parts covering this are free and long,
the operative procedure is simple. Two such operations as are described
for single harelip, the latter performed at an interval of some weeks,
are required. Thereby the intervening flap is united first to one side,
and then to the other.
If the flap is short and free, without osseous projection, the
operation may be concluded at once, thus:324— The edges are pared on both
sides, and the parts brought together as in single harelip, the small
intervening flap not preventing apposition below. One pin is passed at
the prolabium, the other traverses the flap. In all cases, in fact, the
operation may be concluded at once.
When the bone projects, and the flap is long, the parts may be rendered
favourable for the operation by gentle and continued pressure; the
osseous prominence being reduced, so as to restore the natural position
of the soft parts.
When, as not unfrequently occurs, there is projection of the bone,
and the soft and hard parts seem to be incorporated with the apex of
the nose—when, in short, little or no intermediate flap exists, the
protruding portion of bone may be removed by cutting forceps down to
the level of the palatine arch; and then the soft parts can be brought
together by one operation, as for single harelip.
In some cases, when the space between the palatine plates of the
superior maxillary bone is wide, it may be necessary, by mechanical
contrivance, fitting on metallic apparatus possessing a strong spring,
to approximate the bones before attempting to unite the lip. The cases
must be very rare, where the soft parts cannot be otherwise brought
together: when they can be united, their equable and continued pressure
will have the effect of gradually approximating the hard parts.
When the hard palate is deficient, the patient is subjected to great
inconvenience from food escaping into the cavities of the nose, and, in
later life, horrid wretchedness of articulation occurs. It can readily
be understood, that surgery is of very little avail here. Recourse
must be had to mechanical contrivance. A plate of metal (gold or
platina), or a piece of ivory, or of sea-horse bone, may be fitted to
the opening, and retained either by accurate adaptation, having sponge
or caoutchouc attached to the upper surface, or by wires, elastic or
not, resting on the neighbouring teeth. It may be made of a piece with
artificial teeth, if any are required. The sponge is objectionable,
as retaining the discharge, and thereby imparting an unpleasant odour
to the expired air. But it is no easy matter, and often altogether
impracticable, to retain such apparatus when the soft palate is also
deficient. The time at which such contrivance is to be adapted may
admit of some dispute. If done early in life, the natural tendency
of the parts to approximate may be interfered with and subverted; if
dispensed with till a later period, the patient gets into a habit
of snuffling and speaking so indistinctly, that the closing of the
aperture is productive of little or no improvement. Perhaps the period
of commencing the child’s education should be delayed till he be seven,
eight, nine, or even ten years of age, and then the artificial palate
may be applied advantageously in every respect.
Fissure of the soft palate is usually accompanied with separation
of the bones from which it is suspended. The size of the fissure is
various, and depends very much upon the state of the hard parts. In
some cases, the extent of separation is great; in others, the edges
are readily approximated by making the patient throw the muscles
into action. The latter class admit of operation with a view to
permanent union of the edges of the fissure. But it is a proceeding325
which, to insure success, requires not only great steadiness,
coolness, and dexterity on the part of the operator, but the utmost
courage, submission and self-denial on the part of the patient. These
qualifications can scarcely be expected in patients under twelve or
fourteen; and, consequently, the operation should not be attempted till
after that time of life.
Before proceeding to operate, it should first be ascertained that the
fissure is not of such extent as to prevent apposition of its edges,
without great dragging of the parts; for, if the separation be wide,
temporary approximation may perhaps be effected by ligatures strongly
applied, but the apposition will not be complete or accurate throughout
the whole fissure, and adhesion will not take place; the palate will be
too much stretched, as to throw off the ligatures by ulceration at the
transfixed points of its margins. The patient must be made aware of the
nicety of the operation, of the responsibility that rests upon himself,
and be exhorted to steadiness and patience. A single exclamation of
pain may subvert the whole proceedings. He is seated opposite to a
strong light, and made to open the mouth wide; if necessary, the jaws
may be kept separate by a wooden wedge, placed so as not to interfere
with the operator. The head is thrown back, and held steadily by an
assistant. The operator depresses the tongue by the forefinger of the
left hand. A long, narrow, sharp-pointed bistoury is passed through
the velum, close to its attachment with the palatine plate, and about
a sixteenth part of an inch from the edge of the fissure: it is then
carried downwards to the point of the uvula, so as to detach a narrow
slip from the whole edge. The same is done on the opposite side of the
fissure during the proceeding, and to facilitate it the point of the
uvula on each side may be held by long and properly pointed forceps.
After allowing the patient a short rest, the coagula and mucus are
cleaned away from the parts, to prepare for union. Long bent needles,
in fixed handles, and armed, are passed through the pared edges on each
side. On one side the ligature is thin, the opposite thick and strong;
the former is attached to the loop of the latter, and withdrawn,
leaving the strong ligature passed through both apertures; and by this
the margins are gradually approximated, and retained by a firm knot. A
second point of suture, and a third, if necessary, is applied in the
same way, and as represented in the “Practical Surgery,” p. 558. Or a
single short curved needle may be used. It is introduced by means of a
portaiguille, with a long handle, and passed through, first from the
outside of one edge, and then from the inside of the other. A ligature,
either of thread or of pewter wire, can thus be conveyed at once; if
the latter is employed, it is secured by twisting, and the ends cut off
by pliers; the needle is attached to the wire by a female screw in its
end. It is advisable to make incisions in the direction of the fissure
on each side, through the mucous lining, in order to take off the
strain from the stitches.
Afterwards, success depends on the patient. All attempts at
articulation, and even deglutition, must be strictly forbidden for
three, four, or five days.
326
Inflammation of the Soft Palate, Uvula, and Tonsils, requires in
general little surgical treatment. Reiterated attacks may sometimes be
traced to the progress of a wisdom-tooth, or to the presence of stumps
in the posterior part of the upper or lower jaw. Perhaps the most
common cause is sudden suppression of the discharges from the skin, and
from the adjoining mucous surfaces, in consequence of exposure to cold.
The affection is accompanied with pain and difficulty in swallowing,
and frequent and difficult excretion of mucus. The secretion of the
saliva is increased, the attempts to swallow it are frequent, and the
inflamed parts being thereby put in motion, the pain is aggravated.
From the inflammatory action extending along the Eustachian tube, the
patient describes the pain as shooting towards the ear. The parts are
red, and soon becomes swollen; in some cases to so great an extent,
as completely to prevent deglutition; occasionally the breathing is
impeded; but the inflammatory swelling must be very great indeed,
to obstruct the openings into both mouth and nostrils, and thereby
threaten suffocation. The voice is hoarse, croaking, and husky; and,
when the swelling is considerable, the patient speaks only in a
whisper. The internal swelling is often accompanied by an external
painful tumour of the lymphatic glands, and the pain is much increased
by external pressure. There is more or less concomitant fever, preceded
by slight shivering.
Removal of the local cause, and mild antiphlogistic measures, are
usually sufficient to effect resolution, and put a stop to the disease.
General bleeding will seldom be required; blood is abstracted locally,
either by scarifying the internal surface, or by applying leeches at
the angle of the jaw. Fomentations afford much relief, and may be
applied either externally, or internally by inhalation of the steam of
water, or of water and vinegar. The greatest benefit is experienced
from this remedy during the early stage, it being then employed either
to promote salutary effusion and effect resolution, or at a later
period to forward the secretion of purulent matter. At the same time,
antimonials, purgatives, warm drinks, diaphoretics, and the pediluvium,
are not to be neglected. In the relaxed state of the parts, after
subsidence of the violent symptoms, stimulating and astringent gargles
may be used with advantage.
But in neglected cases, or those originally violent, suppuration,
sometimes extensive and dangerous, occurs in the cellular tissue,
betwixt the pillars of the soft palate, or betwixt the layers of the
velum. The swelling thereby formed may be so large as to impede the
passage of air by both the mouth and nostrils. The mouth is opened with
difficulty and pain; deglutition is seriously impeded, or altogether
impracticable; the voice is weak and indistinct; and the countenance
is swollen and discoloured. Life is endangered by the risk of the
purulent matter bursting out suddenly during the painful and laborious
efforts at respiration, and escaping into the air passages; fatal
results have thus taken place, and to prevent such the abscess should
be opened early. When the swelling is large, and attended with alarming
symptoms, the matter is most conveniently evacuated by a flat and long
trocar and canula. If the abscess be small, and the breathing not
affected, there will be no danger in327 allowing the collection to burst
spontaneously. Suppuration may also occur in the external glandular
tumour, or in the surrounding cellular tissue. When sloughing to any
extent takes place, it is in patients of an extremely debilitated habit
of body, or when the affection is attendant on disease of a malignant
character. Metastasis may take place to the larynx, to the trachea,
or to the lungs, either spontaneously, or in consequence of repellent
applications.
Chronic abscesses are occasionally met with in these parts, or
behind the upper part of the pharynx, unconnected with disease of the
subjacent bones. The matter must be evacuated as soon as its existence
is ascertained. No great accumulation should be allowed to take place
in any situation, far less in the immediate neighbourhood of important
parts.36
Scarification of the tonsils and surrounding membrane is seldom
required. A lancet concealed in a canula, with a spiral spring
to withdraw its point, is used for this purpose, and for opening
abscesses; but dangerous and fatal results may ensue, and have actually
followed such incisions of these parts. A sharp instrument directed
outwards, made to penetrate either by the rash thrust of an ignorant
and careless practitioner, or by a hurried movement of an unsteady
patient, may reach the common trunk of the temporal and internal
maxillary arteries, or even the internal carotid. The sheathed lancet
may be useful in the hands of such as are not habituated to the use
of instruments; but scarification of the parts and puncturing of
abscesses can be effected safely by a straight, sharp-pointed bistoury,
covered with a slip of lint to within three-quarters of an inch of its
point. The patient’s head is steadied by an assistant, the point of
the instrument directed backwards, not at all outwards, and its edge
upwards so as to avoid wounding the tongue, which is also to be kept
out of the way by the forefinger of the left hand.
New formations about the isthmus faucium are rarely met with. Small
warty excrescences, and small pendulous, fatty, or polypous tumours,
are occasionally seen. These, if productive of inconvenience, can be
easily removed by cutting instruments.
Enlargements of the uvula and tonsils are common, impeding deglutition,
and producing indistinct and burring articulation. If large,
respiration is interfered with.
328
Elongation and Enlargement of the Uvula attends inflammatory attacks
in the fauces, but may continue for a long time afterwards. The
organ is increased in volume, both in length and in breadth, from
interstitial deposition of new organised substance, and from unusual
vascularity. The inconvenient size produces nausea and cough; it is
even said that the tumour has, in some instances, got entangled in the
rima glottidis, suffocating the patient, or at least giving rise to the
most alarming symptoms. In some cases the elongation appears to have
kept up cough and expectoration for months or years.
The parts may be touched with a bit of sponge, dipped in the tinct.
muriatis ferri; but a more useful remedy is the powder of alum, applied
either on a spatula, or by insufflation. Astringent decoctions, or
solutions, are of little use. But in cases of large and long continued
enlargements, the swelling cannot be expected to subside under
such treatment, and recourse must be had to curtailment by cutting
instruments, of which the best for this purpose are long blunt-pointed
scissors and forceps, with hooked points. The patient is made to open
his mouth wide; the surgeon then introduces the instruments into the
month, and watching an opportunity when the uvula is nearly stationary,
suddenly seizes and clips off a sufficient portion. This is followed by
instant relief.
Frequently an œdematous swelling of the uvula, of a crystalline
appearance, resembling a large grape, accompanies ulceration in the
neighbourhood; puncturing of the part, and attention to the cause of
the affection, are sufficient for the cure. When the bloodvessels of
the uvula are in a state of chronic enlargement, scarification is also
employed with advantage.
Chronic Enlargement of the Tonsils occasionally takes place in
children, but generally in persons from eighteen to twenty-four
years of age, or in such adults as are subject to irritations in the
neighbourhood of the organs. A delicacy of constitution is supposed to
be indicated by the affection. One or both tonsils may be enlarged,
usually both. The surface of the tumour is irregular; the mucous
follicles are enlarged, and often filled with sebaceous matter. The
swellings in each side gradually approach each other, meet, and by
narrowing the isthmus, seriously interfere with the functions of the
parts. Little pain is felt, and that is dull, occasionally shooting
through the ear. Respiration is at all times fettered, and during
sleep noisy. Occasionally the swellings exceed their usual size,
from some accidental excitement of the circulation. They may subside
very considerably on the removal of the cause, or abatement of its
operation, for there is nothing malignant in their nature. It is true,
as I have seen, that the tonsils may be involved in malignant disease
spreading from the neighbouring parts; but in the affection under
consideration, no mark of malignancy appears, as far as I know. There
is mere enlargement and opening out of the texture, without much, if
any, change in structure or consistence; the part may be cut into
without the risk of exciting unhealthy action, and the divided surface
cicatrises readily.
Deobstruents, and iodine, as the most efficient, may be given, with329
perhaps some effect. In the adult, when the affection is troublesome,
permanent, and of long duration, the exuberant matter must be removed,
and this is accomplished either by ligature or by incision. The
former method is the more difficult, tedious, painful, inconvenient,
and dangerous. It is seldom that one ligature, with a simple noose,
suffices; it is necessary to transfix the tumour, and, separating
the portions of the ligature, to include the upper and under halves
in distinct nooses. The latter method is the preferable. It is not
requisite to cut out the whole tonsil, and there is risk in attempting
such a measure, but that part only is removed which projects beyond the
arches of the palate and the natural level of the gland. Long curved
scissors may be employed, but the straight probe-pointed bistoury
is more convenient; and this, to insure security, may be blunted to
within an inch and a half of its point, or rolled so far in lint.
To facilitate incision, the tumour is laid hold of by a sharp hook,
or, what is better, by a vulsellum. Occasionally violent attempts
at retching occur during the operation; but there is little pain or
hemorrhage. The complicated machines invented for this purpose are
worse than useless. The healing of the sore is hastened by fomentations
and mild gargles, and by either stimulating or soothing applications,
as circumstances require.
Excision of the tonsils is said to produce the bad effect of changing
the pitch of the voice—taking from the high, and adding to the
low notes. I have performed the operation, as above described, on
professional vocalists, to remedy indistinctness of articulation and
constant hoarseness, with the desired effect, and without altering
either the pitch, quality, or compass of the voice. No doubt,
unpleasant results might follow extensive incisions of the parts, as
division of the anterior fold of the palate, and removal of the whole
tonsil; but by paring off the prominent parts of the glands no risk is
incurred.
Ulcers of the Palate, &c., are said to have arisen almost uniformly
from contamination of the system, following sores on the genital
organs. Now, at least, they seldom and scarcely ever occur from this
cause, unless most execrable practice has been resorted to. Foul and
extensive ulcers of the membrane of the mouth, of the tongue, of
the gums, and of the folds of the palate, are common in those who
have used mercury recently; and those whose constitutions have been
saturated with mercury, or who have taken only alterative doses for a
considerable time, are for a long while liable to ulcerations of these
parts on exposure to moisture and cold—one set of sores healing, but
others soon breaking out. It is, indeed, very rare to meet with sores
in these situations that are not thus accounted for: certainly such
as are by recurrence deep, extensive, and troublesome, are not seen
unless in those who have suffered from mercurial medicines. Slight
excoriations are not uncommon in individuals of the soundest and most
untainted systems; but even in very young subjects, if the sore is of
considerable size, and slow in healing, it will generally be found
that some preparation of mercury, probably calomel, had been given
previously, and perhaps without precaution and care. Calomel, as well
as other forms of the mineral, is too often and too freely given,330
and without proper consideration; the ruin of many good constitutions
is attributable to this cause, and to this cause alone. How long
mercurial poisons continue to exercise a prejudicial influence on
the constitution, is a question not easily determined. In many, its
dominion is long and powerful. Frequently its effects are developed
years after its exhibition, from accidental circumstances, such as
change in the mode of living, derangement of the stomach and its
appendages, exposure to inclement weather, change of climate, &c.
Sores form in various situations, between the pillars of the fauces—in
the site of the tonsils—on the uvula, and by its side—on the posterior
and anterior surfaces of the pendulous velum; sometimes the ulceration
appears to have extended from the nostrils. Often the uvula is entirely
lost; it is not long since I saw two uvulæ, in one day, as black as a
bit of coal, surrounded by ulceration, and just about to drop away.
Ulceration of the posterior surface of the velum is marked by dark
redness, and swelling of the anterior. Sometimes it happens, that
by deepening of the ulcers, the velum is perforated at one or more
points, and the edge of the opening healing, a permanent deficiency
remains. The whole of the soft palate may be destroyed, either by one
extending ulceration, or by repeated attacks. When cicatrisation takes
place, the posterior nares are narrowed, deformed, or even completely
closed. Along with ulceration of the fauces, abscesses frequently form
in the coverings of the hard palate; they are either the consequence
or the cause of necrosis of part of the bone. Whatever their origin,
more or less of the bone with which the matter is in contact, dies and
separates; and thus openings are established between the cavities of
the mouth and nostril. This is productive of great inconvenience, the
patient speaks very indistinctly and, when taking food, a part of the
more fluid ingesta returns by the nostrils. During the progress of the
exfoliation, the breath is intolerably fetid.
Such is an outline of mercurial products in the mouth. Eruptions and
ulcers on the surface of the body often accompany or follow them;
and the patient gets into a bad state of health—becomes, in short,
cachectic.
The state of the system must be ameliorated if possible; and chiefly
by attention to the digestive organs. These may be improved by such
medicines, as ipecacuan, taraxacum, gentian, rhubarb, scammony,
aloes,—given in various doses and combinations, according to the
circumstances of the individual case. The first two possess many of
the good qualities of calomel, in regard to the biliary secretion, and
leave no evils behind them. Sarsaparilla is a most important remedy,
and the form of its exhibition should be varied when its effects begin
to diminish. The different applications which may be made to the sores
have been mentioned formerly; of them all, the nitrate of silver is
the most generally useful, either in solution or in substance. It is
used at intervals of two or three days, not to destroy living texture,
but to diminish irritability and dispose to heal. If there be no great
loss of substance, deficiency in the soft parts may be repaired by
operation after the ulcerative disposition has ceased. In deficiency
of the palate—during the progress of the ulceration in331 the bone and
the parts investing it, and for some time after it has ceased—the
inconvenience is lessened by filling the opening with crumb of bread
softened, and made into a paste by kneading; this must be frequently
renewed, otherwise it collects discharge, and becomes offensive.
After cicatrization of the margins, and contraction of the opening, a
metallic plate may be fitted in.
ULCERS OF THE TONGUE.
Ulcers of the Tongue.—Such as are not of a malignant kind are readily
healed on improving the state of the digestive organs and general
health. The state of the organ indicates that of the chylopoietic
viscera, it enjoys intimate sympathy with the other parts of the
alimentary canal, and why it should suffer from derangements of them is
readily understood. The sores may be continued by local irritations, as
by friction on encrusted tartar, or sharp or decayed portions of teeth,
or by repeated application of heat, as in smoking. In consequence of
long-continued irritation, like similar ulcers of the lips, they take
on malignant action. The malignant ulcer generally occurs in patients
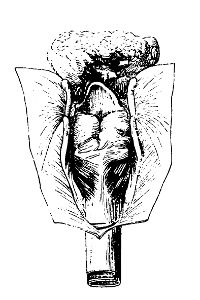 past the meridian of life. Yet I have seen the greater part of the
tongue involved in carcinomatous swelling in young subjects; from one
girl, twelve years of age, I was obliged to remove one-half of the
organ vertically. Stony induration surrounds the exposed surface to
a considerable extent, and the sore presents all the characteristic
appearances of cancer. In many cases the induration precedes
ulceration, in others follows it. A most extensive and dreadful disease
of the organ is here represented; along with induration of the whole
organ, ulceration had penetrated like a tunnel from the apex to the
base; œdema of the glottis supervened. Sooner or later the absorbents
are affected, becoming swollen, painful, and hard; and, as in malignant
affections of other parts, the disposition and action is not limited to
those in the immediate neighbourhood of the primary disease. The tongue
is subject to simple induration, which is totally unconnected with
malignant disposition, and subsides on improvement of the digestive
organs; occasionally repeated leeching of the part accelerates the cure.
past the meridian of life. Yet I have seen the greater part of the
tongue involved in carcinomatous swelling in young subjects; from one
girl, twelve years of age, I was obliged to remove one-half of the
organ vertically. Stony induration surrounds the exposed surface to
a considerable extent, and the sore presents all the characteristic
appearances of cancer. In many cases the induration precedes
ulceration, in others follows it. A most extensive and dreadful disease
of the organ is here represented; along with induration of the whole
organ, ulceration had penetrated like a tunnel from the apex to the
base; œdema of the glottis supervened. Sooner or later the absorbents
are affected, becoming swollen, painful, and hard; and, as in malignant
affections of other parts, the disposition and action is not limited to
those in the immediate neighbourhood of the primary disease. The tongue
is subject to simple induration, which is totally unconnected with
malignant disposition, and subsides on improvement of the digestive
organs; occasionally repeated leeching of the part accelerates the cure.
Enough has already been said about removing the local irritating cause,
when such can be discovered; and the maxim, though most important,
need not be formally repeated in regard to affections of the tongue.
The simple ulcer heals under the usual applications to sores or mucous
surfaces, the general health being at the same time attended to. For
malignant disease, nothing but very early removal of the part can
avail. But this is not always either advisable or practicable: the
disease may have involved the organ too extensively, and the lymphatics
may have too widely participated in the action.332 When the diseased
part is small, and nothing contraindicates surgical interference, it
may be removed by the bistoury; usually the bleeding is very slight,
but if troublesome it is easily arrested by the cautery. When the
disease is extensive, ligatures are to be employed. During the process
a vulsellum is useful for grasping the morbid part, and securing the
organ. The ligatures should be strong, and are introduced by needles
in fixed handles. They may either be passed at once, or be preceded by
finer ones, by which they are afterwards drawn through. The tongue is
transfixed beyond the induration, and, if one ligature is sufficient,
its noose is divided, and the parts tied separately, so as to include
the mass. But frequently several ligatures are required, and their
portions must be so disposed as not only to isolate all the indurated
and ulcerated part, but also some of the neighbouring sound structure.
They are tied firmly, to cut off vitality as completely as possible,
and at once. Considerable swelling and profuse salivation follow, but
gradually subside. In a short time fresh ligatures are passed through
the old perforations, and drawn from time to time, till the part
sloughs and drops away. This will not be found necessary if incisions
are made betwixt the parts of the ligature in the first instance, so as
to permit of their being tightly drawn. The swelling may be relieved
by hot fomentations, and opiates mitigate the pain. The discharge is
profuse and fetid. A weak solution of the chloride of soda, vinegar
with honey, or a solution of the mel boracis, may be used as gargles.
The healing of the wound is to be promoted by applications suited to
the appearances which it may assume.
Inflammation of the Tongue occasionally occurs during certain
eruptive diseases, and sometimes in consequence of accidental
circumstances, as stings in the part from venomous insects; but it
is not a common, affection, and is generally produced by the abuse of
mercury. When that poison was used more freely than now, the disease
in question was by no means rare. It was then customary to see
patients who were made to spit some gallons in a day, for the cure of
 a venereal affection, supposed or real, with their faces swollen, and
their tongues protruding from their mouths, enormously enlarged. This
consequence of the exhibition of mercury is more apt to occur in some
constitutions than in others, and I have seen it produced in a violent
form by the patient’s taking only two Plummer’s pills. In this case
the patient, an old gentleman of broken constitution, had been filled
brimful of mercury, over and over again, for one disease or another in
warm climates.
a venereal affection, supposed or real, with their faces swollen, and
their tongues protruding from their mouths, enormously enlarged. This
consequence of the exhibition of mercury is more apt to occur in some
constitutions than in others, and I have seen it produced in a violent
form by the patient’s taking only two Plummer’s pills. In this case
the patient, an old gentleman of broken constitution, had been filled
brimful of mercury, over and over again, for one disease or another in
warm climates.
The tongue swells rapidly, fills the mouth, and protrudes of a brown
colour, from effused serum, with great enlargement of the papillæ.
The patient is unable to speak, deglutition and respiration are much333
impeded, and thirst is excessive. In some instances the inflammation
proceeds to suppuration, but the more general termination is resolution.
In the more mild cases, a cure will generally be procured by
evacuating the bowels freely by means of saline purgatives, and by
local abstraction of blood; the blood may be obtained either from
the application of leeches, from opening several of the enlarged
superficial veins, or from slight scarifications. Afterwards astringent
lotions may be employed. But in more severe cases of glossitis, the
tumour is productive of very great inconvenience to the patient,
and is not unattended with danger; the difficulty in breathing may
amount almost to suffocation, and in such the treatment must be
active. Several free incisions are to be made longitudinally on the
dorsum of the tongue; from these the effused fluids are evacuated, a
considerable quantity of blood escapes, and consequently the tumour
speedily subsides. Superficial incisions are not sufficient, and
the practitioner should not shrink from cutting tolerably deep; for
although the wounds may appear ghastly in the engorged and tumid
condition of the organ, yet when the swelling subsides, and the tongue
regains its usual bulk, their size, as in other situations, is so
remarkably diminished, that they resemble trifling scarifications, and,
in some instances, are almost imperceptible. Their extent and number
must vary according to the size of the tumour, and the urgency of the
concomitant symptoms. If such practice should fail in diminishing
the swelling, and affording relief to the respiration, it may become
necessary to perform tracheotomy. If the inflammation terminate in
suppuration, the abscess must be treated on the same principles as
those occurring in other parts of the body.
The tongue is also subject to gradual and permanent enlargement. A
remarkable case of this nature occurred to me some years ago, and I
shall here detail it shortly. The patient was a male, aged 19. The
tongue was of a very large size, compressible and elastic, projected
three or four inches from the lips, and completely filled the cavity
of the mouth. It was of a dark brown hue, in some places livid; its
surface was rough, at some points granulated, at others fissured,
and at many traversed by large venous trunks. At the back part of
the dorsum, the papillæ were much enlarged, granulated points were
numerous, and several plexuses of dilated blood vessels ramified
immediately beneath the investing membrane. There was occasional
bleeding from an ulcerated fissure near the centre of the dorsum,
and also from the lateral parts of the protruded portion: in the
latter situation, several cicatrices were visible. Saliva flowed in
a continuous stream from the apex of the tumour. The lower jaw, much
separated from the upper, was elongated and unusually narrow; the
teeth, particularly those in front, were placed at a distance from each
other, were covered with tartar, and projected almost horizontally
from the sockets. A depression was felt at the symphysis mentis, as
if the two portions of the jaw were asunder, and the intervening
space occupied by ligamentous matter. The enlargement was congenital,
and the organ swelled rapidly, it was stated, every three months to
a much larger size, and subsided gradually. The bleeding was most334
frequent and profuse when the swelling was greatest, and then too he
suffered much pain in the part. Articulation was very indistinct,
and could be understood only by those who were accustomed to be
near him. He swallowed, and even masticated pretty freely. From the
periodical enlargement and diminution, from the repeated hemorrhages,
and from erectile tissue being visible on many parts of the surface,
I considered the structure of the tumour to be in part similar to
that of aneurism by anastomosis, and to be throughout extremely
vascular. I therefore did not attempt removal by incision, but in the
first instance intercepted its vascular supply by tying both lingual
arteries. The tumour was not affected immediately on the application
of the ligatures, but soon began to diminish gradually. Everything was
proceeding favourably; but, on the seventh day, the tongue was attacked
with inflammatory swelling, which advanced unsubdued, notwithstanding
the most active treatment. Sloughing commenced at the apex, and
appeared extending backwards; I then isolated the protruded portion
of the organ by ligature, and thus removed it in three or four days.
At that time he complained of no pain, and felt very comfortable.
But his system became much disordered soon after; abscesses formed
rapidly over both wrists and on the hands, unhealthy infiltration of
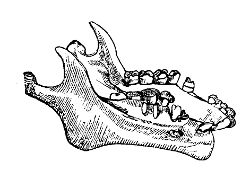 the cellular tissue took place at the root of the tongue, and amongst
the deep muscles at the upper part of the neck, the parts became
gangrenous, and he died. Dissection showed that the greater part of
the tumour was composed of erectile tissue. A sketch of the lower jaw
is here appended, in order to show the alteration in form, both at the
symphysis and in the rami, which had resulted from the pressure of the
organ and the necessarily constant open condition of the mouth.
the cellular tissue took place at the root of the tongue, and amongst
the deep muscles at the upper part of the neck, the parts became
gangrenous, and he died. Dissection showed that the greater part of
the tumour was composed of erectile tissue. A sketch of the lower jaw
is here appended, in order to show the alteration in form, both at the
symphysis and in the rami, which had resulted from the pressure of the
organ and the necessarily constant open condition of the mouth.
Enlargement of the tongue occasionally takes place in young subjects,
a sort of simple hypertrophy, which often proceeds to a very great
extent. The increase goes on in a remarkable manner after the organ is
extruded beyond the lips, so that the patient is incapable of covering
it. Portions of the swelling of a V shape have been removed in such
cases, and the edges of the wound put together. But by well managed
and continued pressure the absorption of the swelling has been brought
about, the organ has been reduced within the oral aperture, and a cure
has then rapidly followed.
Division of the Frænum Linguæ is sometimes, though rarely, required.
Division can be necessary only when the frænum is so short as to
confine the point of the tongue, prevent free motion of the organ,
and thereby cause indistinctness of articulation. Infants are often
supposed by anxious mothers to have their tongues unduly confined,
when no such malformation exists; in such circumstances, it is
almost needless to observe that the part ought not to be interfered335
with. And even when there is confinement, division should not be had
recourse to, unless the child is prevented from taking nourishment. The
operative procedure is simple and safe. The tongue is raised towards
the palate, either by a spitula or split card—or, what is better, by
the fingers—and the frænum is cut across to a sufficient extent by
blunt-pointed scissors.
Ranula is a swelling produced by accumulation in, and distention of,
the extremity of the combined ducts of the sublingual and submaxillary
glands. The extremity of the duct contracts, or is completely closed,
and in consequence of the saliva and mucus (the one the secretion of
the gland, the other of the duct) collect, distend the canal, and cause
thickening of the parietes. Thereby a tumour is formed, which, in
some instances, attains a very large size, displacing in some measure
the neighbouring parts, and incommoding the tongue in particular.
Indistinct utterance and impeded deglutition result.
The orifice of the duct, if discovered, is to be dilated gradually
by occasional introduction of variously sized probes. Often it is
necessary to make a small incision in the situation of the orifice, and
introduce a bit of gum-elastic bougie, by continuing the use of which
for some time, permanency of the opening may be obtained.
Deposition of Earthy Matter—principally phosphate of lime—not
unfrequently takes place in the extremity of the submaxillary and
sublingual ducts, and the concretion so formed is often of considerable
size; some are larger than an almond. The colour is either white or
yellowish, and the surface either smooth or roughened by nodules;
in all the calcareous matter is friable, and disposed in concentric
layers. They are of the same nature as the earthy deposits, called
tartar, which form on those teeth opposite to the extremities of the
salivary ducts. The foreign body produces uneasiness in the mouth,
swelling, and indistinctness of speech; occasionally painful swelling
of the salivary gland and surrounding parts takes place. Concretions
also form, though very rarely, in the extremity of the parotid duct,
and are attended with like inconvenience; of this I have seen only two
cases.
The foreign body is easily removed; an incision is made through the
membrane of the mouth, and the concretion dislodged by forceps, a
scoop, or the fingers. The saliva regains its course, and irritation
subsides. Sometimes the foreign body is exposed by ulceration, and
might ultimately escape from its bed spontaneously.
 A figure of a salivary calculus of considerable size is here given.
When the concretion is small, its extraction is not so easily
accomplished as might be supposed. It is apt to slip back out of reach,
so that it cannot be seized, brought forward and extracted either by
scoops or forceps. The flow of saliva must be promoted by giving the
patient something to masticate; the probability is, that the foreign
body will336 then be presented, and perhaps expelled, if the opening of
the duct has been previously dilated. A young lady was brought to me
lately suffering great uneasiness from the presence of a concretion,
not larger than a millet-seed. She complained of great pain under the
jaw on seeing anything savoury, that, as the vulgar phrase is, made her
mouth water. Various unsuccessful attempts had been made to remove it.
A small incision of the surface of the duct was made, but the foreign
body eluded the grasp of the forceps, and completely disappeared. The
patient was given a bit of bread to chew, and almost immediately the
concretion was expelled.
A figure of a salivary calculus of considerable size is here given.
When the concretion is small, its extraction is not so easily
accomplished as might be supposed. It is apt to slip back out of reach,
so that it cannot be seized, brought forward and extracted either by
scoops or forceps. The flow of saliva must be promoted by giving the
patient something to masticate; the probability is, that the foreign
body will336 then be presented, and perhaps expelled, if the opening of
the duct has been previously dilated. A young lady was brought to me
lately suffering great uneasiness from the presence of a concretion,
not larger than a millet-seed. She complained of great pain under the
jaw on seeing anything savoury, that, as the vulgar phrase is, made her
mouth water. Various unsuccessful attempts had been made to remove it.
A small incision of the surface of the duct was made, but the foreign
body eluded the grasp of the forceps, and completely disappeared. The
patient was given a bit of bread to chew, and almost immediately the
concretion was expelled.
Tumours, unconnected with the salivary ducts, occasionally form
in the loose cellular tissue under the tongue. They may be either
sarcomatous or encysted; the former are rare. I have removed several
solid tumours, principally adipose, from this situation. They were
loosely connected, and taken away without almost any dissection; indeed
they were lifted out with the fingers, after division of the membrane
of the mouth and of the cellular cyst which surrounded them. One was
as large as an orange, and of a flattened form. The tongue had been
displaced by the swelling, and articulation, deglutition, and breathing
impeded. The patient, an old lady, had a good recovery. The case had
been by some mistaken for ranula; and I mention this circumstance, lest
others may reckon more on the situation of a swelling, than on its feel
and other external characters. A sketch of the tumour is given at page
137.
Encysted tumours below the tongue are common. The cysts are generally
thin and adherent, the contents albuminous and glairy. They attain a
large size, and prove very inconvenient. Occasionally the cysts are
thick and more loosely attached; such usually contain atheromatous
matter. I removed one uncommonly large, from the inner surface of which
numerous hairs were growing.
Encysted tumours here can seldom be removed by dissection; the depth of
their situation, their firm connexion, the awkward situation in which
the patient is necessarily placed, and the risk of hemorrhage, forbid
the surgeon from attempting regular extirpation. A more simple and
equally effectual procedure is as follows:—The membrane of the mouth
and the cyst are divided by the point of a bistoury; and if the tumour
be large, and the distention great, an oval portion of the parietes
may be cut out. The contents are thus evacuated. The bleeding is
allowed to cease, and the cavity having been wiped out clean, a stick
of caustic potass is applied to the surface, so as to annihilate the
cyst effectually. This I believe to be the only radical and safe mode
of removal; after any other, the tumour is certain to be reproduced.
It has been recommended to pass a seton, so as to excite inflammatory
action, and lead to obliteration of the cyst. I have made trial of this
practice, but most dangerous swelling ensued, the mouth was rapidly
filled, and the system alarmingly shaken; after all the disease was not
eradicated.
Tumours beneath the tongue, however originating, occasionally inflame,
and become the seat of unhealthy abscess. A large and painful swelling
forms, and projects under the chin. The matter337 gradually approaches
the surface, and perhaps evacuates itself imperfectly into the mouth,
or the integuments give way, and afford an external issue. In such
cases, an early incision from the mouth may prevent the internal
mischief, and the disfiguration of the countenance which would
otherwise ensue may, in short, limit the suppuration; at a later period
a free opening requires to be made below the chin, in the mesial
line, and in the direction of the muscular fibres. A ready drain is
thus obtained for the matter, and the cavity of the abscess gradually
contracts.
Tumours of the Gums are usually hard, and not inclined to increase
rapidly. They are of the same consistence as the parts to which they
are attached, and grow either inwardly, outwardly, or both. They
surround one or more teeth, which at last become loose, the alveolar
processes then soften, and form part of the swelling.
These may degenerate, and grow rapidly, or the tumour may be soft
(tumor mali moris) from the first. The attention of the patient is
directed to the part by the occurrence of discharge from about the
teeth, which loosen one after another. A soft tumour arises from the
sockets after either extrusion or extraction of the teeth, it grows
rapidly, and involves more and more of the gums and alveolar processes.
Angry ulceration attacks the prominent parts of the swelling; the
bone is softened to a considerable extent around; the discharge is
thin, bloody, and profuse. Ultimately the lymphatics become affected,
neighbouring parts are contaminated, malignant action acquires a firm
footing, and extends, the patient becomes hectic, and dies.
Each kind of tumour should be removed freely and early; the untoward
results of the latter have been already mentioned; and I believe
that, if the former be allowed to proceed unchecked, the tumour may
ultimately extend to the bone, and osteosarcoma of the jaw, more or
less extensive, be established. The disease must be attacked at an
early period of its existence, and teeth, sockets, and soft parts taken
freely away, by means of a strong knife and saw, or cutting forceps.
After excision, the actual or potential cautery should be applied,
otherwise the disease is apt to recur. Portions of involved bone, which
may have escaped the knife, are by the caustic made to exfoliate. When
the potassa fusa is used for the purpose of destroying what cannot be
readily reached by the knife, and when it is pushed into the alveoli
and applied to the altered gum, its action must be limited by the
immediate use of vinegar, diluted or not.
Inflammation of the gums and neighbouring parts is attended with
violent pain, swelling, and throbbing, difficulty in opening the mouth,
headache, and fever. Inflammation of the soft parts runs its course
speedily, and, as the cause is seldom removed during the existence
of the inflammatory action, generally terminates in suppuration, so
giving rise to what is termed parulis or gumboil. Frequently the
inflammation extends to the sockets of the teeth, which seldom resist
the action long, but from their low degree of vitality soon become338
necrosed; and by the presence of the dead portions of bone, a fresh
accession is given to the disease. Severe pain is experienced on
touching the teeth whose alveoli are affected; they project and become
loose; purulent matter is secreted, and oozes out between the loosened
teeth and diseased gums. Abscesses form, and point in different
situations; the gums are tumid and spongy; through the openings in them
the bone can be felt bare, and the purulent matter is situated within
or around the alveoli, and under the mucous membrane and cellular
tissue which invest them.
When the inflammation has been either intense from the first, or of
long duration, it not unfrequently happens that abscesses form within
the substance of the jawbone, and occasionally to a considerable
extent—a portion of the bone having become inflamed, and the action
terminating in suppuration and partial caries. This is more apt to
occur in the inferior than in the superior maxillary bone; and,
if allowed to proceed, the osseous cyst containing the purulent
matter gradually enlarges, the plates of the bone are separated and
expanded, the parietes become attenuated, and the affection is termed
spina ventosa. Purulent collections in this situation also seem, in
many instances, to arise from, or at least to be preceded by, the
formation of a cyst around the decayed root of a tooth. Such cysts
are generally of small size, and pyriform shape; externally they are
 smooth, membranous, and of rather a delicate texture; internally,
they are lined by lymph of soft consistence, and contain purulent
matter. In fact, they are purulent depôts, which form in consequence of
inflammation around the fangs of the teeth, and from which the matter
is occasionally discharged through a small aperture at the upper part
of the cyst, and by the side of the affected tooth. They sometimes
attain a very considerable size.
smooth, membranous, and of rather a delicate texture; internally,
they are lined by lymph of soft consistence, and contain purulent
matter. In fact, they are purulent depôts, which form in consequence of
inflammation around the fangs of the teeth, and from which the matter
is occasionally discharged through a small aperture at the upper part
of the cyst, and by the side of the affected tooth. They sometimes
attain a very considerable size.
Mercury is perhaps the most common cause of this disease; but it is
also produced by certain operations on the teeth, and by the presence
of carious teeth or of stumps.
Caries of the teeth is an extremely common affection, and in some
instances seems to arise from an unhealthy state of the constitution;
but it is most frequently produced by the teeth having suffered from
chemical agents, as when the mineral acids have been taken for a
considerable time as medicines, or when the individual is in the habit
of consuming sweetmeats, and confections. Sometimes the disease remains
almost stationary, and may give little or no annoyance for a number of
years; in other instances, its progress is very rapid. A portion of the
tooth gradually decays, and this is at first unattended with any uneasy
sensation; but when, from continuance of the destructive process, the
central cavity has been exposed, the pain is excruciating, attended
with headache, and swelling of the surrounding soft parts. In general,
the progress of the disease may be arrested by removing the diseased
portion, and stuffing the cavity, before any pain has been felt.
But after the central cavity of the tooth has been exposed, filled
with fungous mass, as here seen, or from their growing in a faulty
direction, and pain consequently experienced,339 the most effectual
remedy is extraction. The patient from whom the specimen below was
obtained, perished in consequence of the extensive abscesses of the
mouth and neck, consequent upon the awkward position of the wisdom
tooth.

From the presence of carious teeth, or decayed portions of teeth, many
evils both local and general ensue, besides inflammation and abscess.
They are frequently the cause—and the sole cause—of violent and
continued headaches; of glandular swellings in the neck, terminating
in, or combined with abscess; of inflammation and enlargement of the
tonsils, either chronic or acute; of ulcerations of the tongue or lips,
often assuming a malignant action from continued irritation; of painful
feelings in the face, tic doloureux, pains in the tongue, jaws, &c.;
of disordered stomach, from affection of the nerves, or from imperfect
mastication; and of continued constitutional irritation, which may give
rise to serious diseases.
Along with abscess of the gums, purulent matter often collects in the
cellular tissue of the cheek or of the chin. In the latter situation,
the inflammation and suppuration are often caused by the teeth in
the front or side of the lower jaw being too much crowded together.
When the teeth are crowded together, the patient, of course, cannot
be effectually benefited till one or more of them are extracted, and
sufficient space allowed for development of the others. The abscess
gives way, and discharges its contents often both externally and
internally, and a fistula remains, which cannot be got rid of, unless,
as in most other affections, the cause be removed. The cavity of the
abscess must be opened into either from without or within, and after
the subsequent irritation has subsided, the cause must be removed;
carious teeth or stumps are not to be taken away during the inflamed
state of the parts, but after the pain and inflammation has subsided in
consequence of free evacuation of the purulent matter. After these have
abated, and not till then, the offending bodies are to be extracted,
both in order to procure a more speedy and effectual cure, and with
a view to prevent recurrence of the disease. If a portion of the jaw
has become necrosed, the sequestra are to be extracted as they become
loose, and openings and counter-openings must be made, according to
circumstances, so as to afford a free outlet to the matter.
THE EXTRACTION OF TEETH
The extraction of teeth, the crowns of which have not been destroyed,
is accomplished most readily by the dexterous use of vari340ously shaped
forceps. Stumps may be occasionally extracted also by forceps, but
the lever is generally required to loosen them from their sockets.
The old key instrument and pelicans are now superseded by those above
mentioned.37
341
 Spina Ventosa of the Jaw often originates, as before mentioned, in
a small cyst at the root of a decayed or dead tooth. An enormously
large one extracted along with the stump attached is here shown: it is
sketched from a specimen in the collection of Mr. Nasmyth, of Edinburgh.
Spina Ventosa of the Jaw often originates, as before mentioned, in
a small cyst at the root of a decayed or dead tooth. An enormously
large one extracted along with the stump attached is here shown: it is
sketched from a specimen in the collection of Mr. Nasmyth, of Edinburgh.
The disease is usually situated on one side of the lower jaw; but
sometimes occurs in the upper, and is at first unconnected with the
cavity of the antrum. Inflammation has taken place in the internal
structure of the bone; matter is secreted by the medullary vessels, and
collects in the cancellated texture. Purulent formation advances, the
cancelli are broken down, the external laminæ of the jaw are extended,
protruded, and attenuated; and then the internal 342cavity enlarges,
containing pus, perhaps mixed with other fluids, and with disorganised
particles of bone. Sometimes the collection proceeds slowly, and the
expansion of the bone is gradual and uniform; in other instances, the
swelling rapidly attains a large size. As the disease advances, the
bony parietes become remarkably thin and delicate, particularly at
the more prominent parts of the tumour; and at many points bone is
deficient, and its place supplied by membranous expansion. Occasionally
alteration of structure takes place in the cyst; solid matter is added,
either bony or fibro-cartilaginous, and morbid action proceeds in the
new deposit. In acute cases, in which the secretion and distension
are rapid, severe pain is felt in the part at the first, and usually
continues but little unabated; when the swelling is slow and gradual,
considerable pain is experienced during the inflammatory stage, but
soon diminishes, or ceases entirely. In every instance, the features
are deformed, and the functions of the mouth more or less impeded.
Osteosarcoma may supervene on spina ventosa—morbid action occurring
in the parietes, and morbid deposit ensuing, as in the following
instance:—The patient was a male, aged twenty-one. Swelling had
existed for a considerable time at the posterior part of the lower
jaw on the left side. The wisdom tooth and last large grinder, their
pulps probably having been blighted, never appeared, and the swelling
occupied their situation. The bone was expanded on each side; the upper
surface of the tumour was soft, its growth had been gradual, and no
great pain or uneasiness was experienced. I cut out an oval portion of
the cyst where it projected into the mouth, and well-digested matter
was evacuated; a seton was then passed out near the angle of the jaw,
and worn for some weeks. The plates of the bone approximated, the
cavity contracted, and the discharge ceased. Two years afterwards rapid
swelling took place in the same situation, suppuration occurred, and
the matter was again discharged by incision; the tumour then subsided.
Again inflammatory swelling occurred twelve months afterwards; the
same course was followed and the patient relieved. A hard swelling
now occupies the jaw from its angle to the canine tooth, it is
increasing in size; the necessity for its removal is apparent, and has
been decided upon. Very shortly after writing the above, the patient
submitted to the disarticulation and removal of fully half of the jaw,
 represented here. He made a rapid recovery, and showed himself to me
and the pupils at the hospital a short time since, and fully five years
from the time of the operation, in remarkably good health, and very
little deformed by his loss. His whisker effectually conceals the mark
of the incisions.
represented here. He made a rapid recovery, and showed himself to me
and the pupils at the hospital a short time since, and fully five years
from the time of the operation, in remarkably good health, and very
little deformed by his loss. His whisker effectually conceals the mark
of the incisions.
But in general, after free evacuation of the purulent matter from a
bony cavity, even of very large size, the space between the parietes
diminishes rapidly, the distended and attenuated bone contracts and is343
condensed, the new deposition is absorbed, and the parts regain their
natural and healthy appearance.
In the slighter cases of spina ventosa, removal of the offending teeth
or portions of teeth, is generally sufficient; the matter escapes
freely enough from the sockets, and the discharge soon ceases. When the
cavity is considerable and its parietes thin, a counter-opening at the
base of the jaw is required; and it is often of advantage to introduce
a small cord from the opening in the mouth through the counter-opening,
and to continue its use for a short time, drawing it backwards and
forwards in the cavity occasionally. For making the counter-opening
and placing the seton at the same time, a strong needle in a fixed
handle is most convenient. This practice I have employed in a good many
instances, and can confidently recommend as successful. In a large
spina ventosa, not complicated with solid growth, the parietes may be
removed freely and with safety; the cavity is dressed to the bottom,
and gradually fills up by granulation. The division of the integuments
to expose the tumour must vary according to the circumstances of the
case; the incision of the bone will generally be accomplished by a
strong bistoury. Such procedure will seldom fail in procuring a cure,
and is less severe, less dangerous, and productive of less deformity,
than division of the jaw and entire removal of the diseased portions,
an operation which can very seldom be warranted for spina ventosa. In
the following case, the tumour was the largest of this kind which I
have met with in the jaw, and yielded to the treatment just noticed.
The patient was a male, æt. 48; he applied to me in 1821. The tumour
had been of three or four years’ duration, equalled a large fist in
size, and involved the left side of the lower jaw at the junction
of the ramus with the body of the bone. The sac extended behind the
coronoid process, and downwards, through the substance of the jaw,
amongst the hyoid muscles. Several carious teeth and stumps were
imbedded in the swelling; the projection was chiefly lateral, the
parietes were yielding, and the line of the jaw could be traced from
below. There was occasional slight discharge of purulent matter from
the neighbourhood of the involved teeth. The cheek was laid open, and
the bony and cartilaginous parietes of the cavity completely removed;
the bleeding from the bony surface was arrested by cautery and pressure.
The soft parts united kindly, and the patient obtained a rapid,
perfect, and permanent cure, returning home with the cheek united in
ten days after the operation.
Solid Tumour of the Lower Jaw—Osteosarcoma—commences in the
internal structure of the bone, frequently in the neighbourhood of
stumps. The origin may be traced to external injury of the part; or the
disease may take place in the jaw, either along with osteosarcomatous
tumours of other bones, or subsequently to their development; in such
circumstances a peculiar disposition of the system is the only cause
that can be assigned. The tumour generally occupies the lateral parts
of the bone. Its growth may be either slow or rapid, and is attended
with dull uneasiness, rather than acute pain.344 At first the morbid
deposit is confined to the cancellated texture, but as it increases
the external laminæ are distended, and at last give way at one or
more points, and the tumour protrudes fungous into the mouth. The
consistence of the mass is various, it may be soft and brain-like,
or cartilaginous, mixed with bone and fibrous matter in various
proportions; but the anatomical characters of these tumours have been
already detailed, and need not be here repeated. The features are much
deformed, the swelling seriously incommodes the neighbouring parts;
the teeth loosen and drop away, and fungi arise from the sockets; a
fetid, thin, sometimes bloody discharge is secreted copiously, and the
health declines. The part protruding around the gums is deeply indented
by the teeth of the upper jaw; it separates the jaws to a greater or
less extent, prevents closure of the lips, induces salivation, and
impedes the taking of nourishment. The tumour is one of those which
are apt to be reproduced, and if unmolested, gradually undermines the
system, and ultimately the patient perishes very miserably. At one time
every instance of it was regarded as hopeless; but of late a great
many tumours, in various stages of advancement, have been removed
successfully by British and foreign surgeons. In some instances,
the portion of the jaw containing the morbid growth has been sawn
out; in others, one half of the bone, or more, has been removed by
disarticulation, after being divided beyond the diseased part. A very
few weeks ago, I had occasion to remove fully three-fourths of this
bone, from the site of the first large molar on the left side to the
condyle of the right. The patient, an elderly female, is convalescent.
The operation is severe, and to a spectator shocking enough; but it can
be undertaken with safety, and in most cases with almost a certainty of
favourable termination. In no other way, assuredly, can the disease be
eradicated. Partial excisions, applications of the cautery, &c., only
hasten the malignant process.
To expose the tumour and admit of the bone being readily divided,
incision of the soft parts requires to be extensive. And previously to
determining on the plan of operation, the extent of the disease must
be ascertained accurately. If, for example, the tumour is included
between the lateral incisor tooth and last molar on the same side—these
teeth must be extracted to permit division at these points. A semilunar
incision may then be made along the base of the jaw, the horns of the
incision pointing upwards and passing over the space which was occupied
by the extracted teeth. The flap is dissected up, and the membrane of
the cheek divided along the line of incision. The bistoury is then
carried along the inside of the bone so as to divide the membrane of
the mouth and separate the attachments of the muscles. The tongue is
pushed aside, and a copper spitula placed under the jaw at the part to
be divided, in order that the soft parts may not be injured during the
sawing. A small narrow saw, or one commonly known by the name of Hey’s,
is applied to the bone at the points where the teeth were extracted,
and by a few motions of this instrument a notch is made of no great
depth; a pair of strong cutting pliers are placed in the track, and by
them division of the bone is accomplished with equal neatness, and345
much more rapidly than if the use of the saw had been continued. The
pliers should be strong in every point, and the handles long, to afford
the advantage of a powerful lever. In edentulous subjects, as the one
alluded to above, there is no necessity for using the saw at all: the
bone is at once and easily cut by the forceps. The chain saw has been
recommended for performing the section of the bone, but I have not yet
seen one to be depended on; it is not only slow, but uncertain, in its
operation.
The incisions may be made otherwise. The cheek may be divided by
passing through it a long narrow bistoury, close to the anterior edge
of the masseter muscle, and carrying the instrument forwards and
through at the angle of the mouth. From each extremity of this incision
another is made downwards, the anterior one inclining forwards, the
other backwards. By reflection of the flap thus formed, the bone is
exposed more easily, rapidly, and perfectly, than by the former mode
of incision. The objection to this mode of procedure is the deformity
occasioned by the scars, though, if care is taken in putting the edges
together, this is very slight indeed, and not remarkable.
In either method, no artery, except the facial, requires to be secured
by ligature. After division of the bone, the attachments of the
tumour, which may not have been separated previously, are cut with the
bistoury, the cavity is filled lightly with charpie, and the incisions
are carefully and neatly put together, and retained by points of
interrupted and twisted suture; the latter form of suture being adopted
at those points where accurate coaptation is most important.
The symphysis of the lower jaw has been removed, and its extirpation
may again be rendered necessary, either on account of tumour commencing
in its internal structure, or from disease of the sockets extending
deeply and approaching the base. I removed it in a case of malignant
disease, by which, and by the applications used as remedies, great
ravages had been made on the under lip; the gums and alveoli were
involved, as also the bone, to a considerable extent, without any
apparent affection of the lymphatics. Nothing untoward occurred in the
operation, and the case was proceeding favourably; but after some weeks
the patient was seized with violent erysipelas of the face and head,
and perished. One objection to the operation is, that the muscular
attachments of the tongue to the symphysis cannot be divided without
some risk; the antagonist muscles are unrestrained; the os hyoides
and root of the tongue may be drawn backwards upon the forepart of
the vertebræ, so as to close the air-passage, and cause suffocation.
This is guarded against by the introduction of a thick ligature. The
disposition to retraction soon ceases.
Disarticulation of one side of the jaw is not unfrequently necessary;
it is absolutely required when the tumour encroaches upon and involves
the angle and ramus. It is a more severe operation than excision
of part of the bone, and attended with greater risk; yet it may be
advised and undertaken with a very fair and probable chance of ultimate
success. The incision of the cheek is made to incline more upwards
than those recommended for partial excision, and is extended to over
the articulation of the jaw; from this point, another is made346 in
the direction of the ramus, and prolonged an inch or more beyond the
angle. A third incision is made perpendicular to the first, or to the
lower lip, over that part of the bone in front which is to be divided.
The flap is turned down, and the muscles and membrane of the mouth
separated from the bone opposite to the last incision; after which,
the finger is passed through to complete the detachment. A preferable
form of incision along the posterior border of the ramus and under the
base of the jaw and tumour to over the point at which the bone is to be
sawn, but without division of the lip, is recommended in the Practical
Surgery. This method I have practised repeatedly; the cicatrix is
then completely out of sight, and in the male is entirely covered and
concealed. During the cure, also, the discharges escape more readily,
the opening being quite dependent. The bone is then divided at that
point by the saw and pliers, the tooth in the line of the track having
been extracted previously to the commencement of the operation. The cut
end of the jaw is laid hold of by the left hand, and depressed, and
the bistoury carried backwards along the internal surface, to effect
detachment as far as the angle. The bone is still more depressed, and
the temporal muscle cut from the coronoid process. The mass is thus
loosened, and forced downwards and backwards on the neck; the forepart
of the capsule is then cut, and the bone twisted out. Separation of
the remaining attachments is completed by a few rapid strokes of the
knife, and the whole mass removed. Hemorrhage is then to be permanently
arrested, but instead of immediately tying every open mouth which
presents itself, it is sometimes better to expose the common trunk of
the internal maxillary and temporal arteries—which is easily effected,
as it emerges from under the digastric muscle—and to pass a ligature
beneath it, by means of an aneurism needle. This is more quickly done
than the applying of ligatures to the many branches of this trunk
which have been divided. The other vessels—the facial, branches of
the lingual, &c.—are then tied, the cavity is filled with charpie,
and the incisions of the soft parts are carefully closed. In these,
union by the first intention usually takes place nearly throughout the
whole extent; suppuration occurs from the deep wound; the charpie is
dislodged gradatim, and removed; granulations spring up; and, after
some time, the cavity is obliterated. The cheek must necessarily fall
inward very considerably, but the deformity is not to be compared to
that caused by the tumour. During granulation, the patient is made
comfortable by the frequent use of tepid gargles, lodgement of pus in
the mouth being thereby diminished. Articulation and mastication are
not so perfect as when the jaw was entire and sound; but the patient
gradually becomes accustomed to the want, and these functions improve.
A contrivance described in the Practical Surgery is used to prevent
the remaining portion of jaw from being drawn towards the mesial line,
and to keep the teeth opposite to those of the corresponding side of
the upper jaw. Partial paralysis of the side of the face necessarily
follows, for there is no possibility of accomplishing disarticulation
of the jaw without dividing many branches of the portio dura.
Supposing that the portion of the jaw between the angle and
sym347physis had been removed on account of osteosarcoma, and that the
ramus subsequently became affected, it is no easy matter to effect
disarticulation, as I have experienced.—The patient was a female, aged
30, of delicate constitution, and subject to toothache from infancy.
I removed an osteosarcomatous tumour, extending from the angle to
the canine tooth, on the right side. Division was made wide of the
existing disease, and the sawn surfaces appeared quite healthy; but
about five months afterwards, symptoms of return occurred in the
ramus, and ten months after the first operation disarticulation was
indispensable. The operation was accomplished with very considerable
difficulty, on account of there being no lever to overcome the action
of the temporal muscle. After separating the attachments as much as
possible, an attempt was made to force down the coronoid process, from
under the zygoma, by pushing the lower end of the bone backwards, in
order to divide the insertion of the temporal muscle; but this proved
ineffectual. The capsular ligament of the joint was then divided, and
the bone with difficulty turned over from behind, forwards. It was then
detached underneath the coronoid process, pulled down from under the
zygoma, and the temporal muscle at length divided at its insertion.
In none of these operations is there a necessity for preliminary
exposure and ligature of either the carotid artery or its branches; by
so doing, a great addition is made to the patient’s sufferings, the
real operation is only commenced when the patient supposes it should
have been finished, and he is thus annoyed and worn out. The flow of
blood is easily moderated, or altogether arrested, by the pressure of
an assistant’s fingers against the forepart of the vertebræ, below the
angle of the jaw.
The position of the patient is either recumbent, with the face turned
from the operator, or sitting with the head supported and steadied.
The instruments required are, a very strong, sharp-pointed bistoury,
for division of the soft parts; saws, of which Hey’s is to be preferred
for notching the bone; strong and long pliers, for completing its
section; an aneurism needle, for securing the common trunk of the
temporal and internal maxillary artery; dissecting and artery forceps,
hooks blunt and sharp, narrow copper spatulæ, ligatures, &c.
Wounds of the Face and Neck.—Accidental wounds of the face may
involve the more important blood vessels and nerves, and interfere with
the eye or its appendages, with the nose, or with the mouth. Injury
of these parts is to be avoided in incisions premeditated for the
removal of disease or deformity; and, in such premeditated wounds, the
line of incision should always be, if possible, in the direction of
the muscular fibres. The bleeding seldom proves troublesome; pressure
on the vessels, as they pass over the bones, arrests it temporarily;
and ligature is seldom required, accurate adaptation of the divided
surfaces proving sufficient for effecting permanent closure of the
divided branches. Paralysis, more or less extensive, follows division
of the nerves and muscles. But paralysis of the face also arises
from a variety of other causes; it348 often remains after injuries of
the head, probably in consequence of extravasation on the brain; it
attends on morbid formations in the substance of the brain, or in its
membranes, and follows long-continued irritation in the neighbourhood
of the nerves. Paralysis from the last-mentioned causes is not likely
to be recovered from; that following simple division of nerve, may
disappear after a considerable time, the nervous tissue reuniting,
and resuming its functions. When there is reason to suppose that the
nervous function is alone deranged, while the structure remains sound
and the continuity undissolved, advantage may follow the application of
strychnine to a raw surface over the course of the affected nerves.
In Tic Doloureux, division of the nerves of the face, as they pass out
of the foramina, is seldom resorted to; nor ought it to be practised,
unless at the urgent request of the patient, and after all other means
have failed to afford relief; and even then the operation is scarcely
warrantable, since it may be said never to have succeeded in affording
permanent relief. We must trust to milder measures, to the removal of
local irritations, to paying strict attention to the digestive organs,
to the administration of purgatives, tonics, and anodynes; occasionally
benefit has resulted from the external use of the nitrate of silver,
applied so as to cause very slight vesication. Ointments containing
veratria and aconitine have been used with advantage, and the endermic
application of the salts of morphia has also been found useful.
Spasmodic action of the muscles of the face, without pain, sometimes
follows wounds and other injuries of the nerves which supply them;
and sometimes no cause can be assigned for the occurrence. In this
affection also, the application of nitrate of silver to the integuments
over the nerves may sometimes be made with advantage.
Division of the parotid duct, or wound of the gland itself, is
occasionally followed by the formation of a fistulous aperture,
discharging saliva over the cheek. We endeavour to prevent this by
accurate union of the recent wound. After the fistula has formed, an
opening is to be made from it into the mouth, and kept pervious; the
external aperture is then closed by suture after excision of the smooth
edges, or is made to contract by the repeated application of a heated
wire; pressure alone is of little use.
All wounds of the face are to be put into the most favourable state
for healing without granulation, so that deformity may be prevented as
much as possible. The twisted suture is best adapted for this purpose;
more accurate coaptation being thereby obtained than by the interrupted
form. In extensive wounds, the parts may be brought somewhat into their
proper position by a few points of interrupted suture; twisted sutures
are then placed in the intervals, and the isinglass plaster is of use
in closing those points which may still gape slightly; in many cases,
the greater part of the approximation may be accomplished by isinglass
plaster alone.38
349
Deep wounds behind the angle of the jaw, and at the lateral and lower
parts of the neck, are highly dangerous; indeed they are almost
certainly and immediately fatal, as can readily be understood when
the large bloodvessels and important nerves are considered which have
their course in these parts, and which must be either wounded or
completely divided. The bleeding has in some cases been arrested by
immediate ligature of the divided extremities of the vessel, by firm
and permanent pressure, or by pressure at first, and ligature of the
trunk of the vessel on the recurrence of hemorrhage after the lapse of
many days; of these methods immediate ligature of each extremity is
certainly the safest and best. In lacerated wounds violent hemorrhage
may take place some time after the infliction of the injury, from
ulceration or sloughing of a large artery; in such circumstances either
permanent pressure may be resorted to, or ligature applied to the
vessel above and below the open point.
Dissections for the removal of morbid growths in the situations
just mentioned must be conducted with much caution, and with a full
recollection of the relative anatomy. Unless the tumour be tolerably
loose and defined, it ought not to be interfered with. But it is to
be recollected that tumours of these parts are bound down by their
condensed coverings—the platysma myoides and cervical fasciæ; and that
after division of these, the tumour, if not intimately incorporated
with the neighbouring tissues, is loosened, and often enough can be
readily detached.
From constant external pressure, tumours growing rapidly spread
amongst the deep parts, and often form firm attachments. The parotid
is displaced, and almost entirely absorbed, by the pressure of tumours
growing out of the lymphatic glands which are lodged on its anterior
surface. Such tumours attain a large size, and occupy the exact
situation of the parotid; on their removal, the space betwixt the
angle of the jaw and the mastoid process is completely exposed, and
the styloid and pterygoid processes can be distinctly felt. From these
circumstances many have been led to believe that they have dissected
out the parotid; but this and the other salivary glands seldom if ever
degenerate. And if the parotid do become the seat of carcinoma or
medullary sarcoma, it is impossible to remove it with either safety
or advantage. Even in the healthy state, removal of the parotid is a
troublesome dissection; and the difficulty must be greatly increased
when enlargement has taken place from disease, when neighbouring parts
are involved, when firm and deep connections have been formed, and
important structures encroached upon. I have taken away many tumours
from the site of the parotid, and 350some of large size, but would
scarcely attempt, or boast, as some have done, of having removed the
diseased gland itself.
The incisions, for the removal of the tumours of which we have been
speaking, are to be made in the direction of the fibres of those
muscles which are interposed betwixt them and the integuments, in the
direction of the bloodvessels and nerves, and towards those points
where the vessels are expected to enter the diseased mass. Attention
to the last recommendation is important in order to save blood. For
when the trunks of the arteries are divided at the commencement of the
dissection, they are easily secured temporarily by the fingers of an
assistant: the operation is proceeded in and accomplished with scarcely
any further hemorrhage, and in many instances no other vessels require
ligature; whereas, if an opposite course be pursued, the same vessels
will be divided three or four different times; the hemorrhage will be
greater, and the operation delayed. By cutting also in the direction of
the vessels and nerves, fewer arteries are divided, and nerves are less
apt to be injured, than if the incisions were made across.
Wounds inflicted with the view of effecting suicide are generally on
the fore and upper part of the neck, and their severity depends on the
resolution of the individual. Some penetrate the integuments merely,
and are consequently of slight extent; there is little bleeding, and
the edges are easily brought together, after the cessation of bleeding
and when the surfaces are glazed, by inclining the head forwards, and
introducing a few points of suture. Others divide the muscles, and
branches of the lingual or of the superior thyroid arteries; such
wounds are gaping, more extensive than the former, and accompanied with
smart hemorrhage. Some penetrate the mouth, separating the os hyoides,
tongue, and epiglottis from the thyroid cartilage. Occasionally the
wound is lower, through the thyroid, or betwixt that cartilage and the
cricoid; and sometimes through these into the gullet; it is seldom
lower. Such are truly horrible; the countenance is contorted, and
presents a frightful expression; inspiration is difficult, hurried,
and noisy, and at each expiration blood frothed with air is forcibly
ejected from the wound. I have seen wounds of the trachea, near the top
of the sternum, but without extensive division of the lateral parts;
large wounds, such as are usually made at the upper part of the neck,
could not be inflicted here without division of the large vessels,
and instant death. Some determined suicides reach the vessels even
high in the neck, dividing everything down to the vertebræ; immediate
dissolution takes place from loss of blood. But, in general, mere
opening of the air-passage is all that is aimed at, there being a
vulgar notion that this is sufficient for the extinction of life. A
considerable quantity of blood is lost, though the branches only of the
external carotid are wounded, and the loss may prove fatal; but the
hemorrhage generally ceases on syncope taking place; and if the patient
be then discovered, means should be immediately adopted for permanently
arresting it. Its recurrence may cause death, on the patient recovering
from the first faint; or he may die some days after, from the effects
of loss of blood. Hemorrhage, though to no very alarming extent, is
always to be dreaded in those advanced in life; though in351 most cases
the fatal result is not attributable solely to the bleeding, but
is expedited by other circumstances, as defective supply of proper
nourishment, and an unfavourable state of the mind.
Some patients seem to be going on most favourably towards a cure, but,
within two days after the injury, are suddenly seized with difficult
breathing, and die in a few minutes. On the examination of such,
blood is sometimes found in the ramifications of the bronchial tubes,
and the lungs can contain little or no air; or the bronchial tubes
and ramifications are loaded with adherent mucus; in either case the
patients die from asphyxia. In others, nothing remarkable is observed;
perhaps passage of the air may have been prevented by inspissated mucus
lodging in the windpipe around the wound, and closing the aperture,
or by faulty adaptation of the divided surfaces. Likewise, during
motion of the head, or attempts to swallow, either the upper or lower
part of the windpipe may change its relative position; the continuity
of the tube will be thereby destroyed, either partially or wholly,
and suffocation ensue. When the wound is large and transverse, as
the majority of such wounds are, there is difficulty in freeing the
air-passage from mucus. This result becomes evident, when we consider
how coughing is effected in the healthy state of parts—that the upper
part of the windpipe is contracted by its own muscles, and the air
driven through, by sudden action of the muscles of the chest, in a
forcible and small stream, so as to carry the mucus along with it. This
process cannot be accomplished when the muscles employed in contracting
the orifice of the larynx are injured, or when an opening is formed
below the glottis, through which the patient breathes, either wholly or
in part.
In other cases, death is more slow. The patient is seized with
dyspnœa, great anxiety, and occasional spasmodic action of the
muscles of respiration, which symptoms gradually become more urgent
and alarming. They are attributable to awkward position of the
parts, to swelling around the wound, inflammatory or œdematous and
rapid or slow, or to bronchitis. To the latter affection patients
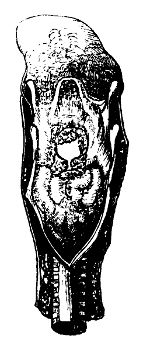 breathing through artificial openings in the larynx or trachea are
peculiarly subject, probably from the inspired air not being heated,
as in natural respiration, before it enters the bronchial tubes. A
view from behind is here introduced of the larynx of a patient who
some weeks previously attempted suicide by wounding the forepart of
the neck. By some mismanagement the edges of the incision were kept
asunder, and they cicatrised. The patient was seized with difficult
breathing, the inspirations were rare, long, and laborious; he had
threatening of suffocation during his disturbed sleep. These symptoms
were disregarded. He started up suddenly in the night, caught hold of
the patient in the next bed, and fell down in a state of asphyxia,
from which he could not be recovered. The œdematous swelling of the
rima glottidis is remarkable; beyond that is seen the rounded opening
betwixt the thyroid cartilage and epiglottis, which is in a normal
state.
breathing through artificial openings in the larynx or trachea are
peculiarly subject, probably from the inspired air not being heated,
as in natural respiration, before it enters the bronchial tubes. A
view from behind is here introduced of the larynx of a patient who
some weeks previously attempted suicide by wounding the forepart of
the neck. By some mismanagement the edges of the incision were kept
asunder, and they cicatrised. The patient was seized with difficult
breathing, the inspirations were rare, long, and laborious; he had
threatening of suffocation during his disturbed sleep. These symptoms
were disregarded. He started up suddenly in the night, caught hold of
the patient in the next bed, and fell down in a state of asphyxia,
from which he could not be recovered. The œdematous swelling of the
rima glottidis is remarkable; beyond that is seen the rounded opening
betwixt the thyroid cartilage and epiglottis, which is in a normal
state.
352
The bleeding is to be arrested as speedily as possible by ligature,
and the patient placed in bed with the head and shoulders raised. The
edges of the wound are brought together by attention to the position
of the head; but, provided the patient breathes easily with the wound
open, closure should not be attempted till after eight, ten, or twelve
hours—that is, not until all oozing of blood has ceased; the time
depends on the extent to which the air-tube has been divided. There
is little chance of immediate union taking place; and the wound not
being approximated when recent and bleeding, does not diminish the
chance, but on the contrary augments it. Adhesion is prevented by the
insinuation of air and mucus betwixt the edges, by frequent motion of
the edges on each other, by the slightest change in the position of
the head, either rotatory or nodding, by the action of the muscles of
the os hyoides, and by attempting to swallow food or saliva. Every
circumstance is opposed to complete approximation and immediate union
of transverse wounds of the throat.
Plasters and bandages surrounding the part are inapplicable, and
unwarrantable from the interruption thereby caused to breathing and
circulation; they likewise prevent the escape of mucus and air.
Emphysema is apt to occur in consequence, and may prove troublesome;
the cellular tissue of the neck becomes filled, so as to interfere
with free respiration, and the infiltration of air extends over the
face and chest. Neither can many stitches be used without bad effects.
The corners of an extensive wound may be kept together by points of
suture; and one may be placed at the middle, through the integuments
only, to prevent overlapping or inversion of the edges. The head is
placed in a comfortable position, inclined forwards, and secured by
a bandage passed round it, with the ends brought down and fixed to a
band round the chest. In many cases the patient requires to be watched
attentively, to have the motions of his hands restrained by proper
means, in order to prevent him from interfering with the wound, or
committing other insane acts which might prove dangerous. The state
of the breathing and of the pulse must be strictly attended to;
inflammatory symptoms must be actively combated, and swelling prevented
from gaining a dangerous extent, by bleeding, general and local. But
depletion is indeed very seldom necessary, the loss of blood in the
first instance proving a pretty effectual preventive of inflammation;
it is more frequently requisite to administer nourishment or even
stimulants; but these must be given gradually in those advanced in
life, and in those who have lost much blood.
The slightest difficulty or noisiness of breathing must be closely
watched, and on the occurrence of any alarming symptoms, energetic
measures adopted. Swelling about the wound, producing difficult
expectoration and a diminished current of air, may require the making
of a longitudinal opening into the trachea below the wound, and the
insertion of a tube. Thus the respiration is quickly relieved; and
the patient is soon able to regulate the size of the aperture; he is
readily taught to apply his finger over part of the orifice of the
tube, when it is wished to clear the passage from mucus. The operation
of tracheotomy should be had recourse to in such cases without
hesi353tation or delay; there is no danger from its performance, but much
from its being withheld.
If the mouth or gullet have not been opened by the cutting instrument,
or only slightly, the patient may be allowed to swallow naturally;
though it is true that even the slightest motion of the parts affects
the wound injuriously. But, as already observed, immediate union is
not to be expected; swallowing, or attempting to swallow, saliva,
produces an involuntary action of the muscles, quite as prejudicial as
the swallowing of liquids in large quantity does; and these motions
cannot be prevented, since the patient has no control over them. If the
wound of the mouth or gullet is extensive, portions of the ingesta are
apt to interfere with the air-tube, particularly if the wound is high,
and the epiglottis cut away or difigured. In such cases, soups and
other nutritious fluids are conveyed through an elastic tube, passed
by the mouth over the root of the tongue to beyond the injured part,
and introduced only when it becomes necessary to administer food; or a
small tube may be passed by the nostril, and retained. If the wound is
very severe, and the necessity for thus conveying nourishment likely
to continue long, the latter method is adopted; it is more difficult
in execution than the former, but when the instrument is once passed,
no further trouble is given to either the patient or surgeon. Small
quantities of nourishment are to be given frequently, of such strength
as the symptoms indicate; many patients have died from inattention on
this score.
Many have died suddenly and unexpectedly (though this should not be,
if symptoms and circumstances were attended to) from the effects of
apparently slight wounds; whilst others have recovered, when recovery
was unlooked for, after dreadful injuries, and these perhaps not
treated in the most approved manner. In illustration, I shall briefly
detail, though it did not fall under my own observation, an interesting
and remarkable case of recovery. A criminal under confinement attempted
suicide by transverse wound of the throat. The larynx was severed at
the upper part of the cricoid cartilage, and the cut extremities had
retracted at least three inches; the œsophagus was also cut across,
but the extent to which it had receded was not ascertained. A large
quantity of blood had been lost; attempts were made to bring the parts
together, but were abandoned on account of the violent dyspnœa which
was induced. The attendant endeavoured in vain to pass an elastic gum
tube into the gullet, from the nose and from the mouth. The patient was
kept alive by nutritious enema. On the second day after the accident,
the cut extremities of the larynx were approximated by two ligatures;
and, the retraction being thereby diminished, it was then discovered
that there was another wound between the cricoid cartilage and the
trachea. All ingesta by the mouth passed through the upper wound. On
the fifth day, the ligatures separated, and the larynx again retracted.
On the sixth, an elastic gum catheter was passed into the inferior
cut extremity of the gullet, and through this nutritious fluids were
regularly administered. The wound granulated, and filled up in some
measure; the patient continued to receive both air and nourishment354
through tubes introduced downwards from the wound in the throat. Whilst
pouring in food, saliva was secreted in the mouth in great profusion.
The sense of smelling remained tolerably acute, and he also possessed
the power of imperfect whispering articulation.
When, from the untoward circumstances of the case, or from neglect,
the opening in the windpipe remains long open, and becomes fistulous,
the larynx contracts, and the voice is in a great measure lost, the
patient breathes almost entirely by the unnatural opening, and all the
respiratory functions are conducted imperfectly. But even this state
of parts may admit of remedy, as is exemplified by the following case:
Elizabeth Oswald, aged twenty-seven, attempted suicide in 1826, and
wounded the larynx through the crico-thyroid ligament. She was under
treatment for several months; but was at length abandoned with loss of
voice, breathing entirely through a silver tube placed in the original
wound. On her applying to me, I found the larynx had contracted; an
exceedingly minute aperture, not capable of admitting a common dressing
probe, extended from the wound towards the glottis, constituting
all that remained of the upper part of the natural air-passage at
this point. Small bougies were introduced from the wound into this
diminutive canal; and by gradually increasing their size, the passage
was brought to its natural diameter in less than three months. Part of
the trachea below the wound had also contracted considerably, and was
dilated by similar means.
A long œsophagus tube was introduced by the wound into the mouth, there
laid hold of and drawn upwards, and then pushed down into the trachea,
so that it extended from the mouth to some inches below the wound of
the trachea. Its introduction was followed by a severe fit of coughing,
which lasted about half an hour. The tube, nine inches long, and equal
in diameter to the largest œsophagus tube, was retained in the windpipe
for fifteen days, during which it caused great salivation; the teeth
loosened, and the strength was extremely reduced.
The callous edges of the wound were removed by incision, and the
opening closed by suture. The tube was removed on the tenth day
thereafter, and the patient breathed well. Within a few hours, however,
respiration became difficult, and tracheotomy (below the isthmus of the
thyroid) was performed. A silver tube was introduced into this recent
longitudinal opening, and retained for five days, when it was replaced
by a smaller one. After twenty days, this tube was also removed, and
in a short time afterwards the wound closed completely. The patient
continued to breathe with ease through the larynx, and slowly recovered
her voice. When agitated, or after sudden and violent exertion, her
inspirations are a little longer than natural, but in other respects
the cure is complete. She was in very good health some years after the
restoration of the air-tube.
Laryngitis, cynanche trachealis, most frequently occurs in children,
and in them it is termed croup; but it also, though rarely, attacks
adults. The voice is brazen, hoarse, and croaking; the355 cough is
barking, and the countenance suffused. Inspiration is long, painful,
effected with much difficulty, and attended with a wheezing or rattling
noise. Expiration, on the contrary, is easy.
Difficult inspiration is a symptom common to all affections of the
larynx, and admits of ready explanation. The membrane lining the
glottis is thickened, and covered also by a viscid mucus; the passage
is thus much contracted; the muscles, by the action of which the rima
is opened, participate in the inflammatory action, and are thereby
incapacitated for the full performance of their functions. While
inspiration is thus difficult, expiration is more easy, all the
powerful muscles of the chest combining to empty the lungs of the
little air which they receive.
In croup, there is confusion and pain of the head, the lips are of a
livid hue, and the veins of the neck are much distended. Respiration
is extremely laborious, the chest and nostrils heave, and all the
auxiliary muscles of respiration are called into play. Sleep is broken
and unrefreshing; the patient starts, much alarmed, from a feeling
of impending suffocation, and catches at the nearest object. The
circulation is accelerated, and becomes weak and irregular as the
disease advances.
A common cause of croup is exposure to cold and damp; but the
frequency of its occurrence in children is attributable to dentition.
Dentition induces a long catalogue of infantile diseases, and is
intimately connected with most cases of croup. Children are besides of
a peculiarly irritable system; and in them disorder of the digestive
organs may, in many instances, be considered as at least a predisposing
cause, and in all cases it is a constant attendant on the disease. It
may also be occasioned by inflammatory action extending to the larynx
and trachea from a neighbouring surface; from the fauces, for instance.
In some instances inflammatory swelling has been produced by the direct
application of stimuli to the membrane; as by the patient inadvertently
swallowing boiling water, and a portion of the hot fluid, or rather
of the steam, being drawn into the windpipe. It is supposed that
certain slight degrees of this affection are to be ascribed to spasm;
in nervous and hysterical females, paroxysms of slight difficulty in
breathing are not of unfrequent occurrence, and in them it may be
ascribed, with much probability, to a spasmodic action. The expiration
may be then performed with difficulty, and occasionally there is almost
complete aphonia. In children, dyspnœa, apparently dependent on spasm,
is produced by some affection of the base of the brain.
The most desirable termination of the disease is of course
resolution—the cough, pain, and uneasiness subsiding, and the
constitution gradually attaining its former state of composure. Too
frequently, however, the inflammatory action proceeds unabated, and
terminates in effusion of lymph, which is generally of great extent,
adhering to the surface of the mucous lining, and forming what is
termed a false or adventitious tubular membrane. On the occurrence
of lymphatic formation, dyspnœa is much aggravated; and the second
stage of the disease is then said to have commenced. Occasionally the
patient sinks before effusion has taken place. The extent to which the356
pseudo-membranous deposit occurs is extremely various; in some cases
it is confined to the larynx, or to the upper part of it; in others
it lines the whole of the windpipe, and often is prolonged, either in
flakes or tubes, into the ramifications of the bronchi. In general,
it is not at every point adherent to the mucous membrane, but more or
less detached, particularly at its inferior extremity, by a quantity
of vitiated mucus which intervenes between it and the mucous surface,
and is intimately adherent to the latter. The mucous membrane is also
slightly elevated by effusion into the subjacent cellular tissue.
By the formation of false membrane, the symptoms may be so much
increased as to cause speedy dissolution; but in many cases the
patient’s strength is not altogether exhausted, and the extraneous
substance by its irritation causes frequent and violent attempts
to expectorate, by which the lymph is not unfrequently expelled
either entire or in irregular portions; the relief thereby afforded,
though considerable, is in general temporary, for lymph is speedily
redeposited, or there is a profuse muco-purulent expectoration, and
the patient succumbs. It has been already stated that a portion of the
false membrane is usually detached from the lining membrane of the
canal, and from this the existence of the membrane is in general easily
recognised; for on its being moved by the passage of air in the canal,
a peculiar sound is frequently audible, and has been compared to that
made by the movement of the valve or clapper of a pump. When perceived
during inspiration, it indicates that the membrane is detached at
its superior extremity; when in expiration, that the separation has
occurred inferiorly. A fatal termination may suddenly take place, in
consequence of the detached extremity being so displaced by the passage
of the air as to form a complete valve, obstructing respiration, and
causing death by suffocation.
When the inflammation extends into the bronchi and substance of the
lungs, laborious breathing and the mucous rattle occur. The bronchi are
obstructed by vitiated mucus, or by lymph, and serum is effused at the
base of the brain; and from either or both of these circumstances the
patient soon perishes. In children the gums should be looked to, and if
swollen or tender, they must be freely scarified; this always affords
relief, and often forms the most important part of the treatment. The
bowels must be completely freed from the fetid dark-coloured matter
which they contain; and if this be effected at an early period, it
will generally be sufficient to arrest the progress of the disease.
Calomel is the medicine usually preferred, not only from its excellent
qualities as correcting and purging out the vitiated secretions,
but also on account of its supposed effect of preventing lymphatic
effusion. To the procuring of copious evacuations from the stomach and
bowels, the attention of the practitioner ought to be chiefly directed
at the commencement. With the same view, emetics are of much service.
The warm bath will be of use in promoting the cutaneous discharge,
and assisting to allay irritation. When the inflammatory symptoms are
violent, bleeding, both local and general, is indispensable, and must
be had recourse to early; for during the commencement only of the
disease can it be of service. The first, or acute, inflammatory stage
is of but short continuance, speedily357 terminating in effusion; and
when this has occurred, the symptoms all denote debility of the system,
and will be irreparably aggravated by depletion. The most effectual
mode of abstracting blood, is by opening the external jugular vein,
and this may be followed by the application of leeches to the forepart
of the neck; in the second stage of the disease, their place is to be
supplied by blisters, and other counter-irritants. Much benefit will
be derived from the continued use of nauseating doses of the tartrite
of antimony; in the first stage the vascular action will be thereby
subdued, and in the second the medicine acts as a powerful expectorant,
determines to the surface, and promotes the evacuations from the
bowels. Often, however, the disease defies all sanative measures, and
advances unsubdued to a fatal termination.
Tracheotomy has been both proposed and performed in this disease.
Recourse to it is not warrantable till the later period of the
affection, and then it will be found unavailing. If performed early,
there is found no obstruction to respiration that can be removed;
it can therefore be of no service, and is not required. If it be
undertaken at a more advanced period, lymph will most probably be found
to extend below the incision; the bronchial tubes and the substance of
the lungs are then the principal seat of the disease, and consequently
the operation is futile, at least in children. When first I entered on
practice I was several times prevailed on to perform tracheotomy on
children labouring under croup; the results were unsuccessful, and from
my own experience I cannot recommend the practice.
The fauces and larynx of children are occasionally injured, as
stated above, by the attempt to swallow by mistake boiling water,
and inhaling the steam. The alarming symptoms follow in a very few
hours, in consequence of the formation of numerous minute vesicles,
with swelling, from effusion of serum into the submucous tissue.
Great pain is generally experienced at the moment, but after crying
violently the child may fall asleep and awaken croupy, and with
threatened suffocation. By this time inflammatory action has been
fairly established, the submucous effusion has begun to take place,
and it is this that gives rise to the danger. The excited action is to
be combated by leeching and exhibition of calomel in small doses, with
or without opium frequently repeated, so as to arrest the lymphatic
effusion, which is apt to supervene. When these means fail, tracheotomy
must be resorted to without delay. The fauces and upper part of the
larynx are only involved at first; this practice is sound, and good
success may be expected from the operation. The breathing has been
suddenly suspended in children by the attempt to swallow acrid fluids,
such as alkaline solutions, or concentrated acids.
Cynanche laryngea, in adults, is of comparatively rare occurrence; at
least that kind of inflammation of the windpipe, which in children
is so rapid in its progress, and so prone to terminate in effusion
of lymph, is not often met with in persons of an advanced age.
Inflammatory affections of the larynx and trachea are, however, by no
means unfrequent in adults; but are of a very different character, as
to symptoms, progress, and termination, from that affec358tion which is
strictly denominated croup. Pain is felt in the region of the windpipe,
and is aggravated by pressure on the forepart of the neck, by speaking,
and by deglutition; expectoration is increased, and ultimately
assumes a muco-purulent character. The voice is altered in tone and
 in strength, and occasionally there is complete aphonia. Frequently
these symptoms, after having continued for a short time, gradually
subside; if not, the mucous membrane, particularly in the upper part
of the larynx, becomes thickened and considerably softened in texture,
with effusion of serous fluid in the subjacent cellular tissue, and
apparently in the substance of the membrane itself. In consequence
of such effusion, the difficulty of breathing is much increased.
Occasionally lymph is effused on the surface of the membrane; but this
is seldom met with, and when it does take place, is generally confined
to the upper part of the larynx. The larynx and trachea of an old lady
of seventy years is here shown, with very extensive false membranes
blocking up the bronchi; a large portion besides was coughed up. The
specimen, a rare one, is in my collection.
in strength, and occasionally there is complete aphonia. Frequently
these symptoms, after having continued for a short time, gradually
subside; if not, the mucous membrane, particularly in the upper part
of the larynx, becomes thickened and considerably softened in texture,
with effusion of serous fluid in the subjacent cellular tissue, and
apparently in the substance of the membrane itself. In consequence
of such effusion, the difficulty of breathing is much increased.
Occasionally lymph is effused on the surface of the membrane; but this
is seldom met with, and when it does take place, is generally confined
to the upper part of the larynx. The larynx and trachea of an old lady
of seventy years is here shown, with very extensive false membranes
blocking up the bronchi; a large portion besides was coughed up. The
specimen, a rare one, is in my collection.
The effusion of serum is often abundant, causing protrusion of the
mucous membrane, and narrowing of the canal; and when it is limited
to the upper part of the larynx, as frequently happens, the disease
is termed Œdema Glottidis. In this affection, the majority of
the symptoms, which have been already enumerated as attendant on
laryngitis, are all present, and in an aggravated form. Inspiration
is extremely difficult and sibilant, and occasionally the patient
experiences a sensation, as if a foreign body were lodged in the
passage, and had changed its position on the muscles of the part being
put in motion. The symptoms of œdema come on gradually in some cases,
in others with alarming rapidity. They often follow ulcerations of the
soft palate, and of the root of the tongue, as shown in treating of
diseases of that organ, occurring on the patient being exposed to cold
or moisture, or supervening rapidly when discharge from the ulcerations
is by any accident suddenly suppressed. The difficult breathing, with
cough and violent attempts at expectoration, takes place in paroxysms,
and often to so alarming a degree as to threaten immediate suffocation,
especially during the night. The patient, if he has fallen asleep,
often starts up suddenly, and catches at the nearest object, having
dreamed probably of drowning or strangulation. Deglutition is seriously
impeded, the strength is exhausted, the body is emaciated, the features
become contracted, and evince great anxiety. As already stated, the
serous effusion is chiefly situated in the upper part of the larynx,
particularly on the lips of the glottis, and on the inferior surface of
the epiglottis; and on introducing the finger, a soft swelling can be
felt beneath this cartilage. Perhaps the following sketch exhibits the
most complete instance of œdematous swelling of the rima glottidis to
be found in collections of morbid anatomy. The patient was brought to
the Royal Infirmary labouring under all the359 symptoms of the disease in
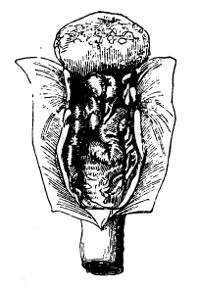 a very aggravated form. Tracheotomy was performed without delay, and
with instant relief. The patient fell into a quiet and profound sleep,
which lasted for six or seven hours. He started up suddenly and fell
down dead; probably the end of the tube had become obstructed by mucus.
It is scarcely to be supposed that the patient could have breathed at
all with such a state of parts at the top of the air-tube, as here
represented. Could any of the swelling have come on in the interval
betwixt the performance of the operation and his sudden death? In some
instances, the disease rapidly proceeds to a fatal termination, the
glottis being speedily and entirely shut by the swelling; in others,
the patient lingers for weeks, or even months.
a very aggravated form. Tracheotomy was performed without delay, and
with instant relief. The patient fell into a quiet and profound sleep,
which lasted for six or seven hours. He started up suddenly and fell
down dead; probably the end of the tube had become obstructed by mucus.
It is scarcely to be supposed that the patient could have breathed at
all with such a state of parts at the top of the air-tube, as here
represented. Could any of the swelling have come on in the interval
betwixt the performance of the operation and his sudden death? In some
instances, the disease rapidly proceeds to a fatal termination, the
glottis being speedily and entirely shut by the swelling; in others,
the patient lingers for weeks, or even months.
Depletion, local and general, especially the former, if employed on
the first appearance of the inflammatory symptoms, will often arrest
their progress; but if practised at a more advanced period, it can
be productive of no benefit, and if any advantage does follow, it
is merely temporary. Sometimes considerable benefit will be derived
from the use of blisters, or from the unguentum tartritis antimonii
being rubbed on the sides of the neck and over the larynx, so as to
produce an eruption of numerous pustules. When all hopes of procuring
resolution have passed, and when the urgent symptoms occasionally
threatening suffocation supervene, tracheotomy should be performed
without delay; and it ought to be borne in mind, that the more early
this operation is resorted to, the greater is the chance of success.
It has been repeatedly stated, that the disease is confined to the
larynx, and, in most instances, to the upper part of it; so that,
by making an opening in the windpipe below the thyroid gland, the
disease is situated above the incision, the patient breathes through
a canal which is in its healthy state, the affected parts are set at
rest, and from their remaining comparatively motionless the disease
often subsides spontaneously; if not, the various applications to the
parts can be employed much more successfully than before; for when
the parts remain subject to constant irritation from the movements
necessary for respiration and nutrition, all medicines and all topical
applications are generally productive of little or no benefit. But if
the incision be made into the crico-thyroid membrane, we shall, in
most instances, cut into the very middle of the disease; at any rate,
the affected parts can be at no great distance from the incision,
and the irritation of the tube will be a sufficient cause to excite
inflammatory action in parts contiguous to the original disease, and
already disposed to assume a similar action; thus the disease may be
extended. I have performed tracheotomy on a very considerable number of
patients afflicted with œdema glottidis, and I may say, with almost360
uniform success. The disease was speedily subdued, and in most of them
there was no great difficulty in closing the artificial aperture, and
restoring natural respiration. The relief afforded by the operation is
almost instantaneous; the performance of it, if skilful, is attended
with no danger; and want of success will generally be found to proceed
from its having been too long delayed.
In consequence of laryngitis, or of long-continued irritation in the
neighbourhood, the mucous membrane becomes indurated, and subsequently
ulcerates; or ulceration may extend from the fauces. In some cases, the
ulcers of the larynx are few, and of slight extent; in others, they are
more numerous, and of considerable width and depth; and in some there
is extensive and uninterrupted destruction of the surface, surrounded
by thickened and elevated mucous membrane. This disease is termed
Phthisis Laryngea. It is characterised by constant tickling cough
with expectoration of purulent matter; by pain in the region of the
larynx increased on pressure; by great prostration of strength, with
general sinking of the vital powers, and frequently by hectic fever.
From extension of the ulceration, the vocal chords, the ventricles
of the larynx, and the mucous folds forming the rima glottidis,
are more or less injured, and frequently altogether obliterated;
partial or complete aphonia is the consequence. In phthisis laryngea,
especially when advanced, swelling from serous effusion, to a greater
or less degree, almost certainly supervenes, the œdema is found in
the upper surface of the epiglottis, beneath the mucous membrane,
upper and forepart of the pharynx, and occasionally also in the
lips of the glottis,—an effect of the contiguous ulceration,—in the
same way as œdema glottidis supervenes on ulceration of the lining
membrane of fauces and pharynx; the usual train of symptoms denoting
phthisis laryngea may thus be interrupted by those of œdema of the
glottis becoming (each paroxysm) more and more urgent, terminating in
suffocation or relieved by tracheotomy.
From the reasons which have been already stated, inspiration is
performed with difficulty, and accompanied with a wheezing and rattling
sound, resembling the passage of air through a narrow aperture lined
with viscid fluid. Deglutition is difficult; and, from the inactive
state of the muscles which naturally close the glottis during
swallowing, and from the greater or less destruction of the epiglottis,
a portion of the fluid taken by the mouth escapes into the windpipe,
produces violent coughing, and is ejected by the mouth or nostrils.
As the disease advances, the lungs become affected, the patient is
incapacitated for ordinary exertion by the dyspnœa which ensues, he
grows weak and languid, and seems, in fact, to labour under phthisis
pulmonalis. Not unfrequently the two diseases are combined; but, in the
majority of cases, the affection of the lungs supervenes on that of
the larynx. Ulcers with tubercular bases are very frequent about the
ventricles of the larynx in subjects dead of pulmonary phthisis. The
chordæ vocales are thus often exposed. The affection of the lungs is
perhaps attributable to frequent and harassing cough, occasioned by the
state of the larynx and ejection of profuse vitiated secretions.
361
When the ulceration extends deeply, portions of the cartilages
sometimes become diseased; the soft parts surrounding them are
destroyed, they become necrosed, and are expectorated along with
a quantity of highly fetid purulent fluid. In some instances, the
expectorated portions are osseous, of loose texture, irregular margins,
and dark colour, exhaling an odour intolerably fetid. It sometimes
happens that the ulcerations proceed still more deeply, perforating
the parietes of the canal, and establishing a communication betwixt
the windpipe and gullet; or, if the perforation is anteriorly, the
communication is with the cellular tissue on the forepart of the neck,
abscess forms which may attain a large size and be productive of much
inconvenience and danger.
The disease has been frequently produced by mercury, when the abuse of
that mineral was common; its abuse is still far from uncommon.
The symptoms may be mitigated by counter-irritation. The parts
covering the trachea should not be subjected to counter-irritation;
in consequence of repeated blistering, the application of irritating
ointments, effusion and thickening of the cellular tissue is
caused, and this may prove a serious obstacle in the performance of
tracheotomy, should that afterwards, as is too likely, be required.
Setons may be inserted on the sides of the neck, and applications made
over the box of the larynx. But tracheotomy affords the only hope of
permanent relief; and if performed at an early period, if the lungs are
not the seat of tubercular disease, as they too frequently are, there
is every reason to expect that it will prove successful. It is followed
by the beneficial results mentioned when speaking of the preceding
disease, and the nitrate of silver can be applied to the more external
ulcers, along with the internal use of sarsaparilla, &c. Ulcers, which
there is every reason to suppose had been both extensive and deep,
have healed even after the discharge of portions of dead, sometimes
ossified, cartilage. The symptoms abate; the patient recovers, though
in general with imperfect voice, as might be expected.
It may even be practicable to employ topical applications to the ulcers
within the cavity of the larynx, as in the following case, which,
though unsuccessful, shows the advantages to be expected from similar
procedure adopted at a more early period. T. C., aged 22, had laboured
under the symptoms of phthisis laryngea for five months previous to his
application. He was much emaciated, and experienced great difficulty in
swallowing, on account of the irritation induced in the region of the
glottis; he had occasional cough, purulent sputa, and aphonia almost
complete. The larynx was painful when pressed, the epiglottis was seen
to be œdematous, and the general symptoms were of a hectic character.
The œdema of the epiglottis was reduced by scarification.
The symptoms increased, notwithstanding counter-irritation and tonic
remedies. The stethoscopic indications regarding the chest were so far
favourable.
Tracheotomy was performed, and the patient felt very much relieved in
consequence. On the tenth day after the operation, the inner surface
of the larynx was touched with a strong solution of362 the nitrate of
silver, applied by means of a bit of lint wrapped round the end of
a probe slightly bent, and introduced upwards from the wound. The
solution was applied every second or third day, and under its use the
patient was remarkably benefited. He swallowed, spoke, slept, and
looked better; the purulent sputa diminished, and the cough abated.
He complained of less pain in the larynx, and seemed to be regaining
strength, though slowly.
But after the lapse of several weeks, from imprudent exposure to
cold, evident symptoms of bronchitis supervened, under which his
constitution already shattered, speedily sank. The larynx was found
extensively ulcerated, but at a number of points there were distinct
marks of recent cicatrisation. The state of the lungs clearly showed
that phthisis pulmonalis had not only commenced, but made considerable
progress. The practice here detailed has been repeated again and again
with good success.
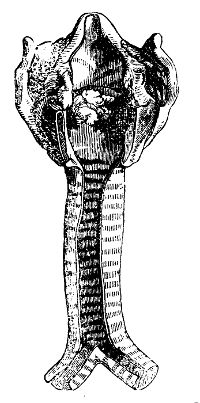 Dyspnœa is caused by other circumstances besides those already
mentioned; some rare cases are met with in which warty excrescences
have grown from the seat of the vocal chords: a beautiful specimen from
the collections of my friends, Messrs. Grainger and Pilcher, is here
delineated. Dyspnœa frequently arises from paralysis of the muscles of
the larynx, in consequence of effusion at the base of the brain, from
long-continued irritation, as from an irritating cause seated in the
mouth, and in old people from a general decay of the animal powers. In
the last case, it is generally a symptom of approaching dissolution, as
is the dysphagia which often attends it.
Dyspnœa is caused by other circumstances besides those already
mentioned; some rare cases are met with in which warty excrescences
have grown from the seat of the vocal chords: a beautiful specimen from
the collections of my friends, Messrs. Grainger and Pilcher, is here
delineated. Dyspnœa frequently arises from paralysis of the muscles of
the larynx, in consequence of effusion at the base of the brain, from
long-continued irritation, as from an irritating cause seated in the
mouth, and in old people from a general decay of the animal powers. In
the last case, it is generally a symptom of approaching dissolution, as
is the dysphagia which often attends it.
Severe dyspnœa is sometimes caused by external violence. A fine
healthy child, aged eight, in running across the street, fell, and
struck the larynx with great force upon a large stone. She was taken
up quite lifeless, and some time elapsed before respiration was at all
established. A gentleman finding her face livid, opened the temporal
artery, and applied leeches to the throat, with some relief. I saw her
about three hours after the accident. The breathing, inspiration more
particularly, was exceedingly difficult; and this appeared to proceed
not only from the injury to the larynx, probably occasioning loss of
power in the muscles, but from the collection of some fluid in the
trachea and its ramifications. The child was evidently in such a state
that, unless active measures were resorted to, and that speedily, a
fatal termination would soon take place. Tracheotomy was performed; a
quantity of coagulated blood and bloody mucus was evacuated from the
opening; and when the discharge and coughing had ceased, a tube was
introduced. In eight days the tube was withdrawn, the aperture closed;
and no unfavourable symptom recurred. In the museum at Chatham is a
larynx showing fracture of the thy363roid cartilage from the kick of a
horse. The immediate consequence was great difficulty of breathing and
rapid general emphysema. The patient, a young soldier, died soon after
the injury.
Large or irregular foreign bodies, as coins, pebbles, portions of
stone or of coal, seeds of fruit, &c., put heedlessly into the mouth,
are apt to become impacted in the rima glottidis, and give rise to
severe and dangerous dyspnœa, or even cause sudden dissolution. Smaller
and smooth substances pass through into the trachea. Such accidents
happen most frequently to children. Peas, beans, small shells, &c.,
slip into the air-passage, are obstructed for a short time in the rima,
but are soon forced by the convulsive actions of the patient into the
trachea, and frequently lodge in the right bronchus, it being more
capacious, and more a continuation of the trachea than the left; or
they remain loose in the trachea, and are moved up and down by the
passage of the air. Immediately on their introduction, most violent
coughing takes place, respiration is convulsive and imperfect, the
patient writhes in agony, and is in dread of instant suffocation;
the countenance becomes inflated and livid, and most strenuous
efforts are made by nature to expel the foreign body. At length he
is exhausted, and an interval of perfect quiet ensues; but this is
soon interrupted by renewed attempts at expulsion. After a time, the
intervals of repose increase in duration, and in many cases are so
long continued, as to lull the patient and his friends into a belief
that the windpipe contains no extraneous substance. But still violent
fits of coughing supervene from time to time, and the dyspnœa is very
alarming; on attentive examination, the presence of this foreign body
may be ascertained beyond doubt by the peculiar noise produced by its
movements in the passage; at the same time, thin mucus is copiously
discharged from the lining membrane. Occasionally the foreign body
becomes so placed in the canal as to form a complete valve, and then
the labours of the patient to dislodge it are most painfully severe;
if they fail, he is suffocated. During laborious breathing the neck
sometimes becomes emphysematous. The parts may at length get accustomed
to the presence of the foreign body, and all uneasiness subside. But
danger, though not immediate, still remains. Foreign bodies have
remained for years without causing much inconvenience; but in such
cases they have generally settled in some remote ramification of the
bronchial tubes; abscess commonly, sooner or later, takes place around,
purulent expectoration follows, all the symptoms of pulmonary phthisis
are established, the patient becomes hectic, and dies.
The existence of the foreign body, when suspected, is to be ascertained
by accurate and attentive examination along the forepart of the neck,
and by listening carefully to the sounds which may be present in the
trachea; but the urgency and continuance of the symptoms will seldom
leave the surgeon to entertain a doubt. If he attentively watch the
patient, he can scarcely be mistaken. It has been recommended to
examine the œsophagus previously to adopting active measures, a large
foreign body impacted in that passage364 being capable of materially
obstructing respiration by compression of the trachea; and it is
safe and prudent to follow this recommendation whenever the least
uncertainty exists regarding the real nature of the case.
When a foreign body has lodged in the windpipe, tracheotomy should be
had recourse to without delay. In general, the offending substance
presents itself immediately after the division of the trachea, and
is expelled by a strong current of air. But in some cases it may
be necessary to introduce instruments—probes, scoops, or small
forceps—upwards or downwards, to dislodge and extract the body. A case
in which a foreign body, which had lodged in the right bronchus for
about six months, was successfully extracted, is detailed fully in the
Lancet, and noticed shortly in the Practical Surgery, p. 416. A
little blood from the wound may cause coughing for some minutes, but
this soon ceases; the wound is closed after a few hours, respiration is
completely reëstablished, and all that the surgeon has then to combat
are the evil effects on the mucous membrane which the contact of a
foreign body may have occasioned.
Tracheotomy is, in nearly all cases, preferable to laryngotomy. In
disease of the windpipe, as formerly stated, it is better to cut into
a sound part of the passage, or at least as far as possible from the
seat of the disease. When an adult, for example, labours under acute
laryngitis, the effused lymph is generally confined to the larynx, as
was already mentioned; an opening below the thyroid gland is removed
from the effusion, and by means of it the patient breathes through
the natural tube yet sound; whereas, if the opening is made in the
crico-thyroid membrane, the surgeon frequently cuts into the middle of
the diseased part; little or no benefit follows, and, if the danger
is not increased, equivocal good is all that can be expected from
such an operation. Tracheotomy is also preferable for the removal of
foreign bodies, unless it is certain that the body is impacted in the
rima, for in such circumstances laryngotomy is much more suitable. In
tracheotomy, the incision of the tracheal rings can be extended with
much less injury than can division of the laryngeal cartilages, when
the largeness of the foreign body, its being firmly fixed, or other
circumstances, require that the wound be of considerable size. The
risk or danger in the one operation is not much greater than in the
other. Division of the crico-thyroid membrane and skin is effected
by one incision; there is nothing important in the way of the knife.
In very young children, when suffocation is threatened, as from the
effects following upon the attempt to swallow very hot fluids, and
the inhalation of steam, this operation may with great propriety be
performed. Tracheotomy, on the contrary, requires to be proceeded in
more carefully, particularly in children, in whom the neck is short,
and the trachea deep. The tube is moreover very small, and not easily
steadied. I had occasion, not long since, to open the passage in a
child under sixteen months old, who had tried to swallow the contents
of a teapot recently filled with boiling water. The difficulty
experienced in such cases is often very great.365 Obstacles may also be
presented by the thyroid and other veins being distended, and the soft
parts are perhaps tumid and infiltrated with serum.
The patient, if adult, should be seated with the trunk erect, and by
throwing back the head, space in the neck is gained. In a female on
whom I operated some years since, this advantage could not be obtained
on account of induration in the belly of the sterno-mastoid muscle,
with contraction. The incision of the integument is commenced in the
mesial line over the cricoid cartilage, and carried downwards, an inch
in the adult, but proportionally shorter in children. The cellular
tissue is divided by a few touches with the point of the instrument (a
small scalpel or bistoury); the finger is then introduced to separate
the sterno-hyoid muscles, and to feel for any stray vessels which may
be in the way; for the thyroid arteries sometimes cross the line of
incision, and it may happen that some of the larger arteries of the
neck, by following an unusual course, become liable to injury, if the
operation were rashly performed. The plexus of veins on the forepart of
the neck is pushed downwards, and the isthmus of the thyroid gland, if
it exist, is displaced slightly upwards; thus the rings of the trachea
are cleared. The patient is desired to swallow his saliva, in order
to elongate and stretch the windpipe; and the surgeon, seizing the
favourable opportunity, pushes the point of the knife, with its back
towards the top of the sternum, into the tube at the lower part of the
incision. The instrument is carried steadily upwards, so as to divide
three or four rings. It is not at all necessary to cut out any part of
the rings of the trachea as recommended by some writers; contraction of
the tube may afterwards result; nor can any good purpose be served by
making the opening crucial.
If the operation has been undertaken for the removal of a foreign body,
its object is usually accomplished immediately on division of the
rings; if not, the substance must be dislodged by proper instruments,
as was previously remarked. The opening is allowed to close after
the oozing of blood has entirely ceased; but its edges must be kept
asunder till then, lest the blood be drawn into the bronchial tubes,
which occurrence, however slowly it take place, is always dangerous.
The union and cicatrisation of such longitudinal wounds are soon
accomplished; they close permanently in a few days, even after having
been open for many weeks with a foreign substance interposed between
their edges. The same obstacles do not interfere as in transverse
wounds; on the contrary, every circumstance is in favour of rapid union.
When the object of the operation is to relieve respiration, impeded by
disease in the superior part of the canal, a silver tube, of convenient
curve, length, and calibre, is introduced into the wound immediately
on the knife being withdrawn, and secured by tapes attached to the
rings at the orifice of the tube, and tied round the neck. Frequently
a violent fit of coughing, alarming to the patient, follows the
introduction, in consequence of some blood having entered the trachea.
But on the ejection of some frothy mucus, mixed with blood, the patient
becomes quiet and tranquil, breathes easily, and feels composed and
relieved. The form of the tube—the calibre366 gradually increasing from
below towards the orifice—completely prevents any farther ingress
of blood, by the uniform compression which it makes on the edges of
the wound. The secretion of mucus in the trachea is increased by the
presence of the foreign body, but the patient easily frees himself from
its annoyance, being instructed to place his finger on the orifice of
the tube, so as to narrow the aperture, when he wishes to cough and
expectorate. In those cases where the operation has been performed
without there being diminution of calibre of upper part by swelling or
otherwise, expectoration through the tube is more difficult. Mucus,
however, is apt to adhere to the inner surface of the tube, and thereby
obstruct breathing; to prevent this, it is necessary occasionally to
introduce a feather, or a probe wrapped round with lint, for some
hours after the operation; the attendance of an assistant may be
necessary for this purpose, but the patient readily undertakes the
duty himself, on being made aware of its necessity. A double tube has
been recommended, to facilitate the keeping of the passage clear, the
inner one being occasionally withdrawn, cleaned, and replaced. But
this is not in ordinary cases necessary. The frequent introduction of
a feather, or probe, is sufficient for some hours after the operation,
and in a very short time the patient finds that he breathes freely,
though the tube is removed for a few minutes, in order to be cleaned.
At first, a funnel-shaped tube is used, to compress the edges of the
wound and prevent oozing, as already mentioned; afterwards, one of
uniform calibre is more easily coughed through. The patient should be
kept in an atmosphere of warm and equal temperature, and it is also
prudent to place some cloth of very loose texture over the tube, that
the temperature of the respired air may resemble as much as possible
that passing through the whole track of the windpipe; thus bronchitis
may be averted.
In some cases, the necessity for continuing the tube speedily goes
off, the larynx, in consequence of rest, having recovered its healthy
state and action. After eight or ten days, on taking out the tube, and
closing the aperture in the trachea, the patient breathes and speaks
well, and continues to do so.
In other instances, the difficult breathing recurs soon after
withdrawal of the tube, the morbid state of the laryngeal mucous
membrane having not been wholly removed. In such circumstances, the
tube must be replaced and continued, but a smaller one suffices, less
mucus is secreted, and a considerable quantity of air passes through
the larynx; in short, the patient requires merely a small tube to
obviate the danger which might arise from complete closure of the
artificial opening, and to compensate for the narrowness of the natural
canal. He speaks tolerably well, on placing his finger over the orifice
of the tube. In course of time, the larynx may recover, and the tube be
no longer necessary.
In some cases, a tube of a certain size must be worn during the
remainder of life; and it does not generally cause much inconvenience.
Attempts to discontinue its use give rise to dreadful suffering; the
difficult breathing, threatened suffocation, and horrible feelings
during the night, all recur. The box of the larynx has fallen in, as367
it were, in consequence of having been long disused, and is unable
to resume its functions to their full extent. Besides, great, though
gradual, change of structure has in all probability taken place. In
several such cases, I have attempted to restore the natural dimensions
of the passage, by the occasional introduction of bougies, gradually
increased in size; but in none have I completely succeeded, except in
the case of attempted suicide which has been already detailed shortly.
In all, my attempts were at first followed by encouraging amelioration,
but untoward symptoms occurring forced me to abandon them, though
repeatedly persevered in. In one man, I succeeded in restoring natural
respiration and closing the opening in the neck, but this was not
of long continuance; a fresh accession of difficult breathing made
renewal of the artificial opening absolutely necessary within a few
months. Still the results are not such as to forbid further trials;
and at any rate, it is now well understood that much greater freedom
may be safely used with the air-tube than was formerly imagined; yet
it must be acknowledged that little benefit can be expected to follow
such, or any treatment, in many cases of contraction of the canal,
from long-continued disease. The larynx and trachea obtained from the
patient whose case is alluded to above are here represented. The poor
fellow had worn a small silver tube in an opening in his windpipe for
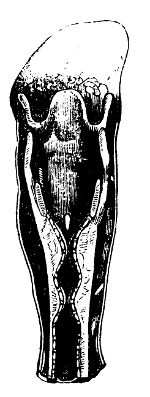 many years. It was originally introduced on account of long-continued
disease of the larynx, with dreadful suffering and constant sense of
impending suffocation. He could not be made to dispense with the tube
entirely, as he felt immediately on the wound closing a threatening
of return of his painful and dangerous symptoms. A small one was
substituted for that at first used. He led a very irregular life, used
a vast quantity of opium, and no small amount of spirituous liquors.
He used to be out in the open air occasionally all night, and suffered
repeatedly under attacks of bronchitis. He was under treatment again
and again in the hospital, on account of rheumatic affection and
deranged digestive organs. He used occasionally to present himself,
complaining of difficult breathing, and stating that his silver tube
was too short. He could articulate tolerably well when he stopped with
his finger the orifice of the silver tube; at all times a part of the
respired air passing through the natural channel. Latterly, he used to
suffer from threatening of suffocation, and he used to relieve himself
of the cause of this, viz., the inspissated and ropy mucus which got
entangled in the trachea, then not suspected to be in a diseased state,
by pushing through the opening in his neck and into the bronchi, long
turkey’s feathers; of these he carried a good store, and some are now
in my possession. This feat he performed without causing the slightest
excitement or coughing. Ultimately, and about twelve years after the
operation had been performed, he died, principally from diseased
viscera. His liver was enormously enlarged368 and altered in structure;
the larynx is seen to be very much contracted at two points. The tube
is observed to be considerably dilated below the contractions.
many years. It was originally introduced on account of long-continued
disease of the larynx, with dreadful suffering and constant sense of
impending suffocation. He could not be made to dispense with the tube
entirely, as he felt immediately on the wound closing a threatening
of return of his painful and dangerous symptoms. A small one was
substituted for that at first used. He led a very irregular life, used
a vast quantity of opium, and no small amount of spirituous liquors.
He used to be out in the open air occasionally all night, and suffered
repeatedly under attacks of bronchitis. He was under treatment again
and again in the hospital, on account of rheumatic affection and
deranged digestive organs. He used occasionally to present himself,
complaining of difficult breathing, and stating that his silver tube
was too short. He could articulate tolerably well when he stopped with
his finger the orifice of the silver tube; at all times a part of the
respired air passing through the natural channel. Latterly, he used to
suffer from threatening of suffocation, and he used to relieve himself
of the cause of this, viz., the inspissated and ropy mucus which got
entangled in the trachea, then not suspected to be in a diseased state,
by pushing through the opening in his neck and into the bronchi, long
turkey’s feathers; of these he carried a good store, and some are now
in my possession. This feat he performed without causing the slightest
excitement or coughing. Ultimately, and about twelve years after the
operation had been performed, he died, principally from diseased
viscera. His liver was enormously enlarged368 and altered in structure;
the larynx is seen to be very much contracted at two points. The tube
is observed to be considerably dilated below the contractions.
The introduction of tubes into the larynx has been supposed likely
to supersede bronchotomy in some cases; and it is said that their
presence does not produce so much irritation as has been stated. But
the practice must, in all cases, be most troublesome to the surgeon,
and painful to the patient; and, in my opinion, continuance of it is in
the great majority of cases impracticable. Besides, it is difficult,
and not unattended with danger. Bronchotomy is quite safe, and not
likely to be followed by such suffering to the patient, or by any other
unpleasant consequence, to which the other method is liable.
Pharyngitis.—Inflammation of the pharynx is of rare occurrence.
The inflammation may extend from neighbouring parts, or be produced
by the direct application of an irritating or stimulating cause, as
the lodgement of foreign bodies, of pins, fish-bones, seeds, portions
of hard food; or by the application of acrid fluids to the membrane,
acids, hot water, &c. In one instance which I met with, it occurred
in a very violent form, in consequence of a large and sharp portion
of an earthenware plate having been swallowed so far by the patient
whilst eating his porridge, and becoming firmly impacted in the lower
part of the pharynx. I have seen a considerable number of instances
in which the disease was produced by the swallowing of soap lees, a
fluid, it would appear, highly acrid, occasioning a severe degree of
inflammation, and even destroying a portion of the parietes.
A man employed by the police in fumigating houses during the prevalence
of cholera, had given to him as a practical joke a glass of sulphuric
acid instead of whiskey. He suffered at the time, as may be supposed,
most excruciating pain, violent inflammation supervened, followed by a
bad stricture of the gullet.
Deglutition is difficult and painful; an exquisite degree of pain is
occasioned by pressure on the sides of the neck, and the circulation is
more or less excited. Redness and swelling of a portion of the mucous
membrane can be observed on looking into the fauces. The changes which
occur in the membrane are similar to those produced in the windpipe by
inflammation.
Resolution will generally be effected by the application of leeches to
the neck, the exhibition of purgatives and diaphoretics, and strict
observance of the antiphlogistic regimen.
If the inflammation does not soon subside, it sometimes happens
that constriction of the passage occurs, either from thickening or
œdematous swelling of a portion of the mucous membrane, or from
effusion of lymph, and adhesion of the opposed surfaces. The common
seat of stricture, as in other mucous canals, is that portion of the
tube which is naturally the narrowest, the lower part of the pharynx
and commencement of the œsophagus, immediately behind the cricoid
cartilage: occasionally it takes place in other parts of the canal. In
general, the contraction is of small extent, and unaccompanied with369
much thickening around. The tube immediately above the constricted
point is more or less dilated, and often to so enormous a size as
almost to resemble a first stomach. In the majority of cases, the
parietes of this pouch are attenuated; but occasionally they are much
thickened, and the seat of a purulent collection, which subsequently
opens into the general cavity. In cases of long standing, ulceration
often occurs, usually limited to the neighbourhood of the stricture.
When the parts immediately below the stricture are ulcerated, the
circumstances is often attributed to the retching which generally
attends the disease; but it appears to be the result of morbid action,
seated in the parts themselves, similar to the ulcerative process in
the larynx following inflammatory affection. But ulceration occurs
as frequently above the stricture as below it; and, besides the
natural cause to which it is referable, is often produced, or at
least aggravated, by injudicious or unskilful attempts to remove the
constriction. Though the ulcers seldom enlarge to any great extent,
yet, in some rare cases, a portion of the parietes of the canal is
perforated, and a communication thus established with the trachea, or
with the cellular substance amongst the muscles of the neck. Or the
ulcers, from either long continuance, or inherent disposition, may
assume a malignant action, extend rapidly in both width and depth,
throw out fungous and unhealthy granulations, form sinuous false
passages, and produce a most horrible and intractable disease. But
strictures are often of temporary duration, and appear to depend on
spasmodic contraction of the circular muscular fibres of the tube. And
dysphagia may also arise from an opposite condition of the fibres—from
paralysis, in consequence of cerebral affection, a fatal symptom in any
disease.
The prominent symptom of stricture of the œsophagus is difficult
deglutition. Some patients can swallow only liquids; and when an
attempt is made to get over any solid substance, this is stopped at
the contraction, and completely obstructs the passage. In such cases
patients will frequently apply for relief, in order that the portion
of food may be pushed through the narrow portion of the canal; with
the accomplishment of this many are quite satisfied, and are unwilling
to submit to farther treatment, obstruction to solid matter being the
only inconvenience experienced. But when contraction is great, and
the involved portion of the canal almost obliterated, little food of
any kind can pass into the stomach, the patient becomes feeble and
emaciated, and ultimately dies from inanition. The subjects of this
affection are generally far advanced in years, and in them it often
occurs without any evident cause.
If pharyngitis have subsided, either spontaneously or after
antiphlogistic treatment, and symptoms of stricture supervene, the
existence or non-existence of this latter disease must be ascertained
by gentle and cautious introduction of a gum-elastic bougie or
ivory-ball probe. If stricture exist, the descent of the instrument
will be resisted at the contracted point, and most frequently at the
lower part of the pharynx: this, in the adult, will be at a distance
of about nine inches from the incisor teeth. When the seat of the
stricture is ascertained, a bougie is to be introduced, sufficiently
small to pass370 through it; and when this has been pushed beyond,
the disease, if unattended with malignant disposition or action, is
completely in the power of the surgeon. After sufficient time has been
allowed for the irritation following the first introduction to subside,
a larger bougie is to be passed, and retained as long as its presence
can be endured. This practice must be continued, till, by gradual
increase of the bougie, the canal is dilated so as to admit readily an
instrument sufficient to distend the gullet in its healthy state. Thus
the passage will be gently and gradually dilated, till it regain its
original calibre. The process is partly mechanical, but also greatly
dependent on vital action; by the presence of the bougie the parts are
stimulated, the fluid, which may be effused beneath the mucous membrane
or into its substance, is absorbed, and the new solid matter is also
gradually removed by increased action of the absorbents. But if the
bougie be rudely and forcibly introduced, or too long retained, the
absorbent action from being salutary becomes morbid, and ulceration is
established, which may proceed to destroy the parietes of the canal,
so producing an additional and equally formidable disease; or if the
ulcerative action subside, the parts will cicatrise and consequently
 contract, so giving rise to a new stricture, and narrowing the canal
to an equal or greater extent than formerly. Before introducing the
bougie, the head must be thrown as far back as possible, as here
seen, and brought to a horizontal position, that the natural curve of
the upper part of the canal may be lessened, and the passage of the
instrument thus facilitated. It is of consequence also to keep the
point of the bougie pushed back towards the vertebræ (the patient being
desired to make an effort to swallow), and to grasp the larynx with the
left hand and pull it gently forwards, that there may be no risk of
the instrument passing into the windpipe, instead of into the gullet;
if such a mistake should happen, the surgeon will soon be apprised
of it by the violent and convulsive coughing which is generally
induced, though not always. Bougies armed with caustic have been
recommended, but are unnecessary, the simple bougie being sufficient
to remove the disease, if skilfully employed; besides, their use is
not unattended with danger, ulceration being frequently produced. In
very bad cases, in which the stricture is long in yielding to the means
already mentioned, and the nutriment which the patient is able to
swallow is necessarily small,—when the canal is altogether obliterated
either at one point or to a considerable extent, as has sometimes
happened, and when there is consequently little hope of success from
any treatment—the strength of the patient may be supported, and life
prolonged for some time by the use of nutritive enemata.
contract, so giving rise to a new stricture, and narrowing the canal
to an equal or greater extent than formerly. Before introducing the
bougie, the head must be thrown as far back as possible, as here
seen, and brought to a horizontal position, that the natural curve of
the upper part of the canal may be lessened, and the passage of the
instrument thus facilitated. It is of consequence also to keep the
point of the bougie pushed back towards the vertebræ (the patient being
desired to make an effort to swallow), and to grasp the larynx with the
left hand and pull it gently forwards, that there may be no risk of
the instrument passing into the windpipe, instead of into the gullet;
if such a mistake should happen, the surgeon will soon be apprised
of it by the violent and convulsive coughing which is generally
induced, though not always. Bougies armed with caustic have been
recommended, but are unnecessary, the simple bougie being sufficient
to remove the disease, if skilfully employed; besides, their use is
not unattended with danger, ulceration being frequently produced. In
very bad cases, in which the stricture is long in yielding to the means
already mentioned, and the nutriment which the patient is able to
swallow is necessarily small,—when the canal is altogether obliterated
either at one point or to a considerable extent, as has sometimes
happened, and when there is consequently little hope of success from
any treatment—the strength of the patient may be supported, and life
prolonged for some time by the use of nutritive enemata.
Dysphagia may also be caused by tumours in the œsophagus; but371 as these
are generally of a medullary structure, and consequently endowed with
malignant action, the treatment can only be palliative—there is no hope
of a radical cure.
Dysphagia may arise from an aneurismal tumour of the arch of the
aorta, or of the large arterial trunks passing off from it, pressing
on the œsophagus, and so narrowing its calibre. In such cases, also,
no hope of success from any treatment can be entertained; often the
case terminates fatally in a very sudden manner, in consequence of
the aneurismal tumour giving way at the point which protrudes on the
gullet; the contents are discharged into the stomach, or ejected by the
mouth. If treatment by bougies be attempted in dysphagia arising from
such a cause, the practitioner not being aware of the nature of the
disease, the fatal issue will be fearfully hastened—a very unpleasant
consequence of any practice.
Foreign bodies lodged in the œsophagus produce difficult deglutition,
and, if large, may obstruct the passage completely; much irritation
is also caused to the parts with which they are in contact, and
inflammatory action kindled in them. A large substance firmly impacted
likewise creates difficulty of breathing, by compressing the posterior
part of the trachea. Indeed every consequence is of such an annoying
nature, as to render dislodgement and removal of the offending
substance necessary, though there were no apprehension of danger
from its long-continued presence. The proceedings must be varied
according to the consistence, form, size, and situation of the foreign
body. There are a great many instruments for effecting dislodgement
and extraction, but the great majority of them are more curious and
ingenious than applicable to the purpose intended; few are of any
use. A probang, mounted with a bit of sponge, or with an ivory-ball—a
blunt flat hook attached to a whalebone probe—and long curved forceps,
constitute the whole useful apparatus. The feelings of the patient are
generally sufficient to mark the position which the body occupies; he
is made to throw the parts into action, by attempts to swallow the
saliva, and during the attempt to point to the seat of pain. But by
this both patient and surgeon may be deceived, for pain and a feeling
of foreign matter being lodged often remain at a fixed point, after the
body has passed down; similar deception occurs in other situations, as
in regard to extraneous substances in the eye, urethra, &c.
Small and sharp substances seldom remain long in the œsophagus, but
readily descend into the stomach and intestines; they then either
escape along with the feces, or, as sometimes happens, penetrate the
parietes of the alimentary canal, generally near its termination. On
leaving the stomach or the intestines, by gradual perforation, they
frequently travel great distances in the trunk or limbs, without
causing much inconvenience,—effusion of lymph surrounding them, and
filling up their track. They will appear, long after their insertion,
at a far distant point, approach the surface, and gradually make their
way through the integument, or be readily extracted. When they enter
from the surface, also, they often come within reach long afterwards,
and far from their point of entrance.372 Needles, thus travelling, become
oxidised. They are easily removed, on coming near the surface, by
fixing them with the fingers, and making a small incision over the more
superficial extremity. A needle may sometimes be taken out, by making
pressure on both ends, and so forcing the point through the integument.
Small pointed bodies, needles, pins, fish-bones, &c., often get
entangled in the root of the tongue or in the folds of the palate; on
opening the mouth they can be seen, and are easily brought away. If
lodged in the pharynx, they can be reached by the finger. The patient
is seated with the head thrown back, and the jaws extended; the finger
is introduced with determination, regardless of attempts to vomit, and
swiftly passed into all the sinuosities by the side of the epiglottis,
into the pouches betwixt the os hyoides and cornua of the thyroid
cartilage, so that no part is left unsearched. The substance, when
felt, may be extracted with the finger by entangling it in the point of
the nail; or curved forceps may be introduced, and applied conveniently
to the body by the guidance of the finger. Great care and caution is
required in dislodging the foreign body, when both ends, as is often
the case, have penetrated the parietes; if it be rudely grasped and
pulled, the parts are lacerated; or it breaks, and the surgeon, after
bringing out the portion held in the forceps, may find great difficulty
in detecting and disentangling the other. I have often found it very
troublesome to remove delicate needles entire. When they are beyond
the reach of the finger, it is of no use to attempt their removal; the
patient suffers great pain during the endeavour, and there is no chance
of successful issue; besides, the surgeon is apt to bring discredit on
himself.
Coins may be removed by the forceps, or by the hook, if lodged at the
narrow part of the passage behind the cricoid cartilage; if lower,
they generally defy attempts at extraction, and slip into the stomach
gradually. Halfpennies, halfcrowns, &c., pass readily along the
alimentary canal, and are voided in a short time.
Tendinous or cartilaginous portions of hard meat, when within reach
of the finger, can be laid hold of by the curved forceps, and pulled
up. Smaller and soft portions, if impeded in the passage, as when it
has been narrowed by previous disease, are dislodged and pushed down
by the cautious use of a small probang or œsophagus bougie. In the
introduction of any instrument, attention should always be paid to the
steps advised when treating of stricture of the gullet.
Œsophagotomy is an operation that may, under some peculiar
circumstances, be required. When a foreign body is of such a nature
that, when once lodged in the gullet, it cannot be removed either
upwards or downwards, without serious læsion of the parts, and, when
breathing is impeded by its projection, incision of the œsophagus may
be warrantable. The operation is easily accomplished. An incision of
about three inches is made in the superior triangular space of the
neck, on the left side,—the gullet usually inclining to the left of the
mesial line. It is commenced opposite to the os hyoides, and carried
downwards parallel with the trachea; the use of the373 knife is continued
till by cautious dissection the wound is brought to the level of the
common sheath of the large vessels. Assistants separate the edges by
thin and broad copper spatulæ, and the cavity is frequently sponged.
The larynx is pulled aside, and turned a little over on its axis; the
pharynx is thus exposed. During the latter part of the dissection, the
laryngeal nerves and thyroid arteries must be looked for and avoided.
The foreign body is felt through the parietes, and these are laid
open to an extent sufficient for its extraction. It is advisable to
nourish the patient for some days afterwards through an elastic tube
passed by the mouth or nares into the gullet, with its extremity one
or two inches beyond the wound. Its introduction requires caution;
an instance is on record of a tube being passed with the view of
conveying nourishment, in which the surgeon did not discover that its
extremity had slipped into the larynx till after the injection of some
fluid. It is recommended to wait for some minutes before proceeding to
inject, and that, if during that time no air pass through the tube, the
instrument may be considered certainly in the œsophagus. It is seldom
that the opening of the œsophagus will close by the first intention,
and therefore accurate approximation of the external wound need not be
attempted.
Removal of noxious matter from the stomach is now successfully
practised by the aid of instruments. This is required when the
excitability of the organ has been impaired or destroyed, and emetics
in consequence do not act.
It is unnecessary here to treat of the emetics which act most quickly,
or which are most proper in different cases, nor of antidotes for
various poisons. Many stomach-pumps have been contrived, and their
merits have caused much rivalry; but they are all constructed on much
the same principle. People, too, seem to indulge the inventors by
swallowing deleterious substances much more frequently than before.
There has been a demand for cases of poisoning, and the supply has kept
pace pretty well with the demand. Now-a-days twenty seem to attempt
suicide by poison for one that did so long ago.
Most vegetable narcotics—those which do not act with great rapidity,
can be removed mechanically; but some of the mineral poisons are heavy
and difficult of solution, and are not so readily extracted. Read’s
apparatus appears to me the simplest and the best, for this and various
other purposes. Ample directions for its use are given along with the
instrument.
Inflammation and Abscess of the Ear are either deep-seated, or
confined to the external meatus. Suppurations in the internal parts—in
the cavity of the tympanum, or in the mastoid cells—are often attended
with the most violent symptoms, excruciating pain, fever, delirium.
Such are highly dangerous in their consequences. Collections nearer
the surface, under the membrane lining the meatus, are, though not so
dangerous, also attended with great suffering and severe constitutional
symptoms. The disease may occur at all ages,374 but is most common
in children during dentition; in them it is often accompanied with
convulsions and head symptoms, leading to a suspicion of hydrocephalus
being established. The symptoms are all much relieved on the occurrence
of copious purulent discharge.
Suppuration in the organ of hearing often follows eruptive diseases;
and both ears, or one, may continue to discharge for a long time. There
is always more or less derangement of the functions of the parts. When
the disease is external, perhaps hearing may not be much affected; but
when, as often happens, the ossicula, nervous expansions, membrane,
parietes, are all destroyed or injured, hearing is lost, or rendered
at least very obtuse. Purulent discharge often continues for the
rest of the patient’s life, at one time scanty, at another profuse,
and preceded or accompanied by inflammatory symptoms. Openings form
over the mastoid process, communicating with the cells; and these are
often connected with abscess betwixt the dura mater and pars petrosa
of the temporal bone. Abscesses, too, of the middle lobe of the
cerebrum, or in the cerebellum, are sometimes evacuated through the
meatus auditorius. In all cases, but in the last more particularly,
the patient suffers extremely on the discharge being suppressed, and
is again relieved on its recurrence. At length, fever and delirium
may supervene, terminating in coma and death; I have dissected many
who have perished in this manner. Or, after long-continued discharge
from the meatus, perhaps with paralysis of one side of the face,
a soft tumour of the dura mater will be found lying over the pars
petrosa, having caused extensive absorption of the bone, and exposed
the semicircular canals, cochlea, tympanum, &c., filled with purulent
matter. Abscess of the tympanum itself discharges long; and large,
flabby, soft granulations fill up the meatus, very different in
appearance from the solid tumours which sometimes occupy that situation.
Ordinary earache—inflammation extending along the meatus externus, and
confined to the lining membrane—will be relieved by leeching behind
the auricle, and by assiduous and regular fomentation afterwards.
But suppuration is seldom prevented. The abscess may sometimes be
opened, with great relief. If deeply seated, the parts are soothed by
fomentation and poultice, till spontaneous evacuation of the matter
occurs; this is then to be washed away, from time to time, by the
injection of a warm and bland fluid; the abscess gradually closes, and
the discharge slowly disappears. In cases of long-continued discharge,
it is generally impossible to ascertain from what depth the matter
comes, and there is always great risk in using means to arrest its
flow. The patient must submit to the annoyance. The discharge can be
moderated, or altogether suppressed, by injections of astringent salts,
but the practice is unsafe, and in most cases unwarrantable. The parts
are to be kept clean by frequent ablution with tepid water, lime water,
or other bland fluids; and cotton or wool may be worn in the meatus to
take up the discharge, and prevent bad effects from cold. Discharge
from the external meatus, and about the auricle, is often kept up by
irritation in the mouth, in both children and adults; this should be
looked to, and the offending cause removed, if possible.
375
Foreign bodies are frequently lodged by children in the meatus
auditorius externus—peas, beads, shells, shot, pins, &c. By awkward
attempts at removal they are pushed deep into the cavity; and the
membrane of the tympanum is sometimes broken, as indicated by effusion
of blood, and swelling of the parts. Violent inflammatory symptoms
may be caused by such substances, and will be seriously aggravated by
unsuccessful attempts at extraction. Sometimes they are allowed to
remain for days or weeks; in such circumstances seeds swell, separate,
and begin to throw out a germ, thus fixing themselves more firmly in
the passage. They are easily removed at first, by a small silver scoop,
of convenient size and form; and even at a later period, a determined,
though not forcible, attempt with the instrument will be followed with
success. The scoop is gently and gradually insinuated betwixt the
membrane and foreign body; and on its handle being then raised the body
is extruded. It is seldom that any excitement follows extraction by
this method: but if large and powerful instruments be introduced, and
force applied, the parts may sustain severe injury, and troublesome
consequences ensue: indeed such proceedings have proved fatal.
Foreign bodies are also occasionally impacted in the nostrils: the
procedure above described is to be adopted. Sometimes they are
discharged by the posterior nares during attempts at extraction.
Polypus of the meatus auditorius externus is generally of pretty firm
consistence, pyriform, sometimes slightly lobulated and warty-looking;
it adheres by a narrow neck to the parietes of the tube near the margin
of the membrana tympani, is attended with slight discharge, and with
deafness to a greater or less extent.
Extraction is the only means of cure. The body of the tumour is
depressed and pulled outwards by the flat end of a probe slightly
bent; delicate forceps are introduced gently, and passed up to the
neck of the polypus, which is then firmly grasped; by combining slight
twisting with gentle extractive force, it is readily removed. Or a
flat scoop, with a sharp round edge, is passed along till obstructed,
and by slight rotatory motion of the edge, the neck of the tumour is
divided. After a day or two, a mild escharotic may be applied with
the view of preventing reproduction; a bit of charpie sprinkled with
the oxidum hydrargyri rubrum may be pushed up to where the tumour was
attached, and the application may be repeated several times, one or two
days intervening. Even after this the tumour sometimes returns, again
rendering extraction necessary.
Deafness is attributable to various causes besides those already
mentioned. Accumulation of cerumen in the external meatus is the most
common. The cerumen is often mixed with wool, and other extraneous
substances, which the patient may have been in the habit of introducing
as preservatives from cold, and thus a large and firm plug is formed,
completely blocking the meatus. It is removable by the assiduous
injection of tepid water, the best solvent of cerumen. The whole may
not be brought away at the first sitting; but the injection must be
repeated again and again, till the membrane of the376 tympanum is free. A
powerful syringe is required. By the use of a speculum, the condition
of the external tube and membrane of the tympanum can be ascertained.
But it is perhaps unnecessary to enlarge farther here on this subject,
for such is the division of labour in these days, that a distinct
profession is founded on the operation of squirting water into the
external ear; it is true that other operations are talked of by these
Aurists, as they style themselves, but the advantage to be derived from
any of them is often very doubtful. They talk of deafness as arising
from a deficient secretion of cerumen, from dryness, or from eruptions
in the meatus; and heating stimulant applications are poured in—oils,
ointments, mercurial salts, acetic acid, garlic, &c., all combined.
They even go so far as to recommend mercurials to correct the state
of the general health, to improve or rectify the functions of the
chylopoietic viscera, the assistant chylopoietic, and the whole of
the digestive organs, upon derangement of which, say they, many cases
of deafness depend. The fools who apply to such charlatans certainly
deserve to have their pockets well drained, but ought scarcely to be
poisoned by them.
It has been proposed to pass probes and tubes into the eustachian
tubes, to reëstablish their continuity if obliterated, or dilate them
if partially closed. No doubt deafness often depends on obstruction
of this outlet from the tympanum, the requisite reverberation being
perhaps thereby impeded. It may be closed by swelling of the lining
membrane, by inspissated mucus, by destruction of its extremity
from ulceration, by the cicatrisation of ulcers in the immediate
neighbourhood, by congenital deficiency, or by pressure of neighbouring
swellings, or of morbid growths, producing temporary or permanent
obstruction. None but the first two causes could possibly admit of
the use of the probe, and even then it can scarcely be required. By
removal of the cause of such turgescence at the end of the tube,
or in the neighbouring parts,—which can often be detected, being
local,—by counter-irritation, &c., a cure is much more likely to be
effected than by the introduction of probes. Not that the operation is
exceedingly difficult; for, after practice on the dead body, a probe
can readily be passed into the eustachian tube of the living from the
nostril. The instrument is fixed in a handle, with its point slightly
bent, and on the handle there should be a mark to show the direction
of the point; the distance of the termination of the tube from the
nasal orifice ought also to be marked. The instrument is passed along
the floor of the nostril, and then its point is directed upwards and
outwards, whilst the handle is pressed towards the septum narium. It
has been proposed, moreover, to force a stream of cold and condensed
air into the internal ear, and to apply ætherial vapours to the
cavity of the tympanum. The attempts have been made on an extensive
scale in all sorts of cases, and quite indiscriminately. This plan of
curing deafness has been well advertised, and unblushingly puffed in
scientific and other journals. Not one case of deafness in a hundred
probably depends upon any affection of the eustachian tube: vitiated
mucus cannot even be displaced by injection of air or other fluid,
unless the membrane of the tympanum be377 ruptured; this has indeed been
accomplished by the operation in question, and then the mucosity could
only be forced into the cavity of the tympanum, so as, if possible, to
make matters worse.
Nervous deafness, like functional amaurosis, may sometimes be relieved
or even removed entirely by stimulating frictions, or the application
of strychnine to a raw surface behind the auricle, and by attention to
the general health.
Puncture of the Tympanum has been recommended as a remedy for
deafness arising, or supposed to arise, from obstruction of the
eustachian tube; but I believe it has not succeeded in above one out
of twenty cases. The puncture is apt to close very soon; and though
the hearing may be improved for a short time, the advantage gained
soon disappears. The means of keeping the puncture open are not
easily applicable; perhaps the most effectual is to touch the edges
occasionally with pencil-pointed lunar stone. The puncture is generally
made with a short-pointed trocar, such as is used for hydrocele. The
canula is passed down to the membrane, and placed on one side of
its centre, lest the long head of the malleus should be interfered
with. The trocar is then pushed on gently, and should penetrate but a
very short distance, for fear of injuring the important parts at the
bottom of the cavity. By some a sharp-pointed probe is used, passed
through a quill; or an instrument about the same size with the probe
is made for the purpose, with a canula to fit. But these are by much
too small; even the puncture with a trocar closes, notwithstanding
the application of nitrate of silver. I have lately used a sort of
punch, such as is employed for making holes in leather, of a pretty
large size, and neatly made, with the edge very keen, and on a small
stalk. This is introduced; and when obstructed, having reached the
bottom of the canal, an attempt is made, with a rapid turn of the
hand, to cut out a portion of the membrane. I have thus succeeded in
improving immensely the hearing of one gentleman, enabling him to
hear at four or five times the distance he could formerly. He had
repeatedly submitted to punctures before I saw him; and, previously to
the operation with the punch, I passed through the membrane a trocar,
made large, and well-pointed for the purpose; but notwithstanding this,
and the application of the nitrate of silver, I was unable to preserve
the advantage gained longer than a very few days. In suitable cases,
the operation is worthy of trial, being unattended with pain or any
dangerous consequences. M. Fabricci has contrived a very ingenious
little instrument for the purpose; by it the piece of membrane is fixed
by a small screw, before being punched out.
Bronchocele is not rare in some districts of Great Britain, but
unattended with the same peculiarities of countenance and mind as in
some other countries.39 The majority of those affected come from378
mountainous districts. The disease generally commences early in life,
and females are more subject to it than males; indeed almost all who
present themselves are females. The tumours are of various sizes,
involving either the whole gland, or only a part. One lobe is usually
in a state of greater advancement than the other. The swelling is
for the most part soft and yielding, the integuments are thin and
moveable, and large veins shine through them. It is unattended with
pain, or any great inconvenience, though sometimes it equals in size
the patient’s head, or nearly so, and then it is troublesome from bulk
alone. In general, there is little or no obstruction to deglutition
or respiration, and the health is not impaired. The tumour is always
of slow growth, at length becomes stationary, and the patient gets
reconciled to the deformity. Its structure is that of the simplest form
of tumour, a genuine hypertrophy, and it is seldom that its action
degenerates. It is often made up also partly of cysts containing
serosity, or glairy albuminous fluid.
Internal remedies have been prescribed, with the view of arresting
the growth, and promoting absorption of the enlarged thyroid—burnt
sponge—muriate of lime—muriate of baryta, &c. The use of iodine,
externally and internally, has in many cases been attended with
beneficial effects. Tumours have diminished, and even disappeared
entirely, during the employment of this medicine; but in others, the
diminution has been either trifling or none. The insertion of setons
has been strongly recommended; and many patients are said to have been
thus cured. I have tried this plan in one case only; it certainly had
the effect of diminishing the swelling; but for some time great trouble
was experienced from bleeding, whenever the cord was drawn, and the
patient afterwards became much weakened by the profuse discharge. The
proposal to tie the thyroid arteries, for the cure of bronchocele, has
been put in practice, but without a favourable result.40
Extirpation of such growths has been repeatedly attempted; but the
patients, almost without exception, have perished from hemorrhage,
under the hands of the knivesmen. The immense supply of blood afforded
to the gland in the healthy state must be kept in mind, as also the
enlargement of the vessels proportional to the increase of the part.
Not arteries alone, but enormous veins, are to be encountered. The
tumour is in the vicinity of important organs, and of the trunks of
large vessels and nerves, and probably has become attached to them. In
short, the operation is attended with such risks, with so 379absolute
a certainty almost of fatal result, as not to be warranted under any
circumstances, far less for removal of deformity only.
Enlargement of the isthmus alone gives rise to more severe symptoms
apparently, and may warrant an attempt at removal; but this can
scarcely be accomplished altogether by incision. Such is my impression,
and under this impression I proceeded very cautiously in a case of
this nature with which I had to deal.—J. R., a rat-catcher, aged
forty-seven, from the Highlands, was admitted into the Royal Infirmary.
The isthmus of the thyroid gland was enlarged to the size of a goose’s
egg. The tumour was extremely hard and irregular on its surface, but
not painful when touched; it appeared to be adherent to the trachea,
and did not admit of much motion. The voice was considerably impaired,
and breathing much impeded, inspiration being difficult and attended
with a loud wheezing noise. On making unusual exertion, even though
inconsiderable, the dyspnœa was much increased; and on ascending a
height, or even remaining for some time in a stooping posture, it
amounted almost to suffocation. There was no pain or uneasiness in
the larynx or trachea. The disease was of three years’ duration. A
seton had been introduced, but effected no diminution, and rendered
the tumour more dense and less moveable than formerly. I surrounded
the lower part of the tumour by two semicircular incisions, and,
dissecting cautiously beneath its base, detached it from its more
loose connections, not interfering with the central portion and its
connection to the trachea. During the progress of the dissection, the
blood flowed most profusely from both arteries and veins, but was
restrained by securing the former with a ligature, and compressing
the latter with sponge. An armed needle was then passed through the
centre of the tumour, as close to the trachea as possible, and its
remaining attachment enclosed by the separate portions of the ligature
firmly applied. Everything proceeded favourably. The tumour soon came
away; the wound healed with a firm cicatrix, and in about a month
the patient went home well. I met him by chance, in Aberdeen, twelve
months afterwards, free of complaint, and breathing easily under all
circumstances, his neck presenting no vestige of the tumour.
Glandular Tumours of the Neck, as formerly noticed, arise from
various irritations; and some constitutions are more subject to them
than others. The nature of the enlargement is dependent on the cause;
it may be simple or malignant. Simple swellings often attain a large
size; the lymphatic glands in both spaces of the neck, and on one or
both sides, get immensely enlarged, the cellular tissue around is
infiltrated with solid matter, and all matted together. Great deformity
is produced; the head is turned with difficulty, and twisted to one
side; often there is not much pain. After some time, the swelling
becomes looser than before; its various portions separate, and
gradually disappear; or the centre becomes soft, suppuration spreads
extensively, and the surrounding hardness either goes off, or becomes
partial.
Discussion of the swelling is to be promoted, and, if possible,
the cause removed; and fomentation, friction, pressure, internal
stimu380lants are to be employed, according to the state of the parts,
along with what are called deobstruents, in the first instance. When
suppuration cannot be arrested, the attention must be directed to
prevent the integuments from being destroyed. With this view, the
abscess should not be permitted to give way spontaneously, lest an
opening be formed whose cicatrisation would cause deformity, and leave
a stain on the race and generation. An artificial aperture must be made
early; and in the upper and most exposed parts of the neck this should
be in the direction of the folds, and small.
When many and extensive collections have formed, when the integuments
have been undermined and attenuated before advice is sought, it is
impossible to prevent deformity. The knife and potass are required, for
reasons assigned in the preceding part of this work; and the detached
glands, as well as the thinned skin, stand in need of their free
application.
Deep-seated collections may originate in glandular disease, or commence
in the cellular tissue; they occasionally follow transverse wounds of
the neck. Great infiltration of the cellular tissue supervenes over
the trachea and sternum, and also under the fasciæ; purulent matter
is secreted in the cells, and the parts are extensively separated;
sloughing is prevented only by free and early incision. The nature
and extent of the coverings of an abscess seated deeply in the neck
are to be kept in view—the platysma myoides, the superficial and
deep cervical fasciæ. Collections under these interfere with the
functions of the neighbouring parts, and are attended with great pain,
which is somewhat relieved by resting the chin on the sternum, and
so relaxing the fasciæ. The matter makes its way to the top of the
sternum, and generally points on the outside of the sterno-mastoid
muscles. But before the integuments become thin, the parts have been
seriously injured—the cellular tissue has sloughed, the muscles
have been separated from each other, with unhealthy purulent matter
interposed—the trachea, the œsophagus, or the mediastinum, opened into.
Such cases have been formerly alluded to.
The lymphatic glands, situated amongst the fat and cellular tissue
between the deep and superficial cervical fasciæ immediately above
the sternum, may become enlarged. When the tumour is large, breathing
is impeded by compression of the parts beneath, and pain and much
inconvenience are endured on account of its limited situation and
resisting investments.
Purulent collections in the anterior mediastinum and under the sternum
are scarcely remediable. These are chronic or acute. One of the great
dangers following the operations on the larger vessels at the root
of the neck, in which the deep fascia is necessarily divided, is
infiltration into, and acute abscess of, the anterior mediastinum.
In chronic collections the parietes of the cavity on one side are
fixed, on the other have constant motion; and thus the surfaces,
however healthy and well disposed, are prevented from coming together
and adhering. The discharge continues, and at length wears out the
patient, pulmonary affection perhaps supervening. The same unfavourable
causes operate in other situations, in the iliac fossa, and in chronic
collections under the cranium. In chronic abscess of the me381diastinum,
no dependent opening can be obtained, unless by perforation of the
sternum. This is perhaps warranted by œdematous swelling over some part
of the bone, indicating, along with other symptoms, the existence of
matter beneath. Purulent collections sometimes form in the substance of
the sternum, communicate with the mediastinum, and involve the lower
part of the neck.
The thymus gland is said to be liable to chronic enlargement in
young subjects of weak constitution, causing serious impediment
to respiration and deglutition; the tumour is confined above and
anteriorly, and consequently presses backwards on the trachea and
gullet. Suppuration may take place in the swelling, and the matter
ultimately be diffused in the mediastinum.
[HYDROCELE OF THE NECK.
An encysted tumour of the neck, to which the term HYDROCELE has been
applied by some writers, is met with in both sexes and at various
periods of life. Its progress is usually slow, and it generally
arises without any assignable cause. Occasionally it has appeared
to be congenital, but this must be considered as a rare exception.
The tumour, seldom larger than a walnut, may acquire the volume of
a Seville orange. When this is the case, it may impede respiration
and deglutition, or even the return of the blood from the head. Its
contents are of a serous or oily character, with an intermixture of
flakes of lymph, and the cyst itself varies in thickness from the
fourth of a line to a quarter of an inch or more. Externally it is
more or less intimately connected to the cellular substance in which
it is developed, while its internal surface often exhibits a rough,
reticulated aspect, not unlike the false membrane of pericarditis.
In cases of long standing the cyst is very firm and tough, or almost
gristly, and closely adherent. The skin covering the tumour seldom
undergoes any change, unless it is very large, when it is apt to become
attenuated at some points and thickened at others. The subcutaneous
veins may also then present a tortuous and distended appearance; but
this is far from being generally the case.
The characters by which hydrocele of the neck may be distinguished
from other affections are, absence of pain and tenderness on pressure,
slight fluctuation, the slow progress of the tumour, years generally
elapsing before it attains much development, and, above all, the
history of the case. When the tumour projects outwardly over the
carotid artery, it might be mistaken for aneurism, from which, however,
it may, in general, be readily discriminated by the elevation of the
entire swelling from the impulse of the blood, and by the want of that
alternate expansion and retrocession which are present in genuine
aneurism. When seated over the thyroid gland, or in its substance,
it may be confounded with bronchocele. In all cases, where any doubt
remains as to its true nature, an exploring needle or trocar should be
introduced, which will at once determine the diagnosis.
The treatment of this affection, like that of the vaginal tunic of
the testicle, may be palliative or radical. The former consists in
evacu382ating the fluid, from time to time, with the knife or trocar; the
latter, in injecting some stimulating fluid, such as wine and water,
or a solution of iodine, or nitrate of silver; or, what is better,
introducing a seton, and keeping it in the sac until it is obliterated
by adhesive inflammation. Incision and extirpation have been practised
successfully by Flaubert, Delpech, Jobert, and other surgeons.]
Distortion of the Neck arises from a variety of causes, and is either
temporary or permanent. The head is often kept in an unnatural position
for weeks by glandular swelling. Enlargement of the superficial glands,
at the upper part of the neck, induces the patient to turn his head
to the opposite side; swellings lower in the neck, and deep seated,
require relaxation of the coverings, and the head is consequently
twisted to the same side. Either rigidity, or spasmodic action, or
both, of the sterno-mastoid muscles, displaces the head and twists the
neck. The head is either bent forward, or turned to one side; usually,
the chin is twisted over the shoulder, on the side opposite to the
offending muscle. Induration of the muscle is sometimes met with, also
causing distortion; it may terminate in abscess, or after a long time
be discussed.
The cause of the spasmodic action in the muscle is sometimes apparent,
sometimes very difficult to be detected. Sources of irritation at
the extremities of neighbouring and communicating nerves are to be
looked for and removed; and the spasms are to be moderated, as much
as possible, by external and internal remedies. Opiate frictions, and
the application of the nitrate of silver over the course of suspected
nerves, are sometimes followed with benefit, and may be accompanied
by the internal administration of antispasmodics, though the efficacy
of these is often doubtful. When the head has been for a long period,
perhaps many years, turned to one side, from any cause, the muscle on
that side naturally becomes shortened, and a change takes place in
the form of the bones. If the patient is still young, the deformity
may, in a great measure, if not entirely, be remedied. Division of the
shortened muscle was a favourite operation of old surgeons for the cure
of wry-neck, and may be resorted to with advantage in some cases. One
of the heads, or both, may require to be detached from the sternum and
clavicle. It is only in cases where the muscle is in fault, it being
shorter than usual, that benefit can be expected from this proceeding.
It is a very simple operation, and can be effected by a mere puncture
of the skin betwixt the two portions. By the cautious use of a blunt
and flat probe or director, the cellular tissue under the origins of
the muscle is separated; this is followed by a narrow and blunt-pointed
knife, by which the attachments to the clavicle and sternum are cut
across.
Distortion of the neck is most frequently produced by some vice in
the bones, as curvature, from softening, attended with deformity of
the trunk or of the limbs. In such cases, the twist is generally to
the right side, the ear approaching the shoulder. No treatment can be
effectual, unless the other curvatures are corrected; for the head
is placed so to preserve the equilibrium of the body. The head is to
be supported, and its weight removed from the vertebral column by a
curved iron rod, attached to the back of stays fastened on the383 loins,
leathern straps passing from the top of the rod under the chin and over
the occiput. By the use of such apparatus for a considerable time,
the vertebral column may regain its perpendicular direction, and all
deformity of the neck be consequently removed. The application of such
a machine is required after the division of the sterno-mastoid, so that
the head may be kept straight until the muscle is reunited of a proper
length, and any change in the form of the bones may be got over. In
slight cases, this treatment is not required; on giving support to the
trunk, and raising the shoulders to an equal level, the muscles of the
back, perhaps stimulated by powerful and repeated friction, gradually
bring the column into its proper form. Then the position of the head to
one side is no longer required to balance the body. But a cure can be
expected only when no material change has taken place in the form of
the individual bones.
Excurvation of the cervical vertebræ,—bending of the head forwards,
and perhaps a little to one side, generally to the right,—takes place
as a consequence of disorganisation of the ligaments and connecting
fibro-cartilages of the vertebræ, with subsequent ulceration of the
bones. The disease generally occurs in the superior vertebræ; in the
articulation of the atlas with the occiput, or with the vertebræ
dentata, or in the articulation of the latter with the one below. The
articulations on the left side are usually affected first. There is
stiffness, pain, and swelling of the soft parts covering the affected
bones, attributed perhaps to exposure to cold, as when sitting in a
draught, and supposed to be merely crick of the neck. The posterior
cervical muscles are weakened, and the head is bent forwards. The
patient is unable to support his head by the usual muscular action, and
when in the erect position places his hands on the temples, to prevent
it from dropping, and to keep it steady. Difficulty of swallowing is a
prominent symptom from the first, as can readily be imagined when the
close application of the constrictors of the pharynx to the forepart
of the affected bones is kept in remembrance. The position of the head
also renders deglutition awkward. The disease is attended with great
suffering, evinced by marked anxiety of the countenance; and the pain
is most violent during the night. The complaint is too frequently
trifled with at the commencement, being not understood, nor its danger
appreciated. The swelling increases, with pain, and the chin falls down
on the sternum. The patient grows emaciated, and perhaps becomes weak
in the lower limbs, and even in the upper; the feces and urine are
imperfectly retained. Occasionally, abscess forms behind the upper part
of the pharynx, increasing the pain and the difficulty of deglutition.
On making an examination through the openings by which the abscess has
emptied itself spontaneously, the bone is felt bare; and portions,
even large, of the vertebræ, or vertebra, are, after some time,
discharged, so as to expose the theca of the spinal cord. Even in such
circumstances patients have lingered on, and that for so long a period
as to allow of some unprincipled fool advertising a perfect recovery.
The termination of caries of the cervical vertebræ, often without
any appearance of abscess, is in general fatal and sudden. The head,
slipping from its support, falls forwards or to a side, causing
imme384diate and complete paralysis of the whole body; dissolution soon
follows. On examination, the articulating surfaces of the vertebræ
are found displaced, and the shreds of ligaments which connected them
ruptured. The atlas is separated from the occiput; or the processus
dentatus, escaping from its situation, in consequence of destruction of
its confining ligaments, is found compressing the medulla oblongata.
This process is very often destroyed almost entirely, or it is so far
detached by ulceration at its root as to be easily broken off. The
disease in general seems to commence in the articulations, whereas in
the vertebræ with larger bodies, abscess and ulceration have their
foundation and origin more frequently in the deposit of tubercular
matter in the cancellated texture of the bones. In other instances, the
termination may be more slow and gradual; the patient is worn out by
long suffering and continued purulent discharge; change of structure
takes place in the theca vertebralis, or in the medulla itself; serous
effusion occurs at the base of the brain; the patient’s sensations are
blunted, and he loses the use of his limbs gradually; his intellects
fail, and coma supervenes, followed by death.
Active and early interference can alone arrest, subdue, or prevent
the dreadful consequences of the disease above described; it is
quite intractable in its later stages. Confinement to the recumbent
posture, and strict rest of the affected parts must be enjoined;
and blood is to be abstracted locally, once and again, according to
circumstances; afterwards counter-irritation is to be employed, and
repetition of moxas or of caustic issues is the most efficacious. When
the painful feelings have subsided, and some impression has been made
on the disease, the patient appearing to convalesce, the head must be
supported by a proper machine for a long time. He will thus be enabled
to use his limbs, to move about, and repair his general health, the
weight of the head being taken from the weakened column.
The External Jugular vein may require to be opened for the
abstraction of blood in affections of the head; or when venesection
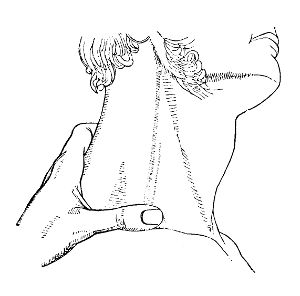 cannot be readily performed at the bend of the arm, from the small and
indistinct condition of the veins in children, or in people loaded with
fat. The vein is made to rise by pressure with the finger or thumb, as
seen in the accompanying cut, above the clavicle. The lancet is passed
though the integuments and platysma myoides into the vessel, midway
between the jaw and clavicle. After a sufficient quantity of blood has
been withdrawn, the pressure below is removed, and the edges385 of the
wound are put together with a bit of court plaster, or by means of a
compress and bandage lightly applied.41
cannot be readily performed at the bend of the arm, from the small and
indistinct condition of the veins in children, or in people loaded with
fat. The vein is made to rise by pressure with the finger or thumb, as
seen in the accompanying cut, above the clavicle. The lancet is passed
though the integuments and platysma myoides into the vessel, midway
between the jaw and clavicle. After a sufficient quantity of blood has
been withdrawn, the pressure below is removed, and the edges385 of the
wound are put together with a bit of court plaster, or by means of a
compress and bandage lightly applied.41
Ligature of the common Carotid may be required for the cure of
aneurism at the angle of the jaw; or on account of hemorrhage from deep
wounds in the same situation, when, from any circumstances, the divided
extremities of the vessels cannot be secured. A deep incision of the
angle of the jaw, towards the base of the cranium, not only divides
important branches of the carotid, but may also wound the vertebral
arteries where they project in a tortuous fashion, betwixt the dentata
and atlas, or betwixt the latter bone and the occiput.
Ligature of the common carotid has been had recourse to, in order to
stop bleeding from the mouth, nostrils, and other parts connected
with the face,—for the cure of large or deep-seated aneurism by
anastomosis,—and as a preliminary step to the removal of large
and firmly attached morbid growths of the face or neck. This last
proceeding, as already remarked, does not in any way enhance the
patient’s safety, whilst it adds much to his suffering.
The carotid has also been tied for the cure of aneurism at the root
of the neck, when it was impossible to place a ligature betwixt the
tumour and the heart. My opinion regarding this practice I have given
formerly, when treating of aneurism in general.
For aneurism at the angle of the jaw, the point of deligation must in
a great measure depend on the size of the tumour. The artery is most
conveniently reached where it is crossed by the omo-hyoideus; and, when
deligation at this point is both practicable and eligible, the vessel
is exposed at the upper edge of the muscle. But circumstances may
require the ligature to be placed much lower.
The patient is placed, either sitting or lying, with the head thrown
back, and turned slightly to the side opposite the tumour. An incision
is made in the upper triangular space of the neck, and in the course
of the vessel, midway betwixt the sterno-mastoid muscle and the
muscles covering the forepart of the larynx. Its extent depends on
the thickness of the neck—on the muscular development and quantity of
fatty matter, whether the neck be long or short. From two to three
inches will in general afford sufficient space. The first sweep of the
scalpel penetrates the skin, platysma-myoides, and cellular tissue. The
cervical fascia is then divided carefully, with the hand unsupported.
During the incision, the parts should be a little relaxed by attention
to the position of the head. The sheath of the vessels is exposed by
cautious division of the cellular tissue which 386occupies the space
betwixt it and the cervical fascia. Thin copper spatulæ, bent to suit
the purpose, are used to keep the edges of the wound apart. In general
there is very little bleeding; but, that the operator may be sure of
what he cuts, it is necessary frequently to clear the cavity with a
bit of soft sponge. Each step of the operation should be slowly and
surely accomplished; the least hurry is culpable. When the slight
oozing has ceased, the common sheath,—which is distinctly seen, with
the descendens noni lying on its forepart,—is to be opened to a slight
extent with the point of the knife—the hand steady and unsupported,
and no director used. The descendens noni is left to the inner side.
The internal jugular vein, swelling up on account of the struggles
and hurried respiration of the patient, has in some cases been found
troublesome at this period of the operation, rendering the opening of
the sheath and the use of the needle difficult. I have not met with any
such obstacle in the cases in which I have been concerned. The aneurism
needle should be slightly curved, with a perforation near the point;
and the point should neither be bulbous, nor at all sharp, but all of
the same thickness, and well blunted at the extremity and edges. It
is introduced, carrying a firm round ligature of flax or silk, well
waxed through the opening in the sheath, betwixt the par vagum and the
artery, and from the outer side. The point is moved very slightly from
side to side, and carried under the artery; no force being used, as it
is unnecessary, and apt to be injurious. The instrument is thus gently
insinuated, not thrust, through the cellular tissue, and made to appear
on the opposite side of the vessel, with its point towards the trachea.
It ought to be passed close to the arterial coats, and care must be
taken to avoid including within its track part of the common sheath, or
the descending branch of the ninth. Unless the surgeon be indeed very
rash, there is little risk of the vein or par vagum being injured; to
include them along with the artery would argue no small degree of most
deplorable ignorance. The loop of the ligature is laid hold of either
with the fingers, with forceps, or with a small blunt hook, and drawn
towards the surface of the wound. It is then divided, and one-half
retained, whilst the other is withdrawn along with the needle. The
vessel must not be raised up from its situation, or detached from its
cellular and vascular connexions, more than is merely sufficient for
transmission of the needle. A single knot is cast upon the remaining
half of the ligature, passed down, and tied firmly on the vessel, by
the forefingers of the operator. This is secured by the finger of an
assistant, whilst the ends are again passed through, so as to complete
the reef-knot, and run down tight as before, the assistant slowly
withdrawing his finger to make way for the ligature. A third knot
may be made to insure security; but is seldom, if ever, necessary.
As already observed, everything must be done with deliberation and
caution, and the operation may be thus safely concluded in a very
few minutes. One end of the ligature may be cut away close to the
knot, or both brought out of the wound. The edges of the wound are
put together, after all oozing has ceased, by one or two stitches,
and the intermediate application of isinglass plaster; bandaging is
unnecessary, and might be hurtful. The patient is placed in bed, with
the head387 elevated considerably, so as to relax the neck. The wound
will probably heal by the first intention, excepting in the immediate
neighbourhood of the ligature; and the separation of this may be looked
for from the tenth to the twentieth day. Then all risk of danger may be
considered as past.
Ligature of the Arteria Innominata has been practised in very few
cases. It may possibly be required for aneurism of the subclavian, or
of the root of the carotid; or for large axillary aneurism, greatly
raising the shoulder, and involving the parts at the root of the neck.
The patient should be placed recumbent, with the head well thrown
back. An incision from two inches and a half to three inches in
extent is made in the course of the carotid, terminating over the
sterno-clavicular articulation. If the incision is made more towards
the inner border of the left mastoid muscle, greater space is gained.
From that point, another is carried along the upper margin of the
clavicle, to the extent of an inch and a half. The sternal attachment
of the sterno-mastoid muscle is separated, the cervical fascia divided,
the cellular tissue betwixt the sterno-hyoid muscles separated, and the
vessel exposed. During the dissection, the internal jugular vein, the
par vagum, and the recurrent branch, the inferior thyroid artery, and
the arterial distributions from the thyroid axis, must be carefully
avoided. The operator should, by free external incisions, make a
dissection sufficiently spacious to admit of his seeing the bottom
of the wound distinctly as he proceeds. It is necessary that he not
only feel but see what he is about to cut; groping in this situation,
and amongst such important parts, is unsafe, to say the least of it.
Caution in passing the needle is here required equally as in ligature
of the carotid. In such deep wounds the aneurism needles of Weiss,
Bremner, Mott, or Gibson, may perhaps be found useful; but in general
the common one is sufficient, and has always answered my purpose
perfectly. During the dissection, it must be borne in mind that the
pleura is not far from the edge of the knife. In one case of aneurism
above the clavicle, and close to the outer border of the sterno-cleido
mastoid muscle, and of the anterior scalenus, I exposed the arteria
innominata by a cautious dissection; but, instead of surrounding that
vessel, applied ligatures to the root of the subclavian and of the
carotid. This latter was closed with the view of insuring the formation
of a clot in the arteria anonyma. The patient suffered under abscess
of the mediastinum, inflammation of the heart and pericardium, and
ultimately he had repeated hemorrhage from the wound. The arteria
innominata and the root of the two vessels were obstructed by firm
coagulum. The blood had come from the distal end of the subclavian, and
had been furnished by the regurgitation through the vertebral, thyroid,
mammary, &c.
Ligature of the Subclavian Artery is required for the cure of
axillary aneurism. That portion of the vessel within the scalenus and
outside of the pneumogastric nerve is unfavourable for operation, in
consequence of many branches being given off in an exceedingly short
space. Besides, important veins and nerves are in the immediate388
vicinity. And though these were avoided, and the vessel reached and
tied, still there would be no likelihood of a favourable result;
obliteration of the vessel would not be expected to take place at the
deligated point, one or more collateral branches arising close to the
ligature. On the outside of the scalenus there is no such objection.
But the vessel is deep, even in the healthy state, and much more so
when aneurism has appeared in the axilla, and has attained but even
a small size. But again, when the tumour is large, the shoulder is
much elevated, and firmly fixed in its exalted level, so as greatly to
increase the depth of the vessel.
The shoulder is to be depressed as much as possible, and the head
thrown to the opposite side. An incision is made along the upper margin
of the clavicle, and a second perpendicular to the first. These must
be proportionate to the size of the patient, and the supposed depth
of the vessel. It is better to err in making the external incisions
too large than too small; neither the pain nor the duration of the
cure is much increased thereby. But, by an opposite course, both
the difficulties and the dangers of the operation are rendered far
greater. The external jugular vein must be avoided if possible by
the knife; it should be detached slightly, and pulled inwards. The
supra-scapular artery, running in a line with the clavicle, ought also
to be saved; it acts a principal part in performing the anastomosing
circulation after ligature of the trunk; and, although the arm would
receive a sufficiency of blood from other branches, it is well to
keep this entire—not to mention the trouble which wound of it would
occasion the operator, by constantly filling his incisions with blood,
and the delay caused by the application of ligatures to the bleeding
extremities. Its division can easily be guarded against, and should
be avoided. The subclavian vein is not in the way; it is lower down
under the clavicle than where the surgeon requires to introduce his
instruments. The fascia and cellular tissue are divided carefully,
until the cervical plexus of nerves appears, and then the artery is
to be looked for on the same level with the plexus, and towards its
sternal margin. But, in cutting for this or any other vessel, it
must be recollected that pulsation is a very uncertain guide. It is
communicated to the neighbouring parts, and often is scarcely to be
felt at all, or is at least very indistinct. In any situation pulsation
is very perceptible before division of the integuments, and other
superimposed parts; but after resistance has been removed by exposure
of the vessel, it ceases almost entirely. The sense of touch is the
principal guide, and, to experienced fingers, the feel of nerves is
different from those of arteries. The ligature has been passed round
one of the cervical plexus, as happened in one of my own cases; the
mistake was, however, not without its use, for, on discovering that it
was a nerve, I retained the ligature, no knot having been cast, and by
it pulled the nerve out of the way, so as to allow of the artery being
more readily secured. The artery is felt as it crosses over the first
rib, and by pressure there, pulsation in the arm is stopt; sometimes it
may be even seen. The knife, guided by the finger, is then used very
cautiously to prepare the vessel for ligature. The vessel may be found
unsound, and dilated to a further extent than had been ex389pected; and
then it may be necessary to trace it towards the heart, and even to
divide the scalenus anticus in part, the phrenic nerve being kept free
from injury, in order to expose a sound portion for the application
of the ligature. This was found necessary in one of my own cases,
and also in one operated on by the Baron Dupuytren. A blunt-pointed
needle is passed, either plain or with a separable point, and the knots
made as was formerly described. A piece of strong wire doubled, and
either notched or perforated at the extremities, affords assistance in
securing the knots in so deep and contracted a space. Various kinds
of serre-nœuds and needles have been recommended; but the simpler the
instruments employed are, and the less a surgeon depends on them, the
more likely is he to succeed in his undertaking.42
390
During the time that this sheet was passing through the press, a case
of aneurism above the right clavicle came under treatment in the
hospital, on which it was proposed to perform the operation of 391tying
the trunks of the subclavian and carotid as they pass off from the
innominata. The necessary incisions were made, but the innominata was
found wanting. After some troublesome dissection, the 392subclavian
artery, which appeared to have come off irregularly, was discovered
crossing from the left to the right side, to take its place betwixt
the scaleni, rather more than half an inch behind the carotid, and
close upon the forepart of the vertebræ. The ligature was placed on the
mesial side of the pneumogastric nerve, and close to it. Up to this,
the twenty-second day, the case is going on most favourably.
The axillary portion of the brachial artery cannot require to be
tied for true aneurism. Were the aneurism seated at the border of the
axilla, and the upper portion of the vessel beneath the clavicle free,
the best, wisest, and safest proceeding is to tie the subclavian. Then,
the shoulder not being raised, the vessel is not so deep as when the
aneurism involves the whole axilla. The incisions are not so deep nor
so extensive, and do not implicate so important neighbouring parts as
those for ligature of the axillary artery; and besides, the vessel is
tied farther from the diseased part.
The axillary artery may be tied on account of wounds, either
immediately upon the infliction of the injury, or some time afterwards.
The dissection is difficult, the vein being much in the way, and the
vessels surrounded by nerves, and intimately connected with them by
dense cellular tissue. The artery is more involved at the middle
portion of the axilla than at the superior and inferior; at that point,
too, the cephalic vein, as well as the axillary, impedes the operator.
To reach the upper portion of the artery, much muscular substance must
be divided. An extensive incision, in the course of the vessel, is
made through the integuments. The pectoralis major is got through by
separation and division of the fibres, the incision in it being made
with as little cross-cutting as possible. Part of the pectoralis minor,
probably the superior half of the muscle, must also be cut. The parts
are then exposed, the vein to the inner side of the artery, and the
nerves interlaced. The vessel is carefully isolated at one point, and
there secured.
It is almost impracticable to reach the middle portion of the
axillary—supposing the vessel to be divided into three equal
portions—without injurious interference with the nerves. If operating
with the view of tying the extremities of the vessels wounded at this
point, the probability is that the nerves have been divided along with
the artery, and then the proceedings are more simple. The incisions are
made 393in the direction of the bleeding point; this is reached, and each
extremity of the vessel securely tied.
The lower third of the artery is less involved with the vein and
nerves, and can be reached without division of muscular fibres. The
arm is abducted and elevated as much as possible. The axilla is thus
exposed. A free incision is made in the course of the vessel, which, by
cautious dissection, is brought into view; it can then be dealt with as
may be required.
Spontaneous aneurism is of rare occurrence, lower in the brachial
artery than its axillary portion. However, it is sometimes met with
at the bend of the arm. But the aneurismal tumour in this situation
is more frequently the consequence of wound of the vessel, inflicted
whilst opening a superimposed vein. The mode of proceeding in
venesection, the precautions to be employed, and the evils that
sometimes follow this little operation, will be treated of by and by.
Wounding of the artery is not so common an accident now as formerly.
Venesection is not so universally and unnecessarily resorted to as
formerly, and is performed by better instructed practitioners.
Puncture of the brachial artery, at the bend of the arm, is not
uniformly followed by extravasation of blood, or by the formation of
aneurism. That it is wounded is known by the impetuous and saltatory
flow of florid blood, accompanied with a wheezing noise. In such
circumstances, the thumb is placed firmly over the wound; the fingers
separately, the hand and the forearm of the patient are all supported
by uniform bandaging; and a graduated compress, supplying the place
of the thumb, is firmly applied, and must be retained for many days.
Thus extravasation is effectually prevented. But the measures must be
adopted instantly, before the edges of the opening are rounded, and any
quantity of blood has escaped into the cellular tissue; the apparatus
must be well applied and retained. When pressure is required on any
point, it is absolutely necessary to give support to the lower part
of the limb, as was formerly insisted on; and the proceeding is, if
possible, more necessary in this case, the requisite pressure being
very great. If ordinary compression only, sufficient to prevent the
flow of blood through the opening in the integuments, is applied,
blood is extravasated into the cellular tissue, breaking it up, and
causing condensation beyond; fluid blood accumulates in the space thus
formed; the surrounding cellular tissue is more and more condensed, at
length constituting a firm sac, confining the fluid, and communicating
with the opening in the artery; in fact, a pulsating and gradually
increasing aneurism is established.
Or a sac is formed, into which blood is propelled from the artery, and
which also communicates with the opening in the vein. This state of
parts is denominated varicose aneurism; it is very rare.
Or, again, no extravasation takes place, and the artery and vein unite
by lymph effused around the openings, the wounds remaining unclosed,
and forming a permanent communication between the vessels. Thus, a
portion of the arterial contents is constantly being injected into the
vein, producing a thrilling sensation, but little or no tumour. The
passage of the blood through the narrow aperture is also accompanied by
a peculiar noise, closely resembling that caused394 by the motion of the
fly-wheel in a musical box. This disease is termed aneurismal varix,
and is not so rare as the preceding. For this treatment is seldom
requisite.
In recent cases of false aneurism, the sac may be cut into, the vessel
exposed, and tied above and below the opening. This is recommended
from its being found that the tumour is sometimes slow of disappearing
after ligature of the vessel at a distance above. But when the tumour
is of considerable duration and size, containing coagula, and the
surrounding parts are separated and altered in structure, there is
no doubt as to the propriety of tying the humeral near its middle—as
also, in the case of spontaneous aneurism. The vessel is not deep, but
much entangled with nerves and veins. A free incision is made over its
course, dividing the skin, cellular tissue, and fascia; the sheath is
opened, and a ligature passed round the exposed artery. But it must be
recollected that high division of the humeral is not uncommon, and,
before casting the knots, pressure should be made on the vessel with
the finger against the loop of the ligature, and the effects on the
tumour watched; if pulsation cease, and the tumour become flaccid,
the ligature should be secured; but, if no effect is produced on the
swelling, high division is demonstrated, and the other branch must
be looked for. Pulsation is certain to return in the tumour, after a
few days, and if slow in again disappearing, gentle pressure should
be employed—the arm, hand, and fingers being previously bandaged, to
prevent infiltration of the limb.43
395
Wounds of the radial and ulnar arteries may require their being
exposed and tied at various points and at various periods—shortly
after the accident, or after the lapse of many weeks—on the occurrence
of secondary bleedings, or after the formation of false aneurism.
This is accomplished by incision in the course of the wounded vessel,
sacrificing as few muscular fibres as possible. Nevertheless, the
incision must always be free, to enable the surgeon to effect his
purpose readily.
Wounds of the Palmar Arches, and of the branches proceeding from them
to the extremities of the metacarpal bones, are exceedingly common; as
also wounds of the radial artery betwixt the thumb and forefinger, of
the arteria radialis indicis, and of the superficial volar branch. The
opening in the integuments and palmar aponeurosis is usually narrow,
and the hemorrhage copious; it is generally arrested by pressure, not
always well or efficiently applied. From these circumstances, blood
is extravasated extensively into the deep cellular tissue, blood
continuing to escape from the artery, and being either imperfectly
discharged, or completely confined. Great swelling, with tension and
acute tenderness, takes place; in fact, rapid inflammatory action is
kindled in the infiltrated parts, and unhealthy abscesses form; the
matter ultimately reaches the surface, but by that time ulceration or
partial sloughing has taken place at the wounded part of the vessel;
profuse and repeated hemorrhages take place, and are with difficulty
controlled. The patient becomes weak and pale. The greater part of
the forearm may become involved in the inflammation, terminating in
infiltration of the cellular tissue, and the formation of diffuse
abscesses.
In the first instance, instead of trusting to pressure,—which almost
uniformly disappoints expectation, does not prevent internal bleeding,
and leads to a severe form of inflammatory action,—it is better at
once to enlarge the wound, and tie the wounded vessel above and
below the injured point. Thus all bleeding is effectually prevented,
and the risk of unfavourable consequences done away with. But after
inflammatory swelling has commenced, such a proceeding is difficult,
often almost impossible, and generally fruitless. The parts are then
full of blood, lymph, serosity, and pus, separated from each other,
and changed both in appearance and structure; the vessel is either
not visible on account of the infiltration around, or its coats are
so diseased as to be incapable of holding a ligature. At any period,
it is unsafe and unwarrantable to dive, pretty much 396at random,
with a sharp needle, amongst tendons, nerves, arteries, and veins,
with the hope of so including the wounded branch. In some cases of
secondary bleeding—if no great inflammatory action has taken place,
and no abscesses have formed—the wound may be dilated freely, and
compression made on the bleeding point by dossils of lint filling the
wound completely, and supported by a bandage. This dressing, retained
for some days, often succeeds perfectly; permanent obstruction of the
vessel, and consolidation of the parts immediately around, having
been accomplished by the effusion and organisation of lymph. When
this method fails—and when the case is more advanced, with pain, and
swelling, and abscess—weakening of the circulation in the part is found
to be effectual. The main artery is to be obstructed at a distance from
the wounded part. It is needless to tie the radial, or the ulnar, or
both; for still blood will be poured in by the interosseous and its
anastomoses. The humeral must be secured in the middle of the arm, as
has been practised in many instances, and with uniform success. Thus
the bleeding is arrested until the wounded vessel recovers, and becomes
permanently closed by salutary effusion; then the inflammatory action,
and its consequences, in the surrounding parts, must be treated on the
general principles of surgery.
Paronychia, or Whitlow, designates inflammatory action and its
consequences, in the structures composing the fingers. The mere
surface may be the seat of the inflammation of the cellular tissue,
or the fibrous structure betwixt that and the sheath of the tendons;
or the firm and true sheath of the tendons, and the synovial surface;
or the investing membrane of the bone, the bone itself, and the
articulating surfaces and apparatus may be involved secondarily, or
from the first. The inflammatory action may commence in any of these
structures, but, if uncontrolled, ultimately attacks the greater
number, or all of them. The deeper seated the action, the more violent
are the symptoms, and the greater the danger to the member. In the
cutis vera of the fingers, there is a plentiful distribution of nerves
of sensation; and, consequently, in superficial whitlow, the pain is
often severe, with throbbing, and an occasional feeling of itching.
The part is swelled and red, and the redness is diffused. After a
short continuance, the swelling increases at some points, often about
the root of the nail, from effused fluid betwixt the cuticle and rete
mucosum; the fluid is sometimes serous, generally sero-purulent. In the
deeper-seated inflammation, the pain, throbbing, heat, and swelling,
are all greater. The pain is more intense, and almost intolerable,
allowing the patient little or no rest; and the throbbing extends
to the vessels of the hand and forearm. A considerable degree of
fever attends. The action either involves one phalanx, or extends
over the whole finger, and ultimately attacks the hand. The palm is
hard, pained, and swelled; and, in advanced cases, swelling takes
place above the annular ligament. Often the surface of the back of
the hand is also inflamed, and the cellular tissue loaded with serum.
The disease, if not actively and properly treated, terminates in a
very397 short time; in two or three days suppuration takes place, with
sloughing of the cellular tissue, of the sheaths of the tendons, and
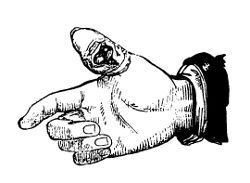 of the tendons themselves. Either ulceration or necrosis—often both in
combination—occurs in the phalanges; or the apparatus of one or more
of the articulations is destroyed. Abscesses also form in the palm,
on the back of the hand and finger, and sometimes under the fascia of
the forearm. The separation of portions of one of the tendons is not
always followed by loss of motion in the finger; neither is exfoliation
of the tendons themselves. Either ulceration or necrosis—often both in
combination—occurs in the phalanges; or the apparatus of one or more
of the articulations is destroyed. Abscesses also form in the palm,
on the back of the hand and finger, and sometimes under the fascia of
the forearm. The separation of portions of one of the tendons is not
always followed by loss of motion in the finger; neither is exfoliation
 of the greater part of the distal phalanx always attended with much
deformity or shortening, a nucleus being often left from which bone may
be reproduced. But destruction of the whole flexor or extensor tendons
of one of the middle or proximal phalanges, or destruction of one of
the articulations connecting them, is not only attended with great
suffering, but followed by total uselessness of the part. The wounds
may, after a tedious process, heal up; but the finger remains deformed
and immovable, in a contracted or extended position, as may be.
of the greater part of the distal phalanx always attended with much
deformity or shortening, a nucleus being often left from which bone may
be reproduced. But destruction of the whole flexor or extensor tendons
of one of the middle or proximal phalanges, or destruction of one of
the articulations connecting them, is not only attended with great
suffering, but followed by total uselessness of the part. The wounds
may, after a tedious process, heal up; but the finger remains deformed
and immovable, in a contracted or extended position, as may be.
The disease may be occasioned by bruises or punctures, the instrument
with which the puncture is inflicted being impregnated, or not, with
some putrid animal matter. Violent inflammatory action almost uniformly
follows opening of the articulations, and also lacerated wounds over
the joints. Compound fractures and dislocations of the phalanges are
certainly followed by a severe form of inflammation. But the disease is
met with in all degrees of intensity, occurring without any assignable
cause. It prevails in spring and autumn; and is common in hard-working
people, in butchers, cooks, &c.
In superficial whitlow, the bowels must be attended to, and blood may
be abstracted locally, either by punctures or by the application of
leeches along the side of the finger, hot fomentation being assiduously
and regularly employed afterwards. Or the nitrate of silver may be
rubbed lightly over the discoloured parts; frequently the inflammation
may be arrested, and resolution speedily effected, by this simple
application, laxative or purgative medicines being at the same time
administered, as required. The collections which form are evacuated by
simple division of the cuticle, and this, when hard, should be clipped
away; poultices are used for a short time, and then the raw surface
is dressed simply, and the finger bandaged daily. The hand should be
kept constantly elevated. The swelling is soon reduced, the cuticle is
regenerated, and free motion of the finger returns gradually.
In more severe cases, fomentation and copious abstraction of blood
by leeching, at a very early stage, may effectually suppress the
in398flammatory action; but patients seldom apply till after the
opportunity for this treatment has passed. When tension has occurred,
whether purulent matter has formed or not, a deep and free longitudinal
incision must be made, including the affected tissues. This is
uniformly followed by great relief, all the violent symptoms subside,
and the action is limited; the effusion, if any, escapes, and the
affected bloodvessels are emptied—further suppuration is prevented,
and the tissues are perhaps saved from destruction. Fomentation and
poultice are used till the swelling begins to disappear, and the
discharge to diminish; and the hardened cuticle is removed, when
detached. The cure is completed by bandaging, and such applications to
the wound as its appearance may render suitable. Should inflammation
recommence and extend, or abscess threaten in other parts, recourse
must again be had to free incision, followed by the treatment already
described.
Destruction of the articulating apparatus, with ulceration of the
opposed surfaces of the bones, is indicated by indolent swelling
around, by unhealthy and profuse discharge, by distinct grating being
produced on motion, and by marked and unnatural looseness of the joint.
In such circumstances, amputation of the finger above the diseased
part is fully warranted. But if the patient is obstinate in refusing
to submit, or if he is in that rank of life where stiffness of the
finger is of no great consequence, the member should be kept steady
in a convenient position, so as to favour anchylosis. By splints and
bandaging it is preserved in a state of semiflexion, so that, after
the cure by anchylosis, it may not be in the way when the patient
lays hold of anything, as it would be were it bent into the palm, nor
exposed when the other fingers are bent, as must be the case were it
kept quite straight. Still the finger is often very useless—worse
than useless—when stiff either from loss of the tendons or from
destruction of the joint; and more particularly when its position is
awkward. So much inconvenience does it give rise to, that patients,
who peremptorily refused amputation whilst the case was recent, often
return, after a tedious and painful cure by anchylosis, soliciting
removal of the deformed and annoying member. When the thumb, however,
is the seat of disease, it is of great moment to save any part of it.
A stiff joint in the thumb is of less consequence than in a finger;
it can still be brought to oppose the rest of the hand in seizing
and retaining hold of objects. To promote anchylosis, the affected
articulation must be kept at perfect rest, and for a very considerable
time. By pursuing this practice, the thumb, represented at page 397,
though in a very bad state, the joint being thoroughly disorganised,
was preserved. In severe cases of whitlow, all the fingers, the whole
hand, and even the wrist, long remain rigid; but the rigidity is
gradually dissipated by friction, and by motion, at first gentle and
passive.
Chronic thickening and contraction of the palmar aponeurosis occurs
occasionally, and, in some cases, to such an extent as to disable the
hand almost entirely. The fingers are permanently bent, the palm is
hard, and the integument puckered. The most severe examples which I
have witnessed occurred in those who were in the399 frequent habit of
playing keyed or stringed instruments; in others no cause could be
assigned. Frictions with all kinds of oils and compound liniments,
plasters, ointments, &c., have been tried as remedies for this
affection, but in vain. The tendinous slips passing to the contracted
fingers have been divided, and the origin of the palmar fascia has been
cut across, but without permanent benefit. Indeed I believe the disease
to be incurable.
The term Onychia is sometimes, and not without good reason,
designated maligna: it is applied to ulceration about the nail.
Some of such sores are small, and not indisposed to heal; others are
very obstinate. They occur at all periods of life, frequently during
infancy. They usually commence in a small and irritable tumour or
granulation by the side of the nail, or at its root, with swelling and
redness around. This may follow bruises or laceration and removal of
the nail, extravasation under it, and various injuries of the part. The
disease is also met with in the toes, most frequently the great one,
causing much lameness; then it is generally owing to the pressure of
tight shoes. In many cases the ulceration is extensive, shreds of the
nail projecting through the angry surface; there is considerable loss
of substance; the discharge is thin, bloody, acrid, and abominably
fetid; the edges of the sore are jagged, and the integuments around
are of either a bright or a dark red, according to the state of the
disease. Sometimes the bone is exposed, and involved in ulceration;
or, instead of having lost substance, it is found of an unusually
spongy and open texture, and with recent osseous matter superadded. A
violent burning pain attends the disease when advanced; the absorbents
are irritated and inflamed, and the glands enlarge along their course.
The general health is often impaired in consequence; frequently the
disease occurs in those of broken-up constitution, along with sores
and eruptions on other parts of the surface, ulcerations of the mucous
membranes, and other indications of cachexia.

By judicious exhibition of purgatives, antibilious medicines, and
preparations of sarsaparilla, and by regulation of diet, the general
health may be improved. The edge of the nail, when in contact with the
ulcerated surface, must be removed—more especially when the great toe
is affected; not that any undue growth is the cause of the disease,
but because the sore, pressing on the sharp edge, pro400duces much
pain, and keeps up the morbid action. About one-third in breadth of
the nail should be taken away; one blade of strong and sharp-pointed
scissors is passed along beneath the nail as far as its root, and
by rapid approximation of the other blade the part is divided; the
isolated portion is then laid hold of by dissecting forceps, or small
flat-mouthed pliers, and pulled away by the root. This should be
performed as quickly as possible, for the operation, though trifling,
is attended with most acute pain; it is quite effectual, the relief is
great, and almost immediate. The nail may also be removed by scraping
and paring; but this method is not so effectual as the preceding,
and almost equally painful. Afterwards the best application to the
ulcerated surface, as to other irritable sores, is the nitrate of
silver, either used solid and followed by poultice, or employed in the
form of lotion. The remedy is almost specific; very few cases prove
obstinate under it. Sometimes it may be of advantage to alternate it
with the black wash. In protracted and unyielding cases, removal of the
whole matrix of the nail has been proposed; the dissection is painful
and tedious, and its efficacy doubtful. When the sore is of a weak
character, discharging a glairy secretion, studded with soft flabby
granulations, connected with unsoundness of the neighbouring cellular
tissue, surrounded by undermined integument, and by considerable
boggy, soft swelling, free application of the caustic potass is highly
beneficial. When the bone is denuded, and involved in ulceration, the
phalanx should be amputated.
Unhealthy children are subject to disease of the phalanges, and of
the metatarsal and metacarpal bones, excited by slight injury, or
originating without apparent cause. Often more than one bone is
affected. There is great swelling of the soft parts around the diseased
bone, indolent, and not painful; at first hard and white, afterwards
more yielding, and of a dark-red hue at one or more points. Imperfect
suppuration takes place, the integuments ulcerate, and the cavity of
 the abscess leads to the exposed bone; a portion of this generally
dies, and is a long time in separating. Great addition of bony matter
is deposited around, in irregularly aggregated nodules; and a large
shell is so formed, partially investing the sequestrum. This affection
may be termed scrofulous necrosis.
the abscess leads to the exposed bone; a portion of this generally
dies, and is a long time in separating. Great addition of bony matter
is deposited around, in irregularly aggregated nodules; and a large
shell is so formed, partially investing the sequestrum. This affection
may be termed scrofulous necrosis.
Or the bone does not die, but is exposed and ulcerated superficially;
or a considerable cavity forms in its interior, apparently from
tubercular deposits and suppurative degeneration of the cancellated
structure. The secretion from the ulcerated surface is thin, acrid, and
often bloody; and new osseous matter is studded around. The surface of
the rest of the bone is unusually open in texture, whilst its interior
is condensed, and the cancelli are filled with lardy substance. This
form may be called scrofulous caries.
Abscesses in the soft parts form one after another, several of the
bones are often affected at the same time, superficial abscesses and401
affections of the joints and bones often take place in other parts, and
the patient grows weaker and weaker.
Whilst the surgeon attends to the general health, and employs
palliative local applications, nature frequently effects a cure. The
sequestrum ultimately separates, or the ulceration gives way to more
healthy action. New bone fills up the cavity, the redundant osseous
deposit gradually diminishes, the openings in the integuments close,
and the swelling subsides. In some rare cases, it may be necessary to
take away the offending part, in consequence of the health alarmingly
declining.
Collections in the Thecæ of the flexor tendons are occasionally met
with. Those of the thumb and forefinger are most frequently affected.
The swelling often attains considerable size. The fluid is colourless
and glairy, mixed with small cartilaginous bodies of a flattened form,
and the size of mustard seeds, or split peas. The swelling sometimes
extends under the annular ligament, and under the fascia of the
forearm. Alternate pressure on the different parts of the swelling is
attended by a very peculiar sensation. Motion of the parts is seriously
retarded.
Accumulation of the fluid is not prevented by any means. Puncture has
been practised successfully in several instances, in others a good
deal of inflammatory action followed. On the escape of the fluid, the
motions of the parts are so far regained.
Ganglia are collections in the bursæ, of various sizes, about the
wrist. They are situated more frequently on the fore than on the back
part. Sometimes they occur, small, on the sides of the fingers. At
first they are attended with pain, afterwards with inconvenience only.
The swelling is usually globular; but when large, as on the back of the
wrist, the form is rendered irregular by the pressure of the tendons.
The cyst is generally of considerable thickness, the fluid glairy and
albuminous. They present an unseemly appearance, and when awkwardly
situated, retard the motions of the limb. Frequently they form without
apparent cause; sometimes they are attributed, and perhaps rightly, to
a twist or over-exertion of the wrist, like windgall in hard-wrought
horses, who have been put to work when young, and before their full
strength has been attained. The affection is most frequently met with
in females of the lower ranks; in them the structure of the limbs is
more delicate than in males, and they are often obliged to use great
exertions with the upper extremities before the growth of the body is
completed.
Friction is of no use. Continued pressure on the swelling, by coins or
small pieces of lead bound down for weeks or months, is very seldom
followed by cure. If the tumour is placed over a bone, sudden and
firm compression should be made with the thumb, so as to rupture the
cyst, or with the same view it may be struck sharply by an obtuse
body. The contents are thus extravasated into the cellular tissue, and
are speedily absorbed; the cyst inflames, and becomes obliterated.
Sometimes the excitement is insufficient for complete402 closure of the
cyst, and the swelling returns. When the cyst is thick, the tumour of
long duration, and the person impatient of pain, it may be punctured by
a cataract needle of any kind; one thin and double-edged is probably
the most convenient. The instrument is introduced through the skin,
at some distance from the swelling; and, by moving the point of the
needle after penetration, the cyst is divided freely. The needle is
withdrawn, and the orifice closed by the finger. The contents are
then squeezed into the cellular tissue, and this is followed by the
same favourable results as in the preceding method. Removal of such
tumours by dissection is unnecessary, and also attended with risk. I
have removed several large ones by incision; but the whole cyst can
seldom be taken away, and there is great risk of inflammation ensuing,
followed by sloughing of the tendons, or by rigidity of the part. From
my experience of the unfavourable consequences of incision, I should
not again adopt such a proceeding. Setons have been passed through the
swellings, but I cannot attest either their efficacy or their safety.
Exostoses of the phalanges of the fingers are rarely met with.
Sometimes bony enlargement occurs, involving many of the phalanges
along with several of the metacarpal bones. In such cases, both hands
are often similarly diseased, and other parts of the osseous system
also affected. When the tumour is limited to one or two fingers of one
hand, then, to get rid of the deformity and inconvenience, the patient
may desire its removal. The whole of the bone affected should be taken
away, lest the disease be reproduced.
Spina ventosa, acute or chronic, more frequently the latter, is
sometimes met with in the metacarpal bones, or in the phalanges. The
same treatment is applicable here, as that already detailed in regard
to similar affections of the lower jaw. Amputation above the tumour may
sometimes be necessary.
The hands of infants are sometimes found deformed, turned inwards,
as the feet are more frequently. Some of the carpal bones are
compressed, from the awkward position of the limb, but become properly
developed, if the parts are placed in their proper position as soon
as the deformity is observed, and kept so. But the displacement is
unmanageable if long neglected. Congenital deficiency of the fingers is
a deformity and inconvenience, but cannot be remedied. Adhesion of one
or more of the fingers, even to their points, is met with occasionally
as a congenital affection. Separation is readily accomplished; but
the dressing requires to be carefully attended to. Adhesions may
result from careless management of extensive abrasion or ulceration,
or from a burn, and such are not so easily remediable. Superfluities
may be abridged. Some children are born with two thumbs or two little
fingers; these have generally only a cutaneous attachment to the rest
of the hand, and that is easily divided by the knife or scissors. The
redundancy should properly be removed by the obstetrical practitioner,
as soon as it is observed.
The Bursa over the Olecranon Process is liable to enlargement, by
gradual accumulation of the secretion, in consequence of habitual403
pressure on the elbow. The contents are either serous or glairy,
usually the latter, and the swelling is indolent. But acute swelling
not unfrequently takes place in this situation, from external injury;
then the tumour is formed rapidly, there is heat and pain in the part,
and the integuments are discoloured around; in such cases the bursa
is filled with pure blood, or with a sero-purulent and bloody fluid.
Inflammation of the bursa often follows bruises and lacerated wounds,
and is apt to extend to the forearm and arm; causing extensive and
deep effusion, great tension of the parts, and severe constitutional
disturbance.
In the chronic cases of bursal enlargement, pressure is to be
avoided; and by the permanent application of an ammoniacal or of a
gum and mercurial plaster, absorption of the fluid may in general
be procured—the swelling disappearing as gradually as it arose. If
the collection is large and obstinate, repeated blistering may be
had recourse to; and if that fail, a seton may be passed through the
cavity. But the last-mentioned practice is sometimes followed by more
action than is desirable, inflammation of the surrounding cellular
tissue supervening, and abscesses forming, perhaps extensive. When the
collection is purulent, a free opening is to be made into the bursa,
and the case treated in other respects as a common abscess. If indolent
swelling of the cellular tissue, and spongy thickening of the synovial
surface of the bursa, remain after incision, the application of the
caustic potass may be required. In extensive and acute inflammation
spreading to the surrounding parts, free incisions are often necessary,
along with proper constitutional treatment, in order to prevent
destruction of the cellular tissue and skin.
Venesection, at the bend of the arm, is too often resorted to by
thoughtless or ill-educated practitioners, to the detriment of the
patient; as after accidents before reaction has occurred, in local
pains not inflammatory, &c. It is very often had recourse to by those
who have no correct ideas of the actions of the animal economy, who
have not within their heads a peg to hang an idea upon; or, if they
have, they are too lazy to think and to combine their ideas, so as
to come to a proper conclusion regarding what is the most proper and
judicious course to be pursued in any one case. They follow a routine,
and bleeding is too generally the commencement of it.
But venesection is absolutely required in many cases, and must often
be the principal dependence of the surgeon for removing or preventing
evil consequences. After injuries, when the circulation has been
restored, particularly when parts important to life are involved—in
the first stage of inflammatory attacks, with violent constitutional
disturbance—in inflammatory affection of vital or important organs—in
these, bleeding is employed to an extent sufficient to control the
action. But, even in such circumstances, the practitioner must be
cautious not to push depletion too far, but to stop short at the proper
time, so that the life of the patient may not be endangered, nor his
health impaired, more by the treatment than by the disease.
404
Venesection is usually practised on either the basilic or the cephalic
vein, or else on the median basilic or the median cephalic. The vein is
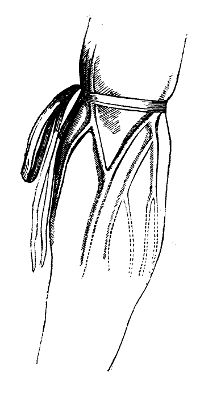 made to rise by obstructing the return of the blood by a ligature on
the arm, applied not so tight as to prevent the flow in the arterial
branches. A vessel removed from the inner side of the tendon of the
biceps,—that is to say, not over or near the brachial artery,—is to be
preferred. But sometimes none sufficiently large or distinct can be
perceived unless in that situation, and then great caution is necessary
in making the puncture; the patient’s arm must be held very steady,
and care taken that the instrument does not transfix the vein. The
branch chosen should also be fixed; one which rolls under the finger
is pierced with difficulty. The vessel is secured by the thumb of one
hand placed immediately below the point to be punctured, whilst the
lancet is held loosely betwixt the thumb and forefinger of the other;
and the surgeon should by practice acquire the use of either hand for
this and other minor operations, being thereby saved much trouble and
awkwardness. The right hand is used for the right arm of the patient,
the left for the left. The lancet should be in very good order, not
too spear-pointed, fine, and with a keen edge. The blade, placed at
right angles with the handle, and held lightly, as above mentioned, is
entered perpendicularly to the vessel. The puncture is made deep enough
to penetrate the vein, and then the edge is carried forward more than
the point, that the opening in the integuments may be more free than
that in the vein. The most convenient line of incision is obliquely
across. The pressure of the thumb is relaxed whenever a utensil is
conveniently placed for the reception of the blood; and the arm is
kept in the same position as during incision, that the openings in the
integument and vein may correspond. Unless this be attended to, the
skin will overlap the puncture in the vessel, and thus the stream will
be completely obstructed, or at least the blood will not come away so
smartly as at first. The blood may also cease to flow quickly from
over-tightness of the ligature, and from threatening of syncope; in
the former case the ligature is adjusted, in the latter the patient
is placed in the recumbent position. When the superficial veins are
emptied, the blood flowing by those deep-seated is to be directed to
the wound by muscular action; with this view the patient is made to
grasp the lancet-case, or any other solid body, in his hand, and turn
it round. If the opening in the integument is too small, the flow
gradually diminishes, and at length stops, in consequence of blood
being insinuated into the cellular tissue, coagulating, and so forming
what is termed a405 thrombus, which plugs the wound. When a sufficient
quantity has been obtained, the ligature on the arm is removed, and
pressure made below the wound. The integuments around are washed and
dried; and two or three small compresses of lint placed on the opening,
one above the other, are retained by a riband or narrow bandage,
applied in the form of the figure 8; the bandage should be so tight as
to prevent the escape of blood, without arresting the flow towards the
heart. The arm should be disused for a few hours; and after twenty-four
or thirty-six hours, the bandage may be removed, when the opening will
usually be found closed.
made to rise by obstructing the return of the blood by a ligature on
the arm, applied not so tight as to prevent the flow in the arterial
branches. A vessel removed from the inner side of the tendon of the
biceps,—that is to say, not over or near the brachial artery,—is to be
preferred. But sometimes none sufficiently large or distinct can be
perceived unless in that situation, and then great caution is necessary
in making the puncture; the patient’s arm must be held very steady,
and care taken that the instrument does not transfix the vein. The
branch chosen should also be fixed; one which rolls under the finger
is pierced with difficulty. The vessel is secured by the thumb of one
hand placed immediately below the point to be punctured, whilst the
lancet is held loosely betwixt the thumb and forefinger of the other;
and the surgeon should by practice acquire the use of either hand for
this and other minor operations, being thereby saved much trouble and
awkwardness. The right hand is used for the right arm of the patient,
the left for the left. The lancet should be in very good order, not
too spear-pointed, fine, and with a keen edge. The blade, placed at
right angles with the handle, and held lightly, as above mentioned, is
entered perpendicularly to the vessel. The puncture is made deep enough
to penetrate the vein, and then the edge is carried forward more than
the point, that the opening in the integuments may be more free than
that in the vein. The most convenient line of incision is obliquely
across. The pressure of the thumb is relaxed whenever a utensil is
conveniently placed for the reception of the blood; and the arm is
kept in the same position as during incision, that the openings in the
integument and vein may correspond. Unless this be attended to, the
skin will overlap the puncture in the vessel, and thus the stream will
be completely obstructed, or at least the blood will not come away so
smartly as at first. The blood may also cease to flow quickly from
over-tightness of the ligature, and from threatening of syncope; in
the former case the ligature is adjusted, in the latter the patient
is placed in the recumbent position. When the superficial veins are
emptied, the blood flowing by those deep-seated is to be directed to
the wound by muscular action; with this view the patient is made to
grasp the lancet-case, or any other solid body, in his hand, and turn
it round. If the opening in the integument is too small, the flow
gradually diminishes, and at length stops, in consequence of blood
being insinuated into the cellular tissue, coagulating, and so forming
what is termed a405 thrombus, which plugs the wound. When a sufficient
quantity has been obtained, the ligature on the arm is removed, and
pressure made below the wound. The integuments around are washed and
dried; and two or three small compresses of lint placed on the opening,
one above the other, are retained by a riband or narrow bandage,
applied in the form of the figure 8; the bandage should be so tight as
to prevent the escape of blood, without arresting the flow towards the
heart. The arm should be disused for a few hours; and after twenty-four
or thirty-six hours, the bandage may be removed, when the opening will
usually be found closed.
Besides puncture of the humoral artery, or of its branches, other
unpleasant circumstances may follow this little operation. The
thrombus—a small bloody tumour from infiltration into the cellular
tissue around the opening in the vein—proves troublesome, as already
remarked, by preventing the flow, and may render a fresh opening
necessary, either in the same arm or in the other. Afterwards it
generally disappears gradually by absorption; or the opening in the
integuments may not close, and the coagulum be separated and discharged
after some days.
Inflammation and abscess round the opening sometimes supervenes. It
is treated by fomentation, poultice, and rest, and the matter must
be evacuated by free incision. Inflammation of the surface, with
diffuse infiltration into the cellular tissue, is also met with after
venesection; the treatment of such an affection is the same as when it
occurs in other situations and circumstances.
The symptoms and consequences of inflammation of the vein have been
already detailed. The affection is attended with great pain, and with
swelling from effusion into the cellular tissue around the course of
the vessel; the integuments are inflamed and tense; sero-purulent
secretion soon takes place in the infiltrated cellular tissue, both
deep and subcutaneous, followed by sloughing, and separation of
the skin from its subjacent connexions; even death of the muscular
structure sometimes ensues—the pectoral muscles have been found black
and soft. The local treatment must be active. Incisions are made early
into tense parts to prevent internal mischief; and if the vein in the
neighbourhood of the wound be filled with pus, it should be laid open
freely. The evacuation of the matter affords great relief; afterwards
bread poultices or water-dressings are to be applied to the wounds,
the other parts should be assiduously fomented, and attention given to
the position of the limb. The bowels are to be attended to, and the
secretions promoted by mercurials with stimulants, as camphor with
calomel, or the hydrargyrum cum creta. When the tongue gets moist at
the edges, tonics and stimulants of a more permanent and powerful
action are necessary.
I have not witnessed any bad effects of venesection attributable to
puncture of the tendon or fascia, or to partial division of twigs of
the cutaneous nerves. In spasmodic or painful affections arising from
the latter cause, slight extension of the incision is recommended, so
as to divide entirely the injured branch.
Inflammatory tumour of the Mamma occurs generally during
lac406tation;44 and is attributable to injury, perhaps slight, during
the then excited state of the secreting vessels—to sudden exposure to
cold—to interruption to the flow of the secretion. It occurs, however,
independently of this state—sometimes at the age of puberty, during
the development of the gland—or at other periods of life, either
spontaneously, or in consequence of external violence. The last class
of cases are usually more severe than those first alluded to;407
some are more indolent than others; almost all are preceded by
shivering. There is swelling of the part, a sensation of weight in
it, and dull pain; then throbbing heat, and increase of suffering.
The surface is inflamed, and the nipple concealed by the tumescence.
The milk cannot be withdrawn. Fever attends, more or less violent.
Such tumours seldom if ever subside or are resolved; suppuration takes
place, and the matter generally comes to the surface at more than one
point. This abscess originates in the substance of the gland; but
collections occasionally form in the cellular tissue beneath the mamma,
either spontaneously, as in bad constitutions, or in consequence of
injury. In either case, and particularly in the latter, the swelling is
great, and the suppuration extensive; troublesome and tedious sinuses
remain unless early and free openings are made.
Leeching is of little use in mammary swelling during lactation; cold
and evaporating lotions seem to do harm by producing determination
from the surface to the deeper parts. The gland is to be kept as free
from secretion as possible, and supported by a handkerchief tied
round the neck; moderate diet should be enjoined, and laxatives given
occasionally. Fomentations are beneficial at first, but are superseded
by poultice when matter appears to have formed and to be making its
way to the surface. Two or more openings are generally necessary, to
afford free outlet to the matter; indeed, an incision is indicated
wherever the integuments are elevated, thin, and shining. Afterwards
poulticing is continued for some days, and succeeded by other suitable
applications. The discharge seldom ceases, so long as the secretion of
milk is encouraged.
Adolescent males are sometimes affected by troublesome fulness and
uneasiness of the mammillæ. Little or no treatment is required, the
inconvenience subsiding gradually and spontaneously.
Indolent enlargements of the mammary gland occur, though rarely. They
sometimes attain an immense size; and are often attributable to the
menstrual discharge having been inopportunely arrested. Such tumours
have, from their great bulk, required extirpation.
Sarcomatous tumours of various kinds are met with, either in
the cellular tissue under the mamma, or in the substance of the
gland—tumours not of the gland, though in it. Such are generally traced
to injury, as to a bruise by falling against the corner of a table
or chair, an accidental push from the elbow of another, &c. Simple
sarcoma is the most frequent formation; but I have encountered tumours,
thus situated, of a worse nature—reproduced, though freely and fully
removed; in fact, taken away along with the gland and neighbouring
adipose substance.
The gland itself is most frequently affected by carcinoma. Sometimes it
is attacked by, or involved in, medullary sarcoma; and bloody tumours
are also met with. In some cases, the gland is enlarged and softened,
and penetrated by cysts of greater or less size, and more or less
numerous, containing a fluid either serous, albuminous, bloody, or thin
and black.
The appearance and progress of carcinomatous and other tumours have
been already described. The mamma is more frequently the408 seat of
malignant disease than any other gland; it is frequently excited, and
much exposed to injury. Often the induration following abscess remains
stationary for several years, and at length takes on a new action,
forms morbid deposit, and is of rapid growth. The disease seldom occurs
in young subjects; though I have met with several well-marked cases
under thirty. Before that time of life, the tumour is generally of a
strumous nature, and this should not be confounded with the malignant;
for the one is remediable under the influence of constitutional means,
the other is not. Malignant disease is in most cases developed about
the period when the menstrual discharge ceases; when the discharge is
irregular previously to its entire cessation, the mamma is excited, and
then hardness is perceptible. The disease also forms, though seldom,
long after the “critical period,” but in such cases its progress is
usually slow. It occurs, also, and not unfrequently, in those who have
never had the mamma excited by lactation; the mammilla is also subject
to malignant disease in males advanced in life.
When the malignant nature of the disease is recognised, the tumour
should be extirpated without delay, before it has made much
progress—before it has contracted extensive adhesions, or contaminated
the lymphatics. The circumstances rendering interference unadvisable
have been fully spoken of when treating of tumours generally. If the
patient is a female, the period of the menstrual discharge, if still
regular, must be attended to, and avoided; indeed this maxim should
apply to every operation on the female. The most favourable time for
operating is some days after the cessation. The position of the patient
should be sitting, unless the dissection is expected to be tedious; but
it ought not to be so,—the extirpation of glands, or the detachment of
the tumour from parts to which it may have contracted firm adhesions,
can alone cause delay; and when these circumstances exist, interference
is not allowable. Any warrantable operation on the mamma can be
completed in a very few minutes. Two elliptical incisions are made from
the border of the pectoral muscle, in the direction of the fibres,
embracing the nipple and any portion of the integument which may be
adherent or altered. The surgeon need never hesitate to sacrifice the
nipple, for in this disease it can be of no further use; besides the
malignant action is apt to return in it when saved, it being almost
always adherent to the tumour: it must be removed. The incisions are
made quickly with either a scalpel, or a sharp-pointed and broad
bistoury; the lower should be the first, that the flow of blood may
not interfere with it and obscure its course. This is carried at once
through the skin and subjacent adipose tissue, and then the upper
is made rapidly, to get over the most painful part of the operation
as soon as possible. The dissection is next proceeded in, from the
axillary region forwards, and the tumour detached first on one side,
and then on the other. A few strokes of the knife will separate the
remaining cellular attachments to the fascia of the muscle, or of the
fascia to the muscle. The surface of the wound and of the extirpated
mass should be carefully examined, so that no part may remain whose
structure is altered.409 The vessels are tied; and after oozing has
ceased, if sufficient integument has been saved, the edges of the wound
are put together and retained. The patient is placed in bed, with the
head raised and the arm slung.
Operation is scarcely justifiable when it is evident that the
absorbents are affected. Yet a small glandular tumour on the border
of the axilla, without any enlargement more deeply seated, may be
removed along with the mamma. With this view, the incisions should
be made so as to include the tumour, and detach it previously to the
mamma being interfered with. But when swelling has taken place deep
in the axilla, it is impossible to ascertain its exact extent, and it
may be considered very certain that a chain of altered and enlarged
glands lie along the course of the axillary vessels. The whole of
such a tumour cannot be taken away, and, in removing even the more
prominent and accessible parts of it, there is great risk of wounding
the axillary vein. This blunder I have seen committed more than once,
and I have also seen the vein, the artery, and the majority of the
nerves, all included in one ligature in order to stop the bleeding. I
need scarcely add that the patients soon perished. When enlarged glands
are perceptible above the clavicle, or in the intercostal spaces, the
practitioner who would advise interference with the original tumour
must be grossly ignorant, or very unprincipled.
After removal of the mamma for carcinoma, in favourable circumstances,
some patients remain healthy. Those practitioners who do not recognise
the malignant disease, and operate for every tumour, and at all ages,
have boasted of great success. But it is not so with those of mature
experience. The disposition to malignant action often remains latent
for many months, sometimes for many years, and at length becomes
fully developed. The disease may return in the skin; the cicatrix
hardens, ulceration occurs, and makes progress. Or tubercles form in
the cellular tissue, enlarge, and involve the skin. Or the glands
become tender and swell; and the swelling is often unattended with
uneasiness. Œdema of the hand and forearm, to a great extent, may have
existed for a considerable time, and on examination extensive glandular
tumours are detected in the axilla and above the clavicle. These,
perhaps, ulcerate; or cough and hectic cut off the patient. In short,
permanent riddance from mammary carcinoma is scarcely to be expected by
operation, or any other means.
Neither are operations for medullary and bloody tumours of the mamma
more successful in their results; though I have certainly witnessed
permanent cures under unpromising circumstances,—when the tumours were
large, of long duration, and even ulcerated.
AFFECTIONS OF THE CHEST.
Inflammation of the pectoral serous tissue would come to be considered
more properly in a work exclusively on the practice of physic; but the
affection not unfrequently occurs in consequence of410 wounds or other
external injuries, and its terminations must be shortly noticed.
Effusion of serum may take place into the cavities, attended with
subsidence of the symptoms of pleuritis. In such circumstances, the
lung collapses, either entirely, or still admits a small quantity of
air; and, if the collection lodge for a considerable time, that side
of the chest enlarges. When the cavity is not quite full, the fluid is
heard to be troubled, and on motion of the trunk a sound of splashing
is perceived. Part of the cavity may be occupied with air which has
escaped from an opening in the lung; or halitus may be extricated
from the accumulated secretion. There are other signs, sufficiently
distinct, imparting a knowledge of such effusion. The previous history
of the case leads to a shrewd suspicion. The chest is unnaturally
immovable, as well as enlarged; the intercostal spaces are widened,
and ultimately protuberant; there is dulness on percussion, and no
respiratory murmur perceptible in those parts where there is fluid; the
sounds are natural in that part of the lung which is permeable to air,
and distended.
Suppuration often is the result of the incited action; and purulent
matter forms in the cavity of the pleura, generally without breach of
surface. The membrane is covered with lymph, more or less extensively
organised. Empyema is established. Suppuration may take place in the
substance of the lungs, and from ulceration the matter may escape, in
small quantity at a time, into the bronchial tubes, giving relief to
the patient; or it may be poured in profusely and suddenly, so as to
cause instant suffocation; or it may work its way into the cavity of
the pleura, and occupy the same place as if it had been secreted by
that membrane. Or, again, if the lung adhere to the costal pleura, the
matter may approach the surface of the body, by the aid of interstitial
absorption of the intervening parts, and the collection may then
be opened, like a common superficial abscess, by division of the
integuments only.
When the pleura is full, the chest enlarges, the integuments become
œdematous; and if, from the preceding and collateral circumstances,
no doubt exist of the presence of matter, paracentesis may be
performed with a chance of relieving and saving the patient. The
patient is placed horizontally, with the shoulders slightly elevated;
and the affected side should be as dependent as possible, that he
may be readily turned over on his face should the breathing become
embarrassed. The position of the diaphragm, in regard to the inner
surface of the false and lower true ribs, must be kept in view. When
the distention is great, this important muscle is displaced; it is
pushed downwards, carrying before it the viscera in the upper part
of the abdomen; it is thus removed far from the place at which the
incision is usually made. The point of election, as it is called, is
between the fifth and sixth ribs, and midway between the sternum and
the spine. An incision is made through the integuments, over the upper
edge of the sixth rib, an inch and a half in extent; in this situation
there is no risk of wounding the intercostal411 artery. If the operator
intend to shut the cavity as soon as the fluid has been discharged, the
integuments are drawn upwards previously to making the incision, in
order that they may afterwards overlap the wound. A cautious opening is
then made through the intercostal muscles, and the pleura punctured.
This is immediately followed by forcible ejection of fluid. The wound
of the pleura is then enlarged by a probe-pointed knife. The thrust of
a trocar, or sharp-pointed bistoury, is here inadmissible, as in some
cases the diaphragm, perhaps the liver or stomach, or even the lung,
might be wounded. The fluid at first escapes rapidly; afterwards it
is ejected chiefly during expiration. After its discharge, a tent is
placed in the wound, over which a compress is put, and the chest is
firmly bandaged. The closure cannot be maintained safely longer than
twenty-four hours; the dressing must be undone, the tent removed, and
the matter again allowed to flow. I would certainly not recommend any
attempt to heal the wound by the first intention. In consequence of
continued closure, the secretion soon becomes very profuse, mixed with
blood, and of a putrid nature; irritative fever is established. The
treatment principally consists in obtaining gradual, and at the same
time free, evacuation of the fluid, restraining the motions of the
chest, and supporting the general strength. As the discharge ceases,
the lung may in part expand; it may, however, continue collapsed,
become consolidated, and the chest fall in. In neglected cases,
absorption of the intercostal substance takes place; the integuments
bulge outwards, and distinct fluctuation is perceived. The skin has
been allowed to become thin, and even to give way, without the nature
of the case being known; but this can be the result only of ignorance
or of inattention. In such cases, the ribs have been denuded, and
become necrosed to a large extent,—the sequestra separating slowly
and in fragments; and causing long-continued and wasting discharge.
It is plain, therefore, that pointing of the matter should never be
waited for. Chronic collections are occasionally met with of some
years’ duration, and producing great enlargement of the chest. Surgical
interference with such is less likely to prove beneficial than with the
acute.
Wounds of the large bloodvessels of the chest, or of the cavities of
the heart, are almost immediately fatal. Mere punctures, however,
of these parts, have closed for a time, and in some cases even
permanently. All wounds of the chest, though not involving bloodvessels
of a large size, are productive of severe consequences—effusion of
blood or bloody fluids into the cavities, escape of air into the
external cellular tissue, collapse of the lung, and inflammation and
its results, are always to be dreaded. The danger is not uniformly
tantamount to the extent of injury inflicted. Individuals have
recovered from extensive wounds causing profuse hemorrhage, and great
displacement and laceration of the parts; whilst, from much slighter
injuries, untoward and fatal consequences have quickly resulted.
Wounds may penetrate the chest, and be continued into the abdomen;
the stomach, liver, and intestines—one or all—may412 be perforated as
well as the lung; in such cases the hemorrhage is in general speedily
fatal. Injury of the intercostal arteries, and of the mammary and its
branches, is attended with serious bleeding. It is easily arrested,
however, by pressure. A piece of fine linen is pushed into the wound,
followed by charpie, so as to form a small bag within the chest, a
little larger than the opening; by pulling this gently outwards and
fixing it, efficient pressure is made on the bleeding vessel. At the
same time the motions of the chest are to be restrained by bandaging;
indeed this is necessary in almost all injuries of that part. When
reaction has been established, antiphlogistic treatment must be
pursued, and it generally requires to be extremely active. Bloody,
serous, or purulent fluids, lodging in the cavity of the pleura, are
to be evacuated, if need be, either by incision or by enlargement of
the original wound. In the course of the cure hectic usually supervenes
to a greater or less degree, and requires the reverse of the previous
treatment.
AFFECTIONS OF THE ABDOMEN.
Inflammation of the peritoneum, when idiopathic, is generally treated
by the physician. But it occurs in consequence of wound, obstruction
from hernia, or affection of the lower bowels. There is a burning heat
in the belly; the pain is constant and increasing, much aggravated
by the slightest pressure or exertion of the abdominal muscles, and
the patient, in consequence, lies with these muscles in a state of
relaxation. The pain is of a very different character from that
arising from spasm, induced by the irritating nature of the intestinal
contents, which supervenes in paroxysms, and is relieved by pressure
or by evacuation. In inflammation the countenance is very anxious, and
generally pale; the extremities are cold and bathed in perspiration;
the patient vomits frequently; and the bowels are generally
constipated. The pulse is small, wiry, and rapid.
Hernia has been classed with tumours. It is a swelling, but of a
peculiar kind, and attended in some states by peculiar symptoms. The
term rupture is in common use instead of hernia, but was at first
applied from a false notion of the disease. There is a descent of
viscera, but not often rupture of the parietes. By hernia is meant
protrusion or escape of the contents of any cavity, but the term is
most frequently applied in regard to the abdomen. The protrusion
may occur at various parts of the abdomen; through the diaphragm,
constituting Phrenic Hernia; through the umbilicus, constituting
Exomphalos; through the dilated apertures for transmission of
vessels, constituting Ventral Hernia; through the inguinal canal,
constituting Inguinal Hernia; through the crural aperture,
constituting Crural or Femoral Hernia. The most frequent forms
are the inguinal and crural,—the effects of pressure or action of the
muscles on the413 abdominal contents being concentrated towards the lower
part of the cavity. It is but rarely that the bowels protrude through
the sacro-ischiatic notch, or through the obturator foramen, or by the
side of the vagina, or betwixt the bladder and rectum.
It is of great importance for the student to study attentively and
reflect on both the healthy and morbid anatomy of this disease. When
a hernia is strangulated, there is an absolute necessity for early
interference; the bowels are obstructed, and their action inverted;
feculent vomiting ensues, and enteritis is threatened, with all its
dangerous consequences. He may meet with the affection at a very
early period of his practice, and may be so situated as to command
no assistance or advice; he must be guided by his own judgment and
knowledge. He should be well aware of the relations of the parts
to each other, and the changes likely to have been occasioned by
the disease. If, through delay, the patient lose his life, or if an
operation be attempted, and its object improperly accomplished, or
not accomplished at all, his reputation may be blasted. But if he
interferes skilfully, and at the proper time, and save his patient,
relieving him at once from all his painful and dreadful symptoms,
great credit and professional fame may be in consequence acquired. An
examination of the healthy anatomy is not sufficient; many changes
take place, which mere anatomical and physiological knowledge could
never anticipate. Extraordinary displacements and adhesions occur. The
parts are altogether changed; and repeated examination of the morbid
state alone can impart the requisite knowledge to one previously well
acquainted with the healthy structure.
In consequence of laceration or separation of fibres, hernia may
occur suddenly, and even in the best formed parts, from very violent
exertion—as in leaping, wrestling, pulling, lifting heavy weights;
from sudden exertion of the abdominal muscles in any way; from blows,
&c. Or the protrusion may come on gradually, after slight exertions,
where the tendons are naturally weak or deficient; or it may be
slowly induced by repeated and almost constant muscular action, as in
urinary, intestinal, and pulmonary complaints: in such cases, slight
pain is usually felt at the site of the protrusion before the tumour
is perceived. The disease is often congenital. But the common cause
of abdominal hernia is powerful action of the abdominal muscles,
compressing the viscera to a greater or less degree, and with more or
less suddenness; the viscera resisting the compressing force, react on
the parietes, and these, yielding at the points which are naturally
weak or deficient, permit enlargement of the coerced cavity by
protrusion of part of the contents. When the compression and reaction
are sudden and violent, the protrusion is the same; but when the former
are not sufficient to overcome the cohesion of the parietes by a single
occurrence, by repetition the morbid end is gradually effected, the
hernia is proportionally slow in making its appearance, and gradual in
its increase.
To understand the nature of congenital scrotal hernia, the student
must recollect that the testicle in the fœtus is lodged in the cavity414
of the abdomen immediately below the kidneys, and resting on the psoas
muscle; that it gradually descends into a process of peritoneum,
called spermatic, which extends from the general peritoneal cavity
down towards the scrotum, and which ultimately constitutes the tunica
vaginalis. The orifice of this peritoneal pouch not closing immediately
after the descent, may permit a fold of intestine to slip into its
cavity, and remain in contact with the testicle. Or the testicle may,
though rarely, contract in the abdomen an adhesion to a portion of
bowel, and in its descent bring this along with it. In either case the
bowel remain in its new situation, and constitutes congenital hernia.
Hernia infantilis differs from the hernia congenita, and is a kind of
protrusion peculiar to the early period of infancy. In the congenital
form the protruded intestine is in immediate contact with the testicle,
and surrounded by the tunica vaginalis testis; but in hernia infantilis
a process of peritoneum is interposed betwixt the intestine and the
vaginal coat. The affection occurs after the abdominal aperture of the
spermatic process has closed, but before the rest of that process has
become incorporated with the spermatic vessels and their surrounding
cellular tissue. In fact, only the peritoneum proper has closed, and
forms the septum between the cavities of the abdomen and of the tunica
vaginalis; but being insufficient to withstand the impulse of the
abdominal contents, yields before it, and descending along with the
protruding portion of bowel, forms its envelope, or the proper hernial
sac, within the cavity of the tunica vaginalis.
Such is the opinion generally adopted in regard to the nature of hernia
infantilis; but its accuracy is doubtful. It seems more probable that
the bowel, covered by a fold of peritoneum, is protruded into the
cellular tissue of the spermatic chord, after closure and contraction
of the spermatic process, and descending till it reach the upper and
posterior part of the tunica vaginalis, adheres to this tunic, bulges
it forwards, and is covered by it. On cutting down in such a case, the
hernial tumour may appear to be lodged within the tunica vaginalis;
whereas the bowel is actually placed exterior to the tunic and behind
it. Indeed, the case is similar to the common scrotal hernia, only the
tumour is behind, not anterior to the vaginal coat. And this relation
of parts is more apt to occur in the infant than in the adult; for in
the former the testicle does not for some time descend fully into the
scrotum, and whilst it is lodged in the groin a fold of peritoneum
protruded into the spermatic chord may soon contract adhesion with
the tunica vaginalis, afterwards descending along with it and the
testicle. The subjoined case, illustrative of the preceding statement,
came under my observation in 1814.—J. S., æt. 21, was admitted into
the Royal Infirmary, with symptoms of strangulation which had been of
eight days’ duration. The hernia had existed from infancy; it was on
the right side, and tolerably large. In the operation, on dividing the
integuments and various coverings, a sac was opened, which proved to be
the tunica vagi415nalis, containing the testicle, a considerable quantity
of serum, and a large, smooth, transparent tumour above the testicle
and behind the posterior layer of the tunica vaginalis. The operator
was puzzled, but finally determined on cutting into this tumour;
it proved to be the hernial sac, covered by the tunica vaginalis,
containing three or four ounces of serum and a portion of omentum. The
protrusion could not be returned; after relieving the stricture, the
omentum was cut away, and the bleeding vessels tied separately. The
patient died on the third day after. An analogous case is on record;
and a third has been related to me by an old and experienced surgeon:
in that instance, both the anterior and posterior layer of the tunica
vaginalis, together with the true sac, were simultaneously divided;
omentum and intestine protruded into the vaginal coat, and for a time
the opening through the posterior part of that cavity and sac was
mistaken for the inguinal ring. On extension of the incision, the
nature of the case became more apparent, the stricture was relieved,
and the protrusion reduced. A case, in many respects similar to those
above described, occurred a few years ago in my practice at the North
London Hospital. It is recorded in the Lancet and in the Practical
Surgery.
Children are sometimes born with deficiency of the umbilicus, and
protrusion of bowel into the loose cellular tissue of the umbilical
chord; the disease is termed congenital exomphalos.
Almost all the viscera of the abdomen and pelvis are liable to
protrusion—the stomach—the spleen—the omentum—the great and small
intestines, and even some of their most fixed parts—the ovaria—the
bladder. Also, right portions of the viscera occasionally escape on the
left side of the parietes, and the left at the right.
Hernial protrusion has received different names, according to the
nature of its contents. When composed of a portion of intestine, it
is termed Enterocele; Epiplocele, when composed of omentum; and
Entero-epiplocele, when both intestine and omentum have escaped; and,
as already observed, different names are also applied, according to the
situation of the protrusion.
The inguinal and crural forms of hernia being the most common, will
chiefly occupy our attention. The inguinal is divided into true or
oblique inguinal, and into direct or ventro-inguinal. In the
oblique, the protrusion passes along the inguinal canal. This course
is in young persons short; but as the muscles become developed it is
lengthened to about two inches, reckoning from the external ring to
the funnel-like opening through the transverse fascia. The appearance
of the swelling in this canal leads to diagnosis betwixt the oblique
and direct hernia; but in chronic cases, this distinction is often
in a great measure done away with. In large and old oblique ruptures
the neck of the tumour is shortened, and the openings of the canal
are approximated and more in a direct line. They are also immensely
dilated, being often enlarged to such an extent as to admit all the
fingers of the hand, when placed in a conical form,—and this even in
the living body, the loose integument receding along416 with the tumour.
The epigastric artery is situated behind the neck of the sac, on its
inner side; and it is much displaced inwards in cases of old standing.
The direct hernia passes through the parietes opposite to the external
ring, and does not come in contact with the spermatic chord until it
has reached that point. Its neck is short, and the epigastric artery
is on its outer side. The coverings of the two tumours are different.
Those of the oblique are such as the chord possesses—a prolongation of
the transverse fascia, a covering from the cremaster muscle, fibres
from the edge of the external ring, and the superficial fascia of the
abdomen. The direct has only the last. A very old woman was operated
upon in the North London Hospital a few days ago, for strangulated
hernia of several days standing. The tumour was high in the inguinal
region: on cutting down upon it, the tendon of the external oblique
was found to cover it completely. The external ring was occupied
by a mass of fatty matter, which probably had been displaced. The
tendon was divided, and the sac, of considerable size, exposed. The
opening through which the protrusion had taken place was very small,
and situated a good deal to the mesial line of the internal aperture
of the canal. The hernia was at the time of operation supposed to be
ventro-inguinal. The patient was relieved for a time, but eventually
sunk exhausted. An opportunity was thus unfortunately afforded of
verifying the opinion formed. The hernia had two proper coverings, the
superficial abdominal fascia and the tendon of the external oblique.
The opening was inside the epigastric. The portion of bowel which had
been extruded and returned was very tender, but it had adhered to the
peritoneum, close to the place where it had been confined.
The oblique inguinal, when recent and small, is termed Bubonocele; but
when large, it generally descends into the scrotum—oscheocele—of course
exterior to the tunica vaginalis; and in females into the labium. The
tumour often attains an immense size, from continued application of the
causes that produced it,—laborious occupations, or straining of muscles
in any way. When of long duration, and not attended to, it is not
uncommon for the swelling to hang as low as the middle of the thigh, or
even down to the knee. In such cases, the testicles often are wasted,
and the penis concealed; indeed the skin of the penis, as well as of
the lower part of the abdomen, is stretched over the tumour. Crural or
femoral hernia is, on the contrary, seldom larger than a small apple.
Sometimes, but very rarely, the tumour is of large dimensions. I have
seen one containing the transverse arch of the colon, the omentum, and
a yard and a half of small intestine. The tumour is represented some
pages further on.
When a very large hernia remains always full, the cavity of the abdomen
diminishes in size; in fact, it adapts itself to its contents; and this
must be kept in mind when interfering with such cases.
Inguinal hernia most frequently occurs in males, the femoral in
females; and the reason of this is obvious on comparing the size
of417 the inguinal and crural openings in the sexes. In the male, the
inguinal opening is much larger than the femoral; in the female, the
femoral is the larger,—the inguinal is small, containing only the
round ligament of the uterus. The causes of hernia act equally on both
openings, and therefore it is to be expected that protrusion will take
place where there is the least resistance, where the parietes are most
deficient.
Hernia can seldom be mistaken for any other swelling, by one at
all acquainted with his profession, and who makes his examination
attentively. The history, and the mode of its appearance, are to be
attended to. The swelling proceeds from above—at times it recedes on
the patient lying on his back and making pressure on the swelling—a
distinct impulse is communicated to it on exertion of the abdominal
muscles, as in coughing—the tumour is generally elastic, and its neck
can be felt extending from the lower abdominal aperture. Also, the two
kinds, inguinal and crural, can scarcely be confounded with each other;
the former is above, the latter below, the ligament of Poupart. It will
be proper, however, to enumerate shortly the diseases for which hernia
may be mistaken.
Cirsocele may be confounded with inguinal hernia. Cirsocele, being a
varix of the spermatic veins, enlarges on coughing and during the erect
posture, like hernia; but in general the composition of the tumour
can be ascertained by the feel which it imparts when handled,—the
veins feel like a handful of earth-worms. Besides, the swelling is
made to disappear, on emptying the dilated veins by pressure upwards;
and, if the surgeon then firmly compress the inguinal aperture, the
tumour will rapidly reappear, on account of the venous flow being
interrupted, particularly if the patient exert his abdominal muscles,
or assume the erect posture. Whereas, had hernia existed, the swelling
could not have been reproduced; and, on the patient being directed
to cough, a distinct impulse would have been felt with the finger.
Hydrocele of the tunica vaginalis may be confounded with scrotal
hernia, if its distinctive characters be not understood or attended
to. The pyramidal swelling presents an equal surface, fluctuates, and
is generally diaphanous; its formation is gradual, commencing at the
lower part, and slowly ascending; the testicle cannot be readily felt
at the bottom of the scrotum; there is no swelling at the inguinal
canal, and the chord is felt free; the tumour is not affected by the
position, motion, or exertions of the patient. These circumstances
plainly indicate the nature of the case. Bubo, sarcocele, and acute
swelling of the testicle, are sufficiently distinguished from hernia
by their situation, form, feel, and history, and cannot be confounded
with it save by the profoundly ignorant. Hydrocele of the spermatic
chord is more likely to lead to deception when large; but it is
generally small and circumscribed, involving the middle of the chord,
leaving the inguinal aperture free, and the upper part of the spermatic
chord distinct. Besides, whatever may be its size, its formation is
always slow and indolent,—it is never capable of being pushed into the
abdomen, and it is unaffected by those circumstances418 which contribute
to mark hernia. But hydrocele of the chord and hernia may coexist, as
in the following instance:—A gentleman had swelling in the course of
the spermatic chord for many years, while in a warm climate. Bandages
were applied, and great pain thereby occasioned. After his return to
this country, pain in the belly and vomiting seized him on a Monday
morning, and continued with more or less violence till the Sunday
following. Then the vomiting became feculent, the belly excruciatingly
painful and tender, the tumour tense, and the pulse weak. A physician
opposed operative measures, having been convinced that his former
complaint was a hydrocele of the chord. But I conceived that the
symptoms warranted cutting down on the parts, and did so. A hernia was
found containing omentum and a fold of bowel; a hydrocele of the chord
lay alongside of it.
Crural hernia has been mistaken for bubo, and vice versâ. Lumbar
abscess and varix of the femoral vein are also supposed to resemble it
in some measure. The situation and form of the tumour in lumbar abscess
is very different from those of hernia; and the mode of examination
recommended in regard to cirsocele is equally applicable to the
detection of dilated femoral vein. The distinctions between crural
hernia and bubo are too obvious to require mention.
Patients with unreduced hernia are constantly in great danger; as
bruising of the swelling, or accumulation of feces in the protruded
bowel, are likely to occasion very unpleasant consequences. They are
generally troubled with indigestion, flatulence, and constipation; a
slight degree of constriction at the neck of the tumour produces an
obstruction to the intestinal contents; the viscera in the sac have not
due support and pressure, hence accumulations take place in them, and
may be productive of serious and even fatal effects. No protrusion,
in which these circumstances are likely to occur, should be allowed
to exist, if possible. So afraid were the ancients of allowing hernia
to remain unreduced, that it was their custom to cut all patients
labouring under rupture who would submit to the operation; and this was
generally performed by itinerant quacks. They returned the protrusion
without opening the sac, and then the neck of the tumour was either
stitched up, or tied along with or without the spermatic chord. The
actual cautery, and the most powerful caustics, were also applied
to the parts by some, and dreadful were the effects; yet after the
neck of the sac had been destroyed, and perhaps the bone exposed and
exfoliated, protrusion again took place by the side of the cicatrix.
By many, castration was considered necessary for the cure of scrotal
hernia. Such harsh measures were founded on erroneous and imperfect
ideas of the nature of the disease, which are not often to be met
with in the present day. Operations for unincarcerated hernia are not
justifiable, and those who have operated in such circumstances give a
very unfavourable account of the experiment.
The external applications employed to reduce hernia are various.
Some are supposed to produce corrugation of the integuments, and419
contraction of the cremaster muscle, and thereby to force up the
protruded intestine; others are of an astringent character, and their
administrator may gravely believe and say, that by them he expects
to tan the living scrotum, to reduce the hernia, and to present an
insuperable obstacle to its reproduction. But all such means are
visionary, and practically ineffectual; no external or internal remedy
can attenuate and reduce the hernial sac, remove adhesion, or produce
contraction of the tendinous and rigid apertures.
Herniæ are either reducible or irreducible. A hernia is said to
be reducible, when the protruded bowel or viscus readily returns into
the abdomen on the application of pressure to the swelling, or on the
patient assuming the recumbent posture. When recent, the swelling may
not be made to disappear without considerable difficulty; but, after
the disease has become of long duration, the aperture through which
the protrusion has taken place dilates and is relaxed, and admits of
the ready passage of the hernial contents: such tumours are usually
of considerable size. But reducible herniæ should not be permitted to
enlarge, since their protrusion can be prevented by simple and safe
means; after reduction, a properly fitted bandage, termed a Truss,
is applied over the aperture and canal, and by the compression thus
made the opening is rendered impervious to the abdominal viscera. In
inguinal hernia, the pad of the truss must make equable compression
over the whole of the canal; in the other species, the aperture is less
extensive, and the pressure more direct. Perseverance in the use of
a well-adapted truss is highly necessary in children from the first,
so that a chance may be afforded of permanent cure by contraction of
the opening and development of the surrounding parts. In young persons
the canal is short, and almost direct, and from its becoming oblique
and elongated during growth, prevention of protrusion may be effected.
Descent must never be allowed during such attempts at cure. But in
adults such a fortunate result can scarcely be expected; the truss
must be constantly worn during the day—in bed it may be disused—and
the patient must rest satisfied with thereby escaping those dangers to
which protrusion of the hernia would render him always liable. Great
care should be taken to ascertain in the morning, before the truss is
applied, that no protrusion exists. If the opening be not much dilated,
it may contract even in adults when protrusion is sedulously prevented.
The patient will also require to avoid the causes of hernia. If he is
subject to cough, or labours under bad urinary disease, by which the
abdominal muscles are called frequently and fully into action, there
is no chance of a cure; nothing but the continued use of a truss will
afford safety.
Hernia is rendered irreducible, 1. By the formation of adhesions
between the sac and the included parts. 2. By induration of the
protruded omentum, and by accumulation of fat in it, or in the
appendiculæ of protruded large intestine. 3. By contraction of the
abdominal cavity from long-continued displacement of a large portion of
its contents. 4. By the nature and connexions of the protruded part,
as in hernia of the sigmoid flexure, or of the caput cœcum coli.420 5.
By firm compression of the abdomen. 6. By the tightness of the opening
giving rise to engorgement of the protruded parts. 7. By accumulation
of feces, solid or fluid, in the protruded portion of bowel. With
care, some of these causes may be got over, and the tumour reduced.
In irreducible hernia the use of a bag truss is indispensable to
prevent increase of the protrusion. In irreducible femoral hernia of
small size, a hollow pad with a weak spring is used with advantage,
to give support to the contained parts, prevent farther protrusion,
and guard the tumour against external violence. The patient must avoid
violent exertion, keep his bowels open, and be careful of his diet; he
is always in danger, and should know it. Many have lost their lives
from blows otherwise not dangerous; and even straining at stool is
sufficient to force additional portions of viscera into the neck of
the sac, and thereby induce most serious distress. Ruptures often come
down during an attack of bowel complaint, or after a dose of purgative
medicine.
The term incarceration of hernia is employed to indicate a slight
degree of strangulation, when the hernial contents are confined from
any cause, and when the circulation in the protruded bowel and the
course of the feculent matter are nevertheless uninterrupted. By many
it is applied indiscriminately with strangulation.
Strangulation arises, not from any change in the neck of the sac or
in the tendinous aperture, but from increase of volume in the protruded
parts, caused by accumulation of the solid, fluid, or gaseous contents
of the bowel, followed by interruption to its circulation; or the
interruption to the flow of blood may precede the distension. The
circulation is more readily retarded or arrested in the veins than in
the arteries, and consequently the engorgement of the bowel is at first
caused by venous turgescence; but when the flow in the arteries is at
all impeded, the infiltration and exudation become more rapid, and the
part quickly perishes—sphacelates. The symptoms which accompany and
indicate strangulation are of a very imposing nature, and cannot be
neglected; and it is fortunate that such is the case, for no disease
is fraught with greater or more immediate danger to the patient, or
requires more the early interference of a skilful and expert surgeon.
The tumour becomes tense and painful, and the integument is sometimes
red and shining; the pain is much increased by pressure, and extends
over the abdomen, but continues most severe near the neck of the
swelling; sickness and inclination to vomit quickly follow; the patient
feels languid; his countenance soon assumes a contracted anxious
appearance; the circulation is hurried; the pulse beats wiry and hard,
though at first it may have been full. If relief is not afforded,
all the symptoms are speedily aggravated; vomiting comes on, and is
frequent; no discharge can be procured from the upper bowels, though
the lower may be, and often are, evacuated by injections or by natural
efforts: if the upper bowels evacuate downwards, the strangulation
cannot be of the whole calibre of the gut, but only of a part. Pain
and heat in the tumour and belly increase; and the former becomes very
tender, and tense as a drum.421 The circulation is more hurried, and
restlessness and intolerable anxiety supervene. The patient becomes
worse and worse every hour; feculent matter in large quantity is
vomited or gulped up with great distress, and is commixed with bile,
with vitiated mucous secretion from the stomach and bowels, and with
whatever may have been recently swallowed; in fact, the peristaltic
action of the alimentary canal above the strangulated part is inverted,
and all the contents are ejected. Troublesome hiccough comes on, and
this symptom is by many considered as a sure sign of gangrene having
taken place; but it is often present when the bowels are quite free
from tenderness or tendency to gangrene. The extremities grow coldish;
the pulse is unequal and fluttering, and with difficulty counted at
the ankles. The countenance sinks, and assumes a leaden hue; the pain
abates suddenly; the eyes are glassy; the tumour becomes flaccid,
and is often livid and emphysematous. Now, the bowel may recede, and
feculent evacuation take place, with some relief; but the patient,
after lying some time insensible, expires. All this may occur, either
within a few days after the occurrence of strangulation, or not till
after the expiration of many days. The rapidity of the symptoms and the
danger are influenced by the size of the tumour and the condition of
its neck, and by the nature of its contents. In small recent herniæ,
the advance from bad to worse is usually very rapid, the aperture
through which protrusion has taken place being small, and producing a
great degree of constriction when distension and engorgement occur.
When the neck of the tumour is large, and completely occupies the
aperture previously to the strangulation, the progress of the symptoms
is also rapid, for a similar reason; but if the hernia be large and
of long standing, and if the protruded parts are not bulky at the
point of protrusion, the constriction is in general not very severe,
and the distressing consequences advance more slowly. The symptoms
are not so violent in epiplocele as in enterocele. In many instances
of the former, the intestinal discharges are never obstructed, though
great irritation and inflammation may be induced by the strangulation.
There is also less danger in entero-epiplocele than in enterocele,
compression of the bowel being in the former instance diminished by the
intervening omentum.
It is scarcely necessary to observe, that, when the train of symptoms
just detailed commences in any case, the surgeon must immediately and
anxiously inquire as to the existence of external hernia, for often
the disease is concealed, particularly by females: all parts where
protrusion is likely to occur must be examined attentively. At the same
time, the surgeon must bear in mind that pain of the abdomen, with
symptoms resembling those of strangulation—in fact, that enteritis,
with obstruction, may exist along with hernia, but independent of
it. A person with hernia is as liable as any other, if not more so,
to inflammatory attacks in the abdomen from a variety of causes. The
portion of bowel in the tumour may participate or not in the general
abdominal affection; if unaffected, it may be reduced; it is neither
painful nor tense. Again, in large ruptures, inflammation of the
contents may take place without strangulation, and without422 affection
of the parts within the abdomen. All circumstances bearing on the case
must be well considered by the surgeon, before making up his mind as to
the nature of the affection.
Returning the contents of the hernia into the abdomen is the only
effectual means of counteracting the direful effects of strangulation;
and the propriety of an early recourse to this measure must be quite
apparent. It is indispensable, and no delay is warrantable. The
means for accomplishing it must be varied, according to the state of
the parts, the duration of strangulation, and the general symptoms.
The most simple method, and that which should first be attempted in
ordinary cases, is the taxis; that is, reduction by pressure with
the hand. In this, the position of the patient is of importance; it
should be such as effects relaxation of the tendinous structures
through which the hernia has protruded, and through which it is to be
returned. With this view he is placed on his back, with the shoulders
and pelvis elevated, and in crural hernia the thigh is bent on the
trunk, and turned towards the opposite side; thus the aperture is
relaxed along with the fasciæ which compose it. Long ago, the positions
into which the patients were forced for the cure of hernia were
various, and generally awkward; they all tended towards more or less
complete inversion of the erect posture, and thus it was supposed that
the abdominal bowels dragged on those protruded, and thereby assisted
reduction. But the viscera are equally pressed on in every position of
the body; it is not they, but the external parts, that are affected by
change of posture. During the attempts at reduction, the patient should
be exhorted not to strain or resist, but to relax his muscles; and it
will be well to engage him in conversation, that he may not have an
opportunity of keeping his lungs distended, and thereby acting forcibly
on the abdomen. At first the pressure should be general, applied either
with one hand or with both, according to the size of the tumour, so as
to diminish the contents. If air be heard gurgling at the neck of the
swelling, the chance of success may be considered good, for a return
of part of the bowel’s contents is thereby indicated. Then a gentle
kneading should be made at the neck with the fingers of one hand, while
with the other general pressure is kept up. The impression made is at
first slight and gradual; but, when a portion of the bowel returns, the
rest of it slips up suddenly. The return of omentum is always slow, and
the last part requires as much manipulation as the first. The direction
of the pressure must be varied according to the case. In inguinal and
ventro-inguinal hernia, it is made in the direction of the neck of the
sac; in the former upwards and outwards, in the latter upwards and
backwards; and previously the body of the tumour should be brought
into the same line with its neck. In crural hernia the pressure must
first be made towards the centre of the thigh, so as to bring the whole
tumour into the same direction with its neck, and then upwards. In
umbilical, the pressure is straight backwards. Small herniæ, and those
of recent origin, are with difficulty reduced; their neck is narrow,
and the passage proportionately small; the crural are usually of this
description. In all herniæ, after strangulation has existed for some423
time, and adhesions formed, particularly at the neck, reduction is
almost impossible.
The taxis is to be neither attempted nor persevered in after the
hernia has become tender and inflamed. No good can be done by it, and
the patient’s chance of recovery by operation is much diminished.
Even when no pain is felt in such circumstances, any degree of force
must be prejudicial. Mortification of the bowels is often hastened in
consequence of the taxis being unskilfully employed by ill-informed
persons, who are often determined, at all risks, and at all stages
of the affection, to accomplish speedy reduction of the viscera. The
surgeon will take care to inform himself of all particulars—as to the
duration of strangulation, the previous state of the tumour, if it was
all, or only in part reducible, as to its size, &c.—before proceeding
in any way. Great mischief is likely to accrue from the tumour being
handled, perhaps roughly, by many people. If the taxis is gone about,
however, in proper time, and in the right way, it ought almost always
to prove successful. It is very desirable indeed that this should
be the case, seeing that all the bad symptoms in ninety-nine out of
a hundred cases instantly subside; whereas, after the reduction by
incision, there is always great risk from the opening of the peritoneal
sac alone.
Certain means may assist the taxis, but they should not be long
continued or often repeated. Venesection can be employed only in
strong plethoric patients, in the very first stage of strangulation,
and before the patient is exhausted by the distressing symptoms. It
is had recourse to in order to induce syncope, or an approach to it;
during which general relaxation takes place, and reduction may be
attempted with advantage. With that view the patient is placed erect,
and a large orifice made in the vein of one or both arms, so that a
moderate quantity of blood suddenly abstracted may have a powerful
effect on the system. In several cases I have found this practice
beneficial, but am inclined to say that, in general, it will not be
followed with success. In a favourable case, one attempt of this kind
may be made, but not repeated. In many states of the constitution, and
in the latter stages of the disease, bad consequences must follow the
practice. But in regard to it or any other remedy, it would be folly
to lay down positive general rules; what may prove useful in one or
two instances may answer very badly in the majority of cases that come
under treatment. Local bloodletting can have no effect in diminishing
the size of strangulated parts; though in inflammation of the contents
of the tumour, without strangulation, no more powerful means can be
employed.
Purgatives have been recommended with the view of extricating the bowel
by increased peristaltic motion; but the symptoms will, to a certainty,
be aggravated by their use. Purgative enemata can do little good: if in
small quantity, they empty only the rectum; if large, they may reach
the strangulated part, but will scarcely have the effect of extricating
it.
Emetics, in full or nauseating doses, have been supposed to be
indicated in this affection as well as in ileus; but there is in
general424 enough of sickness and vomiting without them, and it is often
difficult enough to allay the vomiting even after removal of the
obstruction.
The warm bath is greatly trusted in by some, and in many cases
it proves a valuable and useful auxiliary to the taxis. It acts
beneficially by inducing general relaxation, or even syncope; during
which, whilst all resistance of the compressing powers upon the
contents is suspended, pressure on the tumour can be employed to good
advantage. By steady perseverance, whilst the patient is in the bath, a
great majority of strangulated herniæ may be reduced. But neither the
general nor the local application of heat, or any other known means,
save the edge of the knife, can relax tendinous apertures farther
than can be effected by attention to position. Irrecoverable and most
precious time may be wasted in preparing the bath; and for this reason
such means should never be resorted to, unless they can be commanded at
the shortest notice.
Fomentation can do no good. The apertures can be neither relaxed
by heat, nor contracted by astringent applications. By the local
application of heat, the size of the parts composing the hernia will be
augmented, the flatus being rarified, and the effusion and engorgement
encouraged.
The cold bath, and the dashing of cold water on the surface, near the
seat of the disease, have been tried in some rare cases with most
marked success; but this is a practice not generally to be relied
on. It can act only by producing sudden and powerful contraction of
the coverings, and uniform pressure thereby on the contents. It is,
perhaps, only applicable to scrotal hernia. Cold has been applied to
the tumour, and even ice, so as to produce frost-bite, but little
faith can be placed in such; the practice becomes dangerous after
inflammation has existed for some time, the application diminishing the
weakened powers of the parts, and accelerating gangrene.
Opium has been given by the mouth, and tobacco by the lower extremity
of the alimentary canal; the former may sometimes prove advantageous,
but the latter had better be dispensed with. The tobacco is thrown up
either as an enema, or in the form of vapour; but the former method is
generally preferred. A drachm of the leaves is infused in a pound of
water for ten minutes, and one-half of the liquid injected; if this
prove insufficient to prostrate the patient, the rest is administered
after the lapse of a short interval. But many people have thus been
poisoned, and the indiscriminate employment of the supposed remedy
cannot be too strongly reprobated; its effects are most severe and
unmanageable; the state of collapse is most complete and alarming, and
it is often difficult, if not impossible, to bring the patient out of
it—to procure reaction. In some cases reduction may be accomplished
during the state of extreme debility which follows its use, but I
have often seen it fail, and have witnessed the operation afterwards
performed on the patients, who were at the time without pulsation,
and from whom little blood flowed after the incisions; they never,
of course, rallied, and sunk rapidly. Indeed the patient is always
in a very unfavourable state for opera425tion after the exhibition of
the tobacco enema, though certainly in a very favourable state for
reduction being attempted. The strong objection to the medicine I
conceive to be its being so extremely unmanageable; it is impossible
to say whether the depression of the vital powers that must ensue will
be just sufficient to induce that relaxation and debility necessary or
favourable to reduction, or whether it will proceed uncontrollable to
such a degree as to extinguish life. In general it produces intolerable
nausea and depression, universal relaxation of the muscles, coldness
of the surface, with clammy exudation, vomiting, violent retching,
vertigo, and perhaps insensibility. Were I so unfortunate as to be the
subject of strangulated hernia, I should certainly have no tobacco
used. After unsuccessful trial of the taxis, I might submit to be bled
ad deliquium, and have a surgeon to attempt reduction during syncope;
if somewhat more advanced in life, I should prefer the warm bath; if
taxis then failed, I should certainly be operated on in a very few
minutes afterwards. If the surgeon, after mature consideration, make up
his mind as to the course of practice he would wish pursued in his own
case, he will be fully alive to the necessity of impressing the utility
of it on his patients, and have little difficulty in persuading them to
submit to his proposals. No time should be dissipated in administering
purges or clysters, or in cold or warm applications.
If the tumour is not very tender, make one good trial of the taxis,
not long continued; if a warm bath can be readily commanded, place the
patient in it, and employ the taxis when he begins to feel faint. If
foiled, and if the patient can bear depletion well, the strangulation
being recent, try a full bleeding to syncope; it may save depletion
afterwards, and at all events the patient will be none the worse for
it. Having failed, as may probably be the case, operate without delay.
The operation, as regards the immediate consequences, is neither
formidable nor dangerous of itself; the delaying of it is attended with
the most serious and irretrievable mischief. It ought to be performed
within a very few hours after the occurrence of strangulation, and,
in most instances, without putting off time with the means considered
auxiliary to the taxis. Under urgent circumstances, it may be necessary
to operate within a quarter of an hour after seeing the patient, as
I have often done. In ordinary cases, time must be taken to converse
with the patient and his friends, to convince them that all those
means likely to assist reduction, and render an operation unnecessary,
have been tried. The surgeon must not appear to be in a hurry, though
he puts off no time unnecessarily; otherwise his motives may be
misconstrued.
The necessity for operating early is greater in small than in large
herniæ, in crural than in inguinal. The groin and neighbouring parts
are to be shaved, and the patient placed in the recumbent posture,
with the shoulders slightly elevated. The mode of operation must be
varied according to the nature of the tumour, its size, and other
circumstances.
426
The operation for inguinal herniæ is conducted as follows:—The patient
is placed recumbent on a table, or, in private practice, on the side of
a bed, his shoulders supported by pillows, and his feet resting upon
a stool. An incision is commenced about an inch above the external
abdominal ring, and continued to the bottom of the tumour. This
latter part of the procedure, however, is applicable only to small
and moderately-sized herniæ; in large tumours the wound is not made
so low, for in them the bowels may be irreducible, from the quantity
protruded, and the contracted state of the abdominal cavity; in such
cases the incision should be only to such an extent as is sufficient to
enable the operator to reach the stricture. The first cut is carried
through the skin and fatty matter, not deeper. The layers are then
divided successively, with the hand unsupported; and this is done only
at the middle and projecting part of the swelling. It is unnecessary
to prolong the incision of the layers along the whole extent of the
wound in the integuments, at this stage of the proceedings. In the
direct hernia, which is of rare occurrence, there is but one proper
layer,—that furnished by the superficial abdominal fascia: not
unfrequently there is an imperfect additional envelope, furnished by
fibres from the edge of the external ring; sometimes the tumour does
not escape through the external ring, and is then of course covered
by the tendon of the external oblique; of this I have seen but one
instance, and that in a female; but in a common inguinal hernia there
are three or four, and these are thickened more or less according to
the size and duration of the tumour. The division of these layers must
necessarily be conducted with great care and caution. At length the
sac is exposed. This is opened by pinching up a portion betwixt the
nails of the thumb and forefinger, or with dissecting forceps, and then
cutting with the blade of the knife laid horizontally. On wounding the
sac, there is usually evacuated a small quantity of brownish serous
fluid. The probe-pointed bistoury is then taken up, and insinuated
into the opening; and by this instrument, guided on the forefinger of
the left hand, the sac and its coverings are divided up to near the
ring, and down to near the bottom of the tumour. The hernial contents
are thus exposed. These are unravelled, and examined attentively; if
only brownish-red, from accumulation of the venous blood, of unbroken
surface and unadherent, they are fit to be reduced. The stricture is
felt for with the forefinger of the left hand, and into it either the
point of the finger or the nail is gently insinuated. The protruded
parts, if voluminous, are held down by an assistant; and along the
forepart of the finger is passed a probe-pointed, narrow, and slightly
curved knife. In carrying this upwards, the blade is placed flat on the
finger, and its point, and no more, is passed through the contracted
part; its edge is then turned forwards, its back resting on the finger;
and by raising the handle gently, a slight incision is made into
the more resisting fibres, in the direction of the mesial line. The
instrument is withdrawn with the same caution as in its introduction.
The finger now enters easily, and by raising it gently and repeatedly
the parts are dilated. It is then passed upwards to the site of the427
internal ring: and if this be found narrow and contracted, the edge of
the knife to be directed against it in a similar way, and dilatation to
a sufficient extent effected. Now reduction is to be commenced, and in
doing so the same precautions are to be observed as in the employment
of the taxis. The hernial sac ought in the first place to be fixed by
the fingers of the assistant placed in the bottom of it, so that it
may be prevented from sliding up along with the contents. A neglect of
this rule is often observed to lead to much embarrassment. The parts
seem to have passed back into the general cavity; but on withdrawing
the pressure they fall down again from the canal, along with the sac
which had slipped up so far with them. In general, the omentum, if any,
is put back first, and then the bowel; but this must depend on the
relative quantity of the parts, and other circumstances. With the right
hand the bowel is to be compressed as uniformly as possible; and, if
at all obstinate, its reduction may perhaps be accelerated by pulling
down a small portion at the neck, so as to facilitate the return of the
fecal contents. By gentle pressure with the forefingers one portion
is put back after another: it is wrong to attempt sudden and entire
reduction; it should be gradual and successive. In many cases, from
adhesion, or from the bulk and nature of the hernia, the parts, though
sound, cannot or ought not to be reduced; a portion may be got back,
but part requires to remain. This can often be ascertained beforehand
by properly conducted and previous inquiry into the history of the
case, as to the duration of the disease, and the period at which the
whole tumour could be made to disappear. In such cases, the stricture
should always be freely relieved. When the bowel is mortified, and its
contents effused into the sac, care is to be taken not to detach or
disturb the adhesions at the neck, and the bowel should be opened so as
to allow of free discharge. When the bowel or omentum are comparatively
sound, though irreducible, the surgeon must rest contented with
relieving the stricture; then cover the parts with the integuments,
and promote union of the wound. If it be considered necessary to
remove condensed and tuberculated omentum, it is cut off, and separate
ligatures of fine thread are applied to every bleeding vessel on the
cut surface; the whole mass is not to be included in one noose, as was
formerly the practice.
In the operation for femoral hernia, the position and preliminaries
are the same as for inguinal. A longitudinal incision is made from
above the margin of Poupart’s ligament to a little below the middle and
most prominent part of the tumour. This is crossed by another at its
lower extremity, the whole resembling in figure the letter T inverted;
and the two flaps so marked out, are reflected. Sometimes a single
incision, from above the neck of the tumour to the lower border of it,
is sufficient to afford room for the after proceedings. For some years
past I have performed an incision along the course of the ligament
of Poupart, with another falling from it over the body of the tumour
like the letter T, with the transverse part a little awry. In cases
of very large femoral hernia, such as that seen on the next page, the
incisions, as in the large inguinal tumour, must be made over the428
situation of the femoral ring, and to a limited extent. In this case
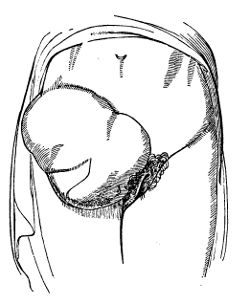 the symptoms had existed for eight days, and had been latterly very
urgent, there being profuse feculent vomiting, and great depression of
the powers of life. There was a large mass of bowel protruded: this
was all returned, and the patient, though well advanced in life, made
a rapid recovery. A cast was obtained after her death, which happened
several years afterwards. It is seldom indeed that femoral hernia
attains such a size. I have seen it in the male, however, nearly one
half the size of the swelling here shown. The tumour is often not
larger than a walnut, seldom exceeding the size of a small apple. One
layer is found covering the sac, furnished by the strong and dense
cellular tissue which occupies the space under the crural arch and
falciform process of the fascia lata: it is generally denominated the
fascia propria, and has been described improperly, it would appear,
as the sheath of the femoral bloodvessels; at the lower part of the
tumour it is generally wanting. It is carefully divided, so as to
expose the sac. This not unfrequently is thickened very considerably, a
quantity of dense fatty matter being intimately incorporated with it;
but in general it is thin, and appears of a dark colour, in consequence
of the bowel and effused bloody serum being seen through it. It is
opened with great caution, part of it being raised and touched with
the edge of the knife held horizontally, or nearly so. The aperture,
thus formed, is enlarged by means of the probe-pointed knife, which is
carried upwards along the forefinger of the left hand. Some recommend
that the sac should be left undivided, and that the stricture should
be relieved by passing the knife on the outside; others, that only the
neck of the sac should remain entire, and the stricture be attacked
also on the outside of the peritoneum. But this appears an unnecessary
and unprofitable precaution. The extreme difficulty of returning the
sac is now well known and generally acknowledged; indeed, reduction of
it, whether opened or not, is practicable only in recent cases. Its
neck, besides, is firmly constricted; and the bowel may and will remain
strangulated when returned along with its sac, for the peritoneum
long retains the contraction at its strictured point. The stricture
cannot be well relieved unless the neck of the sac is cut along with
the resisting fibres exterior to it. After the sac has been opened,
the forefinger of the left hand is passed up to the crural ring; and
it should be recollected that this opening is very small, even in most
cases in which a hernia of ordinary size has existed for some time. It
is capable of great dilatation, gradual however, so that, in429 very old
and large ruptures, it may admit two or three fingers easily. But in
general only the nail of the finger can be insinuated into it; and this
is a better and safer conductor for the knife than a grooved director.
The edge of the stricture is felt very sharp; the point of the finger
is turned towards the pubes, and along it a narrow, blunt-pointed,
curved bistoury is passed in close contact, and with the edge towards
the pubes; its mere point is pushed beyond, and then the position of
the blade is changed: its back is turned upon the finger. This slight
motion is of itself often sufficient to relieve the constriction on
the protruded parts, and permit their reduction; if not, a few more
fibres are cut by raising the handle of the knife gently from the palm
of the hand. The direction of this incision is towards the tuberosity
of the pubes, inwards and forwards. Thus only the crescentic portion of
the crural arch is cut; and the division of this produces sufficient
relaxation of the neighbouring parts. There is danger in cutting
directly forwards, particularly in the male, at least if the incision
be made to any considerable extent; there is a risk of wounding the
spermatic chord, and the obturator artery has also been met with in a
few instances coursing round the neck of the sac. This distribution of
the artery, however, is rare, and can occur only when the epigastric
and obturator arise by a long common trunk, and even then it may not
encircle the neck of a hernia, as I have witnessed. Occasionally a
vessel of considerable size passes round the opening, connecting the
epigastric with the obturator, when these arteries follow their usual
course; and this also may surround the neck of the sac. If vessels
should exist in this situation in a person the subject of operation,
as has not happened so far as I know, they would be felt by the finger
used to conduct the knife. And the bistoury should never be passed—for
there is no necessity for it—through the opening so far as to meet
with a vessel, even if awkwardly placed. The danger of cutting forward
and to any extent has already been spoken of; such incision can answer
no good purpose. The stricture is not in Poupart’s ligament—though at
one time it was proposed to cut this through without interfering with
the tumour at all—but in the crural arch underneath, and in a manner
independent of the strong tendinous chord and expansion. The crural
arch is formed by the junction of the fasciæ of the thigh and abdomen,
superficial and deep. It is inserted into the linea ileo-pectinea,
where the tendon of the external oblique has no connection, and is
strengthened by fibres from the internal oblique, transverse, and
recti muscles. The crural aperture formed by this arch is relaxed by
flexion and inversion of the thigh, and by relaxation of the abdominal
parietes. And this fact requires to be attended to, after operation
as well as during the taxis, so as to facilitate replacement of the
protruded parts.
the symptoms had existed for eight days, and had been latterly very
urgent, there being profuse feculent vomiting, and great depression of
the powers of life. There was a large mass of bowel protruded: this
was all returned, and the patient, though well advanced in life, made
a rapid recovery. A cast was obtained after her death, which happened
several years afterwards. It is seldom indeed that femoral hernia
attains such a size. I have seen it in the male, however, nearly one
half the size of the swelling here shown. The tumour is often not
larger than a walnut, seldom exceeding the size of a small apple. One
layer is found covering the sac, furnished by the strong and dense
cellular tissue which occupies the space under the crural arch and
falciform process of the fascia lata: it is generally denominated the
fascia propria, and has been described improperly, it would appear,
as the sheath of the femoral bloodvessels; at the lower part of the
tumour it is generally wanting. It is carefully divided, so as to
expose the sac. This not unfrequently is thickened very considerably, a
quantity of dense fatty matter being intimately incorporated with it;
but in general it is thin, and appears of a dark colour, in consequence
of the bowel and effused bloody serum being seen through it. It is
opened with great caution, part of it being raised and touched with
the edge of the knife held horizontally, or nearly so. The aperture,
thus formed, is enlarged by means of the probe-pointed knife, which is
carried upwards along the forefinger of the left hand. Some recommend
that the sac should be left undivided, and that the stricture should
be relieved by passing the knife on the outside; others, that only the
neck of the sac should remain entire, and the stricture be attacked
also on the outside of the peritoneum. But this appears an unnecessary
and unprofitable precaution. The extreme difficulty of returning the
sac is now well known and generally acknowledged; indeed, reduction of
it, whether opened or not, is practicable only in recent cases. Its
neck, besides, is firmly constricted; and the bowel may and will remain
strangulated when returned along with its sac, for the peritoneum
long retains the contraction at its strictured point. The stricture
cannot be well relieved unless the neck of the sac is cut along with
the resisting fibres exterior to it. After the sac has been opened,
the forefinger of the left hand is passed up to the crural ring; and
it should be recollected that this opening is very small, even in most
cases in which a hernia of ordinary size has existed for some time. It
is capable of great dilatation, gradual however, so that, in429 very old
and large ruptures, it may admit two or three fingers easily. But in
general only the nail of the finger can be insinuated into it; and this
is a better and safer conductor for the knife than a grooved director.
The edge of the stricture is felt very sharp; the point of the finger
is turned towards the pubes, and along it a narrow, blunt-pointed,
curved bistoury is passed in close contact, and with the edge towards
the pubes; its mere point is pushed beyond, and then the position of
the blade is changed: its back is turned upon the finger. This slight
motion is of itself often sufficient to relieve the constriction on
the protruded parts, and permit their reduction; if not, a few more
fibres are cut by raising the handle of the knife gently from the palm
of the hand. The direction of this incision is towards the tuberosity
of the pubes, inwards and forwards. Thus only the crescentic portion of
the crural arch is cut; and the division of this produces sufficient
relaxation of the neighbouring parts. There is danger in cutting
directly forwards, particularly in the male, at least if the incision
be made to any considerable extent; there is a risk of wounding the
spermatic chord, and the obturator artery has also been met with in a
few instances coursing round the neck of the sac. This distribution of
the artery, however, is rare, and can occur only when the epigastric
and obturator arise by a long common trunk, and even then it may not
encircle the neck of a hernia, as I have witnessed. Occasionally a
vessel of considerable size passes round the opening, connecting the
epigastric with the obturator, when these arteries follow their usual
course; and this also may surround the neck of the sac. If vessels
should exist in this situation in a person the subject of operation,
as has not happened so far as I know, they would be felt by the finger
used to conduct the knife. And the bistoury should never be passed—for
there is no necessity for it—through the opening so far as to meet
with a vessel, even if awkwardly placed. The danger of cutting forward
and to any extent has already been spoken of; such incision can answer
no good purpose. The stricture is not in Poupart’s ligament—though at
one time it was proposed to cut this through without interfering with
the tumour at all—but in the crural arch underneath, and in a manner
independent of the strong tendinous chord and expansion. The crural
arch is formed by the junction of the fasciæ of the thigh and abdomen,
superficial and deep. It is inserted into the linea ileo-pectinea,
where the tendon of the external oblique has no connection, and is
strengthened by fibres from the internal oblique, transverse, and
recti muscles. The crural aperture formed by this arch is relaxed by
flexion and inversion of the thigh, and by relaxation of the abdominal
parietes. And this fact requires to be attended to, after operation
as well as during the taxis, so as to facilitate replacement of the
protruded parts.
The same attention to the state of the parts in judging of the
propriety or not of reduction after operation, and the same after
treatment, both general and local, is requisite in crural hernia as
in inguinal. When the parts are reduced, the edges of the wound are
brought together by means of a few stitches; a graduated compress, of
proper dimensions, is applied, and retained by a spica bandage. If
this430 is neglected, there is a risk of the parts again descending.
Afterwards large mild enemata are to be administered, and, after some
hours, purgatives, so as to procure copious and free evacuation of the
bowels. In many cases after reduction, the bowels cannot by any means
be got to act downwards. This seems sometimes to arise from a sort of
paralytic state of the fibres of the part which has been extruded and
 compressed. Again, it often arises from an indentation of the coats
of the bowel at the point where they have been tightly embraced and
compressed by the sharp edge of the opening, as here represented.
The engorged and dark state of the upper portion of bowel contrasts
well with the lower, which is generally empty, contracted, and pale.
If the stomach continue unsettled, a sinapism may be applied to the
epigastrium, or solid opium exhibited. Subsequently it may be necessary
to bleed locally, or generally, or both; in other cases the strength
from the first requires support. After cicatrisation, a well adapted
truss must be constantly worn.
compressed. Again, it often arises from an indentation of the coats
of the bowel at the point where they have been tightly embraced and
compressed by the sharp edge of the opening, as here represented.
The engorged and dark state of the upper portion of bowel contrasts
well with the lower, which is generally empty, contracted, and pale.
If the stomach continue unsettled, a sinapism may be applied to the
epigastrium, or solid opium exhibited. Subsequently it may be necessary
to bleed locally, or generally, or both; in other cases the strength
from the first requires support. After cicatrisation, a well adapted
truss must be constantly worn.
Umbilical hernia is generally congenital. The tendinous parietes are
often deficient to a great extent, and there is consequently much
fulness along the umbilical chord. The plan of embracing such tumours
in children by ligature, as at one time extensively practised, is
now abandoned, there being much risk of peritoneal inflammation and
fatal issue. The surgeon is now content with reducing the hernia,
and applying a truss, to prevent displacement, as in other forms of
protrusion; and if this be done in early life, and the apparatus
carefully worn, the opening contracts, and the patient may ultimately
be cured. The tumour may become strangulated, though rarely in the
adult; it is generally large, and almost solely occurs in females. The
sac has no covering but the skin and cellular tissue and fatty matter.
A small incision is made through the sac and its investments, either
on one side of the tumour, or in the mesial line at its lower aspect.
The stricture is then divided with care, the parts reduced, the wound
approximated, and a compress applied. Opening the tumour throughout its
whole extent is hazardous and unnecessary. The same remarks apply to
the proceedings in cases of ventral hernia. In corpulent females the
tumour is sometimes scarcely prominent, and is only discovered as a
flattened cake through the fatty matter.
The contents of hernia are often in a very bad state, either
dark-coloured throughout, or studded with dark tender spots. Lymph is
often effused all over the parts, gluing them to one another, and to
the sac. This effusion, which generally takes place to the greatest431
extent at the neck of the sac, is a wise provision made by nature
against the accidents of the disease; inasmuch as a barrier is thereby
formed between the cavity of the abdomen and the extruded parts,
preventing, in a great measure, the destruction of the latter from
affecting the abdominal viscera. For example, a portion of protruded
intestine sloughs, the feculent matter is effused, and, had not this
adhesion to the neck existed, the gut might have slipped back into the
abdomen, its contents would have escaped there, and a fatal result
would have been the inevitable consequence. Still, notwithstanding
the salutary effusion, the bowel may ulcerate at its upper part, and,
giving way within the belly, produce rapid death. The bowel, where
embraced by the stricture, is contracted and thickened, and dilated
above. At the lower part of this dilatation the coats are apt to give
way by ulceration, even after incision of the constricting parts and
reduction. The contraction does not disappear quickly. In some cases
it continues to such an extent as to keep up obstructions to the fecal
matter, and cause a fatal issue from this cause alone, as noticed above.
Often, on opening the sac, in long neglected cases, a discharge takes
place of fetid air and thin feculent matter, the bowel has mortified
either entirely or in patches; in the latter case, presenting
the appearance of having been perforated at various points. Few
constitutions can bear up under such mischief. In some, if an opening
be not made, the integuments slough, and the patient, rallying after
discharge from the bowel takes place, recovers after losing a portion
of integument, of intestine, and perhaps of omentum. In others, and
they constitute the majority, the system sinks, before discharge from
the bowel is effected, by sloughing of the external parts.
The surgeon is called on to operate in the worst possible
circumstances, provided the patient is not in articulo mortis. Even
after many days of feculent vomiting the bowels may be found tolerably
healthy. The sac must be opened carefully, and the stricture is to be
relieved without disturbing the adhesions that have formed. The bowel,
when dead, or evidently gangrenous, is to be opened, and the discharge
of feces by the wound promoted. If returned into the abdomen, the
sloughs will separate, in all probability, and feculent effusion take
place, causing death in a very few hours. Sometimes the patient lingers
longer than could be expected, and I have known a female survive
upwards of a hundred hours after the occurrence of effusion into the
abdomen, from the giving way of an ulcer in the stomach. The dressing
should be light, and the patient’s strength must be supported in every
way, by the mouth, and by the anus when the injured part is high in the
canal. The separation of the sloughs is to be encouraged. The extent of
sloughing need not dishearten the surgeon, for large portions of bowel,
several feet in length, have mortified, and the patients recovered,
with artificial anus, either temporary or for life.
In artificial anus, when this has followed upon destruction of the
bowel to a considerable extent, the intestine has contracted firm
adhesion to the hernial sac at the opening in the abdominal parietes;
through the opening in the bowel exterior to this the feculent matter432
is discharged externally, and by the adhesion is prevented from being
effused into the abdominal cavity. The protruded bowel in which the
sphacelation has occurred may be said to be thereby divided into an
upper and an under portion,—one, the upper, discharging, the other,
collapsed and empty; these lie parallel to each other, in close
contact, and usually adhering, from the abdominal or crural ring
downwards, to each other, and to the hernial sac. The hernial sac
seldom sloughs entirely; in almost every case its neck remains sound;
to this remaining part the intestine adheres. The deficiency in the
integuments and cellular tissue, through which the feculent matter
escapes, gradually contracts, and the aperture in that portion of the
hernial sac which is exterior to the intestine also diminishes; but
at the same time dilatation takes place in the immediate vicinity
of the intestinal orifices, so that a funnel-like cavity is formed
for the evacuation of feces, extending from the opening in the bowel
to the opening in the skin—its narrowest part being at the latter
situation, its most capacious surrounding the intestine. The cellular
tissue intermediate between the integument and hernial sac becomes
condensed, and forms a membranous lining. By this cavity an imperfect
communication is established between the two portions of bowel, part of
the feculent matter returning through the lower intestinal orifice, and
part escaping externally. But this communication must be indeed very
imperfect at first, since the two portions of bowel lie parallel to
each other, and their coalescing sides form an acute angular projection
into this funnel-shaped cavity. The lower portion is necessarily much
diminished in calibre, being in a great measure unaccustomed to the
usual distension, and its collapsed orifice is retracted a little
higher than that of the superior. On account of these circumstances
feculent matter cannot pass straight onwards from one portion of bowel
to the other, but must first traverse the funnel-shaped cavity; and
even then it is but a small quantity that reaches the rectum. Indeed,
in most cases of artificial anus, nothing but occasional flatus passes
by the original outlet for weeks or months. After some time the
bowel retracts, but cannot leave the adhesion in the groin: by this
retraction the orifices may be brought in a more direct line with each
other, and the natural passage of the feces be somewhat assisted.
When one or more slight patches of discoloration are observed after
division of the sac, it may be returned, it being most probable that
the parts will recover after removal of the stricture. When any portion
has given way, of course no one can contemplate reduction; and when the
whole calibre has sloughed it is absurd to attempt separation of the
adhesions which must exist, dividing the external from the internal
parts.
In mortification of a protruded knuckle, or part only of the calibre
of bowel, the symptoms are at first severe. These are vomiting, pain,
and symptoms of enteritis; perhaps the bowels are obstructed for some
time, but evacuation again takes place, as happened in the following
remarkable and instructive case. A gentleman, nearly eighty years of
age, was, during the action of medicine, suddenly seized with pain in
the groin. A very small tumour was observed433— he became sick—and when
I visited him for the first time two days after, he had no further
evacuations from the bowels, he vomited constantly bilious fetid
matter, and he began to complain of pain in the abdomen. Pressure was
kept upon the tumour, which protruded at the crural aperture, for some
time, with the effect of diminishing its size very considerably. On
returning in a couple of hours with Sir B. Brodie, with the intention
of cutting down upon the swelling, the bowels had been freely relieved,
the vomiting had entirely ceased, and there was not the slightest
vestige of tumour to be perceived or felt, on the most attentive
examination. The patient had a good night, but in the morning had a
recurrence of the symptoms: these continued, and a fatal termination
shortly occurred; still no tumour could be detected before or after
death. It was supposed that the obstruction might have been caused
by a continuance of the constriction of the bowel, where it had been
nipped by the stricture. On a post-mortem examination, there was found
an exceedingly small portion of the coat of the bowel still entangled
 in the crural ring, whilst a larger portion, which bore marks of
having been protruded, was thus entangled, and confined to the spot.
The bowel, though not completely obstructed, was narrowed by the
confinement of part of its parietes.
in the crural ring, whilst a larger portion, which bore marks of
having been protruded, was thus entangled, and confined to the spot.
The bowel, though not completely obstructed, was narrowed by the
confinement of part of its parietes.
Abscess often occurs externally to a small swelling of this nature, and
on the giving way of the integument, matter, flatus, and thin feces
are discharged. A fecal fistula remains for some time; but, by the
aid of lymph and granulations, the breach in the parietes of the bowel
is repaired gradually, the feces resume their natural course, and the
external opening heals.
When the whole calibre has sloughed, and even when a large extent
of bowel has come away, and there is still a chance of the patient
recovering from the artificial anus by natural means, after the lapse
of many months. As already remarked, the intestinal orifices retract,
and come more into a straight line. A mucous discharge occurs from the
lower bowels along with the passage of flatus, and at last part of the
feces is voided by the rectum. The discharge from the external opening
diminishes, and ultimately ceases, perhaps only a minute fistula
remaining, through which a few drops of fluid, sometimes feculent,
sometimes limpid, may occasionally escape. The funnel-shaped cavity
previously contracts into a narrow fistula. This desirable result may
be assisted and hastened by gentle pressure; and, after the feculent
discharge has nearly ceased from the fistulous opening, the healing of
this may be accelerated by the cautery lightly applied. It has been
proposed to destroy the projecting septum between the two portions
of bowel, either by ligature or by the pressure of forceps; but this
should not be attempted unless nature seems unable to effect a cure.
The former434 method consists in including a considerable part of the
septum in ligature, so as to induce condensation of the parts by
effusion of lymph, and destruction of the projecting portion. This has
not been found very successful. The application of forceps presents a
more rational expectation of cure. The external opening is dilated,
and the situation of the septum ascertained. One blade of metallic
forceps, with blunt serrated edges,—Dupuytren’s,—is passed into the one
intestinal orifice, and the other into the opposite; the handles of the
instrument are then approximated, locked, and fastened with a screw,
and by means of the last-mentioned part of the apparatus the degree
of pressure is regulated. Pain of the abdomen, furred tongue, loss of
appetite, sickness, vomiting, and constitutional irritation, generally
follow this proceeding, but gradually subside on the employment of
enemata and fomentations, and on lessening the pressure of the forceps.
The septum cannot long withstand the continued compression, and by its
destruction the chance of cure is greatly augmented. The proceeding is,
besides, not so dangerous as might at first be supposed; for effusion
of lymph takes place to a considerable extent above the part grasped
by the forceps, gluing the portions of bowel firmly to each other,
and forming a new barrier against any of the feculent matter escaping
inwardly. Attempts may be made to repair the loss of substance in the
skin by paring the edges of the opening, and affixing a flap taken from
the neighbourhood.45
435
There is a greater chance of recovery from the inconvenience of
artificial anus after hernia than after wounds. If the opening in the
bowel be near the stomach, the patient will die from inanition. When
it is lower in the intestinal tube, nutrition is more perfect, and the
patient can be further supported by nutritive enemata. When no natural
cure is likely to take place, the inconvenience will be palliated by
a truss with a soil pad being worn, so as to retain the feces till a
favourable opportunity occurs for evacuation; or a soft plug of lint
may be inserted into the aperture, and retained by a compress and
roller. Prolapsus of the mucous membrane of the gut sometimes takes
place through the artificial anus, and is reduced with difficulty. The
use of a truss or tent, already mentioned, will tend to prevent the
occurrence. Great attention to cleanliness is required when the opening
cannot be closed.
Operations for other kinds of hernia, if discovered during life, are to
be conducted on similar principles with those for inguinal and crural.
The surgeon must be guided by his anatomical knowledge. No positive
rules can be given.
In Ascites, or accumulation of fluid in the peritoneal cavity, the
surgeon is not unfrequently called upon to relieve the patient, when
the abdominal parietes are much distended, and the functions of the
viscera of the abdomen and thorax interrupted. He must, however,
exercise his own judgment in regard to the case, and convince himself
of the propriety of operating. He must examine into the symptoms, and
ascertain that the tumour is really caused by accumulation of fluid
in the bag of the peritoneum. In ascites, the abdomen has swelled
slowly and uniformly, and distinct fluctuation is felt when the hand
is placed on one side of the swelling, and gentle tapping made at the
other. There is considerable difficulty of breathing, uneasiness in the
abdomen, usually increased by pressure, thirst, and scanty secretion
of urine. It ought to be remembered that other affections have been
confounded with ascites, and lamentable operative mistakes committed in
consequence. Trocars have been thrust into the belly for tympanitis,
either of the bowels or of the peritoneum—for solid tumours of the
viscera—for enlargement of the ovaria.
As already hinted, the operation of tapping the abdomen is to be
undertaken only when the distention is very great, when the functions
of the thoracic and abdominal viscera are interfered with, and when
diuretics, and other means of getting rid of the fluid, have failed to
diminish the accumulation. The trocar employed is either flat, with
a spring steel canula, or round; when the latter is used, and the
abdominal parietes are not very tense, a small incision is first made
with a lancet or bistoury; a large trocar with blunted edges and point
can then be readily and safely introduced; the flat one enters easily,
and requires no previous wound, but does not permit so rapid and free
a flow. The point usually chosen for the puncture is either in the
linea alba, a little below the umbilicus, the bladder being previously
emptied,—a precaution which should always be attended to, though in
general there is little danger of wounding this organ—or midway betwixt
the superior anterior spinous process of436 the ilium and the umbilicus,
with the view of penetrating the parietes in the linea semilunaris. The
latter situation, however, can seldom be obtained with accuracy, for
the parietes yield irregularly. Little bleeding follows the puncture at
either point; but the risk of hemorrhage is greater at the latter, for
branches of the circumflex artery may be wounded. More serious bleeding
is liable to occur, from the veins ramifying on the abdominal viscera
giving way, on removal of their support, as the serum flows off.
Fainting, also, may take place from accumulation in the branches of the
vena portarum, unless the fluid is withdrawn slowly, and the precaution
adopted of supporting the parietes with a broad band both during and
after evacuation. Bandages are made for this purpose, with tapes and
straps attached, and are well fitted for it. Three or four yards of
flannel, however, with each end split, are equally effectual, and can
always be readily obtained—a consideration of consequence in the choice
of all apparatus. After the band has been applied, a person is placed
on each side to tighten it gradually by steady pulling at the ends,
which are carefully crossed behind. An opening is made in the cloth,
opposite to where it is proposed to puncture, and the operation is then
proceeded in. Sometimes the flow is impeded by the omentum or a fold
of bowel falling forward on the canula, and closing or diminishing the
opening; this is remedied by passing a tube along the canula, closed
at the extremity, but perforated at the sides near it, and about half
an inch longer than the canula. After the cavity has been emptied, the
patient is placed recumbent, and a long broad flannel bandage applied
over the whole abdomen, and retained, so as to prevent shifting, by
straps passed over the shoulders and under the perineum.
Collections occur in the ovaria. The fluid is generally glairy,
sometimes thick and gelatinous, often turbid and dark coloured. Not
unfrequently the main cyst is subdivided, either by membranous septa,
or by an aggregation of smaller cysts of the nature of hydatids. The
swelling is at first on one side, and gradually rises out of the
pelvis; often it remains long moveable; it increases, becomes more
fixed, and ultimately fills the abdomen, displacing the viscera, and
giving rise to feelings of much uneasiness, deformity, and loss of
health. The cyst is generally thick; sometimes it is thin at one or
more points, and this may give way, causing effusion of the contents
into the peritoneal sac. Fluctuation is perceptible in many cases; in
others it is obscured by the thickness of the cyst and viscidity of its
contents. Many such swellings may be punctured both with advantage and
with safety, but generally the tapping requires frequent repetition.
Some patients require tapping, merely as a mean of improving the figure
and relieving uneasy feelings, once, twice, or thrice a year; their
existence is not much embittered or abridged by the disease. A large
round trocar is necessary for the purpose; and the puncture is made at
the softest and most prominent point of the tumour, a small incision
through the integument being premised.
The ovaria become enlarged by degeneration of their structure and the
addition of solid matter in great abundance. The consistence and437
structure of such tumours are very various; they are sometimes, though
rarely, medullary, often fibrous, with or without cysts, sometimes
melanotic. In the majority there are cysts, varying in size, number,
and contents; sometimes the bag contains hydatids, or it is filled
with curdy matter, sometimes with glairy colourless fluid, sometimes
with a turbid and flaky serum, sometimes with blood; and in them, as
well as in the enlargement from accumulated fluid, though perhaps
more rarely, are occasionally found teeth, hair, and membranous
looking matter; some are intermixed with bone, cartilage, and fat.
 The situation and attachments of such tumours cannot be correctly
ascertained by examination during life, far less can their internal
structure and dispositions be arrived at. Indeed an accurate diagnosis
is exceedingly difficult, if not impossible. Innumerable mistakes have
been made, which have led to most unjustifiable proceedings. In one
case, the abdomen was, after two or three dry tappings, opened by an
incision from the ensiform cartilage to the pubes; the viscera were
turned over and over, but no tumour could be discovered. The woman was
sewed up, and did not die. The following was a still more complete
failure in diagnosis. In a case of large tumour of the belly, many
persons accustomed to manipulate abdominal swellings considered that
extra-uterine conception had taken place; and that the child had come
to maturity and perished. The history of the case countenanced the
supposition; the symptoms had been such as indicate impregnation. The
woman, to avoid exposure, went to a distance to be relieved of her
burden, which was becoming more and more troublesome and bulky. The
usual period passed over. It was thought that the head and thorax of
an infant could then be felt readily through the parietes, and perhaps
some one might have been found heroic enough to have divided them and
explored the tumour. The young woman, however, was in the last stage
of phthisis, and soon died. A wonderfully tuberculated omentum, a very
small portion of which is here represented, filled the peritoneal
cavity; the uterus and its appendages were quite healthy.
The situation and attachments of such tumours cannot be correctly
ascertained by examination during life, far less can their internal
structure and dispositions be arrived at. Indeed an accurate diagnosis
is exceedingly difficult, if not impossible. Innumerable mistakes have
been made, which have led to most unjustifiable proceedings. In one
case, the abdomen was, after two or three dry tappings, opened by an
incision from the ensiform cartilage to the pubes; the viscera were
turned over and over, but no tumour could be discovered. The woman was
sewed up, and did not die. The following was a still more complete
failure in diagnosis. In a case of large tumour of the belly, many
persons accustomed to manipulate abdominal swellings considered that
extra-uterine conception had taken place; and that the child had come
to maturity and perished. The history of the case countenanced the
supposition; the symptoms had been such as indicate impregnation. The
woman, to avoid exposure, went to a distance to be relieved of her
burden, which was becoming more and more troublesome and bulky. The
usual period passed over. It was thought that the head and thorax of
an infant could then be felt readily through the parietes, and perhaps
some one might have been found heroic enough to have divided them and
explored the tumour. The young woman, however, was in the last stage
of phthisis, and soon died. A wonderfully tuberculated omentum, a very
small portion of which is here represented, filled the peritoneal
cavity; the uterus and its appendages were quite healthy.
Operation has also been proposed, when, on dissection, the liver was
found to compose the abdominal swelling. Such cases, a long list of
which might be given, render the prudent surgeon very cautious in his
diagnosis of abdominal tumours, and chary of operative interference
with them. The abdomen has been opened, as already stated, and the
result has been such as to render the perpetrator438 indictable for
culpable homicide, and to qualify him for such punishment as his rash
and reckless conduct richly deserved. A less severe censure might have
sufficed, had not the example been followed by similar proceedings,
and equally direful results; and these have been such as to render any
condemnatory remarks not only justifiable but absolutely necessary. A
great many unfortunate women have, I am afraid, been sacrificed to a
desire for false reputation. The attempts to remove abdominal tumours
by incision of the parietes were some time ago very numerous; and,
as might have been expected, the issues were highly unsatisfactory
to those concerned. Such doings, however, were recorded in print,
represented in plates, and moreover puffed and placarded ad nauseam.
The majority of those who were thus “dissected, to see what part was
disaffected,” perished within forty-eight hours. One woman survived
for some time, after having been subjected to this operation,
improperly so termed. In her there was a tumour, but of such a size,
and so connected, that it could not be removed. A second survived
the extirpation of one ovarium; and the other, also diseased, was
left for a further exhibition of daring intrepidity. It is not easy
to conceive how the proposal could have been seriously entertained
by any sane individual, far less put in practice and persevered in,
when disaster after disaster crowned every attempt. It is my opinion,
and I believe that I express the sentiments of a very large portion
of the profession, that the repetition of any such incisions and
gropings would be unpardonable.—1. On account of the difficulty, nay,
impossibility, of forming a correct diagnosis; of ascertaining with
certainty what organ is involved; of ascertaining the structure and
disposition of the tumour, if any, and to what parts it is adherent.
2. Because the ovarian disease, in general, even though extensive,
does not threaten imminently a fatal termination, being slow in its
progress, and the greater number of the swellings being not of a
malignant nature. The solid tumours are sometimes of a bad kind, as
already stated; but enlargement by fluid is much more frequent in
the ovaria than that by solid and new matter. 3. If the tumour be
malignant, it will be impossible to ascertain to what extent the
parts are involved by the diseased action, or whether the lymphatics
are affected or not. There is a strong probability of the lymphatic
system being involved, even at a very early period; and then the
extirpation of the tumour—supposing the mass to be so situated as to
admit of removal without difficulty or danger—cannot be attended with
any advantage; in every point of view, therefore, interference is
unadvisable. 4. The operative attempt is attended with imminent danger.
There is almost a certainty of the patient being almost instantly
destroyed by it, as shown by the sad experience of the past. “We are
not the arbiters of life and death of those who apply to us for relief.
If people die in consequence of disease, it cannot be helped. They
submit to it because they know it is inevitable. But we had better
refrain from making such experiments as may probably destroy them, and
bring disgrace upon the profession.”
Bruises of the abdomen are apt to be followed by inflammation of the
contained parts, particularly of the serous membrane. Occasion439ally
lacerations of the viscera, both solid and floating, but more
frequently of the former, are produced by bruising or squeezing of the
abdomen, as by a blow, or by a heavy body passing over; they may also
follow a violent concussion of the parts by falling from a height.
The liver is the organ most frequently torn, and death is commonly
the result, rapid, and principally from hemorrhage. The laceration is
generally on the convex surface; extravasation takes place under the
peritoneal covering; or this is torn, and the effusion is into the
abdominal cavity. When the quantity of blood is not so great as to
cause speedy dissolution, the patient may survive for some time, and
even ultimately recover. Reaction is slow, the patient continuing a
long time pale, exhausted, and almost pulseless; there is tenderness in
the hypogastric region, with swelling. The spleen is liable to similar
injury, and pours out a large quantity of blood.
The gall-bladder has sometimes been torn, as also portions of the small
intestines, by a blow or kick, or by a heavy body passing over the
abdomen, as the wheel of a loaded wagon. The escape of the contents is
followed by sickness, rigour, quick, weak, and indistinct pulse, most
excruciating pain, a sense of heat diffused all over the abdomen, and
rapid sinking of the powers of life; a fatal termination generally
occurs within twelve hours. The same train of symptoms supervene
when the contents of the intestinal canal have been effused into the
peritoneal cavity, through an opening in the stomach or bowel, caused
either by slow destruction of the coats, the peritoneum giving way
last, or by a rapid ulceration or sloughing process, as in hernia.
The patient may live in agony for a day or two, but death generally
takes place much within twenty-four hours. The same may be said of the
rupture of the bladder, from external violence, with effusion of urine
into the peritoneal sac. No treatment is of any avail; venesection
hastens the sinking. Fomentation over the abdomen, and sedatives either
by the mouth or by the anus, soothe the patient, and render his last
moments more calm.
Penetrating wounds of the peritoneal cavity, if they reach the solid
viscera and large vessels connected with them, are attended with
effusion of blood externally and internally, in quantities proportioned
to the size of the external aperture, the importance of the vessels
concerned, and the vascularity of the part. The patient may perish from
the bleeding, either instantly or after some time; or inflammation and
its consequences supervene in the violent form, and destroy him at a
more remote period. The mere opening of the peritoneal cavity, and to
a very slight extent, without the slightest injury of the contained
parts, is often attended with a great shock to the system, and is
followed by inflammatory action, which may run on to a fatal issue, in
spite of the most active and judicious management. The inflammatory
symptoms are to be combated by free abstraction of blood; in short,
the utmost endeavours must be made to keep the action within bounds.
When the intestines are wounded, the injured part may protrude; or the
relative size of the openings through the parietes and bowel may be
such, that the intestinal contents do not escape into the peritoneal
bag. A natural cure sometimes takes place by adhesion of the surface
of the bowel to the lining of the parietes round the wound, feculent
matter continuing to be discharged440 externally; after a time the
opening may contract, and the discharge diminish and ultimately
cease; or an artificial anus may be permanently established, and this
is not so easily cured as that following upon hernia. Wounds of the
intestines, whether transverse or longitudinal, attended with feculent
escape into the peritoneal cavity, are not uniformly fatal. Effusion of
lymph takes place around, gluing the wounded bowel to the peritoneal
surface of a neighbouring fold, or forming a sort of pouch within which
the extravasation is limited. The treatment consists in absolute rest,
and most rigid antiphlogistic regimen; manual interference with the
wounded part is not generally advisable.46
441
Lumbar Abscess is generally chronic; the collection of matter is
gradual and slow. Sometimes it is acute, and rather rapid in its
ap442pearance. It may originate in the sheath either of the psoas or of
the iliacus muscle; more frequently it seems to form behind these, and
is connected with diseased bone. The precursory symptoms are often
not particularly attended to; these are rigors and pain of the loins.
As the disease advances, the patient feels great pain in the erect
position, and in general the pain is aggravated by extending the thigh.
Thickening and slight glandular enlargement takes place in the groin;
there is an evident fulness there; and then swelling appears on the
inner side of the femoral vessels, beneath the pubal portion of the
fascia lata. This swelling is more prominent in the erect position,
and is also increased by exertion of the abdominal muscles; an impulse
is given to it on coughing. As it advances, and comes more to the
surface, fluctuation is perceived. This is the most common site in
which the abscess presents itself; but it is not unfrequently met with
on the outside of the vessels, either lower or higher in the thigh,
above Poupart’s ligament, in the loins over the crest of the ilium,
and occasionally the matter is insinuated under the pelvic fascia and
appears by the side of the anus. Large and neglected collections may
work their way to the surface in two or three of these situations at
the same time.
The disease is often attributable to a sprain or wrench of the loins,
or to exposure to cold and over-fatigue. Occasionally the mischief is
confined entirely to the soft parts; the vertebræ, a portion of the os
innominatum, or the sacrum, may be denuded and of irregular surface,
but this is evidently the result of the pressure of the abscess. A
striking example of this, and of the extensive destruction of parts
which this affection sometimes produces, may be shortly stated.—A very
large lumbar abscess formed within a few weeks, in consequence of
great and continued fatigue and exposure to bad weather. At first it
had been trifled with. At last it was opened in the usual situation in
the thigh, and a vast quantity of matter evacuated. Thirty-six hours
afterwards, the patient was suddenly suffocated by a flow of purulent
matter into and through the air passages. On dissection, the cavity
of the abscess was found to be immense, opening through the diaphragm
into the lung which was adherent, and communicating with the bronchi.
The forepart of the lumbar vertebræ was exposed, and in some parts
stripped of the theca; but there were no cavities in the bone, and no
disease of the interposed cartilages. Such cases are now and then met
with, of abscess in the loins not originating in any vice either of
the bones or of any other part of the apparatus of the spinal column.
Most frequently, however, the collections have their foundation
in ulceration of the bodies of the vertebræ. The patient has had
tenderness in the part, weakness of the back and of the lower limbs,
and increase of pain on pressing or striking some particular spinous
processes—perhaps slight excurvation. Then pain in extending the thigh
supervenes, followed by swelling and other signs of abscess. This is
preceded generally by deposit of tubercular matter in their cancellated
texture. Sometimes the disease seems to originate in the ligaments
and articulating surfaces; occasionally portions of443 the bone perish,
 and are found lying in the cavity of the abscess, as seen in this
specimen, taken from a young subject. When the bodies of the vertebræ
are attacked by ulcerative absorption, and sometimes the disease is
very extensive, involving perhaps four, five, or six of the bones,
there is more or less curvature of the spine outwardly—excurvation.
If the disease affects one or two bones, and their bodies are almost
destroyed, then the projection is sharp and angular. When the disease
is more extensive the curve is greater, and more gradual ulceration
sometimes exists to a considerable extent in one articulation, without
change of form externally in the spinal column, and sometimes without
any great collection of pus. When curvature commences there is very
generally more or less weakness of the limbs, though curvature,
whether from ulceration or interstitial absorption, is by no means of
necessity attended by any degree of paralysis. The power of motion of
parts supplied by nerves in the neighbourhood of disease is diminished
earlier in general than the sensation, in consequence, possibly, of the
mischief commencing in the anterior part of the bodies of the vertebræ.
It is wonderful to what extent disease may extend in the vertebral
column, without much impairment of the functions of the spinal chord,
and how perfectly the functions are restored in cases where it has
suffered. The lumbar vertebræ are those most fre444quently affected,
but the ulceration may also be either in the dorsal region or in the
pelvis. Disease of the last lumbar vertebra at its connection with
the sacrum, or disease of the sacrum itself, is attended with abscess
around, which descends into the pelvis, displacing the bowel, and
appearing by the side of the buttock.
and are found lying in the cavity of the abscess, as seen in this
specimen, taken from a young subject. When the bodies of the vertebræ
are attacked by ulcerative absorption, and sometimes the disease is
very extensive, involving perhaps four, five, or six of the bones,
there is more or less curvature of the spine outwardly—excurvation.
If the disease affects one or two bones, and their bodies are almost
destroyed, then the projection is sharp and angular. When the disease
is more extensive the curve is greater, and more gradual ulceration
sometimes exists to a considerable extent in one articulation, without
change of form externally in the spinal column, and sometimes without
any great collection of pus. When curvature commences there is very
generally more or less weakness of the limbs, though curvature,
whether from ulceration or interstitial absorption, is by no means of
necessity attended by any degree of paralysis. The power of motion of
parts supplied by nerves in the neighbourhood of disease is diminished
earlier in general than the sensation, in consequence, possibly, of the
mischief commencing in the anterior part of the bodies of the vertebræ.
It is wonderful to what extent disease may extend in the vertebral
column, without much impairment of the functions of the spinal chord,
and how perfectly the functions are restored in cases where it has
suffered. The lumbar vertebræ are those most fre444quently affected,
but the ulceration may also be either in the dorsal region or in the
pelvis. Disease of the last lumbar vertebra at its connection with
the sacrum, or disease of the sacrum itself, is attended with abscess
around, which descends into the pelvis, displacing the bowel, and
appearing by the side of the buttock.
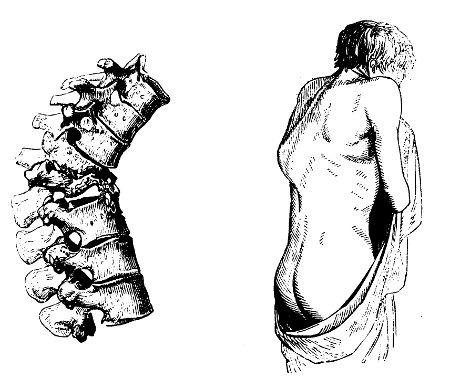
Such abscesses may have been allowed to come to the surface, and to
discharge their contents spontaneously; or they may have been at
a late period opened either at one point or at several. In these
circumstances, the discharge is generally profuse, long-continued, and
attended with exhaustion and hectic, gradually but surely destroying
the patient. But, by good management, a perfect and permanent recovery
may in many cases be obtained. When the vertebræ are affected, absolute
rest must be enjoined and enforced; and a drain is to be established
by the sides of the spinous processes, either by moxa, potass, or
seton—it is immaterial which. The discharge is kept up by occasionally
dressing the issue for a few hours with an acrid ointment, so as to
reproduce a slough. When the abscess begins to present, it should be
opened as early as possible, and a free exit allowed to the matter; the
discharge should be at no time confined. The opening of the cavity, and
again shutting it up, however carefully conducted, is in almost every
instance followed by alarming and hazardous results. Rapid accumulation
of putrid and bloody matter takes place, and air is extricated within
the cavity; the vessels of the cyst, being unsupported, part with
their contents; irritative fever is lighted up, with rapid pulse,
anxious countenance, and delirium. These symptoms are relieved only
by immediate evacuation of the fluid. Some slight constitutional
disturbance follows the making of a free opening, but quickly subsides;
then the discharge improves in quality, becomes more pure and unmixed,
diminishes in quantity, and gradually ceases. During the discharge the
strength requires support; and the attention to the original mischief
must not be neglected or intermitted.
Spina Bifida is a congenital fluctuating tumour, with deficiency of
the subjacent vertebræ. It is usually situated in the lumbar region,
sometimes in the dorsal, and often over the sacrum. The size of the
swelling varies according to the age of the child, and the extent of
deficiency in the parietes of the spinal canal. The spinous processes
are either imperfect or altogether wanting, and over the space so
formed the tumour is situated. Its contents are usually of a serous
character, thin and colourless; sometimes they are turbid and flaky.
The parietes seem to be a continuation, or protrusion, of the membranes
of the spinal chord, thickened and somewhat altered in structure,
and usually in close contact with and adherent to the integuments.
By pressure the size of the tumour is diminished; but, if firm or
long continued, unpleasant effects are apt to result. There is often
debility of the lower limbs, and the disease is not unfrequently
coexistent with hydrocephalus. Children with this affection seldom live
more than a few years.
The application of gentle, uniform, and continued pressure affords
support to the parts, and prevents increase of the tumour; and, under
this palliative treatment, life may be both rendered more comfortable445
and prolonged. It has been proposed to combine continued pressure with
occasional puncturing of the cyst by means of a fine needle, with
the view of diminishing the tumour and ultimately obtaining entire
obliteration of the cyst. The practice has been made trial of, and the
result may warrant repetition; caution, however, is necessary, for the
too free opening of the tumour is often followed by a rapidly fatal
issue. A case occurred to me not long since, in which the tumour, of
large size, was situated over the sacrum. The fluid was evacuated by a
small trocar and canula, the parietes shrank, and a very satisfactory
cure resulted.
AFFECTIONS OF THE RECTUM AND NEIGHBOURING PARTS.
Of Hemorrhoids or Piles.—Piles are blind, furnishing no discharge,
except a mucous or puriform fluid; or open, pouring out a greater
or less quantity of blood from time to time. They are usually of
small size, invested by the mucous membrane, thickened, congested,
and consequently of a dark colour; and either within the sphincter
or projecting externally. Internally, they may sometimes consist of
blood, coagulated or not, effused between the mucous and muscular coats
of the intestine; but in general their inner structure is venous,
at least in the first instance. Branches of the hemorrhoidal veins,
ramifying near the inner surface of the gut, become varicose, probably
from their superior trunks being compressed by hardened feculent
matter or other obstructions. The varix protrudes the superimposed
mucous membrane; and at first the excrescence is composed of the
dilated venous trunks containing fluid blood, and invested by the
membrane, which inflames, thickens, loses its villous character, and
discharges a vitiated secretion. In this stage the tumour is easily
compressible, and by pressure may be made to disappear almost entirely,
the communications between the varicose vessels and the trunks above
being still unobstructed. But inflammatory action is soon kindled in
the incommoded venous branches, as frequently happens in varix of
the lower extremities; their coats become changed, are thickened,
effuse lymph externally and internally, adhere to one another, and
are ultimately matted into one confused and solid mass; the contained
blood coagulates, becomes fibrinous, the whole tumour feels hard and
firm, and often is exceedingly painful. At length all traces of venous
structure disappear; the tumour seems to consist chiefly of effused
lymph, condensed cellular tissue, and coagula.
In not a few instances, however, the contents of the veins remain
partially fluid, and a communication exists between the vessels of the
tumour and those of the surrounding parts.
That such is the usual structure of piles I am convinced, from repeated
and careful dissection of the tumours.48
446
The neighbouring parts often swell and inflame. Sometimes one or two
tumours only exist; or they occur in numbers, clustered together, and
form a large irregular mass, inflamed, and often ulcerated. Acute
pain is experienced in the part, when touched and after straining at
stool; by straining too, such as are attached within the sphincter are
pushed out, together with folds of the mucous membrane, and, if allowed
to remain, are constricted by the sphincter, swell in consequence,
ulcerate or slough, and discharge blood. The bleeding often is very
violent in such cases, or when the tumour is punctured; the blood
flowing in great quantity, and in a rapid stream. The hemorrhage is
often periodical, both in males and females; in the latter, it would
seem occasionally to take the place of the menstrual flux. The soft
bluish tumours that are compressible, and fluctuate when large, furnish
blood more readily and profusely than the hard and tuberculated.
Much irritation is produced by piles, and some of them are more
irritable than others. There are often extensive excoriation of the
nates around, and profuse discharge from the raw parts, particularly
when the tumours are external. In such cases, flat, hard, warty
excrescences often form in the cleft of the nates, and increase the
irritation; and these are termed fici, mariscæ, and condylomata.
In internal piles, a frequent desire to go to stool is induced, and
more or less of the mucous coat of the rectum is protruded and swollen.
The tumour, along with the protruded portion of bowel, may become
strangulated if not replaced. By such or other causes inflammation is
excited, which often extends to the neighbouring parts, and terminates
in abscess; but this is not so apt to occur from tumours seated high in
the rectum as from those about the verge of the anus.
447
The usual cause of piles is obstruction to the return of blood in the
hemorrhoidal veins; and this may be occasioned by advanced pregnancy,
habitual distension of the colon and sigmoid flexure, with hardened
feces, or tumours of the abdominal viscera.
Inflammation of the Rectum is attended with excruciating pain,
burning heat, and a feeling of contraction, increased very much when
the parts are thrown into action by evacuation of the contents of the
bowel, or of the bladder. The heat may be felt on introducing the
finger, with the view of examination; by doing so, dreadful torture is
produced, and such manipulation should not be had recourse to unless
there is a suspicion of foreign matter lodging in the part, by removal
of which the action might be cut short. The bladder is often affected
sympathetically; there may be frequent desire to empty it, or else
retention of its contents: this latter occurrence not unfrequently
follows operations on the bowel, as for the removal of hemorrhoids,
by ligature or extensive incision, which is neither warrantable nor
requisite. The inflammation extends to the cellular tissue round the
rectum, with swelling and increased pain; the pain is aggravated by
pressure, and the patient is unable to sit erect. As the painful
symptoms abate, puriform discharge from the membrane of the gut takes
place, and often is very profuse. The morbid action sometimes extends
to the other intestines, attended after a time with mucous or even
bloody evacuations. When the affection is confined to the rectum, the
feces and vitiated secretion are distinct from each other, and the
former are usually of their natural appearance; but when the other
intestines participate, to a greater or less extent, the feces are
fluid, and intimately mixed with the morbid secretion.
Ulceration of the mucous coat, with continued discharge, often
supervenes. Sometimes the peritoneal coat of the bowel is affected
secondarily, and then the pain is much more acute and more aggravated
by pressure.
Patients affected with hemorrhoidal swellings,—the action of whose
bowels is irregular, and in whom the vessels about the anus are
congested,—are peculiarly liable to inflammation and abscess in the
rectum or its neighbourhood, from the application of cold or wet to the
surface, particularly that of the lower part of the body. Ascarides
often produce violent irritation in the extremity of the rectum, both
in children and in adults; and the morbid excitation is communicated
to the bladder, as will afterwards be noticed. Not unfrequently the
inflammation is induced by a foreign body, either lodging in the cavity
of the bowel or imbedded in its coats—as hardened feculent matter,
alvine and biliary concretions, bones of small animals, needles, pins.
Effusion often takes place into the loose cellular tissue round
the bowel, with hard swelling, followed by unhealthy and extensive
suppuration. Rigors generally precede the formation of matter, and
violent fever almost always attends, abating, along with all the
painful feelings, on evacuation of the fluid. Still the discharge
continues, and the patient is kept uncomfortable and unhappy.
Resolution can448 very rarely be produced; suppuration is the almost
uniform termination of the action, and in persons of bad habit this
sometimes occurs in these parts without any assignable cause, and
without previous warning. The purulent collections are often very
extensive, both externally and internally, the integuments are all
undermined, and in some cases it is difficult to ascertain the depth of
the abscess, even with the aid of a long probe.
Owing to the loose nature of the texture surrounding the gut, abscesses
near the anus often attain a great size, and extend deeply before
there is much external indication of their existence; a hardness is
felt on pressing the fingers deeply by the side of the tuberosity of
the ischium; this is at first obscure, but gradually becomes more
developed; and at last a small dark red spot appears, indicating that
the matter has approached the surface, and is most superficial at that
part. But the surgeon should not wait for the pointing here, as the
matter may burrow much previously, and abscess form in the substance
of the sphincter, or exterior to it. If the matter does not cause
ulceration of the coats of the intestine, and escape into its cavity,
pointing takes place, and the pus is discharged externally, in general
through a small opening. The matter is of a very offensive odour. The
external aperture, and even the whole cavity of the abscess, may be at
a distance from the gut, but in most cases the matter is close to it:
its coats are denuded, and often ulcerated through. The surrounding
degree of induration, the quantity of contained matter, the extent of
the cavity, and the situation of the opening, vary almost in every
instance.
Cases occur of induration, often very extensive, in the neighbourhood
of the anus, on one or both sides, with dark discoloration of the
integuments, and burning pain. The affection resembles carbuncle.
The precursory symptoms are soon followed by partial suppuration,
and extensive sloughing of the cellular tissue. At first there is
excitement of the system, but symptoms of debility, and flagging of
the vital powers, soon present themselves—irregular pulse, delirium,
disordered stomach, hiccough, vomiting, and cold extremities. The
disease is one of great danger, and the patient can be saved only by
free and early incision, and the judicious employment of stimulants.
In some instances the inflammation is merely superficial, seated merely
in the integuments, and followed by slow collection of matter.
It is indeed seldom that a cavity formed by abscess near the anus
fills up entirely, however large and free the opening into it may have
been. The parietes contract, but the hardness around is not entirely
dissipated; the opening may close for a little while, but is soon found
again discharging, and may continue to do so for months or years. A
sinus is thus formed. Fresh collections and openings, either externally
or internally, are apt to occur, with extensive induration of the
cellular tissue, and disease of the gut. Instead of a single sinus, a
number of collateral ones are formed, all running into the main canal,
like branches to a common-sewer, or by-lanes opening into one spacious
street. The disease is one of frequent occurrence449 amongst females; and
often from a false sense of delicacy its existence is not declared till
it has advanced to a state of truly horrible perfection.
Fistula is generally the consequence of abscess in the cellular
substance near the anus. By the term is understood a sinus or track,
with narrow orifice and hard parietes, discharging thin gleety matter.
If the track extends from the cavity of the gut to the surface, flatus
must often pass through the narrow and tortuous canal, and, from a
peculiar noise being produced by its passage, the name of Fistula has
probably been adopted. The term cannot be properly applied to recent
cavities of abscesses, but only when their sacs have contracted,
their lining has become callous, and their discharge thin and almost
colourless.
The fistula may be one of three varieties—blind external, blind
internal, complete. The first denoting that the sinus opens externally,
but does not communicate, either at its origin or elsewhere, with the
cavity of the bowel. The second, that it communicates with the bowel,
but does not open externally. The last, that it both communicates
with the bowel and opens externally. Some contend that fistulæ are
always complete, that they commence from within, and that the internal
opening is always at one particular point; but such, according to my
experience, is far from being the case.
Fistulæ occur in children, though rarely; generally in people advanced
in life. The cavity of the sinus, after long continuance, becomes
coated with an expansion resembling mucous membrane, and secretes a
discharge of mucous character.
In every case, it is necessary that the surgeon should ascertain, as
accurately as possible, the extent and nature of the fistula; and,
with this view, examination with the probe is requisite. The probe is
introduced into the canal, when the fistula is an external one, and
directed through its windings, so as to discover its direction, length,
and divarications; the guidance of the instrument is facilitated,
and the information augmented, by the forefinger being placed in the
rectum. Sometimes all the by-paths cannot be detected, until the
orifice of the canal is enlarged. When the fistula is complete, the
probe, entered at the external extremity, can be passed into the bowel
so as to be felt by the finger in the rectum; but it must be remembered
that the internal opening is not always at the inner termination of
the sinus, but often seated more externally—the cellular tissue being
destroyed to a considerable extent above it, so as to form a large
unhealthy abscess, communicating with the main track of the fistula.
But the gut may not be opened into, though denuded to a large extent,
and forming part of the walls of the sinus; and in some instances, the
sinus may not come within a considerable distance of the bowel.
An internal fistula is more difficult of detection. The symptoms
leading to a suspicion of its existence are—puriform discharge from
the bowel, increased on going to stool, and then accompanied with
tenesmus; pressure on the side of the anus, causing pain, and sometimes
an augmentation of discharge; and in many instances hardness, deeply
seated, is felt. On introducing the finger into the rectum, the
aper450ture in the coats of the bowel is perceived, or a part of the
bowel feels more boggy and tender than the rest; through this point
a curved probe, introduced along the finger, may be passed into the
sinus, and being then directed downwards, reaches the outer extremity
of the canal, causes the integuments to project, or is readily felt
from the surface. The internal opening is usually immediately within
the sphincter, seldom higher.49 The discharge, in general, is
rather profuse, the bowel is very irritable, desire to evacuate it
is frequent, and the feces are often tinged with blood. There is a
sensation of itching about the fundament, the heat of the parts is
felt by the patient to be increased, he is unable to bear pressure
there, and sits on one buttock: in most cases the bladder sympathises
considerably. The giving way of the bowel may be produced by ulceration
commencing in the mucous membrane, but is more frequently the result of
inflammatory action in the surrounding cellular tissue. The aperture
is the seat of acute pain when pressed upon, and during evacuation
of the bowel. Great light is thrown on such cases by the use of a
proper speculum. But its introduction can seldom be borne in cases
of inflammation, abscess, or recent fistula. In ulceration of the
coats within the sphincter it is useful. Considerable information
can certainly be obtained by the finger; but to the sense of touch,
however acute, it is better, when admissible, to add that of vision.
The speculum, made of silver or steel, and having its internal surface
highly polished, is introduced gently into the anus, and expanded
fully; and by changing the situation of the instrument, and holding a
light so as to illuminate the interior, the surface of the bowel for
five or six inches above the anus can be examined accurately, as if it
were an external part of the body.
Simple indurations and contractions of the lower part of the bowel
follow long-continued irritation and inflammation of its parietes. The
part is not an uncommon seat of stricture, and sometimes the bowel is
constricted at two or more points near each other; frequently the451
stricture is extensive and firm, in other cases it is narrow,
consisting merely of a thin band. It is often complicated with fistula;
if so, the internal aperture is immediately above the stricture, and
is caused by ulceration; abscess sometimes forms above the stricture,
destroys the coats of the bowel at that point, burrows around, and not
unfrequently points at a great distance from its origin; or sloughing
and ulceration may take place in the coats of the bowel, and feculent
matter be discharged through the opening of the abscess. In females,
the vagina may be opened into in consequence of unhealthy suppuration
in the cellular tissue, between that organ and the gut.
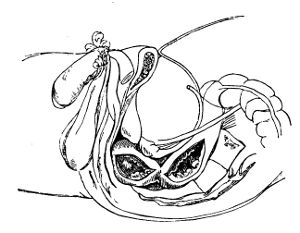
The existence of stricture is in general readily ascertained by
examination with the finger; its most common situation is here shown;
the medical practitioner must not suppose that every obstruction,
however slight, to the passage of a bougie into the bowel is owing to
organic disease; the top of the sacrum naturally projecting forwards
on the commencement of the rectum, in some degree opposes the entrance
of any large body, and this circumstance is laid hold of by the
unprincipled or ignorant; the patient is very often declared to labour
under stricture of the bowel, when none exists. Some practitioners
discover stricture in almost every patient with disordered digestion;
the whole digestive apparatus is certainly thrown into disorder by
obstruction in the lower part, but this obstruction is fortunately
rare. In cases of tight stricture, the bowels are distended with feces
and flatus; and if evacuation is not procured vomiting ensues, followed
by enteritic symptoms, as in strangulation of the higher bowels. The
gut above the stricture is always more or less dilated.
The symptoms which lead the surgeon to suspect the existence of
stricture, are—difficulty in voiding the excrements; a long time
occupied in the evacuation, with pain and much straining; small thin
portions of feculent matter coming away, when the matter is consistent;
discharge of puriform fluid, mixed with a slimy mucus; itching and heat
in the parts; and irritability of the urinary organs.
Strictures of the urethra and rectum often coexist, as exemplified
by452 the following case:—A middle-aged man, when in Holland, laboured
under a very deep and extensive fistula in ano. Sinuses were divided in
all directions, and some healed; one, however, remained open, leading
towards the gut from near the tuberosity of the ischium on the left
side. He was desired to keep this open by means of bougies, which,
as many were used, he manufactured himself out of cloth and plaster.
On one occasion a portion passed deeply, and could not be extracted;
but his alarm at this occurrence was appeased on being told that the
foreign body would be absorbed. His condition at that time was very
miserable; and inflammation was often excited in the parts, with fresh
collections of matter. At the same time, he laboured under stricture
of the rectum and urethra. He applied to me fifteen years after the
commencement of the disease. Then the most troublesome symptom was a
constant itching in the perineum, and round the anus, preventing sleep,
and causing much excoriation from involuntary scratching; besides, he
was annoyed by seminal emissions, and frequent desire to make water.
I first divided a small internal fistula, and some time afterwards
operated on a large complete one; in the latter instance, a foreign
body was felt deep in the wound, the incision was extended, and a large
portion of bougie, firmly impacted, was with some difficulty withdrawn.
Some days after, other portions of bougie were extracted along with
numerous hairs; and these continued to be discharged for many weeks.
The symptoms were much relieved. An occasional itching remained, but
disappeared after the cure of a very bad stricture in the urethra. He
recovered perfectly from the complication of diseases.
Schirro-contracted Rectum, a malignant and truly horrible disease,
may be the consequence of inflammatory action, or of neglected
stricture. The neighbouring parts are involved in cartilaginous
induration; the surface of the bowel is lobulated and ulcerated, its
cavity is contracted, and the discharge is profuse, sanious, bloody,
and putrid; there is frequent desire to void the contents of the gut,
but in general nothing but flatus and puriform fluid is evacuated;
when feces do pass, dreadful pain is excited, and continues for some
time. The difficulty of voiding feculent matter becomes greater and
greater, frequent attacks of ileus occur, and in one of them the
patient expires. During the progress of the disease, the functions of
the bladder become disturbed; change of structure in it and in the
vagina takes place; and frequently the cavities of the rectum, bladder,
and vagina are laid into one by inveterate and malignant ulceration.
The affection is more common in females than in males, and rarely
occurs in young persons. The countenance has the sallow hue peculiar to
carcinoma, and in the advanced form of the disease becomes still more
cadaverous from profuse discharge of matter and frequent hemorrhage.
The cellular tissue, anterior to the rectum, is liable to become the
seat of tumour. Malignant medullary formations occasionally form here,
causing most distressing symptoms; by displacing the bowel they may
obstruct its canal, and simulate stricture or schirro-contraction.
453
Prolapsus Ani. Folds of the lining membrane of the lower portion of
the rectum are apt to protrude during evacuation, as already mentioned,
in those labouring under hemorrhoids. These are readily replaced,
and the painful feelings relieved, if the attempt be made before
swelling and engorgement of the vessels and cellular tissue take place.
Protrusion, however, is sometimes to a great extent; the sphincter is
relaxed, and the lower part of the bowel is retained within it with
difficulty; indeed there is often more of the lining membrane of the
gut without the sphincter than within it. The mucous lining becomes
insensible, thickened, and white; and the patient is subject to attacks
of inflammation, with additional swelling, excoriations, and ulcers
of the parts. Slight protrusion is very common, and patients who
have long laboured under it are in the habit of reducing the bowel
after every stool, in the intervals wearing a supporting bandage.
They are subject, however, to constant uneasiness, and more or less
puriform discharge from the parts; often there is a flow of blood
while at stool; the health is undermined, and comfort diminished;
all exertions are gone through with difficulty, and undertaken with
reluctance. During exertion protrusion is almost certain to occur, and
apt to be increased. The part most commonly prolapsed in time becomes
hard, thick, and in a measure insensible; and new folds appear on
extraordinary straining at stool, in coughing, or any exertion of the
abdominal muscles.
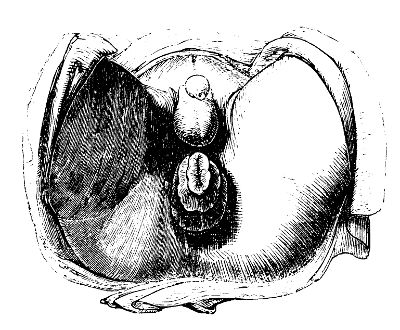
Tumours occasionally grow from the coats of the rectum, and are of
various consistence. They may be either vascular, or deposited in
consequence of increased vascular action, and afterwards increased by
addition of solid matter. They are to be removed either by ligature or
incision, according to their situation, nature, and attachments.
Foreign bodies may lodge in the rectum—as bones, portions of454 hard
indigestible meat, &c., introduced by the mouth—or clyster-pipes,
bougies, &c., which have been passed up per anum. From being the source
of constant irritation, and obstructing the functions of the part,
they demand removal. Alvine concretions are now rare; they are usually
situated in the caput cæcum coli, sometimes in the sigmoid flexure, or
in the arch of the colon; they may descend into the rectum, and lodge
there.
Children are sometimes born with the anus imperforate, the extremity of
the rectum being covered merely by integument, or the bowel terminating
an inch or two above the usual site of the anus; or the rectum may be
wholly deficient. In the last case, the colon may end in a blind sac at
the fundus of the bladder, or it may open either into that viscus or
into the vagina.
Treatment of Affections of the Rectum.—In the treatment of
hemorrhoids, the cause should be removed if possible; and this may
suffice for the cure. When the tumours are recent and small, they may
be made to disappear by the use of astringent ointments or decoctions,
as of galls, kino, oak-bark, and by sedulous attention to cleanliness
of the part. In inflamed tumours, blood may be extracted by leeches or
punctures, and hot fomentations afterwards used. Recent hemorrhoids are
sometimes got rid of at once by the puncture of a lancet,50 by which
a clot of grumous blood is discharged, with immediate subsidence of
the swelling, and abatement of pain. When constriction of the internal
tumours or folds of bowel by the sphincter has occurred, the tumour
should be replaced if possible. In irritability of the sphincter, a
bougie is sometimes used with advantage; and incision of the muscle,
by which rest is afforded to the parts, will often effect a cure,
after the failure of all other means: this is essential when rugged
ulcers or fissures occupy the orifice; the division may be made on
either side, certainly not in the mesial line. In most cases, the
tumour must be got rid of by the knife or ligature. When the piles are
internal, removal by ligature is to be preferred; the patient being
made to strain, and thereby bring the tumours as low as possible, a
ligature is placed round the base of the swelling, provided its form
conveniently admits of it; otherwise the base is pierced by a fixed
needle armed with a double ligature, the separate portions of which are
applied tightly to the corresponding parts of the base. This operation
is very inconsiderately and indiscriminately employed. It can only be
warrantable when the tumours are so large as to obstruct the orifice so
perfectly as to prevent evacuation, unless they are extruded. Before
proceeding to this measure, the 455bowels should be emptied by mild and
repeated purgatives, and afterwards all stimuli should be avoided.
It is imprudent to apply ligature to several tumours at once, for
serious consequences will most probably ensue, inflammation of the
bowel, obstinate constipation, and general excitement.51 Excision of
such piles is contraindicated by the risk of profuse hemorrhage. The
bleeding is into the cavity of the bowel, a coagulum is there formed
which encourages the flow; and from this cause, and the peculiar
situation of the bleeding point, it is with difficulty arrested. When
the tumours are external, ligature may certainly be adopted; but
here there is no objection to the use of the knife, and excision is
much less painful and more speedy. The tumours, along with protruded
portions of the mucous lining of the rectum that cannot be reduced,
and are changed in structure and function, are readily taken away by
the rapid stroke of sharp curved scissors. Or they may be laid hold
of and stretched, and their base divided by one or more sweeps of a
bistoury. The removal of these tumours, or of a portion of the loose
fold of skin or altered mucous membrane which occupies the sphincter
in the direction of the bowel, is in general followed by a cure of the
prolapsus. The sphincter now acts fully, and on the cicatrisation of
the open surface contraction of the tissues occurs to such an extent
as to produce a permanent cure without interference with the internal
parts. Should hemorrhage follow upon the removal of external tumours or
folds, the surgeon has it completely under command. Pressure by a large
graduated compress is generally sufficient.
In inflammation of the rectum, the exciting cause often is not
discovered; when detected it should be removed without delay. In
simple inflammation of the part with violent fever, general bleeding
may be required; and in all cases blood should be abstracted locally
and freely. Leeches are to be applied to the verge of the anus, and
the lower part of the perineum, and hot fomentations afterwards used.
Internal antiphlogistics are at the same time not to be neglected.
In retention of urine, or great irritability of the bladder, in
consequence of the affection of the rectum, the perineum should be
leeched and fomented, perhaps, also, the lower part of the abdomen;
the use of the catheter should be avoided if possible. When induration
takes place in the cellular tissue by the side of the anus, or in the
perineum, suppuration must in all probability occur, and poultices,
with occasional fomentation, are to be used, though only for a 456short
time; for, as already mentioned, pointing of the matter is not to be
waited for in this situation; incision must be had recourse to early,
in order to prevent bad consequences. Leeching is sometimes used here,
as in purulent formations in other parts, from gross ignorance of the
real state of matters; and sometimes their use is continued after
fluctuation is distinct, and until the pus begins to ooze through the
leech-bites; such is very useless and very dangerous practice; in most
cases the internal parts are extensively destroyed before the matter
comes spontaneously to the surface.
In the carbunculous state of the cellular tissue, near the rectum, with
extensive infiltration, dark integument, and a tendency to sloughing,
an early and free opening must be made wherever matter is suspected
to have formed, however deeply seated, and in whatever quantity, and
whether the parts are indurated or not; nothing but mischief can result
from delay. When the cellular substance is destroyed, the incision
must be proportionally extensive, to afford a free exit for slough
as well as matter. During the suppuration which follows, the system
will require good support, and most probably a free administration of
stimuli.
It has been recommended that, in abscess extending along the gut, the
cavities of the bowel and abscess should be at once laid into one by
incision. I have done so, but always found the cure to be tedious. It
is better that the matter should first be evacuated through an external
opening, that the painful symptoms and constitutional disturbance
should be allowed to subside; and that after the cavity has contracted,
and the extent of the sinus has been ascertained, the operation should
be performed. In the operation the knife is now employed; but in former
times the ligature and cautery were in constant use. The old surgeons
supposed that there was something malignant in the hardness and
callosity attending this disease, and were not contented with opening
the cavities, but endeavoured to dissect out the whole parts; and, if
foiled in this, they finished the work with a red-hot iron. Indeed the
practice of excision was recently in vogue in the Parisian hospitals.
But the operation for fistula has been much simplified. The bowel is
generally so much separated from its connexions as to be incapable of
again adhering, or of furnishing granulations; and, though capable,
healing is effectually prevented by the frequent motion of the parts
caused by the action of the sphincter and levator of the anus. One
side of the cavity is fixed, whilst the other is in motion. It becomes
necessary to lay the cavities of the bowel and of the fistula into one.
This can generally be effected with great ease; a salutary degree of
excitement follows the use of the knife, rest to the parts is procured,
the edges are allowed to retract and adhere to the opposite surface,
and the wound heals quickly from the bottom. The surgeon, in his
operative procedure on these parts, must use both hands equally well,
otherwise he must vary his position, and often put his patient in a
very awkward predicament, more particularly if a female. The patient
is placed in a stooping posture, with the legs unbent, or kneeling on
a chair, and resting his arms on its back, the fundament being turned
towards the light. The surgeon inserts457 the finger, well soaped and
oiled, into the rectum, and with the other hand insinuates a curved
probe-pointed bistoury into the sinus, using the instrument merely as
a probe. Having reached the extreme depth of the canal, the direction
of the instrument’s point is changed so as to apply its cutting surface
to the coats of the bowel, at that part. The instrument on being thus
passed into the bowel is fixed by the finger, and by drawing both
outwards, the coats of the bowel and the parts intervening between them
and the sinus are divided. All collateral sinuses extending towards
the perineum and buttock must be freely divided, for they cannot be
expected to contract otherwise. Such is all that is necessary in the
generality of cases; but it is evident that the steps of the operation,
and the extent and number of incisions, must be varied according
to circumstances. A great part of the affected bowel may be pulled
down by a director before being cut, as is sometimes done; but the
practice is useless and painful. Should hemorrhage take place, it may
be restrained by stuffing the wound gently with lint; if this fail,
the bleeding vessels are to be secured by ligature; but this is seldom
necessary. The bowels should be well cleared out before the operation,
so that two or more days may pass over without the parts being required
to perform their functions; and, if the bowels are naturally loose,
opiates may be administered. Afterwards copious evacuation is to be
procured by enemata or gentle laxatives. It is necessary to prevent
the external part of the wound from adhering, until the whole has
contracted equally, and begun to be filled up by granulations from the
bottom; and with this view a piece of lint is interposed between the
margins. Stuffing the wound daily with large dossils of lint, smeared
or not with irritating ointments, is attended with much pain, and
certainly impedes the cure. The dressing should be simple and light,
and introduced with gentleness and care. The first should be allowed
to remain undisturbed till spontaneously discharged along with the
feculent matter. In the greater number of cases, a second interposition
of dressing is all that is required. In all cases, dressing should
not be continued long; but as the cavity gradually contracts,
discharging laudable pus, and becoming coated with healthy florid
granulations, the interposed pledgets should be daily diminished,
and soon omitted entirely. If the surgeon continue long to stuff the
wound it cannot contract, will become callous as before, and a fistula
will be reproduced. Injections into the wound, or the application of
lint soaked in a gently stimulating lotion, are often beneficial in
promoting contraction. But, as already stated, most fistulæ get well
after proper incision, with but one or two dressings, and without any
after application excepting abundance of soap and water. During the
cure, the general health must be kept vigorous, and the state of the
bowels strictly attended to.
In ulcer of the mucous lining, with irritability of action in the
bowel, injections of tepid or cold water are useful, by removing
irritating matters from the part. By means of a speculum ani the
ulcer can be readily exposed; it maybe touched occasionally with the
nitrate of silver, in substance or solution, or, if very indolent,
with a458 solution of the bichloride of mercury. When the irritation is
very great, and the lower part of the bowel frequently in a state of
spasmodic action, the sphincter may be divided so as to allow the parts
to remain quiet; and anodyne suppositories or soothing enemata will
then be used with much greater advantage than previously. To obtain
reparation of breach of structure in any part, rest is a principal part
of the treatment; and in the case of the rectum and other mucous canals
it is preëminently required.
Strictures of the rectum are treated by bougies of wood, plaster, or
elastic gum, introduced at intervals, and gradually enlarged. The
bougie should be smooth in the surface, and rounded at the point;
also slightly curved, so as to suit the figure of the bowel; and
with a narrow neck, so as to remain without the irritation caused by
distention of the sphincter. At first it should be of such a size as
can without much difficulty be pushed past the stricture, and, as this
relaxes, the size of the instrument must be proportionally increased
till it completely fills the bowel when dilated to the natural calibre.
The bougie may at each time be retained from a quarter of an hour to
an hour, according to the feelings of the patient. Suppositories and
enemata are at the same time employed; the latter to clear out the
lower bowels, the former to allay the irritation which accompanies
the disease, and which may be increased temporarily by the bougies.
When the stricture is callous, and will not yield by dilatation, it
may be divided with the knife, and notched at various points of its
circumference; and, when the parts have begun to granulate, recourse to
the bougie will soon effect a cure. When fistula and stricture coexist,
both are got rid of at once by the usual operation for the former, and
by the after treatment peculiar to each.
In malignant contractions of the gut, all that can be done is to
palliate the disease by anodynes, administered by the mouth, or
applied topically. Injections, bland, and occasionally anodyne,
tend to diminish irritation; bougies aggravate the disease. At the
commencement, the diseased parts may be removed by the knife or by
ligature, and relief and exemption follow, at least for a time; but
no operation is warrantable in this or any other cancerous affection,
when the morbid action has gained ground, and the disease is extensive.
Female patients have by some been cruelly treated; the vagina and
diseased bowel have been laid into one loathsome cavity, and though
the patients have continued to pass excrement and discharge through
this cloaca, with the symptoms undiminished, themselves miserable and
obnoxious to others—still such cases have been reported as cures!
In prolapsus ani, the protruded parts are to be carefully reduced,
and kept so by means of a compress supported by a T bandage; often
a spring with a pad is used with advantage. In inflamed prolapsus,
with ulceration of the mucous coat, the patient is confined to the
recumbent posture, and soothing applications employed; and when thus
the irritation has been removed reduction is performed; but the
bowel seldom remains up till after the ulcerations have been healed.
In chronic obstinate cases, the altered parts within the verge are
removed by the knife or scissors with safety; contraction attends
the459 cicatrisation, and so further protrusion, as already noticed, is
prevented.52
By the speculum ani, assisting the eye and finger, the nature and
position of foreign bodies in the rectum are ascertained, and their
removal facilitated. They are to be extracted by the finger, by a
scoop, or by forceps. It has been proposed by some to cut into the
colon from behind, so as to open that part of the bowel which is
unconnected with the peritoneum, when it is distinctly ascertained that
alvine concretions lodge there. This might be put in practice when the
case is clear and the symptoms urgent, but, as already observed, such
foreign bodies are now very rarely met with.
In imperforate anus, when the bowel terminates high, it has been
proposed to cut through the abdominal parietes, and open the sigmoid
flexure, so as to establish an artificial anus. The proceeding is
unwarrantable, both in congenital deficiency and in malignant disease
of the bowel. There is no doubt a possibility of life being thus
prolonged, but it is by no means probable, and scarcely desirable.
In the more common cases, the bowel is opened, and the meconium
evacuated, by a slight and safe incision in the site of the anus.
Even through a considerable depth of soft parts, the impulse of the
fluid in the bowel is distinctly felt during exertion of the abdominal
muscles. If incision through the integuments and cellular tissue
prove insufficient, a sharp-pointed bistoury is pushed onwards in the
direction of the bowel, under the guidance of the forefinger of the
left hand, carefully avoiding the bladder, vagina, and uterus, as also
the vessels within the pelvis. To reach the bowel is an object of
great consequence, yet the risk incurred in its accomplishment must be
considered, and the incisions made within certain limits. The opening
scarcely requires to be kept pervious by the use of bougies, the
functions of the parts being sufficient for the establishment of the
anus.
460
[Persons often suffer from pruritus or itching of the anus, or in the
parts immediately around. The affection is most common in old people,
and in such as are of a weakly constitution. Women who have recently
ceased to menstruate are also prone to it. The exciting causes are
generally ascarides, hemorrhoidal excrescences, and a morbid state of
the alvine secretions. Sometimes the skin around the anus is covered
with an eruption of papulæ, or even tubercles, the former of which are
often attended with vesication and the discharge of a thin, watery,
irritating humour. Patches of a similar description are occasionally
seen on other parts of the cutaneous surface; as the scrotum, thighs,
back, and even the face and neck.
The pruritus, which is often very troublesome on retiring at night, so
much so, indeed, as to prevent the patient from sleeping for hours,
usually subsides after a few months, but is certain to return from the
slightest irregularity in the diet, from fatigue, loss of rest, or
from exposure to heat. “From constant rubbing the skin about the anus
becomes thick, dense, and furrowed, even when there are no hemorhoidal
tumours. The furrows assume a radiated direction, and converge in the
anus; they vary in number from six to ten, and are from a quarter of an
inch to an inch in length.”53
In the treatment of this affection the first object should be to
ascertain, and, if possible, to remove, the exciting cause. Proper
attention should then be paid to the general health, which, as was
before stated, is often much impaired. Under such circumstances tonics
may be demanded, such as iron, bark, or quinine, either alone or
combined with blue-mass, sarsaparilla, or Plummer’s pill. The latter
articles are particularly serviceable when there is an eruption around
the anus. The most useful topical remedies are, a solution of acetate
of lead and laudanum, yellow-wash, the nitrate of silver, and the
ointment of the proto-ioduret of mercury. Cold ablutions also afford
great relief, and are indispensable to the patient’s comfort.
Neuralgia of the rectum, a disease first described, I believe, by
Dr. Montegre, of Paris, in 1812, is occasionally met with. It is most
common in persons of a nervous, irritable temperament, from the age of
thirty to forty-five or fifty, and who are subject to similar attacks
in other parts of the body, particularly the face, stomach, testicle,
or mamma. It is characterised by paroxysms of pain, which is usually
described as of a tearing, burning, or lancinating nature, situated
at the extremity of the rectum, from which it frequently extends to
the sacrum, the loins, pubes, and genito-urinary organs. Defecation
is painful, and the urine is discharged in jets or drops, attended
with a burning or scalding sensation. The attacks commonly subside in
eight or ten hours, but recur with tolerable regularity about the same
period the following morning or evening, though sometimes not until
the second or third day. During the intermissions the patient is, in
great measure, free from pain, and passes his feces and urine without
difficulty. The affection often continues for years, and the paroxysms
are then apt to be more frequent and irregular.
461
A remarkable instance of this disease is given by the late Professor
Bushe. His patient was a middle-aged physician, of active habits, in
tolerable health in other respects, but of a nervous temperament, and
subject to occasional attacks of neuralgia of the face, stomach, and
testicles. Several times a year he would be seized with pain at the
extremity of the rectum and at the pubes, accompanied with frequent
desire to void his urine; sometimes he suffered excruciating torments
at the end of the penis, or posterior part of the urethra. The attacks
generally subsided in twelve or twenty-four hours, and were almost
always either preceded or followed by neuralgia in other situations.
No remedies were of any avail. In another case—that of a nervous
female, thirty-five years of age—the pain was seated over a spot about
the size of a shilling, on the left side of the bowel, less than half
an inch above the verge of the anus. For weeks the pain would almost
wholly subside, when it recurred with extreme violence; her distress
was generally greatest towards evening, and was always much increased
during defecation. Mr. Mayo of London mentions the case of a man who
laboured for several years under paroxysms of neuralgia of the rectum
and the teeth. The attacks came on frequently during the day, without
any assignable cause.
Neuralgia of the rectum, as other parts of the body, is almost
invariably attended with a deranged condition of the digestive
apparatus, and hence a mild but systematic course of purgation
constitutes a primary object in the treatment. On no account should
the rectum be allowed to become distended with fecal matter. After due
attention has been paid to the secretions of the stomach, liver, and
bowels, the best remedies will be quinine, iron, arsenic, strychnine
or nux vomica, stramonium, the warm bath, and blisters to the sacrum.
During the paroxysm, hot fomentations, anodyne injections, and opiate
suppositories will be beneficial. In spite, however, of these and other
means, the disease often continues for years with little mitigation,
baffling the skill of the surgeon, and compelling the patient to spin
out a miserable existence.—ED.]
Affections of the Mucous Membranes of the Urinary and Genital
Organs.—It has been previously observed, that these membranes closely
sympathise with the skin and with the mucous linings of the digestive
organs. Stimulating substances introduced into the stomach frequently
produce irritation of the urinary organs; and if the stimulants be
employed in large quantities, and continued for some time, inflammation
of the mucous membrane, investing the bladder and urethra, will be
induced, with vitiated and increased secretion from the parts. In
children, dentition is a common cause of urinary irritation; and not
unfrequently discharge from the urethra comes on during the cutting of
the teeth. The application of acrid matters, as cantharides, to the
skin, will occasion unpleasant effects in the urinary organs; and these
unpleasant and distressing symptoms often supervene upon disappearance
of cutaneous diseases. In short, the practitioner, in attending to
affections of these parts, must ever bear in mind the close sympathy
which exists between them and the462 external surface, the stomach, and
the intestines, particularly the lower.
Of Gonorrhœa, or Inflammation of the Urethra.—The morbid action is
usually limited to the extremity of the canal, seldom extending more
than two or three inches from the orifice. There is itching and heat
at the orifice, with swelling and redness of the glans, and of the
lips of the urethra, and generally the whole penis appears more full
than natural. When making water, the patient experiences acute heat
and pain, often most agonizing—chiefly referable to the extremity of
the passage, and extending for two or three inches backwards. The
urine is discharged in a small and scattered stream, the anterior part
of the urethra being diminished in calibre by the swollen and turgid
state of its lining membrane. The diminution may be in part caused
by spasm of the muscles surrounding the canal, in consequence of the
morbid excitement in it; or by fear, as the patient dreads making
water, well knowing the excruciating pain which he must in consequence
undergo. During erection, there is great increase of pain. The lips
of the urethra, and the glans around, are often tender, and partially
excoriated through neglect of ablution. There is seldom, if ever, any
breach of structure in the canal; there is discharge of increased and
vitiated secretion, without ulcerative absorption; the matter is poured
out from the relaxed, but entire, mucous membrane.
In severe cases, the erections are abnormal, and attended with much
pain, constituting chordee. This troublesome symptom usually occurs
during the night; the inflamed membrane is stretched, and great
pain is felt along the course of the urethra. From extension of the
inflammation to the vascular tissue around the canal, and effusion of
lymph into it, the penis is bent downwards during erection, the corpus
spongiosum not admitting of so complete distension as the corpora
cavernosa. Sometimes a portion of the spongy body is obliterated
permanently by the effusion, causing deformity of the organ, and
imperfect erection. I have also seen the penis bent to an inconvenient
extent from a similar affection of the corpora cavernosa.
After the uneasy and painful sensations have continued for some time,
puriform matter, of a greenish or yellow colour, is secreted by the
inflamed membrane, and discharged in profusion. The discharge changes
very much as to quantity and quality, according to the intensity of
the action and duration of the disease, and is also modified by the
constitution of the individual. When the discharge is suppressed,
either from the imprudence of the patient, or from bad treatment, the
inflammation is much increased; and when the secretion returns it is
in general thin and bloody. As the disease abates, the matter becomes
thick, ropy, and less abundant, is seen only in the morning, and in
quantity little more than sufficient to glue together the lips of
the orifice; ultimately it loses its whitish or streaked appearance,
becoming clear and colourless. The first attack of the disease is
generally the most severe.
In neglected cases, the prepuce swells, often to a great size463 During
the progress of the gonorrhœa there is always a tendency to serous
infiltration in the prepuce; and if the patient walks much without
supporting the organ, or have the part exposed to friction, swelling
will inevitably take place. From this cause Phymosis and Paraphymosis
are apt to recur—affections that will be afterwards described. The
inguinal glands often enlarge, but such swelling is generally small,
and seldom suppurates.
Induration and enlargement sometimes occur along the urethra from
effusion of lymph, or from obstruction and distention of the lacunæ.
Suppuration may take place at these points, and the matter escape
either into the urethra or externally. Swelling of the lymphatics of
the penis is by no means uncommon in severe or neglected cases of
gonorrhœa; a hard chord, tender, and extremely painful when pressed,
is felt running along the dorsum penis, and terminates in the inguinal
cluster of glands, which are in general also affected. Inflammation
and abscess under the strong tendinous sheath that envelopes the penis
occasionally follows the affection of the lymphatics. The whole penis
swells greatly, with fever and much pain; the matter is confined,
burrows under the unyielding sheath, and appears either at the junction
of the glans and prepuce, or over the symphysis pubis.
Occasionally the inflammation is not confined to the extremity of the
urethra, but pervades its whole extent, in consequence of maltreatment,
neglect, or idiosyncrasy. On this account, abscess in the perineum, or
over that part of the urethra which is covered by the scrotum, is no
uncommon consequence of a badly managed clap; the inflammatory action
extending from the urethra to the cellular texture exterior to it. The
formation of matter is preceded by fever and great pain; the patient
is unable to sit; and occasionally retention of urine takes place.
The part affected feels hard, and extremely painful when pressed; it
gradually softens, and at last fluctuates and points. But if the matter
form deeply, behind the bulb and in the cellular texture beneath the
perineal fascia, or in the situation of Cowper’s glands, it may be a
long time of appearing externally. Fluctuation should never be waited
for; and in most cases there are distinct enough signs of the presence
of matter long before fluctuation can be felt.
Some people are much more liable to inflammation of the urethra than
others, and many are exposed to the ordinary causes of gonorrhœa
without suffering, whilst perhaps they are readily affected by such
animal poisons as produce disease of the prepuce and glans. Patients
often give very ridiculous accounts of the way in which their clap was
contracted. They will say that the infection was received in a common
necessary, that the disease was produced by a blow, by a strain of the
back, by taking drugs that did not agree with them, by drinking out
of the same cup or smoking the same pipe with an affected person, by
wearing tight boots, falling into a dirty pond, &c. They will exert
their ingenuity to the utmost, in order to deceive their surgeon, and
attempt preserving their moral character untainted. Discharge from the
urethra may be occasioned by dentition, &c., as already mentioned;
or may take place from calculi passing along and464 getting fixed in
the urethra, or from irritations about the anus. Inflammation of the
passage not unfrequently arises, to a greater or less extent, from the
acrimonious condition of the urine. The most common cause, however,
is the application of irritating matter to the lining membrane;
and this may take place during coition with females suffering from
leucorrhœa, or during their menstrual discharge; but gonorrhœal matter
is the specific virus, and the application of it to the orifice of
the urethra is by far the most frequent cause of inflammation of the
canal. Irritating substances injected into the passage may, and often
do, produce or aggravate the inflammatory action. Besides all this,
irritability of the urethra is common in gouty individuals.
Gonorrhœa has been termed virulent when caused by gonorrhœal
infection—simple, when induced by irritations such as those previously
enumerated; the distinction is seldom attended to, and is of no
practical importance. It has been supposed that the poison which
produces chancre is the same with that which gives rise to gonorrhœa,
the action being modified by the texture in which the virus is lodged:
such an opinion has been found to be wholly untenable.
Gonorrhœa supervenes at various periods after exposure to the
infection, from twenty-four hours to six or eight weeks, but generally
in from ten to twenty days; often the time cannot be correctly
ascertained; much depends on the idiosyncratic susceptibility of the
urethra, on the degree of acridity in the matter applied, and other
contingent circumstances.
When the discharge becomes more clear and thin, and the inflammatory
symptoms have disappeared, the disease is termed Gleet. The passage
remains contracted in some degree, from relaxation of the mucous
surface; there is a desire to make water more frequently than usual,
and the urine is passed in a tortuous or scattered stream; in many
cases the discharge continues profuse. There is now no pain nor
scalding during the passage of urine, but these are readily reinduced
by slight excess; perhaps there is a trifling chordee. After connexion,
the discharge returns as if fresh infection had been caught, though
such be not the case; both in simple gleet, and in that attending
stricture, the seemingly virulent symptoms come on speedily, often
appearing within a few hours after the coitus. In gleet the matter is
no longer green or yellow, but whitish and flaky; the globules are
contained in a mucous instead of a serous fluid. The disease is usually
attendant on stricture, but occurs frequently without any organised
contraction, the discharge being furnished by the vessels of the
surface, which have become weak and relaxed in consequence of previous
excited action. In feeble constitutions, inflammation of the urethra is
almost always followed by long-continued and intractable discharge.
A practitioner is not unfrequently asked when the infection of
gonorrhœa is not communicable, and if an individual in whom the
discharge is very slight, or has just disappeared, is likely to
contaminate a healthy female. The question is a difficult one to
answer. In general it is prudent to err, if at all, on the safe side—by
expressing doubts, and dissuading from intercourse until all discharge
shall465 have entirely ceased for a considerable time. Discharge is
often brought back, as already observed, by the excitement of sexual
connexion.
In simple inflammation of the urethra, with discharge, little or
no treatment is required; if the patient keep quiet, and avoid the
causes which give rise to the affection, the symptoms will disappear
in a short time. But virulent gonorrhœa is often very unmanageable,
particularly if it has been allowed to follow its own course, and
consequently to make head before it is attacked. It is no easy
matter to arrest it after the parts have got into the habit of
furnishing discharge, and particularly if it has been aggravated by
thoughtlessness and imprudence of the patient. All violent exercise
should be avoided, as also indulgence in venery and liquors. A great
variety of remedies, both external and internal, have been employed.
General bleeding has been recommended, but never can be required
in simple clap. If the bladder, or other important organ, become
affected, depletion will be indispensable. Abstraction of blood by
leeches from the perineum may be required, when from any cause the
inflammation extends beyond its usual seat; and great relief is
afforded by afterwards employing hot fomentations, or the bidet, and
by diaphoretics given internally. Mercury was used in clap by those
who conscientiously believed that the disease was the same as what
they called syphilis. But it had been better far for mankind had
such a term, or the notions associated with it, never been broached;
or at least had mercury never been considered as necessary for the
cure of affections of the genital organs. In gonorrhœa mercury may
do much harm; it never can do good, either in the way of cure or
prevention. The disease has often been contracted, whilst the system
was saturated with the mineral. Frequent and violent purgings with
neutral salts—a common plan of treatment amongst the unprofessional and
inexperienced—are hurtful; the extremity of the rectum is irritated,
and may inflame, and the urethra, from intimate sympathy, will suffer
accordingly. Turpentine, copaiba, cubebs, buchu, &c., have been long
employed in all forms of the disease; of these, copaiba, administered
from the first, and not after the inflammatory symptoms have subsided,
is perhaps the one chiefly to be relied on. It maybe taken pure, with a
little water or bitter tincture, or mixed with an equal part of honey;
the copaiba may be given in gelatinous capsules, or made into pills
with magnesia; it should be given at bedtime, and in a large dose, from
a drachm to two drachms. The medicine may with prudence be continued
after the disappearance of the discharge, though its beneficial effects
are scarcely observable, excepting during the inflammatory stage.
An unpleasant eruption, resembling urticaria, sometimes follows its
employment; it appears on the inside of the lips, and on the glans
penis, and if the drug is continued, the eruption spreads over the
whole surface. Cubebs, though somewhat similar to copaiba in its
virtues, often disappoints the practitioner. The two medicines may
be given very advantageously together, made into a confection, and a
bolus of it taken occasionally in wafer paper. This class of remedies,
instead of stimulating, diminish greatly the irritability of the
urethra or466 the other parts of the urinary organs. In severe cases
it is of importance to increase the quantity of urine, and thereby
diminish its acrimony, by the free employment of diluents, mucilaginous
drinks, and alkalis; on this principle, infusion of linseed, containing
more or less of nitrous æther, is very efficacious. The patient suffers
much when the urine is scanty, and contains a large proportion of
saline particles. Rest and moderate diet are of paramount importance
as means of cure. Support of the penis, by a suspensory bandage,
or otherwise, should always be attended to when the patient takes
exercise, for many bad consequences will thereby be avoided; indeed it
is a measure requisite in all affections of the organ, and particularly
in gonorrhœa—when the prepuce, or even the whole penis, is liable to
swell enormously. By low diet, and the frequent use of warm bathing
of the part, or of the whole surface, the disease often disappears
rapidly; but when the cure is supposed complete, a hearty meal and a
few glasses of wine will suffice to bring it back with all the violent
symptoms.
Cooling washes applied externally to the penis are of little use, and
will seldom be long submitted to by the patient. Fluids injected into
the urethra, so as to be applied to the affected part of the mucous
membrane, are much more efficacious. When slightly stimulating, the
relaxed membrane is constringed by them, the action in the part is
changed, and a healthy secretion ensues; such are applicable after the
inflammatory symptoms have subsided. But in many instances astringent
injections are of much service from the very commencement; the morbid
action seeming to be arrested, and the parts quickly brought into a
healthy condition. Yet the use of such is not unaccompanied with risk,
and the mildest are sometimes hurtful; the incited action is apt to
extend along the passage; the discharge may be suddenly suppressed,
and inflammation of the bladder or testicle will generally supervene;
in short, the prominent symptom, discharge, may be arrested, but at
the same time such violent inflammatory action may be induced as
will be followed by change of structure in the canal, callosities,
contractions, abscess, &c. The injections may contain nitrate of
silver, sulphate of copper, sulphate of iron, sulphate of zinc, acetate
of zinc, super-sulphate of alumina, or bichloride of mercury, in
various proportions, or vegetable astringents may be used, as kino,
galls, &c.: their strength may be gradually increased according to
their effects. These solutions and infusions are injected by means of
either a small syringe, or an elastic bottle fitted with an ivory tube,
the point being smooth and rounded. This is carefully introduced into
the orifice of the urethra, and the patient is recommended to press on
the canal with his finger to prevent the fluid from passing farther
than an inch or two. It may be thrown in two, three, or four times
during the day, according to circumstances, and retained for a few
minutes; at each time the patient should make water immediately before.
The quantity injected at one time should not exceed a teaspoonful;
more is unnecessary, and may do harm. By passing bougies or other
instruments along the canal during active inflammation much mischief is
done. When excitement has gone off, and discharge remains, advantage
may be obtained467 by the internal administration of lytta or other
stimulants. When contraction of the passage is suspected, or when,
in spite of all means, no progress is made towards a cure, slight
discharge continuing long without pain, and probably furnished by a
relaxed portion of the membrane, recourse must be had to the occasional
introduction of a full-sized bougie. Cold bathing, local or general, is
sometimes useful.
If during the violent symptoms the discharge be from any cause suddenly
suppressed, inflammation of the bladder, swelled testicle, or both, are
to be dreaded; and endeavours should be made without delay to procure
its return, as by leeching the perineum, fomentations, and the general
warm bath.
The Consequences of Gonorrhœa occur in parts closely connected with
the urethra by sympathy and function; or they are such as affect the
constitution.
Of Hernia Humoralis, or swelled testicle. Pain and swelling occur
in the epididymis, and soon affect the body of the testicle. The
pain is most excruciating, the unyielding nature of the tunica
albuginea preventing the vessels from relieving themselves fully, and
inducing compression of the enlarging organ. Effusion takes place
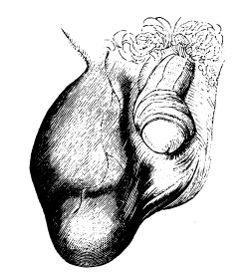 into the cavity of the tunica vaginalis, and thereby the tumescence
is still more increased, this tunic from its great dilatibility
readily accommodating itself to the accumulation of fluid within.
Sometimes the effusion is bloody, more generally serous, and not
unfrequently composed of serum more or less tinged with blood. The
epididymis remains enlarged longer than any other part, often during
the remainder of life. Sickness, vomiting, and violent fever, attend
the progress of the swelling. Pain in the lower part of the abdomen
is not infrequent, and may be mistaken and treated for enteritis. The
spermatic chord becomes enlarged and tender. The pain is much increased
when the patient assumes the erect posture, from the enlarged and
pendulous gland stretching the inflamed chord. Uneasy feelings are
complained of in the back, and pain there is sometimes so acute as to
be compared by the patient to the sawing of his loins asunder. When the
inflammation is violent, and effusion into the substance of the gland
extensive, suppuration may occur; and in infirm constitutions this is
not an infrequent, though remote, consequence of hernia humoralis.
The testicle is said to be rendered useless by the supervention of
this disease. Certainly it is in danger468 of having its functions
destroyed when the incited action is intense and the effusion great,
and particularly if suppuration follow. The disease may be induced by
violent exercise during inflammation of the urethra, bruising of the
organ, suppression of gonorrhœal discharge, the imprudent introduction
of bougies, the use of strong urethral injections, or debauchery of any
kind, during inflammatory gonorrhœa.
into the cavity of the tunica vaginalis, and thereby the tumescence
is still more increased, this tunic from its great dilatibility
readily accommodating itself to the accumulation of fluid within.
Sometimes the effusion is bloody, more generally serous, and not
unfrequently composed of serum more or less tinged with blood. The
epididymis remains enlarged longer than any other part, often during
the remainder of life. Sickness, vomiting, and violent fever, attend
the progress of the swelling. Pain in the lower part of the abdomen
is not infrequent, and may be mistaken and treated for enteritis. The
spermatic chord becomes enlarged and tender. The pain is much increased
when the patient assumes the erect posture, from the enlarged and
pendulous gland stretching the inflamed chord. Uneasy feelings are
complained of in the back, and pain there is sometimes so acute as to
be compared by the patient to the sawing of his loins asunder. When the
inflammation is violent, and effusion into the substance of the gland
extensive, suppuration may occur; and in infirm constitutions this is
not an infrequent, though remote, consequence of hernia humoralis.
The testicle is said to be rendered useless by the supervention of
this disease. Certainly it is in danger468 of having its functions
destroyed when the incited action is intense and the effusion great,
and particularly if suppuration follow. The disease may be induced by
violent exercise during inflammation of the urethra, bruising of the
organ, suppression of gonorrhœal discharge, the imprudent introduction
of bougies, the use of strong urethral injections, or debauchery of any
kind, during inflammatory gonorrhœa.
In the treatment, complete rest occupies a prominent station. The
inflamed organ must be supported; and all means which may have been
employed with the view of checking gonorrhœal discharge must be
abandoned. General bleeding may be necessary when the system is much
excited; and in all severe cases blood should be abstracted copiously
from the part, by the application of leeches or the opening of the
scrotal veins, and the organ is afterwards to be fomented for some
time, and then enveloped in a warm poultice. The bowels must be kept
open, the diet must be very low, and the value of antimonial medicines
as a powerful remedy in all inflammatory affections must not be
overlooked. Cold applications are of little or no service at any period
of the disease, and frictions with mercury and camphor had better be
dispensed with. When the violent symptoms have subsided, bathing the
part with a tepid solution of the murias ammoniæ is often useful; or
it may be rubbed gently with an ointment containing a small portion
of iodine, or with a liniment of soap and camphor, with tincture
of iodine. Much relief is experienced from interposing between the
scrotum and suspensory bandage a soap plaster, or one composed of
equal parts of the gum and mercurial plasters; thereby the organ is
defended from irritating friction and motion, and slight stimulation is
produced and kept up on the surface. Blisters promote discussion if the
swelling become indolent, but are very annoying to the patient. They
require repetition, but generally are in the end effectual; perhaps
the rest necessary during their use is of as much benefit as the
application.54
469
Inflammation of the Bladder and posterior part of the Urethra may
arise from other causes than suppressed or badly treated gonorrhœa;
but, however induced, its symptoms and consequences are the same. The
presence of calculi or other foreign bodies, over distention, &c., will
be treated of hereafter, as causing irritation and inflammation of
the viscus. Much vesical irritation is often produced and kept up by
disease of the kidney.
When inflammation of the bladder is slight, it is attended by uneasy
feelings referred to the perineum, pelvis, and glans penis; frequent
desire to empty the organ; pain felt acutely before evacuation of the
urine, and relieved immediately afterwards; scanty secretion of acrid
and highly coloured urine; a discharge of slimy, tenacious mucus,
either pure or voided along with the urine. In severe cases, most
excruciating pain is experienced during the discharge of the contents
of the bladder. The urine is often bloody; in general it is of a milky
appearance, containing lymph or puriform matter, and vitiated secretion
from the lining membrane. Micturition is almost constant, small
quantities being voided at a time. Sometimes the inflammation extends
to the ureters and pelves of the kidneys, causing violent pains in the
loins, nausea, occasional vomiting, and colicky affections.
In very violent cases lymph is effused on the inner surface of the
bladder, and may become organised; but such effusion is rare. I met
with one remarkable instance of it in my own practice, and have seen
several others. An old pensioner fell from a scaffolding, and sustained
a severe contusion of the back. Retention of urine came on; it was
drawn off regularly for some weeks, but then severe pelvic symptoms
supervened, and at last nothing but a small quantity of purulent
matter flowed through the catheter. The symptoms became urgent, the
bladder was very much distended, and rose to the umbilicus; all
endeavours to evacuate the urine per urethram failed, the instrument
being always closed by the thick pus, and I was obliged to open the
bladder pretty freely above the pubes. Much purulent matter mixed
with fetid urine escaped from the wound, as also a false membrane
which invested the mucous coat of the viscus. The membrane presented
a flocculent appearance, in some places distinctly fibrous, in others
was thin and transparent; its internal surface was irregular, as if
from the deposition of minute granules of recent lymph. The patient
died exhausted, after having survived about three weeks, voiding
his urine partly by the wound, and partly per urethram. It should
perhaps be mentioned, that those who saw 470him immediately after the
accident supposed that blood was extensively effused into the bladder,
and attempted to extract the suspected extravasation by means of an
exhausting syringe through a catheter, probably not passed into the
bladder.
Occasionally, though rarely, the inflammation extends to the peritoneal
covering of the bladder, and thence to the external surface of the
intestines.
The bladder becomes thickened, and lymph is effused between its
coats, from repeated attacks of inflammation, or from long continued
irritation in consequence of resistance to the expulsion of its
contents. The mucous membrane is thickened, relaxed, and of a
flocculent appearance; the fibres of the muscular coat are enlarged,
and, bulging out, form projections along their course; the mucous
membrane is extended often to a considerable extent between the
projections of the enlarged muscular fasciculi, forming pouches. The
cavity of the organ is generally diminished in proportion to the
thickening of its parietes, and there is a loss of balance betwixt the
retaining and expelling powers.
Irritable bladder is generally a symptom of some other affection.
There is profuse mucous discharge; frequent micturition; pain,
increased by distention of the organ, and relieved by evacuation.
The coats are more vascular than in the natural state; sometimes the
muscular is strengthened, and ulceration of the mucous membrane is not
infrequent. Occasionally this latter tunic is the seat of tumour.
In the treatment of inflammation of the bladder, after removal of its
causes, antiphlogistic means occupy a prominent situation, and are to
be regulated according to circumstances. Leeches to the perineum and
hypogastrium—soothing injections into the rectum—opium or hyoscyamus,
either by the mouth or in the form of suppository—fomentation and the
warm bath—are all valuable remedies in this affection. When injections
into the rectum are used, they should not exceed three or four ounces,
and they should contain from thirty to sixty drops of laudanum, or a
corresponding quantity of the liquor opii sedativus. But an anodyne
suppository is perhaps more simple and more efficacious. The effect
of these remedies is almost instantaneous; all pain goes off; the
patient becomes quiet, loses all recollection of his former sufferings,
and often remains in a state of great comfort for twelve or sixteen
hours. The suppository may be repeated as need be; the preferable time
for its exhibition is the hour of sleep. Camphor, given by the mouth
in full doses, is a powerful remedy for allaying irritation of the
bladder, from whatever causes induced; as is copaiba, less nauseous
and more trustworthy than cubebs or buchu. The copaiba will often
remove speedily the most intense irritation, when all other means have
failed. The bowels are to be kept gently open, and all stimuli disused;
diet should be low, drink copious and bland. Washing out the bladder
with anodyne or other fluids, and the application of blisters to the
perineum and neighbouring parts have been recommended, but are often
more injurious than useful.
Of Stricture of the Urethra.—By stricture is understood a nar471rowing
or contraction of a mucous canal, from deranged action, or from
morbid alteration of its structure. It may arise from relaxation and
turgescence of the parietes, or from effusion of lymph either under
the lining membrane, or on its surface. Spasmodic stricture has been
spoken of by some writers, but is most probably an imaginary disease.
An irritable urethra, in which organic disease does not exist to any
great extent, may contract at some point, diminish the stream of urine,
and prevent the introduction of instruments, or retain them by closing
firmly round, and in such circumstances the obstruction does probably
depend on spasm of the muscular fibres surrounding the urethra; yet to
such a state of the canal the term stricture cannot be applied with any
degree of propriety.
True, organic, or permanent strictures of the urethra vary in their
degree of constriction, becoming tighter when irritated by improper
treatment, hard living, or exposure to damp or cold; indeed all mucous
canals are sensibly affected by cold and damp. From these causes a
combination may be produced of permanent stricture and spasmodic
action; but, as already hinted, it would perhaps be well that this
latter term, applied to urethral stricture, were forgotten, instead
of remaining a convenient excuse for want of knowledge or dexterity.
Spasms of canals and cavities, unusual membranes, adhesions, sacs,
and cysts, are too often met with in the practice of surgery, and are
said to prevent the practitioner from accomplishing the objects of his
operations, so as to put the patient to a great deal of unnecessary
suffering, and even endanger his life. The old writers supposed that
obstruction of the urethra arose from growths, warts, caruncles, or
carnosities in the passage; and even in the present day such causes
would sometimes appear to be more accredited than they ought; small
excrescences do sometimes form on the membrane, though very rarely.
The true stricture is the result of inflammatory action in the part: at
first possibly serous effusion takes place beneath the membrane, and
elevates it into an œdematous swelling, which, according to its extent,
obstructs the canal; the lymph is deposited both beneath the membrane
and external to it, becomes organised, and forms a permanent and more
unyielding obstruction. Strictures are of various kinds. The bridle
stricture is rarely met with; a membranous band of organised lymph is
said to traverse the canal, and, according to the thickness of this
membrane, the flow of urine is more or less impeded; in the majority of
cases the morbid formation is thin and delicate, but still sufficient
to scatter and diminish the stream. When a soft bougie is introduced,
it is resisted by the stricture, and on examining the instrument when
withdrawn, the transverse and central impression on its point marks
the existence of the bridle. The urethra is sometimes narrowed by a
circular membranous ring projecting into its canal, composed of swollen
mucous membrane with subjacent effusion, and presenting the appearance
of a thread having been tied round the passage. Other strictures occupy
a considerable portion of the urethra, from a quarter of an inch to
two inches or more; differing from the preceding only in the effusion
and membranous swelling being more extensive. Others are irregular,
the472 contraction being not uniform at the narrowed point, and sometimes
only one side of the canal is affected. Some are very firm and gristly,
the effused lymph having become much condensed after organisation;
others are less dense in their structure, and exceedingly elastic. From
repeated attacks of inflammation at the constricted part, and around,
additional lymph is effused and organised, and thus the extent and
tightness of the stricture is increased.
The urethra is generally constricted at those parts which are naturally
the tightest; at the orifice—betwixt three and four inches from it—and
betwixt six and seven inches from that point; the most frequent site is
perhaps anterior to the sinus. Contraction of the orifice is frequently
the consequence of cicatrisation, and generally proves obstinate; in
some cases the smallest probe is passed with difficulty. Considerable
portions of the anterior part of the canal suffer contraction from the
effect of ulceration; and congenital malformations of the orifice give
rise to many affections both of the urethra and bladder. Contractions
in different parts of the canal depend much upon one another.
When a tight stricture exists, the passage anteriorly is never fully
distended, and becomes permanently contracted in consequence; whilst
more or less dilatation is produced behind the tight part, wherever
that may be. The enlargement often is very great, the urine lodges in
the cavity formed by dilatation, and can be pressed out in a stream,
or dribbles away after the patient supposes that he has done making
water. Mucous and sabulous deposits often lodge in it; and calculi are
occasionally retained there, may attain a large size, and may give
rise to very unpleasant and even dangerous symptoms. Not unfrequently
ulceration takes place behind the stricture, and the urine becomes
insinuated into the cellular texture; but this tissue immediately
around is in general condensed previously to the giving way of the
canal, and so prepared by lympathic effusion as to oppose effectually
extensive infiltration. Such is not the case, as will afterwards be
explained, when solution of continuity in the urethra, or of the cyst
of an abscess, takes place in consequence of distention of the bladder.
In the gradual escape of urine by ulceration behind the constricted
point—the urethra being neither altogether obstructed, nor nearly
so—abscess forms in the cellular tissue, exterior to the ulcerating
part. The suppuration is often slow in its progress, and imparts to
that part of the perineum a stony hardness. Repeated collections of
matter may form, and, if the cause be not removed, numerous openings
will form in the scrotum and perineum, and through them fetid matter
and urine will constantly and involuntarily distil. The patient is
reduced to a miserable state; the neighbouring parts are excoriated,
and exhale a noisome odour, his body and bed-clothes are soaked and
rotted by the discharge, and the atmosphere to a considerable distance
around offends the nostrils. Fistula in perineo is established.
Ulceration and perforation of the urethra from stricture seldom takes
place anteriorly to the scrotum; but ulceration often is induced there
by retaining instruments long in the passage, and may be fol473lowed by
sloughing of the integuments, abscess in the cellular tissue, or both.
Occasionally the urethra communicates with the rectum in consequence
of ulceration, escape of urine into the cellular tissue, and formation
of matter. The symptoms of stricture are often much relieved after the
formation of fistulous openings; and the cure can then be much more
easily accomplished than formerly, the passage being less irritable.
When the fistula is free and open, allowing the urine to escape
readily, the natural passage contracts, and will become almost entirely
obliterated, unless means are taken to dilate it, and to diminish the
unnatural opening. Neglected aggravated cases are met with, in which
the urine has passed entirely through the false passages for years,
the urethra and penis, anterior to the stricture, being both rendered
completely useless; but even such cases can, by proper management, be
relieved, or permanently cured. Ulceration of the urethra, originating
in consequence of stricture, may proceed even after the stricture is
removed, and give rise to abscess and fistula.
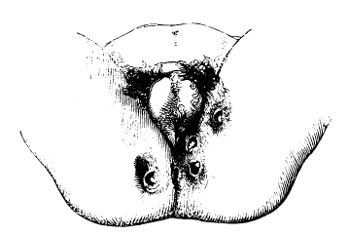
Many patients labour under stricture, and even tolerably bad ones,
without being aware of it. But the surgeon is led to suspect the
existence of stricture, by complaints which the patients wish to
be relieved of, and which they often suppose to arise from totally
different causes—pains in the loins or hips, indolent swelling of the
testicle, or of the inguinal glands, irritability about the fundament,
gleet. On inquiring about the stream of urine, the patient may declare
that it is as good as possible; and many say so without intending to
deceive, for the stream diminishes so gradually, that the patient is
not aware till after he is relieved that he has been voiding his urine
in a very shabby and imperfect manner. On questioning further, it
is discovered that the stream is forked or twisted, or divided into
several small ones; that there is frequent desire to empty the bladder,
during the night particularly; and that at first the urine comes away
only in drops. A long time is occupied in passing even a small quantity
of urine, and the patient has to strain much; in bad cases he is almost
always obliged to go to the water-closet when inclined474 to make water,
lest the contents of the rectum be evacuated by the great exertion
of the levator ani and abdominal muscles, necessary to overcome the
obstruction in the urethra. By the straining hernia is also frequently
induced.
In consequence of the almost constant endeavours to overcome the
resistance afforded by the stricture, the bladder becomes much
strengthened in the coats, and diminishes in size. All the coats
are affected, but particularly the muscular; the surface becomes
fasciculated; the fibres grow fleshy and strong, and are collected in
large bundles. Cysts form, often of a large size; some are caused by
interlacement of the enlarged muscular fibres, others are produced
by outward protrusion of the mucous coat. This membrane being, by
excessive muscular action in the viscus, pushed between the enlarged
fasciculi, dilates into a bag, and forms a cyst of greater or less
size, communicating with the cavity of the bladder, generally by a
narrow neck; the protruded membrane is thickened by new deposit, and
ultimately the parietes of the cyst, in some degree, resemble those of
the bladder. Cysts of this description are usually situated near the
fundus of the organ, and often attain a large size; in some cases the
cyst nearly equals the bladder in capacity; and the two seem to form
one large organ contracted near the middle. The secretion from the
surface of the bladder and cysts becomes vitiated, is much increased
in quantity, and passes off along with the urine or after it—sometimes
in solution, often separately. In severe cases the ureters and pelves
of the kidneys dilate, and their mucous surfaces also contribute to
furnish the discharge, in general slimy, ropy, and tenacious, sometimes
puriform. Discharge also takes place from the stricture, or rather
from the dilated portion behind it; it is a kind of gleet, very apt
to be increased by excess in drinking and venery. After debauchery,
the stream of urine—which was previously not much affected, at least
to the patient’s observation—comes to be very small; and frequently
the urine can be voided only in drops, and that with much labour.
Besides, the balance between the retaining and expelling powers of the
bladder is often lost, and either incontinence or retention of urine
is the consequence. Though the urine be much obstructed, even when the
stricture is not very tight, the flow of the semen is not; the degree
of contraction must be very great to prevent ejaculation of the latter
fluid. Indeed, during the healthy state of the parts, the whole urethra
is much narrowed, as well as shortened, during seminal emission in
coitu, from forcible action of the surrounding fibres, and injection
of the corpus spongiosum; and the momentary contraction of the passage
in such circumstances is perhaps greater than almost ever occurs in
consequence of disease. Sometimes the seminal fluid passes back into
the bladder, from an inverted action of the canal, and is evacuated
along with the urine; nocturnal emission is a frequent concomitant of
stricture. That an inverted or sort of antiperistaltic motion sometimes
exists in the urethra, is shown by a soft bougie being in such cases
drawn into the bladder after having been passed but a short way into
the urethra.
In cases of bad stricture, the complexion is sallow, the countenance475
anxious, and the general expression of the features so peculiar as to
be almost pathognomonic. The lower limbs become emaciated and weak.
Gout often accompanies stricture, and paroxysms of it are induced by
irritation of the urethra; the canal itself is said to be sometimes
affected with a gouty action.
Stricture may be caused by inflammation or long-continued irritation
of the urethra, however induced—by mismanaged virulent gonorrhœa—by
stimulating acrid injections—by piles, and other irritations about the
fundament—by calculi passing along the urethra. That gonorrhœa is a
very frequent cause of stricture has been long known—“If the case be
slubbered over, and long delayed, caruncles arise in the urethra, and
in progress of time a carnosity.” The passage or lodgement of calculi
in the canal has induced stricture even in children: and calculus in
the bladder is supposed sometimes to produce disease in the urethra,
and vice versâ. Strictures are often caused by falls or blows on
the perineum, and such cases are of the very worst kind; in some the
urethra becomes almost entirely obliterated; in most the stricture
is extensive and callous; and in all the disease is overcome with
difficulty.
When stricture is suspected, the urethra must be examined. A soft
white-wax bougie is very well adapted for ascertaining the state of the
parts, but must be used very gently. If pushed forwards rashly and with
force, the instrument yields before the stricture, and when withdrawn,
is found twisted like a screw, or doubled backwards on itself. The
vessels of the urethra may be torn, and hemorrhage, with great pain,
ensue. The bougie should be slightly curved in its farther extremity,
warmed either at the fire or by friction with the fingers, and well
oiled, previously to its introduction. It is then passed softly along
the canal till its progress is arrested; thus the situation of the
stricture is ascertained. Then a little more pressure is employed for
a short time; if the instrument have not become insinuated into the
constricted part, it will resiliate on removal of the pressure from
its free extremity; if it is passed into or beyond the stricture, it
is firmly grasped by that part of the urethra, and retained; thus
we discover the degree of contraction; and from the extremity of
the bougie receiving and retaining the impression made on it by the
contracted part, we can form an accurate diagnosis regarding the
nature and extent of the stricture. The information thus acquired is
afterwards acted on.
The principles on which the cure is to be conducted are the same in
almost all cases; but the particulars of the treatment must vary
according to circumstances. In slight cases, the gentle introduction of
a moderately-sized bougie produces a cure by removing the irritability
or susceptibility of the surface; the relaxed membrane is stimulated
by the distention made with a bougie, and soon regains its natural
tone. It may be necessary to repeat the introduction of the bougie
a few times, at considerable intervals. In tight organic stricture
something more is required; the constricted part must be dilated
gradually. Much dexterity and management is often required to pass an
instrument through a tight stricture, particularly if inflamed; and in
such circumstances the attempt should not be made but on476 good grounds,
and to relieve urgent and dangerous symptoms; but after a bougie or
catheter, however small, has been got past, the disease is completely
under the control of the surgeon, and a cure must follow if the
treatment be properly conducted, and if the bladder and kidneys have
remained tolerably sound. The effect of an instrument passed through
an organic stricture is to remove the irritability of the lining
membrane, to excite the absorbents to remove the newly-formed parts,
and to dilate the passage: it may be supposed to act in some measure
on the same principle as a bandage applied to a swelled extremity. The
instruments introduced must be gradually enlarged till one readily
passes of the full size; that is, one that enters the orifice with
some difficulty, and fully distends the rest of the canal. Numerous
contrivances have been employed for the dilatation of strictures; but
the preferable instrument is a silver catheter, or a sound made of
silver, of steel, or of plated metal. A soft or gum-elastic bougie
is sometimes useful in ascertaining the nature and situation of the
stricture; but in the treatment it must give place to the metallic,
slightly conical at the point. This, in the hands of a well-qualified
person, can be more surely and readily directed than a flexible one,
and in its use there is less risk of injury being inflicted on the
passage; besides, it does not yield to the action of the diseased part.
The practitioner must be provided with a full assortment of catheters
and metallic bougies, each one differing from the other in size;
for, as already observed, the size of the instrument passed must be
gradually increased; and, besides, the calibre of the canal varies much
in different individuals; what is a full size for one person may be but
a trifle in the urethra of another. The bougies are arranged by what
is termed a size-plate, or gauge, a flat piece of metal, containing
fifteen or sixteen circular perforations, which commence about the
size of a small crow-quill, and gradually enlarge in diameter. These
apertures are numbered, and the bougie which fills one has the
corresponding number imprinted on it. By reference to the numbers, the
surgeon is at once made aware of the progress he has made towards a
cure.
In the more common and simple cases, a regular and gradual ascent
in this scale is all that is required, allowing a proper interval
to elapse betwixt the introductions. But in tight and unyielding
stricture, small, firm, silver catheters are required, one of these of
a size proportioned to the contraction of the canal—and the calibre
often must be extremely minute—is passed through the stricture or
strictures by dexterous, persevering, and at the same time gentle
pressure in the proper direction. If the diseased part be anterior
to the bulb, it can be grasped between the fingers of the left hand,
whilst with the right the instrument is insinuated into it; thus the
part is steadied, and the course of the catheter made more certain
and safe. If it be posterior, assistance in the introduction, and
information as to the direction and progress of the instrument are
obtained by the forefinger of the left hand being placed in the bowel;
and this is the more necessary when the stricture is of an elastic
nature. Considerable experience is requisite to enable the surgeon
to be aware of the progress he is making with the instrument, and
whether or not477 it is advancing fairly in the canal; much information
as to this is imparted by the sense of feeling. If the point of the
instrument be within the contracted part, it will be felt embraced and
obstructed, and on withdrawing the pressure, it will be stationary;
if it have not entered the stricture, but is pushing it before it,
resilience will be felt as soon as the pressure is either diminished
or removed. The sensation imparted when the instrument has left the
canal, and is entering into a false passage, is of a peculiar grating
nature, and when once felt, will scarcely be forgotten or mistaken. By
means of a good knowledge of the natural course of the urethra, and an
acquaintance with the feelings just alluded to, but which cannot be
graphically described, the surgeon of experience is enabled to avoid
blunders, and to pass an instrument with safety through the tightest
strictures. It is, however, an operation of very great difficulty in
aggravated cases, perhaps the most difficult in surgery; facility in
passing the catheter is acquired only by practice and experience. The
greatest caution is required, along with considerable fortitude and
perseverance.
When the instrument has been fairly lodged in the bladder, it is to
be retained. A tape is attached to each of the rings at the neck of
the catheter, is brought under the thigh, and fastened to a bandage
passed round the waist; this simple retentive apparatus is quite
effectual, and suits the erect as well as the recumbent posture. A
peg, of metal or wood, is placed in the mouth of the catheter, that
the patient may be kept dry, and at the same time have it in his
power to relieve the bladder as often as necessary. The instrument
should be retained for twenty-four hours at least, and, if the patient
can bear it, for forty-eight, or even more. At first it occasions
considerable uneasiness, pain, and excitement, but these gradually
subside; when severe, they may be allayed by opiates. The parts make
efforts to get rid of the foreign body, and these efforts are salutary.
Discharge takes place from the membrane, and oozes by the side of
the catheter; relaxation occurs, often to a very great extent; and,
on moving the handle of the instrument, it is found to be not only
less firmly grasped, but to possess considerable freedom of motion
in the contracted part. Thus a most successful inroad is made upon
the disease, and the after treatment thereby happily abridged. The
instrument is withdrawn, and time afforded for the parts to become
quiet. After the lapse of two, three, or four days, according as the
uneasy feelings disappear, a larger instrument is introduced, and
retained perhaps for half an hour; and the successive introduction
of instruments—sounds being now adopted—at proper intervals, and in
proper graduation, is continued as in ordinary cases. Sometimes, though
rarely, the good effects of the first introduction and retention of
the instrument quickly disappear, the stricture becoming tight and
unyielding as before; when this takes place, the practice is to be
repeated, but not till after several days, and then the instrument will
be retained with advantage for a longer time than before, provided
no untoward symptoms are caused by its lodgement. There are very few
strictures, indeed, which will not yield to this treatment, when
judiciously planned and perseveringly followed.
478
Fistulous openings generally close in a short time, when once the
urethra has been widened. Their contraction may sometimes, however,
prove slow and imperfect, even after the stricture has been entirely
removed, and the application of the cautery may be requisite; to
accomplish this, when the opening terminates in the rectum, a speculum
ani is required, by which to view the aperture, and ascertain its site,
and along which to pass the heated wire with safety to the bowel. The
cautery is not to be applied so as to produce an extensive slough, and
much loss of substance, but lightly to the edges. On the separation
of the superficial eschar, the margins are raw, excited, and swollen,
with a disposition to granulate; and during cicatrisation of the sore,
considerable contraction takes place, independent of the formation of
new matter. After the contraction thus effected has occurred to its
full extent, and not before, the cautery is reapplied; and by a few
repetitions of the instrument at long intervals, the opening is brought
to close.
At one time attempts to destroy the contraction of the urethra, by the
application of caustic to the stricture, were in great vogue; but the
total inefficiency of such practice is now generally acknowledged.
The armed bougie was in many cases applied hundreds of times, at
considerable intervals; and the mode of treatment, though trying,
tedious, and hurtful to the patient, must have proved useful to the
surgeon—but to him alone. Years were spent in such trifling, and not
unfrequently serious consequences followed this treatment, or rather
neglect, of the disease. Cutting catheters are dangerous, as well as
inefficient for the cure of stricture; thrusting at the end of a long
stricture can avail but little, and in the hands of most practitioners
the instrument is as likely to perforate the coats of the urethra as to
enter the stricture.
Incision of stricture may be required in retention of urine, scarcely
otherwise. The practice is noticed under the treatment of retention.
In stricture anterior to the scrotum, it is well to avoid incision,
if possible, as it generally is so, for a wound there is healed with
difficulty, if at all.
Retention of Urine is not to be confounded with suppression of the
secretion from the kidneys, arising from disorder of the structure or
function of these organs. The kidneys perform very important functions
in the animal economy, and complete suppression of their secretion
under any circumstances is a very suspicious and dangerous occurrence.
In the healthy state of the urinary organs, when the powers of each
correspond, the urine passes without almost any exertion on the
part of the patient; the action of the levator ani and abdominal
muscles is scarcely required. But when either structure or function
is disordered, the balance between the parts is upset; additional
assistance is necessary for expulsion of the contents of the bladder.
The symptoms of retention differ according to the state of the parts
and the cause which has induced it. The bladder varies in size, and
in distensibility. In some cases the organ yields readily to the
accumulation of fluid within it, rising high in the belly, reaching
even479 the umbilicus, and forming a large, oval, tense, fluctuating
swelling, apparent to the most careless and casual observer. The
swelling and fluctuation are in such circumstances so distinct, that
the disease has actually been mistaken for ascites. Again, all the
symptoms of retention may exist, and all its bad consequences result,
without any apparent swelling of the abdomen. But then the distended
bladder can always be felt by the finger introduced into the vagina or
rectum; indeed its posterior fundus bulges in towards the cavity of the
gut, in every case, before it ascends upwards in the abdomen. Sickening
and agonizing pain, with great anxiety and ineffectual straining,
generally attend distention of the bladder to any great degree. When
the distention is allowed to continue, urinous fever supervenes, the
circulation is accelerated, the patient perspires profusely, and
exhales a urinous odour; delirium comes on, followed by sinking, and,
if the cause is not removed, coma terminates the distressing train of
symptoms. In other instances the painful feelings subside after some
time, and the urine is discharged involuntarily from the urethra. The
ureters lose the valvular structure of their vesical terminations, and
become dilated; the pelvis and infundibula of the kidneys also enlarge,
and all are distended by the accumulating urine. On relieving the
bladder artificially, the pressure is taken off the secreting part of
the kidneys, their secretion is generally renewed with great vigour,
and the bladder is again filled rapidly. If the bladder is not relieved
the secretion of urine is suppressed.
In many cases the urethra—the bladder more rarely—sloughs or ulcerates,
unless preventive measures are adopted, and extravasation of urine
takes place into the cellular tissue of the pelvis, of the perineum,
of the groins, of the lower part of the abdominal parietes—into
the cellular substance of the scrotum, and of the penis—the parts
infiltrated depending of course on the point at which the urinary
canal has given way. Under such circumstances the patient is sometimes
rapidly destroyed, the extravasated urine appearing to induce speedy
sinking, similar to the effects of inoculation with a most virulent
poison. If the urine escapes into the cavity of the abdomen, the
patient inevitably perishes, and that very speedily; and when the
cellular tissue of the pelvis is the seat of the extravasation, little
hope can be entertained of recovery, though the fatal termination
may not be so rapid as in the former case. When the urine is effused
into more external parts, as into the perineum or scrotum, the danger
is also imminent, if the fluid is allowed to accumulate and become
extensively infiltrated; but when it freely escapes externally, either
spontaneously or by incision, there need in general be no great
apprehension of immediate danger. In such cases the aperture in the
urethra is found to be at first irregular and ragged; afterwards its
inner surface becomes rounded off, and a papilla presents externally.
The infiltrated cellular tissue is dark, fetid, broken down, and
soft, sometimes seemingly in part dissolved by the putrescent urine;
and, when the patient has survived a considerable time, it frequently
resembles closely in appearance a portion of suppurated lung. When
active practice is not adopted after extravasation of urine has taken
place, the cellular tissue around sloughs along with480 the integuments;
rapid depression of the powers of life ensues, with great disturbance
of the sensorial functions. Death very soon relieves the patient from
his sufferings; some few struggle through, and recover, after losing
the coverings of the penis, of the testicles, and of the perineum.
The causes of retention are many; but the surgeon must know them all,
as the treatment must vary according to the cause. They may be divided
into such as weaken the power of expulsion, and into such as impede the
progress of the urine in the urethra.
Retention of urine is caused by paralysis of the bladder, from
over-distention, from injury or disease of the spinal chord, from
pressure on the spinal chord or nerves. In such cases the bladder often
attains a very large size. At first the accumulation produces all the
uneasy symptoms formerly mentioned, but after some time these subside,
and the urine drains away according as it is secreted, without,
however, the original accumulation and tumour being diminished. This
state of the urinary system is very common in old people, who neglect
natural calls to empty the viscus during the night, or while sitting
socially after dinner. The uneasiness gradually goes off, and when they
at length think of making water, none can be got to flow. Sometimes
they remain in this state—the bladder full, and becoming more and more
distended—for days, drinking gin and water, juniper tea, or other
popular remedies. Incontinence then takes place, and the dribbling of
the urine affords considerable relief; this state of matters is often
allowed to continue for weeks. Thus the power of expulsion may be lost
for ever, though sometimes it is regained even under very unfavourable
circumstances. I recollect attending a man upwards of eighty, labouring
under retention of urine with incontinence, and whose bladder required
relief by the catheter for ten or twelve days; at the end of that
period the bladder regained its expulsive power and retained it; and
cases are on record in which the power of expulsion has returned
after the lapse of several months. Retention thus induced is often
complicated with disease of the prostate gland or of the urethra. The
patient, perhaps, has been for a long time incapable of emptying his
bladder completely; a portion of the urine always remains in the most
dependent part of the viscus, and the quantity retained becomes greater
and greater, until from some slight cause the power of expulsion is
lost entirely. In these cases the bladder, though much increased in
capacity, is also much thickened.
Retention from inflamed urethra, attended with swelling and spasm about
the neck of the bladder, is preceded by hardness and tenderness in the
course of the urethra, and a smarting felt when a drop of urine passes
along. Retention not unfrequently takes place during gonorrhœa, from
the dread which the patient has of making water; and from the swelling
of the lining membrane.
Retention from abscess in the perineum was formerly noticed.
Retention from injuries in the perineum. The urethra is either severely
bruised, perhaps lacerated, or torn completely across; and if the
patient attempts to make water before proper means are adopted, blood
and urine are extravasated into the cellular tissue481 exterior to the
canal. In cases of slighter injury, retention may occur on account of
the inflammatory swelling of the parts supervening secondarily.
Retention from stricture of the urethra is of very frequent occurrence,
and most difficult to manage. The state of the urethra and bladder
in this disease has been already adverted to, but it is necessary to
bear in mind the thickening of the latter, and the dilatation which
uniformly takes place behind the stricture. All the urgent symptoms of
retention may, in this case, arise from the accumulation of but a few
ounces of urine. The bladder contracts frequently and very forcibly,
causing great suffering. Temporary relief is experienced when the
urethra gives way by ulceration, and the urine becomes extravasated
into the cellular texture; the patient gets up, and, if in the dark,
thinks that the stricture has yielded, and that he is passing urine
naturally. But soon he feels a glowing heat in the perineum; the
parts swell and become livid; violent constitutional symptoms come
on, the discoloration advances, the integuments slough, ill formed
matter is discharged, and disorganised cellular tissue mixed with
putrid sanies is exposed. The parts exhale a urinous odour, which,
when once smelt by the practitioner, can never afterwards be mistaken.
Occasionally œdematous swelling of the penis takes place, particularly
of the prepuce, when it has been pulled at and bruised during the
patient’s efforts to make water, and this must not be confounded with
infiltration of urine; I have seen it occur some time after the bladder
had been relieved by the catheter. Infiltration of putrid serosity
into the cellular tissue of the prepuce, the subcutaneous tissues of
the penis, scrotum, and lower part of the abdomen, occasionally also
takes place to a great extent, after the bladder has been relieved by
the catheter, the coverings are destroyed, and the patient may, even
despite of active treatment, perish in consequence. In such cases, a
small quantity of urine may possibly have escaped into the cellular
tissue before the bladder has been relieved, so as to commence the
mischief.
Retention from the lodgement of calculi. Temporary obstruction to the
flow of urine is sometimes experienced from calculus in the bladder.
Complete and fatal retention has arisen from calculi having become
impacted in the urethra, and been allowed to remain there, blocking up
the passage entirely.
Retention from affections of the prostate gland and neck of the
bladder, inflammatory or indolent. In acute inflammation of the
prostate gland and cervix vesicæ, the other parts around swell, the
mucous membrane becomes turgid, and the mucous secretion is increased.
Suppuration may take place, and an abscess, chronic or acute, form
in the substance of the gland, or in the cellular tissue exterior;
the parietes of the abscess may give way, and the matter discharged
into the bladder, into the rectum, or into the cellular tissue of
the perineum. Bloody and mucous discharge from the urethra, frequent
desire to make water, sudden stoppage of the urine whilst making water,
pain in the glans penis, and other symptoms of stone in the bladder,
followed a fall on the back. Afterwards, a tumour pointed into the
rectum, and was opened; purulent matter was pro482fusely discharged, and
afterwards urine escaped through the aperture. The patient died in
three weeks, from irritative fever, with gastro-enteritic symptoms.
Along with thickening of the bladder, and disease of its mucous coat,
there was found a large abscess of the cellular tissue, communicating
with an abscess in the third lobe of the prostate gland, and that with
the cavity of the bladder.
When the affection is less acute, the prostate slowly enlarges, from
opening out of its texture, and deposition of new matter in the
interstices, it becomes hypertrophied. The whole gland may enlarge
uniformly, but generally one part protrudes more than the others. When
the third lobe enlarges, it necessarily projects into the bladder, or
into the prostatic portion of the urethra, and there, acting like a
valve, causes much more formidable obstruction to the flow of urine
than does enlargement of the lateral lobes; the obstruction is the more
complete the greater the distention of the bladder. At first, this lobe
is but slightly prominent, and of a conical form; but as it enlarges,
its regularity of shape disappears, the tumour is nodulated, and in
general somewhat pyriform. It occasionally projects to one side of the
passage. The affection is seldom met with, unless in old people.
In consequence of prostatic enlargement, pain is felt in the perineum,
with occasional throbbing, and a sense of weight; there is frequent
desire to make water, the bladder is irritable, and discharges ropy
mucus. There is more or less irritation of the lower bowels; there
is an almost constant desire to empty the rectum, from a feeling of
fulness there, and pain, often severe, is felt on going to stool; when
the enlargement is great, the bowel is considerably compressed, and
the feces, when solid, are passed flattened like portions of tape.
Frequently there is thin mucous discharge from the urethra. In making
water, the urine, as it were, hesitates, and after a while passes
away, at first in drops, and afterwards in a scanty and irregular
stream; pain is felt at the point of the penis, in the loins and
hips, and often in the inside of one or both thighs. On attempting
to pass the catheter, its extremity is obstructed in the prostatic
region, and the swelling can be felt by the finger introduced into the
anus. Examination of the tumour, per anum, is very often a painful
proceeding; it is best accomplished after a catheter or sound has
been introduced. The disease is often coexistent with calculus in
the bladder. The tumour is very seldom malignant, but proves both
troublesome and dangerous from its size. The bladder may become
distended in consequence, though retaining the power of partially
relieving itself; or the urine may come away involuntarily after some
time; or retention may be complete, and, if not relieved, the bladder
may slough.
It is to be recollected, that in retention of urine, from whatever
cause, and particularly in that arising from prostatic enlargement,
the urethra is elongated, and the bladder rises into the abdomen like
the gravid uterus. The reason of such change of relative situation is
sufficiently obvious, being chiefly mechanical.
Fungous, or other tumours, furnishing blood or vitiated puriform
matter, now and then grow from the internal surface of the bladder,
unconnected with the prostate gland. Worms, too, occasionally lodge483
in the bladder. Either of these circumstances may induce retention of
urine. Another cause of obstruction is hernia of the bladder.
There is no disease in which the patient is more liable to be ‘bungled
out of his life,’ than in retention of urine. Great credit is to be
gained by judicious and skilful management of the various stages,
and by expert use of the catheter in difficult cases, when other
practitioners, perhaps, after being foiled, have proposed operations
alarming to the patient, and, in themselves, dangerous. In no disease
are patients more grateful for relief, for in this the agony is often
unbearable. Immediate abatement of all painful symptoms follows skilful
and prompt measures; and the superior science of one man over others
is made apparent to the most ignorant observer. In over-distended
bladder from paralysis, the catheter can in general be passed without
difficulty. It should be of a large size, and its introduction should
be repeated as often as nature calls for relief, perhaps three or four
times during the twenty-four hours, until the viscus regains its tone;
and this, unless irrecoverably lost, will generally be restored in a
few weeks at most. Repeated introduction of the instrument is here
preferable to the retaining of it; the latter measure should always be
avoided, unless absolutely indispensable, for a foreign body lodging
in the urethra and neck of the bladder must always be a source of
more or less irritation; and experience shows that the bladder sooner
recovers its tone when the instrument is introduced only to draw off
the urine, when the uncomfortable feelings of distention come on,
than when it is constantly retained. The patient soon learns to pass
the instrument himself, and thereby saves the surgeon from frequent
attendance, whilst, at the same time, the bladder is opportunely
relieved. Stimulants, as the tinctura lyttæ, given internally, with
external friction, blistering, and the application of strychnine to the
raw surface, may contribute towards restoration of the muscular power
of the organ. Injections into the bladder have been recommended, but
are both hurtful and inefficient. Enemata, containing turpentine, or
other stimulating fluids, are of service.
In retention from inflamed urethra, the catheter should, if possible,
be dispensed with. The introduction of it is excruciatingly painful,
and will certainly aggravate the original affection. Blood should be
abstracted both from the system and from the perineum; fomentations,
with the warm bath or the hip bath, are afterwards to be employed.
The retention is usually induced by hard exercise, or intemperance
in living; these of course must be abandoned, and their opposites
enjoined. Camphor alone, or combined with opium or hyoscyamus, is to be
given internally in large doses. Opium may also be useful, administered
in the form of an enema or suppository. If relief is not soon afforded
by such soothing measures, the bladder must be relieved by the
catheter; and if the surgeon be foiled in the introduction of this,
as he ought not to be, the only resource is to puncture the bladder
from the rectum—a harsh measure, to be sure, and one not indicative of
surgical talent, but still preferable, in the eyes of both patient and
practitioner, to death.
In retention from abscess in perineo, a little delay is allowable484
under the employment of palliatives, when the affection is acute. The
abscess must be freely opened as soon as its seat is discovered; and
until the evacuation of the matter, the use of the catheter should be
deferred if possible. In cases of chronic abscess, the catheter must be
used, and does no harm.
In retention from injury of the perineum, the catheter should be passed
before the patient attempts to make water, and the instrument must be
retained; thus extravasation of urine in addition to the blood into
the cellular tissue will be avoided. If extravasation has occurred,
the perineum, scrotum, or other parts, must be freely incised wherever
the urine has been effused, in order to prevent the direful effects
of lodgement of that fluid; and then the catheter should be passed
and retained as in the former instance. If the surgeon be foiled in
introducing an instrument, as he may be, and if the prostate be sound,
the bladder must be relieved by puncture from the rectum.
Retention from stricture is, as already observed, the most difficult
to manage. No time can be put off in bleeding or warm bathing, in
giving internal remedies, or exhibiting enemata. The viscus is making
violent exertions to relieve itself, and if these are left unassisted,
or not rendered unnecessary, they may prove the patient’s destruction.
The system may be drained of blood, and the body parboiled, without
the patient being relieved. The case requires immediate and decided
practice; for whilst the surgeon is consulting about what is to be
done, the urethra may give way, and the patient be lost. The discharge
of a small quantity of urine may follow the introduction of small
flexible bougies, up to the contracted point, but the bladder is not
relieved. The throwing of cold water on the thighs may, in slight
cases, induce such contraction of the expelling muscles as may overcome
the resistance in the urethra, and this method has been had recourse
to after failure with the catheter; but he must be a very poor surgeon
indeed who is foiled, when such practice afterwards proves successful.
Immediate recourse must be had to the firm silver catheter,
proportioned in size to the tightness of the stricture, and the
difficulties afforded to its introduction must be overcome by skill
and perseverance; it is no easy matter to pass the instrument in
many cases, and particularly when ineffectual attempts have been
made previously. By gentle insinuation, and perseverance in moderate
pressure, properly directed, the obstacle can always be overcome,—and
that without the infliction of any injury to the parts. I may here
observe, that I have never yet been foiled in passing the catheter,
though very many severe and difficult cases have fallen to my lot; in
other words, I have never been obliged to abandon my attempts to obtain
an exit for the urine by its natural passage, and, as a last resource,
to mutilate and endanger a patient by making an unnatural aperture
in his bladder. Yet circumstances may soon occur to me in which the
introduction of an instrument along the urethra shall be impossible; no
man, it has been said, can be always wise or always fortunate; and he
who pretends to invariable success must be either a knave or a fool.
Should the surgeon fail in passing the catheter, the bladder must485 be
relieved at all hazards; and if the prostate be sound puncture by the
rectum may be performed. This is neither a difficult nor a dangerous
operation, else it would not be so often resorted to; it does not
require so much skill and management as does the passing of a catheter.
Neither is it painful to the patient; the parts to be perforated are
thin, there is scarcely any effusion of blood, and all is done in the
dark. But it is an operation which should never be thought of, unless
as a last and desperate remedy; it is one in which I have had no
personal experience, though when a student of surgery I have seen it
done a few times. The procedure gives temporary relief, but then the
urethra still remains to be put into a proper condition; a man cannot
always void his urine and excrement through one common cloaca. If the
urethra be cleared, the recto-vesical aperture may soon close. After
the bladder is relieved, the urethra may become quieter, and admit
of an instrument being more easily passed; but it is of very great
consequence to effect the introduction of a catheter at the first.
Rather than puncture the bladder, the stricture should be cut down
upon, and an opening made into the dilated part of the urethra
behind the obstruction. A firm silver catheter is passed down to the
stricture, and retained there by an assistant; an incision in the
line of the central raphe—supposing the constricted part to be in the
perineal region—is made over the extremity of the instrument, the
contracted part of the urethra is divided, and the catheter passed on
into the bladder. Thus, even in the worst cases, the natural canal is
at once established. In every instance of difficulty and complication,
the catheter, however passed, should be retained for two or more days.
The above is the only admissible mode of puncturing by the perineum.
It has been proposed to reach the bladder from the perineum either
by extensive incisions or by the random thrust of a long trocar; the
latter mode is unscientific, the former is unnecessarily painful,
serious, and difficult; both are dangerous, and to be avoided.
The symptoms of extravasation of urine have been already detailed.
The practice must be bold, and adopted without hesitation or delay.
No bulging or fluctuation in the perineum is to be waited for. It is
to be kept in view, that the escape of urine into the open cellular
tissue may occur in a case of bad stricture, from rapid ulceration or
sloughing, without any of the dilated portion of the canal behind,
induration or abscess having preceded it; in the greater number of
cases the infiltration arises from the giving way of the parietes
of a cavity comunicating with the canal. Urinary infiltration thus
supervenes upon urinous abscess. Extravasation can never be mistaken or
overlooked by a man of any experience, and who is endowed with common
observation. The effect and extent of the perineal fascia must be borne
in mind; it diminishes or precludes—when the point at which the urethra
has given way is interior to it—external appearance of the mischief,
and by confining the deleterious fluid increases the infiltration
internally. A free and deep incision holds out the only chance of
relief; punctures or trifling scratches are worse than useless; neither
is there any need of passing bougies or catheters, or of puncturing the
bladder.
486
The following instructive case may be briefly detailed. A man applied
at a public hospital for relief, with a large swelling in the
hypogastrium, occasioned by extensive infiltration of urine into the
cellular tissue of the abdominal parietes. The tumour was mistaken for
distention of the bladder, and a long trocar was plunged in above the
pubes without a drop of urine escaping. The patient died during the
night. The bladder was found contracted, and the external cellular
tissue of the abdomen full of urine, from the giving way of the urethra.
When judicious and energetic practice is adopted without delay,
patients often make wonderful recoveries. The following may serve as
an example:—An elderly man laboured under retention, and his bladder
became distended to a very great degree; attempts had been made to
relieve him, but proved unsuccessful. A catheter was passed, and
retained for three days. During my absence in the country retention
again occurred, followed by extravasation. On my return I found him
insensible, but immediately turned him round in bed, and opened the
perineum freely, giving vent to fetid urine, sloughs, and matter.
Next day he was delirious, and knew no one; he hiccoughed, and had
cold extremities; “he fumbled with the sheets,” and “his nose was
as sharp as a pen.” A physician in attendance, well acquainted with
disease, declared that he could not live six hours. But the urine had
a free exit, the hiccough ceased on the exhibition of spiritus ammoniæ
aromaticus, and wine and brandy were poured into him liberally, the
only favourable symptom being, that he still retained the power of
swallowing—when that is lost, all is generally lost. He took soup along
with the stimulants readily and greedily, and, to the astonishment of
every one, recovered rapidly; afterwards the stricture was got rid of,
and restoration to perfect health completed. Many cases of similar
import might be related, all showing the great danger of extravasation
of urine, and the advantage of early and decided treatment. I once
also witnessed, in the Royal Infirmary, an unexpected recovery from
extravasation into the corpus spongiosum urethræ. This occurrence is
always attended with most imminent risk; and is generally the result
of retention from stricture. The urine escapes into the bulb, or
anterior to it. Alarming constitutional symptoms quickly supervene;
rapid sinking is threatened. The whole penis, scrotum, and perineum
are swollen, but the swelling is hard, and most marked in the glans
and along the course of the urethra. The glans blackens, unhealthy
abscesses form in the spongy body, and before these give way, or
at least before the sloughs begin to separate, the patient usually
perishes. The man to whom I allude, however, recovered, retaining
a part of the penis, as well as a considerable portion of its
integuments; the rest sloughed and were discharged.
In regard to retention from swelling at the neck of the bladder, it may
be observed, that spasm of that part of the viscus has been, by some,
considered as a cause of the affection; it is not easy to explain or
understand how this should occur, and such an idea is a bad one for him
to entertain who enters on the treatment of the disease. The capacity
of the bladder varies much in cases of enlarged prostate;487 in general
the organ bears a good deal of distention, and the urgent symptoms
do not appear rapidly. Nevertheless, it is the duty of the surgeon,
immediately on being called, to relieve the bladder. When the prostate
is very large, and retention has continued long, it is impossible to
reach the cavity by a common catheter. Those who employ this instrument
in such cases are often much puzzled; they continue long in their
fruitless endeavours, and, from rashness, generally produce a discharge
of much blood, but no urine; they then become alarmed on finding the
instrument always filled with coagulum, and suppose that blood has
been effused into the bladder, and that the symptoms of retention have
been thus introduced. A catheter is to be used, which is two or three
inches longer than the common one, possessing a larger curve, of such
a size as to admit of being passed easily, and not so small as to
render it liable to interruption from entanglement in the lacunæ of the
urethra. The posterior part of the urethra is elongated to no slight
extent by the enlargement of the prostate, and, besides, the whole
canal is stretched by the distended bladder rising high in the abdomen.
In short, the bladder is farther away from the surgeon than it is in
other cases of retention, and he requires an instrument proportionally
long in order to reach it. No time is to be put off. A cautious and
persevering endeavour must be made to bring away the urine by the
natural passage. Force is prejudicial and unnecessary. It is true
that the projecting third lobe of the prostate has not unfrequently
been perforated by the catheter, and no unpleasant consequences have
resulted, the urine continuing to flow, perhaps freely, through the
artificial opening there; but still it is always an injury, often an
unnecessary injury, and as such to be avoided. The catheter is to be
passed steadily on till it approaches the prostatic region; it is then
to be guided by the forefinger of the left hand introduced into the
rectum, and when the point is lost in passing through the gland, the
instrument is carefully carried forward by depressing the handle, and,
if long enough, it will infallibly reach the urine and relieve the
bladder. It must, indeed, be a very extraordinary case in which the
bladder cannot be reached with the catheter.
When enlargement of the prostate, whether of the whole gland or
principally of the third lobe, presents an insuperable obstacle to the
passage of the catheter, and when the surgeon has taken care to assure
himself that such is the case, I conceive that he ought to perforate
the gland in the direction of the natural course of the urethra, not
with the catheter, but with an instrument better adapted for the
purpose—a long canula, or catheter with open end, very slightly curved
towards the extremity, provided with two wires, one blunt and bulbous
at the extremity, the other pointed as a trocar, both made so as to
project a short way beyond the end of the canula. The canula is passed
on to the resisting body, its orifice occupied by the bulbous wire,
which is then withdrawn, and its place supplied by the trocar, the
instrument being held steadily in the proper direction. The trocar, or
stilet, is pushed forwards along with the canula; the former is then
withdrawn, and the latter retained. This proceeding I consider quite
safe in the hands of an experienced surgeon, one well488 acquainted with
the urinary passages—but not otherwise. It is in every way preferable
to puncture of the bladder above the pubes, to puncture behind the
prostate, or to puncture of the prostate along with wound of the rectum.
As before noticed, I never have had occasion to puncture the bladder
but once—and that was above the pubes, and for an unusual affection
of the bladder, the particulars of which have been already detailed.
The result of the experience of several eminent surgeons, both in this
country and abroad, is similar.
Elastic gum catheters have been recommended in this affection, and it
is said that after the instrument has been passed to the prostatic
region, its entrance into the bladder is facilitated by gently
withdrawing the stilet, the point of the catheter being thereby
curved upwards, and, as it were, lifted over any central projection
of the prostate that may impede its straightforward introduction. But
according to my experience, this instrument is far inferior to the firm
and long silver catheter.
In all cases of retention when the urine cannot be brought away per
vias naturales, and when no farther assistance or advice can be
procured immediately, the surgeon should puncture the bladder rather
than leave the patient to his fate; and the operation should be
performed early. He must not temporise till all chance of recovery has
gone by. By not operating till late, in this or any other disease, when
by the delay no reasonable chance of saving the patient remains, our
department of the profession is brought into discredit and contempt.
Delay is more dangerous than even the worst mode of making an opening
into the bladder; and while life exists, the patient should have his
chance. Some defer extreme measures from day to day, either from
hesitation or from a false hope that matters may ultimately change for
the better, but the delay of one hour is in many cases most hazardous.
In retention from disease of the prostate extravasation of urine is
more dangerous—more certainly fatal—than in other circumstances.
Here a part of the vesical parietes gives way by sloughing, and the
fluid is effused within the ilio-vesical fascia; in other cases the
extravasation is usually beyond that fascia, and beneath the fascia of
the perineum.
Puncture by the Rectum is, in cases of enlarged prostate,
inadmissible and highly dangerous; the operator must either perforate
the gland, or enter the cavity of the abdomen. Even in the healthy
state of parts, there is very little space between the posterior part
of the prostate and the reflection of the peritoneum. The operator
having ascertained that the prostate is sound, and the rectum empty,
introduces the fore and middle fingers of the left hand into the bowel,
and along these passes a trocar and canula from four to five inches
in length, of moderate calibre, and of a curve rather greater than
that of the sacrum. He places the point of this instrument on the part
to be perforated, and fixes it there, the point of the trocar being
hitherto withdrawn within the canula; the stilet is then protruded,
and both carried onwards into the bladder. The part to be perforated
is immediately behind the prostate and in the mesial line. Puncture
above the Pubes is easily enough performed when the489 bladder is
capacious, but it is at best a dangerous operation. The wound is made
through loose cellular tissue; urinary extravasation into that tissue
is apt to occur, and often proves fatal. If the bowels are inflamed, or
evince a tendency towards inflammatory action, the danger is increased,
for a formidable wound is made in the immediate vicinity of the bowels.
The operation has been resorted to when the catheter might have been
passed without much difficulty; this statement may appear harsh, but
it is too true, and can be borne out by indisputable facts. It is
brought forward more as a caution to the young than as a reflection
on the senior members of the profession. Some patients have recovered
from the operation, and lived in misery for months and years, passing
their urine through a canula retained in the wound. An incision is made
above the symphysis pubis, in the mesial line, dividing the integuments
and cellular tissue, to the extent of from one to two inches; on thus
exposing the coats of the bladder, a flat trocar with a canula is
pushed into the cavity of the viscus, at the lower part of the wound;
the trocar is withdrawn, and the urine evacuated.
The treatment of enlarged prostate is palliative—attention to the
general health, the occasional administration of anodyne suppositories
or enemata, prevention of accumulation in the lower bowels, either by
gentle laxatives or the throwing up of bland fluid, and the avoiding as
far as possible all sources to excitement, of mind as well as body. The
radical cure, it has been said, is extirpation of the gland, but the
cool proposal of such an operation would indicate either ignorance, or
dereliction of principle, or mental obliquity, or all combined.
In retention from effusion of blood into the cavity of the bladder, a
long catheter will sometimes evacuate the urine, and after some time
also the blood; for the latter, though at first coagulated, ultimately
becomes dissolved in the urine, and passes off along with it, even
through a catheter of no very large calibre. Should this fail, and the
symptoms continue urgent, an exhausting syringe should be employed,
well adapted to the extremity of the catheter. After the urine has been
thus evacuated, should a suspicion remain of coagula being still in the
bladder, tepid water may be injected with the view of promoting the
breaking down of the clots, and then the exhaustion may be repeated.
Incontinence of Urine, as already observed, is a common result of
distention of the bladder and of stricture. But it also occurs as a
primary affection, particularly in young people, from irritability
of the posterior part of the urethra not suffering the urine to
accumulate within the bladder as in ordinary circumstances. It is
sometimes removed by the application of a blister to the perineum,
and by the patient attending to empty the bladder at intervals during
the night. Attention to the state of the bowels is necessary in such
cases. The clearing them of worms or sordes, and the exhibition of
tonics is sometimes also useful. Children, and even mothers, sometimes
have recourse to a more effectual method, the application of a tight
ligature round the penis. But of the folly and danger of such practice,
the following may serve as an example. A. R., when 8 years old, passed490
a brass curtain-ring over his penis to prevent incontinence of urine
during the night, and thereby escape chastisement, to which he had
been frequently subjected. Great swelling soon took place round the
ring, and he was unable to remove the jugum. He experienced much pain
and difficulty in voiding his urine; the integuments under the ring
gradually ulcerated, the ring appeared to sink into the substance of
the penis, and the swelling subsided. The integuments met and adhered,
the foreign body was concealed, and all uneasiness soon ceased. The
penis performed well all that was required of it; the urine passed
easily, and after a while he became the father of a fine family. When
between fifty and sixty years of age, he applied to me. For some years
previously difficulty in making water had been coming on, and frequent
desire to pass it in the night-time rendered him very uncomfortable.
He was under the necessity of having a vessel constantly in bed, and
was generally disturbed every half hour. The penis had become very
unserviceable, and he was now anxious to have the ring removed. A
broad hard substance was felt surrounding the penis, close to the
symphysis; an incision was made into the urethra at that part, and a
calculus easily extracted. The uneasy symptoms quickly disappeared,
and the patient recovered with a small fistula at the incised part,
which could have been removed without difficulty, had not all treatment
been obstinately resisted. The calculus resembled a prune in size, of
a crescentic form, with one of the apices detached, and was apparently
composed of uric acid, coated with the ammoniaco-magnesian phosphate.
On making a section of it, about two-thirds of the brass curtain-ring,
partially decomposed, were found firmly impacted in the centre. It
would appear that a portion of the ring had speedily made its way into
the urethra, had been acted upon and washed away by the urine; while
the remainder, coming more gradually in contact with that fluid, had
become incrusted with deposit, and formed the nucleus of the calculus.
It is strange that the penis should have been efficient,—that the
erectile tissue should have remained pervious—after having been cut
completely through near the symphysis.
Of Gonorrhœa Præputialis vel spuria.—By this term is understood
discharge of puriform matter from the lining membrane of the prepuce,
and from the surface of the glans, accompanied with an itching and
smarting sensation. The affection may arise from mere inattention
to cleanliness, the natural secretion being allowed to collect and
deteriorate; or from the application of acrid matter, gonorrhœal,
or leucorrhœal. It often attends discharge from the urethra, and is
usually met with in those who, from the natural tightness of the
prepuce, uncover the glans with difficulty, if at all. It may occur
without impure connexion; mucous discharge accumulates, becomes
acrid from stagnation, and is washed away by profuse secretion of
puriform matter; the parts then become quiet, and resume their healthy
functions, but are apt from slight causes to be again the seat of
discharge. Generally, the surfaces of the prepuce and glans are relaxed
and turgid, but there is no breach of continuity; in neglected cases
there is superficial patchy ulceration, and sometimes a deep and
sloughing sore. The matter is often confined by tightness of the491
præputial orifice, and mischief thereby occasioned to the glans;
a large purulent collection forms, and, if the case is neglected,
ulceration takes place, either of the glans or of the prepuce, or of
both; the latter becomes thin, and at length gives way; the aperture
thus formed extends, and occasionally is of such a size as to admit
of protrusion of the glans. Œdematous swelling generally takes place
to a great extent in such cases. The glands of the groin sometimes
swell, and through inattention may suppurate. The absorbents of the
penis may also become turgid and painful. Tenderness of the glands and
prepuce often exists, in a greater or less degree, for years; in such
circumstances the affection may be termed gleet of the prepuce, and is
usually the consequence of irritable urethra.
The treatment consists in cleanliness and rest, applying astringent
washes to the parts, and suspending the organ. When swelling of the
prepuce or inflammation of the lymphatics is threatened, constant rest
must be enjoined. In obstinate cases, disease of the urethra is to be
suspected as the cause, and the state of that canal should therefore be
ascertained; if derangement of structure or function is detected, then
means must be forthwith adopted for its removal, the applications to
the prepuce and glans being at the same time not neglected. Mercury can
be of no use.
Phymosis and Paraphymosis are often connected with gonorrhœa of the
prepuce, or of the urethra. The edge of the prepuce may be rendered
tight by inflammation, swelling from effusion, or cicatrisation
of sores; the tightness also attends irritability of the urethra,
particularly in young subjects; often it is congenital. The affection
is termed Phymosis when the prepuce occupies its natural relative
situation, but cannot be drawn back so as to uncover the glans. The
contraction exists in various degrees; sometimes the orifice is so
tight that the flow of urine is obstructed, the præputial cavity
becoming swelled and distended every time the patient attempts to
make water. In other instances the uninjected glans can be exposed
either in part or entirely, though with difficulty. In consequence
of the præputial cavity being frequently filled with urine, in cases
of great contraction, urinary concretions have even formed or been
detained there or in the orifice of the urethra, giving rise to very
annoying, and sometimes alarming, symptoms. In consequence of Phymosis,
the urethra and bladder may become diseased. It is often attended
with profuse puriform discharge, with sores of different kinds, or
with warty excrescences on the glans and prepuce; sometimes the whole
surface is completely covered with granulated prominences of various
sizes, some large, but the majority small, some broadly attached,
others suspended by narrow necks; all generally furnish discharge of
thin acrid matter. Adhesion may take place between the raw surfaces of
the prepuce and glans, provided the parts be not frequently displaced
for the purpose of ablution.
Paraphymosis arises from the same state of the orifice of the prepuce
as the former affection, only the parts are in different relations
to each other. In phymosis the prepuce covers the glans, the tight
part is anterior to it; in paraphymosis the prepuce is reflected over
the492 glans, the tight part acts as a ligature round the penis behind
the glans, and such swelling speedily arises in consequence of the
constriction so as to prevent reduction. The glans and lining membrane
of the prepuce swell anteriorly to the stricture, the integuments of
the penis swell behind, and the stricture is depressed and concealed
between. The cellular tissue there is necessarily very loose, so
as to admit of free motion and change of relative position, and
consequently the engorgement is often very great. The infiltration
is at first serous, and the swelling is easily compressed; but, from
continuance of the inflammatory action, lymph is effused, and becomes
organised, and the turgescence is more solid and unyielding. When the
stricture is very tight, the patient cachectic and irregular in his
mode of life, and the case injudiciously or inertly treated, sloughing
takes place rapidly, or phagedenic ulceration occurs anterior to the
stricture. But in most cases the prepuce is not so tight as to cause
complete strangulation, yet obstructs the flow of blood sufficiently
to induce swelling of the included parts, breach of surface more
or less extensive, and an unhealthy appearance of the ulceration.
The ulceration is generally in the neighbourhood of the stricture,
at first limited and superficial, but increasing both in depth and
extent so long as the cause remains. The stricture is not situated
anteriorly to the swelling, as has been sometimes supposed, but near
its middle—where the tight orifice of the prepuce grasps the penis, and
causes a depression in the swelling. On separating the anterior and
posterior tumours, the stricture is readily exposed, though previously
effectually concealed.
In slight cases of phymosis, the orifice may be dilated by frequent
fomentation, and perseverance in withdrawing the prepuce as far
as possible. When ulceration or secretion of matter has occurred,
astringent injections, at first mild, and gradually strengthened,
should be frequently thrown into the præputial cavity. Suspension of
the penis should be enjoined, along with rest—of the whole body, as
well as of the affected organ in particular. When much inflammation
exists, antiphlogistic remedies must be put in force, followed by
fomentations. In bad cases, the prepuce must be divided in order to
expose the seat of morbid secretions, of ulceration, and vegetations.
The preferable situation for incision is close by the side of the
frænum, much less deformity ensuing than when the prepuce is divided
either laterally or in front. The flaps are at first loose and flabby,
but shrink as the œdematous swelling subsides. A straight director
is introduced within the præputial orifice—the groove pointing
downwards—and passed down to the reflection, close to the frænum; a
sharp-pointed curved bistoury is slid along the groove till it also
reaches the reflection; by raising the handle and pushing it forwards,
the integuments are transfixed there, and withdrawal of the knife by
a rapid sweep completes the incision. Care must be taken not to pass
the director into the urethra instead of into the præputial cavity. It
is very seldom that ligature is required to arrest bleeding. Should
the cellular tissue of the divided part not have been the seat of
solid effusion, the integument and the lining membrane of the prepuce
separate, leaving a large raw surface; and to prevent this a small493
suture should be passed between the membrane and skin on each side
of the wound; these may be withdrawn on the second or third day, the
cellular tissue having then become consolidated, so as not to admit
of retraction. A warm bread poultice, or water dressing, is the best
application for the first few days; afterwards healing of the cut
surfaces may be promoted by the application of a gently stimulating
lotion. Should œdema of the prepuce remain, this may soon be effaced
by bandaging. By this operation sufficient space is obtained for
uncovering the glans, under any circumstances; and besides, to this
part of the organ is still preserved its natural investment, not in
the least curtailed either in size or in efficiency—the glans can be
uncovered and covered at will; whereas by any other mode of incision
the unseemly flaps always fall away, leaving the greater part of the
glans constantly uncovered, and placing the patient, if not in a worse,
at least in the same predicament, as if he had been subjected to
regular circumcision.
There is danger in allowing the state of phymosis to exist long; it has
been already observed, that this condition of the parts predisposes to
ulceration, vegetations, and morbid secretions; but besides, experience
has shown, that very many cases of cancer of the penis are attributable
to phymosis, either congenital, or of long duration. In all cases, when
the orifice of the prepuce is so tight as not to admit of exposure of
the glans, the operation is expedient, the existing state of parts
being very inconvenient; but it becomes a matter of absolute necessity,
when there are extensive sores on the prepuce or glans, when there is
much tumefaction or hardening of the parts, when urinary concretions
lodge in the præputial cavity, or in the orifice of the urethra, when
vegetations or warts form on the glans, and when the præputial orifice
is so contracted as seriously to impede the flow of urine.
In paraphymosis there is a necessity for early interference, in
order to save the organ; indeed active and decided measures are as
imperiously called for here, as in the case of strangulated hernia: and
it ought to be remembered that the organ is one of importance, and that
its loss would render most people very miserable. To attempt relaxation
by fomentations, and such like, is absolute folly; the stricture cannot
yield to such remedies; and, from increase of swelling, strangulation
will become more and more complete. Cold, too, is incapable of reducing
the swelling; cold, or astringents, cannot possibly diminish the size
of the vessels, whilst return of the blood in them is prevented by
tight stricture; and so long as the stricture remains, the serous
effusion cannot subside, but will increase. Besides, the application
of cold may hasten the occurrence of gangrene, inasmuch as it tends to
diminish the power of parts which are already in a weakly condition.
The parts must be instantly replaced. With the fingers of the right
hand, the surgeon grasps the glans, and by firm and continued pressure
diminishes its volume, whilst with the left he endeavours, by steady
pulling, to reflect the swollen prepuce over the glans, which he is
at the same time pushing back, as well as lessening. By uniformity
and perseverance in these manipulations, more than by any force,
replacement will often be accomplished.494 He will be able to judge,
from the duration of the disease, and from the appearance and feel of
the parts, whether simple reduction, that is, without having recourse
to the knife, be practicable or not. In some cases, particularly when
gangrene is imminent, and when the ulceration is extensive, there is
danger of materially injuring the glans, if attempts at reduction are
injudiciously persevered in. When he is foiled in reduction, or deems
the attempting of it imprudent, the stricture must be divided; and in
this simple operation great errors are often committed from ignorance
of the nature of the disease, and of the relative situation of the
parts. It is necessary to divide only the edge of the prepuce, which,
from being reflected, alone composes the stricture. The anterior
and posterior swellings are to be separated as far as possible, and
in the very bottom of the depression between them the stricture is
exposed; a slight incision, a scratch, through this, either with the
point of a bistoury, or with a lancet, is sufficient; the tight edge
of the prepuce—the only part in fault—is divided, and then, by the
process already detailed, reduction can be readily effected. After
reduction, a minute notch in the extreme edge of the prepuce is the
only deformity visible, except the swelling. But if, from ignorance of
the true seat of the stricture, extensive incisions have been made,
pretty much at random, the organ may be considerably disfigured—and
that unnecessarily. By fomentations, rest, and low diet, the effusion
will be dissipated in a very few days. Reduction is difficult when the
contraction has continued for some time, and the tissues have become
glued together by effused lymph.
Malignant ulcer, with induration of the surrounding parts, and
contamination of the lymphatics, occurs occasionally on the glans
penis, or on the lining membrane of the prepuce. As before observed, it
is most frequently met with in those who have laboured under congenital
phymosis; in that state of the organ, its extremity is apt to inflame,
swell, and ulcerate, in consequence of accumulation and acrimony of the
secretions from the membrane of the prepuce; indolent swellings form
in the groin; and in one case, I recollect, these assumed a malignant
action, a frightful ulcer formed, and the patient was destroyed, after
division of the prepuce, and after the ulceration on it had been
long healed, and the part had apparently become quite sound. Early
removal of the diseased part, by incision wide of the indurated and
altered structure surrounding the ulcer, is the only means of saving
the patient, of preventing glandular inguinal tumour, ulceration
of it, hemorrhage, hectic, and death. When the prepuce solely is
involved, removal of this is sufficient, either entirely or in part,
as circumstances may demand. When the glands and coverings, as also
the body of the organ, are involved, amputation is to be performed,
provided the lymphatics still appear unaffected. In this operation the
integuments must be freely removed, otherwise the cut orifice of the
urethra will be obstructed by their puckering and contraction during
cicatrisation of the wound. With this view, the skin is drawn forwards
and stretched by the left hand, and then with one sweep of a long knife
a transverse incision is made at once through all the parts composing
the organ. Two or three vessels by the side of the septum may require
ligatures. The skin retracts495 considerably, leaving the cut surface
free; the wound granulates, contracts, and cicatrises. It is advisable
to cut the urethra a little longer than the body of the organ. If
diminution in the canal of the urethra be threatened during the
cicatrisation, it is to be obviated by the occasional use of a short
conical bougie.
Imperfections about the orifice of the urethra are by no means
uncommon. Often there is a mere vestige of the orifice of the urethra
in the natural situation, the opening being situated half an inch or a
whole inch behind, and on the lower part—Hypospadias; in such cases
the prepuce is generally short.
Sometimes the urethra is deficient to a great extent, terminating
immediately before the scrotum, or even behind it. A child had passed
no water thirty hours after its birth. The bladder was distended. The
genital organs were imperfect; the urethra was wanting, and the penis
was diminutive and abnormal. A small trocar was passed from the vestige
of the orifice onwards, in the proper course, guided by the finger in
the rectum. The urethra seemed to have terminated at the bulb; the
canula reached this, and was retained for twenty-four hours. Afterwards
the urine passed readily through the canal, partly natural, but
principally artificial, and the power of retaining it became perfect.
In adults the hypospadias is inconvenient; the orifice is often
contracted, and the whole parts are irritable; and the ejaculation
of the seminal fluid is unsatisfactory to the parties concerned. The
deficiency may be repaired in some measure, when there is abundance
of skin to spare, but no rules can be laid down for such irregular
operations.
Imperfection of the urethra anteriorly, on the dorsum, is
rare—Epispadias. The following is rather a remarkable instance:—The
man was aged 26, robust and healthy. The whole extent of the urethra
anterior to the pubes was exposed superiorly, there being a wide
fissure through the corpora cavernosa and glans. The penis was
retracted considerably, so that the posterior part of the fissure
lay beneath the symphysis pubis. The numerous lacunæ of the urethra
were beautifully distinct, and the mucous membrane was seen covered
by their secretion. When the patient made water, the urine, after
emerging from beneath the pubes, divided into numerous small streams,
some of which spread over the side of the penis, while others passed
along the exposed urethra. The callous margins of the fissure, formed
by the corpora cavernosa and glans, were carefully pared, and, a
catheter having been introduced, the raw surfaces were retained in
apposition by suture. The wound healed perfectly, almost entirely by the
first intention; and the organ both looked well and proved efficient.
The malformation was congenital, and was considered by the patient
as analogous to harelip; but the story related to account for it in
consequence of an impression made in his mother’s imagination, was not
very plausible.
The disease of the external parts of the male genital organs,
commonly called Chimney-sweeper’s Cancer, is one of a formidable
and496 intractable nature, but fortunately not very often met with. The
scrotum is the part usually attacked. A wart forms, generally at the
lower part, assumes an irritable appearance, and quickly degenerates
into open ulceration of a malignant character. The ulcer extends
rapidly, consuming the neighbouring integument, and involving the
testicle and other subjacent parts in induration and enlargement.
The induration extends along the spermatic chord, and the lymphatics
participate in the diseased action at an early period. The discharge
from the sore is acrid, sanious, and possessed of much fetor; sometimes
fungi protrude, but more commonly the surface is excavated and smooth.
Not unfrequently the skin surrounding the ulcer is studded, to a
considerable extent, with numerous clusters of warts, of an unhealthy
and angry aspect. A very aggravated specimen of the disease is here
represented. The general health is soon undermined, and the disease
advances from bad to worse with the usual certainty and rapidity of
malignant action. It seldom occurs till after the age of thirty or
 forty; and though most frequent in chimney-sweeps, is not peculiar
to them. No treatment can be expected to arrest its progress at an
advanced stage; the only opportunity of saving the patient is at the
commencement of the disease, when the affected part is small, and
before the lymphatics have become involved. Local application and
internal remedies are not to be trusted to; in the early stage the
parts may be excised. An incision is made wide around the wart or
ulcer, and the included parts are dissected away to a considerable
depth. When the testicle has become affected, the chance of success is
much diminished; but still, if the inguinal glands appear sound, and
the chord tolerably free, castration is to be performed as the last,
though desperate, means of eradicating the disease.
forty; and though most frequent in chimney-sweeps, is not peculiar
to them. No treatment can be expected to arrest its progress at an
advanced stage; the only opportunity of saving the patient is at the
commencement of the disease, when the affected part is small, and
before the lymphatics have become involved. Local application and
internal remedies are not to be trusted to; in the early stage the
parts may be excised. An incision is made wide around the wart or
ulcer, and the included parts are dissected away to a considerable
depth. When the testicle has become affected, the chance of success is
much diminished; but still, if the inguinal glands appear sound, and
the chord tolerably free, castration is to be performed as the last,
though desperate, means of eradicating the disease.
By Hydrocele is meant a tumour caused by accumulation of fluid either
in the chord or within the cavity of the tunica vaginalis testis. It
has been divided into diffused and encysted. By the former term is
understood effusion and accumulation of serum in the cellular tissue,
the cells gradually dilating to accommodate the increasing fluid, and
ultimately becoming converted into vesicles of large size: the parts
around are thickened and condensed. This affection is very rarely a
local one, but almost uniformly combined with and forming a part of
anasarca arising from constitutional causes. When the swelling proves
troublesome, it may be diminished by drawing off the fluid through one
or several punctures; in the chronic form of the disease free incision
is attended with risk, and is besides unnecessary.
The scrotum is sometimes distended rapidly by effusion of serum often
of a putrescent and acrid nature. This affection supervenes497 upon
ulcers or sinuses in the groin, perineum, or neighbourhood of the anus,
in patients out of health. It occurs also occasionally as a consequence
of injury of the genital organs, or interferes with bad strictures,
without any disease of these parts, and without the least cause for
the suspicion of urine having escaped into the cellular tissue. This,
together with the skin, is destroyed, and the testicles exposed. The
only chance of saving the tissues consists in early and free incision
of the most dependent part of the swelling, generally the inferior and
posterior. Some cases and remarks on this subject will be found in the
Medico-Chirurgical Transactions, vol. xxii., p. 288.
Encysted hydrocele of the chord occurs in children more frequently than
in adults. The fluid is thin and clear, and contained in a distinct
cyst, of a smooth, shining, serous appearance internally; this cyst
may be either an unobliterated portion of the congenital spermatic
process, or composed of thickened and condensed cellular tissue,
strengthened exteriorly by the expansion of the cremaster muscle. The
tumour is seldom large, usually of an oval form, and situated nearly
midway between the testicle and groin; causing no pain, but proving
inconvenient simply from its bulk and situation; fluctuating, and
sometimes partially diaphanous; evidently circumscribed, the chord both
above and below being natural to both sight and touch; not altered by
change of posture or by muscular exertion. Sometimes it encroaches both
on the groin and on the testicle, but even then attentive manipulation
readily distinguishes it from swellings connected with these parts.
Discharge of the fluid by means of a small trocar and canula, not
only dissipates the swelling, but often effects a permanent cure,
particularly in young persons—the cyst either ceasing to exercise a
secretory function, or becoming obliterated. If reaccumulation take
place, the treatment is to be conducted on the same principles as in
hydrocele of the vaginal coat.
Hydrocele of the tunica vaginalis is exceedingly common, particularly
amongst labouring people, and occurs apparently with equal frequency at
all ages. It is a gradual accumulation within the tunica vaginalis of
a fluid partaking more or less of the serous character, furnished by
the exhalants of that membrane,—but whether from excessive secretion
or deficient absorption, it is difficult to determine. It is probable
that the accumulation is the result of excited action in the part, for
its origin is most frequently attributable to external injury—blows or
bruises, followed by rapid swelling, which, after a time, subsides,
leaving perhaps some enlargement of the testicle, or of the more
superficial tissues, and succeeded by the gradual appearance of the
disease in question. Sometimes it is attributed to powerful and
habitual muscular exertion, as in blowing wind instruments, lifting
heavy weights, &c.; and perhaps the impediment to the venous return,
so produced, may be the cause of the effusion. The accumulation, as
already stated, is gradual, and consequently the formation of the
swelling is proportionally slow. It commences at the lower part of
the scrotum, and by degrees ascends, at first globular, afterwards
of a pyriform shape; after it has attained a considerable size, the
testicle cannot be felt in its usual situation, for it is now placed
not at the bottom of the bag but towards its middle and posterior498
aspect, and if the tumour be tense it can scarcely be felt at all.
The raphe is displaced to the opposite side, the usual puckering of
the scrotum has disappeared, and the tumour feels light in proportion
to its size. On manipulation it is found yielding and elastic, and
in all ordinary cases a distinct fluctuation is communicated to the
fingers during alternate pressure. And by using the hand as a shade,
the rays of light are made to permeate the swelling, rendering it
more or less transparent according to the thickness and density of
the covering, and the hue of the contained fluid. It is seldom that
the distention of the vaginal coat is to such an extent as to reach
the groin, consequently the spermatic chord is felt to be free, as
also the inguinal aperture; and even when the swelling does reach so
high, the upper part is the least tense, permitting displacement of
the fluid and distinct perception of the chord. The patient complains
of a sense of dragging and weight in the parts, and of uneasiness and
inconvenience during exertion, but seldom of pain. When large, the
tumour is necessarily covered by borrowed integument, often so as
almost entirely to conceal the penis. In many cases the testicle is
increased in size and indurated, and sometimes this enlargement forms
a considerable part of the swelling. Occasionally the spermatic veins
are varicose; and this has been, by some, considered one of the causes
of the disease. Hydrocele is occasionally complicated by the presence
of hernia, when a careful examination must be instituted in order to
understand the exact share each disease has in the production of the
swelling. In cases of very slow increase, and in persons of advanced
age, the vaginal coat and its investments are not unfrequently much
thickened, so as to obscure the sense of fluctuation, and destroy the
transparency of the tumour. Sometimes deposit of earthy matter takes
place between the layers of the membrane, rendering it hard, rigid,
and in a measure osseous; in such cases cholesterine has been found in
the contained fluid; sometimes the cavity is intersected by membranous
filaments, delicate and reticulated; sometimes complete septa subdivide
it into several compartments. The fluid is generally thin, albuminous,
and of a straw colour; in some cases paler, and coagulating on cooling,
being gelatinous; in others of a dark colour, probably from admixture
of blood.
The treatment is either palliative or radical. The former consists
in evacuating the fluid from time to time, according as the feelings
of the patient demand it; in children this simple tapping is often
successful in preventing return of the disease. But here the disease
often enough disappears under the use of a stimulating lotion, as a
strong solution of the muriate of ammonia.
The swelling is grasped from behind by the left hand, and compressed
so as to render the middle and fore part tense and prominent; into
this a trocar and canula are plunged, piercing the coverings in a
perpendicular direction, and then inclining the canula upwards, the
stilet having been partially withdrawn, so as to avoid wounding the
testicle. The venous branches apparent on the surface must be of course
avoided. When fairly passed within the cavity, the trocar is withdrawn
entirely, and the fluid escapes through the canula—gentle pressure
being employed towards the conclusion.499 The wound usually heals in a
few hours. Various means of radical cure have been proposed—incision,
seton, caustic, and the injection of stimulating fluids. Incision and
the seton are now abandoned, and do not require notice. The application
of caustic perhaps may prove efficient in children when tapping has
failed, and in youths; an aperture is thus made, through which the
fluid escapes, and at the same time considerable excitement is induced,
which may prevent reproduction. I at one period made trial of it in
several instances, and generally with success; but am now inclined to
avoid it, having more than once experienced much difficulty in keeping
within moderate bounds the inflammatory action which succeeded its
application. Injection is now generally practised; and if carefully
performed, it is unattended with risk, and is almost invariably
successful. Various fluids may be employed—cold water, wine, wine
and water, spirits, a solution of the sulphate of zinc, &c. I have
generally used pure port wine; and have scarcely ever seen its effects
either excessive or deficient. I can remember very few cases in which
the disease returned after this injection. Having ascertained that the
testicle is sound, or but slightly enlarged—for injection of the tunica
vaginalis is incompatible with diseased testicle—the fluid is drawn
off by means of a round trocar. The canula is left in the wound, and
to it is adapted the nozzle of a brass stop-cock attached to a small
elastic bottle. By means of these instruments the wine is injected in
sufficient quantity to distend the tunic moderately, taking care that
the extremity of the canula is completely within the cavity, otherwise
the cellular tissue will be injected, and violent inflammation ensue,
terminating in unhealthy suppuration and sloughing. By turning the
cock, the wine is retained until the patient begins to feel pain
shooting upwards to the loins, when it is to be evacuated. He may not
feel any uneasiness, however, and then it will be necessary to draw
off the fluid and inject a fresh quantity. If this, too, fails, a more
stimulating fluid must be used, a solution of sulphate of zinc, spirits
and water, or pure ardent spirits. It is supposed that this treatment
is effectual by inducing adhesive inflammation, and obliteration
of the cavity by adhesion of the tunica vaginalis to the tunica
albuginea; but this does not by any means frequently happen. There
may in some cases be a little lymph deposited, but not in sufficient
quantity to cause adhesion. The excitement following injection seems
to change the action in the parts without altering their structure or
relation—to reëstablish the healthy balance between the exhalants and
absorbents. Its first effect is to produce increase of swelling from
fresh effusion into the cavity of the tunica vaginalis, accompanied
with redness of the integument and considerable pain—sometimes with
slight fever. This fluid, however, is quickly absorbed—usually in from
four to six days—the swelling subsides, as also the pain, and the
patient remains free of the disease. Whilst this salutary action is
in progress, the recumbent posture must be strictly enjoined, along
with low diet and suspension of the organ; and sometimes, though
rarely, it may be necessary to have recourse to more active means to
moderate inflammation. Should the excitement appear insufficient after
a day or two, the surfaces500 may be rubbed against each other with the
fingers, and gently squeezed, or the patient may be directed to walk
about occasionally through his room until pain is felt. If the disease
return, as need scarcely be dreaded, injection is to be repeated,
either again with wine, or with a more potent fluid.55
501
The term Cirsocele is applied to varix of the spermatic veins. The
affection seldom extends to the inguinal aperture, and is usually
situated on the left side.56 The tumour is somewhat pyriform,
the larger extremity resting on the testicle, and by its peculiar
appearance and feel its structure is at once apparent; the veins are
seen through the integument. Pressure from below upwards, during the
recum502bent posture, diminishes the swelling; pressure above augments
it, particularly if the patient change his posture, and exert the
abdominal muscles. Sometimes a dull pain in the back is complained
of, relieved by suspension of the scrotum, and often wasting of the
testicle slowly advances. In some cases the swelling attains a large
size, elongating the scrotum, and proving a source of very great
uneasiness to the patient—so great that some have requested and urged
castration.57 Commonly it is sufficient to wear a bag truss, and
avoid all causes of irritation to the parts; thus increase of swelling
is prevented, and the inconvenience rendered trifling. If pain,
with redness of the integument, and additional enlargement, should
supervene, rest and the recumbent posture must be enjoined for a time,
combined perhaps with low diet and local depletion. But in cases of
large inconvenient tumour, accompanied with atrophy of the testicle,
rather than accede to the wishes of the patient and perform castration,
the treatment recommended many centuries ago may be put in practice—the
application of a heated wire to the veins. The upper part of the tumour
is grasped and made prominent, the veins are separated as much as
possible from the other parts composing the chord, and a small-pointed
cautery, a glover’s needle, for example, is inserted at several points.
This is followed by some pain, and increase of swelling. Inflammation
and obliteration of the veins is produced at the cauterised points, the
swelling gradually diminishes, and ultimately a dense chord is all that
remains. The cure is radical, and I have never seen the effects prove
too severe. Rest and antiphlogistic regimen are of course necessary for
some days after the application; abstraction of blood will seldom be
required. Within the last few years I have been in the habit of passing
two needles under503 the veins at an interval of about half an inch from
each other, and twisting a thread firmly over them and the superimposed
integuments. Of course the other parts of the chord are held aside by
the finger and thumb, and the needles are withdrawn within a few days;
as soon, in short, as consolidation of the interposed substance has
taken place. This operation is preferable to any other.58
Hæmatocele is an effusion of blood, either into the cellular tissue
of the scrotum, or within the tunica vaginalis, or in both. It is
generally the consequence of a bruise or wound. From the loose nature
of cellular tissue, the effusion into it is apt, if proper attention be
not given, to take place to a great, and, to the patient and friends,504
alarming extent. This I have witnessed after the operation for hernia,
and after removal of the testicle—bleeding from some small artery
continues, the blood is by the dressings or pressure prevented from
escaping externally, it is consequently extravasated into the cellular
structure, giving rise to tumour, often of a very dark colour; and in
some cases this swelling, occurring after the operation for hernia, has
been mistaken for re-descent of the bowel. The blood must either be
absorbed or discharged. Absorption is the more safe and desirable, but
necessarily tedious, and more or less thickening and enlargement may
remain for a long time. Discharge, whether spontaneous or by incision,
is usually followed by unhealthy suppuration of the infiltrated
and partially broken down cellular tissue, sloughing of it, tardy
separation of the dead parts, and tedious, perhaps exhausting, flow of
matter.
Hæmatocele of the vaginal coat may supervene on hydrocele, in
consequence of external injury; or bloody effusion may take place from
the vessels of the membrane, from sudden abstraction of their customary
support, after evacuation of the serous fluid, and whether injection
has been resorted to or not;—as happens in careless tapping for
ascites. Some of the diagnostic marks of hydrocele are thereby lost;
there is no translucency of the swelling, and fluctuation is either
indistinct, or altogether imperceptible. The appearance of the contents
varies according to the time which has elapsed betwixt their discharge
and the occurrence of the extravasation; if short, coagula float in
a thin bloody fluid; if considerable, the liquid is thick, dark, and
putrid.
Bloody effusion into the scrotal cellular tissue produces a dark
appearance of the integuments, and the swelling has a doughy feel. At
one or more points, where the cells are broken down and much blood
 has collected, fluctuation is perceived more or less distinct. The
treatment consists of rest, the recumbent posture, support of the
swelling on a small cushion, and the employment of fomentation when
the parts are painful. The absorption proceeds slowly; and after some
time, when all painful feelings have ceased, stimulant embrocation may
be used, with the view of expediting it; a solution of the muriate of
ammonia, of the sulphate of alumina, or of other astringent stimulating
salts, may be employed in strength proportioned to the feelings of the
patient and the progress of the case. If the tumour suddenly become
painful, and increase in size, indicating putrefaction of the blood,
and commixture of it with puriform matter, a free incision is to be
made, and poultices applied. When the parts have become quiet, and
suppuration has been established, poulticing is to be discontinued, and
mild and light dressing employed.
has collected, fluctuation is perceived more or less distinct. The
treatment consists of rest, the recumbent posture, support of the
swelling on a small cushion, and the employment of fomentation when
the parts are painful. The absorption proceeds slowly; and after some
time, when all painful feelings have ceased, stimulant embrocation may
be used, with the view of expediting it; a solution of the muriate of
ammonia, of the sulphate of alumina, or of other astringent stimulating
salts, may be employed in strength proportioned to the feelings of the
patient and the progress of the case. If the tumour suddenly become
painful, and increase in size, indicating putrefaction of the blood,
and commixture of it with puriform matter, a free incision is to be
made, and poultices applied. When the parts have become quiet, and
suppuration has been established, poulticing is to be discontinued, and
mild and light dressing employed.
When, on tapping a hydrocele, the fluid is found to be bloody,
in505jection is not to be resorted to, though the other circumstances
of the case should appear favourable. Rest is enjoined; and a radical
cure is not to be attempted till the fluid has collected a second, or
perhaps a third time, and become colourless.
Acute inflammation of the testicle, from sympathy with the urethra, and
sudden suppression of discharge from the anterior part of the canal,
has been already treated of. The inflammation may also be the result
of external violence. When the urethra is diseased, the testicle is
irritable, and its circulation easily excited. After subsidence of the
inflammatory attack, swelling, particularly of the epididymis, or of
the posterior part of the gland, seldom altogether disappears. The new
matter is not entirely absorbed; and thickening and induration remain,
to an extent depending on the violence of the action and the propriety
of the treatment.
Enlargements of the body of the gland are generally attributed to
injury. But often they occur without such cause being assignable;
and may be the result of chronic excited action, kindled in deposit
produced by a previous acute inflammatory attack. Such indolent
swellings attain considerable size. The tumour is of an irregular
surface, and feels hard and unyielding; there is always more or less
effusion of fluid into the cavity of the tunica vaginalis, adding to
the bulk of the swelling. Indeed, the size and consistence of the
tumour can be correctly ascertained only after evacuation of this fluid.
Many of these tumours, as already observed, are of firm consistence;
others are soft and doughy. They occur at the middle period of life, or
before it. Some are resolved easily, and by ordinary attention. Others
enlarge, notwithstanding the most judicious treatment; they gradually
soften, and at length fluctuation becomes apparent. Curdy matter is
evacuated by incision, perhaps mixed with a small quantity of thin
unhealthy matter; and from the wound projects a pale fungous growth
furnishing profuse discharge. The gland has now lost all appearance of
its original structure; a section of it presents a homogeneous surface,
of a greyish colour, and soft consistence, at some places broken down
and mixed with tubercular matter and pus. The fungus is of the same
nature as the rest of the tumour, but softer, and often with puriform
depôts in its base. In this disease there is nothing malignant; it
occurs in people of impaired or originally weak constitution, and is
generally known as the scrofulous testicle.
In the more simple swellings, the gland at some points retains its
original texture, but the greater part has no tubulous appearance, and
seems to consist principally of lymphatic deposit, dense, pale, and
equable. Such often accompany and are attributable to a diseased state
of the urethra,—part of the canal being in an irritable and contracted
state; and all efforts to discuss them usually prove fruitless, unless
the urethra have been previously restored to a healthy condition. The
soundness of this canal is therefore to be inquired into in the first
instance, and if stricture, or irritability independent of contraction,
be discovered, the practice must be directed towards it. The506 urethra
being sound, counter-irritation is to be applied to the testicle;
and the part should be suspended, though not in function altogether;
walking exercise, and the friction which it occasions, must be avoided
as much as possible. A gum and mercurial plaster protects the part,
and induces a moderate irritation of the surface usually sufficient
to dissipate the swelling slowly; if ineffectual, either repeated
blistering, or the insertion of a seton under the integuments, may be
had recourse to—from either or both much benefit is often derived. In
obstinate cases the recumbent posture must be enjoined. In general,
slight enlargement and induration of the epididymis remains.
The scrofulous swelling often does not yield to the means for
discussion, but advances to suppuration. The abscess is to be opened,
and the unhealthy contents discharged; endeavours are then to be made
to effect closure by granulation, and after that counter-irritation
may dissipate the tumour, or at least diminish its size. If protrusion
occur, as generally happens, it may be cut away; and by then keeping
the granulations on a level with the integument, either by pressure or
escharotics, at the same time attending to improvement of the general
health, cicatrisation may be procured, though tedious: or escharotics
may be used from the first, instead of the knife. For example,
sprinkling the fungous surface occasionally with the acetate of lead,
I have found in several instances effectual; repeated sloughing of the
protruded matter takes place; it sinks to the level of the integument,
and ultimately below it, and then the employment of slightly
stimulating dressing induces contraction and closure.
Not unfrequently the testicle is attacked by swellings of a more
serious nature—medullary sarcoma is common, as also both fibrous
and soft tumours, with cysts; scirrhus is more rare. These morbid
alterations may take place at once—that is, the swelling may be from
the first malignant—or they may supervene on tumours originally simple
and benign. The tumour increases with the usual rapidity; to describe
minutely the successive stages, would be but repetition of what has
been already stated more than once, in treating of similar diseases
in other organs. The medullary tumour often attains a very large size
before the integuments give way; it may in some cases be mistaken for
hydrocele, unless the history be attended to, and careful manipulation
made: elasticity must not be confounded with fluctuation. After
ulceration has taken place, the formation of a bleeding fungus is not
uncommon: indeed, the testicle is one of the most frequent seats of
fungus hæmatodes. The inguinal glands are in general affected early,
and swell to a large size, ulcerating extensively, bleeding, and
throwing out fungi; not unfrequently the chord feels free and soft,
presenting to all appearance a healthy structure between the inguinal
and scrotal swellings. In the advanced stages of scirrhous testicle,
the chord and its integument are thickened and hard. The progress of
this tumour is slower than that of the medullary, but equally certain.
The cystic sarcomata, when fibrous, may remain long apparently in an
indolent state, and without affection of the lymphatics; but when soft,
the cystic contents are often bloody, the medullary matter soon breaks
down, and then the integuments yield, and the malignant advance is
rapid. It need scarcely be observed,507 that in such cases nothing but
the knife, used at an early period, when the tumour is yet latent and
the lymphatics uninvolved, can save the patient. Castration must be
performed; and even this is in too many cases insufficient to annul
the malignant disposition of which the parts have become the seat. As
already stated, it must be had recourse to before hard and knotted
swelling in the groin, with thickening and induration of the chord, has
commenced, otherwise it can be of no avail.
The patient is placed recumbent. An incision is commenced a little
above the inguinal aperture, and carried downwards; on reaching the
tumour it is inclined to one side, so that with a similar one on the
opposite side an elliptical portion of integument may be included.
This is always necessary when the tumour is adherent to its coverings,
or when a fungus has been protruded. One straight incision may be
sufficient for removal of the tumour; it is sometimes necessary to take
away more or less skin, so that a large, loose, and flabby bag may
not remain after the extirpation. This preliminary wound penetrates
only through the skin and cellular tissue, and should be made rapidly.
At its upper part the chord is then to be cut down upon, exposed,
and divided; but the division should not be made until the chord has
been isolated for some distance, so as to afford a firm hold to an
assistant, and not before the assistant has secured it firmly in his
fingers, otherwise it may retract within the inguinal canal, rendering
the bleeding from the spermatic artery troublesome. The dissection
is now to be continued downwards, rapidly, and yet cautiously; the
tumour is detached on all sides, and removed along with a sufficient
quantity of integument. In dissecting off its posterior surface, care
must be taken not to wound the septum of the scrotum. All adherent
skin must be taken away, and in the case of fungus, the incision of
the integument must be wide of the projecting part. But, at the same
time, unnecessarily extensive removal of skin is always to be avoided,
otherwise there will sometimes be a difficulty in covering the root
of the penis and the remaining testicle. The assistant has, during
the extirpation, retained his firm grasp of the chord, so restraining
hemorrhage from that quarter; now the branches, generally two, of the
spermatic artery are pulled out by the forceps, and a ligature applied
to their extremities, inclosure of any of the surrounding parts being
studiously avoided. To tie veins, artery, nerves, vas deferens, and
cellular tissue, in one mass, would lead to most serious mischief, not
to mention the immediate and excruciating pain occasioned. It has been
recommended either to pass a temporary ligature round the chord, before
its division, to prevent retraction, or to tie the artery before it is
cut across. I have never found either practice necessary; the latter
retards the operation; the fingers of an assistant are generally as
effectual as a ligature, and inflict less injury to the parts, and
less pain to the patient. Should the chord slip, there can be but
little difficulty in pulling it down again by means of a hook; at the
worst, slight extension of the incision upwards may be necessary. The
scrotum is to be sponged clean of coagula, and its bleeding vessels508
secured: they are often numerous. The incision is brought together by
several points of suture, and cold cloths applied. In no operation is
secondary bleeding more frequent, occurring within an hour or two after
reaction has been established, and the patient begun to get warm in
bed. The flow is always from the scrotal vessels in the lower part of
the wound, and often profuse. The dressing must be partially undone, so
as to expose the vessels, and permit of the application of ligature.
On this account, it is well not to approximate the lower part of the
wound in the first instance, but to fill the cavity with charpie or
dry lint, retaining this until risk of hemorrhage has passed over, or
better still to have the wound quite open for five or six hours, and
then to bring the edges together. The upper part of the incision often
heals by the first intention, but this is seldom effected in the lower;
suppuration takes place, and the cavity fills up slowly by granulation.
Indeed, attempts to procure primary union of the scrotal wound are
scarcely to be recommended; they are very seldom effectual; and should
bleeding take place, the patient is either put to much pain, by removal
of the stitches, and separation of the edges, or the blood is confined,
accumulates in the cavity, and is infiltrated into the cellular tissue,
producing much tumour, which terminates in extensive and unhealthy
suppuration. Such retardation of the cure is avoided by open dressing
of the lower part of the wound from the first.
Not unfrequently infiltration of the cellular tissue over the chord
takes place within a few days after the operation, extending upwards
under the superficial fascia of the abdomen, with discoloration of
the integument, diffused doughy swelling, and much irritation of the
system. Matter soon collects at one or more points. Early incision
will check the advancement of this affection, followed by fomentation,
and poultice, and attention to the constitution. Collection of the
matter should never be waited for; and when depôts have formed, a free
and dependent opening should be made early. Sometimes the patient may
perish, exhausted by the profuse discharge and the disturbance of the
system, in cases that have been neglected, or in which infiltration is
rapid and extensive and the powers of life weak.
Calculus Vesicæ. Morbid action of the kidneys, producing altered
secretion of the urine and deposition from it, takes place in
consequence of derangement of the digestive organs—often occasioned by
the free use of acids, or of acescent diet, such as fruit tarts, or
drink containing a great quantity of saccharine matter. Many causes,
which have not as yet been well ascertained or understood, seem to
influence and predispose to calculous disorders. The prevalence of
these affections in particular districts has been attributed to the
quality of the water, or to the use of peculiar food or beverages;
but such opinions, in all probability, have been adopted neither on
very good grounds, nor after due inquiry and consideration. The county
of Norfolk, and the eastern part of Scotland from the Frith of Forth
northwards, are districts very similarly situated, exposed to cold and509
piercing winds, and appear to furnish a greater number of cases of
stone than the rest of Great Britain, with Ireland to boot. The reason
of this, as already stated, has not been satisfactorily explained.
 But this disorder, like gout, seems also to adhere to families, to be
transmitted from one generation to another. Some children seem almost
to come into the world labouring under calculus.59 The symptoms are
noticed very soon after birth, and often patients labouring under stone
are presented to the surgeon at the tender age of twelve or eighteen
months.
But this disorder, like gout, seems also to adhere to families, to be
transmitted from one generation to another. Some children seem almost
to come into the world labouring under calculus.59 The symptoms are
noticed very soon after birth, and often patients labouring under stone
are presented to the surgeon at the tender age of twelve or eighteen
months.
The depositions from the urine are various. The deposit chiefly
affecting children is of a dark colour, dense, hard, and crystallised;
but one lighter coloured, and more friable, sometimes precedes the
formation of this dark concretion. As seen here, the nucleus is
surrounded by an oxalate of lime calculus, and then follows layer after
layer of urate of ammonia. The dark sand or stone is occasionally,
though much more rarely, met with in older individuals; 510but in them
 the red, dark brown, yellow, and white deposits are more common. And
in them, too, the diathesis or disposition to the formation of one or
other variety evidently alternates, as is well demonstrated by section
of urinary concretions. An alternating calculus is here represented.
the red, dark brown, yellow, and white deposits are more common. And
in them, too, the diathesis or disposition to the formation of one or
other variety evidently alternates, as is well demonstrated by section
of urinary concretions. An alternating calculus is here represented.
The red deposit, by much the most common, at least in adults, consists
principally of uric acid, soluble by solutions of the alkalies.
The brown and yellowish are also composed of uric acid, often in
combination with a base, and are likewise soluble in alkaline
solutions, or in alkaline carbonates. The white is most commonly the
ammoniaco-magnesian phosphate, soluble in acids; rarely, it consists
of phosphate of lime, not so white or friable as the preceding, but
likewise soluble in acids; or it may be a compound of phosphate of
magnesia, ammonia, and phosphate of lime, very white and soft, and
imparting a stain to the finger, soluble in acids, but principally

 characterised by its fusible property. Specimens are here given of the
phosphate of lime, and of the triple phosphate formed as is usual on a
nucleus of uric acid, with some base, or upon the mulberry concretion.
The dark, hard deposit, chiefly occurring in children, consists of
the oxalate of lime, either pure, or in combination with one or other
of the preceding, very dense and soluble in acids. When these, by
accumulation within the bladder, are formed into concretions, they are
always mixed with more or less of a peculiar animal matter deposited
from the urine. Passed by the urethra, and settling at the bottom of
the vessel as the urine cools, they are termed either morphous, or
amorphous, according as they are crystallised or not.
characterised by its fusible property. Specimens are here given of the
phosphate of lime, and of the triple phosphate formed as is usual on a
nucleus of uric acid, with some base, or upon the mulberry concretion.
The dark, hard deposit, chiefly occurring in children, consists of
the oxalate of lime, either pure, or in combination with one or other
of the preceding, very dense and soluble in acids. When these, by
accumulation within the bladder, are formed into concretions, they are
always mixed with more or less of a peculiar animal matter deposited
from the urine. Passed by the urethra, and settling at the bottom of
the vessel as the urine cools, they are termed either morphous, or
amorphous, according as they are crystallised or not.
To correct the calculous diathesis is an object of much importance;
solution of the concretion in the bladder is now allowed to be
impracticable. The principal attention is to be directed to the
digestive organs and skin; these must be brought into a sound state by
attention to diet, and the exhibition of laxatives, tonics, antacids,
&c., as the individual case may require, by exercise and baths. And
much benefit is also derived from the use of either alkalies or acids
in solution, according to the nature of the deposit. The uric acid
diathesis is the most frequent; in that, alkalies, as the carbonates of
soda or potash, are to be employed; the potash is preferable. Diuretics
and diluents are useful in carrying off the sand, and relieving the
painful symp511toms; Venice turpentine with squill is on this principle
often a valuable remedy, and in some cases colchicum proves of benefit.
The symptoms attendant on the collection and passing of sand, or
gravel, as it is commonly termed, are,—pain in the loins; heat in
making water; heat in the urethra occurring afterwards, continuing
for some time, and usually at the orifice; frequent desire to empty
the bladder; and an occasional mixture of blood with the urine. When
aggregations of the deposit, forming concretions of some size, pass
along the ureters, violent pain is felt in the course of these tubes.
Often the patient complains of colicky pains all over the abdomen,
and of sickness without vomiting. There is pain in the thighs and
testicles, with retraction of the testicle on the affected side.
The calculous deposit may, instead of passing off along with the urine,
be accumulated in the body, forming concretions. It is produced by
the kidneys, and in them the concretions may be formed and lodged; or
it may not accumulate until it has reached the bladder. Usually the
stones are produced in the former situation, and after having attained
some size descend by the ureters, causing much pain. It is not often
that they remain in the pelvis or infundibula till they have become
too large to descend; in such cases they increase in their original
situation, producing, in general, much more uneasiness and greater
danger than if they had reached the bladder. Or they may enter the
ureters, and lodge in these canals, distending and obstructing them.
The concretions may be caused by the lodgement of extraneous substances
in the urinary passages. Foreign bodies introduced, even in the most
healthy persons, are soon incrusted by calculous matter; and the
rapidity of the incrustation is in proportion to the tendency to the
calculous diathesis. At first the deposit is generally of a brownish
colour. Catheters retained in the bladder are soon blocked up by it.
Needles, bodkins, leaden bullets, seeds of vegetables, kernels of
fruit, bits of catheters or bougies, have been found forming nuclei to
urinary calculi—more frequently in females than in males, for obvious
reasons.
Some concretions are formed on the nucleus of condensed vitiated
secretion from the mucous coat of the bladder, and partly consist of
this deposit from the membrane. Such are generally of a dirty white
colour, soft, friable, small, and numerous; it is seldom that they
are collected into masses of any considerable size. They are usually
adherent to the mucous membrane, sometimes forming a broad and thin
sheet covering it extensively; other stones, though composed of
calculous deposit from the urine, are equally friable as the preceding,
and also both numerous and small. So brittle is their structure that
they frequently break up by rubbing upon one another, or by being
compressed one against the other by the action of the muscular coat of
the bladder. Their laminæ in fragments, and the nuclei entire, are,
in consequence, often evacuated along with the urine in considerable
numbers. Even large and apparently very solid concretions break up most
unaccountably in the bladder. This may be, perhaps, so far understood
when more than one stone is present. A sketch from a specimen in my
collection is here introduced. It512 was obtained from the body of a
medical man. He had, it seems, laboured under symptoms of stone for a
long period, and ten years previously to the attack which terminated
fatally, had himself ascertained by sounding the existence of calculus
in his bladder. One Sunday morning I met this gentleman in consultation
about a case of injury of the hip-joint. In three days afterwards I
was called to visit himself, nearly moribund, from inflammation of the
urinary apparatus, his urethra being blocked up by large fragments
of stone. It appeared that on parting with me he had been suddenly
summoned to an urgent case of midwifery. He ran quickly down a steep
street, and at the bottom of it was seized with an urgent desire to
make water, which he did in small quantity, mixed with much blood. He
passed some pieces of stone with very sharp angles. He went on from bad
to worse; he had retention, and the urethra was found much obstructed;
suppression followed, and death terminated his sufferings in a very
few days. Many portions of the calculus were voided; much stone, with
the nucleus, occupied the bladder and urinary passage; the kidneys
were dark-coloured, and one approached to a gangrenous appearance. The
practice in the first instance, and so soon as the nature of the case
was fully ascertained, should have been to cut into the bladder and
clear it of the nucleus and fragments.
It has been elsewhere noticed, that cysts are apt to form in bladders
which have been long subjected to irritation from any cause; it need
therefore excite no surprise that such formations should be found in
patients afflicted with calculous disorders. In one of these unnatural
cavities a stone may lodge, both at first small. The concretion
receives gradual increase, fills the cyst completely, and then dilates
it in proportion to its own enlargement. So long as it is covered
by the cyst, the patient suffers but little from it; but when, from
the addition of calculous matter, it projects through the opening
of the cyst, coming in contact with the coats of the bladder during
contraction of the viscus, the usual symptoms of stone are manifested.
Sometimes there are several encysted calculi in the same bladder, but
in such cases they are seldom of large size.
The stone in the bladder—whether formed in the kidney, and
having descended, or originally concreted in the bladder, either
spon513taneously or in consequence of the presence of foreign
matter—produces very marked and distressing symptoms. There is frequent
desire to empty the bladder, and the uneasiness is not relieved by
doing so. There is pain during and after the evacuation, referred to
the course of the urethra, particularly to the orifice. In children,
the patient is induced by the pain to grasp the penis, and pull
forwards the prepuce, often so habitually as after a time to cause
considerable elongation of the latter part. The flow of urine often
stops suddenly, and immediately afterwards the pain is unusually
severe; the stream reappears on change of position. The body is usually
inclined much forwards during the attempts to make water; sometimes
the patient rests on his knees and elbows, or on the top of his head,
having found that he obtains most ease in these postures. The urine
is mixed with ropy mucus, and in long-continued cases with a puriform
fluid. After exercise, or unusual exertion, the urine is bloody, a
bearing down pain is complained of during the making of water, and
often there is simultaneous and involuntary evacuation of the contents
of the rectum; the close sympathy between the bowel and the bladder
has been already adverted to. In young persons afflicted with stone,
prolapsus of the rectum is common, and sometimes it occurs also in
adults. Occasionally there is pain in the testicle, or in the back of
the thighs, and very frequently a burning heat in the hollow of one or
both feet; sometimes there is a fixed pain in the last situation.
Some of the symptoms are more prominent than others, nor is the
severity of these uniform. At times the patient is tolerably free from
uneasiness; but then a fit of increased suffering supervenes, often
attributable to intemperance, or to over-exertion. The intensity of
the symptoms also depends on the nature and size of the concretion,
and on the idiosyncratic irritability of the patient; in some people
the bladder is naturally so acutely irritable as to be thrown into the
utmost disorder by the most trifling cause, whilst in others sources
 of greater irritation produce but very little uneasiness. The mulberry
or oxalate of lime calculus, a specimen of which is here sketched, is
of very rough surface, and gives rise to the most violent symptoms.
But the projecting portions of this, or of other rugged concretions,
may become covered by additional and smoother deposit—or the surface
may become smooth, polished, and water-worn, receiving no addition for
a long time—and in such circumstances the sufferings are mitigated.
However, in consequence of fresh incrustation, they may soon become
again much aggravated, and almost intolerable.
of greater irritation produce but very little uneasiness. The mulberry
or oxalate of lime calculus, a specimen of which is here sketched, is
of very rough surface, and gives rise to the most violent symptoms.
But the projecting portions of this, or of other rugged concretions,
may become covered by additional and smoother deposit—or the surface
may become smooth, polished, and water-worn, receiving no addition for
a long time—and in such circumstances the sufferings are mitigated.
However, in consequence of fresh incrustation, they may soon become
again much aggravated, and almost intolerable.
The increase of the stone is in some cases exceedingly slow; after many
years, the size may not exceed that of half a walnut. In others, large
dimensions are attained within a short period. The mulberry is always
of gradual formation; and the rapidly increasing are generally of the
alkaline and earthy or alternating character.
The symptoms above detailed—many, and sometimes all of514 them—may be
produced by other causes than stone in the bladder. Irritation of the
bowels, more particularly of the lower, by worms, foreign bodies, or
feculent matter of a bad kind—irritation of the kidney—alteration of
structure of this viscus, and the lodgement of concretions in its
pelvis—are all attended by many of the symptoms of vesical calculus.
Irritability of the bladder, the nature of which has been elsewhere
detailed, also possesses somewhat similar indications; but the pain
is usually referred to the hypogastric region and the perineum, as
well as to the point of the penis, perhaps more frequently, and is
generally relieved after evacuation of the urine: such is not the case
in calculus.
The symptoms and sizes of stone, when severe, will lead the patient
to take such means as are necessary to ascertain the cause of them—to
ascertain whether or not stone exists in the bladder. The term
sounding is applied to such examination. In this proceeding the
bladder should contain some urine, so that the object may be effected
more readily, and with less pain to the patient; he should be desired
to retain his urine for one, two, or three hours, as he may be able;
or from four to six ounces of tepid water may be injected. In the
contracted state of the viscus, the stone may escape detection, if
of no great size, from being embraced by the bladder, and concealed
in its folds; or, on the contrary, it may be discovered either after
or during evacuation of the urine, having eluded the surgeon’s
search during an over-distended state of the viscus. Also, it may
be discovered in one position of the patient, whilst it is lost in
another. When the symptoms are decided, examination is to be made, both
during the recumbent posture, and during the erect, with the body bent
forwards, and likewise with the bladder in various states of fulness;
and if unsuccessful, the search is to be repeated. But in general no
difficulty is experienced in discovering the stone. The instrument
used should be pretty large, with a smooth metallic handle, and either
with a large curve and long point, or straight till near the farther
end, and then having a short curve. The latter form is preferable,
as admitting of the curved part being introduced completely within
the bladder, and turned in all directions and into every part of the
viscus—the urethra being brought into a straight line by the remaining
part of the instrument. The posterior fundus, behind the prostate, is
the situation most commonly occupied by the stone during the recumbent
posture; and there it is in a measure concealed, when small and the
gland enlarged. The surgeon, aware of this, examines that part of the
organ very carefully, and, as already stated, explores every corner
with the utmost gentleness, and at the same time minutely, never
employing the slightest force or rudeness of search. Upon bringing
the instrument in contact with the foreign body, or moving it quickly
upon it by turning the handle, the sharp clear sound of the stroke can
be distinctly heard; and this is one reason why the instrument should
be throughout metallic. The prudent surgeon is not satisfied of the
existence of calculus in the bladder without this sign.
Not a few practitioners have been deceived, and have subjected their
patients to incision of the bladder when no stone was there. A515 false
and deceptive grating is sometimes felt during the passage of the
instrument through the prostate; or the point may be made to rub
against dense and rough fasciculi of the bladder; or a more distinct
feeling, as of stone, may be communicated from the instrument being
brought in contact with particles of sabulous matter entangled in
mucus, and adherent to the inner coat. The last deception is to be
expected only in those advanced in life. But the greater number of
those cut necessarily have been young persons. In them the symptoms of
stone are closely simulated by irritations of the alimentary canal, and
the crying of the patient prevents the stroke on the stone from being
distinctly heard.
Perhaps the practitioner may be very anxious to discover a stone and
have the glory of removing it, and is satisfied with feeling a rubbing
or grating of the instrument; he cuts into the bladder, and to his
dismay and discomfiture nothing is found. No foreign body may have
existed; or perhaps some small particles of sand which gave rise to the
feeling may have escaped detection, being carried off along with the
urine and blood. On the contrary, cases have occurred in which a stone
actually existed, but was overlooked; and the patient, after recovering
from the first incisions, has been relieved by a second and better
conducted operation. In diseases of the urinary organs, the surgeon
cannot be too cautious and considerate in all his proceedings and
interferences. For example: I on one occasion went to see an operation
for stone in the bladder, and was asked to feel the stone, but could
not. There was merely a sense of grating during the introduction of
the instrument; and the operator was dissuaded from his intention. The
patient did not live many weeks; a small ulcerated cavity was found in
the situation of the verumontanum, but no stone.
By a dexterous use of the sound the size of the foreign body can be
tolerably well judged of, as well as the state of its surface, and it
may also be known whether there are more stones than one. The bent
part of the instrument is passed over and beyond the calculus, and
then under it, if possible, so as to ascertain its thickness; and by
moving it on each side, the other dimensions are also arrived at. No
information can be obtained as to the size of the stone—at least in
adults, and when it is not encysted—from any examination by the rectum.
Concretions resembling horse-beans in size, and even larger, can
be brought through the adult urethra without incision, by means
of properly constructed forceps. The facility with which this is
accomplished will depend much on the state of the passage, whether
naturally capacious and free from morbid contraction or not, and also
upon the condition of the prostate gland. Notwithstanding the greater
irritability of the parts in young persons, this operation may be
readily performed on them; on several occasions I have removed from
children concretions of considerable size through the natural passage.
Various contrivances have been used for the purpose. Modifications of
what are called Hunter’s forceps have been recommended,—two elastic
blades shut by being withdrawn into a canula, and made either straight
or curved; but they are not so applicable as the forceps of Sir A.
Cooper, as modified by Weiss. These are of516 different curves and sizes,
and the handles should be made of metal, smooth on the flat surfaces;
for thus the concretion will be more readily felt. The instrument is
passed along the urethra, and used in the bladder as a sound; when
it has touched the stone the blades are opened, and by raising the
handle, pressing the convex part downwards, and then allowing the
blades to close slowly, the concretion is embraced. If the stone lie
on the forepart of the instrument, on its concavity, it will fall
between the blades as soon as they are sufficiently separated. By
observing whether or not the wire goes home into the canula, it is
ascertained whether or not the foreign body is between the blades; if
it is not, the manœuvring must be repeated; if it is, the instrument
is to be withdrawn carefully—of course bringing the concretion along
with it. Some slight resistance is felt in passing the prostate, as
also anterior to the sinus; and on reaching the orifice, some little
force is requisite to complete the removal, or the orifice may be
dilated by a slight incision so as to facilitate the disentanglement
of the forceps with the concretion. By one or more operations of this,
nature many stones may be removed, and the patient thus freed entirely
from the disease. There is no great risk of seizing and pinching the
coats of the bladder with this instrument, whilst there is a tolerable
certainty of doing so with most of the others.
On one occasion, when practising the operation on the dead body, I
found that the instrument had got several stones in its grasp, and
was kept so dilated as to be withdrawn with much difficulty—there
being no means of disentangling the stones but by farther expansion of
the blades, which was impossible. A great many foreign bodies—pieces
of pebble—had been introduced; but had the same number of urinary
concretions been laid hold of—which is scarcely possible—those farthest
from the point and most compressed would have crumbled down, and thus
the expansion of the blades would have been diminished. I have not
experienced the least difficulty in operating with this instrument, in
numerous cases, and at all periods of life. The preferable instrument
for the purpose is, however, the small screw scoop. The concretion can
by its use be crushed and reduced in volume, so that the urethra does
not suffer in the extraction, and the patient is saved much pain. The
safety of the proceeding is its greatest recommendation. It is very
seldom that any unpleasant symptoms follow; there may, perhaps, be a
trifling effusion of blood, and some slight pain in making water may
continue for a day or two. Should either irritability of the bladder,
or symptoms indicating inflammation of the mucous coat supervene, these
must forthwith be combated.
Concretions of such a size as cannot be made to pass through the neck
of the bladder, and along the urethra, and yet are not much larger than
a filbert, may, if soft and friable, be laid hold of in the bladder by
properly contrived instruments, and acted upon so as to be reduced to
powder and fragments, which may either pass off along with the urine,
or be extracted by means of forceps. This proceeding is not advisable
in children, owing to the small size of the parts and their greater
irritability, and in consideration also of the concretions in them
being in general exceedingly dense; as formerly noticed,517 they are most
frequently composed of the oxalate of lime. In the adult, it cannot be
adopted with safety and propriety, when the bladder is irritable and
will not bear a certain degree of distention, and when the prostate
gland is large. The cases in which the concretion is small, soft, or
brittle, and the parts sound and free from irritation, form but a small
proportion of those labouring under stone who present themselves to
an operating surgeon. However, the bruising, grinding, and rubbing
down of stones has been tried in all kinds of cases, but with neither
a satisfactory nor an encouraging result; a case will now and then be
met with favourable to these proceedings, but they can never become
generally applicable, and attempts to make them so will, as experience
has shown, be followed by disappointment and disaster.
A stone of a larger size than I have indicated, and of dense
structure, may be laid hold of in the bladder, and may by repeated
and tedious operations be broken into fragments; but each sitting,
as it is called, of the patient, and each attack upon the stone, is
attended with more pain, greater risk, and far more exhaustion, than
its removal by incision would inflict. The repeated introduction of
the instruments, their expansion, and the turning of them about in
the bladder, and, if their object is accomplished, the action of the
angular and rough surfaces of the fragments on the mucous coat, are
certainly followed by an attack of inflammation of the viscus, always
tedious and annoying—often excruciating, dangerous, perhaps fatal.
Attacks of inflammation of the testicle are also not uncommon, probably
from irritation of the prostate, and from the pinching and bruising
of the verumontanum, which it is almost impossible to avoid, whatever
care and precaution be adopted, when the three-branched instrument is
used. In turning to the records of Lithotrity—and under this term we
shall include all attempts to break down stones within the bladder,
whether by drilling, or filing, or hammering—it will be found that many
patients have died from the mere exploration; and altogether, nearly a
half of those who have fallen into the hands of the experimenters and
adventurers have perished in consequence. Every successful case is well
advertised; the dead men rest in peace.
But still the operation of breaking up a stone in the bladder is very
advisable in certain cases, and may be resorted to with every prospect
of a safe, speedy, and successful conclusion. But it can be recommended
and employed only within certain limits; the case must be well chosen,
and every circumstance must be perfectly favourable as regards the
condition of the urinary passage and of the bladder, and the size and
nature of the stone. Every operating surgeon should make himself well
acquainted with the instruments and their mode of application, so that
he may resort to them as occasion requires.
A great deal of ingenuity has been expended of late years in inventing
and improving upon the apparatus. Many useless, inapplicable, and
highly dangerous machines have been produced, a few efficient and
perfectly safe.
The knowledge of the fact that the curvature of the urethra can be518
effaced, and a perfectly straight instrument, or one with a short
curve can be passed into the bladder with equal ease and freedom from
uneasiness as a largely curved one, has facilitated very much the
application of means for seizing and acting upon a stone in the bladder.
The three-branched instrument, which it is unnecessary to describe, as
it can be readily seen and obtained, can be without difficulty brought
in contact with the stone, the bladder being partially distended by
urine, or filled to the requisite extent by tepid water injected
through the outer canula of the apparatus. The branches are then so far
expanded, and the drill withdrawn; and by a little cautious management,
turning the instrument, altering the degree of expansion, and sounding
with the drill, the stone is seized, and then fixed by pulling back the
inner canula. By turning the drill with the fingers, and pulling back
forcibly the inner canula so as to close the branches, the concretion
may at once be pulverised; or it may be again seized, and attacked
by the drill on a different side. The operation may, if necessary,
be repeated after the lapse of eight or ten days, or sooner, if the
irritation caused by the former have subsided. Diluents are to be given
so as to facilitate the washing out of the detritus, and strict rest
and abstinence from stimuli must be observed for a few days.
Various forms of drill have been contrived for acting on a large
surface of the stone; others for scooping it out, the shell to be
afterwards broken into fragments and triturated; they are all unsafe
and ineffectual. The instrument is also so constructed that a drill-bow
may be used, and the apparatus may be fixed by what mechanics call a
bench, or it may be attached, by complicated machinery, to the table on
which the patient is laid, and be there secured in a proper position.
But all this implies an intention of attacking large and dense stones,
and a repetition of the attempts. So far as my experience goes—(and
besides having seen Civiale and others operate, I have myself employed
the instruments in many cases, and very successfully,)—I should
dissuade from all endeavours to rid the patient of stone by such means,
unless its size and consistence were such that it would yield to one or
two attacks.
A plan of crushing the stone, by forcing one part of an apparatus
against another by the stroke of a hammer, has been lately promulgated,
and by a person who previously maintained that the grinding and rasping
was quite perfect, though now regarding them as nought. This percuteur
has a short bend at its farther extremity, one-half separates from
and slides on the other, and both are provided with teeth. It is very
possible to entangle a portion of the bladder betwixt its blades; and,
besides, these may bend or break, as they have done in several very bad
and abominable cases, in which incisions were required to disengage the
instrument from the patient’s urethra or bladder A stone may also be
laid hold of by the apparatus, and being so hard as not to yield to the
impulse of the hammer, may become fixed in such a way as it cannot be
freed from the grasp, there being no provision for pushing it out as in
the lithotriteur.
It will be seen from what has been stated, that I am not so
san519guine—and I trust I shall be excused of presumption in giving an
opinion upon the subject—as to suppose that the breaking up of the
stone in the bladder will ever entirely supersede lithotomy. That it
would do so was at one time industriously represented, and perhaps
believed, by some of the advocates and promoters of lithotrity. If,
by some miraculous interposition of Providence, the deposits from the
urine should uniformly be pulverisable, and that bladders be made of
less irritable stuff than they are, and if, above all, the affected
individuals could only be prevailed upon to apply in due time, then
might such pleasant anticipations be entertained, and then might we
with some reason hope to see them realised; but as matters now are,
urinary concretions must, in a great many instances, be cut out of the
bladder. Nor is it a circumstance to be very much deplored, since,
in good hands, the patient neither endures so much suffering, nor
incurs so much risk, as by the proceedings already detailed. The cure,
besides, is far less tedious. The stone-grinders, whilst they conceal
their own unfortunate results, endeavour to depreciate lithotomy by
blazoning abroad the practice of some unlucky surgeon, who, perhaps,
loses four in twelve, or six in twelve, of the patients who come under
his knife.
It has been said that lithotrity is applicable, when, from the advanced
age of the patients and the rigidity of the parts to be cut, lithotomy
is not. This statement is incorrect, at least the latter part of it.
Old people, from 70 to 80, and even beyond that age, recover, when the
operation is conducted quickly, without loss of blood, and so as to
guard against infiltration, as certainly and rapidly as young persons.
Within the last few years the apparatus for breaking up stones has been
very much simplified and improved upon. The screw lithotrite can with
great propriety and safety be employed in cases in which the concretion
has not attained any very large size, and in which also the urinary
apparatus is healthy, and tolerably free from irritability. The cases
for this operation must be well chosen, and the proceedings conducted
throughout with great caution, gentleness, and judgment. Very full
directions are given in the “Practical Surgery” for the performance
of this operation.
Perhaps no operative procedure has been more canvassed than that of
lithotomy. The subject has been discussed, and the operation attempted,
by many not very eminently qualified. All sorts of contrivances have
been made and promulgated in connexion with this operation; the greater
number intended to supply the want either of anatomical knowledge or of
operative dexterity. A volume would scarcely contain a catalogue even
of the instruments which are in my possession,—crooked staffs, knives,
spoons, and forceps. I shall content myself with describing what
appears to me the most simple, safe, and certain procedure.
The bladder may be opened, for the removal of stone, in various
situations; at its forepart, by incisions above the pubes; in the
posterior fundus, by division of the sphincter ani and a portion of
the bowel; at its neck, by cutting upon it through the perineum. The
first mode is termed the high operation, the second the recto-vesical,520
the last the lateral. The lateral shall be first considered: it is the
safest, the most advisable, and the most frequently resorted to.
Keeping the patient in suspense for days after operation has been
agreed on, with the view of preparing him as it is called, is
prejudicial. Unless his digestive apparatus be in disorder, or
he be labouring under some other affection incompatible with his
safety should an operation be performed, the sooner he is cut the
better. Delay often inflicts much mental suffering, is apt to induce
despondency, and to weaken the defensive and reparative powers of the
system. On the night before the operation, a dose of castor-oil, or
other mild purgative, is to be administered, so as to obtain an empty
state of the lower bowels; should this fail, an enema must be given.
The existence of a stone should be ascertained immediately before
proceeding to the operation; it is not enough that the sounding was
satisfactory the day before, or at any former period; and the operator
will also, for his own sake, satisfy those who are met as his advisers
and assistants of the fact that there is a stone in the bladder. All
apparatus that may be required should be at hand. A grooved staff,
a knife, forceps, a scoop, and an elastic-gum tube, are in general
sufficient. A Read’s syringe should also be provided, lest the stone
should prove brittle, and crumble under the forceps. When the operator
has, by previous examination, ascertained that the stone is of an
unusually large size, then he must be provided with a narrow, straight,
and probe-pointed knife, with forceps of considerable length and grasp,
and also with forceps so constructed as to effect crushing of the
stone, should this prove necessary.
The staff should be curved, of a size sufficient to fill the urethra,
or nearly so, and with the groove placed betwixt the convex surface and
the side presented to the left of the patient. This form of instrument
will prove the most convenient guide into the bladder. It is introduced
fairly into the viscus, and made to touch the stone audibly. Its
concave surface is raised towards the arch of the pubes, and retained
thus, firmly hooked under the bones—as if with the intent of lifting
the patient from the table—perpendicularly straight, without any
inclination of the handle, or any bulging of the convexity towards the
perineum. After being properly placed, the instrument is intrusted to
an experienced assistant, who keeps it exactly in the same position
from the beginning to the conclusion of the incisions. He at the same
time elevates the scrotum, and standing behind the patient, leaves the
surgeon with both his hands at liberty, and with the patient’s perineum
all clear. The operator is thus enabled to guide the knife by the left
hand; whereas, if he use a straight staff, his left hand must be solely
devoted to the management of this instrument during the most delicate
part of the incisions.
The staff is introduced either before or after the patient has been
secured. The fixing of the patient is in this operation very necessary
and important; on the proper management of that depends much the
facility of completing the operation quickly and satisfactorily.
Children are easily and conveniently held on the lap of an assistant,521
who, grasping the knees, places and secures the limbs so as to expose
the perineum. In adults ligatures are indispensable; the hands and
ankles are to be fixed together by means of strong and broad worsted
tapes; and, in addition, the pelvis requires to be secured, and the
limbs must be retained well separated, by two steady and powerful
assistants, pressing obliquely down towards each other. A band may also
with advantage be passed under the hams, and tied round the patient’s
neck: the proper position is thus still further secured. The patient is
placed on a firm table, of a height convenient to the operator, who is
seated on a low stool. A table from two feet and a half to three feet
in height, with a stool about a foot lower, will be found to suit very
well. The instruments likely to be required are disposed in the folds
of a towel placed on the floor, on the right side of the operator, and
at a convenient distance.
Before proceeding to incise, the finger is introduced into the rectum
to ascertain that it is in an empty state, and also to promote its
contraction. A knife is used, with blade and handle somewhat longer
than those of a common dissecting knife, and without any edge till
within an inch and a half from the point,—held lightly in the fingers,
the end of the handle resting on the palm. It is introduced close to
the raphe, on the left side, and nearly opposite to where the erector
penis and accelerator urinæ approach each other. Its point is made
to penetrate through the skin, fat, and superficial fascia of the
perineum, and is carried downwards with a slight sawing motion, by
the side of the anus—about midway betwixt the anus and the point of
the tuberosity of the ischium—and is continued till nearly past the
lower part of the orifice of the bowel. The forefinger of the left
hand is then introduced into the wound, and the resisting fibres of
the transverse muscle of the perineum, and of the levator ani, are
touched with the edge of the knife directed downwards. Wound of the
rectum is avoided by pressing it downwards and to the opposite side by
the finger; indeed the finger should be constantly in the wound as a
guide to the knife. In this stage of the proceedings, incision upwards
would be likely to interfere with the artery of the bulb, whatever
its distribution may be,—whether the vessel come from the pudic,
or from the posterior iliac. It occupies nearly the same relative
situation in either case, and by care can always be avoided during
the second incision. Division of it occasions most profuse, alarming,
and dangerous hemorrhage. I have seen the patient lose much blood in
consequence during the incisions; and after the occurrence of reaction,
have seen the blood soaking through the mattrass, dropping from the
foot of the bed, and collecting in pools on the floor. The bleeding is
difficult to arrest; the application of ligature is very troublesome,
if not impracticable, and efficient pressure cannot be made with safety.
In my own practice I have had little or no trouble from
hemorrhage—chiefly, I believe, from never cutting upwards after the
first incision. One instance of secondary bleeding occurred. The
patient was sixty-one years of age, and had laboured under symptoms of
stone for eight years. He had been dyspeptic for some weeks before the
operation, but otherwise appeared a favourable subject. Very522 little
blood was lost during the operation, but on the fifth day hemorrhage
occurred to the extent of seven ounces; on the eighth day, the same
amount was lost; on the twelfth, a pound; on the sixteenth, five
ounces; on the seventeenth, about a pound. The bleeding was uniformly
preceded by a feverish attack; and the blood had a florid, arterial
appearance, and flowed rapidly. It proceeded from the interior of the
wound, and a suppurating cavity in the neighbourhood of the prostate
was felt by the finger. From the prostatic side of this abscess the
blood appeared to spring; probably a considerable branch of the pudie
ramifying in this situation had been opened by unhealthy ulceration.
Pressure proved always effectual at the time, the hemorrhage recurring
on the loosening and separation of the lint. After the last bleeding
the dressing was retained for some days, and on its removal no
recurrence took place. The patient had been much exhausted by this
severe loss of blood, but, notwithstanding, made a good, and by no
means tedious, recovery. In one case, also, troublesome hemorrhage
occurred within twelve hours from the operation on a patient advanced
in life. The bleeding was arrested with some difficulty by ligature and
pressure. The patient died on the third day. The cause of the bleeding
was found to be ossification, as it is called, or earthy degeneration
of the coats of the vessels. The bleeding was from the external
hemorrhoidals. The artery of the bulb was untouched.
Many patients have perished within the first day or two from bleeding,
owing to the using of the knife too freely, and in an improper
direction. By very slight application of the edge to the resisting
fibres, and by gentle dilatation with the finger, the membranous
portion of the urethra is reached. The knife is passed over the back of
the forefinger in the wound, and lodged in the groove of the staff; it
is then carried forwards through the prostate, with the edge directed
downwards and outwards, cutting the gland obliquely. In this incision
the knife is raised very little from the groove, the object being to
divide the gland to the extent of no more than barely three-quarters
of an inch. By so doing, the reflection of the pelvic fascia remains
uninjured, and the boundary is left entire betwixt the external
cellular tissue, and that loose and very fine texture immediately
exterior to the bladder—betwixt it and the fascia lining the pelvis;
thus the risk of urinary infiltration is done away with, at least much
diminished. There is great danger in dividing the base of the prostate
completely, and much more in cutting any part of the coats of the
bladder. When the knife enters the groove of the staff, this latter
instrument must be held very steady; if it be at all withdrawn, its
point may escape through the wound, and mislead the knife.
There is no great risk of wounding the trunk of the pudic artery,
unless by using either a broad instrument called the gorget, or a
concealed knife. The former is now almost wholly abandoned. Besides
endangering the pudic, it is apt to lacerate the neck of the bladder,
pushing the prostate before it, and so tearing its cellular connexions.
The latter, the lithotome caché, makes the internal wound larger than
the external; the coats of the bladder are slit up to an unnecessary
extent, being cut much more easily than the prostate, and the
instrument not affording sufficient resistance to the gland.
523
Through the prostatic opening the finger is easily passed into the
bladder, and the stone felt. The staff is then withdrawn. Sometimes
it is a troublesome matter to reach the bladder with the finger, in
consequence of the straining and struggling of the patient, causing the
organ to ascend in the pelvis; the difficulty is overcome by patiently
waiting till these exertions cease. By steady and gradual movements of
the finger in the wound of the prostate, the opening is much dilated,
so as to admit of the ready introduction of instruments for laying hold
of and removing the stone. Indeed, the neck of the bladder is capable
of dilatation without any incision. In a case of perineal abscess
containing a portion of exfoliated bone, on account of which incision
was made, it was found that the cavity communicated with the urethra;
lest other foreign matter should remain, I introduced my finger into
this aperture in the membranous portion, and found that by the most
gentle movement I could not only easily reach the bladder, but dilate
the opening in it to a very considerable extent.
By the finger in the bladder, the size and position of the stone is
ascertained; and no extracting instrument should be employed till after
the finger is in contact with the stone. When it is of moderate size,
and after having been turned, if necessary, into the most favourable
position for extraction, the forceps are introduced. This instrument
should be tolerably long, so as to afford power in its use; and the
extremities of its blades should be covered with coarse linen, for
thus it is not so likely to slip or to chip the stone as those with
raised and projecting teeth. For flat stones, the forceps should
be flat-mouthed; for round, more open, hollowed, and bent at the
points; or for the latter description of stone, forceps with a sliding
joint may be used. The object is to lay hold of the concretion by
as many points as possible—to bring a large surface in contact with
the instrument. Those with the sliding joint are of no service when
the stone is flat, as it either cannot be caught by them at all, or
merely by their points, or near the joint; they are applicable only
to round stones of considerable size, but they are very troublesome
to manage. The instrument is introduced shut, along the finger, and
on reaching the prostate is gently insinuated, whilst the finger is
at the same time withdrawn. It is brought in contact with the stone,
and carefully opened, the handles being raised. One blade is passed
under the stone, the other remaining above, and then the instrument is
closed, firmly but not forcibly. By the finger, again introduced, along
the side of the forceps, it is ascertained whether or not the stone is
held securely, and in the proper direction; if not all right, it may
then be turned by using the point of the finger and slightly relaxing
the grasp. Now the handles of the instrument are depressed, so as to
avoid resistance from the bones in the front of the pelvis, and the
extraction is commenced, in a steady and gradual manner; if difficulty
is experienced, dilatation is effected, and the process facilitated, by
moving the forceps gently backwards and forwards; no force or violence
is required, either in pulling or dilating; all should proceed smoothly
and with deliberation.
The forceps must be proportioned in length to the size of the stone;524
a large concretion requires long forceps, both that it may be grasped
securely, and that sufficient power may be afforded for the extraction.
Some stones are of such a size as will not admit of passage through the
section of one side of the gland. By using the blunt-pointed knife,
directed by the finger, without any additional external incision, a
wound is made on the right side of the prostate, in the same direction
and to the same extent as that on the left. Thus a triangular flap is
formed, the apex towards the membranous portion of the urethra, and
through the opening thereby afforded any stone, which will pass through
the bones of the pelvis, can be extracted without much difficulty. But
no benefit can result from cutting both sides of the prostate, either
by the double lithotome or in the manner just detailed, in all cases.
It is time enough to incise the opposite side when, by introduction
of the finger through the usual wound, it has been ascertained that
the stone is too large to pass through it. Then it is safer to cut the
other side, than to enlarge the original opening, either by the knife,
or by laceration in cruel attempts to extract the stone through an
insufficient opening.
When the stones are small, the scoop is the preferable instrument.
By it the bladder may be soon cleared, even when the concretions are
numerous. It is introduced along with the finger, is brought in contact
with the foreign body, and passed beyond it or beneath it. Then the
point of the finger is placed on the lower part of the stone, so as to
steady and secure it, and the scoop and finger retaining this relation
are gradually withdrawn along with the stone. More than one, perhaps,
may be removed at each withdrawal of the instrument. The flat and
slightly bent lever, usually forming the handle of the scoop, is useful
should the forceps unfortunately slip during extraction, leaving the
calculus impacted in the wound; by insinuating this instrument behind
the stone, and employing it partly as a lever, partly as an extractor,
removal is completed.
If the stone break, which should not often happen if the forceps be
used properly, the fragments must be carefully brought away, the larger
by the forceps, the others by the scoop. The sand and detritus which
may remain are washed away by injecting tepid water into the bladder,
afterwards promoting copious secretion of urine by diluents.
After almost every operation for stone, particularly when the
concretions are numerous, or when they have broken into fragments,
a searcher is useful to ascertain whether or not all have been
removed. It is a slightly curved sound, with a bulbous point. Having
been introduced by the wound, it is passed into every part of the
bladder with great care, with the view of detecting small calculi, or
fragments, which may have escaped the search of the finger, forceps,
and scoop. Besides this precaution, the extracted fragments should
be carefully examined, and the stones built up, that the surgeon may
better judge if they be all there. The surface of the stone affords
considerable information; if it be uniformly rough, the likelihood is
that it is solitary; if one or more points are smooth, it is probable
that these have been occasioned by the attrition of other calculi.
If suspicion525 still exist of part remaining, examination may be made
through the wound, during the suppurative stage, six or eight days
after the operation, before it has closed much.
It has been proposed to break the stone when very large, to facilitate
its extraction, and many instruments have been contrived for the
purpose. I have had no experience of the proceeding, but consider
the following description of instrument as the best adapted for the
purpose—strong, massy forceps, of considerable length; the blades
proportionally narrower, but much thicker, than those of the extracting
forceps, and armed with several strong teeth, thick at their origin,
tapering gradually, and terminating in a sharp ridge; the handles also
thicker than they are broad, that they may not yield to the compressing
force, and approximated by means of a combination of the lever with the
screw. The foreign body is secured firmly between the blades closed
on it; the handles are then fixed by a screw and nut, and compressing
force is exerted by the lever acting both as a lever and a wedge. The
screw, turned by the fingers, will suffice to crush many concretions;
and none can withstand the full power of the instrument. But it is,
perhaps, safer to open the bladder above the pubes, and extract the
stone through a wound in that situation, when it is too large to pass
betwixt the rami of the ischia.
When the stone or stones have been extracted, and the surgeon
has satisfied himself that no more foreign matter remains in the
bladder, the next step in the lateral operation is the insertion of a
gum-elastic tube, from four to six inches in length, according to the
depth of the perineum, in calibre a little larger than a full-sized
catheter, provided with a noose attached to each of two rings at its
neck, and at its farther extremity open at both point and sides. It is
introduced along the forefinger in the wound, and its extremity lodged
fairly within the bladder; a double tape is attached to each of the
nooses at its orifice; one is passed up in front, and secured to the
fore part of a broad band round the loins; the other is brought under
the thighs, and fixed behind. The object of its introduction is to
facilitate the escape of urine externally, and prevent infiltration of
the cellular tissue by this fluid. The wound, when made according to
the directions which have been given, is both conical and dependent—the
external opening is free, the internal small, the intermediate space
gradually contracting as it approaches the bladder, and the inferior
part of the wound of the integument is lower than the corresponding
portion of the prostatic section; thus the draining away of the urine
is favoured, but it conduces very much to the patient’s safety to
ensure still farther its free escape by the insertion of a tube—part
passes through the tube, and drops from its orifice, part flows by its
side according to the laws of capillary attraction. For some hours
after the operation, it is necessary to clear out the instrument
frequently by means of a feather, otherwise its extremity will soon
become obstructed by coagula; in short, this must be persevered in
till colourless flow from the orifice shows that the internal oozing
of blood has ceased, and that nothing is passing but urine. When by
salutary effusion from the vessels the surface of the wound526 becomes
consolidated and imperviable to the urine, the tube is to be withdrawn,
but not till then; in young persons it may be removed after twenty-four
hours, but in those advanced in life and of relaxed habit it must be
retained for forty-eight or more.
The tube is also of service should bleeding continue from branches of
the superficial pudic, from small arterial twigs in the neighbourhood
of the prostate, or from venous ramifications and the plexus which
surrounds the neck of the bladder; for it admits of the application of
efficient pressure to the bleeding point, without interfering with the
escape of urine, and so increasing the danger of infiltration. Slips
of lint are pushed along it to a sufficient depth, and are retained,
if necessary, by compress and bandage, the orifice of the tube being
left clear. But, as already stated, it is indeed very seldom that this
proceeding will be required, if the operation has been conducted with
proper caution.
After the tube has been secured by its tapes, or during this process,
the patient is unbound; he is placed in bed with the thighs separated
and bent, and must be kept very quiet. Diluents are administered
copiously, to encourage the secretion of urine; he cannot wet too
much. His nourishment must be very sparing, consisting chiefly of
bland fluids; and all sources of inquietude and irritation must be
carefully avoided. Depletion, whether general or local, will very
seldom be required; danger is not to be apprehended from inflammation
so much as from infiltration of the cellular tissue by urine. In the
fatal cases, unconnected with hemorrhage or exhaustion, the peritoneum
is not found vascular or coated with lymph, nor is there collection
of morbid secretion from this membrane within the abdominal cavity,
but the cellular tissue, along the track of the wound, is black,
disorganised, easily lacerable, putrid; or, if the infiltration has
not been to such an extent or in such a site as to kill speedily
as if by poisoning, unhealthy suppurations are found, extensive,
uncircumscribed, composed of sanies, urine, and dead cellular tissue,
horribly mixed. Should fixed and increasing pain be complained of in
the hypogastrium, the part is to be leeched and fomented; this is the
only indication of inflammatory action which has occurred in any of my
patients, and it has yielded to the simple treatment here mentioned;
so far as I recollect, in only three cases out of more than a hundred,
was the leeching necessary. Some patients require support very soon,
almost from the first; others evince sufficiency of action throughout,
and in them it is very necessary to pay strict attention to the
state of the stomach and bowels, lest the action should exceed; some
proceed favourably for a time, and then become torpid and stationary,
their spirits and constitutional power flagging, in consequence of
confinement and the discharge and irritation of the wound,—such also
require judicious support, and perhaps slight stimulation.
Union of the wound by the first intention is not desirable; attempts to
procure it are dangerous, as conducing to infiltration; the presence
of the tube effectually prevents both. Discharge and granulation take
place, and the cavity contracts gradually and uniformly. By the sixth
or eighth day—sooner in young people, and later in those527 far advanced
in life—the urine begins to flow in part by the natural passage,
causing considerable pain in consequence of the urethra having been for
a time unaccustomed to its stimulus; and as the opening in the prostate
contracts, the escape of urine by the wound proportionally diminishes.
When the natural course is completely restored, the wound closes more
rapidly than before, granulations soon fill it up, and cicatrisation
takes place. Sometimes, though very rarely, a small fistulous opening
remains for some time, through which a few drops of urine may
occasionally distil; should it prove obstinate in not closing, it may
be touched with a heated wire. And sometimes also, when the urine is
unusually slow of coming by the urethra, this may be expedited by the
occasional introduction of a catheter or bougie.
It is not often that the operation of lithotomy requires to be
repeated. In some few cases, however, the calculous diathesis
continues, a new concretion is formed, and the patient again applies
for relief, perhaps several years afterwards. In such circumstances,
the incisions are to be made in the right side of the perineum; for
the track of the former wound is now consolidated, firm, and hard,
and would be cut with difficulty. But when, from neglect or want of
dexterity, the first operation has been imperfectly performed, one
or more stones being left behind, the wound may not heal, nor even
contract to any considerable extent; and then dilatation of the
existing opening, with fresh section of the prostate, will probably be
sufficient, though at an interval of many months.
It has been proposed to divide the operation into two parts, with
an interval of several days between; first to make the incisions,
leaving the stone undisturbed, and after suppuration has been fairly
established, and the parts become relaxed, then to extract the
foreign body, provided it have not in the mean time been discharged
spontaneously—in short, to perform the operation à deux temps.
This method is liable to serious objections. Two operations must in
general be more severe than one. The patient is rendered despondent and
miserable after the first, by knowing that the object of his suffering
has been imperfectly accomplished, or rather not accomplished at all.
Much, and often serious irritation is produced by the wounded bladder
being contracted on the hard and rough foreign body; patients have sunk
under this torture, and the cure is always tedious. From the earliest
times it has been quite well understood, that when the stone cannot be
got out it must be left in; but the proposal of always leaving it in,
on principle and not from necessity, is really absurd. There is room
for suspecting that this mode of operation originated as a virtue from
necessity; the extraction of the stone is always the most difficult
part of lithotomy, requiring much skill and dexterity, and the
operator, finding himself baffled in his attempts to effect it, wisely
desists from his futile efforts at the time, and waits for another
opportunity. This is certainly better practice than the using of much
force, or dilating the wound by incision to a dangerous extent, but it
is very far from being so good as the immediate removal of the foreign
body, smoothly and quickly, skilfully, and without violence; and it has
been already observed, that the cases are very few indeed528 in which
the stone cannot be removed through the prostatic opening without the
employment of any force, and, without inflicting any injury to the
parts through which it passes—without hazard and without delay. The
sooner the method à deux temps is expunged from the list of surgical
operations, the better will it be for suffering humanity and the credit
of our art.
In those rare cases in which the stone is so large that it cannot be
brought through the outlet of the pelvis, it must either be broken
into fragments, or removed entire through incision above the pubes;
as already stated, it is probable that the high operation is the
safer proceeding. It is, however, an operation attended with much
danger. The wound is necessarily extensive, and important parts are
liable to be interfered with; and, from not being dependent, the
escape of the urine by it is almost certain to cause infiltration
of the cellular tissue surrounding the bladder—an occurrence almost
always proving fatal and that rapidly. The first part of the procedure
is to insure distention of the bladder, so that it may rise in the
pelvis, and afford sufficient space between its lower part and the
anterior reflection of the peritoneum; but this may prove either very
difficult or altogether impossible, even with the aid of injection by
the urethra, in consequence of the unyielding contracted state of the
viscus, and the great thickening of its coats. An incision is made
through the integument and fatty matter, from three to four inches in
length in the mesial line, and terminating over the symphysis pubis;
the recti and pyramidal muscles are then separated, the cellular tissue
cautiously divided, and the fore and lower part of the distended
bladder exposed. The coats are pierced at the most inferior part, and
an opening made sufficient for the introduction of the finger. By the
finger the dimensions of the stone are ascertained, and then the wound
is enlarged upwards to such an extent as will by dilatation admit of
the extraction. Forceps are introduced, of sufficient length and grasp,
and the foreign body removed without laceration or bruising of the
parts. The patient is then laid on his side, a piece of dressing being
interposed between the edges of the wound to favour the discharge of
the urine externally. The escape of this fluid maybe free and copious,
and the wound may close favourably; but the majority of the patients
on whom this operation has been performed, have perished either from
urinary infiltration, from peritoneal inflammation, or from exhaustion.
Fortunately, I have never had occasion to resort to it.
It has been proposed to combine this mode of operation with wound of
the posterior part of the urethra from the perineum, in order that a
free and depending outlet may be afforded to the urine, and also, that
by introducing instruments into the bladder from the lower opening,
the organ may be elevated and stretched so that its fore part may
afford sufficient space for the high incision without danger to the
peritoneum. With this view the perineum is incised, similarly but to a
less extent than in the lateral operation, and the membranous part of
the urethra opened. Through this aperture the sound with a stilet for
elevating the bladder is passed, and intrusted to an assistant; the
incision above the pubes is then made, the stone extracted,529 and a tube
is left in the perineal wound for discharge of the urine. The plan,
though complicated, appears feasible, and likely to diminish hazard by
preventing infiltration.
The recto-vesical method should never be resorted to in preference
to the lateral; in other words, it is unwarrantable, in my opinion, in
those cases to which lateral operation is applicable. It consists in
exposing the neck of the bladder by division upwards of the sphincter
ani and lower part of the rectum, and then either making a section
of the prostate in the usual way, or dividing also the coats of the
bladder in the posterior fundus, when the concretion is large. The
cure is tedious and harassing: the urine and feces are discharged
together, and hardened feculent matter may accumulate within the
bladder; the wound is long in contracting, and often cannot be made
to close completely without much trouble, and after a long time;
often a fistulous opening remains, communicating with the bladder and
rectum, and through this the urine continues to be in part discharged.
It has been argued, that the recto-vesical method is advisable, with
the view of obtaining more room for extraction of the stone; but
to me it appears that the divided rectum will occupy just as much
space in the outlet as when entire and empty. Circumstances may,
however, occur, rendering this operation, or a modification of it,
absolutely necessary, as in the following case—the only instance in
which I have encountered an encysted stone. The patient, aged 64,
of a spare habit of body, was seized with symptoms of stone in the
bladder about twenty-four years previously to my seeing him; at that
time he was sounded, but no stone could be discovered. The symptoms
gradually subsided, and ultimately disappeared, and he remained for
considerably more than twelve years totally free from any affection of
the urinary organs. But, about three years previous to the operation,
the symptoms returned, and again attentive examination of the bladder
was made, without detecting any stone; on introducing the finger into
the rectum, however, as high as possible, a firm substance was felt,
globular, of considerable size, and very slightly moveable. From this
time the symptoms gradually increased in severity, ultimately becoming
almost intolerable. At length the presence of a stone was distinctly
ascertained by sounding, and the instrument was passed beneath as well
as over the calculus; from simultaneous examination by the rectum, it
was evident that the hard bulging body was connected with the foreign
matter struck by the sound. The lateral operation was performed, and,
expecting to meet with a large stone, both sides of the prostate were
divided. The forceps were introduced, but the stone, though easily
laid hold of, could not be moved. Attempts with the instrument were
accordingly abandoned, and further examination made by the finger,
when it was found that the stone lay fixed in the lower and anterior
part of the viscus, that it was firmly enveloped by a cyst situated
between the rectum and posterior part of the prostate, and that only
a part, small in proportion to its body, projected into the cavity of
the bladder. Of this unusual and untoward circumstance, the medical
gentlemen present were also satisfied by manual examination. It
was quite apparent that it would be impossible to divide the cyst
sufficiently530 without wounding the rectum, and I therefore determined
to lay the bowel, the cyst, and the track of the wound into one cavity.
This was effected by cutting the upper and anterior part of the cyst,
passing a blunt-pointed and curved bistoury behind the remainder of
the cyst, insinuating it through the coats of the gut at that part,
meeting the point with the forefinger of the left hand passed per
anum, and then carrying the instrument forwards to the surface. A
strong scoop, much curved, was passed behind the stone, and without
much difficulty extraction was thereby completed. Not above a few
tablespoonfuls of blood were lost during the operation, in which not
much time was occupied, and no bleeding took place after reaction was
established. The cure proceeded favourably, though necessarily slow
and tedious, the more so since the patient had been very much reduced
by the previous suffering. Some superficial sloughing took place in
the wound, but the sloughs soon separated, and healthy discharge and
granulation followed. By keeping the bowels gently open, the annoyance
from feculent evacuation by the wound was in some measure diminished.
The patient was daily out of bed, and took food in good quantity and
with relish. At the end of the fifth week, however, he was seized with
a severe bowel attack—vomiting, purging, cold extremities, &c.—and the
effects of this were never surmounted. The real Asiatic cholera was at
that time prevalent, and the patient was under great apprehension of an
attack. The weak state in which it left him continued and increased:
he was soon confined entirely to bed, the wound made no progress in
closing, sloughing of the back took place, and he sank about the end of
the eighth week from the operation.
Calculi sometimes lodge in the urethra, obstructing the flow of urine,
becoming firmly impacted, and increasing in size. If in the perineal
portion of the canal, they are to be fixed and made prominent by being
grasped with the fingers, and then exposed by an incision made in the
raphe: they are turned out, either with the finger, or by means of
a small scoop. If situated in the part covered by the scrotum, the
opening should be made, if possible, behind, not anterior to it, for a
wound in the latter site will be closed with difficulty. When in the
posterior part of the canal, they are reached by incision on the left
side of the perineum and opening of the membranous portion. After such
operations, the wound, if not anterior to the scrotum, usually closes
in a few days.
Calculus of the female is exceedingly rare. Concretions are not
so apt to be retained in the bladder as in males; they are passed
by the urethra. The symptoms are similar to those which have been
described as indicating stone in the other sex. Sounding is easy; it is
performed with an instrument slightly bent at the farther extremity,
and considerably shorter than those employed in the male. Even when
the calculi are of considerable size, they can be removed, as well as
other foreign matter, by dilatation of the urethra, effected gradually.
Portions of gentian root, and sponge tents, were formerly used for
this purpose; but of late years various dilators have been contrived.
Some are really new, others have been published as such,531 though
correctly represented in works some hundred years old. Their blades are
made to separate in a parallel direction by peculiar adaption of the
screw; and, by gradually and very slowly increasing their separation,
uniform dilatation is effected. Very soon the opening is sufficient
to admit the finger; then the size of the stone is ascertained, and,
if necessary, the dilatation is continued to a sufficient extent.
When thus the canal has been widened so as to admit of the passage
of the stone, forceps are introduced, and extraction accomplished in
a direction downwards, that is, towards the vagina. Incontinence of
urine is apt to continue for some time after this operation, if the
dilatation have been considerable, as well as after the removal of
larger stones by incision.
Incision has been proposed in various directions—into the vagina, or by
the side of it, upwards and outwards; and it has also been recommended
to cut the bladder, on the fore and lateral part of its neck, without
interfering with the urethra.
By the latter method the chance of incontinence remaining is
diminished, but there is a risk of urinary infiltration, and this will
require to be provided against by the use of a tube, as after the
lateral operation in the male. A staff is introduced, and by it the
urethra is depressed towards the vagina. An incision is then made by
the side of the crus clitoridis, and through this the finger reaches
the neck of the bladder, more by dilatation than by additional use of
the knife.
In one case I removed a very large stone by incision. By a straight
grooved staff the urethra was depressed; a straight blunt-pointed
bistoury, being slid along the groove» was carried upwards and
outwards, first on the left side, and then on the right—dividing
the urethra and parts exterior, so as to form a track of wound,
which, after dilatation, would admit of the ready passage of the
stone. Extraction was easy. Incontinence continued for many months,
but ultimately was in a great measure removed by promoting farther
contraction of the opening by the cautery. The preferable plan, and
one I have since then followed in a few instances, is dilatation to
some extent, and by a proper instrument; then slight incision on each
side upwards and outwards; then further dilatation; in a few minutes,
without much pain, the finger is admitted, then the forceps. The
stone is then extracted quickly, with but little pain, and no bad
consequences follow.
Gonorrhœa in females is often confounded with Leucorrhœa, which
is a very common complaint both in married and unmarried women.
Leucorrhœa sometimes occurs at a very early period of life, at the
age of ten or sooner; and in such circumstances affections of the
glandular and osseous systems often supervene. Frequently it precedes
the accession of the coloured menstrual discharge, and in many
instances is substituted for it; it is always most profuse after the
menstrual period. In leucorrhœa there is generally neither heat nor
pain during the passing of urine, and the colour of the discharge
differs from that of gonorrhœa, though sometimes very slightly; the
stain of gonorrhœal matter is yellow with a black border; leucorrhœal
is white or yellowish, but does not possess the latter charac532teristic.
The application of leucorrhœal matter will induce discharge from the
urethra or from the external parts of some males, but the affection
thus caused is, perhaps, not so violent, nor of so long duration, as
that which arises from specific contagion. The effects of leucorrhœa
on the system are very troublesome. There is general debility,
disorder of the stomach, pains of the back, sides, and limbs, a sallow
bloodless complexion, paleness of the lips. It is often a cause, at
other times a consequence, of miscarriage. Sometimes it is accompanied
with a prolapsus uteri, sometimes with thickening of the os uteri. The
discharge which attends ulceration of the parts, from whatever cause,
is generally bloody, sometimes it is thick, and of a laudable aspect,
sometimes thin and fetid. More or less discharge attends polypus, and
is often profuse and coloured.
In gonorrhœa the inflammation is usually limited to the external
parts, but sometimes extends along the vagina. In neglected cases
great tumefaction of the labia takes place, along with excoriation of
the neighbouring parts, patchy ulceration around, and swelling of the
absorbents and of the inguinal glands. Heat, pain, and scalding, are
experienced in making water, but in comparison with the other sex,
females suffer little or nothing from this disease. The parts are much
less complicated; and bad effects seldom follow either the affection or
the remedies employed, however strong.
The inflammatory stage must be subdued by antiphlogistic measures,
proportioned to the intensity of the action and the state of the
constitution; they seldom, if ever, require to be at all severe.
Turpentines, and other internal remedies, which may prove beneficial in
the gonorrhœa of males, are of little use. The external means are to be
chiefly trusted to, consisting of astringent and stimulating washes;
when the vagina is affected, the solutions must be thrown up by means
of a syringe. In leucorrhœa, the same external treatment is required,
and the use of a syringe is always necessary. The washes most commonly
employed are—solution of the sulphate of zinc, of alum, and of the
nitrate of silver, or a decoction of oak bark or galls. In leucorrhœa
the internal exhibition of preparations of iron and of tinct. lyttæ in
pretty large doses may be considered as almost a specific, stimulating
the whole system, and correcting that state of morbid debility, both
general and local, on which the vitiated secretion depends; and the
injection for the vagina, which is perhaps most efficacious, is the
solution of the nitrate of silver. The solid caustic may often be
rubbed over the surface of the vagina affected by bad leucorrhœa or
gonorrhœa, when exposed and brought into view by the speculum, with
the best effects. When the menstruation is irregular, blisters and
sinapisms may be applied to the loins, with cold bathing, general and
local. In gonorrhœa, when only the external parts are inflamed and
furnish discharge, the application of a solution of the sulphate or of
the acetate of zinc to the parts, by means of lint, effects a cure in a
few days—along with strict attention to cleanliness, the observance of
rest, regulation of diet, and occasional doses of gentle physic.
Gonorrhœal Lichen not unfrequently follows suppression of the533
discharge both in males and females. It is preceded by smart fever,
headache, and violent pains in the limbs. Inflammation of the fauces
is generally present, with superficial ulceration or excoriation; and
sometimes the abraded portions of the mucous lining are covered with
a whitish exudation. The symptoms subside on the appearance of the
eruption, which is papular. It generally appears first on the breast
and arms, and then extends over the whole body, accompanied with slight
itching. If the case proceeds favourably, the red papulæ disappear
in a few days, leaving blains in their stead. Desquamation of the
cuticle generally follows. This affection must not be confounded with
a cutaneous eruption which sometimes follows the use of copaiba, and
which is a species of urticaria.
When the fever is violent, bleeding must be had recourse to, but not
to a great extent, and only when it cannot with safety be avoided.
Gentle laxatives are to be given. Diaphoretics are very beneficial,
and the patient should not be exposed to cold or wet, but kept rather
warm, otherwise the eruption may be repelled, the affection thereby
prolonged, and the constitutional disturbance augmented. The fauces
soon recover under the use of simple gargles. Mercury is hurtful.
Retention of Urine in females arises from tumours, natural or morbid,
of the uterus, or of the vagina and appendages, from displacement
of these parts, or from foreign bodies lodged in them. But the
consideration of such affections belongs to the accoucheur.
Retention takes place in females from paralysis of the bladder, and
the same treatment is necessary as in the case of the male. Hysterical
women often take it into their heads that they are unable to empty the
bladder, and will not attempt it; and though it may be difficult to
convince them of their mistake, yet when they are left to themselves
for a little, and begin to feel some of the torments which attend
retention, they contrive to get rid of their burden, and that without
any very great exertion. Sometimes they omit attempting to empty the
bladder when they could, and then they cannot effect it when they would
do so. Others are still more whimsical, and will push into the viscus
needle-cases, bodkins, portions of tobacco-pipes, and such like. The
surgeon should be aware of such whims and fancies.
There is, in general, no difficulty in passing the catheter. A short
one is preferable, there being less chance of giving pain; and the
operation must, of course, be proceeded in with the utmost regard to
delicacy. The forefinger is placed in the upper part of the orifice
of the vagina, and the point of the instrument, when placed a little
above this mark, readily slips into the urethra. It is recommended to
use the clitoris as the guide, placing the finger on this, and moving
the point of the instrument thence downwards; but when this method is
pursued, the catheter is apt to enter the more patent passage. The
instrument is to be carried gently onwards, in a horizontal direction,
till the urine flows. In some cases of enlargement and displacement
of the neighbouring parts, the urethra is elongated, and its course
irregular; in such, a long elastic catheter is required. If objections
are made to the use of the catheter, at an early period of534 retention,
nitrous ether may be given internally, fomentations applied to the
hypogastrium, and a turpentine enema administered. Puncture of the
bladder can seldom, if ever, be necessary in the female; if it should
be required, the opening may be made either above the pubes or
through the vagina. From the latter method there is a risk of fistula
remaining; but this, as will afterwards be noticed, can in some cases
be ultimately made to close. The operation above the pubes has, in some
instances, been necessary during parturition, when instruments could
not be passed by the urethra, nor through the coats of the vagina and
bladder.
False communication betwixt the vagina and bladder, termed
Vesico-vaginal fistula, is usually the result of mismanagement during
parturition. The bladder has been allowed to become over-distended, and
in this state to be pressed upon and bruised by the child’s head; or it
may have been compressed and bruised by instruments employed in tedious
delivery. The consequence is inflammation, violent, and followed by
sloughing. On the separation of the sloughs, the urine escapes, perhaps
six or eight days after delivery; or the anterior surface of the
vagina, and the coats of the posterior and lower part of the bladder,
have been lacerated by the imprudent use of the crotchet, or some such
crooked and awkward tool; then the escape of urine is immediate. The
unnatural flow continues, diminishing after a time, and if the opening
be at first not large, and have gradually contracted, ultimately it may
escape in but small quantities, at least during the recumbent posture.
Of course, the size and site of the opening are very various. I have
been consulted in some dreadful cases, incurable and loathsome—the
consequence of most culpable neglect and ignorant rudeness on the part
of the accoucheur;—the bladder, without any part of its posterior
fundus, has been rent so as to admit the fingers; the rectum also
torn extensively—in some, merely a shred of the sphincter remaining;
feces and urine constantly mixing in one vast offensive cavity. But
in general the opening is in the neck of the bladder immediately
behind the commencement of the urethra, and nearly in the mesial line;
sometimes it is considerably further back. It can be felt by the
finger, and is readily brought into view by means of a proper speculum,
a copper spatula being at the same time used to prevent the folds of
the vagina from interrupting the view; the speculum opened by handles
attached to the blades, and prevented from shutting by a serrated
semicircular plate interposed, is the most convenient and suitable.
Attempts have been made to close the aperture, by paring the edges,
and then inserting sutures; but this is a proceeding both difficult
in execution and not likely to prove successful; the thinness of the
parts, the presence of a secreting surface on each side, and the
oozing of acrid urine betwixt the edges, all militate strongly against
adhesion. No benefit can be expected from any treatment, unless the
opening be of no great size, and in such cases the cautery will be
found most effectual. The speculum is introduced into the vagina,
so as to expose the aperture, and guard the neighbouring parts from
the cautery; and should the opening not appear distinct, a flexible
wire is passed by the urethra, and insinuated through it. A small535
heated cautery is then slid cautiously along the speculum, and applied
lightly to the margins, with the view of producing a superficial
slough; this separates, and during the consequent cicatrisation the
opening contracts. When the edges have again become smooth, the cautery
is applied as before, and by several repetitions complete closure
may ultimately be obtained. The interval between the applications
is necessarily considerable; each must be allowed to have its full
effect. Once I attempted to combine the cautery with the suture; first
applying the heated wire, and after separation of the slough, and when
the margins were tumefied, excited, and apparently prone to adhere
by the formation of new matter, then approximating them by a species
of twisted suture. At first, matters proceeded favourably, but the
ultimate result was not very successful—it was such, however, as to
render the plan worthy of being again tried; if fortunate it would very
much abridge the cure. By the cautery I have succeeded in relieving
many, and in curing a few perfectly. I cannot quit the subject without
expressing regret at the frequent occurrence of such cases. I have
had three or four cases in the hospital at one time, and they are
constantly being presented for relief.
Imperfections of the female genital organs are sometimes met with.
The external parts may be well formed, while the vagina is short, and
the uterus and its appendages are wanting; or these may be perfect, and
the vagina closed at its external orifice, either by a thin and dense
membrane, or by a thick and fleshy substance. Young children are not
unfrequently presented with the latter kind of imperfection, but in
them there is no need for interference; the urine is not obstructed,
and it is only towards puberty that a necessity arises for removal of
the deficiency. At this period, the menstrual discharges are retained,
if the vagina continue closed, and accumulate in great quantity,
producing much distention of the canal, pain in the hypogastrium,
general uneasiness in the parts, and sometimes swelling of them to a
great extent. On division of the membrane, there is sometimes an escape
of many pounds of dark, thick, putrid fluid, and all the symptoms
quickly subside. A cautious incision is made in the mesial line, until
the obstruction be completely divided; if an opening be found, a probe,
or director, is introduced, and by this the knife is guided. There is
seldom any risk of the parts again coalescing; when the obstruction,
however, is unusually thick, the insertion of dressing between the
edges during granulation may be necessary to prevent contraction.
Unnatural adhesions of the external labia occasionally take place,
occurring in early life from the healing of excoriation and ulceration
caused by neglect of cleanliness. Perhaps the closure is not to such
an extent as to prevent escape of the discharges, but still it is
inconvenient and requires attention. The parts must be divided in the
proper direction and to the necessary extent, and, by the interposition
of dressing, reclosure is prevented.
Contraction of the vagina at a distance from the orifice sometimes
occurs. On one occasion I was requested by an accoucheur to536 examine
and divide a very tight, firm stricture, scarcely admitting the finger.
Labour had commenced, and the expulsion of the fœtus was prevented
by the stricture; it was attributed to injury inflicted in a former
delivery. By a probe-pointed bistoury, guided on the finger, it
was notched pretty deeply at many points—a proceeding which I have
frequently followed with advantage in simple stricture of the rectum.
Everything proceeded happily.
Occasionally the contraction of the vagina is to a great extent; the
uterine discharges are not permitted to escape at all, and great
uneasiness is thereby occasioned. In one case, in which the canal may
be said to have been wholly obliterated, from what cause or at what
period it did not distinctly appear, I ascertained the position of the
uterus by the finger passed into the bowel, pushed a curved trocar
on to it through a considerable thickness of parts, and afterwards
dilated this artificial passage by bougies gradually increased in size.
The vagina was thus reëstablished, and menstruation again occurred,
and without interruption. A case, in which the vagina was obliterated
to the extent of from two to three inches, occurred some months ago
at the North London Hospital. It took place, it appears, after an
accouchement, the genital organs being raw and sore, with considerable
loss of substance from phagedænic ulceration. A large tumour could be
felt betwixt the hand placed on the hypogastric region and the finger
in the rectum. The patient was exceedingly urgent in her entreaties
to have the canal restored, and the attempt was made. The contiguous
viscera being emptied, a trocar, guided by the finger in the bowel,
was pushed in the course of the vagina as far as was thought safe; the
canula was retained, and, some days after its withdrawal, the part was
farther dilated by gentian root. It was intended to have carried the
pointed instrument farther, but symptoms of peritoneal inflammation
supervened about the tenth day, and in spite of active treatment proved
fatal. The uterus, os uteri, and from an inch and a half to two inches
of the upper part of the vagina, were enormously distended with dark,
putrid, grumous, and bloody fluid, of the consistence of tar; the
trocar had reached the parietes of the cavity, and, if pushed forward
another line, must have entered the vagina, and allowed the fluid to
escape. There was a quantity of putrid and dark-coloured serosity in
the cellular tissue of the pelvis and behind the peritoneum. It is to
be regretted that I did not feel warranted in the first instance in
pushing the instrument forward more boldly. Had the fluid been allowed
to drain off, the probability is, that the future infiltration and
peritonitis would not have occurred. The intention was, being foiled
in the first attempt, to dilate the canal sufficiently to admit the
finger, and by the direct guidance of that to carry the perforation
farther.
Violent and deep inflammation of the external parts of generation
is not uncommon,—the result of bruise or wound. It is generally met
with in the lower class of prostitutes. The inflammation often attacks
the vagina and neighbouring parts, followed by great swelling; and,
if not allayed, extensive abscess forms, with much fever537 and pain;
pointing takes place betwixt the external and internal labia. The parts
must be copiously leeched, and afterwards fomented; strict rest and
antiphlogistic regimen must be observed, and when matter has formed,
a free opening should be made early, to prevent deep and extensive
mischief. A sinus sometimes, though rarely, results; generally the
cavity fills up, and the discharge ceases in a very few days. These
parts are much more vascular than the lower part of the bowel, and when
in a diseased condition, are not of necessity so frequently put in
action; hence extensive incision and division of the sphincter is here
very seldom necessary.
Tumours of various kinds are met with about the external female
organs; more rarely, internally. Encysted tumours of the labia are not
uncommon, and sometimes solid swellings, varying in size and structure,
grow from these parts. I had occasion to remove one of the latter
description, which weighed many pounds, and had been productive of
great and long inconvenience. The general rules for the extirpation of
tumours apply to them. Considerable hemorrhage may be expected. The
operation must be done so as to deform and impair the functions of the
parts as little as possible.
New and unnatural growths, or enlargements of the natural parts, as
of the prepuce, of the clitoris, or of the internal labia, sometimes
occur, and may require curtailment.
The external parts of elderly females may be the seat of warty
excrescences, degenerating into malignant ulcer, and demanding free
removal by incision.
Tumours of a medullary nature sometimes proceed from the interior
of the pelvis, and displace and interfere with the functions of the
vagina, bladder, and the neighbouring parts; such cases are of course
hopeless, and the treatment must be merely palliative.
Polypous tumours, of various size, structure, and consistence,
sometimes grow from the cavity of the uterus, or from its orifice,
or from the parietes of the vagina. They are generally attached by a
narrow pedicle, except when of a truly malignant nature—occasioning
discharge, mucous and vitiated, sometimes bloody, often profuse.
Bearing-down pains are complained of, and the health declines in
consequence of the discharge. Most of such tumours are benign,
troublesome only from their bulk and situation, and from the irritation
which they produce in the surrounding membrane. They very frequently
have their origin in the substance of the uterus, and are extruded from
it, covered by the mucous lining. Removal by ligature is generally
the most advisable method of extirpation. The site and nature of
the attachment are ascertained, and a strong wire of fine silver,
or a piece of whipcord, is noosed round the base by the finger, and
pushed down close to the origin, care being taken not to include the
healthy parts beyond the growth. The ligature is tightened by passing
it through a canula, or along a strong probe, with a ring at each
extremity, to the lower of which it is secured. It is drawn more
tightly from time to time, till the tumour drop away. A double canula,
the portions of which can be separated, is often used for the purpose.
By practice only can dexterity in such mani538pulation be acquired; the
object being understood, it must be attained by perseverance.
Malignant disease of the uterus is common. Various morbid alterations
are here met with; soft, or hard, or bloody masses, earthy deposits,
&c. The disease generally commences in the neck, with fulness and
thickening; in many females it is attributable to faulty menstruation,
to leucorrhœa, or to other irritations in the neighbourhood. Ulceration
sometimes occurs, not of a malignant nature, from similar causes;
but in old females this is either of a bad kind from the first, or
degenerates, presenting all the usual characters of malignant sore on
a mucous surface. The surrounding induration is usually great, and
quickly spreads to the neck and body of the organ, contaminating also
the neighbouring tissues and the lymphatics.
Some bloodthirsty accoucheurs and operators have attacked the uterus
unrelentingly; more than one appears to have been seized with the
monomania of cutting out part or the whole of the organ. Numerous
females, at a period of life when malignant diseases rarely show
themselves, have been subjected to excision of the os and cervix uteri.
Some forty and fifty were operated on within a very few months; in
almost all of these cases the proceeding was, without a doubt, cruel,
reckless, and unnecessary. Attention to the general health, with local
applications, would, in all probability, have restored the parts to a
healthy condition in the greater number.
Malignant disease affecting the uterus may be removed, at an early
stage, by incision, with propriety and safety, and I have done so
successfully. The part is examined by means of a hollow tube of tin,
polished inside, gently and cautiously introduced. A dilator as well
as a speculum is required in the operative proceedings for removal
of the parts; and for this purpose the instrument mentioned, when
treating of vesico-vaginal fistula, is to be employed. When this
has been introduced, the os uteri is laid hold of by one or more
vulsella, and pulled down; the diseased portion is then removed by
a blunt-pointed knife, the incisions being carried beyond the hard
and altered part. There is not much loss of blood, and it is easily
arrested by stuffing the vagina. Afterwards bland fluids are injected,
and, after a time, those of a gently stimulating nature, to wash away
the superfluous discharge, and promote healing. The state of the sore
can be occasionally examined by means of the speculum, and nitrate of
silver or other applications employed when necessary.
When the disease is in an advanced stage, the neck of the uterus
is involved completely, and there is an uncertainty as to how far
the morbid alteration extends. Only palliative treatment can be
adopted,—soothing applications, and internal remedies according to the
symptoms. The practice of some, however, is more bold and decisive.
The uterus has been cut out by incision of the abdominal parietes. It
has also been removed through the outlet of the pelvis. As was to be
expected, the patients have perished from loss of blood, and the shock
of such barbarous proceedings; one or two, perhaps, survived, only to
die from extension of the disease to the internal parts, within539 a very
few months. Such doings are not justifiable; and, if repeated, should
be punished by the execration of all professional men of sound sense
and principle.
The Common Iliac artery may require ligature, on account of extensive
aneurism, involving the internal iliac, or its branches at their
origin, or encroaching on the external iliac to near the bifurcation.
It may also be necessary, in consequence of wound of the artery, or in
cases of secondary hemorrhage from branches of either the external or
the internal iliac.
An incision is made through the abdominal parietes, commenced over
the passage of the cord through the transverse fascia, and extending
upwards, and a little outwards, for five or six inches; its extent
depending on the size of the patient, the thickness of the parts to
be divided, and the consequent depth of the vessel. By this first
incision, the skin and superficial fascia of the abdomen are divided,
and then the muscles are penetrated, the line of the preliminary
wound admitting of their being cut in the direction of the fibres.
After the external oblique has been passed, the proceedings require
to be conducted with great caution. The fibres are cut by the hand
unsupported, and then the transverse fascia is scratched through,
slightly and with great precaution, cutting upon the finger or a
director introduced at the lower angle of the wound. By means of the
finger, the opening is dilated, and the fascia separated from the
peritoneum. This membrane and the parts within it are then, with
the utmost gentleness, pushed inwards and upwards, by the hands of
an assistant, so as to expose the bottom of the wound. The course
of the vessel is now felt for, and by separating the edges of the
wound, either by the fingers, or by broad and thin copper spatulæ, its
bifurcation may be seen. About an inch or so above this point, the
artery is slightly detached from its connections by the point of the
knife, separating it from the vein on its posterior and inner surface,
and a blunt-pointed needle, armed with a firm ligature, is pushed
beneath, without force, and close to the coats of the vessel. The
deligation is made firmly, and both ends of the ligature are brought
out at the wound; this is then approximated by a sufficient number of
stitches, and a compress and bandage applied.
This operation is not often required. I had recourse to it once in
bleeding, after very high amputation of the thigh, occurring some days
after the operation. The hemorrhage was effectually arrested, but the
patient did not recover from the effects of the previous loss of blood,
and continued to sink.
Aneurism of the branches of the internal iliac, whether spontaneous
or the result of wound, is rare. When it does exist, its signs are
sufficiently distinct. The old operation—opening the tumour by direct
incision, and tying the vessel close to the cyst—has been performed
successfully in one remarkable case on record. But this is attended
with much risk, there being no means of commanding the bleeding during
the incisions, nor until the ligature is placed and secured. The
preferable proceeding is to tie the internal iliac near540 its origin,
as has been put in practice successfully in a few cases. The same
incisions are made as for reaching the common iliac, and then the
sacro-iliac junction is felt for; with the nail of the forefinger the
cellular tissue is cautiously and gently separated, and a needle and
ligature placed under the vessel. In a corpulent adult, a needle, with
a moveable point, may perhaps be useful, as also the copper spatulæ,
to keep the parts aside; and a serrenœud may assist in the securing of
the noose. It was the fashion once, and perhaps is so still, for every
young and aspiring surgeon, when he was about to attempt lithotomy
for the first time, to invent or alter some strange crooked tool, for
smoothing, as he thought, his way into the bladder. The rage now,
more especially on the other side of the Atlantic, is all for curious
aneurism needles and tonsil shavers. It ought never to be forgotten,
that the simplicity of any proceeding and of every machine is the
measure of their perfection. I have had by me a lot of needles, all
very ingenious, at the various operations for aneurism which I have
had occasion to perform—many of them of the most difficult nature—and
the simple needle has always been found to answer the purpose most
perfectly.
Aneurism in the groin is not uncommon, and is very easily recognised.
The old operation has been attempted, and unsuccessfully. Ligature
has been placed on the distal side of the tumour, with no favourable
result. One horrid example of the latter operation is on record, in
which the femoral artery had been completely obliterated spontaneously,
and nerves, vein, and portions of the muscles, were all included in
ligature, by one random thrust of a large sharp needle. The external
iliac is to be tied—a proceeding now regarded as one of the regular
operations of surgery, and likely to insure a favourable result. It was
first undertaken in a case of secondary bleeding after ligature of the
femoral, and since, has often been performed for the cure of inguinal
aneurism, with almost uniform success. It has also been practised
successfully, on account of hemorrhage after amputation. I was under
the necessity lately of putting a ligature round the external iliac,
on account of profuse bleeding from an opening in the groin, made
five weeks previously, to secure the common femoral, on account of
hemorrhage from a stump of the thigh. This operation should have been
had recourse to in the first instance, the deligation of the common
femoral being an operation not likely to be followed by permanent
closure of the vessel, in consequence of its shortness, and the
branches given off from it both above and below. The patient ultimately
recovered from these three capital operations. The incisions are made
in the same direction as recommended for ligature of the common and
internal iliacs, but not nearly so extensive. This is preferable to
incision, either in the direction of the vessel, or of a semilunar form
with one of the corners pointing upwards; the abdominal muscles are
less weakened, less injury being inflicted on them, and no troublesome
bloodvessels are encountered. The artery is well circumstanced for the
application of ligature, affording a considerable extent without the
giving off of any branches. It is easily exposed by cautious separation
of the cellular tissue, and the ligature is541 secured either towards its
middle, or at its upper part, according to the size and situation of
the aneurism.
Popliteal aneurism is of more frequent occurrence than any of the
preceding; and in regard to it, also, the old operation has deservedly
fallen into disuse. It seems in most cases to be occasioned by partial
laceration of the coats of the vessel; a sudden pain, and a feeling as
of the receipt of an injury on the part, are generally felt, during
some violent or unusual exertion; the pain continues, and an unwonted
beating is soon perceived in the ham, along with inconsiderable
swelling; the tumour with pulsation increases, and may ultimately
attain a large size, causing pain, general uneasiness in the limb,
and lameness, sometimes œdema. In cases of long duration, and when
the patient is cachectic, the bones become diseased, absorption being
caused by the pressure of the tumour, and deep extensive abscess may
form in the soft parts.
The superficial femoral is to be tied, and the preferable point is
where it is crossed by the sartorius muscle. This is always a better
practice than removal of the limb, which has not unfrequently been
resorted to in cases of large aneurism; there is great risk in such
a proceeding, the anastomosing vessels in the thigh are all much
enlarged, profuse hemorrhage takes place during the incisions, not
completely arrested by any pressure, and probably twenty arteries or
more require ligature, as I have witnessed; after all, the occurrence
of secondary bleeding is not unlikely. I have tied the femoral artery,
with a favourable result, in some cases of very large aneurismal
tumour, and in one instance after the cyst had been imprudently
punctured. An incision is made from three to four inches in length,
and in an oblique direction in regard to the thigh, tracing the inner
border of the sartorius muscle, and so placed that its middle may
correspond with that part of the artery on which the ligature is to
be put. In order to insure the wound being thus situated, there is no
need for measurements; these are but a clumsy substitute for anatomical
knowledge. The surgeon, well acquainted with the relative situation of
the parts, finds it sufficient to ascertain the exact course of the
muscle by manipulation, whilst the thigh is slightly bent, and then
guides his knife by the eye, unfettered with mathematical diagrams. The
muscle is exposed almost by the first incision; the dissection is then
continued through the cellular tissue on its inner border, until the
sheath of the bloodvessels is reached, the branches of the crural nerve
on the fore part being carefully placed aside uninjured; the sheath is
cautiously opened immediately above where the muscle conceals it, and
the artery separated from its connections to a very slight extent; the
needle is then passed, and the ligature applied. The operation, when
thus conducted, is exceedingly simple. But embarrassment and delay have
often been experienced from following an opposite method, cutting down
on the outside of the sartorius; the muscle must either be dissected
from its attachments and turned over, or cut across; or the artery
cannot be found, and an additional external wound is necessary.
The artery may require ligature at a higher point, either in
conse542quence of wound, or for the cure of femoral aneurism. This
disease, however, is very unfrequent. When it does exist, it is usually
so situated as not to admit of the favourable application of a ligature
below the origin of the profunda; and it may be considered necessary to
tie the common femoral. The course of this artery being superficial,
is easily ascertained; an incision of convenient extent is made in the
same line, penetrating the skin and fatty matter; the cellular tissue
is carefully separated, and the sheath exposed; a limited opening is
made, with corresponding detachment of the vessel, and the ligature
applied, close to the lower edge of the ligament of Poupart. But
ligature of the external iliac is in all cases to be preferred, for the
reasons already given. This has proved successful in more than one case
of double aneurism, one in the groin, the other in the ham.
In ligature of the common and of the superficial femoral, the vein is
in more danger than the nerve, and the utmost caution is required lest
it be punctured. It has been wounded—I witnessed one instance of it;
the opening was drawn together and closed by ligature, inflammation of
the vein supervened and proved fatal.
When secondary bleeding occurs, on the separation of the ligature,
either after this operation or after that for popliteal aneurism,
compression is not to be trusted to, nor should the vessel be tied
higher in the thigh. From imprudent reliance on the former method I
have known patients perish. An incision must be made in the same line
as the former, and a ligature placed on the vessel both above and below
the bleeding point, as may be necessary.
The arteries of the leg very seldom require ligature, except for
wound. In such cases, the source of the bleeding must be the guide to
the incisions, and these should be placed so as to interfere with the
muscles as little as possible, always in the direction of their fibres.
When the bleeding point is arrived at, the vessel is exposed to a short
distance, and tied above and below the wound. During the dissection,
it will in most cases be necessary to arrest the bleeding by pressure
in the ham, either by the fingers of an assistant, or by means of a
tourniquet.
The thigh may be the seat of aneurismal varix, the result of wound,
as in the following case. Fourteen years ago, a young man wounded the
lower part of his thigh deeply by the accidental thrust of a narrow
chisel. The puncture was in the direction of the femoral artery;
violent hemorrhage was the immediate consequence, and after he had
fainted the wound was stuffed and compression applied. In eight days
the parts had healed, and he returned to work as usual. But about
twelve months afterwards, troublesome pulsation was perceived in the
part, at the same time the veins of the leg became varicose, and a
succession of ulcers formed on the lower and anterior portion of the
limb. The affection attracted but little of his notice till about six
months since, when he observed a considerable swelling in the site of
the wound, beating strongly, and the pulsations accompanied with a
peculiar thrilling sound and feel—not confined to the tumour, though
strongest there, but extending to the groin along the course of the
femoral vein, which was evidently much dilated throughout its whole
course. At present the tumour is nearly equal543 to the fist in size,
of regular surface and globular form, pulsating very strongly, and
imparting to the hand the peculiar sensation of aneurismal varix,
remarkably distinct and powerful. The pulsation and thrilling are
continued, in a less degree, to Poupart’s ligament, and down to the
calf of the leg. On applying the ear close to the tumour, or listening
through the stethoscope, the peculiar noise is not only felt, but
heard of almost startling intensity—somewhat resembling the noise of
complicated and powerful machinery, softened and confused by distance.
By making firm pressure on the tumour, the thrill is lost, and the
regular pulsation alone perceived; at the same time, the turgescence of
the femoral vein disappears, and on compressing the femoral artery in
the middle of the thigh, both pulsation and thrilling are arrested, and
the swelling much diminished,—but only temporarily, for the collateral
circulation is free and complete. He feels little pain, but exercise
and exertion of every kind are seriously impeded; constant and firm
pressure on the swelling, with uniform compression of the whole limb,
has been employed, with the effect of relieving all the symptoms, and
rendering the limb much more useful, and by its continuance it is to be
hoped that the disease will at least be considerably palliated.
In the lower extremity, as in the upper, the bursæ become enlarged,
in consequence either of pressure or of external injury. The
affection may be acute, following a blow or squeeze, but is most
frequently chronic, enlarging gradually and with little or no pain,
and caused by habitual pressure on the part. From this, it will at
once be understood, why the bursa over the patella should be the one
most commonly affected. Its vulgar name, housemaid’s-knee, marks
its cause—the avocations of such persons requiring them to rest on
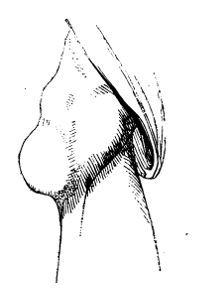 one or both knees, frequently, and often for a long time. It also
occurs in shop-keepers, and other persons accustomed to shut drawers
with their knee, or in other ways to make frequent pressure on that
part,—in gardeners, and those employed in similar pursuits. In the
acute swelling from injury, local depletion, fomentation, and rest
are required, and these are generally sufficient to arrest the
swelling, and promote its subsidence; but, in some cases, the fluid
is deteriorated and the surface inflames, free incision is required,
followed by poultice, and afterwards by simple dressing. In the
chronic collection of clear fluid, gentle and continued stimulation
of the surface, as by the gum and mercurial plaster, causes gradual
decrease by absorption; the causes of the affection being at the
same time studiously avoided. The tumour sometimes, as here shown,
attains a large544 size, and from repeated inflammatory attacks
becomes consolidated. The cyst is thickened, and lymph is effused
into the cavity so as to convert an encysted swelling into one of
solid consistence. In such cases as these, the tumour may cause such
inconvenience as to make the patient desirous to have it dissected
out. This is easily and safely effected; the incisions are made in the
direction of the limb, and it is kept at rest in the extended portion
for some time, so as to favour the healing of the wound.
one or both knees, frequently, and often for a long time. It also
occurs in shop-keepers, and other persons accustomed to shut drawers
with their knee, or in other ways to make frequent pressure on that
part,—in gardeners, and those employed in similar pursuits. In the
acute swelling from injury, local depletion, fomentation, and rest
are required, and these are generally sufficient to arrest the
swelling, and promote its subsidence; but, in some cases, the fluid
is deteriorated and the surface inflames, free incision is required,
followed by poultice, and afterwards by simple dressing. In the
chronic collection of clear fluid, gentle and continued stimulation
of the surface, as by the gum and mercurial plaster, causes gradual
decrease by absorption; the causes of the affection being at the
same time studiously avoided. The tumour sometimes, as here shown,
attains a large544 size, and from repeated inflammatory attacks
becomes consolidated. The cyst is thickened, and lymph is effused
into the cavity so as to convert an encysted swelling into one of
solid consistence. In such cases as these, the tumour may cause such
inconvenience as to make the patient desirous to have it dissected
out. This is easily and safely effected; the incisions are made in the
direction of the limb, and it is kept at rest in the extended portion
for some time, so as to favour the healing of the wound.
Unyielding parts, habituated to pressure, defend themselves by the
interposition of a moveable bag containing fluid; betwixt them and the
surface the cellular tissue condenses into a cyst, its internal surface
assuming a serous appearance, and secreting a fluid resembling the
synovial. Such adventitious bursæ are not unfrequent on the ankles and
feet, as in tailors, or others usually sitting cross-legged. They may
attain a considerable size, and so produce deformity; but they should
not be interfered with unless they become inconvenient, as from excited
action.
When the extremity of the metatarsal bone of the great toe is large,
and consequently the seat of pressure, a bursal formation is produced
in the soft parts covering it; this from increase of pressure, or other
irritation, may inflame—forming the painful and troublesome disease
termed Bunnion. Sometimes unhealthy abscess occurs, with thickening,
infiltration, and condensation of the surrounding cellular tissue; in
such cases, incision and poultice are required, and occasionally it is
necessary to destroy the unsound cellular tissue and the degenerated
cyst by free application of the caustic potass. The cyst is thus got
rid of, healthy granulation takes place, and by afterwards avoiding
undue pressure upon the part, a permanent cure is obtained.
It has been elsewhere mentioned, that cartilaginous bodies sometimes
form within articulating cavities, occasionally attached by a narrow
and slender connection with the secreting surface, but generally
loose, seldom numerous, and usually of no great size. They are most
commonly met with in the knee-joint, producing inconvenience by
impeding progression. Sometimes they are neither painful nor annoying,
being small, and seldom becoming interposed between the articulating
extremities of the bones during motion; such ought not to be interfered
with. But when large, they may be so troublesome as to warrant incision
and removal. The foreign body is made to project on one side, and,
having been made as superficial as possible at a favourable point, is
fixed by the fingers of an assistant. The integuments are then drawn
to one side, and an incision made over the body, the capsule is cut to
as limited an extent as possible, and removal effected by pressure—or
it may be laid hold of by a hook, and extracted; if the cartilaginous
substance be attached by a pedicle, this must be divided, but with
great caution. The integuments are immediately allowed to resume
their natural situation, and so to close the wound of the capsule by
overlapping it; the skin is then accurately approximated by adhesive
plasters. The limb is kept extended, and not the slightest motion
of the joint permitted. The patient is confined constantly to the
recumbent posture, purged, and545 kept on low diet; the utmost vigilance
is necessary to prevent inflammation of the synovial apparatus. In some
patients on whom I have performed this operation, the wound closed
by the first intention, and no untoward symptom threatened, motion
and the erect position being resumed in a few weeks. But in the last
case which came under my care, though the extirpation was performed
with the utmost care, most violent inflammation supervened; the wound
opened, synovial secretion flowed out in large quantity, profuse escape
of unhealthy matter followed, and exhausting discharge continued for
many weeks. At one time the constitutional disturbance was so great
as to endanger life; the limb was saved with difficulty, the joint
anchylosed. From the result of this case, I am disposed to dissuade
operative interference, unless the patient strenuously urge it, and be
willing to take the responsibility for the consequences on himself.
[The most common distortion to which the human body is liable is
Club-foot; an affection which has at all times attracted the notice
of the profession, but which has received unusual attention within the
last ten years on account of the novel operation suggested for its
cure by Dr. Stromeyer of Hanover, in Europe. The lesion is, for the
most part, congenital. It may, however, be developed after birth, and
even at an advanced period of life, from the foot being accidentally
placed in a constrained position, and so retained until the soft
structures—particularly the muscles and ligaments—are moulded into a
new shape, or until they become fixed in their new situation. Various
mechanical causes may give rise to this malady, such as splints and
bandages, by which the parts to which they are applied are injuriously
compressed, or thrown out of their natural relations. Similar results
are produced by convulsions, dentition, nervous irritation, contusions,
sprains, fractures, partial luxations, and preternatural laxity of the
ligaments. In some instances the defect is occasioned by the presence
of a corn, an ulcer, or some other disease which induces the person
to walk on one side of the foot, the tip, or the heel, to ward off
pressure from the tender parts. A vicious habit is thus established,
which, if it be kept up, as it often is, for any length of time, leads
to irregular action in the muscles, and to distortion of the bones into
which they are inserted.
The formation of congenital club-foot has never been satisfactorily
explained. By some—as Meckel, St. Hilaire, Serres, and Breschet—it has
been ascribed to an arrest of development. This theory, however, for
various reasons, is untenable, and has therefore not been generally
adopted by surgical men. Mons. Martin, a recent French writer, thinks
it is mainly occasioned by the pressure of the parietes of the uterus
on the feet of the infant during gestation, owing to a deficiency of
the amniotic fluid; an opinion in which he is joined by Professor
Cruveilhier. That the disease may proceed from this source in some
instances maybe readily supposed, but that this is the only cause, is
what few will believe. The most plausible hypothesis, in my opinion, is
that of Mons. Guerin of Paris. He supposes that the primary mischief is
in the nervous system, and that the spasmodic546 and permanent shortening
of the muscles of the affected limb is altogether consecutive. He
sums up the results of his numerous observations in the following
propositions:—1. Congenital club-foot is the effect of a convulsive
contraction of the muscles of the leg and foot. 2. In the absence of
general or direct traces of the convulsive affection we may almost
always discover some immediate characters which indicate the nature
of the exciting cause. 3. There are three constituent elements in the
retraction of the muscles of the part: namely, the immediate shortening
of their substance and tendons; a certain degree of paralysis; and,
lastly, a consecutive arrest in the development of their substance.
4. There are no other causes of genuine congenital club-foot than
convulsive muscular retraction. The pressure of the parietes of the
uterus on the fœtus appears, indeed, in some cases, to produce a
deformity of the limbs and feet, similar to but not identical with
club-foot. The views of Mons. Guerin are confirmed, in some degree,
by the history of those cases which occur after birth; but future
observation must determine whether they are correct or otherwise.
The congenital variety of this distortion often affects both feet
simultaneously, though rarely to the same extent. In one hundred and
sixty-seven cases reported by Dr. Detmold of New-York, the disease
was double in nine-three; in forty-one it occurred in the right foot
only, and in thirty-three only in the left. Of eighty cases collected
from various sources by Mons. Bouvier of Paris, or observed by
himself, two-fifths were double; one-third affected the left limb, and
one-fourth the right. Of sixty-one cases furnished by Martin, another
French writer, twenty-six were double and thirty-five simple: of the
latter, eighteen were of the right and seventeen of the left foot.
Mons. Helt has published the results of thirty-one cases, in nineteen
of which the disease was double; in two it was more distinctly marked
on one leg than on the other; and in one instance the calcaneal form of
the lesion was united with the inverted. In twenty-one cases observed
by Scoutetten, both feet were deformed in nine; and in the other twelve
the right limb was exclusively involved seven times; the left five
times.
The disease would appear to be more frequent in males than in females,
though the relative proportion has not been ascertained. The following
table, embracing three hundred and twenty-nine cases, will throw some
light on this subject:—
| Authors. | Number. | Males. | Females. |
| Detmold | 167 | 98 | 69 |
| Bouvier | 80 | 48 | 32 |
| Martin | 61 | 45 | 16 |
| Scoutetten | 21 | 13 | 8 |
| | —— | —— | —— |
| | 329 | 204 | 125 |
There are certain facts which would seem to show that club-foot is
sometimes hereditary; or, at all events, that it may occur in several
members of the same family. Thus, Dr. Detmold states that he has547 been
able to trace the hereditary predisposition to this deformity in not
less than eighteen cases, and in all excepting one, to the father’s
side. Whether this was a mere coincidence, or obtains generally,
it is impossible to say. Mons. d’Ivernois relates an instance in
which four brothers were all born with the feet twisted inwards; and
another writer, Mons. Helt, speaks of a family, which consisted of six
children, all of whom were afflicted with congenital club-foot. In the
latter case the disease was probably hereditary, as one of the parents
was labouring under the same infirmity. It should be observed, however,
that club-footed parents do not always produce club-footed children.
Club-foot may be conveniently divided into four varieties—the inverted,
everted, phalangeal, and calcaneal—which differ from each other not
only in regard to the character of the distortion and the accompanying
phenomena, but likewise in relation to the frequency of their
occurrence and the nature of their proximate causes. The most common
form by far is the inverted, usually denominated varus, in which
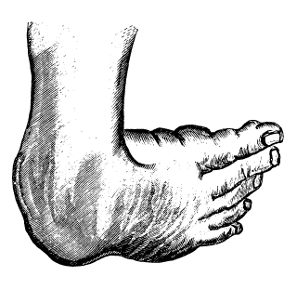 the patient walks upon the outer ankle, the great toe being directed
inwards and upwards. The muscles of the calf and the adductors of the
foot are contracted, and hence there is not only elevation of the
heel, but a peculiar inward twist of the foot, analogous to supination
of the hand. This alteration occasions the most serious impediment
to progression, and when it reaches its highest point imparts a most
disagreeable aspect to the affected limb. In the higher grades of the
disorder, the sole of the foot is literally scooped out, as it were,
as well as deeply furrowed; the instep, on the contrary, is unusually
convex and prominent; the small toes generally present in a vertical
position, while the big one, separated from the rest, looks upwards
and inwards; the outer margin of the foot, which, in conjunction with
the corresponding malleolus, chiefly sustains the weight of the body,
is almost semicircular in its shape, rough, and callous; and the
tendo-Achillis, forced obliquely towards the inner side of the leg,
forms a tense, rigid chord beneath the skin.
the patient walks upon the outer ankle, the great toe being directed
inwards and upwards. The muscles of the calf and the adductors of the
foot are contracted, and hence there is not only elevation of the
heel, but a peculiar inward twist of the foot, analogous to supination
of the hand. This alteration occasions the most serious impediment
to progression, and when it reaches its highest point imparts a most
disagreeable aspect to the affected limb. In the higher grades of the
disorder, the sole of the foot is literally scooped out, as it were,
as well as deeply furrowed; the instep, on the contrary, is unusually
convex and prominent; the small toes generally present in a vertical
position, while the big one, separated from the rest, looks upwards
and inwards; the outer margin of the foot, which, in conjunction with
the corresponding malleolus, chiefly sustains the weight of the body,
is almost semicircular in its shape, rough, and callous; and the
tendo-Achillis, forced obliquely towards the inner side of the leg,
forms a tense, rigid chord beneath the skin.
Sometimes both feet are affected with varus, so that their points form
an acute angle with the leg; or approach so nearly as to touch, or
even overlap one another. In the majority of cases the thigh and leg
retain their natural conformation, being merely somewhat atrophied;
occasionally, however, one or both knees project slightly548 inwards or
outwards, owing to the contraction of the hamstring muscles.
The second variety of this deformity, anciently called valgus, may
be regarded as the opposite of varus, the patient treading on the
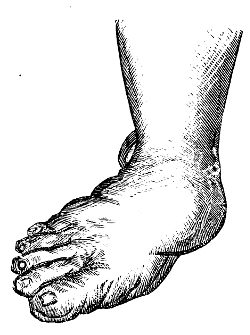 internal margin of the foot, while the external is entirely removed
from the ground. The sole is directed outwards and slightly backwards,
the toes are more or less elevated, and the outer ankle is in a state
of semiflexion. The heel is drawn upwards and somewhat outwards, the
internal malleolus is uncommonly prominent, the instep is flatter than
natural, and the muscles of the calf, together with the adductors of
the foot, are permanently contracted. When the disease has attained its
highest point, the patient has an unsteady, vacillating gait, from the
difficulty which he experiences in preserving his centre of gravity.
Valgus is comparatively rare; and, like the first variety of the
distortion, it may affect one or both limbs. It is seldom a congenital
affection, but is almost always produced by some local injury—as a
sprain or blow.
internal margin of the foot, while the external is entirely removed
from the ground. The sole is directed outwards and slightly backwards,
the toes are more or less elevated, and the outer ankle is in a state
of semiflexion. The heel is drawn upwards and somewhat outwards, the
internal malleolus is uncommonly prominent, the instep is flatter than
natural, and the muscles of the calf, together with the adductors of
the foot, are permanently contracted. When the disease has attained its
highest point, the patient has an unsteady, vacillating gait, from the
difficulty which he experiences in preserving his centre of gravity.
Valgus is comparatively rare; and, like the first variety of the
distortion, it may affect one or both limbs. It is seldom a congenital
affection, but is almost always produced by some local injury—as a
sprain or blow.
The phalangeal club-foot—the pes equinus of the older writers—is
 caused by a shortening of the gastrocnemial and soleal muscles, aided,
in some cases, by the flexors of the toes. In this species of the
deformity the individual walks upon the ball of the foot, the toes,
or upon the metatarso-phalangeal articulations, without the heel or
any other part of the sole touching the ground. The distance at which
the heel is raised varies in different cases, from six lines to four
or five inches, according to the extent of the contraction upon which
the distortion depends. Considerable diversity is observed in regard
to the manner in which the person treads on the ground; most commonly
the ball of the little toe bears the brunt of the pressure, but in some
instances the weight is thrown upon the great toe, or it is diffused
over the whole of the fore part of the plantar surface. In the worst
gradations, the heel is so much elevated that the foot forms nearly a
straight line with the leg, the toes are much deformed, the instep is
unnaturally convex, the plantar aponeurosis is greatly contracted, and
the skin above the heel is thrown into dense wrinkles.
caused by a shortening of the gastrocnemial and soleal muscles, aided,
in some cases, by the flexors of the toes. In this species of the
deformity the individual walks upon the ball of the foot, the toes,
or upon the metatarso-phalangeal articulations, without the heel or
any other part of the sole touching the ground. The distance at which
the heel is raised varies in different cases, from six lines to four
or five inches, according to the extent of the contraction upon which
the distortion depends. Considerable diversity is observed in regard
to the manner in which the person treads on the ground; most commonly
the ball of the little toe bears the brunt of the pressure, but in some
instances the weight is thrown upon the great toe, or it is diffused
over the whole of the fore part of the plantar surface. In the worst
gradations, the heel is so much elevated that the foot forms nearly a
straight line with the leg, the toes are much deformed, the instep is
unnaturally convex, the plantar aponeurosis is greatly contracted, and
the skin above the heel is thrown into dense wrinkles.
549
In the fourth variety—the calcaneal, recently described by Mons.
Scoutetten—the limb rests upon the heel, the toes being drawn upwards,
 towards the anterior surface of the leg, with which they sometimes
form an acute angle. The immediate cause of the deformity seems to be
a contraction of the anterior tibial muscle and of the extensor of the
great toe, assisted occasionally by that of the common extensor of the
foot. The tendons of these muscles form an evident protuberance under
the skin, where they present the appearance of tense, rigid chords,
which powerfully resist the extension of the limb. The inner margin of
the foot, as seen in the cut, is sensibly elevated above the outer, and
there is always considerable atrophy of the leg. The distortion, which
is almost always congenital, is exceedingly rare. Occasionally the foot
inclines slightly outwards, owing to the inordinate contraction of the
common extensor muscle.
towards the anterior surface of the leg, with which they sometimes
form an acute angle. The immediate cause of the deformity seems to be
a contraction of the anterior tibial muscle and of the extensor of the
great toe, assisted occasionally by that of the common extensor of the
foot. The tendons of these muscles form an evident protuberance under
the skin, where they present the appearance of tense, rigid chords,
which powerfully resist the extension of the limb. The inner margin of
the foot, as seen in the cut, is sensibly elevated above the outer, and
there is always considerable atrophy of the leg. The distortion, which
is almost always congenital, is exceedingly rare. Occasionally the foot
inclines slightly outwards, owing to the inordinate contraction of the
common extensor muscle.
The changes which the bones, ligaments, and muscles undergo, vary, not
only in the different species of club-foot, but in the different stages
of the same case. The greatest alteration appears to exist on the
part of the tarsal bones, which, although they are rarely completely
dislocated, are generally somewhat separated from each other,
twisted round their axis, variously distorted, atrophied, or marked
by irregular spicula or exostoses. The calcaneum, cuboid, scaphoid,
and astragalus, always suffer more than the other bones; which,
however, as well as those of the metatarsus and of the toes, usually
participate, more or less, in the deformity. The ligaments, in recent
cases of club-foot, do not present any material changes, but in those
of long standing, or in the higher grades of the affection, they are
invariably stretched in the direction of extension, and relaxed in that
of flexion. In some instances the original structures are partially
replaced by bands of new formation, of a dense fibrous character—the
volume and resistance of which vary according to the duration of the
disease and the pressure of the parts which they serve to connect
together. The muscles also are not much altered in the first instance,
except that they deviate from their natural direction, and that, like
the ligaments, they are elongated on the one hand and shortened on
the other. In ancient cases the whole limb is always considerably
wasted, and many of the muscles are remarkably thin and pale, or
even transformed into soft, fatty bundles. The cellular substance is
condensed and diminished in quantity; the adeps is absorbed; and even
the vessels and nerves supplying the affected part are apparently
reduced in volume. The skin of the foot, which receives the principal
brunt of the pressure in standing and walking, is generally very much
thickened and indurated, and large synovial bursæ are often formed
beneath it, which are apt to550 inflame, and thus add to the suffering
of the patient. Such is an outline of the more important changes
experienced by the different textures in cases of club-foot: to enter
more minutely into the subject would be foreign to the design of this
article, the object of which is merely to present a general idea of the
nature, causes, and treatment of this singular distortion.
The treatment of this affection should be delayed as little as
possible. The sooner, indeed, it is attended to, the more probable will
be the chances of effectually removing it. This is equally true, both
of the congenital and of the accidental form of the disease. The bones
in early life and in recent malformations are much more easily restored
to their normal position than in youth and manhood, or in cases of long
standing; and the muscles also regain much sooner, as well as more
completely, their original power. In the worst grades of the disease
it is often exceedingly difficult, if the treatment be delayed until
after the age of puberty, to accomplish a cure without great carving of
the tendons, and the constant employment for months of various kinds of
apparatus.
It is still a disputed point, whether, in the treatment of this
affection, particularly in infants and young subjects, it is necessary,
or even justifiable, to divide, as a preliminary step, the tendons
of the muscles which are instrumental in keeping up the distortion.
Without endeavouring to settle this question, for which the time has
not perhaps yet arrived, I must express my conviction that the present
rage for tenotomy is calculated to do a vast deal of harm, not only
in individual cases, many of which do not require it, but, what is
worse and more deeply to be lamented, in bringing discredit upon an
operation, which, if judiciously performed, cannot fail to be of the
greatest benefit. In most of the cases occurring in children under
two or three years of age, division of the tendons is altogether
unnecessary; indeed, one of our most distinguished orthopedic surgeons,
Dr. Chase of Philadelphia, seems to trust almost entirely to the
employment of apparatus, and to resort to tenotomy only in the worst
grades of the disease. Whether this practice will ultimately be
adopted by the profession generally, or the division of the tendons be
restricted to particular cases, it would be premature to predict; but
my opinion is, that much more cutting is now done than is necessary,
or than would be done if the treatment of the disease were better
understood than it appears to be.
Different kinds of apparatus are in vogue for the cure of this
deformity, and it is therefore impossible to determine which is the
best, or which should be employed to the exclusion of the others. Every
practitioner seems to have his own notions on the subject, and to
adopt such measures as whim, fancy, or caprice may dictate. Whatever
apparatus be resorted to, the great caution to be observed, on the
part of the surgeon, is, that the extension be made in a slow and
gradual manner, that the skin be protected from friction and uneven
pressure, and that the dressings be steadily retained during the night,
as well as during the day, until several weeks after all deformity
has disappeared. The object of these directions is self-evident, and
too important to be neglected in our curative procedures. The time551
required for restoring the limb to its normal position must necessarily
vary in different cases, and depend upon so many circumstances as to
render it impossible to lay down any specific rule. From six weeks
to four months, however, may be considered as a fair average, though
occasionally a much longer period will elapse. The division of the
tendons of the contracted muscles generally expedites the cure by
several weeks.
In the operation for dividing the tendo-Achillis the patient may
either lie on his abdomen or sit on a chair, and the heel is to be
drawn downwards by an assistant with the left hand, the right being
placed upon the plantar surface of the toes. The necessary tension
being thus given to the part that is to be cut, the surgeon passes a
narrow, straight, sharp-pointed bistoury through the skin, from one to
two inches above the internal malleolus, flatwise between the tendon
and the deep-seated structures. The knife is then pushed on until it
reaches the opposite side of the tendon, when its edge is brought in
contact with the anterior surface of the chord, which is now completely
divided by steady pressure upon the handle of the instrument. The
separation of the parts is indicated by an audible snap, and by the
immediate cessation of the tense resistance of the tendo-Achillis.
Scarcely a drop of blood is lost during the operation, which is
almost unattended with pain, and is accomplished in a few seconds. A
strip of adhesive plaster is applied over the little puncture, which
generally heals by union by the first intention; and the limb, laid in
an easy position, should be supported by a paste-board splint and a
common roller. The apparatus for keeping up permanent extension may be
advantageously employed in three or four days after the operation.
The interval between the divided extremities of the tendon is filled
up with coagulating lymph, which is often poured out in considerable
quantities. As in other situations, it becomes gradually organised,
and is finally converted into a firm, dense substance, not unlike the
original structure.
The tendon of the posterior tibial muscle may be cut most
advantageously about two inches above and behind the internal
malleolus. The operation is conducted upon the same principles as in
the preceeding case, and the only particular caution to be observed
is to avoid the posterior tibial artery and nerve, which might be
endangered by carrying the knife too deeply. The most favourable
situation for dividing the anterior tibial muscle, is where it passes
over the ankle-joint: the long flexor of the great toe may be cut in
the sole of the foot, where, when it interferes with the rectification
of the limb, it forms a tense, prominent chord.—ED.]
The phalanges of the toes in general resemble those of the fingers in
their diseased actions. Exostosis of the extremity of the distal
phalanx, however, has no analogy in the upper extremity; it is by no
means an uncommon affection, and usually occurs in the great toe. The
growth is generally globular and rough in its extremity, narrow at its
origin, attached on the dorsal aspect, projecting obliquely upwards,
and always of similar structure with the phalanx. Sometimes552 they are
 met with of a size nearly equal to that of the bone from which they
spring, but the majority are considerably smaller. The only one I
have met with springing from a small toe is here sketched. At first
the patient complains merely of pain in the part while walking; soon
the pain increases so as to impede progression very seriously; then
the nail is found to be raised at its margin, and to cover a hard,
unyielding, and tender swelling. The elevation of the nail increases,
and the tumour becomes more apparent, covered by hardened cuticle,
causing great uneasiness, and almost entirely preventing walking
exercise.
met with of a size nearly equal to that of the bone from which they
spring, but the majority are considerably smaller. The only one I
have met with springing from a small toe is here sketched. At first
the patient complains merely of pain in the part while walking; soon
the pain increases so as to impede progression very seriously; then
the nail is found to be raised at its margin, and to cover a hard,
unyielding, and tender swelling. The elevation of the nail increases,
and the tumour becomes more apparent, covered by hardened cuticle,
causing great uneasiness, and almost entirely preventing walking
exercise.
It has been recommended to expose the tumour by incision, and remove
it at its origin. This affords temporary relief, but the disease is
generally in no long time reproduced, and the incision must either be
repeated, or the phalanx amputated. The preferable practice, according
to my experience, is to remove the phalanx at once. It is less tedious
and painful than the incision, produces very little, if any, impediment
to progression, and of course is quite effectual in eradicating this
most annoying though apparently simple disease.
Of Fractures.—Deformity, shortening, loss of power, unnatural motion
on extending and moving the part, pain, and grating, mark solution of
 continuity in bone, or fracture. Swelling, with spasmodic of these
symptoms may be wanting; there is little deformity, and no shortening,
when one of two or more action of the muscles, soon takes place. One or
several parallel bones is fractured. In fracture of the extremities,
extrication of air into the cellular tissue, about the ends of the
bone, is not unfrequent, though difficult to account for—giving rise
to crepitation, superficial, and quite a distinct sensation from that
imparted by the broken bone.
continuity in bone, or fracture. Swelling, with spasmodic of these
symptoms may be wanting; there is little deformity, and no shortening,
when one of two or more action of the muscles, soon takes place. One or
several parallel bones is fractured. In fracture of the extremities,
extrication of air into the cellular tissue, about the ends of the
bone, is not unfrequent, though difficult to account for—giving rise
to crepitation, superficial, and quite a distinct sensation from that
imparted by the broken bone.
Bones become brittle as age increases, and fragility is also induced by
certain disordered and debilitated states of the constitution. In some
patients, the bones give way on very slight force being applied, after
what may have been supposed a rheumatic attack; the thigh is broken by
turning in bed, or by walking from the bed to a chair. In one instance,
I had put up a fracture of the thigh with a long splint, and in three
weeks afterwards the humerus was broken over the end of the splint
during an attempt by the patient at change of posture. In many such
cases union either does not take place, or is very imperfect.
In children, the bones frequently contain little earthy matter, bend
easily, and often break partially on the convexity of the curve. Even
at the age of twelve or thirteen, bending of the bones from injury
sometimes occur to a great extent, as of the forearm from a fall on
the palm of the hand; in adjusting the parts, a slight crackling is
heard when they are brought nearly straight. Complete553 solution of
continuity, though more rare, is occasionally met with in very young
subjects.
Fractures are generally the result of great force applied directly
to the shaft of a bone, or to its extremity; but they are also not
unfrequently caused by twisting of the limb whilst the muscles are in
a powerful action. Bones are broken transversely; but more frequently
there is a degree of obliquity in the fracture, and the fragments are
generally detached. A bone may be split longitudinally, as from a
musket-ball striking its shaft in the centre; and fissures often extend
from a cross break to a considerable extent, sometimes into joints.
Swelling is often rapid, from extravasation of blood; at other times it
is slow, and of a serous character. At first it is soft and yielding,
but after a time painful inflammatory tumescence supervenes, the
violence and extent of which will depend on the severity of the injury,
and very much also on the treatment to which the parts are subjected.
If the bones be put as nearly as possible into their original position,
and retained so, judiciously—the limb being laid in a comfortable
and unconstrained posture, and the bandages, splints, &c., properly
adapted—little or no pain or inflammatory swelling will occur; no more
action ensues than is required for reparation of the injury. If, on
the contrary, the bones are allowed to remain unreduced—perhaps after
being well handled—their broken ends, laying among the soft parts, are
pulled out by violent spasms, lacerations of the muscles and vessels is
increased, effusion, swelling, and violent inflammatory action occur,
the pain becomes excruciating, fever and delirium follow; there is an
imminent risk of gangrene, and extensive suppuration among the muscles
is almost inevitable. If the patient recover, the union is bad, and the
limb deformed.
A fracture is said to be simple, where there is no wound of the
superimposed integuments. The external parts may be bruised, or the
deep structure much injured, with laceration of the vessels and rapid
and great swelling; or there may be little or no injury of the soft
parts. Great danger may exist without division of the integuments;
these, yielding under the force, may remain entire, whilst by great and
direct violence the bone is comminuted, the muscles broken up, and the
vessels and nerves torn,—the limb is infiltrated with blood, and must
become gangrenous as soon as reaction takes place. But usually these
untoward circumstances do not exist in simple fractures, the soft parts
being but slightly injured.
Fracture is compound when the integuments are divided by the external
force, so as to expose the broken bone. But the wound may not penetrate
to the bone; and then the accident is termed fracture with wound, not
compound fracture. The soft parts are often divided by the sharp end of
the bone; this is frequently the case in oblique fracture, occasioned
by a fall from a height, the lower fractured extremity being pushed
forcibly upwards. The muscles are usually much injured. The wound is
either large or small, lacerated or clean.
Fracture, simple or compound, is comminuted when the bone is divided
at the broken point into fragments, either small and loose, or large
and adherent to the covering of the bone and other soft parts.
554
Fracture may be complicated with wound or displacement of a
neighbouring joint, and with laceration of large bloodvessels and
nerves.
 Union of divided bones, as of soft parts, is preceded by incited
circulation in the part, and effusion of organisable matter. The
extent of action is regulated by that of the injury, whether inflicted
by accident or by operation. If the soft parts have not been much
bruised, if the bone and its covering are merely separated and slightly
displaced, and then speedily put in contact, the incited action and the
effusion are limited to the divided parts. There is no irregularity
afterwards at the point of fracture, the new matter that is not
required being absorbed soon after deposition; the bone is smooth and
even as before. The deposit of new matter under the periosteum and
into the medullary canal is here well exhibited. By this means only
is the bone kept together for a very considerable period; afterwards
the broken ends are united, and the temporary callus absorbed. If, on
the contrary, there is much displacement, and if that is not entirely
removed, intense action ensues both in the soft and hard parts, there
is great effusion of new matter, or callus, soft and yielding at
first, but gradually becoming hard and dense—bony particles being
deposited from the vessels ramifying in the extremities, or in the
attached fragments, of the old bone. When detached portions of callus
are found lying in the soft parts, a piece of old bone which retained
its vitality has generally formed the matrix of the deposit. When the
ends of bones have been badly placed, and meet each other at an angle
or curve, occasionally osseous deposit seems to form in the concavity.
This increases in size, unites with the portions of the shaft, and
forms a sort of bridge uniting them. This by M. Gulliver has been
termed accidental callus.
Union of divided bones, as of soft parts, is preceded by incited
circulation in the part, and effusion of organisable matter. The
extent of action is regulated by that of the injury, whether inflicted
by accident or by operation. If the soft parts have not been much
bruised, if the bone and its covering are merely separated and slightly
displaced, and then speedily put in contact, the incited action and the
effusion are limited to the divided parts. There is no irregularity
afterwards at the point of fracture, the new matter that is not
required being absorbed soon after deposition; the bone is smooth and
even as before. The deposit of new matter under the periosteum and
into the medullary canal is here well exhibited. By this means only
is the bone kept together for a very considerable period; afterwards
the broken ends are united, and the temporary callus absorbed. If, on
the contrary, there is much displacement, and if that is not entirely
removed, intense action ensues both in the soft and hard parts, there
is great effusion of new matter, or callus, soft and yielding at
first, but gradually becoming hard and dense—bony particles being
deposited from the vessels ramifying in the extremities, or in the
attached fragments, of the old bone. When detached portions of callus
are found lying in the soft parts, a piece of old bone which retained
its vitality has generally formed the matrix of the deposit. When the
ends of bones have been badly placed, and meet each other at an angle
or curve, occasionally osseous deposit seems to form in the concavity.
This increases in size, unites with the portions of the shaft, and
forms a sort of bridge uniting them. This by M. Gulliver has been
termed accidental callus.
In badly reduced fracture the swelling is great and hard. The callus
is exuberant, much being required for the union of the fractured ends
that overlap, and are perhaps far from being in contact; the vascular
action and accompanying effusion are great, according to the necessity
for them. The bone at the united part is enlarged to perhaps double
its original thickness, or even to a greater size. After some time,
the ends of the old bone, and part of the new deposit, are rounded off
by absorption of the protuberances, and the part becomes more shapely.
The canal of the bone and the cancellated texture is again restored.
The accompanying sketch of a section of the humerus shows a double
fracture. The superior one near the neck, where there is still some
thickening, had been555 well adapted, and the canal is quite perfect.
In the other and more recent there is considerable overlapping. The
portion of outer osseous shell projecting into the medullary canal
would in the end have been removed by the absorbents, and the deformity
much diminished.
When the ends of the bone are not well placed, or when they are moved
occasionally whilst the uniting medium is still soft, there is danger
of a false joint being formed—the callus either giving way, or being
all along imperfect, and the extremities at the soft part becoming
smooth and moveable on each other; or incited action may run high and
terminate in suppuration, with death or ulceration of portions of the
bone.
Fragments are sometimes entirely detached at the time of the accident,
and perish at once; or are so slightly connected with the shaft that
they lose their vitality on the first accession of inflammation, become
surrounded by purulent matter, part from their slight attachments, and
come towards the surface. Or the shaft itself may be so bruised by the
violence of the injury as to be incapable of resisting incited action,
though slight. By malpractice, such untoward consequences as the
preceding, and many others beside, are frequently induced.
The uniting medium of separated bones remains soft for some time,
as was already observed; and often, whether from the state of the
constitution, or the circumstances connected with the fracture, the
parts remain long moveable. Pregnancy is said to prevent union; but
I have often seen fractures in pregnant women unite as speedily and
firmly as if the patients had been in that state, and otherwise in
robust health; profuse uterine or vaginal discharges, or determination
to particular parts or organs, will certainly retard union.
In ordinary cases, the limb, if not lying altogether straight, can be
moulded into a proper form after the lapse of eight or ten days from
the time of injury, without the patient suffering any great degree of
pain, without the process of union being at all interrupted, or the
cure protracted; even at the late period of five or six weeks, badly
united fractures may sometimes be much improved by gradual pressure
and change of position. A gentleman fell from his horse, and sustained
simple fracture of both bones of the leg, near the middle. It had been
laid and retained on its side. I saw him exactly six weeks after the
injury; the leg was much curved forwards, and the foot turned outwards.
The limb was placed on the heel, and a long splint, with a foot-piece,
applied on the outside; by attention to its position, and by gradually
tightening of the bandages, it soon became quite handsome. Care should
be taken not to allow the patient to rest too soon on the fractured
limb; for though quite straight, symmetrical, and of the proper length,
when the retentive apparatus is discontinued, it may become short and
deformed in a few days from even slight weight being put upon it.
The period at which firm union takes place varies; the process is more
rapid in young people than in those advanced in life, and will depend
more on the extent of the injury, and its vicinity to the centre of the
circulation than on the size of the broken bone. The requisite556 length
of confinement is regulated by these circumstances, and by the use to
which the part is to be afterwards put; the lower limbs require longer
time for consolidation than the upper.
In the treatment of fracture, as in solution of continuity in the soft
parts, great advantage is gained by placing the disjoined parts as
nearly in their original position as possible, retaining them so, and
allowing of no motion. These indications ought to be accomplished very
soon after the accident; many evils are thus prevented—the further
laceration of the soft parts, the inflammatory effusion into all the
tissues, and the consequent startings and spasms of the muscles. This
cannot be too much insisted on. There is much folly and absurdity in
allowing a broken limb to lie unrestrained—leaving the ends of the
bones displaced, the one riding over the other—whilst attempts are
being made to keep down the inflammation, by applying leeches, cold
lotions, or large poultices—all perfectly ineffectual so long as the
palpable cause of incited action remains unheeded. The circumstances
which kindle and keep up inflammation should always be understood;
they are easily discovered in fracture, and when understood should
never be lost sight of. If the parts be replaced there will seldom be
inflammation; if they remain displaced, the inflammation is so great
that it is impossible to subdue it by any means short of removal of the
cause. There is also an impossibility,—not to mention the patient’s
sufferings,—of reducing bones to a good position some weeks after the
accident. Such practice has been extensively followed and recommended
by some, even modern writers; they set about reducing a fracture at a
period after the accident, at which, by proper treatment, union would
have been completed, or at least far advanced. The confinement and
suffering of the patient are increased threefold, and after all the
cure is bad, and there is a risk of false joint.
In all fractures, whether simple or compound, comminuted or
complicated, if an attempt is to be made to save the limb, let
reduction be immediate; coaptation and retention of the separated parts
cannot be made too soon. A neglected case may be met with, in which
the intensity of inflammatory action in all the tissues may forbid
immediate interference. But even though inflammatory action has taken
place to some extent, there are no surer means of arresting it than
removal of its cause—the irregular ends of the bones being taken away
from among the soft parts—provided it can be done without violence
or increase of tension. Reduction is facilitated by proper position
of the limb, by relaxation of certain sets of muscles. Extension and
counter-extension are made, and but very little force is required;
the surgeon extends the limb with one hand, and resists with the
other; when the system is excited, and the muscles act spasmodically,
an assistant may be required to steady the limb, and to resist the
extending power which the surgeon employs. Then the position of the
limb and of the patient, when long confinement is required, must be
considered, and rendered as easy as possible, though at the same time
secure. The apparatus for retaining the bones in the right position
must be varied according to circumstances.
In compound fractures, when the wound is so small and clean557 that
adhesion readily takes place, the cure is as rapid as in the simplest
form of accident; but when the soft parts are much lacerated, the
breach in them must be repaired by granulation; there will be profuse
discharge from the wound, with risk of deep suppuration, and union of
the bone will be slow. To accomplish reduction, long and sharp pieces
of bone may require to be removed by means either of the saw or of
the forceps, or else the wound must be dilated; both proceedings may
be necessary in some cases. Detached portions of bone, and foreign
bodies, if any, must be taken away; and the edge of the wound may be
approximated when a reasonable chance of adhesion exists. The limb
must then be properly placed and secured. Inflammatory action, should
it threaten, must be kept down, but bleeding and purging are to be
employed with caution. The action and its consequences are moderated
by one or two depletions, but these must not be had recourse to
without due consideration of circumstances; strength is required to
effect the action necessary for union, and to withstand the subsequent
suppurations, though these may be prevented or at least moderated by
timely depletion. Abscesses are to be opened early, the parts are
fomented, and then perhaps poulticed. The limb must all along be kept
in a correct position, dead portions of bone must be removed when
detached, and the strength supported by generous diet and wine. Opiates
are of great use in alleviating the pains and twitchings in the limb.
Poulticing is to be continued only for a short time; in many cases it
may be altogether superseded by fomentations; and the latter should
be used only when abscess is threatened, or when the patient is much
pained at one or more parts of the limb. Support and gentle pressure
are indispensable soon after evacuation of the matter, when no fresh
collection is threatened.
The injury is often so great as at once to demand removal of the
limb. There is no alternative, when, from laceration of the soft
parts, superficial, deep, or both—comminution of the bone to a great
extent—rupture of large vessels—and opening of joints—either gangrene
or an overpowering suppuration are rendered not only probable but
almost certain. The period at which the operation is to be undertaken
requires judicious selection. Some patients are not affected
constitutionally even by great and violent injury, such as dreadful
laceration of the limbs; whilst others, even after slight wounds, are
seized with delirium, tremors, vomiting, lowness of spirits, depressed
circulation, paleness of the surface, and appear on the eve either
of rapid sinking or of immediate dissolution. In the first class of
patients immediate amputation may be had recourse to with safety and
advantage. In the second, the patient must be reassured, and stimulated
both by external and internal means; in short, reaction must be brought
about, and then let the surgeon operate. If he amputate before this,
his patient will most probably die on the table, or very soon after his
removal from it; reaction will never take place, and sinking of the
vital powers be accelerated by the ill judged interference. A greater
or less time is required for the occurrence of reaction in different
individuals; the usual period is from two to six hours. Commencement of
it is a sufficient warrant for operation;558 the surgeon must not delay
till inflammatory fever has been lighted up, for then he will interfere
with great disadvantage. He must then subdue the inordinate action
as much as possible, and wait for the suppurative stage. When the
patient has become hectic from profuse and long continued discharge,
when, perhaps, no union has taken place—then also the limb must be
removed. In civil practice, patients as often recover from secondary as
from primary amputation. But according to the experience of military
surgeons, the result is otherwise—many recover after primary and few
after secondary; much may depend on the accommodation of the patient
afterwards. A great deal must necessarily be left to the judgment,
discretion, and conscientiousness of the surgeon.
Fractures of the cranium were treated of as connected with
disturbance of the important organ which it protects.
The bones of the face are occasionally broken and displaced. The
frontal sinus is sometimes opened by fracture of the external plate. No
small degree of force is required to effect this injury:—I recollect
an instance of it, with opening into the sinus, occasioned by an
attempt at suicide; the man had struck his forehead violently with a
large stone, wishing to knock his head to pieces. The integuments are
generally divided, and, during expiration, blood, sometimes frothy,
is poured out through the opening. When there is no wound of the
integument, emphysema of the forehead and eyebrows has resulted from
disruption of the bones that compose this cavity, or others connected
with the nostrils.
The ossa nasi are fractured and displaced by direct violence. They
may be broken and comminuted without much displacement, or separated
from their connections and depressed without much fracture. Even slight
cases are generally attended with laceration of the Schneiderian
membrane, and with profuse hemorrhage from the nostrils. The soft parts
over the bones are thin and tense, and consequently in many cases
divided. Great swelling is apt to ensue, at first either bloody or
œdematous. Inflammatory swelling to a great extent, both externally
and internally, is to be dreaded and guarded against. Abscess of the
Schneiderian membrane, frequently of the septum narium, occurs from
slight injuries, if neglected; and, if not actively and properly
treated, may terminate in loss of substance and consequent deformity of
the features.
The existence of fracture of the ossa nasi is very readily ascertained;
the part is distorted, being either uniformly depressed, or hollow at
some points, and abruptly prominent and sharp at others. With the view
of remedying deformity produced by displacement, and preventing the bad
consequences already spoken of, the bones must be restored to their
original position. They are to be raised by means of a strong probe
or director, covered with lint, and introduced high into the cavity.
Whilst, by means of this instrument, pressure outwards is made, the
fingers of the surgeon are applied externally, so as to mould the organ
into a proper shape. Unless force be again applied to the part, there
is no risk of subsequent559 displacement; no apparatus is required to
preserve the bones in situ.
In compound fracture the detached spiculæ are to be picked out, and
the wound cleansed of blood and extraneous bodies; its edges are to be
brought neatly together, and retained by one or more stitches, with
slips of unirritating plaster. Inflammatory symptoms are to be warded
off and combated by purgatives, antimonials, local abstraction of
blood, and fomentations. Formation of matter in the nasal cavity is
to be prevented, by scarification of the swollen membrane that fills
the nostrils and precludes the passage of air; and if matter has been
allowed to collect, it must be early discharged.
Opening into the frontal sinus, whether the result of accident or
of exfoliation, may sometimes be closed by paring the edges of the
integuments and bringing them together, or by covering the deficiency
with a flap borrowed from a neighbouring part. Such measures should not
be resorted to, in the case of opening from accident, till after all
inordinate action has subsided, otherwise adhesion will fail.
Cases of fracture of the superior maxilla, os malæ, and zygoma,
have been met with. Great displacement cannot occur, nor is any
peculiarity of treatment required. If the fracture is compound, loose
portions of bone may require removal.
The inferior maxilla is exposed to violence, but from its
construction and consistence is capable of resisting a great degree of
force. It may be broken at various points; the usual site of fracture
is where the canine or the first small molar tooth is implanted; but
it not unfrequently gives way at the symphysis, or near the angle.
The alveolar processes are often detached, with loosening of one or
more teeth. The fracture is frequently compound; being produced by a
direct blow, as the kick of a horse. The bone sometimes breaks at a
part not struck, as at the symphysis from a blow near the angle. The
accident is easily recognised; in fact, the patient, if sensible, has
himself discovered fracture before he applies for assistance. There is
distortion of the part, and the broken extremities, when moved, are
felt grating on each other; there is discharge of blood, perhaps of
teeth, from the mouth; and in compound fracture the ends of the bone
are visible. At the symphysis the parts are not much displaced; they
are more so when the fracture is in the site of the first molar. In the
latter situation it is occasionally difficult to replace the bone, and
retain it in its proper position.
The face swells to a greater or less extent, according to the severity
of injury done to the soft parts, and the time which has elapsed before
reduction. The parts within the mouth swell; often there is great
infiltration of the loose cellular tissue under the tongue. Sometimes
extensive abscess forms, showing itself in the mouth or under the chin.
The bone is to be brought to its former shape by pressure of the
fingers on the outside, and of the thumbs placed within the mouth
on the corners of the teeth. Motion is prevented, and the parts
are retained in their proper situation, by a wedge of cork or wood
interposed on each side of the jaw, and grooved so as to receive the
teeth both above and below. The wedges are placed with their thick560
ends anteriorly, and are retained by the lower jaw being firmly bound
towards the upper; sufficient space for the introduction of food must
be left between the wedges at the fore part of the mouth. Pasteboard or
leather is applied externally, cut so as to fit exactly the fractured
bone; it is previously softened in warm water, that it may adapt itself
to the shape of the parts, and form a case over them; a thin layer of
tow or wadding is placed between it and the skin, and the whole is
retained by a roller, which is preferable to split cloths. The patient
should not talk, or in any way attempt motion of the injured bone,
and the food given should not require mastication. Inflammation is to
be kept down by the usual means, and abscesses, if they form, must be
early evacuated. Detached teeth and splinters of the jaw are to be
extracted at the first; if teeth loosen much during the cure, they
should be considered as foreign bodies, and removed, otherwise they
will keep up the discharge, and tend to prevent union.61 From three
to six weeks is generally sufficient time for consolidation of the
fracture. In severe cases union may be prevented by necrosis of part of
the bone; or, though the bone unite, the external wounds may not heal,
and the discharge may continue till the dead portions separate and are
discharged.
Fracture of the Spinal Column is attended with alarming symptoms,
and often terminates fatally, from the pernicious effects necessarily
produced on the spinal chord, either immediately or consecutively, when
the bones forming the column are disjoined to any great extent. The
injury is effected by great violence—by the body being projected and
alighting awkwardly—by a fall on the breech from a height, the head and
trunk being bent forcibly forwards—by direct blows on the spine.
Displacement of the bones forming the spine, seldom takes place without
fracture to a greater or less extent. Pure dislocation of the spine,
from the rupture of ligaments and fibro-cartilage, is a very rare
accident; few cases of it are on record, and in them the injury was in
the cervical region; I have only met with two instances of complete and
pure dislocation. The ligaments are of great strength, and the bones
yield sooner than they do; and in the greater number of severe injuries
of joints this is the case more or less.
A very well marked specimen of luxation, without the slightest fracture
of the fourth from the fifth cervical vertebra is delineated on the
next page. The injury was occasioned by the person falling backwards
over a high paling, on which he was sitting, and alighting561
on the back of the head: along with the proper ligaments, the spinal
chord is seen to be torn. The patient, of course, did not survive many
days, being almost perfectly paralysed.
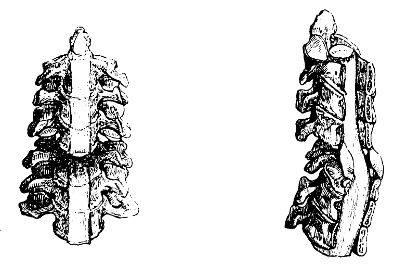
In general, either the bodies or the processes of the vertebræ are
broken, and sometimes comminuted; occasionally the bodies are broken
entirely through, with considerable displacement, the upper or lower
end, as may be, projecting. There is twisting or bending of the trunk
or neck, the articulating processes on one side only being displaced,
whilst the ligaments on the other remain pretty entire. In some cases,
either the spinous processes, or the articular, are separated without
yielding of the bodies of the vertebræ, or of the interposed substance;
then there is bending of the trunk forwards.
The symptoms vary according to the site of the injury, and the extent
of violence inflicted on the spinal chord. This important organ may
suffer concussion without fracture or displacement of the bones; its
functions may be consequently more or less disturbed, and paralysis
occasioned of those parts that are supplied with nerves from below the
injured point. Without fracture, too, vessels may give way within the
canal, and by compression from effused fluid urgent symptoms will be
produced.
The power of motion may be lost whilst sensation is retained, and vice
versâ; but in general both are either impaired or destroyed. In one
case that came under my care, there was power of motion in one limb and
no sensation, whilst in the other there was no motion but the usual
sensation.
Patients may recover from the effects of a severe blow on the
spinal column and consequent concussion of the chord, but very
frequently they do not. Changes may take place at a late period
in the chord or its membranes, in consequence of the injury—as
thickening of the coverings—bloody, serous, or lymphatic purulent
effusion—disorganisation and softening of the medullary matter.
Inflammation of the membranes, or of the chord itself, may supervene,
either very soon after the accident, or long afterwards; its intensity
and562 period of accession will depend on the extent of the injury, and
on the treatment. The muscles act spasmodically, the circulation is
excited, the sensorium and nervous system are disordered, delirium
ensues, and is followed by paralysis and coma.
In some cases of displacement, even to no small extent, the spinal
chord escapes being bruised, torn, or compressed; no bad symptoms may
ensue; or paralysis to a greater or less degree occurs and gradually
goes off, probably occasioned by bloody effusion, which is afterwards
absorbed. This I have witnessed in several instances—in a boy who fell
from a high rock—in a woman who fell from a window; both lighted on the
breech, and the trunk was bent forwards. The lad remained stout, but
his trunk was somewhat deformed by an excurvation; the woman recovered
perfectly. In these cases there was evidently laceration of the
interspinal ligaments, though probably not of the ligamenta subflava,
for the spinal chord must be stretched or otherwise injured when these
are torn.
The chord is more or less injured in the majority of cases of fractured
spine. If the injury occurs high in the cervical region, immediate
death ensues, from compression or laceration of the medulla oblongata.
Respiration is arrested by compression or destruction of the chord
above the origin of the phrenic and other respiratory nerves. If
the chord is injured in the middle of the cervical region, there is
paralysis of the upper and lower extremities, with distention of
the bowels, and inability to void the urine; the lower bowels have
become insensible to the stimulus of distention from want of nervous
influence, and the sphincter ani is paralysed. The bladder becomes
distended, and then incontinence of urine follows; and frequently there
is priapism. The quality of the urine is changed, the secretion of
mucus from the bladder is vitiated and increased. Slow inflammation of
that organ is induced, the urine becomes bloody and mixed with ropy
mucus; lymph is deposited on the lining membrane.
Bruises of the loins often lay the foundation for degeneration and
abscess of the kidney, with many of the symptoms of calculus vesicæ,
attended with red tongue and hectic, ultimately terminating fatally.
The effects of concussion of the spine are frequently developed long
after the infliction of the injury. There is formication, numbness, and
difficulty of regulating the motions, in one or more limbs. Still the
muscles are not shrunk, nor unable to perform powerful movements; but
the patient cannot put his hand or foot to the place he wishes, and
cannot support the weight of the body without assistance. Sensation
in the limbs is lost to a greater or less degree, their heat is
diminished, and it is found difficult to preserve their temperature
equable. The symptoms increase till the limbs become totally useless.
Along with the lower limbs the bladder is affected, though not always.
The urine is not voided with force, and incontinence occurs from
distention. Sometimes excitement of the viscus follows; the secretions
from its surface are increased, and often mixed with blood. Yet
patients survive long under such circumstances, digestion and the
other important functions are well performed, and the intellect is
unimpaired.
563
Prognosis in injuries of the spine is unfavourable, as well as in
disease of the chord, whether the result of injury or not.
From the treatment much need not be expected; but still no chance is
to be thrown away, even in the most unfavourable cases. The attention
must be directed towards alleviation of the symptoms. The comfort of
the patient must be looked to in regard to the situation of the injured
bones and other parts, even where there is reason to believe that the
chord is lacerated or completely divided, and that there is no chance
of recovery. In less severe cases, by placing the injured parts in
their proper position, and retaining them by splints placed along the
sides of the spinous processes;—by keeping down inflammatory action,
palliating all the symptoms as much as possible, and attending to the
state of the bladder if necessary—unlooked for recoveries have taken
place.
 It has been proposed to treat the spine, in cases of severe and
alarming fracture, in the same manner as the cranium—by trephining; and
some have recommended this in almost all kinds of injuries. I allude
to the practice only to condemn it. The spinal chord is generally
displaced and compressed by the lower portion of the fractured body
of the bones. One cannot easily comprehend what an operation is to
effect in such cases. Further notice of this proceeding is unnecessary,
seeing that, as far as I know, it has been unanimously discarded by the
profession from amongst the list of surgical operations.
It has been proposed to treat the spine, in cases of severe and
alarming fracture, in the same manner as the cranium—by trephining; and
some have recommended this in almost all kinds of injuries. I allude
to the practice only to condemn it. The spinal chord is generally
displaced and compressed by the lower portion of the fractured body
of the bones. One cannot easily comprehend what an operation is to
effect in such cases. Further notice of this proceeding is unnecessary,
seeing that, as far as I know, it has been unanimously discarded by the
profession from amongst the list of surgical operations.
When the patient has borne up against the shock of the injury,
and the more immediate consequences, and when partial loss of
sensation and motion has supervened, great benefit is obtained from
counter-irritation, by blisters, issues, or moxa. But these are not
advisable, but to a certainty injurious, till after time has been
allowed for subsidence of the immediate effects—for union of the
divided parts, and disappearance of acutely excited vascular action.
The endermoid application of strychnine is also efficacious in many
cases where the injury has been slight—as in the following. A young man
was struck on the back of the neck with a leaden plummet. The immediate
effects were loss of power and sensation in the whole body. The use
of the upper limbs was regained gradually and completely; and when he
applied to me, the remaining symptoms were diminished sensation and
irregular muscular action in the lower limbs. The mode of progression
was very remarkable; supported on the points of the toes and assisted
by a staff, he made two or three quick steps as if running, and then
suddenly stopped, a few more rapid steps and another abrupt halt, and
so on. A succession of small blisters was applied along the sides
of the spine in the dorsal and lumbar regions,564 On the raw surface
strychnine was sprinkled, commencing with half a grain daily, and
gradually advancing to a grain and a half. He made a perfect recovery
in less than three weeks.
In another patient, in whom sensation in one limb without motion, and
in the other motion without sensation, remained after severe injury of
the spine by a fall from a high window, complete recovery was obtained
by the internal use of strychnine, and repeated application of the moxa.
Slow degenerations of the spinal chord are not easily combated with
success. Considerable changes of structure have taken place, as shown
by the symptoms, before the patient becomes alarmed and applies for
relief. He has had a feeling of distention about the lower part of the
bowels, and voids his urine with some difficulty; perhaps he suspects
stricture of the urethra as the cause. He lifts his feet awkwardly,
sets them down clumsily, and all of a piece; his knees totter, there
is no feeling about his buttocks, and a numbness round the anus. At
length he is for the first time alarmed by incontinence of urine having
supervened, or by the limbs having sunk under the weight of the trunk,
and by his coming to the ground with violence. The remedial means
are local abstraction of blood from over the seat of the disease,
followed by friction and counter-irritation. Strychnine may be tried in
some cases. But it is indeed seldom that the progress of the case is
satisfactory.
Fracture of the Clavicle.—This bone is liable to be broken by
indirect violence, as by falls on the point of the shoulder, from
horseback, or from the top of a carriage; or by a fall with a carriage,
the person being inside—of this accident I have met with three or four
instances. It may also be broken by direct violence, as by a blow on
the bone, or by the person striking it against a hard substance in
a fall. It generally gives way about the middle. The fracture, when
occasioned by force applied to the acromial extremity, is usually
oblique; transverse when the force is applied to the shaft of the
bone. The displacement is in most cases great; but when the fracture
is at the bend near the scapular extremity,—a not very uncommon
accident,—disjunction of the fractured extremities is prevented by
the attachments of the conoid and trapezoid ligaments. In ordinary
cases, that fractured extremity projects which is attached to the
sternum, whilst the scapular portion is depressed and carried inwards.
In short, the scapular portion is displaced, the sternal is nearly in
situ; though, from the depression of the former, the prominence of the
latter appears to arise from displacement. The arm falls forwards and
downwards.
The fracture is sometimes compound. The wound is generally small, and
occasioned by the projection of the sternal portion; or the integument
may be divided by the external force.
The nature of the accident is readily recognised. The deformity is very
apparent. There is swelling, from extravasated blood, over the bone;
the shoulder is unnaturally approximated to the chest, and depressed.
The motions of the extremity, those above the565 shoulder, are impaired.
Crepitation is felt on raising the arm, and carrying it backwards so as
to bring the fractured surfaces into contact.
When the patient is seen immediately after the accident, the bones
are to be placed in apposition, and retained, without delay, and
before inflammatory swelling has come on. No complicated apparatus is
required. A pad, firm, though of soft material, and large enough to
fill the arm-pit completely, is rolled in a shawl and placed in the
axilla; it is retained by tying the shawl over the opposite shoulder,
a soft pad being interposed between the knot and the skin to prevent
excoriation, and is farther secured by tying the ends under the axilla
of the uninjured extremity, which should also be protected by a small
cushion. A few turns of a roller, or a handkerchief, are placed round
the arm and chest, so as to secure and fix the limb; so the retentive
apparatus is completed. The shoulder is thus raised, and removed from
its unnatural position; and the fractured extremities of the clavicle,
previously placed in accurate contact, are prevented from being again
displaced. The elbow and forearm should be supported by a sling,
otherwise the unsupported weight of the limb dragging on the shoulder
will cause considerable pain, and subsequent displacement will be apt
to occur. In order to prevent swelling, it is sometimes advisable to
support by a bandage the hand and forearm. The apparatus should be
looked to occasionally, adjusted and tightened; and the cushions should
be replaced by fresh ones, to prevent excoriation and uneasiness.
The bone will be found to lie quite smooth, to remain of its proper
length, to unite, generally within twenty days, and that without any
unseemly exuberance of callus. No evaporating lotions are necessary.
No compresses or splints need be applied over the bone. If the patient
be bruised in other parts, and become feverish, it may be requisite
to abstract blood and exhibit antimonials, purgatives, &c. But all
inflammation, arising from the fracture, subsides on the accomplishment
of reduction, adaptation, and retention of the portions. If the
fracture be compound, the edges of the wound should be brought together
and retained, so as to favour immediate union.
The body of the scapula is broken, generally by a severe injury of
the chest, as by a hard and heavy body passing over it. There is little
or no displacement; and the accident is not easily detected, more
especially after swelling has taken place.
It is sufficient to restrain motion; and this is effected by passing a
bandage round the chest, over the scapula, and round the arm.
The acromion process may be broken off; but the accident is rather
uncommon. The fracture is produced by direct violence—a blow or a fall
on that point. The spine of the bone also is sometimes broken by a
like cause. Portions of the acromion may be separated along with the
ligaments connecting the clavicle to it, in the accident of dislocation
of the scapular extremity of that bone. The acromion is occasionally
broken into fragments by heavy falls on the point of the shoulder.
566
There is a slight appearance of flattening of the shoulder at first,
and then great swelling. Crepitation is felt by pressing gently and
alternately with the points of the fingers over the fractured part.
The arm requires to be raised and supported by a sling.
Fracture of the Ribs.—One rib, or more, may be broken by injuries
in various ways—by blows of the fist—falls on hard bodies—pressure
on the chest by heavy bodies passing over or falling upon it. They
generally give way anteriorly to the angles, at the most convex point;
but sometimes near the spine or the sternum. At the same time they may
be partially luxated at either of the extremities. The fracture is
generally transverse; occasionally, and rarely, oblique. Sharp portions
are seldom detached. The skin is sometimes divided, but more frequently
the pleura and lungs are torn by the spiculæ projecting internally;
hence effusion into the chest, and emphysema of the subcutaneous
cellular tissue near the fracture, take place. The emphysema, if
permitted, extends over the greater part of the chest, and even farther.
Fracture of the ribs is attended with pain, particularly during full
inspiration; and if the injury is severe, the patient is incapable,
without great pain and exertion, of accomplishing full inspiration. He
uses his handkerchief, sneezes, and coughs, with the utmost difficulty.
Crepitation is felt by the patient, and is easily detected by the
surgeon, by placing the hand on the suspected point, and desiring the
patient to attempt full inspiration so as to grate the surfaces on each
other. Motions of the trunk, and often of the upper extremities also,
are attended with aggravation of the symptoms. In some cases attentive
examination is necessary to discover crepitus—in certain situations,
and when perhaps one rib only has given way, especially if some time
have elapsed betwixt the infliction of the injury and the application
of the patient for relief.
In the slighter cases, it is sufficient to restrain the motions of the
chest by a broad bandage applied firmly round it; and a split cloth,
or a scapulary, may be passed over the shoulders and attached to the
circular bandage to prevent its being displaced. Great and immediate
relief is thus afforded. In those of a plethoric habit, blood may
be taken from the arm, some hours after the injury, with relief and
advantage; it may ward off an inflammatory attack—and it is absolutely
necessary to adopt this practice on the slightest indication of
such supervening. The appearance of the countenance, and the state
of the pulse and respiration, must be watched; and on the first
becoming anxious, the second strong and accelerated, and the third
hurried and imperfect, active measures must be employed—venesection,
antimony, purgatives, diaphoretics, anodynes—one or all according
to circumstances. In the more severe injuries the same practice is
pursued; and the symptoms are watched with great care. The air in
the cellular tissue, if effused in great quantity about the neck
and face, and interfering with the functions of the parts, is to be
evacuated by punctures. If the emphysema is slight, and confined to the
neighbourhood of the injured part, farther extrication is prevented
by the timely and accurate application of a bandage; the air567 already
in the cellular tissue speedily disappears. The effusion into the
chest is also in general absorbed; but it may remain and increase,
and from violence of action purulent secretion may be mixed with the
serous. The breathing then becomes embarrassed, the chest swells, and
the integuments are œdematous. The action of the lung is either much
impaired or entirely arrested, as is ascertained by auscultation. In
such circumstances, evacuation of the effused fluid may be required.
The Sternum is sometimes fractured, or, in young persons, the bones
composing it disjoined; but the occurrence is exceedingly rare. The
displacement is not great; and is rectified by changing the position of
the trunk. The same treatment is required as for fracture of the ribs.
Abscess has formed under the bone, as the result of the injury; but
by antiphlogistic means, local and general, this may be in most cases
prevented.
Fracture in the vicinity of the shoulder-joint requires to be most
accurately examined, that a correct diagnosis may be formed, and the
practice be judicious and decided.
Portions of the upper part of the humerus are torn off, along with
the attachments of the short muscles, during violent exertions,
particularly if the limb is in an awkward position. This is followed
by want of power, great swelling, and considerable deformity. Some
indistinct crepitation is perceived; the articulation is afterwards
stiff, and the bone of an unnatural form. But these indications of the
injury gradually disappear.
More extensive solution of the continuity of the bone takes place,
generally in consequence of a direct and violent blow on the shoulder.
The patient is unable to raise the arm, though with great pain it
can be placed in any position that it occupies naturally; it can be
abducted and raised, perhaps to a greater extent and more readily
than when sound. The shoulder is flattened, and the limb apparently
lengthened. The elbow is readily put to the side. On raising the
humerus, rotating it, and moving it to and fro, crepitation is
distinctly perceived—but not so readily after swelling has taken place.
The swelling also obscures the appearances observed immediately after
the infliction of the injury,—the flattening of the shoulder, and
apparent elongation of the arm. By the fingers of one hand, pressed
deep into the axilla, the head of the humerus can be discovered; and,
on rotating the shaft of the bone with the other hand, grasping the
elbow and pushing upwards at the same time, crepitation is perceived,
and the upper portion of the bone is ascertained to be unaffected
by the rotation of the shaft. The nature of the injury is then
sufficiently apparent.
But the shaft of the humerus may, by such manipulation, be ascertained
to be entire. Still, from the direction of the force which effected the
injury, the flattening of the shoulder, the remarkable falling down of
the arm, the loss of power, the free motion, and from the crepitation,
though perhaps indistinct, it is evident that fracture has occurred.
Then, by the fingers in the axilla, whilst the humerus is raised and568
moved in different directions, crepitation is recognised deeper and
less distinct than in the former case; and the surgeon is warranted
in believing that the glenoid cavity has suffered—that it is broken
into fragments, or that it is separated from the body of the scapula
by fracture of its neck; he is also warranted in adopting the means
of cure suitable to such an accident. Many such injuries are supposed
to occur, yet it is strange that preparations illustrative of it are
scarcely to be met with in our collections of morbid specimens.
How both detachment and luxation of the head of the humerus should
occur, can scarcely be explained. Luxation certainly cannot take
place after fracture; no force can be applied to the head of the bone
sufficient to displace it. It is barely possible, that after luxation,
force may be applied to the bone so as to fracture its neck. This
accident is of very rare occurrence, though by some supposed to be
otherwise. I have had an opportunity of examining but one case, and
that was very distinct; the head of the bone, completely detached from
the shaft, lay in the axilla. Comminution of the head of the bone, with
displacement of the fragments, is not uncommon.
Separation of the head of the bone occurs occasionally in young
persons, presenting the same appearances and symptoms as fracture of
the neck of the humerus in later life. Each, by a little care, is
distinguishable from dislocation, even after swelling has supervened.
And it is highly necessary that the diagnosis should be correct and
prompt, otherwise atrociously cruel and unnecessary proceedings will
be adopted, and irreparable mischief occasioned. Luxation is attended
with flattening of the shoulder and elongation of the arm, to a greater
or less degree, according to the position of the head of the bone. But
the elbow does not come to the side, and the motions of the limb are
abridged; it cannot be abducted to any extent, if the scapula is fixed.
The head of the bone is felt under the pectoral muscle, or in the
axilla; and on rotating the arm gently, by laying hold of the forearm,
and using it, when bent, as a lever, the head and shaft are found
to move simultaneously, all of a piece, and no crepitation is felt.
Besides, the history of the accident is an excellent guide towards
correctly ascertaining the nature of the injury. If the patient, in
falling, have involuntarily stretched out his arm, in order to save
himself, and alighted with his whole weight on the palm or elbow,
dislocation will most probably have occurred. If, on the contrary, he
have pitched upon the shoulder, without any intermediate breaking of
the fall, fracture is to be expected.
The evil consequences of false diagnosis, and of treatment formed
thereon, are very apparent. A dislocation may be put up and treated
as a fracture, perhaps till too late for reduction; and the patient
will possess but weak and imperfect motion of the limb, after having
undergone long suffering. On the contrary, dreadful torments are
inflicted on the patient when fracture is treated as luxation. The
force applied with the view of reduction is in all circumstances very
painful, but, when exerted on a fractured bone, must prove absolute
torture; and during the whole treatment, the fragments are, perhaps,
every now and then, by renewed attempts, torn separate, and union so
prevented. Severe inflammatory action fol569lows the reductive violence,
and is kept alive or regenerated by the loose and projecting fractured
ends of the bone; extensive suppurations, attended with fever, ensue,
and may destroy the patient. Undetected fracture may also be treated
as a bruise of the soft parts only; then every motion of the body and
limb is productive of excruciating pain, and there is much risk of
uncontrollable inflammation being excited—all which would have been
warded off, by placing the bones in a proper and steady position in the
first instance; the adaptation of a pad in the axilla is followed by
immediate and great relief. Such mistakes are quite inexcusable. By one
careful examination,—productive no doubt of considerable uneasiness to
the patient in some conditions of the parts—the real state of matters
should be ascertained; and then the practice founded on the knowledge
so obtained will be followed with speedy cessation, or at least great
diminution of pain, and with every probability of restoring the limb to
strength and usefulness.
Fractures of the glenoid cavity, of the neck of the scapula, and of
the neck of the humerus, are all treated by the same simple, though
effectual, apparatus as employed for injuries of the clavicle. It
requires to be re-adapted occasionally, to have the parts under the
crossings of the bandage, and under the knots of the shawl retaining
the pad, well protected by soft pads, and it must be worn for four
or five weeks—perhaps, in some cases, even a short time longer.
Then gentle passive motion of the limb is to be employed, gradually
increased as the painful feelings abate. If the parts are at once
placed in apposition, and accurately retained, no abstraction of blood,
either general or local, is required at the time, and is not likely to
be called for during any stage of the treatment. No cold evaporating
lotions are necessary; fomentations are sometimes useful.
Fracture of the shaft of the humerus is either oblique or transverse,
according to the direction of the force applied. There is considerable
displacement. The limb is always shortened to a certain extent, and
the natural contour destroyed; the arm is useless, and bent towards
the trunk, and the muscles are in a state of spasmodic contraction.
The nature of the injury is at once and readily recognised. There is
unusual and unnatural mobility of the arm, and distinct crepitation
at the fractured point. There is great pain from the pressure of the
lower extremity of the bone upon the nervous trunks. The large vessels
are seldom torn—though the branches of the humeral artery, and the
vessel itself, have in a few cases been ruptured—but there is often
considerable bloody swelling in this as in all fractures. Occasionally,
when the violence has been great, either the upper or the lower
fractured end is thrust through the skin.
When the inferior part of the shaft is broken, there is less
displacement than when the fracture is towards the middle of the bone.
Fracture above the condyles sometimes extends through them; and the one
may be detached from the other either with or without fracture of the
shaft. When such an accident is suspected, the position of the condyles
in regard to the ends of the bones of the forearm should be accurately
observed. Flexion and extension of the forearm570 can be readily
performed, though with pain; not so, when the bones are luxated.
Crepitation is detected along the line of fracture, during motion of
the limb, and when the condyles are laid hold of and moved upon each
other, or on the shaft.
In fracture of the middle of the shaft, coaptation is easily
accomplished; slight extension is made by one hand grasping the
elbow, whilst, by the other, the bones are brought together, and the
straightness and outline of the limb restored. The proper position is
readily maintained by two splints of bookbinders’ pasteboard, or of
leather prepared for the purpose; one applied from over the acromion
process to beyond the point of the elbow, the other from the axilla,
and also passing over the elbow on the inside; thus the neighbouring
joints are fixed, and the muscles rendered inactive. The conjoined
breadth of the splints should be sufficient to embrace the limb almost
entirely; some space being left, so that when the swelling subsides,
they may neither meet, and consequently lie loose, nor overlap each
other. They are softened by steeping in hot water, so that they may
embrace every part of the limb to which they are applied; and the
extremities should be rounded off, to prevent galling of the parts.
They are padded with soft flannel, lint, or cotton wadding, or, what
is better, with finely carded tow, and retained by a circular roller
applied from the points of the fingers up to the shoulder. The binding
should proceed from below upwards, to avoid swelling from obstructed
circulation, and do away with the necessity of removing the apparatus
arising from this cause. It is well to place a wooden splint on the
outside, retained by an additional bandage, so as to steady the parts
till the pasteboard or leather has dried, and formed a firm mould or
case for the limb; then the wood is no longer necessary, and should be
removed. The forearm is bent at right angles, and the humerus fixed
to the trunk. In simple fracture, there is in general no necessity
for interfering with the apparatus until the bandage slackens, in
consequence of the swelling subsiding; then, usually at the end of
eight days, it is to be reapplied. One splint is carefully raised,
whilst the other is kept fixed and the parts steadied, and the limb is
ascertained to be straight and of a proper length; if not, then, or
even later, the position of the bones may be rectified without causing
much uneasiness. The patient need not be confined to bed on account of
a simple fracture; he may walk about with the arm supported in a sling.
In compound fracture similar splints are applied, after due attention
has been paid to the wound and to the position of the bones. The
patient is placed on his back in bed; and the splints are retained by
slips of bandage, double, one end being passed through the loop and
secured to the other by a running noose. This method of deligation
affords facility for the removal of the splints, in order to examine
into the state of the limb and dress the wound. It also permits the
apparatus being slackened in the first instance during the swelling,
and of being afterwards tightened, without lifting the limb or
disturbing its position.
Fracture at the distal extremity of the humerus is managed most
conveniently with the limb in the straight position. The fragments571 are
placed accurately together, and one splint placed on the fore part,
another posteriorly. The forearm is kept in a state of supination. At
the end of about twenty days the apparatus should be removed, and the
position of the articulation changed if possible. The forearm is to be
bent slightly, and a splint applied,—made to fit accurately, and with a
joint corresponding to the bend of the arm. This should be occasionally
removed, provided consolidation of the fractured bones has advanced so
far as to admit of it, and slight passive motion of the elbow-joint
employed. Obstinate rigidity of the parts is thus guarded against.
Fracture of the condyles has been already alluded to. It may be farther
observed, that the exact nature of the accident is often difficult to
detect; in all cases accurate and careful manipulation is required.
Displacement of one or other of the bones of the forearm almost
uniformly attends this fracture, sometimes rendering diagnosis obscure.
Fracture of the olecranon process of the ulna is occasioned by
falls on the point of the elbow; or the bone may be snapped asunder
by powerful and sudden action of the triceps extensor cubiti, when
the arm is much and quickly bent. The injury is readily recognised;
there is inability to extend the forearm by its own muscular powers,
a considerable space is felt between the separated portions of the
bone, and the upper fragment is moveable as well as detached; these
marks of the injury are rendered more conspicuous by bending the joint.
Crepitation is produced by moving the limb when extended, and the
separated parts thereby approximated. Bloody swelling soon takes place,
large and extensive when bruising of the soft parts has been great—and
this is usually the case, in consequence of the injury being almost
always the result of direct violence. In some cases the process is
comminuted.
Compound fracture is rare, and likely to be productive of serious
consequences. I have treated and witnessed several cases. In one the
process was cut off by the patient falling out of bed on an earthenware
vessel, which broke under the limb. The joint is necessarily opened.
Violent inflammation soon commences, and can very seldom be kept
within moderate bounds. Discharge of increased and vitiated synovial
secretion takes place, followed by profuse and unhealthy suppuration.
The cartilages ulcerate, and then the bones. The cellular tissue
around becomes infiltrated, the parts swell and are discoloured,
and collections of matter form probably at more points than one;
perhaps there is a succession of abscesses. The condyles, and often a
portion of the shaft of the bone, are denuded by the suppuration, and
superficial necrosis results. Ultimately the patient grows hectic.
Amputation had to be resorted to in three of the cases which have come
under my observation, at the end of some weeks or months from the
receipt of the accident.
Union of the simple fracture will take place by bone, if the portions
be retained accurately and permanently in contact; but there is a risk
of the joint remaining stiff, and of re-separation being produced572 by
even slight violence. Union by ligament is as rapid as that by osseous
matter; and if the ligament is short, the arm is quite as useful.
Approximation of the broken surfaces is favoured by extension of the
elbow-joint, the triceps muscle being thus relaxed. The limb must not,
however, be but perfectly straight. The position is preserved by a
splint placed on the fore part of the limb, extending from the middle
of the arm to the lower part of the forearm, and retained by a roller
applied, not over-tight, from the fingers upwards. The application
of apparatus to the separated portion, with the view of forcing it
into contact with the shaft of the ulna, is useless. The figure of
8 bandage, and such like, are hurtful. Permanent relaxation of the
triceps, with prevention of motion, is sufficient. This is continued
for three or four weeks; by that time the fracture will in all
probability have united, and then gentle and gradual passive motion of
the joint is to be commenced.
In compound fracture the prognosis is always unfavourable. Means must
be taken to avert incited action—the limb must be properly placed
without delay, the edges of the wound accurately approximated, and
antiphlogistic measures pursued. Purulent collections must be opened
early. Rest of the joint is to be insured, and support afforded, by
bandaging and by the application of a splint. The patient will be
fortunate if he escape mutilation by the amputating knife; but when the
wound is trifling, and the parts not much lacerated or bruised, and
the treatment carefully conducted, a cure may be effected by the same
process as the simple fracture.
Fractures of the bones of the forearm, of one or both, are common;
generally simple. The Radius may be broken at various points—at the
upper part—near its head—at the middle—most frequently near the distal
extremity. At the two first points the fracture will probably have
been produced by direct violence; but near the carpus, it is usually
the result of force applied to its extremity, as by falls in which the
weight of the body is thrown on the palm of the hand. The ulna is
usually broken by force directly applied, as when the arm is brought in
contact with hard bodies in falls. By direct violence also, both bones
may give way about the middle, and at corresponding points: or, when
force is applied in the direction of the bones, the ulna may be found
broken near the wrist, and the radius near the elbow.
When one bone is broken, there is little displacement. The power of
motion is lost to a considerable degree, and there is some deformity,
but little or no shortening. The existence of fracture is ascertained
by tracing the bones with the fingers, and by gently rotating the limb;
the broken portions moving on each other produce distinct crepitation.
When the radius is broken near its middle, the forearm is kept
pronated, and the broken extremities are drawn towards the ulna; by
bringing the limb towards the supine position, the ends come together,
and the one bone is removed from the other. Fracture of the radius near
or through its distal extremity produces displacement of the wrist,
with great deformity; and this is increased573 by bloody effusion into
the sheaths of the tendons, and into the superficial cellular tissue.
In fracture of both bones, there is much deformity and shortening of
the limb; the power of moving the hand is lost; the muscles are bruised
and torn, and great swelling soon results.
There is little difficulty in remedying the slight displacement which
takes place when but one bone is broken, and in retaining the parts
in a favourable position. In children, occasionally, one of the bones
of the forearm is broken, the other being bent very considerably, so
as to cause great deformity.62 When both have given way, slight
extension is required, and the forearm is placed in the middle state
between pronation and supination. Two pasteboard splints, softened in
hot water, and padded with tow, are applied, one on each aspect, from
a little above the elbow to over the fingers; the outer should extend
to the tips of the fingers, the inner need not pass the palm; they are
retained by a roller. In fracture of both bones, a wooden splint should
be retained on the outside of the limb for a few hours; 574but this
precaution is scarcely required when but one has suffered. Similar
treatment, along with attention to the wound, is required in compound
fracture.
The metacarpal bones and phalanges of the fingers are subject to
fractures, both simple and compound. The metacarpal bone supporting
the little finger most frequently suffers from force applied to the
knuckle, as in pugilistic encounters. The other metacarpal bones are
occasionally broken from crushing of the hand, as by a heavy body
falling on it, or by its becoming entangled amongst machinery. The
injury is readily ascertained by moving the fingers, and pressing in
the course of the bone. On laying hold of the distal end of the bone
suspected to have given way, placing the fingers over the shaft, and
attempting slight motion, distinct crepitation is perceived. For the
cure, motion of the parts must be prevented for a sufficient time,
and inflammation warded off when threatened; there is a little or no
displacement, and consequently retentive apparatus can be almost wholly
dispensed with.
Simple fractures of the phalanges are recognised and treated by even
the most unlearned in the surgical profession. The deformity is so
striking as to render mistakes as to the nature of the accident
impossible; reduction is accomplished without difficulty; and the bones
are kept in their proper places by a small splint, either of wood or
pasteboard, placed on each side of the finger, and retained by a narrow
roller fixed by glue or starch.
Compound fractures of the phalanges are almost uniformly followed
by most violent inflammatory action in all the tissues, terminating
in disease of the joints, and in death of the tendinous and fibrous
tissues. The suppuration is profuse and unhealthy, and the infiltration
of the soft parts extensive. The diseased action not unfrequently
pervades the palm of the hand. In the great majority of cases,
necessity for amputation arrives sooner or later.
Fracture of the bones composing the pelvis occasionally takes place,
but can be produced only by the application of great force, as by
a loaded vehicle passing over the body, or by a fall from a great
height. The accident is usually attended with serious injury of the
viscera contained in the pelvic cavity, or in that of the abdomen;
they may be either ruptured, or lacerated by sharp projecting spiculæ,
or merely bruised. The nature and extent of the injury is not easily
ascertained. There is great pain on motion of the body or of the limbs,
and usually extensive extravasation of blood in the soft parts; these
circumstances, along with the symptoms that may arise from internal
organs which have been injured, and a knowledge of the way in which the
injury was inflicted, lead to a strong suspicion of fracture of the
pelvis.
A portion of the crest of the ilium may be broken off, without serious
mischief ensuing, and may unite favourably. More extensive fractures,
deeper in the pelvis, as in the neighbourhood of the acetabulum, are
attended with excruciating pain on the least motion; in these the
existence of fracture may be suspected from the first, but575 the extent
of the injury is not fully known till after death. Fractures near the
symphysis, and of the rami, either of the os pubis or ischium, are
usually attended with injury to the bladder or to the urethra. Wound of
the bladder is almost necessarily fatal; extravasation of urine, with
all its fearful consequences, taking place in the loose cellular tissue
connecting the upper part of the viscus to the parietes of the pelvis,
and in the cellular tissue behind the peritoneum. The urethra may be
lacerated by the sharp edge of fractured bone, or it may be ruptured
by direct violence applied to itself. The latter case sometimes
accompanies partial diastasis of the symphysis, produced by the person
falling astride on a beam. Either injury separately is sufficiently
dangerous, and a patient with both is in a very precarious situation.
Great extravasation of blood takes place in the perineum, scrotum,
penis, and tops of the thighs, infiltration of urine quickly follows,
retention supervenes, abscesses form, and the patient perishes under a
train of symptoms already detailed when treating of the urinary organs.
The treatment is seldom satisfactory. Absolute rest must be procured,
and with this view the limbs are to be secured, and a broad band
passed round the pelvis. The state of the viscera must be attended
to; collections of matter must be evacuated; and all other untoward
symptoms must be actively met, and their consequences either adverted
or got over as far as possible.
Fracture of the Sacrum is uncommon, as also detachment or fracture of
the Coccyx. The former accident happens in consequence of a fall from
a great height. There is little or no displacement whether the fracture
is transverse or longitudinal; sometimes there is splintering of the
bone. Acute pain is occasioned by motion of the limbs and of the trunk,
and by pressure over the injured part. Abscess is apt to follow, both
under the integument, and in the concavity of the bone, and the chief
duty of the surgeon is to prevent this if possible.
Fractures of the Thigh.—On account of the thick muscular covering,
much attention is required to enable the surgeon to form an accurate
diagnosis regarding the effects of an injury of the upper part of
the femur. The necessity for ascertaining what the injury really is,
need not be insisted on. Consequences dreadful to the patient have
too often followed blunders in diagnosis. As in the accidents of the
shoulder-joint, some idea as to the exact injury may be formed by
ascertaining how the force was applied; but this, alone, may sometimes
mislead. Careful manipulation is to be chiefly trusted to.
Fracture within the capsule is met with most frequently in those
of advanced age, when the form of the neck of the bone has been
altered,—when it has become shorter, and attached less obliquely to the
shaft, as is sometimes the case; the bones, too, are then more brittle
than in earlier life. The accident often happens from slight force,
applied either to the farther end of the bone or to the trochanter, as
by a fall in going up or down stairs. Though the height often be not
great, yet the patient’s energies are weakened, he can make no576 effort
to break the fall, and the weight of the body is thrown on either the
fore or the back part of the trochanter. Though the fracture, in such
an accident, generally extends beyond the capsule, and the processes
are broken to a greater or less extent, yet occasionally the head of
the bone is separated by transverse break of the neck without farther
injury. This fracture occurs sometimes in those of middle life; and
even in children, separation of the head of the bone may on good
grounds be supposed occasionally to take place.
The marks of fracture within the capsular ligament are inability to
move the limb, pain about the joint on attempts being made to move it,
and shortening to a slight extent, as ascertained by comparison with
the sound limb; the patient being laid straight on his back, with the
crests of the ilia in a line, either the knees or the ankles are looked
to, and the comparative length of the limbs thereby observed. In some
cases, neither shortening nor deformity is apparent for some time after
the accident; there is merely want of power, and crepitation produced
by rotation; but retraction of the thigh would after a time inevitably
occur, and has done so when the nature of the injury was not at first
ascertained, nor proper treatment adopted. Most frequently there is
eversion of the toes, and to a considerable extent; sometimes there
is inversion, and this is owing to the limb either having been placed
in that position in falling, or having acquired it after the injury
has been inflicted. The rotators outward are the more powerful; the
limb naturally inclines outwards, and when in the recumbent posture,
the weight of the foot favours eversion. But in fracture the muscles
do not act as in a sound limb; and when the limb is once placed, the
patient will not by his own efforts alter the position. Thus it is that
inversion not unfrequently happens in this form of fracture, although
the opposite state is that which, from a consideration of the muscles
involved, is à priori to be expected. In inversion the limb presents
somewhat of the appearance arising from the most common luxation; but
it possesses greater mobility, and has not the want of prominence
occasioned by displacement of the articulating extremity of the bone.
The facility of lengthening the member, and the crepitation felt on a
proper and more attentive manipulation, will remove all doubt.
On examining the injured hip, motion to some extent can be effected,
though with excruciating suffering to the patient. On stretching the
limb to its original length, and then rotating slightly, crepitation
can be felt by the hand, or heard by the ear, placed over the
trochanter major.
Fracture is much more frequently met with outside of the capsular
ligament, generally passing obliquely through the trochanters, and
communicating with fissures in various directions. Splinters are often
detached, and sometimes the small trochanter is broken off. Here, also,
there is inability to move the joint, violent pain on attempting it,
swelling and deformity of the member; there is shortening to a greater
extent than in the fracture within the capsule; there is free motion
in all directions; rotation, abduction, adduction, flexion, and often
extension, can be effected to an unnatural and unusual extent—the
degree of motion is no longer limited by the ligamentous577 attachments
of the head and neck of the bone. Here, also, the limb is most
frequently everted, but occasionally inverted; and that even when, from
the direction and extent of the fracture, neither the rotators outwards
nor the rotators inwards have been deprived of the power of acting.
In some cases of fracture, partly within and partly without the
capsule, all the usual marks of this injury are present, but it is
impossible to move the limb without employing considerable force. This
arises from the broken portions being jammed together, the neck of
the bone being, as it were, driven into and wedged in the cancellated
texture of the trochanter major, or of the upper part of the shaft.
The trochanter major is sometimes, though rarely, detached, without
separation of the neck of the bone from its shaft. In this injury there
is apparent lengthening of the limb, and flattening of the hip; the
patient is able to use the member, though not freely. Before swelling
has taken place, crepitation can be perceived on laying hold of the
trochanter whilst the limb is in motion; and the trochanter itself is
found to be in a slight degree moveable.
Fracture of the upper part of the shaft is attended with immediate and
great shortening; the limb is much misshapen, and lies on its outer
side, with the knee partially bent. The upper fragment of the bone
projects; the resistance to the action of the psoas and iliacus is in
a great measure done away with, consequently these muscles raise the
upper, whilst the lower end falls back and is drawn upwards behind
the other. In mismanaged cases, I have found on dissection the lower
end of the bone lying in the sacro-ischiatic notch, and a process
advancing very different from reparation—necrosis. The marks of this
accident are so conspicuous, that the surgeon is satisfied of what has
happened without enquiring for crepitation. Rapid and great swelling
takes place, if reduction and coaptation are not soon resorted to;
the bloodvessels are torn more and more by the ends of the bone, and
effusion of blood into the intermuscular cellular tissue is easy. Very
soon more extensive and dangerous swelling takes place, the result of
inflammatory action, accompanied with startings of the muscles and
greater retraction of the limb.
Fractures of the middle and lower thirds of the bone are not attended
with such great risk, and are more manageable in every way. There is
less disfiguration—the ends of the bone are not drawn by the action of
the muscles so far apart. The fracture is either oblique or transverse,
according to the direction of the force applied; and the bruising and
the degree of swelling are also dependent on the same circumstance.
From transverse fracture fissure sometimes extends, separating one or
other condyle.
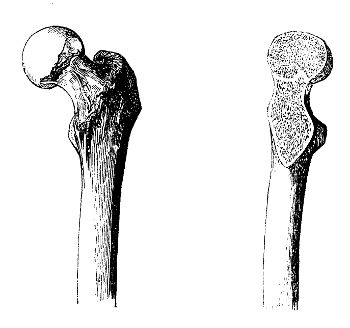
The reparation of injury in the upper part of the femur is opposed by a
variety of circumstances. Fractures of the neck of the bone are almost
uniformly met with in those whose powers of life have been nearly
exhausted. The whole injury is confined within the synovial capsule,
and the fibrous tissues which support that are unyielding, and but
slightly vascular; consequently, in fracture of the neck of the femur,
there occurs none of the swelling and increased vascularity of the
surrounding tissues, which follow fracture of other578 bones, or other
parts of this bone: no temporary callus can be formed; from this
cause, support of the disunited parts is deficient. The head and neck
of the bone are not so well supplied with bloodvessels as the other
parts; those arteries which pass along the ligamentum teres are the
chief support. And perhaps the influx of blood is not increased, in
consequence of injury, to such a degree as in other parts; in these,
when the surrounding parts are bruised or otherwise injured by fracture
in their immediate vicinity, their vascular action is soon excited,
the vessels ramifying on the periosteum are enlarged, and blood is
poured into the bone at all points. Instead of these salutary changes,
the secretion of synovia is increased, and a fluid, perhaps vitiated,
surrounds the bone, and is interposed betwixt its ends. There is also
difficulty in performing accurate adaptation of the broken ends, and
in securing retention so long as is necessary for union; the limb has
a tendency to retraction; in readjusting the apparatus, when become
loose, the broken surfaces are rubbed on each other, and thus any union
which may have been in progress is interfered with. In consequence of
all this, union seldom takes place by bone; it has occurred, and will
occur, in favourable cases, when the fibrous investment of the neck
of the bone does not happen to be torn, and under good treatment. Two
sketches which, through the kindness of Sir Astley Cooper, I am enabled
to introduce here, show the union complete: the patient from whom this
was taken had received other severe injuries, and very little attention
had been paid to that of the hip. But it is an undeniable fact, that
the circumstances which of a necessity follow fracture at this point
are inimical to its effective reparation. The broken ends are sometimes
united by fibrous tissue. Most frequently no union takes place, and the
broken surfaces gradually become smooth, polished like a bit of china,
and adapted to each other; a false joint is formed, but at the579 same
time the capsular ligament, and tissues exterior to it, are thickened
and strengthened, and so the unnatural motion is limited. The rough
and irregular portions of the bone are absorbed, and the neck of the
femur, from interstitial absorption, almost disappears; its diminished
head lies in and is attached to the cotyloid cavity, and is rubbed
upon by the opposed surface of the shaft. Shortening of the limb is
an inevitable result: at first the power of motion is slight, and the
support afforded to the body weak; in course of time the member becomes
strong and useful.
Many bones are preserved and exhibited, in which fracture of the neck
of the thigh-bone, with bony union, is supposed to have taken place;
but there are strong grounds for suspecting that many such have not
sustained actual fracture. The neck of the bone may be shortened,
and set on awkwardly, and there may be masses of new osseous deposit
round the neck and the trochanters. Perhaps the history of the case
is known.—An old person sustains an injury of the hip by falling,
or by a blow on the trochanter; great lameness ensues, and, after a
confinement of many weeks, the patient begins to use the member, which,
however, remains considerably shortened. But all this may have taken
place, and on examination after death, the parts may have presented the
appearances above alluded to, without any fracture. The change in the
bone is the consequence of diseased action induced by the injury. The
bloodvessels of the bone and its coverings are excited, and new osseous
matter is formed at various points; at the same time, interstitial
absorption of the cancellated texture of the neck gradually advances,
and the bone is consequently altered in length and form. These
appearances alone, therefore, do not warrant the confident belief of
fracture having occurred, even though the history should seem to favour
the assumption. And it ought to be recollected, that mere bruising of
the parts about the hip is not unfrequently attended with inability to
move the limb, with eversion of the foot, so as to relax the muscles
which have suffered, and sometimes with slight apparent lengthening.
This change in the form of the head and neck of the thigh-bone is not
found only in old subjects. Some drawings from patients under forty and
fifty years are given at pages 87 and 88, exhibiting in a remarkable
manner this deformity.
In many patients advanced in life, who have sustained fracture of the
neck of the femur, there is little, if any, chance of union. In these
cases, the application of apparatus with the view of adapting and
retaining the parts, is productive of great annoyance, and is apt to
produce either ulceration or sloughing of the integuments at various
parts; and confinement to one constrained position for a considerable
time has a mischievous effect on the general health. Instead, the
limb is placed in the easiest posture, either extended and slightly
retained, or bent over a double inclined plane formed by pillows,
with the knee of the affected side fixed to the opposite; a broad
band is passed round the trochanters and pelvis, so as to restrain
motion without causing inconvenience; and when pain about the thigh is
troublesome, fomentation may be used. After some weeks, when the uneasy
feelings have subsided, the position is580 changed, the patient is set
up, and encouraged to move about, supporting the weight of the body
upon crutches.
In more favourable subjects, whether the fracture is suspected to be
without or within the joint, either entirely or partially, the broken
surfaces are to be brought in contact, and retained immoveably in
apposition for a time sufficient to admit of union. The limb is put
up in apparatus not requiring removal, and but little readjustment.
This can be effected only in the extended position. Many splints,
with foot-boards, straps, and screws, are intended for this purpose,
some to be attached to the injured limb, others to the sound one; but
the apparatus which is most simple, and easily procured at all times
and in all circumstances, is at once the best and the most efficient.
This is a straight wooden board, not too thick to feel cumbrous, and
not too thin to be pliable or easily broken; in breadth corresponding
to the dimensions of the limb, in length sufficient to extend, from
two, three, or four inches beyond the heel, to near the axilla, deeply
notched at two places at its lower end, and perforated by two holes
at the upper. The splint, well padded, is applied to the extended
limb, the ankles being protected by proper adjustment of the pads.
The apparatus is retained by bandaging. A common roller is applied
round the limb, from the toes to near the knee, so as to prevent
infiltration, which would otherwise follow pressure above by the rest
of the apparatus. The splint is then attached to the limb by involving
both in a roller from the foot to above the knee; and in doing this,
the bandage, after having been turned round the ankle, should be passed
through the notches, so as to be firmly attached to the end of the
splint, thereby preventing the foot from shifting. A broad bandage is
applied round the pelvis over the groin, and down the thigh, investing
all that part of the limb left uncovered by the previous bandaging. A
broad band, like a riding belt, is fastened round the pelvis, so as to
bind the splint to the trunk, and thereby keep the broken surfaces of
the bone in contact. A large handkerchief, or shawl, is brought under
the perineum, and its ends secured through the openings at the top of
the board. It is evident that, the splint being thus securely fixed and
made as part of the limb, tightening of the perineal band will extend
the member, and preserve it of its proper length. By care and attention
in applying the apparatus, and in adjusting the cushions about the
ankle and perineum, there is little or no risk of the skin giving
way. The bandages will require to be reapplied once or twice during
the cure, and the perineal band should be tightened frequently. The
apparatus is retained for six or eight weeks, the time necessary for
union varying according to circumstances. After its removal, great care
must be taken at first in moving the limb and in putting weight upon
it: it should be accustomed to its former functions very gradually.
The same apparatus in the most effectual for all fractures of the
thigh; but those near the distal extremity, and in the lower third
of the bone, may be managed tolerably well on the double inclined
plane—M’Intyre’s splint, the thigh-piece of which is double, the one
portion sliding on the other, and made to shorten and lengthen by means
of a screw, without removal from the patient. To this581 the limb is
secured by bandaging from the toes upwards; the upper bandage, which
should be broad, being continued close to the perineum, and then passed
several times round the loins. By elongating the thigh-piece by means
of the screw, extension is kept up. Great complaint is commonly made by
the patient of pain and stiffness in the knee for a long time after the
treatment of broken thigh in the bent position.
There is no possibility of treating fracture of the thigh, with any
satisfaction or credit, on the outside of the limb with the knee bent;
however attentively the splints are placed, shortening, eversion of
the foot, and deformity of the whole limb, are sure to follow. No
greater absurdity and cruelty are conceivable than leaving the fracture
unadjusted for weeks, making attempts to subdue consequent over-action,
and then endeavouring to reduce and retain the bones at a period when
otherwise they should have been firmly united. “Experience teacheth”
not “fools,” and cannot amend those whom prejudice has blinded.
Compound fracture of the thigh, if circumstances do not forbid attempts
to save the limb, is to be reduced and retained in the same way as
the simple, the wound being attended to, and means taken to subdue
inflammatory action. Abscesses must be opened timeously, the limb must
be equably supported, and the powers of the system preserved.
The application of force may, in young persons, detach the epiphysis
of the lower end of the femur, and displace it to a greater or less
extent; and if the accident be not detected, the epiphysis will become
consolidated with the shaft in this unnatural position, impairing
the usefulness of the member, and probably laying the foundation
for disease in or around the articulation. Reduction is easy, and
the retentive treatment is the same as that recommended generally
 for fracture of the thigh near the knee-joint. I have met with one
well-marked case of this form of diastasis. A girl sustained an injury
of the knee when fourteen years of age, in consequence of the limb
having been entangled amongst the spokes of a carriage-wheel in motion;
the knee continued painful and swollen, and she had a halt in walking.
After the lapse of about three years, extensive suppuration occurred in
the lower part of the thigh and round the knee-joint, and amputation
very soon became indispensable for the preservation of life. The
synovial apparatus was much diseased, and the epiphysis of the lower
end of the femur was found displaced forwards and upwards, so that only
the posterior part rested on the tibia; in fact, it was turned, as here
shown, almost half round on the shaft: firm union by bone had taken
place.
for fracture of the thigh near the knee-joint. I have met with one
well-marked case of this form of diastasis. A girl sustained an injury
of the knee when fourteen years of age, in consequence of the limb
having been entangled amongst the spokes of a carriage-wheel in motion;
the knee continued painful and swollen, and she had a halt in walking.
After the lapse of about three years, extensive suppuration occurred in
the lower part of the thigh and round the knee-joint, and amputation
very soon became indispensable for the preservation of life. The
synovial apparatus was much diseased, and the epiphysis of the lower
end of the femur was found displaced forwards and upwards, so that only
the posterior part rested on the tibia; in fact, it was turned, as here
shown, almost half round on the shaft: firm union by bone had taken
place.
Fracture of the Patella is generally simple. It is occasioned either
by great force applied to the bone directly, or by the action of the
strong extensor muscles—the knee being suddenly bent,582 and the bone
snapped across over the end of the femur. The degree of immediate
swelling, and of incited action, will vary according to the mode of
infliction. When the injury is caused by a blow upon the part, the bone
may be broken either transversely or vertically, or both; either the
upper or the lower portion may be vertically split, usually the upper;
sometimes there is considerable comminution. Muscular action produces
transverse fracture only.
The nature and extent of the injury is readily ascertained. The patient
is unable to extend the limb, and cannot support weight on it; in the
bent position, a space is felt in the situation of the patella, the
lower portion is found nearly in its place, but the other is drawn
upwards on the fore part of the thigh; by extension of the limb and
flexure of the thigh the portions are approximated, and crepitus
is perceived when they are brought in contact. These symptoms are
perceptible through any quantity of bloody effusion. By attentive
manipulation, comminution and vertical splitting may also be detected.
The circumstances attending the accident will, in most instances, lead
to a tolerably accurate expectation of the state of parts.
The ligament of the patella does not often give way from muscular
action; it is much stronger than the bone, and the latter consequently
snaps. It may be, and has been, divided, along with the superimposed
integument, by a fall on a sharp substance. This accident is followed
by lameness, the ligamentous tissue does not soon unite, and the limb
is long in regaining its usefulness; sometimes the union is imperfect,
and the member remains weak.
Division of the integuments over a fractured patella is a very serious
accident. The joint is opened, and such a state both of the limb and
of the constitution must in general sooner or later occur as to cause
necessity for amputation. Cases have, however, occurred, in which
compound fracture of the patella has been cured.
The bone unites, under favourable circumstances, in the same way as any
other. In longitudinal fracture there is almost always bony union. In
transverse, the obstacles to correct apposition are great; the upper
portion is acted on by the muscles on the fore part of the thigh, to
a greater or less degree, in almost any position; there is increase
and vitiation of the synovial secretion, and when the bones are
approximated, this fluid is interposed. The union is therefore almost
uniformly ligamentous, and, fortunately, this is as strong and as
rapidly effected as that by bone. When the treatment is not of the most
approved kind, a long portion of ligament is produced, and the limb
remains weak. But union by a short ligament is undoubtedly the most
desirable result, the member is as useful as when bone is the uniting
medium, and ligament is less subject to disruption; bony union is, for
a long time, apt to give way on the application of even slight force.
The fragments are to be approximated, and brought nearly into contact,
by placing the limb, with the knee extended, and the thigh slightly
bent on the pelvis. The limb is retained in this position by the
application of a straight splint behind, hollowed at the extremities,
extending from a little below the tuberosity of the ischium to below
the middle of the leg, and retained by a roller, not at all tight;583 the
foot and lower part of the limb must be previously bandaged to prevent
infiltration. All apparatus with straps, buckles, and apertures to
receive the portions of the bone, are worse than useless. The splint
requires to be worn for some time after the patient gets into the erect
position, which ought not to be before six weeks after the accident.
Fracture may occur at any part of the leg. One or both bones
may give way, either transversely or obliquely, according to the
application of the force. The transverse fracture is produced by a
direct blow, by a heavy body striking or falling on the limb, or by the
lower part of the limb being fixed whilst the body is in rapid motion;
the oblique is caused by force applied in the direction of the bones—as
when a person falls or leaps from a height, and alights on one foot,
the limb being extended and the body erect. In the latter description
of accident, it is frequently supposed, erroneously, that but one bone
has given way; fracture of the tibia perhaps is perceived some few
inches from the distal end, whilst the fibula at that part is entire;
but, by attentive manipulation, it will often be found that the fibula
has sustained fracture, within a short space of its upper extremity;
the force was applied to the ends of the bones, and they gave way, each
at the weakest part.
The tibia is broken at its upper part near the tuberosity, with
or without similar injury of the fibula. There is considerable
displacement, particularly in the bent position of the knee; there is
no restraint to the action of the extensor muscles inserted immediately
above the point of fracture, and these, though not acting with unusual
power, cause protrusion of the upper end of the tibia, the condyles of
the femur serving as a fulcrum over which the muscles are stretched.
This injury is usually the result of direct violence.
Fracture of one bone, at a point lower in the limb, is not attended
with much displacement or deformity. Indeed, attentive manipulation
is often required to detect the site of the injury; and a sense of
crepitation is perceived, only when the lower and upper portions of the
bone are pressed on alternately or during rotation of the foot. When
both bones are broken, the displacement and swelling are great. The
foot is sometimes turned inwards, but usually it falls outwards; and
if there has been much laceration of the soft parts, with or without
division of the integuments, the lower portion of the limb hangs quite
loose.
By the application of great force, as by a rope being twisted round
and run tight on the limb, both bones and soft parts may be reduced
almost to a pulp, without much or any division of the integument. Such
an accident is followed by rapid and great swelling, violent incited
action, gangrene, and severe constitutional disturbance. The progress
of the mortification is not in all cases uniform; in some, the swelling
and discoloration extend to the groin and trunk in two or three days,
attended with furious delirium; in others, the disorganisation of the
limb is very slow, some days elapsing before it reaches the knee, and
in these the constitutional symptoms are less severe.
In some cases there is extensive wound of the integuments, with584out
serious injury of the bone, muscles, or vessels. The skin either has
been divided by the external force acting upon the resisting bone, or
the sharp fractured end of the bone has been thrust through. Sometimes
the bone is protruded to a considerable extent, and entangled amongst
the more superficial soft parts.
Fractures of the lower portions of the bones are generally the
consequence of twisting and partial displacement of the ankle. The
fibula is most frequently broken by twisting of the foot outwards, and
the fracture is almost uniformly between two and three inches above the
articulation. The broken ends are displaced inwards upon the tibia. The
injury is detected by moving the foot, and tracing the line of bone;
after swelling has taken place, examination, though almost equally
easy, is productive of much more pain, and it is of importance to
ascertain the nature of the injury at once, and immediately after the
accident. The outer malleolus sometimes gives way from the same cause;
or it may be snapped off by a direct blow. The lower portion of the
tibia is sometimes longitudinally split by bending inwards of the foot,
the patient having fallen from a considerable height; occasionally
the inner malleolus is broken transversely. Inquiry as to how the
accident happened, particularly as to the direction of the twist, the
displacement of the foot, and the degree and extent of crepitation,
will determine the nature of the injury.
The astragalus, os calcis, the other bones of the tarsus, and those
of the metatarsus, are sometimes broken by the application of great
force, but they are not much displaced. Sometimes the foot is violently
concussed in consequence of a fall from a height, and though no
fracture may have occurred, the patient is equally lame and pained;
severe inflammation is sure to supervene rapidly, and may terminate
untowardly.
Fracture of the upper part of the tibia is to be treated in the
straight position, for it has been already observed, that when the
knee is bent the upper portion necessarily projects. A hollowed splint
of wood, extending from the middle of the thigh to near the heel, is
applied behind, whilst one of pasteboard may be placed on each side:
all are secured by bandaging, the foot and lower part of the limb being
rolled previously to prevent infiltration; by this simple apparatus,
motion of the knee-joint, and of the ends of the bones on each other,
is completely prevented; the heel is raised, if necessary, for complete
adaptation.
Fractures of the middle and lower portions of the bones are treated
most advantageously, whether simple or compound, in the bent position,
the angle being made more or less obtuse, according to the degree of
flexion most conducive to easy reduction and retention. Extension is
made on the limb, and the parts brought into as natural and handsome
a shape as possible; in doing so, the appearance of the sound member
should be kept in view. There is seldom any difficulty in accomplishing
reduction; the extending and counter-extending power need be but
slight; the upper part of the limb is steadied by an assistant, whilst
the lower is stretched and moulded by the hands of the surgeon. In
compound fractures at this part, the portions of bone completely
detached from the hard and soft parts585 are to be extracted. And if
reduction cannot be effected in consequence of a sharp and long end of
the bone projecting through a narrow wound, either the portion must be
abridged by the saw or cutting pliers, or the wound must be enlarged.
Sometimes the one mode is preferable—sometimes the other—occasionally
both are required. When the protruding portion composes but a small
portion of the shaft, though perhaps of considerable length, it should
be taken away; when, on the contrary, it is more thick than long, it is
better to enlarge the wound; but on this subject no general rules can
be laid down. The splint is the same as that recommended when treating
of fractured thigh, composed of a thigh and leg-piece, with a moveable
foot-board—the double inclined plane, improved by the late Mr. M’Intyre
of Newcastle and others. A very simple and efficient apparatus has been
used in our hospital for some years back. It answers every purpose
fully better than the others, and can be had of all the instrument
makers for a third of the expense of those previously in use. The
foot-board is fixed so as to make the leg-piece of the proper length,
and the splint is secured at a convenient angle. It is padded by means
of a cushion filled with oat chaff. The foot is rolled separately;
the limb is then raised carefully, and laid down on the splint placed
quickly beneath by an assistant; it is retained in a proper position by
the hands of the assistant, whilst a roller is carried from the toes
round the foot-board, and along the limb to the knee. A broad roller
is then made to surround the thigh and splint, and having been turned
several times round the loins, is secured to the upper part of the
cushion. The limb is thus rendered independent of the motions of the
trunk; it is made as of a piece with the splint. It should be raised
considerably above the level of the trunk, whilst the patient is in
bed, in order, by favouring the return of blood, to prevent swelling
and inflammatory action. The wound, if any, is to be approximated. If
discharge follow, part of the bandage may be undone from day to day,
for the purpose either of employing fomentation or of applying suitable
dressing, and still the limb is kept perfectly steady. Abscesses must
be opened early—spiculæ removed—constitutional symptoms warded off,
and, if they do occur, combated,—at one time inflammatory action must
be kept down—at another and more advanced stage, the strength must
be supported by all means. In simple fracture it is seldom necessary
to undo the bandage, till the apparatus is loosened by subsidence of
the swelling—and if the fracture be early reduced, and kept steady,
that will be but slight. Then the bandages are undone and reapplied,
and the position of the limb attended to. It is seldom necessary to
interfere with the leg during readjustment, but should there be any
deviation, even considerable, from the proper position, it is easily
remedied at the end of the first, second, third, or even of the fourth
week; but the sooner the better. The patient may be removed from bed,
and may sit up during the greater part of the day, with the heel on a
level with the pelvis, within the first week. His health, appetite,
and spirits, are thus kept up, sore back is avoided, the tedium of
confinement diminished, and the cure greatly accelerated. At the end
of five, six, seven, or eight weeks, according to the age, and as
the586 consolidation advances, the patient may be allowed to move about
on crutches, some few days after removal of the apparatus, the foot
and leg being still bandaged, and supported by light splints, or the
bandages may be starched and applied moist, with portions of coarse
brown paper interposed. A firm case is thus formed for the protection
of the limb and retention of the bones. No weight should be put on the
limb for several weeks after, otherwise a leg cured well and straightly
may become bent, twisted, and deformed.
Fractures of the lower extremities of the bones, and of the malleoli,
are reduced by placing the foot straight, and retaining it so by
the application of a wooden splint; the parts are protected by a
wedge-shaped pad, and the whole is retained by a common roller. The
splint is made to project two inches or two inches and a half beyond
the ankle, and to reach near to the knee-joint. It has two perforations
in the upper end; to these a bandage is attached by its split end, and
it is then carried down along the inside of the splint, and rolled
round the foot and ankle; thus the apparatus is prevented from shifting
upwards. The other extremity of the bandage, during its convolutions
round the foot, is made to pass through notches in the farther end of
the splint; the foot is thus turned to the side opposite to that in
which it was placed by the accident, and ought to be retained so till
consolidation has taken place. The splint is of course always placed on
the side of the limb opposite to the fracture.
Disunited Fracture.—In some cases union takes place very slowly.
On removing the splints, with the expectation of finding the bones
firmly united, the ends can be moved very freely on each other without
crepitation or much pain. This, as already stated, may be referrible
to various causes,—necessary or accidental evacuations, natural or
not—diversion of the nutritious fluids to some particular organ, as
in pregnancy—the period of life—a diseased state of the bone of the
periosteum or medullary web. By keeping the parts immoveable and firmly
compressed for some time longer, consolidation may be brought about.
But in spite of every care, the ends of the bones in some cases remain
unconnected by any save a soft medium. This happens, however, very
rarely under proper management. I have had but one case of it in my own
practice, when the patient was from the first under my own inspection
and care; and in that the occurrence of false joint was attributable
solely to the absurd conduct of the patient. He was tripped up on the
street by some individuals following their avocation as pickpockets,
fell, and broke his forearm. The fracture was immediately reduced and
splints applied—one of pasteboard on each side, with a wooden one
exteriorly till the pasteboard hardened. He soon cut away the ends of
the splints—within thirty-six hours after they had been put on—so as
to allow motion of the fingers and hand, sufficient for indulgence in
card-playing. The splints were still farther shortened, and wholly
removed much too soon; shortly afterwards he fell from horseback. No
union took place by bone. Unless in the case of previous disease of
the bone, disunion is generally attributable to some carelessness or
recklessness, either of the surgeon or of the patient.
587
If any osseous deposit has taken place, it is absorbed; the ends of the
bone are diminished in size by interstitial absorption; ligamentous or
fibro-cartilaginous tissue is formed round the wasted extremities; and
the surrounding cellular tissue being thickened and condensed, a sort
of synovial pouch is formed, in which the ends, by this time smooth and
rounded off, move freely. The limb is shortened in some degree, and its
actions are very much diminished in force, there being no sufficient
support for the muscles. The bones of the leg and of the forearm are
occasionally the seat of false joint, sometimes the femur, but most
frequently the humerus.
By the tight application of a firm and broad belt of leather, the part
is steadied, and the limb rendered more serviceable. Various measures
have been proposed and practised with the view of promoting a salutary
increase of action in the parts, by which osseous deposit in sufficient
quantity to form a firm uniting medium might be procured. The ends of
the bones have been exposed by incision, and removed either by the saw
or by cutting pliers; they have then been placed together, retained by
proper apparatus, and the case treated as one of compound fracture.
The ends have been cut down upon, rubbed over with escharotics, as
caustic potass, and afterwards treated as in the former method. Setons
have been passed between the ends of the bones, and been retained till
sufficient action has occurred; they have been then withdrawn, and the
limb steadied by splints and bandaging.
To the last method I would, from some experience, give the preference.
It is the least severe, both immediately and consecutively; it is the
most readily accomplished, and the most likely to be followed by a
successful result. The exact site of the ends of the bones must in
the first place be ascertained; the position of the bloodvessels and
nerves must be looked to, that they may be avoided; a bistoury is then
passed through the skin and down into the substance interposed between
the ends of the bones. A strong and sharp needle, fixed in a handle,
and with its eye near the point, is passed, in the track of the knife,
fairly betwixt the bones, and pushed through the soft parts on the
opposite side of the limb. A cord is then passed through the eye, and
by withdrawal of the needle the seton is properly lodged. The effects
must be attentively watched, and when sufficient action is supposed
to have been excited, perhaps at the end of the first week, the cord
is withdrawn, and the limb placed immoveable in a proper position. If
action is slow in supervening, the chord may be smeared with irritating
substances, as the unguentum oxydi hydrargyri rubri, or the unguentum
cantharidis, &c. In this manner I have treated false joint in several
situations successfully, but I have also been sometimes foiled in
effecting my purpose. The seton must not be long retained, the object
being to excite action, not to perpetuate discharge, by the profusion
of which the end will be effectually frustrated. Much will depend on
the period at which the practice is adopted.63
588
Dislocations.—Some joints are so contrived—their composing bones
are so notched into one another, and connected by such power589ful
apparatus—and they are crossed by tendons, and tied together by
ligaments in such a manner,—that dislodgement can scarcely be effected
but by the most violent means. Nothing short of immense force is
sufficient, and the displacement is uniformly attended with fracture of
portions of the bones, or of their processes. Other bones are loosely
joined, permitting free and unrestrained motion in all or in many
directions, and but little force, applied in particular directions,
suffices to separate and luxate them. In every joint the processes
are liable to be broken, and the attachments of the ligaments to be
torn off; ligamentous tissue withstands a greater degree of sudden
violence than the osseous. The synovial membrane, and the fibrous
tissue exterior to it, are almost always torn in complete luxation;
but the extent of laceration varies in different joints, according to
the direction of luxation and the degree of displacement. The rent
may be small, closely embracing the neck of the bone; or there may be
an extensive gap on the side opposite to that on which the luxation
has taken place. In an articulation surrounded by muscular substance,
there is also laceration of this to a greater or less extent. In some
individuals, dislocation is very apt to occur, perhaps from peculiar
laxity of fibre; and if in any person luxation of a joint has once been
produced, the accident is apt to occur again and again from but slight
causes.
In general, the mobility of the luxated joint is much diminished;
590the limb is either shortened or lengthened; its contour is changed;
the injury is attended with violent pain; the patient is sick and
pale; the system receives a shock, from which it gradually recovers
after some time. Then swelling, from effused blood, takes place; and
this is followed, after some hours, by excited action of the vessels
and farther effusion, giving rise to greater stiffness and pain on
attempts at motion. If no means are taken to replace the bone, and
painful feelings subside along with the swelling, the limb remains
long useless, and is the seat of occasional lancinating pains, but
at last motion and utility are to a certain extent restored by the
formation of a new joint—the head of the bone, and the parts on which
it rests, mutually accommodating themselves to each other, by degrees,
and permitting a limited extent of motion. Post mortem examination,
years after the occurrence of the injury, shows change in the form of
the bones—the head is flattened, and in the bone on which it lies there
is a corresponding depression, formed partly by the deposition of new
matter, partly by absorption of the old; in dislocation on the dorsum
of the ilium, for example, there is excavation by absorption opposite
to the centre of the head of the femur, and round this new osseous
matter is deposited so as to form the cavity into a cup resembling
the acetabulum. New processes are formed for the attachment of the
muscles, and the old are absorbed to a remarkable extent. There are
also new ligaments; and a sort of capsule is formed by condensation of
the surrounding cellular tissue. The new articulating surface becomes
quite smooth internally, and is covered, if not by cartilage, by a
smooth substance which answers the purpose tolerably well; the old is
gradually filled up and obliterated, the prominences being absorbed,
and the cavity occupied by new deposit. These changes do not take place
so rapidly as is generally supposed; the cartilage and synovial surface
are not much altered for months after the occurrence of luxation;
and if replacement be effected, the functions of the parts are soon
performed as before the injury.
In some articulations, on account of the formation of the opposed
surfaces, attempts at reduction prove ineffectual after the lapse of
two or three weeks; in others, of more simple construction, it may be
accomplished after some months. The simple mode of reduction is to put
the patient off his guard, so that the muscles may be in a state of
relaxation, and then to move the limb artfully in the proper direction,
without much force. Occasionally, the bone is pulled into its place
by the action of the muscles, during the patient’s efforts to place
the limb in a comfortable position. Considerable force, however, is
sometimes required in even recent luxations of large joints, and means
must also be taken to weaken the muscular power. The patient, if young
and robust, may be bled to syncope, or placed in the warm bath till
a sense of fainting supervenes; or an enema of tobacco infusion may
be administered, and smoking of tobacco may have the same effect when
the patient has not been addicted to the noxious habit; or antimonial
solution may be given in nauseating doses. Several or all of these
methods may be necessary in some cases, particularly if the dislocation
be of long591 standing. When thus general exhaustion has been procured,
counter extension and extension are to be had recourse to. The former
consists in having the patient, and the bone next to the trunk, fixed
immoveably by fitting lacques and belts; and the latter is made by
one or more assistants, or, if need be, with the help of pulleys.
During extension, advantage is in many cases gained by lateral force
and by rotation of the limb, the bone being thereby moved from its
position, and brought within the sphere of muscular action, by which
it is drawn suddenly into its proper place. In some cases, there is
no doubt but considerable laceration is occasioned by the efforts at
reduction, and perhaps this is in some degree necessary to a successful
issue—as when the capsule has been slightly lacerated by the accident,
and in consequence interposes an obstacle to the head of the bone
slipping into its socket. After reduction, inflammatory action in the
articulation and its neighbourhood is to be expected, to a greater or
less degree, particularly when much force has been employed, and means
must be taken to avert this; local remedies are generally sufficient,
along with perfect rest.
In luxation of the lower jaw, both articulating ends are most
frequently dislodged. They can escape in but one direction, forwards
into the temporal fossæ; when both are dislodged, the mouth is widely
open, and fixedly so, the chin is drawn downwards and backwards. When
one is displaced, the jaws are partially opened, the chin is twisted to
a side, and immoveable. Great pain is experienced from the pressure of
the condyles of the bone on the temporal muscles, from stretching of
the fibres of the pterygoids, and from interruption to the functions,
by pressure, of the contiguous bloodvessels and nerves. Mastication
is impossible, the speech is altered, and indeed articulation may be
said to be impracticable.
It is supposed by the vulgar that the accident is particularly apt to
happen to infants and young persons. Nurses are in consequence careful,
when a child yawns, to support the chin, and pronounce an accompanying
blessing. The articulating cavity is then shallow, yet luxation must be
rare in young subjects. In my own experience no instance of dislocated
jaw has occurred but in adults; and then, either from over-opening of
the jaws, or from powerful muscular action during depression of the
inferior maxilla.
The nature of the injury is at once known; and the displacement
is easily remedied. But I have met with instances where, through
ineffectual attempts at reduction, the unnatural position has been
allowed to continue for many hours, to the great distress of the
individual. The object in view is to depress the ramus—one or both,
as may be—and to raise the chin. This is effected by pressure with
the thumbs on or in the situation of the molar teeth, whilst with the
fingers the jaw is moved upwards and backwards. The thumbs need not be
protected by a glove, as is generally recommended; on the bone resuming
its place, they are easily slipped into the space betwixt the jaw and
the cheek. There is no necessity for bandaging, as retentive apparatus;
the patient is not likely to yawn for some time after.
592
Luxation of the clavicle, at either end, is produced by force applied
to the point of the shoulder. It is seldom that the sternal extremity
is separated from its connexions. When this accident does happen, it
is easily recognised; the end of the bone is prominent and loose, and
is distinctly felt riding over the top of the sternum. Replacement is
effected by bringing back the shoulder; but the bone is with difficulty
retained in the proper position, and is long in becoming fixed; a
certain degree of deformity is ever after present.
Displacement of the scapular extremity is by no means rare, and occurs
to a greater or less extent, according to the laceration of the
ligaments. If those only are torn which connect the end of the bone
to the acromion, there is mere rising of the end. But if—as is often
the case when the violence has been great, as in a fall either from
a height or with great velocity—the conoid and trapezoid ligaments
connecting the tuberosity of the bone with the coracoid process, have
given way, then the end of the bone projects, pushes out the deltoid,
and gives rise to considerable flattening of the shoulder. The arm
falls forwards, and cannot be moved but with pain; nor is the patient
able to raise it by its own muscular power. If the surgeon grasps the
middle of the bone, he finds the end moveable; and the evident and
deforming projection puts an end to any doubt regarding the nature of
the case. The bone is readily reduced by raising the arm, and carrying
the scapula backwards. The limb must be retained in the proper position
for many weeks, if a cure without interruption, and with as little
deformity as possible, is desired; but after the utmost care and
patience, there still remains, in almost every case, some projection
more than before the accident. The ligaments are slow in uniting, and
the union is imperfect and weak. The requisite apparatus is the same
as for fractured clavicle, but must be retained for a longer time. The
patient experiences great relief from the limb being put up in this
manner and maintained so; and inflammatory action, with much of the
swelling, is averted.
The inferior angle of the Scapula occasionally escapes from under
the border of the latissimus dorsi, usually with some laceration of
the muscular fibres. The displacement is occasioned by raising the arm
above the head to an unusual extent. The angle of the bone projects
considerably, and the muscle is felt playing beneath it distinctly
during motion of the parts; the movements of the limb are limited and
painful. The parts may be brought into their original position by
pressing the angle of the scapula towards the ribs, whilst the arm
is much raised; and the bone is afterwards confined in its proper
place by a broad bandage passed pretty tightly round the chest. The
retentive apparatus must be continued for a considerable time, and in
some cases a cure may be so effected; but in general the bone soon
regains its former unnatural position, and continues to do so, however
often and however easily it may be replaced. The parts gradually become
accustomed to the change in relative position, and little inconvenience
is experienced.
Luxation of the Shoulder-joint is prevented, by the arrangement
and structure of the parts, from taking place in any direction
ex593cepting towards the axilla—downwards into the hollow of the armpit,
downwards and forwards under the lower border of the pectoral muscle.
Occasionally, though very rarely indeed, displacement occurs backwards.
On the anterior and inferior aspects, the articulation is not
supported, as at its other sides, either by muscular substance or by
processes of bone. The accident is occasioned sometimes, though rarely,
by direct violence, as by a blow on the back part of the shoulder; and
of such I have seen a few examples. But, in almost every instance, the
displacement is caused by force applied to the distal extremity of the
humerus; either immediately, as by falling on the elbow, or through the
forearm, as when a person endeavours to break a fall by stretching out
the arm, and alights with the whole weight of the body on the palm.
The accident may also result from forcible abduction of the extremity,
particularly when the power is applied near the extremity of the limb.
There is laceration, to a greater or less extent, of the capsule, and
of the muscles immediately investing the fibrous tissue round the
articulating cavity. Without disruption, complete luxation cannot
exist—the articulating surfaces cannot be separated, nor can the head
of the humerus be altered in position; subluxation, or, in other words,
a sprain, may occur in such circumstances, but true luxation cannot.
Bruises of the shoulder, with or without fracture, either of the
scapula or of the upper part of the humerus, must not be mistaken
for dislocation, for the consequences of such a blunder are fearful.
In both descriptions of accident, the appearances of the limb are
somewhat similar, and hence the examination requires to be particularly
accurate and careful. In both there is flattening of the shoulder, but
in fracture there is crepitus, motion to an unnatural extent, though
painful, and greater suffering during manipulation; in dislocation
no crepitus at all resembling that in fracture can be perceived, the
motions of the limb are very limited, and the displaced head of the
bone can almost always be felt. The direction of the force, too, as
already observed, when on the subject of fracture, is an important
assistant in diagnosis; from falls or blows upon the shoulder we
may expect fracture, from falls on the elbow or palm, luxation. In
dislocation an indistinct feeling, sometimes amounting to obscure
crepitation, is occasionally perceived during rotation of the limb;
and this arises from one or more of the tendinous attachments of the
muscles having, during their disruption, torn away a portion of their
osseous attachment.
Great pain attends on dislocated humerus, from the head of the bone
compressing and stretching the axillary plexus; and the interruption to
the flow of the blood produces tingling at the points of the fingers,
numbness of the whole limb, and after a time swelling of the hand and
forearm. Flattening of the shoulder, and depression under the acromion,
are the most prominent marks of displacement having occurred, and are
at once apparent. They are more distinctly perceived on comparing the
two shoulders; then the acromion on the affected side stands remarkably
outwards. The projection is not so apparent when the immediate swelling
from effused blood has been fully formed, but the hollow under the
acromion can594 be felt through any quantity of extravasated blood. The
arm admits of very little motion, is lengthened and abducted. The
elbow cannot be brought close to the side, and attempts to do so are
productive of great suffering. The patient has little or no muscular
command over the upper arm. Rotation and elevation of the limb require
considerable force, and are practicable only to a very limited extent;
during attempts at the former, as already mentioned, obscure crepitus
is sometimes perceived. The abduction is most remarkable in the
dislocation directly downwards; and in this form of the accident, the
fingers easily detect the head of the bone lying in the axilla, deep,
yet distinct, particularly during attempted rotation. When the head of
the bone lies forward by the coracoid process, and under the pectoralis
major, it can be felt, and the prominence occasioned by it can be
clearly seen in thin people, before swelling has occurred, and after
its subsidence. The bone sometimes lodges in an intermediate situation,
and then the signs peculiar to each form of displacement are mixed.
When reduction is not accomplished, the bloody swelling first occurs to
obscure the signs; this may in part subside, but then the inflammatory
supervenes; both after a time disappear, the muscles waste, and then
all the signs are very apparent. After some weeks, the motions of the
limb become more extensive, not in consequence of the head of the
humerus having changed its position, or returned into the glenoid
cavity, but from the scapula moving on the ribs more freely, and to a
greater extent than usual. At last, but not till after a long period,
considerable motion betwixt the bones can be effected; the scapula,
where the head of the humerus rests, having furnished an adventitious
cavity, to which the latter has adapted itself. But free motion can
never be regained, for the movements that are effected are chiefly
produced by the action of the muscles of the scapula.
Replacement, even in very recent cases, sometimes is accomplished with
difficulty in those whose muscles are fully developed. But in general
a successful result will follow simple measures, particularly if the
patient is taken unawares—as by rotating the arm with one hand whilst
the fingers of the other are placed in the axilla, then suddenly
lifting the head of the bone outwards, and at the same time performing
abduction—the patient being all along assured that he will not be put
to pain, and that there is no intention of attempting reduction. In
this manner reduction may often be accomplished by the surgeon and one
assistant; the trunk and scapula being fixed by the assistant, either
grasping the patient in his arms, or holding a sheet or towel passed
round the body, close to the axilla, whilst the surgeon extends and
rotates the extremity, and at the same time lifts the head of the bone
from its situation. The rotation is made by using the forearm, bent
to a right angle, as a lever; thus considerable power can be exerted
on the head of the bone, and the long head of the biceps muscle—the
stretching of which, no doubt, affords an obstacle to reduction—is
at the same time relaxed. In luxation downwards, there is no more
successful method than that by counter-extension with the heel in the
axilla, and extension by the surgeon grasping the wrist. The patient is
placed recumbent, on a couch or on the floor, and the surgeon, sitting
by his side, lodges his595 heel in the axilla, and with both hands
extends the arm; after a short continuance of extension, he performs
a sudden and powerful combination of both movements, and so jerks the
bone into its natural position. In some recent, and in all old cases,
it is necessary to apply considerable force, steadily, and for a long
time, so as to tire out the muscles, and dislodge the head of the
bone. An assistant effects this by means of pulleys. These are fixed
to a laque, applied above the elbow with a clove-hitch, and to a ring
fastened either in the wall or to a post; two small iron rings which
can be screwed into a beam are useful in private practice, and should
always accompany the pulleys. When all is prepared, the assistant pulls
the end of the rope steadily, and with considerable power, whilst the
surgeon rotates the limb, and endeavours to lift the head of the bone,
at the same time regulating the degree of extension. The directing of
the degree and continuance of the force is not the least difficult
part of the procedure, for, when excessive, there is a risk of the
axillary nerves and artery giving way; such accidents have happened,
and been accompanied with serious and even fatal consequences; and from
laceration of other tissues, the muscular, fibrous, or cellular, fatal
inflammation and abscess have resulted. The surgeon is therefore called
upon to exercise judgment and discretion—not to continue extension to a
pernicious extent, and not to abandon attempts at reduction too soon,
leaving his patient disabled for life. For making counter-extension to
the extension by pulleys, a broad strong belt is useful, perforated
near the middle for transmission of the injured arm; it is passed round
the body so as to fix the trunk and scapula, coming under the axilla of
the sound side, and being then fastened by means of a hook to a ring in
the wall.
Luxations of the shoulder-joint may be, and have been, reduced after
the lapse of two or three months; but the difficulty increases, and
the chance of success diminishes, in proportion to the time which has
elapsed since the date of the accident. And in deciding upon making
the attempt, many circumstances are to be weighed and considered—the
patient’s period of life and his occupations, the state of the parts,
the degree of motion that has been acquired, and the treatment, if
any, which has been previously followed. Perhaps the most important
consideration is regarding the state of the parts, as indicated by the
degree of motion. If the movements be to such an extent as to favour
the supposition of the head of the bone having been furnished with a
new recipient cavity, to which it has in a great measure accommodated
itself, and that the glenoid cavity has, from disuse, become altered,
the surgeon can scarcely hope for advantage to his patient from
attempts to break up the new articulating apparatus, and reëstablish
the old. The patient will, most probably, be put to a great deal of
pain and some danger, without experiencing improvement to the limb;
indeed the motions and power may prove less than before. In old men,
too, force sufficient for reduction cannot be employed without great
risk of laceration of nerves, bloodvessels, and muscles. But if the
patient be young, the motions still limited, and the articulation
apparently not changed by solid effusion, reduction may be attempted
with a fair prospect of success, and without injury. In all such cases,
however, the surgeon must watch596 every step of the proceedings, and
have sufficient experience to stop short of inflicting irreparable
mischief. No standard can be fixed for the degree of force that is
necessary and safe; he may be foiled, even after the most powerful
efforts, in a dislocation of two or three weeks’ duration; whilst, by
the use of but slight force, he may succeed in one of as many months.
Much assistance is obtained by the means formerly adverted to, as
auxiliary, by weakening the muscular energy. Of these, nauseating
doses of antimony are most generally employed, and being the most
safe, may be recommended to be tried first; and if these fail to
produce the desired effect, the patient may be bled freely, if he be
young and robust, more especially since this will assist to avert
the inflammatory action likely to follow the violent reduction.
Tobacco produces the most complete prostration of muscular power, and
may consequently be resorted to in extreme cases; but it ought, if
possible, to be avoided, as its use is far from being void of danger.
The warm bath cannot always be procured; when at hand, it merits
adoption, being both safe and effectual, particularly if combined with
antimony or bleeding. The extension should not be commenced till these
means have begun to take effect, but everything should be prepared, so
that it may be applied at a moment’s warning. After all attempts at
reduction, whether successful or not, it is necessary to moderate the
inflammation that ensues, by local bleeding and fomentation, combined,
if necessary, with nauseating laxatives: general depletion is seldom
required.
Luxation of the Elbow-joint is an extremely common accident,
particularly in young persons, before the bony processes have been
fully formed. It is produced by wrenches, or by force applied to the
farther end of the forearm, the bones neither breaking nor bending.
Sometimes, though very rarely, it is caused by direct violence, as in
a fall, and then may be combined with fracture of one or both bones
of the forearm; but in other circumstances, fracture and luxation can
scarcely coexist. In general, both bones of the forearm are displaced
backwards, sometimes a little to the ulnar side. The coronoid process
occupies the cavity for the reception of the olecranon, and the head
 of the radius lodges behind the external condyle; the extremity is
shortened, and looks twisted; it is slightly flexed, and in the middle
state between pronation and supination. Unnatural lateral motion can
be produced, but flexion is impracticable, the limb cannot be brought
quite into the extended state, and rotation is difficult and painful.
Swelling soon takes place, and consequently the hollows are filled
up, and the processes of the bones obscured. Yet the olecranon and
inner condyle can always be recognised and felt, and their relative
position ascertained; the form of the end of the humerus, its hollows,
and its prominences, can be distinctly discerned, both before and
after the swelling, the soft parts being stretched over the bone;
and by rotating597 the limb with one hand, whilst the other is placed
over the outer and back part of the joint, the situation of the head
of the radius is detected. Thus the relations of the bones to one
another are discovered; and this must be done at once, whatever pain
may be produced by the examination, for it is a saving of suffering
in the end. Yet the nature of this injury would seem difficult of
detection—a fact scarcely intelligible by any one who is careful in
his manipulations, and who possesses common observation, and a sound
knowledge of anatomy. Many cases of unreduced luxation are met with;
I have seen it in both elbows of the same person; and I have had a
dozen of cases, in as many months, of unreduced elbows shown too late
for attempts at reduction. The frequent occurrence of such blunders is
the more lamentable, as it is almost impossible to replace the bones
after three or four weeks; indeed, I have been foiled at the end of two
weeks. The parts soon accommodate themselves to their new position,
the olecranon process shortens, motion rapidly increases, and the
bones get more and more secure in their new relations,—osseous matter
being deposited laterally, forming cavities for their lodgement, and
new ligamentous matter confining them thereto. After a time, flexion
can be made to a right angle; and the limb becomes tolerably useful.
By unsuccessful attempts to restore the natural position, inflammation
is excited; and thus the salutary processes, commenced by nature for
reparation of the displacement, are interrupted and delayed; in young
persons such disease of the joint may be produced as might lead to loss
of the extremity.
of the radius lodges behind the external condyle; the extremity is
shortened, and looks twisted; it is slightly flexed, and in the middle
state between pronation and supination. Unnatural lateral motion can
be produced, but flexion is impracticable, the limb cannot be brought
quite into the extended state, and rotation is difficult and painful.
Swelling soon takes place, and consequently the hollows are filled
up, and the processes of the bones obscured. Yet the olecranon and
inner condyle can always be recognised and felt, and their relative
position ascertained; the form of the end of the humerus, its hollows,
and its prominences, can be distinctly discerned, both before and
after the swelling, the soft parts being stretched over the bone;
and by rotating597 the limb with one hand, whilst the other is placed
over the outer and back part of the joint, the situation of the head
of the radius is detected. Thus the relations of the bones to one
another are discovered; and this must be done at once, whatever pain
may be produced by the examination, for it is a saving of suffering
in the end. Yet the nature of this injury would seem difficult of
detection—a fact scarcely intelligible by any one who is careful in
his manipulations, and who possesses common observation, and a sound
knowledge of anatomy. Many cases of unreduced luxation are met with;
I have seen it in both elbows of the same person; and I have had a
dozen of cases, in as many months, of unreduced elbows shown too late
for attempts at reduction. The frequent occurrence of such blunders is
the more lamentable, as it is almost impossible to replace the bones
after three or four weeks; indeed, I have been foiled at the end of two
weeks. The parts soon accommodate themselves to their new position,
the olecranon process shortens, motion rapidly increases, and the
bones get more and more secure in their new relations,—osseous matter
being deposited laterally, forming cavities for their lodgement, and
new ligamentous matter confining them thereto. After a time, flexion
can be made to a right angle; and the limb becomes tolerably useful.
By unsuccessful attempts to restore the natural position, inflammation
is excited; and thus the salutary processes, commenced by nature for
reparation of the displacement, are interrupted and delayed; in young
persons such disease of the joint may be produced as might lead to loss
of the extremity.
Luxation of the Radius alone, backwards on the outer condyle, is
sometimes met with; but this bone is seldom singly displaced far from
its original site. A hollow is felt below the end of the humerus,
on the outer and fore part, and there is a corresponding prominence
behind; the head of the bone is found unnaturally moveable on rotation,
and this motion is difficult and painful; the arm is extended,
presenting a twisted appearance, and flexion is very limited. Extension
is to be made, along with pronation.
Sometimes the radius is displaced forwards. The coronoid process of the
ulna is occasionally broken off; there is no deformity during flexion
of the elbow, but when the limb is extended, the olecranon is drawn
upwards.
In luxation of both bones, reduction is much facilitated by position
of the arm. The arm and forearm are extended, and the limb is brought
well behind the trunk, so as to relax the triceps; then the surgeon
performs extension and counter-extension, pulling the forearm with one
hand, whilst he pushes with the other placed on the scapula. If the
force thus employed prove insufficient, as it seldom will in recent
cases, the patient may be placed on his face, on a couch, and on the
limb being brought into the favourable position already noticed,
counter-extension may be made by the heel planted against the inferior
costa of the scapula, whilst the wrist is pulled with both hands.
It is seldom necessary to employ pulleys, excepting in cases of old
standing; if so, the only peculiarity in their application to this
joint is the direction of the force, backwards. And this I con598sider to
be a very material part of the manipulations, for, by attention to it,
I have succeeded after previous failures,—after great force had been
applied, causing excoriation and swelling of almost the whole limb. In
luxation of the radius, backwards, flexion and pronation, combined, if
necessary, with extension, will generally effect replacement.
Dislocation at the Wrist is very unfrequent. The articulation
is naturally strong, admitting of little motion, the bones being
accurately fitted to each other, whilst the retaining ligamentous
apparatus is both copious and unyielding; on this account greater
force is required to effect displacement here than at either the elbow
or shoulder-joints, and violence applied to the hands usually causes
fracture of one or both bones of the forearm, not luxation of their
extremities. Luxation, however, sometimes occurs, either from violent
twisting, or from falling on the palm of the hand; and the displacement
may be either of both bones or of one. In the latter case, it is almost
uniformly the radius that suffers; in the former, the luxation is
forwards.
Dislocation of the distal extremity of the radius is generally produced
by a sudden wrench or twist. The bone is felt loose and prominent,
sometimes riding over the upper part of the carpus. The position of
the hand is towards pronation, supination cannot be performed, and,
on attempting it, great pain is occasioned. Reduction is readily
accomplished, by pulling the palm with one hand, whilst with the other
the head of the bone is pressed backwards into its situation.
Displacement of both bones is more frequently the result of a fall on
the palm, with the hand bent much backwards. In this case there are
two projections, so distinct as at once to mark the true nature of the
accident, one anteriorly, formed by the ends of the radius and ulna,
the other posteriorly by the carpus; above the posterior prominence
there is a considerable depression. Here also reduction is easy; it is
sufficient to perform simple extension with one hand, whilst with the
other the wrist is moulded into its proper form. The after treatment,
however, requires attention, for extensive laceration of tendinous
and ligamentous tissue, perhaps combined with fracture of the bony
processes to a greater or less extent, must have taken place to admit
of displacement; in consequence violent inflammation is to be expected,
and means must be taken to avert it. On account of this laceration,
also, mere reduction is not sufficient, retentive apparatus must be
applied; as soon as the limb has been made straight, a pasteboard
splint is to be applied on each side, as in fracture of the forearm,
and retained with a roller, a wooden splint being placed exteriorly
until the pasteboard hardens. This precautionary measure is also
necessary to avert redisplacement in dislocation of the radius singly;
in both accidents the apparatus should be retained for at least a
fortnight. Afterwards, passive motion, gradually increased and combined
with friction, is requisite to prevent stiffness of the joint.
In mere sprain of the wrist, large swelling soon forms anteriorly,599
from extravasated blood, resembling somewhat projection of the
bones, and so leading towards fallacy in diagnosis; indeed it is
not unreasonable to suppose that dislocation here does not occur so
frequently as is imagined. Fracture also near or through the distal
extremity of the radius, an accident formerly mentioned as exceedingly
common from falls on the hand, is very apt to be mistaken for luxation.
On this account, and because in every injury of the wrist the parts are
soon obscured by bloody swelling, there is a strong necessity for early
and accurate examination.
Subluxation not unfrequently occurs; in other words, the attachments
of the bones of the forearm to each other are broken up, and their
extremities separated to an unnatural distance. The accident is
distinctly marked by the deformity, the absence of hard projection, and
by the unusual space between the radius and ulna occupied by a soft and
yielding swelling. Replacement is accomplished much in the same manner
as in complete luxation, the bones being compressed towards each other
with one hand, whilst extension is made with the other; afterwards
splints must be applied and retained.
Compound luxations of the wrist are occasionally met with, and, like
compound fractures in this situation, are always troublesome, and often
terminate unfavourably. The soft parts are sparing, possessed of little
vitality, and much injured by the accident; consequently reparation
proceeds very slowly, and is generally superseded by unhealthy and
profuse suppuration, perhaps accompanied with more or less sloughing
of tendons and integument. If the ends of the bones protrude bare,
shattered, and split, they should be removed by means of either the
saw or the cutting pliers, previously to attempts at reduction; the
wound should then be approximated, and the cure conducted on ordinary
principles.
Sometimes a single bone of the Carpus is displaced, usually
backwards. It is quite loose and moveable, and is easily replaced,
but in almost every case redisplacement occurs, the bone at one time
occupying its proper situation, at others forming an inconvenient and
unseemly prominence on the back of the wrist, diminished by extension,
and increased by flexion of the joint. The accident, however, is rare.
I have never seen simple dislocation of any of the metacarpal bones.
Dislocation of the Fingers is produced by force applied to the
extremities of the phalanges; the displacement is always backwards,
excepting at the middle joint, where the bone of the middle phalanx is
sometimes, but very rarely, luxated forwards. The remarkable projection
on the back part of the finger marks the nature of the accident, even
to the most careless observer. Reduction is accomplished by extension
combined with flexion. In the case of the distal phalanges, it may
sometimes be necessary to fasten a cord to the tip of the finger, in
order to obtain sufficient extending power. After replacement, the
application of temporary splints and bandage is prudent. Compound
luxations, however carefully treated, almost uniformly come to
amputation.
Luxation of the first joint of the thumb is rather an uncommon600
accident, and is not easily managed. The base of the first phalanx
is displaced backwards upon the distal extremity of the metacarpal
bone, causing a remarkable prominence on the dorsal aspect, and a
corresponding depression on the palmar. The thumb is shortened,
deformed, and almost immoveable; the swelling and pain are severe.
This displacement is generally produced by the application of force
to the point of the thumb, as in falling on it, or in coming against
a resisting body with the thumb straight. The deformity is such as
at once to apprise even the most inattentive or inexperienced of the
true nature of the injury; but the treatment is very difficult and
puzzling even in the hands of the best informed surgeons. The base
of the bone seems to slip through the lateral ligaments, and remain
firmly locked in their embrace; and these being very strong, and in
a state of complete tension, defy all usual attempts at reduction.
The end of a silk handkerchief, or thick soft cord, is to be attached
to the distal extremity of the displaced phalanx, by means of the
clove-hitch; and with this extension is made, either by the surgeon
alone, or by one or more assistants,—frequently several are required.
Counter-extension is made by the surgeon or assistant grasping the
forearm, or another handkerchief may be passed betwixt the thumb and
forefinger for an assistant to hold on by. The extending force should
be made in a direction towards the palm, and almost uniformly requires
to be great and long continued, even in recent cases. The bone may
occasionally be jerked into its place by a sudden attempt at flexion of
the joint, during steady pulling that has been continued for some time.
But cases have occurred in which all attempts have proved ineffectual,
and it has been found necessary to divide one of the lateral ligaments.
From what has been already stated, the reason why this proceeding
should facilitate reduction is sufficiently obvious. I had recourse
to it in one instance,—one in which difficulty of reduction was not
to have been expected. The accident was very recent, not an hour had
elapsed; the patient was an old man, and very drunk; no resistance to
the reductive measures could have been offered by muscular energy;
yet very powerful force was applied and persevered in without avail.
At last the external lateral ligament was divided by the point of a
very narrow and fine bistoury, and then replacement was immediate and
easy. Some inflammation followed, but was kept within bounds, and the
man regained the use of the articulation. In other cases, again, the
bone is replaced by the use of but very slight force, provided it be
applied, as already stated, in a direction towards the palm of the
hand. The last phalanx is equally liable to luxation in the thumb as in
the fingers, and has no peculiarity of treatment.
Luxation of the Hip-joint.—The great strength of the ligaments,
the depth and fitness of the body and cartilaginous cavity for the
reception of the head of the bone, and the great power of the muscles
surrounding the articulation, render dislocation here both difficult
and rare. The accident is generally produced by great and sudden force,
applied either to the distal end of the femur, or to the farther
extremity of the limb, as by falling from a considerable601 height, by
the foot slipping whilst the person is supporting a heavy weight, by
falls from or with a horse, &c. The luxation, in a great majority of
cases, takes place upwards and backwards, the head of the bone lying
on the dorsum of the ilium. The limb is shortened to the extent of
from an inch and a half to two inches and a half, the toes are turned
in, the thigh is slightly bent upon the pelvis, and very firmly fixed.
Before swelling has occurred, and also after it has subsided, the head
of the bone can be felt lying under the gluteus. The trochanter is
evidently out of place, being depressed, and lying farther up and back
than usual. This is strikingly observable on comparing the injured
limb with the opposite. Attempts to move the limb and effect rotation
produce great pain. Large swelling soon follows, along with greater
stiffness and immobility. If the head of the bone is not replaced, the
pain gradually subsides, and, after some months, freedom of motion is
regained to a slight extent; the patient is able to walk, but with a
great halt.
At first, reduction is accomplished with no great difficulty. Within a
very short time after the occurrence of the injury, before the patient
had recovered from the shock, whilst he still lay sick, faint, and
powerless, I have succeeded in effecting reduction of the femur quite
unassisted,—extending with one hand, grasping the thigh behind, and,
at the same time, rotating it outwards by pressure of the forearm on
the leg, counter-extension being made by the left hand on the symphysis
pubis. When a few hours have intervened, assistance and apparatus are
requisite. The patient is secured by a broad band,—a common sheet suits
very well,—passed under the perineum. The lacque is fixed above the
knee, with a knot that will not run, a towel wrung out of cold water
being applied next to the skin, in order to increase the security
of the hold and prevent excoriation. A well-padded broad iron ring,
tightened on the limb by a screw, and provided with suitable straps
for attachment of the pulleys, is very useful,—fully more convenient
than the common woollen lacque. Extension may be made by one or more
assistants; but this may prove ineffectual, and it is better at
once to have recourse to the pulleys: these are not alarming to the
patient, and, being efficient, will in the end materially diminish his
suffering. The extension should be gradual, steady, and persevering;
the rotation of the limb during extension should be principally
outwards, effected by laying hold of the ankle, and using the leg as a
lever. This motion is peculiarly successful when the bone has yielded a
little to the extension, when it has changed its place, and come nearly
on a line with the cotyloid cavity. In some cases, even of no long
standing, auxiliary means are required,—bleeding, antimony, &c., as
formerly noticed. In old cases, no attempts at reduction should be made
until the patient has been brought into a relaxed state, approaching
to collapse, by one or more of the auxiliary means, and by such as
are best suited to the particular circumstances of the case; in such
instances also the extension, rotation, &c., must be persevered in for
some time,—they are not at once successful. Frequently, particularly
in recent cases, reduction is accompanied and indicated by an audible
and perceptible snap, occasioned by the head of the bone slipping into
the602 cotyloid cavity; the motions are again readily performed, and the
limb resumes its proper length and shape. The muscular and articulating
apparatus must be kept quiet for some time afterwards; a band should
be passed round the knees, and the patient strictly confined to the
recumbent posture; at the same time, fomentations are to be used about
the joint, to the perineum, and to the part where the lacque was
applied. It is rarely necessary to have recourse to abstraction of
blood from the neighbourhood of the articulation.
There is no great risk of the bone again escaping from its situation.
I have but once witnessed such an accident. A female suffered luxation
of the hip nearly a month previously to her admission into the Royal
Infirmary, and reduction was unavoidably deferred for three days more.
It was accomplished without difficulty, and the usual precautions were
afterwards adopted; but next day it was discovered that luxation had
again taken place. The patient had cunningly contrived to have ardent
spirits brought to her, and indulged freely in these, got out of bed,
and slipped down. Replacement was again effected, more easily than
before; the limbs were firmly secured to each other, confinement to bed
and no farther indulgence in liquor were strictly enjoined, and after
thirteen or fourteen days the limb fully regained its functions.
Luxation of the hip downwards and forwards, the head of the femur
lying in the thyroid foramen, is generally produced by a fall under a
heavy load, the thigh being at the same time forcibly abducted. I have
also seen it occasioned by a fall with a restive horse. The limb is
elongated considerably, and advanced a little forwards; the trochanter
major is depressed, the toes are inclined neither outwards nor inwards;
the limb is immoveably fixed, and this most unequivocally marks the
nature of the accident.
The limb is lengthened when the trochanter major is split off, as also
when severe bruise of the glutei has been inflicted without breach of
continuity in any part of the bone, and without displacement. In the
first stage of morbus coxarius, too, a somewhat similar appearance
and position of the limb is presented; there is lengthening, but then
there is also more or less wasting of the muscles, more mobility than
in the dislocation, and a marked history attached. Complicated cases
occasionally occur—as when a patient who has been labouring under
hip-joint disease, perhaps not in an aggravated form, falls heavily,
and on being lifted up is found to be incapable of moving the joint,
the limb at the same time being elongated, and having a distorted
appearance. An instance of this nature impressed strongly upon me the
great necessity for accurate diagnosis in the first instance, and
that such was to be acquired only by taking every circumstance into
consideration. A young man was engaged in cleaning a slaughter-house,
standing on two blocks of wood with his legs considerably apart. One of
the blocks suddenly slipped from under him, and he fell with his limbs
spread. He was carried home in great pain, and next day I was asked to
visit him. The limb was elongated, and the hip flattened; the joint was
stiff, and attempts at motion produced great pain; but by perseverance
the limb could be put in various positions, and the trochanter was not
so much depressed as in luxation downwards. By cross-examination603 it
was discovered that the patient had halted in walking for many weeks
previously, had felt as if the limb was longer than the other, had pain
in the groin and knee; in fact, morbus coxarius had been advancing, and
the pain, immobility, and greater elongation had been occasioned by
the fall, causing violent excitement of the morbid action previously
in progress. Dreadful consequences must have resulted from mistake
in diagnosis and practice founded upon it. I have observed, in other
cases, great and rapid elongation of the limb in consequence of injury
to the hip-joint previously diseased; and I have known instances in
which persevering and forcible efforts were made to reduce the supposed
luxation.
The reduction is in many cases difficult. In young and muscular
individuals, after the lapse of some hours, when reaction has occurred,
the muscles are rigidly contracted, and the head of the bone is not
easily dislodged. Extension, made to a certain extent and continued, is
not so useful or essential here as in other forms of luxation of this
joint. Adduction, carrying the injured thigh quickly and forcibly over
the other, is generally successful; and the reduction is favoured by at
the same time raising up the neck of the bone, by means of a towel or
wooden roller passed under the upper part of the thigh. There is also
no such advantage from rotating the bone as in other luxations. It is
very often necessary, even in recent cases, to adopt measures to weaken
muscular exertions; and again, in cases of three weeks’ duration, I
have found no difficulty.
The head of the bone, when dislodged from the foramen obturatorium,
may slip past the cotyloid cavity, for it is impossible to regulate
its direction; it comes to be acted upon by muscles which have been
displaced, some being compressed and partially paralysed, whilst
others are excited; they have been put out of their usual condition
and relation, and act irregularly. The head of the bone may, from this
cause, get into the sacro-ischiatic notch. This has occurred to me; but
I have found no difficulty in removing it from thence, and effecting
reduction satisfactorily.
Displacement into the sacro-ischiatic notch is attended with great and
remarkable inversion of the toes, slight shortening of the limb, the
prominence of the head of the bone felt under the gluteus maximus.
It is the least common form of luxation. Reduction is attempted by
extension and rotation outwards, at the same time pulling the head of
the bone towards the acetabulum by means of a towel passed under the
thigh.
Luxation of the head of the femur on the pubes is perhaps more frequent
than any other, excepting that on the dorsum of the ilium. The limb
is not much shortened, the toes are everted, the trochanter major is
depressed, and nearer to the anterior superior spinous process of the
ilium than usually, and the head of the bone is both seen and felt
prominent in the groin. Much pain, swelling, and sometimes more or
less paralysis of the limb, are occasioned by this displacement; the
femoral artery and vein lie immediately interior to the head of the
bone, and are compressed, and the crural nerves are stretched over it.
In attempting reduction, rotation inwards should be employed during
extension, accompanied with endeavours to lift the upper part of the
bone towards the acetabulum.
604
[Congenital Luxation of the Hip-joint is sometimes met with, though
on the whole a very rare affection, especially in this country.
Female children are more apt to suffer from it than males, and it is
also more common in such as are of a scrofulous habit than in such
as are endowed with a good constitution. Of twenty-six cases of this
malformation observed by Dupuytren, not above three or four were males;
a disproportion probably not altogether dependent upon chance. The
immediate causes of this variety of displacement are, first, shortness,
total absence, or extreme obliquity of the neck of the thigh-bone;
secondly, partial or entire obliteration of the cotyloid cavity;
thirdly, deficiency, extraordinary elongation, or complete absence of
the round ligament.
The characters of this malformation are, shortening of the affected
limb, unnatural projection of the great trochanter, ascent of the head
of the femur into the iliac fossa, inversion of the leg, and obliquity
of the pelvis. The motions of the joint, particularly those of
abduction and rotation, are constrained and imperfect; the muscles of
the upper part of the thigh are retracted, or drawn towards the iliac
crest; the limb is thin, wasted, and out of all proportion to the rest
of the body; the tuberosity of the ischium is almost uncovered, and
consequently unusually prominent; the upper part of the trunk is thrown
backwards, while the lumbar portion of the spine projects forwards,
being concave behind; the pubes is placed almost horizontally on the
thighs; and the ball of the foot alone touches the ground when the
child stands erect.
In the recumbent posture, when the weight of the trunk is taken off,
and the muscles are relaxed, most of the symptoms of the luxation
disappear, and the limb may be shortened or elongated at pleasure. In
walking, the body is inclined towards the sound side, and the head
of the dislocated bone sinks towards the cotyloid cavity by its own
weight. As age advances, the limb becomes shorter, in consequence of
the femur ascending higher and higher on the ilium; the obliquity of
the pelvis augments; and the power of locomotion, already so much
impaired, is completely destroyed.
Congenital dislocation of the hip-joint may, in general, be easily
distinguished from other accidents or maladies, by the affection being
observed at or soon after birth, by the obliquity of one or both
thighs; by the absence of pain, swelling, and ulceration; by the head
of the femur being displaced without any external violence; and by the
ability of the surgeon to lengthen or shorten the limb at pleasure. In
disease of the hip there is always more or less pain, with a feverish
state of the system, and gradual failure of the strength; the parts
about the joint are tense and swollen; the limb, at first somewhat
lengthened, becomes afterwards shortened, and cannot be extended
without the greatest suffering; and the motions of the ileo-femoral
articulation are forever impaired.
The post-mortem appearances vary. In general the cotyloid cavity
is partially obliterated, or entirely deficient, being replaced by a
small, irregular, osseous prominence, devoid of cartilage and synovial
membrane; the head of the femur, often flattened at its antero-internal
aspect, rests in a sort of superficial fossa on the dorsal surface of
the ilium; the round ligament, as was before remarked, is elon605gated,
partially worn away, or even altogether absent; and the surrounding
muscles are either atrophied, transformed into a species of yellowish
fibrous tissue, or preternaturally developed. In the latter case, their
action is preserved; in the former, it is very much restricted, or
totally impeded.
The prognosis is always unfavourable, as the patient dies either young,
or remains permanently lame and deformed.
The treatment can be only palliative; and as the weight of the trunk
is the main agent in aggravating the displacement, repose is obviously
indicated: but it is not necessary to confine the patient to the
recumbent posture; since, in the act of sitting, there is no stress
on the femur, the body resting principally on the tuberosities of the
ischia. Dupuytren thought favourably of the cold bath: it should be
strongly impregnated with salt, and the body immersed for three or four
minutes at a time. He was also in the habit of using a well-stuffed
belt, about four inches wide, for surrounding the pelvis and fixing the
great trochanters; thus binding the ill-adapted parts together, keeping
them at the same height, and preventing that continued motion to which
they are otherwise so much exposed.]
Luxation of the Bones of the Leg.—separation of them from the end of
the femur—seldom occurs. It can be the effect only of great violence
and great laceration. Most frequently fracture is concomitant, perhaps
with wound; and such accidents require amputation, either primarily
or secondarily. Subluxation, from laceration of the internal lateral
ligament, is not so unfrequent. It is most common in females, the
natural conformation of their thigh-bones disposing them to bend
inwards; and from falling awkwardly, particularly if carrying a weight,
the ligament is apt to give way. The limb is pained, deformed, and
unable to support the body, and swelling to a considerable extent soon
follows. Reduction is extremely easy; and the parts are retained in
site by the application of a wooden splint, to either the outer or
the posterior side of the joint, the leg and foot being previously
bandaged. The joint remains long weak, and never recovers entirely; a
sustaining apparatus, fitted on the outside, retained by straps, and
with a joint opposite to the articulation, is required to be constantly
worn when the patient wishes to use the limb.
Luxation of the Patella is spoken of by some as common. Others of
much experience have not met with a single instance of it. I have
never seen this accident. The bone, it is said, may be displaced
outwards, inwards, or upwards. The first form of luxation is the
most frequent, and is caused by a severe fall, with the foot twisted
outwards and the knee inwards. Displacement inwards is produced by
direct violence applied to the outer part of the bone, or by the foot
being turned inwards in a fall. Displacement upwards can occur only
after laceration of the ligamentum patellæ, the bone being then drawn
up by the unresisted action of the muscles on the fore part of the
thigh. In dislocation outwards, the bone has been found “resting with
its inner edge upon the outer surface of the condyle, the fore part
facing obliquely forwards and inwards.” In this last form of606 accident,
sudden, forcible, and complete flexion of the limb is said to produce
immediate reduction. In dislocation outwards or inwards, the muscles
are to be relaxed by raising the heel, extending the limb, flexing the
thigh, and then forcing the bone to its proper site by manipulation. In
the dislocation upwards with rupture, the limb is to be kept extended
and raised, and the bone is brought as nearly into its place as
possible by bandaging. When a peculiar laxity of the apparatus about
the joint exists, whether as a cause of luxation or not, the support of
a well-made knee-cap is required.
As formerly stated, Dislocation of the Ankle cannot take place
inwards or outwards, without fracture of the end of the tibia or of the
fibula, either above the articulation, or where they project by the
sides of the astragalus for the greater security and strength of the
joint. Subluxation, however, or sprain, may occur without injury of
the bones: in this accident, should the parts not have spontaneously
resumed their original situation, no difficulty is experienced
in putting them to rights; simple manipulation is sufficient.
Occasionally, the foot is luxated forwards, by force applied either
to the heel or to the fore part of the leg whilst the limb is fixed.
The heel is shortened, the foot elongated; indeed, the marks of the
injury are so distinct, that comparison of the limbs is sufficient for
diagnosis. Luxation may also take place backwards; and in this case
the heel is elongated and the foot shortened. In these accidents it
is not unfrequently found that one or other malleolus has given way,
or that the lower end of the tibia is split. Reduction is sometimes
difficult. Extension is to be made by grasping the foot and pulling
whilst the limb is fixed, at the same time making pressure either
backwards or forwards, as may be required. To retain the bones in their
proper situations, it is always necessary, at least prudent, to apply a
paste-board or leathern splint to each side of the limb, particularly
when fracture of the malleoli is conjoined.
Displacement of the Bones of the Tarsus may result from great force;
for example, when the foot is squeezed under a heavy weight, one or
more bones may escape from their connections, and project. Reduction of
such displacement is exceedingly difficult at any period, and becomes
almost impossible when inflammatory action is allowed to supervene
previously to attempts being made. The astragalus is sometimes pushed
out of its place; though it is difficult to conceive how, to a bone so
hid and so firmly connected, such force should be applied as to cause
protrusion of it from its natural situation. It has been found lying
on the dorsum of the foot, causing swelling, lameness, great pain,
shortening and deformity of the limb; and the shape of the bone can, in
such circumstances, be distinctly felt and seen through the integument.
As already observed, reduction is almost impracticable, and, with
the view of remedying deformity, it has been proposed to cut out the
displaced bone; but as to the expediency of such practice I can give no
opinion.
I have seen but one instance of displacement of this bone backwards,
and most probably another will never occur to me. A heavy young man,
in a state of utter intoxication, fell backwards down a607 stair, and in
the fall his foot became entangled in the railing. The astragalus was
found lying betwixt the back of the tibia and the tendo-Achillis, its
upper articulating surface facing forwards, the lower in contact with
the tendon. All attempts to reduce the bone proved fruitless. Violent
inflammatory action followed, but was reduced by active measures; and
the limb ultimately became very useful; in fact, though not till after
many months, little lameness or shortening was perceptible.
By Sprain is understood subluxation or partial displacement of a
joint, with stretching, and more or less laceration of the articulating
apparatus—ligaments, tendons, sheaths, and bursæ, being all involved
in the injury. Sometimes small portions of the processes of bone are
separated, being torn away, attached to ligament or tendon. All joints,
both large and small, are liable to the accident. In the proximal,
or in the middle joints of the finger, for example, one or other
lateral ligament is stretched or torn; the finger is twisted to a
side; the joint is swelled; and this swelling, with pain, is of long
continuance, perhaps increased by repeated twists, or by imprudent
use of the joint. The elbow and shoulder are frequently sprained, as
also the hip and knee; but the injury most frequently occurs in the
wrist and ankle. It is generally occasioned by a fall, the foot or
hand coming awkwardly to the ground, the muscles being at the time
relaxed and unprepared; by over-exertion in lifting heavy weights; by
entanglement and twisting of the limb, &c. The ankle is often sprained
by what is called a false step; the fore part of the foot comes in
contact with an obstacle unexpectedly, the foot is twisted under the
limb, the weight of the body is thrown on the apparatus of one side
of the joint, and this is in consequence immoderately and unnaturally
stretched. Violent pain immediately occurs, and the patient is sick and
faint. Discoloration and rapid swelling take place from extravasation
of blood into the cellular tissue, into the sheaths of the tendons,
and perhaps into the synovial pouches, in consequence of laceration of
the bloodvessels. Effusion of serum and increased secretion of synovia
afterwards occur, from incited action of the vessels. Thus the joint is
deformed. Attentive examination is required to guard against mistakes;
the existence or non-existence either of displacement or of fracture
must be at once ascertained by determined and perfect manipulation; the
parts must be pressed and moved, to such an extent as is necessary,
notwithstanding the pain thereby occasioned, and notwithstanding the
resistance afforded by the patient. It has been already stated that
luxation of the wrist is not uncommon; that separation of the one bone
of the forearm from the other, and transverse fracture or splitting of
the radius, at the distal extremity, are accidents by no means rare.
Great disfiguration follows simple sprain, much swelling taking place
on the fore part of the limb from effusion under the fascia, and there
is also much serous and bloody infiltration of the cellular tissue on
the back of the hand and forearm. In the ankle, the ends of the bones
must be carefully examined, and also the fibula in its whole extent,
that the existence or non-existence of fracture may be ascertained, and
that the surgeon may be guided to a correct mode of treatment. If the608
joint is not put at rest immediately, the extravasation is increased,
and, in consequence, the pain and inflammatory swelling also; and parts
of the joint at first not involved in the injury may thus be made to
suffer. Many diseases of synovial membrane and articulating cartilages
are attributable, and can be traced, to badly managed sprains; and
in some constitutions, but slight injury, combined with a little bad
treatment, suffices to destroy a joint. When, the case is well managed,
the pain is never great, and soon abates; the swelling after a few days
slackens; the discoloration becomes greater, the serum being absorbed,
and the effused blood shining through the skin; the integuments
appear green, blue, red, purple—these hues either being present all
at the same time, or occurring successively; the discoloration often
extends far from the joint. The mobility and strength of the joint are
recovered gradually.
Perhaps no injury is more frequently mismanaged, by those both in and
out of the profession. Every old woman thinks she can cure a sprain;
most absurd and hurtful measures are resorted to; the injured parts
are kept in motion; cold lotions and cold effusions are employed, and
at the same time stimulating frictions: probably attempts are made,
either by leeching or by puncturing, to extract the effused blood; and
many similar follies are committed. The proper treatment certainly
appears to consist principally in absolute rest and position. If there
is any displacement it must be rectified immediately. If there is any
fracture; or if there is a tendency to redisplacement after reduction;
or if the patient is restless either from folly or from insensibility,
as when the head has been injured by the accident, when the patient
is under the influence of strong liquors, or when he labours under
delirium tremens,—a splint or splints must be applied to secure
immobility of the parts, at the same time without such compression as
may interfere with swelling from effusion; the effusion is a salutary
process, and should be encouraged, not repressed. By absolute rest
and elevation of the limb, the extent of the swelling is limited, and
inflammation warded off. Fomentations, properly employed, afford much
relief; at first they probably encourage the serous effusion. The
integuments soon become relaxed, during the regular use of fomentation,
and tension and vascular action subside, as also pain. The swelling
then abates, and is no longer hard; it pits on pressure, and the skin
has a puckered appearance. Then gentle friction becomes advantageous,
and uniform support should be afforded by the application of a flannel
roller. The longer the limb is disused, the more perfect and rapid is
the recovery, provided the rest of the cure be properly conducted. In
general nothing more than what has been stated is required. But if
the limb be moved, or stimulated in any way, early, then necessity
will arise for antiphlogistic measures—perhaps venesection, certainly
copious and repeated abstraction of blood by leeches, accompanied with
fomentations, and the internal exhibition of antimonials, purgatives,
&c. When such is the case the cure is tedious, the joint long remains
swelled and stiff, the patient is lame and incapable of exertion.
Leeching or puncturing at an early period, with the view of allowing
extravasated blood to escape, is useless and hurtful. The effused and
coagulated blood cannot be evacuated, and suppuration, followed609 by
destruction of the cellular tissue, has often been the consequence of
such ill-advised proceedings. Friction with stimulating liniments,
or even simple friction, at an early period, is also hurtful, as
tending to excite vascular action, and to convert simple swelling
into inflammatory. The application of cold at any period is of little
use, and ought certainly to be avoided immediately after the injury,
as adding to the sufferings of the patient, and interfering with the
natural processes which have commenced for the reparation of that
injury.
In limbs that have remained stiff after severe and mismanaged sprain,
the dashing of water, either cold or tepid, has been strongly
recommended. The practice is not ineffectual; the vessels of the
surface are excited, perhaps as by other friction, and perhaps by
the reaction which follows the chill. But the limb is apt to become
rheumatic; and, on this account, the state of matters will not be
improved by this proceeding, unless it be resorted to with proper
precautions.
In severe sprains there is reason to think that sometimes even the
tendons yield a little—that many of the fibres give way, and that
thus the tendon is thinned and elongated. Such injury happens often
in horses, in what is called breaking down. In them the tendon is
occasionally snapped entirely through, and the ends widely separated.
The same occurs in the human subject. Separation of the muscular
fibres, however, is rare; laceration of the tendon itself, or
separation of the tendon from the muscle, is more common. The yielding
of the broad tendons on the upper and fore, lateral and under parts
of the abdomen, affords an example of laceration of tendinous fibre
from violent exertion. The tendons of the limbs are more frequently
injured, and in the lower oftener than in the upper. I have more than
once seen the tendon of the biceps torn in violent exertion. In the
thigh, too, some fibres occasionally give way from a similar cause.
The supra-muscular fascia in the arm and thigh is apt to give way at
one or more points during powerful exertion of the muscles, causing
deformity by protrusion of muscle through the torn space. But it is
in the apparatus for extending the foot, and raising the weight of
the body, that laceration of tendon most frequently takes place.
The accident is uncommon till after the middle period of life, when
the body has become heavier, when muscular exertions have been less
habitually practised, and when the fibre has grown more rigid. The
person in raising himself over some slight obstruction in walking,
perhaps attempting to pass a small ditch or stile, suddenly “breaks
down.” Or in dancing,—an amusement which he has long discontinued—a
sudden snap is felt, with immediate lameness and slight pain in the
back of the limb; swelling and discoloration follow; and these symptoms
and signs vary in intensity according to the extent of the injury.
Laceration may have been slight; the pain, swelling, and lameness are
proportional, and at first an inconsiderable void can be felt at the
upper part of the tendinous termination of the gastrocnemii. Sometimes
no change is perceptible, and in such cases some have been of opinion
that the slender tendon of the plantaris has given way and caused
the lameness; but this is doubtful, and it seems more probable that
stretching and yielding has taken place in some part of the tendon
of the gastrocnemii, which610 had been in powerful action—probably,
the tendinous and muscular tissues have been separated to a slight
extent. Occasionally the tendo-Achillis is found completely torn
through, and its upper end retracted; in such cases a large space is
occasioned at the injured part, when the knee is extended and the
foot bent. Sometimes the tendo-Achillis is cut through; I have seen
both completely divided in the same individual—he received a wound
by a cutlass across the back of both limbs, while endeavouring to
escape from the mate of a vessel, in which he had been stealing. In
rupture without breach of surface, the torn bloodvessels pour out their
contents into the cellular tissue to a considerable extent, and if a
proper mode of cure be not adopted immediately, inflammation quickly
supervenes; and this is apt to terminate very unfavourably in the
infiltrated tissue.
The tendon is united by the deposition of new matter, and the
conversion of this into substance resembling the original structure
from the vessels of which the deposit has taken place. The quantity
of new formation necessarily depends on the extent of laceration and
the space thereby occasioned. That such reparation of tendon does take
place, and that to a very great extent occasionally, is placed beyond
all doubt by the results of veterinary practice. “Knuckling over” in
horses is occasioned by contraction of the flexor tendon; the heel
does not reach the ground, and in order to effect this the tendon has
been in many instances completely divided. The cut ends immediately
separate, to the extent of some inches, and after a time this large
space is filled up by a substance similar to tendon; so similar,
indeed, that on post mortem examination, some years afterwards, a
careless observer could scarcely distinguish any difference in the
appearance of the various portions of the tendon. The same is observed
after the operations for deformity of the foot in the human subject.
The treatment of lacerated tendon consists in placing the parts so as
to relax the muscles whose tendons have suffered. In rupture of the
tendo-Achillis, the knee should be bent and the foot extended, relaxing
the muscle and approximating the separated ends. This is readily and
conveniently affected by placing a slipper on the foot, and attaching
to its heel a firm band, which is then fastened to a ring or strap
placed on the thigh. This apparatus must be worn for six or eight
weeks. Afterwards a high-heeled shoe should be used for some time; or
if the union be still weak and imperfect, a splint may be placed on the
fore part, resting on the dorsum of the foot and the fore part of the
leg.
Bruise.—The effects of bruises or contusions are, separation of the
cellular connexions, rupture of bloodvessels, and effusion of their
contents into the cells; a cavity, often large, is thus formed partly
by the direct injury, and partly by the subsequent effusion, and this
is quickly filled with blood, partly fluid and partly coagulated.
Immediate tumour forms; and the integument is discoloured, often beyond
the principal swelling. The injury may, or may not, be attended with
division of the integuments, or with fracture or displacement of the
bones; but all injuries of the hard parts are attended with more or
less bruising of the soft. Bruise is most frequently produced by611 a
blow, and is most severe when the violence is resisted by an unyielding
part, as by bone; a squeeze between two bodies, particularly if they be
in motion, also inflicts extensive contusion. The swelling continues to
increase for some time, and then gradually disappears along with the
pain. As the tumour subsides, the discoloration increases; the thinner
parts of the effusion have been absorbed, and the clot then shines
through the skin, imparting to it various hues.
Bruise may be followed by inflammatory action. Then effusion is
increased, bloody fluid is poured both into the cavity and into the
unbroken cellular tissue, the whole parts become extremely tender,
the surface inflames, and the excited action is apt to terminate
unfavourably in the various tissues. Not unfrequently sloughing takes
place, both of the skin and of the cellular tissue and fatty matter,
with unhealthy suppuration and infiltration; and constitutional
disturbance accompanies. All this is likely, nay, certain, to follow
admission of air into the cavity filled with effused blood, whether
by accidental wound or by intentional division of the integument.
Meddlesome surgery is unfortunate here, as well as in many other
cases. After scarifications, punctures, leechings, or incisions, the
blood often seems to undergo a putrefactive process, and unhealthy
suppuration is quickly established.
Sometimes the clot is not entirely absorbed, and considerable
swelling remains for a long time, perhaps with slight tenderness of
the part; a foundation is thus laid for abscess, either chronic or
acute. Frequently the inflammatory action following on bruise is not
so violent and rapid as that above described, but is limited in its
consequences chiefly to the effusion of coagulable lymph. This may
not be altogether absorbed along with the other effusion, it may
become organised, and be the nucleus or germ of a new growth, of a
tumour contrary to nature—deposit increases in and around the nucleus,
and this formation, though at first of a simple nature, may become
rapid in its growth, and may assume a troublesome or even a malignant
action; and sometimes all this may occur at an early period, before the
attention either of the patient or of the practitioner has been drawn
to the action or to its effects. Many tumours can be traced to the
effects of a bruise.
In the treatment of bruise, the parts should be placed in a state of
absolute rest, and methodically fomented. Local bleeding is seldom
required, and is of little use; at first it is hurtful. When, from the
extent or number of the bruises, fever follows, general antiphlogistic
measures must be resorted to. Cold and astringent applications, and
other repercussives, as also stimulants, are pernicious in the first
stage, and are not very useful at any time. Opening of the cavity must
be carefully avoided, excepting when absorption has ceased, when the
tumour has increased and become painful, and when the effused blood is
putrescent, and unhealthy suppuration has commenced. Then the cavity
should be opened freely, and by poulticing the clots and sloughs
are got quit of; afterwards the parts must be supported, as also
the strength of the patient. When from long want of use, in tedious
cases, the parts have become cold, shrunk, and weak, as also happens
in sprain, friction, champooing, tepid affusion, passive motion, and
voluntary motion short of giving pain, will612 all be of use as tending
to restore the circulation, the nervous energy, and the muscular
development. If œdema remain, bandaging or a laced support will be
required.
Amputation.—Every endeavour, which skill and experience can suggest,
must be made before mutilation of the body, by the removal of even
the smallest portion of one of its members, is resorted to. But
there are cases in which mutilation, though a harsh remedy, is still
indispensable for the saving of life. There are others in which it is
prudent and proper to resort to operation, in consequence of a member
becoming perfectly unserviceable, and likely to impair the usefulness
of the individual. Such are very bad and complicated fractures and
luxations—laceration of the soft parts of a limb to such an extent as
to impress the experienced surgeon with a certainty that in a short
time gangrene must ensue, and render the success of any attempt to
save life very problematical. When the extent of injury is such that,
though gangrene may not be dreaded, yet it is plain that extensive
suppurations and exfoliations must necessarily take place, a question
may arise as to whether immediate amputation is to be performed or
not. This will be decided by the circumstances in which the patient is
placed, and often also by his own feelings upon the subject. He may
choose to run some risk, and endure much suffering, with even a very
slight chance of ultimately preserving his limb. In cases of traumatic
gangrene of the chronic form, amputation is not only justifiable, but
imperative; as also in those cases of severe fracture in which the
patient is sinking under profuse discharge, with disunited bones. And
the same absolute necessity for operation exists in many diseased
joints, and in some diseased bones, when the patient’s safety would
otherwise be endangered, or when, on mature consideration, it is
evident that the member, if retained, must for ever be an encumbrance,
and worse than useless. Certain tumours of bones, tumours involving
joints, tumours and ulcers of the soft parts of a malignant nature, and
without appreciable disease of the lymphatic system, will also demand
recourse to the amputating knife. Patients, too, will be met with,
who, after undergoing all the suffering attendant on disease of long
duration—as exfoliation of bone and sloughing of tendons, following
deep suppuration—will, to get rid of the annoyance of the stiff and
deformed member, or part of a member, not only submit to, but urge and
insist on, the removal of the offending part. Amputation will also
occasionally be required for badly-formed stumps, as those in which
the end of the bone protrudes through ulcer of the integument, and is
necrosed—or those in which the bone has been sawn of an inconvenient
length.
Many precautions are to be observed in this operation. It is not to be
commenced without due consideration as to the position of the operator,
and of his assistants—their several duties—the form of incision—the
length of the stump—the difficulties, if any, which may be expected,
and the best means of obviating them. The most prominent objects are,
to save undue effusion of blood, to effect the incisions with as little
suffering to the patient as possible, and to make them of such a form
as to cover the end of the bone effectually613— so that pressure may,
after a time, be borne without risk of ulceration of the soft parts, or
exfoliation of the bone.
In all cases, and in all situations and circumstances, hemorrhage
can be restrained during completion of the incisions, and during the
employment of means to close the cut ends of the vessels, by means of
very slight but exact pressure on the trunk of the principal vessel.
The point at which this is to be applied should be at as short a
distance as possible above the place of incision, and at the same time
above the origin of any branches which must be cut. Not the slightest
pressure should be made until the instant when the incisions are
about to be commenced, so that no venous congestion may take place
in the limb. All the blood in the limb, below the incisions, must
necessarily be lost. The veins are more easily compressed than the
arteries, and pressure, made a short time before the operation, may
arrest the return of the blood, whilst it may not completely stop its
influx; thus engorgement of the lower part of the limb is produced, and
the quantity of blood that must be lost is increased. For a similar
reason, pressure, sufficiently firm to stop arterial hemorrhage, is to
be continued till the principal branches are tied, and then entirely
removed; for the continuance of even slight pressure will increase
the flow from the surface of the stump—blood, flowing in, and being
arrested in its venous return, trickles out through the open ends of
the veins. If a circular band be used for the compression, such as the
screw tourniquet, it should be put on quickly, and screwed up at once,
and then the incisions should not be delayed one instant after; there
should be no relaxation of the pressure at any part of the operation;
and as soon as the principal vessels have been secured, the apparatus
should be altogether removed—otherwise, as already stated, rapid oozing
will continue from the face of the stump. It is my confirmed opinion,
that much more blood is lost from the use of a tourniquet than without
it. I would rather trust to a no very efficient assistant, than put on
a tourniquet. It is evident that compression on the whole circumference
of a limb must completely interrupt venous return, and cause the
increase of hemorrhage already mentioned; whereas pressure on only two
points of the same circumference, as is effected by the hand of an
assistant, is not liable to this objection. Besides, the latter mode
is more quickly applied, and more readily removed, causes infinitely
less pain to the patient, and is equally effectual in arresting the
flow in the main arterial trunk. Neither does it interfere with the
due contraction and retraction of the divided tissues. The incisions
should always be made rapidly; and after their completion, the surgeon,
if distrustful of his assistant, or if his hand has become cramped and
tired, may himself grasp the limb and compress the vessel, giving the
forceps or ligatures to another.
The first step in the operation is to arrange the measures for
temporary arrestment of the bleeding. The patient is placed in a
favourable position, either sitting or lying, as may be most convenient
for the particular amputation, and is firmly secured by one or more
assistants; all the apparatus must be in good order and conveniently
placed, and an assistant should be stationed to attend to them, and
hand those required. The compressor and the operator are each at614 their
post, and ready to act in concert. The incisions may be made either
from without inwards, or from within outwards, after transfixion of the
limb. The latter mode is to be preferred when practicable, as requiring
less pressure; the parts are more stretched than in the former method,
are therefore more easily and rapidly cut, and consequently less pain
is inflicted. To the inexperienced transfixion may appear cruel, it may
appal them, but in reality it is almost unattended with pain; it is
rapidly executed, and renders the operator capable of completing his
work with great quickness and little suffering, and at the same time
with neatness and precision. The knife should be of a size and length
proportioned to the incisions, straight-backed, and with a good point;
of a form to pass through readily, yet strong, and not too broad. With
one sweep of this, the incisions are made at once, through the muscles,
through the cellular and fatty tissues, and through the integument—or
vice versâ if the mode from without inwards be preferred. By these
parts being cut rapidly and at once, their connexions with each other
are not separated, the cut surface is smooth, and the parts are in
the most favourable state for becoming agglutinated and consolidated;
the bone is more deeply covered, and the stump of a handsomer and
more useful shape, than when the parts are cut successively and with
detachment.
The operator places himself so that he may grasp the part to be
removed, during the sawing of the bone, without change of position.
The incisions are made with the left hand free; but as soon as the saw
is in the right, the left should take firm hold of the limb below the
wound. During the operation, the limb is supported by an assistant,
either sitting or kneeling before the patient; but the regulating of
the position of the limb, during sawing, is not to be intrusted to
him alone. He may, from anxiety to facilitate the action of the saw,
snap the bone and splinter it when it has been little more than half
divided; or, from dread of this, he may lock the instrument, and so
delay completion of the operation. The management of the lower part of
the limb should always be by the person using the saw. This instrument
should have its teeth well set, and be provided with a workmanlike
handle. It is worked steadily and not hurriedly, with very slight
pressure, and that pressure employed only when pushing forwards.
Before its application, all the soft parts must necessarily be divided
completely; and this is done by carrying the knife, after formation
of the flaps, round the bone, with its edge rasping on it, and as
high up as possible. The instrument is then placed accurately on the
point thus exposed, close to the soft parts, and during the sawing the
flaps are well retracted by the hands of an assistant. The saw may be
worked either horizontally or vertically; the latter direction is to be
preferred, for thus, when the section is nearly completed, the uncut
part of bone is deep, and less likely to snap on the weight of the limb
being allowed to operate, or when undue pressure is made downwards.
If splintering of the bone have occurred, whether from neglect of the
foregoing precautions, or by other accident, the sharp projecting parts
should be taken away, and the cut surface made quite smooth by means
of the bone pliers; and with this instrument also, the sharp edge of
the bone may be rounded off, in cases615 where subsequent pressure might
cause ulceration or sloughing of part of the integument of the stump.
The arteries are tied close to their connexions. Their cut ends are
laid hold of with the dissecting forceps, or by those represented at
page 170, and pulled out; a small firm thread, either of linen or silk,
is then applied tightly, and one end immediately cut away close to the
reef-knot. Separation of the ligatures generally takes place from the
sixth to the tenth or twelfth day; they produce little discharge or
irritation during their presence, and no source of irritation connected
with them is left behind. But when both ends are cut away close to the
knot, separation is often long of taking place, and though the parts
may heal over them kindly enough, the stump never can be considered
sound till all are discharged. Probably several of these knots remain
deeply imbedded after cicatrisation of the integument, and when the
patient considers himself cured, and is moving about the room or ward,
actively and cheerfully, painful hardness forms deeply, part of the
stump reddens and swells, matter forms, and at length the insignificant
origin of the mischief is discharged; and this may occur more than
once. Generally such suppurations are limited, and soon cease; but
occasionally the abscess formed round the knot is extensive, deep and
free incision is required, the filling up of the cavity is necessarily
slow, the cure is long protracted, and both practitioner and patient
are disappointed and annoyed. Besides, the suppurations thus
occasioned, though slight in extent, may, when in the neighbourhood
of a principal arterial branch, cause ulceration of the coats of the
vessel, producing troublesome hemorrhage at a late period. All these
untoward consequences of cutting off both ends I have experienced in a
series of cases, and from the results of a faithful comparative trial
of both methods, I am now fully determined always to leave one end of
the ligature hanging from the lips of the wound.
No one now, it is presumed, dreams of the absorption of ligatures,
whether composed of animal substance or not; therefore the catgut
ligature, at one time much recommended, has no superiority over the
linen or silk thread,—besides it is not so convenient of application.
Twisting or bruising the cut ends of arteries has been long known as
effectual in arresting bleeding. Vessels of a large size can be so
treated with sufficient facility, and they may not bleed after; but
well-tied ones are much more secure. The smaller cannot be pulled out
and twisted, ligatures must be used for them; and the application of
one or two more ligatures, namely, to the large arteries as well as the
small, will add to the patient’s safety, and to the operator’s comfort
and peace of mind, and can have little effect in increasing irritation.
I have made trial of the method of torsion after amputation, and for
the above reasons, and because the manipulations are more tedious, I
disapprove of the plan, and decidedly prefer the ligatures. I am not
aware that the proposal of leaving the vessels both untwisted and
without ligature has been tried in this country; one would think that
it must always be troublesome, and not unfrequently hazardous.
In some cases, as when the incisions are made in the neighbourhood of
diseased bone, the soft parts are so condensed that the vessels cannot
be pulled out by means of the forceps; they are to be616 transfixed by
a sharp hook or tenaculum, and a ligature is then applied round the
parts which the instrument holds; or the vessels may be encircled by a
thread passed round by means of a curved needle; in both methods more
or less of the surrounding tissues must necessarily be included in the
noose, though always as little as possible. Sometimes an artery of the
bone, whether sound or inflamed, bleeds sharply; in such circumstances
the application of ligature is impossible, and I have occasionally been
obliged to insert a wooden peg into the opening; to this a chord is
attached by which it can be removed after a few days.
When bleeding has been satisfactorily arrested, the surface of the
wound is to be cleaned of coagula, either with the fingers or with
a warm and soft sponge, the ligatures are brought to the margin at
convenient points, and the edges of the integument are then put
together by interrupted sutures—two, three, or more, according to the
extent of the wound. They need not be numerous, for they are only
temporary, effecting partial approximation, and showing the line in
which the parts are to be brought together by the after dressing.
The stump is then covered with lint soaked in cold water, and this
application is renewed frequently so long as any trickling of blood
continues. Farther dressing is delayed for six or eight hours, when
the oozing has entirely ceased, and the visible cut surface become
glazed. Under this management, there is less chance of bleeding
breaking out afresh than when the limb is encompassed by bandages
and pledgets of lint, perhaps compressed so as to interfere with the
return of the blood, and heated by superfluous dressings. If bleeding
to any extent should occur, as there is always a risk of, after the
patient has become warm and comfortable in bed, and reaction has been
established, there is but little pain or annoyance in reaching the
bleeding point, and taking measures to stop the flow; the few stitches
are soon clipped away, and then the surface of the wound is completely
exposed, and ligatures can be applied to those vessels which require
them. Then, after removing all coagula, sutures are placed in the same
perforations, and the stump is in as favourable a state as previously.
I now generally leave the wound quite open, until all risk of
hemorrhage has ceased, and, if one or two stitches are required, these
are put in at the time of applying the plaster.
After six or eight hours, as already stated, any clots that have
formed are to be taken away gently, and the glazed edges of the wound
are then brought accurately and neatly together by the adhesive
composition already recommended,—with the difference of its being
spread upon slips of oiled silk, which I have found to be more pliable,
and altogether preferable to the glazed riband. Interstices are left
for the sutures and the ends of the ligatures, and the latter may
now be abridged slightly. This mode of keeping the edges in contact
I can confidently recommend from experience. The plasters are much
more adhesive than those in common use, do not irritate, and are not
loosened by discharge. After twelve or twenty-four hours, often much
earlier, the sutures are clipped through and removed. No other dressing
is required till the end of the cure, provided this proceed favourably.
The part is kept cool, and the slight discharge which occurs in a day
or two is wiped617 up from time to time, if it be in such abundance as
to reach the oiled cloth over the pillow on which the stump is laid.
No disturbance of the parts is necessary as when ointments, bandages,
and compresses are employed, or straps that require frequent removal
and reapplication. The patient suffers comparatively nothing; and the
surgeon is saved much troublesome and dirty work,—for union by the
first intention seldom fails.
Bleeding within a few hours after the operation, before excited action
of the vessels has commenced, is easily arrested by exposure of the
surface, removal of all clots, for by these hemorrhage is encouraged,
and by including the open vessels in ligatures. For the accomplishment
of this, the period and mode of dressing, above recommended, afford
great facility, as has been already observed. Hemorrhage at a later
period is not common. It happens occasionally in consequence of the
stump having acquired an unhealthy condition, from sloughing,—or from
abscess, as when this occurs round ligatures which have been retained,
along with the slough of the vessel and cellular tissue, both ends
having been cut away. The matter formed during separation of the
ligature in the usual way, escapes readily along the protruding end,
but when there is merely a knot, the integuments have most probably
closed over, there is no direct outlet; the matter is confined,
and causes ulceration of the coats of the vessel as well as of the
surrounding tissues. In this kind of hemorrhage, it is needless
to attempt finding the bleeding point by tearing open the stump,
separating any adhesions that may have formed, causing much pain and
retardation of cure. And even though the bleeding vessel or vessels
could be found, they are not in a state to hold a ligature. The artery
is surrounded by sloughing cellular substance, its coats are tender,
and in no condition to assume a healthy action necessary for permanent
closure after deligation. If ligature is applied, the included
part quickly separates, and then the vessel is as open as before.
Astringents, and even the cautery, are useless. Ligature of the main
arterial trunk, above the origin of branches supplying the stump, so as
to weaken for a time the circulation, is found to be effectual. I have
had recourse to this in many cases, and uniformly with success. Some
years ago, several occurred in the Royal Infirmary, within a very short
time of one another; it was during rather an unhealthy season, and at
the time I was making trial of cutting off both ends of the ligatures.
They were all after removal of the lower limb; one patient died—the
amputation was high, through the trochanter minor, and the vessel tied
secondarily was the common iliac; this had the effect of completely
arresting the hemorrhage, but the previous loss of blood proved too
much for the system to recover from; transfusion was had recourse
to, and produced temporary benefit. The others, cases of amputation
below the knee, made most favourable recoveries after ligature of the
superficial femoral, and in more than one the stump healed very rapidly
after its readjustment. Indeed, it is not unfrequently found that when
the flaps are separated, from whatever cause, and replaced when the
granulations have appeared, there follows a rapid union and cure.
When healing by the first intention has failed, fomentation and618
poultices are generally the most grateful and beneficial applications
for a day or two. Afterwards, when suppuration has been fairly
established, and the stump begins to be flabby and œdematous, simple
dressing and uniform support by bandaging are required, sometimes along
with compresses on particular points to prevent lodgement of matter.
Sometimes the secondary hemorrhage is not an arterial and rapid flow,
but a slow and continued oozing from a cavity, ulcerated, dark, and
angry, round the end of the bone; this seems to arise from diseased
action in the cancellated tissue of the bone. Removal of the coagula,
stuffing the cavity with dry lint, and the application and continuance
of firm pressure, generally suffice for its arrestment.
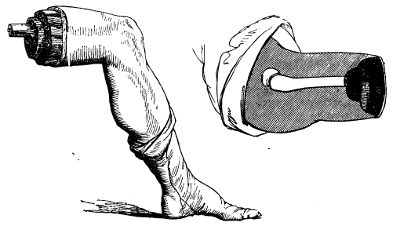
Hitherto, these general observations on amputation have regarded the
operation by flaps only; the circular method has not been mentioned.
The reason is, that the circular amputation has been, it is hoped,
in a great measure abandoned in this country. And its inferiority to
the method by flaps is so obvious, and so generally acknowledged,
that detail of the different steps of the operation is, I conceive,
here altogether unnecessary. It is more tedious in performance, more
painful to the patient, does not afford so good a covering for the end
of the bone, and consequently not so convenient and useful a support
for an artificial limb, and the cure of the wound is protracted. The
stump is almost always conical, the end of the bone is, ultimately at
least, covered only by integument, and from even very slight pressure
this is apt to ulcerate; exfoliation of the bone follows to a greater
or less extent, or unhealthy nicer of the soft parts continues, along
with caries of the bone, and partial death of its surface; and at
length it becomes necessary either to perform a second amputation or
to curtail the length of the bone. It may sometimes succeed tolerably
well when there is but one bone: when there are two, it is altogether
inadmissible. In very muscular limbs, when amputation is demanded on
account of destruction of the bones and joints, with laceration of the
soft parts, as when the patient is not required to have pressure made
on the stump, it suits well to619 make the flaps of integument only, and
to cut the muscles short, as will be noticed more fully afterwards. The
advocates for the circular amputation, my excellent friend Sir George
Ballingall, and others wish it to be believed, (and this is their
main argument,) that the exposed surface of the flaps is much greater
than that in their favourite method. Some of the philosophers of the
Modern Athens have been appealed to, and have measured, it is said,
the area of the one and the other, and given their verdict in favour
of the round about incision. The accompanying drawings from nature,
and the corresponding diagrams, speak pretty plainly in favour of the
other method. In the first there is a cone formed by the cut skin
and muscles, with a corresponding hollow and ragged cavity; and the
second set shows two smooth, nearly triangular surfaces, which the said
philosophers may measure and report upon at their leisure.
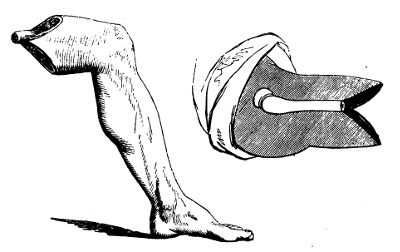
Various accidents and diseases require removal, either primary or
secondary, of the fingers, or of parts of them. Amputation is most
easily accomplished at the articulations, and ought therefore always
to be performed at these points, when the circumstances of the case
permit. The last phalanx may require removal either on account of
severe injury, or from incurable disease, as onychia maligna, necrosis,
caries, &c. The operation is one by single flap, and may be conducted
in one of two ways. The doomed phalanx is grasped, on its anterior and
posterior aspects, by the fore and middle fingers of the left hand;
and the articulation is flexed almost to the full extent, in order
that incision into it may be facilitated. A straight, narrow, and
sharp-pointed bistoury is carried in a semicircular sweep over the back
part of the joint, so as to divide the integuments, and open completely
the articulating cavity. The remaining ligamentous investments of the
joint are divided by one or more additional touches of the knife, so
as to loosen the base of the phalanx. The fingers of the left hand
are then changed from the fore and back parts of the phalanx to its
sides, the edge of the knife is passed behind the base of the bone,
and the surgeon, by carrying the blade forwards620 and downwards, forms
a flap of sufficient dimensions to cover the wound, and removes the
offending part. There is seldom any trouble from hemorrhage; no
ligatures are required. The flap is turned up so as to form a cushion
over the exposed surface of the middle phalanx, and is retained so by
the adhesive composition formerly mentioned, or by one or two turns
of a linen bandage. The other method of operation is the reverse of
the preceding. The joint is extended, the bistoury is made to transfix
close to the joint and at its anterior part, and by then carrying it
downwards and forwards, as before, a similar flap is formed; this
is retracted by an assistant, and with one sweep of the knife the
articulation is divided from before backwards. By either method the
flap is the same. By similar procedure the amputation at the middle
articulation is performed.
It is sometimes an object to save as much as possible of the proximal
phalanx, when amputation is rendered necessary by disease of the middle
articulation, or of the distal extremity of the bone. In such cases,
two semicircular flaps are made by cutting from without, either on the
lateral, or on the thenal and anconal aspect, and the bone is divided
either by a small saw or by the cutting pliers. The flaps are retained
in apposition, and the bleeding arrested by bandaging.
Amputation at the proximal articulation is also performed by double
flap. In the previous operations an assistant steadies and supports
the hand; in this he has likewise to bend the rest of the fingers,
and to separate as widely as possible those neighbouring to the one
about to be removed. The operator seats himself before the patient,
grasps the finger so as to manage its movements with the left hand,
and holding the knife perpendicularly, with its point upwards, lays
it over the knuckle, and carries it obliquely upwards so as to open
that side of the articulation. He then pushes the finger towards the
opposite side, and with the point of the knife completes the loosening
of the articulation; for this the blade of the instrument should never
be employed, otherwise the integument will be cross-cut and mangled.
After separation of the base of the phalanx by the point, the blade
is passed behind, and carrying it downwards and outwards, a flap is
formed similar to the first—both proportioned to the size of the wound
which they are to cover, and the bone which they are to protect. The
fingers may also be removed by the oval method, as described and
delineated in the Practical Surgery. The flaps are retained in
contact by bringing the neighbouring fingers towards each other. This
also suffices, in general, to suppress the bleeding, but sometimes one
or both digital arteries require ligature. At first, cold cloths are
probably the best applications, with the view of stopping the oozing,
and warding off inflammatory action. Vascular excitement is very apt
to follow this amputation, when performed for disease of the finger,
as after neglected or severe whitlow; the soft parts in which the
incisions are made are generally infiltrated and condensed, and prone
to inflammation. The surface around is red, tense, and shining, on
the second or third day; the back of the hand, the palm, and perhaps
the forearm, are then involved in inflammation of the surface, and
infiltration of the cellular tissue; and in all probability, free
incisions, followed by poultice621 and fomentation, will be necessary
to restore the parts to quietude. Such consequences are to be guarded
against as much as possible, by attention to the system, and by
avoiding all irritating dressing.
The phalanges of the thumb are removed in the same manner as those of
the fingers. Amputation of the metacarpal bone is accomplished thus.
The thumb is grasped by the fingers of the left hand, and so managed.
The bistoury, held in the same manner as for amputation at the proximal
articulation of the finger, is placed with its point on the web betwixt
the thumb and forefinger, and carried in one sweep rapidly upwards in
a slightly oblique direction, till it is stopped by the os trapezium.
The point is used to effect disarticulation, the member being at the
same time pushed steadily outwards; the blade is then placed behind
the base, carried downwards close to the side of the bone, and is not
to be brought out till sufficiently low down for forming a flap to
cover the whole wound. The flaps may be formed otherwise, and much more
handsomely, by transfixion of the ball of the thumb, as shown in the
Practical Surgery, p. 360. After arresting the hemorrhage, the flap
is laid smoothly down, and retained in its proper position by bandage
or slips of the adhesive plaster. The metacarpal bone of the little
finger is removed by the same method of incision as for the thumb.
In amputation of the fingers, the incisions sometimes require to extend
beyond the proximal articulation, on account of disease having involved
that part; in other words, it may be necessary to remove more or less
of the metacarpal bone along with the finger. The method of incision
will vary according to the extent to which the bone is diseased. When
the operation is required for disease of merely the distal extremity,
the incisions are made in the same form as for amputation of the joint,
only they are on each side sufficiently high to be beyond diseased
bone. They may either be made from below upwards in the usual way, or
be commenced at their highest point on the dorsum of the metacarpal
bone. After the soft parts have been separated from the bone, by a
few touches of the knife after formation of the principal incisions,
removal is completed either by the cutting pliers or the metacarpal
bow-saw—the former I have found the more convenient instrument. It is
applied perpendicularly, and should always have its smooth surface in
contact with the part to be retained, otherwise the cut part will be
rough and irregular. Section is completed more rapidly than by the
saw, and, by attention to the above precaution, the stump is equally
smooth, if not more so. The wound is brought and retained in contact
by approximation of the fingers. But in taking away any considerable
portion of the metacarpal bone, it is of importance to preserve the
palm uninjured. With this view, the knife is entered over the centre
of the bone on its dorsal aspect, above the diseased part, and carried
straight downwards till near the articulation, when it is made to
diverge for the formation of lateral flaps; the integuments in the
track of the longitudinal wound are then dissected backwards, so as to
expose the bone completely, and the bistoury is passed round the bone
throughout its whole extent, the edge being kept close to it,—in order
that the soft parts may be separated, and that without unnecessary
width of wound or implication of the palmar arches and branches
proceeding622 from them. Then the bone is clipped at the proper point by
the cutting pliers; or the section of the bone may be performed before
separation of the soft parts from its under surface, as, by raising
the cut end, this part of the operation may be facilitated. Here the
metacarpal saw is inapplicable.
Before quitting this part of the amputations, it may be observed, that
no good can result from taking away a metacarpal bone and leaving a
finger, or from removing a proximal phalanx and leaving the distal. The
parts so left can be of no use, they have no support, and the muscles
cannot act upon them: they must prove an incumbrance, and as such will
either form the subject of a second amputation, or remain a proof of
the unsuccessful result of the first.
Amputation in the forearm, may be necessary at various points, on
account of accident or disease, but should never be resorted to, in
either case, so long as part of the hand can be saved. The preservation
of even a small portion of this useful member, even of one finger or
a part of one, is of great importance to the patient. When, however,
this is hopeless, all must be removed; and, if the wrist be sound,
amputation may be performed at that joint. Hitherto, no mention
has been made of the temporary suppression of bleeding, for in the
amputations detailed there is scarcely ever any necessity for adopting
such measures; but in those of the forearm and arm, a steady assistant
must be placed ready to compress the humeral artery as soon as the
incisions are commenced; in the case of the forearm, the pressure is
made on the lower portion of the artery; in the arm, the point of
pressure will necessarily depend on the point of removal. The patient
may be either seated or recumbent. One assistant compresses, another
steadies the limb in the supine position. The surgeon holds the hand in
his left, standing on the inside of the right limb, and on the outside
of the left. Suppose the right wrist is to be operated on,—the end
of the ulna is felt for, and at that point the knife is entered, and
drawn across the wrist on its dorsal aspect in a semilunar direction,
the convexity of the curve of course pointing towards the fingers. The
joint is opened by retracting and dissecting back the flap so formed;
the knife is then passed behind the scaphoid and lunar bones, which
are exposed and turned out by division of the ligaments, and by rapid
and gentle sawing motion downwards and forwards, a flap of sufficient
size is then formed on the palmar aspect. The dorsum of the hand may
be so diseased or injured as not to afford sufficiency of sound parts
for a posterior flap; in such circumstances the anterior must be made
proportionally large, that it may alone cover the ends of the bones.
After suppression of the bleeding, the flaps are approximated by one
or two points of suture; these are afterwards removed, and their place
supplied by the adhesive plaster.
Amputation, at any point between the wrist and elbow-joints, requires,
in all, the same method of incision, but the nearer to the elbow the
better is the stump; at the wrist the flaps are composed principally
of integuments and tendons, and the cushion so formed for the bones
is very inferior to one of muscle. Compression is made and the limb
steadied as before; the surgeon with his left hand grasps623 the wrist,
and places the forearm in the middle state between pronation and
supination. In the right forearm, the knife, held perpendicularly, is
entered over the centre of the radius, and its point, after reaching
the bone, is inclined inwards so as to pass round it; transfixion is
then made, the knife passing close to the palmar surface of the bones,
and emerging at a point opposite to its entrance; and then by rapid
motion downwards and inwards, a proper flap is formed. The instrument
is again introduced over the radius, at a little distance from the
upper part of the first wound, and passed on the opposite side of the
bones, emerging also in the first incision and at a similar point;
another flap is made. These are retracted, the knife is swept round the
bones, and passed freely between them, to divide the remaining muscular
substance, and after this has been completed, the saw is applied.
During the sawing it is well to preserve the limb in the same position
as during the incisions, and to apply the instrument perpendicularly;
thus both bones will be divided at once, and the risk of splintering
diminished. In transfixion, great care is required that the point of
the knife pass across, not between, the bones, and with this view a
slight change of position is useful; during the transfixion for the
inner flap, the surgeon, as soon as he feels the knife rounding the
radius, rotates the forearm gently inwards, and in transfixing for
the outer flap similar rotation is made outwards. In this situation,
and others where the soft parts are less thick in one aspect than
the other, it is by much a preferable plan to make a flap first, by
cutting from without inwards, as already described in regard to the
wrist, and then to transfix for the formation of the second flap. This
is delineated in the Practical Surgery, p. 367. Sometimes slight
difficulty is experienced in tying the interosseal artery. The flaps
are brought together, and treated in the way already mentioned.
In all amputations of the upper extremity, it is of importance, and
indeed a rule scarcely to be departed from, to leave as much of the
limb as possible; for here the longer the stump, the more useful is
it to the patient. In accordance with this maxim, amputation at the
elbow-joint may be required, when either disease or injury extends too
high for amputation in the forearm, but not too high for the formation
of an anterior flap over the joint. The limb is steadied in the supine
position, compression being made near the middle of the humeral artery;
the knife is passed horizontally across the condyles close to the bone,
and brought downwards and forwards to a sufficient extent for the
production of a flap, which is alone to form the protecting cushion.
The joint is then cut through, the knife is passed down till obstructed
by the olecranon, and with one sweep a semicircular incision of the
posterior integument is made. All soft parts in this line are divided,
and then the saw is applied to the olecranon process. This amputation
is easy, rapid, and beautiful in execution; and, when the flap is
sufficiently large,—as it always may be, for there is no want of soft
parts in front,—the stump is well formed and useful. The flap is laid
down, and attached by suture to the integument posteriorly; in due
time the adhesive dressing is applied. The circumstance of a secreting
surface forming the stump does not seem detrimental, either here, or in
the wrist-joint. The synovial fluid soon ceases to distil, and union
is not interrupted by it. There624 is no necessity for scarification,
or scraping the cartilage, with the view of hastening cessation of
secretion and granulation of the surface.
Amputation of the arm is performed by the formation of lateral flaps,
at any point below the insertion of the deltoid muscle. Compression
is made on the upper part of the humeral, or on the axillary artery.
The limb is held well separated from the side; and care should be
taken that, when so raised, its height be convenient to the operator.
The knife is entered perpendicularly to the shaft of the bone, passed
fairly down to it, and then inclined along its side; the operator now
grasps the limb below the line of incision with the left hand, and
pulls the muscles towards him—it is supposed that the right arm is
being amputated, the surgeon standing on the inside, and an assistant
supporting the forearm—and then completes transfixion, inclining the
handle of the knife towards himself, in order that its point may pass
round the bone and emerge at as distant a point in the circumference
of the limb as possible. By a rapid sawing motion, downwards and
inwards to the proper extent, the inner flap is formed; and by
attention to the grasping of the muscles and the inclination of the
knife, its base is so large as to admit of the more easy performance
of accurate transfixion for the outer—that is, the instrument is more
easily brought through the same incision. The assistant seizes the
extremity of the inner flap as soon as formed, and retracts it, but
only to a slight extent; it is simply held out of the way. If it be
pulled backwards, as in retraction during sawing, the formation of the
second will be much impeded. The knife is again entered about half an
inch below the commencement of the first incision, and by inclining
the handle the point is brought round the bone, and made to appear on
the opposite side also in the first incision; this is facilitated by
pulling the soft parts outwards with the left hand. Then the outer
flap is completed. The knife is swept rapidly round the bone, so as to
expose it completely at the upper part, the assistant at the same time
retracting the flaps fully. The saw is applied, the arteries tied, the
flaps approximated, and the operation completed.
In performing the second transfixion, the reason why the knife is
entered lower than in the first, is, that cross-cutting of the corners
of the wound is thereby avoided. For a long time I was surprised and
annoyed to find many stumps present an unseemly cross-cutting of the
integument at the upper parts, particularly after approximation of
the flaps, although the incisions seemed to have been made smoothly
and accurately. It is occasioned by the sawing process for making the
second flap, and when this is commenced at the same height as for the
first, irregularity of incision at the upper part is unavoidable. The
precaution, however, of making the second transfixion considerably
lower than the first I have found quite effectual. The disparity
between the bases of the flaps is readily and quickly remedied, after
their formation, by a sweep of the knife upwards on the lower side.
Irritable and painful stumps are more frequently met with after the
amputations of the arm and forearm than any other. The occurrence,
however, is less common than formerly, and this may625 be fairly
attributed to the improvements in the operation—to the method by
flaps having superseded the circular, and nothing but the arteries
being surrounded in ligature. Still the affection is occasionally met
with, and there can be none more painful and troublesome. Generally,
no obvious cause can be found for the attack of this malady; but in
some of the cases there would seem to be a constitutional and innate
tendency, as it were, towards this irritability of the cut and bulbous
extremities of the nerves—as in the following case:—A gentleman, aged
53, underwent amputation of the thumb, in consequence of laceration of
the hand. Amputation was very soon afterwards performed at the middle
of the forearm, on account of hemorrhage and infiltration of the hand,
after fruitless attempts to secure the arteries. After cicatrisation
of the wound, he complained of great pain in the stump, and in the
situation where the tourniquet had been applied. Amputation of the arm
was then performed, but the stump was not well made. The pain returned,
and he applied to me, with the view of again submitting to amputation.
It was performed nearer to the shoulder-joint, and in order to guard
against recurrence of the disease, the nerves were laid hold of, pulled
outwards, and cut across as high as possible. The patient was relieved
of many of his sufferings, and continued tolerably comfortable for
nearly two years; again, however, the painful symptoms have returned,
though in a slighter degree. On examining the removed stump, all the
nerves, particularly the musculo-spiral, were found greatly enlarged
in their extremities, and intimately adherent to the cicatrix and the
ligamentous covering of the rounded extremity of the humerus. More
desperate operations have even been performed to free patients from
irritable stump. The lower limb has been hacked off bit by bit, even
to the coxo-femoral articulation, without much, if any, relief. Such
operations are hardly warrantable.
Amputation at the shoulder-joint is more frequently required for
accident than for disease. It has always been the custom to trust for
suppression of bleeding, during this operation, to the hands of an
assistant; and when the method has been found effectual in the case of
the large axillary artery, why should it be objected to, on the score
of inefficiency, in the minor amputations? particularly when it is
evident, putting efficiency out of the question, that it is preferable
to compression by the tourniquet, or any other circular apparatus;—more
quickly applied and relaxed; less painful, less formidable; always
ready, and independent of the instrument-maker. The compression is made
above the clavicle, so as to secure the subclavian, where it passes
over the first rib. The thumb of a steady assistant is placed deeply
into the cavity of the lower triangular space of the neck, immediately
above the first large sinuosity of the clavicle. The pressure thus made
is quite effectual; but as it requires to be firm and uniform, and as
there is always a risk of the thumb giving way from exhaustion, it is
better to interpose some mechanical contrivance when the assistant is
either diffident or inexperienced. The best apparatus for this purpose
is a common door-key. A bit of lint or cloth is wrapped round the
handle, and this part is then pressed down626 on the vessel. As in other
amputations, the pressure is not commenced till the knife is about to
enter.
The flaps may be double, on the outer and inner aspects, or one may be
made sufficiently large to cover the whole wound. The patient is seated
on a chair, and secured by a person placed behind. The arm is raised
a little from the side, and supported by an assistant. Two oblique
incisions are made, commencing high on each side of the shoulder, and
converging gradually till they meet near the insertion of the deltoid.
The triangular flap, so marked out, is dissected rapidly upwards, close
to the bone, and kept raised by an assistant. The person supporting the
arm then uses it as a lever, carrying it downwards and backwards; the
joint, thus made more palpable, is cut into by a semicircular sweep
of the knife across it; the head of the bone is now dislocated, and
the rest of the capsule and fibrous tissue exterior to it divided;
the blade of the knife is insinuated behind the head of the bone, and
carried rapidly through the remaining soft parts. In no amputation can
I conceive any necessity for suspending the incisions, in order to
secure vessels, provided the pressure is well applied, and the knife
used dexterously. Here very little blood should be lost. The vessels
divided in the formation of the flap are small, and the axillary is not
cut till the incisions are nearly completed; as soon as the limb has
dropped, the surgeon places his finger on the mouth of the artery, and
then applies his ligature as quickly as possible; the pressure may now
be removed, and the minor vessels secured leisurely. The flap covers
the wound completely, and is easily retained.
Or two flaps may be made by transfixion. In operating thus on the right
limb, the surgeon, standing in front of the patient, enters the knife
a little below the point of the acromion, passes it across the outer
aspect of the joint, and by inclination of the handle outwards, makes
its point to appear on the inside of the outer margin of the axilla; by
carrying it downwards and outwards to a sufficient extent, the outer
flap is formed. This is immediately elevated by an assistant, and then
the arm is pushed upwards, and across the chest, so as to render the
joint more accessible; the ligaments are cut, the bone disarticulated,
the knife passed beyond its head, and placed with the edge parallel to
the shaft of the humerus, and the arm restored to its former position;
the inner flap is then made by carrying the instrument downwards and
inwards. In the left limb, the knife is entered on the inside of the
outer border of the axilla, and brought out below and in front of the
extremity of the acromion, reversing the order of the former incisions;
after the outer flap has been so formed, the joint is cut across, the
knife passed beyond the head of the bone, and the inner flap made as
before.
Accidental injury, as already stated, is the most frequent cause for
amputation at this part, and this will always influence the method
of incision. There is nothing peculiar in the after-treatment of the
stump. But it ought always to be remembered, that the operation is one
of great severity; that a large part of the body has been suddenly
removed; that, consequently, there is risk of the mere shock being
dangerous, and of an untoward constitutional condition supervening—and,
therefore, the after-attendance should be zealous and careful.
627
The phalanges of the toes are removed in the same way as those of
the fingers. This latter operation may be required on account of bad
onychia, large exostosis or injury. This and the other must also
be removed on account of diseased bone, such as here represented
with affection of the interposed joint. The osseous shell formed
by the enlargement of the original tissue encasing a segmentum is
well represented. In the amputation at the proximal joint, it is to
be recollected that the extremity of the metatarsal bone lies more
removed from the web of integument betwixt the toes than the metacarpal
bone does from that of the fingers. The incision upwards, therefore,
requires to be deeper; but in other respects the operations are
precisely the same.
In amputating at the proximal articulation of the great toe, there is
often a difficulty in obtaining a sufficient covering for the wound, on
account of the presence of the sesamoid bones, and the general bulging
of the heads of the bones. The knife is entered on the dorsum of the
metatarsal bone, about half an inch above the joint, and then inclined
to each side, marking out lateral flaps of considerable length;
these are then reflected,—in making the outer, the instrument being
dextrously passed round the sesamoid bone,—and the disarticulation
completed.
In removing the great toe, along with the metatarsal bone, the bistoury
is entered over the articulation of the metatarsal bone with the
tarsus, and carried straight downwards, along the centre of the dorsum
of the bone, till near its extremity; it is then inclined to each
side, in the manner described for amputation of the metacarpal bones.
The integuments are dissected off on each side of the longitudinal
incision, and the knife run up along the inside of the bone, till
stopped by the tarsus. The surgeon now presses the toe outwards, so as
to assist the disarticulation; and after this has been completed, the
bistoury is carried downwards, close to the outside of the bone, and
not brought out till past the lower articulation. The external flap
thus formed is then laid accurately down, so as to cover the wound, and
retained. The preferable mode of making the flap, so as to expose the
metatarsal bone for division or disarticulation, is well illustrated
in the Practical Surgery, p. 375. The entire bone628 must be removed
in such cases as that here sketched. In cases in which the shaft is
comparatively sound, and the disease is principally seated in the
articulation with its distant extremity, the shaft may be divided with
the cutting forceps at a point sufficiently removed from the disease.
The operations on the other metatarsal bones are the same as those on
the metacarpal. They may be removed, either entirely or in part, along
with the corresponding phalanges, by operative procedure similar to
that practised on the hand.

Sometimes disease of the foot is not so extensive as to require
or justify removal of the whole organ; the metatarsal bones are not
involved throughout their whole extent. The same remark applies to
injury by accident. In such circumstances, amputation is performed at
the articulation of the metatarsal bones with the tarsus. The operator
first ascertains the exact site of these joints, and then transfixes
the foot at that point, passing the knife close along the plantar
aspect of the bones; carrying the instrument downwards, a sufficient
flap is formed to cover the stump, or a semicircular flap may be made
and reflected by cutting from without inwards. The integuments on the
dorsum are then divided in the line of articulation, the joints divided
successively, and the parts removed. The flap is raised, adjusted,
and retained. In dividing the articulations, it is to be recollected,
that the base of the second metatarsal bone, reckoning from that of
the great toe, is lodged considerably higher than the others; and,
therefore, the knife must be inclined upwards at that point, or
else the use of the saw is requisite. The stump thus formed proves
exceedingly useful: the subsequent lameness is not great; the heel and
tarsus compose a very efficient support for the weight of the body, and
the flexion is unimpaired; by attention, too, the deformity may be in a
great measure concealed. In short, the surgeon who amputates above the
ankle, for disease or injury not extending to the articulation of the
metatarsus with the tarsus, is guilty of a serious error.
The disease may reach higher than is compatible with the preceding
operation, and yet it may be possible to save the heel. In such cases
amputation is performed in the articulations of the os calcis with the
os cuboides, and of the astragalus with the os naviculare. The plan of
the incisions is the same as that for the operation at the bases of the
metatarsal bones.
No amputation is more frequently performed than that of the leg.
Operation near the ankle is inadmissible; sufficiency of soft parts,
for the protection of the stump, cannot be procured lower than
the629 calf. Incision is completely limited to two points, either
immediately below the tuberosity of the tibia, or in the bellies of
the gastrocnemii. The former is the situation to be preferred in
hospital practice, and amongst the lower orders generally; the latter
is suitable to the better classes of society, that is, to those who
can afford to purchase an expensive artificial support. The amputation
below the tibial tuberosity being the most frequently required,
will, with propriety, be described first. Suppose the right leg is
to suffer:—The operator places himself on its inner side, according
to the general rule formerly inculcated, and grasps the lower part
of the limb with his left hand, an assistant supporting the foot at
a proper height, and controlling motion. The knife is entered over
the fibula, on its outer aspect, and carried upwards along that bone
for an inch and a half, or two inches; it is then brought across the
limb in a semilunar direction, the convexity of this incision pointing
towards the foot, and after reaching the inner and lower part of the
tibia transfixion is performed, the instrument being pushed along
the posterior surface of the bones, and made to emerge at the upper
part of the fibular incision. By then carrying the knife downwards,
a posterior and larger flap is formed sufficient to cover the stump.
All this is effected by uninterrupted sweeps of the knife, that is,
without ever removing the point or edge from the track of incision.
The integuments on the fore part are then dissected upwards a little,
by a few touches of the knife, so as to form a small semilunar flap;
at this part of the operation there is no necessity for laying down
the knife and using a bistoury. The muscles in the interosseous space
are then completely divided, and the knife swept round the bones to
detach the soft parts still uncut. The saw is applied, either in a
horizontal or perpendicular direction; I prefer the latter for reasons
already assigned. The vessels are secured, and there are generally but
three—the popliteal, and two sural. I now generally aim at cutting
the vessel before it divides, and seldom fail in doing so. There is
then possibly the popliteal only requiring ligature, and there is less
chance of secondary hemorrhage. This has occurred, so as to prove
fatal at a considerable period after the operation, in consequence of
the posterior tibia being cut close to its origin, and no clot having
formed in it. Before adjusting the flap, it is well to assist nature
in rounding off the end of the tibia, and thereby prevent danger to
the integument; with this view the sharp anterior ridge of the bone
is cut away and rounded off by means of the pliers. This must be done
sparingly if at all, and with great caution. The nipped surface is
liable to exfoliation, or the medullary web is apt to be injured, and
this is inevitably followed by more or less death of bone. To some the
fibular incision may appear unnecessary; but I have long practised
it from conviction of its advantage. It is an excellent mark for
transfixion, and assists greatly in preventing entanglement of the
knife betwixt the two bones; besides the soft parts in this situation
must be divided at one or other step of the operation, and hence the
procedure cannot be objected to on the ground of causing unnecessary
wound. In operating on the left limb, there is not the same danger in
transfixion, and consequently so long a preliminary630 incision on the
inside is not requisite; in other respects the steps of the operation
are the same as for removal of the right. In muscular subjects two
semilunar flaps had better be made, one from the anterior aspect of the
limb, the other from the posterior, the muscles being cut short in the
ham, and the incision made to reach the popliteal artery.
It has been proposed to excise the head of the fibula after formation
of the flap, instead of sawing it across at a corresponding point
with the tibia. At one time I put this modification into extensive
practice, with the effect of improving the appearance of the stump
very considerably; but in several cases, untoward consequences took
place. Discharge of synovia occurred on the second day, followed
by very profuse suppuration, which proved of long continuance, and
very exhausting; in more than one case, the joint became anchylosed,
rendering the stump very inefficient as a means of support, in
consequence of being fixed at an inconvenient angle; and one patient
sank, exhausted by the profusion of the discharge. I then found, from
repeated examination of the parts on the dead subject, that it was
very difficult, nay impossible, to excise the head of the bone without
dividing the capsular ligament, and wounding the synovial pouch, or
opening a bursal cavity, beneath the popliteus muscle, communicating
with that of the knee-joint. It is scarcely necessary to add, I have
since wholly abandoned this method of operation.
It has been already observed that high amputation of the leg is
preferable amongst the working classes. The limb is of much greater
use to the patient than were the stump longer; he is able to follow
his occupation with greater ease and security, and at less expense,
by resting on the knee, than by using the artificial limb applied to
the middle of the leg. The wealthier patient, however, can afford a
more expensive support, and a less efficient, though more handsome
continuation of the limb suffices. In such circumstances, amputation
is performed at the middle of the leg; after cicatrisation, the artist
supplies an artificial support resembling the natural limb; and thus
the motion of the knee is preserved. The same directions apply to this
operation as to that immediately below the knee.
In amputation of the thigh, the same method of incision is followed
as in amputation of the arm. But, according to the point of removal,
the direction of the flaps varies. If in operating high in the limb
the flaps be made laterally, there will be imminent risk of the bone
protruding through the upper part of the wound; for the patient
uniformly raises the stump towards his abdomen. No antagonist muscular
power is left to oppose the action of the muscles inserted into the
trochanter minor, and the elevation of the stump is involuntary: it
always occurs to a remarkable extent in young persons. On this account,
anterior and posterior flaps are here far preferable to the lateral;
for then the more the stump is raised, the better is the end of the
bone covered—the anterior flap folds over it. Transfixion is therefore
made horizontally; and the posterior flap should be a little longer
than the anterior. But in the lower part of the limb, lateral flaps
are not only not liable to the same objection, but preferable to the
anterior and posterior. In the neigh631bourhood of the knee-joint, the
soft parts consist almost entirely of ligamentous tissue on the fore
and back part, and proper cushions can be obtained only from the sides.
Transfixion is therefore made perpendicularly. Thus the bone will be
well covered by parts likely soon to adhere; and there is no risk of
protrusion, for muscles are left to counteract the elevators, and there
is sufficient lever in the limb whereby to control its motions. And
it may be here mentioned, that after all amputations, when startings
of the muscles are not only painful, but disturb the position of the
stump, the limb should be bound down by a broad band, passed across it
a short way above the wound, and fastened firmly at each end to the bed
or pillow; at the same time anodynes are to be administered. I have
long since come to the conclusion that the femur in amputation should
not be sawn lower than its middle; the method by anterior and posterior
flap is therefore the only one applicable.
Amputation at the hip-joint is deservedly ranked amongst the most
formidable operations in surgery. It ought, therefore, never to be
performed but as a last and necessitous resource for the salvation
of life. At the same time, when necessity for it is obvious and
acknowledged, and no other means can be of any avail, hesitation and
delay should never take place; otherwise the last and only chance of
saving the patient will pass away, and the operation, when at length
performed, will but hasten his exit from this world,—and besides
inflict an injury to science, by intimidating practitioners, and
affording subject of reproach and ridicule to the thoughtless and
uninformed part of the public. I prefer the formation of anterior
and posterior flaps,—as follows:—The patient is placed recumbent on
a firm table, his nates resting on, or rather projecting a little
over, the front edge. The sound limb is separated from the one to be
removed, and held aside by an assistant. Or it is secured to the foot
of the table by a towel, the necessity for an additional assistant
being thus done away with, and more freedom in his movements afforded
to the operator. Indeed, in all amputations of the lower extremity,
this is the preferable method of fixing the sound limb. The other
limb is supported by an experienced and intelligent assistant, who
understands, and is able to perform, the movements to facilitate the
different steps of the operation. The compression is intrusted also to
an experienced and steady assistant, who, standing by the patient’s
side, presses firmly with one or both thumbs on the femoral artery,
where it passes over the pubes; and in this more than in any other
operation should the pressure be delayed till the instant of incision,
for otherwise the blood lost in the limb will be immense. Transfixion,
by a knife proportioned in size to the dimensions of the limb, is made
horizontally, the instrument being passed in a somewhat semicircular
direction, so as to include as much of the soft parts as possible; an
anterior flap is made by cutting downwards. During the passage of the
knife across the joint, the assistant rotates the limb a little, so as
to facilitate the bringing of the instrument out with its point well
inwards; in the left limb the rotation will be inwards, in the right
outwards. After formation of the flap, the assistant abducts forcibly,
and presses downwards; the joint is opened, the round ligament cut,632
the capsule divided, and the blade of the knife placed behind the
head of the bone and the large trochanter; the posterior flap is then
made rapidly. After transfixion for the superior flap, and when the
sawing motion downwards has advanced but a little way, the compressing
assistant shifts one of his hands into the incision, immediately behind
the back of the knife, and so obtains a firm grasp of the femoral
artery previously to its division. He retains this hold, at the same
time retracting the flap, during the rest of the operation. As soon as
the limb has been separated, the surgeon secures the vessels on the
posterior flap, partly by his fingers, partly by compression with a
large sponge, and ligatures are applied as quickly as possible. The
femoral is secured last; for, as long as the assistant retains his
hold, hemorrhage from it is not to be dreaded. Thus, when both surgeon
and assistants are quick and cool, the operation may be completed
with the loss of much less blood than might be expected. I have had
occasion more than once to perform this operation, and thus speak from
experience. In cases of accidental injury requiring this operation, the
lever use of the limb must frequently be wanting; and in such cases,
too, the parts may be so injured as not to afford flaps anteriorly and
posteriorly. In these circumstances, the surgeon must be guided by
experience and judgment in adopting the mode of procedure which appears
most applicable; in ordinary cases the operation above detailed appears
the preferable.
Excision of diseased portions of bones, is practised occasionally
with the view of removing a source of irritation and exhaustion
from the system, without sacrifice of a limb. When the operation
proves successful, the beneficial effect on the general health is
as remarkable and rapid as after removal of the hectic cause by
amputation; the pulse falls and grows firmer, diarrhœa and sweating
cease, the hectic flush leave the cheek; in short, the constitution
makes a complete and successful rally. It is had recourse to in order
to take away disease in the following situations,—in the cancellated
articulating extremity of a long bone, in part or the whole of a short
bone, and in part or the whole of long bones. Even a long bone, from
one articulating surface to the other, may be removed; the metacarpal
bone of the thumb, and the metatarsal bone supporting the great toe,
may, for example, be taken away in their whole extent. I have seen
these bones so treated, but the result was unsatisfactory. As has
already been observed, the part of the member that is left is without
support, and not under the influence of muscle; it is consequently
loose and useless.
Operation for the removal of necrosed, or softened and ulcerated
portions of the carpal and tarsal bones, is sometimes successful. But
operative interference, either with these, or with more extensive and
formidable articulations, is not advisable unless the soft parts are
not largely involved, and when the general health is tolerably good—the
patient either having suffered less than usual, or having rallied and
begun to gain strength after exhaustion by discharge and fever. If the
ligaments, bursæ, and cellular tissue are much affected, as is often
the case, there is no chance of discharge ceasing, and the patient
regaining health, even though the bone be removed to any633 extent—a
second operation will be required, namely, amputation above the
diseased parts. And when this becomes requisite, after failure of the
first to restore or even improve the health, the patient is apt, as has
too often been the case, to sink under the accumulation of suffering.
He might, even though much exhausted, have been able to bear up against
the shock of one and a successful operation, but he cannot endure that
of a second, or perhaps third, serious and protracted attack of the
knivesman. The disappointed hope of a cure from the first operation
is a secondary, though nevertheless a sure contributor towards the
unfortunate issue.
No particular rules can be laid down for the operative procedure.
By converting two or more natural openings into one, extending the
incisions as much as possible in the direction of the limb and of
the muscles and tendons, and avoiding the course of the larger
bloodvessels and nerves, room is made for an accurate examination of
the diseased parts. A strong and firmly pointed knife is required for
these incisions, for the soft parts are much consolidated, and are
cut with difficulty. The extent of disease is ascertained both by
the probe and by the finger, and farther measures, if necessary, are
then adopted for complete removal. Loose portions of bone are taken
away; and often large sequestra of the cancellated tissue are found
lying in the cavity, either loose or easily separable; for extraction,
forceps and the fingers, and sometimes a lever, are required. A firm
scoop is useful for removing such portions of diseased cancellated
tissue as are still continuous with the shaft of the bone. When an
opening in the cancellated tissue, leading to an internal sequestrum,
is minute, enlargement is effected by means of either the trephine or
the cutting pliers: afterwards, gouges, gravers, &c., may sometimes be
useful in operating on the soft texture underneath,—but they are seldom
requisite. The bleeding from the soft parts is free; the vessels do not
retract, and may require the application of a needle and ligature. That
from the bone is easily arrested by pressure: the cavity is filled with
charpie or with dossils of lint, and these are supported by a bandage.
Some days after, this dressing is removed, having been previously
softened and loosened by fomentation and poultice. The cavity should
now be examined carefully, to ascertain whether or not all the diseased
parts have been taken away; it is then dressed daily from the bottom.
If parts of the surface assume an unhealthy aspect, the granulations
being either backward or flabby, to these escharotics should be
applied—the most suitable is the red oxide of mercury. Gradually the
cavity fills up, and a depressed, firm, and permanent cicatrix is
obtained. It need not excite surprise, however, if, in not a few cases,
after matters have proceeded apparently very favourably for some time,
the surface become pale, soft, and glistening; the discharge thin,
acrid, and profuse; the integuments around tumid and discoloured,—if,
in short, the disease be in no long time fully reëstablished.
The tarsal and carpal bones are often the subjects of this operation.
In a few cases I have removed several, in others one or a portion of
one, with success. In one instance the greater part of the astragalus
was taken away, along with the ends of the tibia and fibula. There
remained, in consequence, a large opening across the joint, through634
which a cord was passed, to facilitate gradual and piecemeal discharge
of remaining portions of diseased bone. The articulation could
actually be seen through. The seton was gradually diminished and the
aperture closed. The foot was thus preserved, and the leg was but
little shortened; the limb proved strong and extremely useful, but
the ankle-joint retained little or no power of motion. I have also
again and again trephined the os calcis, and removed large portions of
it; the cuboid likewise has been taken away, along with the base of
the metatarsal bone or bones in connection with it; in some of these
cases an excellent cure followed, in others amputation of the foot was
afterwards necessary.
Some have ventured to cut away the articulating ends of the bones
composing the knee-joint. This may be accomplished without much
difficulty. The patella is either removed entirely or turned to a
side, the ligamentous and tendinous attachments are divided, and the
ends of the bones thus exposed; by cutting close to and towards them,
little risk is incurred of wounding the bloodvessels and nerves in the
popliteal space. The saw is readily applied in a horizontal direction.
After tying the vessels, and approximating the edges of the wound,
the limb is placed in the straight position, and retained fixedly so
by the application of splints. Much constitutional disturbance is to
be expected, as well as profuse and tedious suppuration. There are
few surgeons so rash as to have recourse to this operation. One or
two patients, it is true, have lived in spite of it, retaining the
limb in a tolerably useful state. But in others,—and these constitute
the majority,—amputation was after all required, and that proved
insufficient to save the patient. In short, the results of excision of
the knee-joint do not justify its repetition.
The articulating ends of the bones composing the shoulder-joint have
been removed; and this may be done with advantage on account either of
disease or of injury. This joint is, like others, liable to ulceration
of the cartilages, either primary, or in consequence of abscess
and degeneration of the soft parts around. The disease is attended
usually with painful feelings increased by motion, and the patient is
indisposed to attempt motion. Sometimes merely weakness of the limb
is complained of, and the attention is drawn to the wasted appearance
of the muscles, particularly of the upper arm; the deltoid seems
shrunk almost to nothing. The motions above the shoulder are lost; and
abduction is impracticable. Much pain is produced by pushing sharply
the articulating surfaces into contact, and is further increased by
rotation. The enforcement of strict and absolute rest of the joint, the
establishment of a drain in the soft parts immediately neighbouring,
and attention to the general health, often prove sufficient to arrest
the progress of this disease. If, however, it is neglected, abscess
forms sooner or later. On cutting into this, and introducing the
finger, the joint is discovered to be open; the head of the bone is
found detached from the soft parts, and unsupported. Or this state
of parts may be ascertained to exist by examination through a sinus,
either with a probe, or with the finger after dilatation. In these
circumstances, an attempt may be made to check disease, and preserve
the arm, by excision of the obnoxious parts of the bone. And this
kind of operation is also justifiable when the head635 of the humerus
has been shattered by musket-shot; or when it has been exposed and
injured by a splinter, or by a large shot, and the joint laid open. The
situation and course of the incisions will be so far regulated by the
openings or wounds already existing. They should always be made in the
direction of the fibres of the deltoid, and the posterior aspect of
the articulation is preferable to the anterior. One incision, from the
back of the acromion process to near the insertion of the muscle, is
sufficient to expose the head of the bone, to allow all its remaining
attachments to be separated, and to admit of its being turned out so as
to be conveniently acted on by the saw. The head of the bone merely is
taken away. In separating the soft parts from its neck, the edge of the
knife should be always directed to the bone, to avoid the nerves and
vessels on the inside. In some cases of injury, very little additional
wound may be requisite. The glenoid cavity may, in consequence of
being seriously involved in disease, also require removal; this is
best accomplished by large cross-cutting pliers. Few vessels require
ligature. The edges of the wound are brought together; the elbow is
supported, and the arm fixed to the trunk, in order to keep the bones
in apposition, and prevent motion. This position must be retained
during the rest of the cure; and when the wound is on the outside of
the shoulder, as recommended, the dressing of it does not interfere
with the retentive apparatus. The discharge gradually ceases, and
cicatrisation is obtained, though not till after a considerable time,
at least in general. The cut ends of the bones accommodate themselves
to each other, and a sort of new joint is formed—but never strong. The
motions of the forearm are perfect, though perhaps weakened; those of
the upper arm are very incomplete. I have both performed and assisted
in the operation repeatedly, and never experienced any difficulty; a
cure has not always followed, but in some cases the limb has become
very useful.
The elbow-joint, on account of its exposed condition, is generally
regarded as the most favourable for excision. The affections of the
joints of the upper extremity are much more manageable than those of
the lower, and may generally be prevented from proceeding so far as
to end in destruction of the apparatus. By care and good management,
disease will be arrested, and the functions and motions of the parts
restored and preserved; or the articulation may become stiff, and even
though the anchylosis be complete, the limb will be very useful if the
joint have been kept in a good position. The health, if previously
undermined, is renovated, so soon as the local disease is arrested.
But some bad cases are met with, in which all the parts surrounding
the articulation are involved, and the strength wasted; in these
amputation is the only safe and effectual procedure. It is only when
the soft parts are not much diseased, when it is ascertainable that
the affection of the bone is only to a limited extent, and when the
usual means of cure have had a fair trial and failed, that excision
is admissible. In determining on the operation, the time of life and
the worldly circumstances of the patient are to be considered: a poor
man requires his limb to be serviceable in labour; handsome appearance
without utility is to him of no value. The motion and usefulness of
the arm may be in a great measure preserved, if only a636 part of the
bone of the arm, or a part of those of the forearm, entering into
the articulation, be removed; but if large portions of all of these
be taken away, the muscles will lose their support, the motions will
never be restored to any extent, and the motion that is of it will be
weak and vacillating. The joint will remain loose and powerless, and
the limb will prove to be but a useless incumbrance. Such, at least,
is the result of my experience on this subject; and I am sorry to add,
that all which has been written on it is not deserving of unreserved
belief. Many patients have, after long and severe suffering, preserved
the arm to little purpose; others have been necessitated to submit
to another operation—amputation after all; some have died after the
first, others after the second mutilation. The operation is attended
with no difficulty in execution, and this in some measure accounts for
its frequent, and it is to be suspected, indiscriminate, performance
of late years. The incisions are made on the posterior aspect of the
joint. One is placed in the mesial line, extending from about two
inches above the olecranon to the same distance below it; and from this
flaps are raised, by making either a cross-cut in the middle, or one
at each extremity; in the one case the flaps are four, and triangular;
in the other two, and quadrangular; by either method the bones are
readily exposed. A more simple form of incision, as described in the
Practical Surgery, will often be found to suffice. The joint is
opened and dislocated, and the soft parts separated to the necessary
extent from the bones. The ulnar nerve is avoided by dissecting close
to the bone. The diseased portions are then sawn off. The wound is
closed, and the arm kept bent. This operation I have performed pretty
often, the cases being carefully chosen for it, and the success has
been highly satisfactory. By the sanguine supporters of this operation,
the after-treatment is advised to be conducted so as to secure motion
in the new articulation. From this I would dissent, for if the
articulating ends of the bones have been actually cut off, the motion
may be extensive enough certainly, but both joint and limb will be
almost altogether impotent. It would be better to procure anchylosis
in the bent position, than to have the arm dangling like a flail; in
the one case the limb will be useful; in the other, ornament, and that
too of an equivocal kind, is all that it can boast. Even anchylosis, in
most cases, can be brought about only after the lapse of a long period.
In the more severe affections of this joint, amputation of the limb is
the operation which must ultimately be had recourse to, if the patient
survive; and it is better to perform this at once, than after the
experiment of excision has been tried and found wanting. I know that
parents have too often had to regret and mourn bitterly their having
departed from sound advice, and lent themselves to such experimental
trials on their offspring.
637
FOOTNOTES:
INDEX.
-
Abdomen, affections of, 412
-
Abscess
-
Adhesion, 25
-
Albugo, 264
-
Amaurosis, 275
-
Amputation, 612
-
Anchylosis, 73
-
Aneurism, 118, 121
-
Aneurismal varix, thigh, 542
-
Anthrax, 63
-
Antrum maxillare, inflammation of, 317
-
Anus, pruritus, 460 artificial, 434
-
Arterial system, diseases, 116, 121
-
Articular cartilages, atrophy and hypertrophy, 75
-
Artificial anus, 433, 434
-
Artificial pupil, 287
-
Ascites, 435
-
Axillary aneurism, 389
-
Bladder, inflammation of, 469
-
Blennorrhœa, 247
-
Bone, diseases, 94
-
Brasdor’s operation, 126
-
Bronchocele, 377
-
Bruise, 610
-
Bubo, 197
-
Bubonocele, 416
-
Bunnion, 544
-
Burns, 211
-
Bursæ, diseases of, 80
-
Calculus, in the female, 530
-
Carbuncle, 63
-
Carcinomatous tumours, 142
-
Caries, 96
-
Castration, 507
-
Cataract, 277, 279, 280
-
Chancre, 201
-
Chemosis, 259
-
Chest affections, see Thorax.
-
Chimney-sweeper’s Cancer, 495
-
Choroiditis, 274
-
Cirsocele, 417
-
Club-foot, 545
-
Compression, 226
-
Concretions, salivary ducts, 336
-
Concussion, 218
-
Congestion, 23
-
Corectomia, 287
-
Corneitis, 261
-
Corodialysia, 288
-
Corotomia, 287
-
Coxalgia, 81
-
Croup, 354
-
Cynanche trachealis, 354
-
Deafness, 375
-
Delitescence, 26
-
Dislocations, 588
-
ankle, 606
-
carpus, 599
-
clavicle, 592
-
elbow-joint, 596
-
fingers, 599
-
hip-joint, 600
-
congenital luxation, 604
-
lower jaw, 591
-
patella, 605
-
radius, 597
-
shoulder-joint, 592
-
tarsus, 606
-
wrist-joint, 598
-
Distortion of the feet, 545
-
Ear, diseases of, 373
-
Ear, polypus, 375
-
Eburnation, 75, 113
-
Ectropion, 254
-
Eczema rubrum, 211
-
Emprosthotonos, 183
-
Empyema, 410
-
Encanthis, 252
-
Encysted tumours, 151, 336, 406
-
of eyelids, 253
-
of the breast, 406
-
Enterocele, 415
-
Entero-epiplocele, 415
-
Entropion, 255
-
Epiphora, 247
-
Epiplocele, 415
-
Epispadias, 495
-
Erethismus, 211
-
Erysipelas, common, 55
-
hospital, 57
-
phlegmonous, 56
-
Erythema, 55
-
Excision, diseased bone, 632
-
Exomphalos, 415
-
Exophthalmia, 266
-
Exostosis, 153
-
Eye, diseases, 245
-
Fever, hectic, 42
-
inflammatory, 19
-
irritative, 43
-
Fistula lachrymalis, 248
-
Fractures, 552
-
clavicle, 564
-
cranium, 227, 558
-
compound, 553, 556
-
disunited, 586
-
face, 558
-
femur, 575
-
humerus, 569
-
metacarpal bones, 574
-
olecranon, 571
-
patella, 581
-
pelvis, 574
-
phalanges, 574
-
radius, 572
-
ribs, 566
-
scapula, 565
-
shoulder, 567
-
simple, 553
-
spinal column, 560
-
sternum, 567
-
tarsus, 584
-
Fractures of the tibia and fibula, 583
-
Frænum linguæ, division of, 334
-
Fragilitas ossium, 110
-
Fungus hæmatodes, 147
-
Furunculus, 62
-
Ganglia, 401
-
Gangrene, 43
-
Genital organs, affections of, 461
-
Glaucoma, 277
-
Gonorrhœa, common, 462
-
in females, 531
-
præputialis vel spuria, 490
-
Gonorrhœal lichen, 532
-
Gums, inflammation, 337
-
Gunshot wounds, 180
-
Hare-lip, 323
-
Hæmatocele, 503
-
Hemorrhage, 129, 166
-
Hemorrhoids, 445
-
Hectic fever, 42
-
Hernia, 412
-
of the iris, 264
-
cerebri, 233
-
congenital exomphalos, 415
-
scrotal, 413
-
crural, or femoral, 416
-
infantilis, 414
-
inguinal, direct, 415
-
oblique, 416
-
scrotal, 416
-
umbilical, 430
-
humoralis, 467
-
Hospital gangrene, 191
-
Humeral artery, 394
-
Hydatic tumours, 161
-
Hydrocele, 417
-
Hydrops articuli, 68
-
Hydrophthalmia, 266
-
Hydrothorax, 410
-
Hypopium, 273
-
Hypospadias, 495
-
Incontinence of urine, in females, 489
-
Inflammation, 13
-
Injuries of the head, 215
-
Iritis, 272
-
Irritation, 20
-
Irritative fever, 43
-
Joints, diseases of, 67
-
growths from synovial membranes, 79
-
hip-joint disease, 81, 91
-
loose cartilages, 80
-
neuralgic affections, 78
-
639scrofulous disease, 77
-
Keratonyxis, 284
-
Larynx, foreign bodies in, 363
-
Laryngitis, 354
-
Leucoma, 264
-
Leucorrhœa, 531
-
Ligature of arteries, 123
-
Ligature, brachial, 392
-
Ligature of innominata, 387
-
Lips, congenital deficiencies, 322
-
Lithotomy, 519
-
Lithotrity, 517
-
Lower jaw, osteosarcoma, 343
-
Lumbar abscess, 441
-
Lupus, 310
-
Luxations, see Dislocations.
-
Malignant pustule, 193
-
Mamma, diseases, 405
-
Melanosis, 142
-
Metastasis, 26
-
Mollities ossium, 110
-
Morbus coxarius, 81
-
Mortification, 43
-
Mucous membranes, inflammation, 65
-
Myocephalon, 264
-
Nasal polypi, 310
-
Nebula, 264
-
Necrosis, 103
-
Neuralgia of the rectum, 460
-
Neck, hydrocele, 381 distortion, 382
-
Noli me tangere, 310
-
Nose, diseases, 308
-
Œdema glottidis, 358
-
Œsophagus, foreign bodies, 371
-
Œsophagotomy, 372
-
Onychia, 399
-
Opisthotonos, 183
-
Ophthalmia, 257
-
Osseous aneurism, 156
-
Osteosarcoma, 154
-
Otitis, 373
-
Ovarian dropsy, 436
-
Ozœna, 310
-
Palate, congenital deficiencies, 332
-
Paracentesis abdominis, 435
-
Paraphymosis, 491
-
Paronychia, 396
-
Periostitis, 94
-
Pes equinus, 548
-
Phagædena, sloughing, 191
-
Pharyngitis, 368
-
Phlebitis, 130
-
Phlegmonous erysipelas, 56
-
Phthisis laryngea, 360
-
Phymosis, 491
-
Piles, 445
-
Polypus, 150
-
Prolapsus ani, 453
-
Pruritus of the anus, 460
-
Pterygium, 256
-
Puncture of the bladder, 488
-
Pus, 29
-
Pustule, malignant, 193
-
Rachitis, 110, 112
-
Ranula, 335
-
Rectum, affections, 445
-
inflammation, 447
-
schirro-contracted, 452
-
neuralgia, 460
-
Resolution, 25
-
Retention of urine, 478
-
Rhinoplastic operations, 312
-
Rickets, 110
-
Sarcocele, 505
-
Scalds, 211
-
Scrofula, 34
-
Serous membranes, inflammation, 66
-
Sinus, 40
-
Sphacelus, 44
-
Spina bifida, 444
-
Spina ventosa, 157
-
Sprain, 607
-
Strabismus, 292
-
Staphyloma, 261
-
Stillicidium lachrymarum, 247
-
Stricture of the œsophagus, 369
-
Struma, 34
-
Subclavian artery, 387, 389
-
Suppuration, 29
-
Sympathies, 19
-
Syphilis, 195 tertiary, 203, 209
-
640Teeth, caries, 338
-
Testis, inflammation of, 467
-
Tetanus, 183
-
Tertiary syphilis, 203, 209
-
Thecæ, collections of fluid in, 401
-
Thorax, affections of, 409
-
Thrombus, 405
-
Tongue, inflammation of, 332
-
Tonsils, abscess of, 327
-
Tonsils, inflammation of, 326
-
Trachea, foreign bodies in, 363
-
Tracheotomy, 364
-
Trichiasis, 255
-
Trismus, 183
-
Tubercle, painful, 149
-
Tumours, 134
-
adipose, 137
-
of the antrum, 304
-
of bones, 153
-
carcinomatous, 142
-
encephaloid, 142
-
encysted, 151, 336, 406
-
fibrous, 138
-
melanoid, 142
-
aneurismal, 158
-
osseous, 158
-
hydatic, 161
-
in the neck, 379
-
in the orbit, 290
-
painful tubercle, 149
-
of the scalp, 243
-
Tympanum, puncture of, 377
-
Ulcers, 186
-
of the genital organs, 195
-
Ulcers, indolent, 188
-
Urethra, stricture of, 470
-
Urinary organs, affections of, 461
-
Urinary calculi, 508
-
Uterus, affections of, 537
-
Uvula, elongation of, 328
-
Vagina, affections of, 534
-
Valgus, 548
-
Varicose aneurism, 393
-
Varix, aneurismal, 393
-
Varus, 547
-
Vein, external jugular of, 384
-
Veins, inflammation of, 130
-
Venesection, bend of the arm, 403
-
Vertebral column, diseases of, 442
-
Vesico-vaginal fistula, 534
-
Whitlow, 396
-
Wounds, 164
-
by stings of insects, 177, 178
-
of the brain, 232
-
bruised and lacerated, 175
-
of the face and neck, 347
-
gunshot, 180
-
of the palmar arches, 395
-
poisoned, 176
-
punctured, 176
-
of the scalp, 215
-
of the temporal artery, 216
-
of the intestine, 440
-
Wry-neck, 382
THE END.
*** END OF THE PROJECT GUTENBERG EBOOK 50640 ***